The patient is an 70 year old man referred for evaluation of claudication that occurred at under a block of walking. He reported no rest pain or tissue loss. He smoked heavily up to a pack a day, with congestive heart failure with an ejection fraction of 40%, prior history of myocardial infarction treated with PTCA, and pacemaker, and moderate dyspnea on exertion.
On examination, patient had a flaccid abdomen through which the AAA could be palpated, and he had no palpable femoral artery pulse bilaterally, nor anything below. He had a cardiac murmur and moderate bilateral edema. Preoperative risk evaluation placed him in the high risk category because of his heart failure, coronary artery disease, and his mild to moderate pulmonary disease.
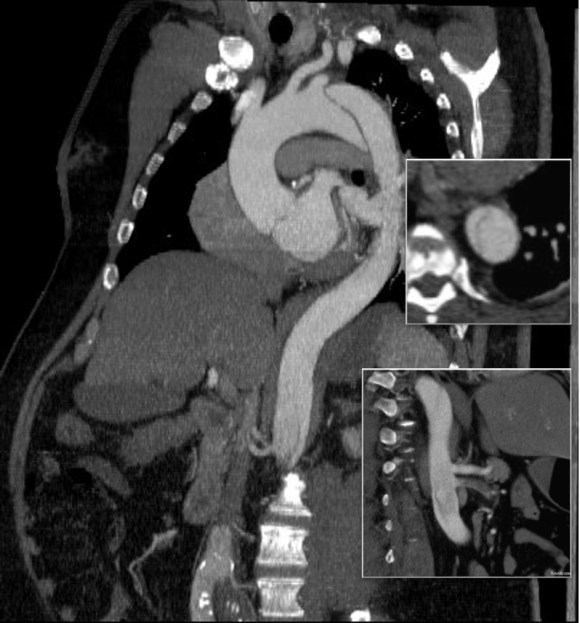
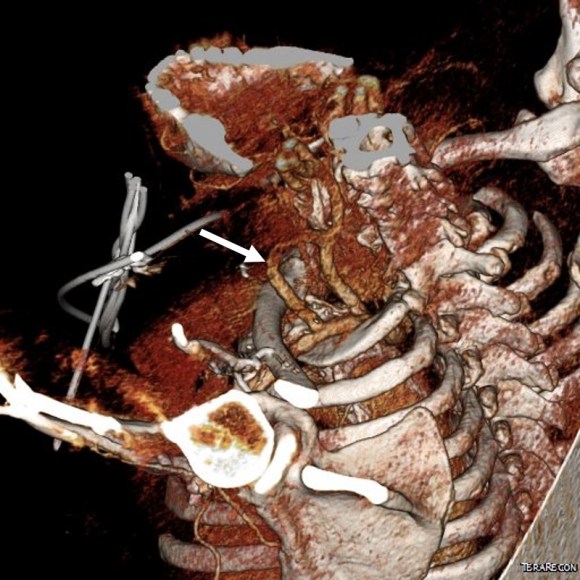
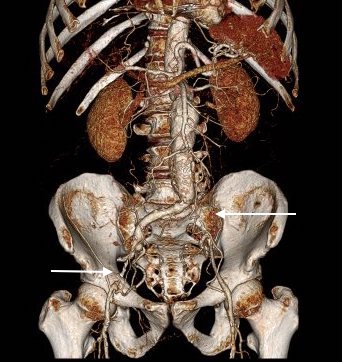
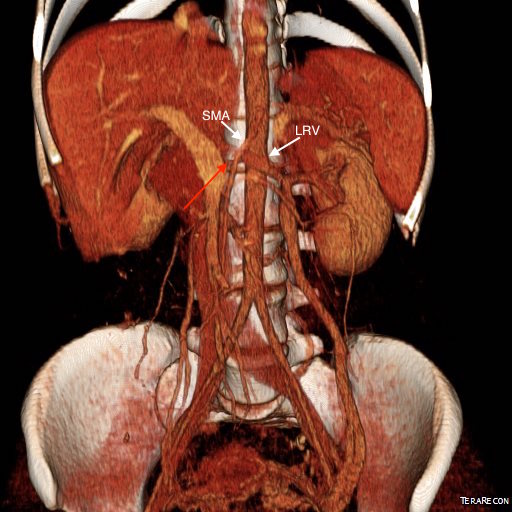
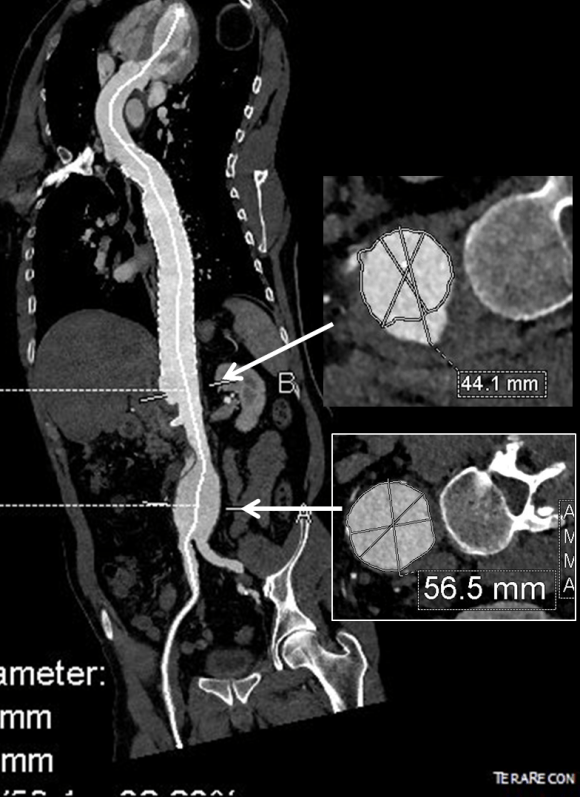
CTA (pictured above and below) showed a 5.1cm infrarenal AAA with an hourglass shaped neck with moderate atherosclerosis in the neck, an occluded left common iliac artery with external iliac artery reconstitution via internal iliac artery collaterals, and a right external iliac artery occlusion with common femoral artery reconstitution. There was calcified right common femoral artery plaque.

Treatment options included open surgical aortobifemoral bypass with exclusion of the AAA, total endovascular repair with some form of endo-conduit revascularization of the occluded segments of iliac artery, or a hybrid repair.
Open aortic repair in patients with heart failure and moderate COPD can be performed safely (ref 1). Dr. Hollier et al, in the golden age of open repair, reported a 5.7% mortality rate operating on 106 patients with severe category of heart, lung, kidney, or liver disease.
Typically, the hybrid repair involves sewing in a conduit to deliver the main body of a bifurcated or unibody stent graft when endovascular access is not possible. Despite techniques to stay minimally invasive -largely by staying retroperitoneal, this is not a benign procedure (ref 2). Nzara et al reviewed 15,082 patients from the NSQIP database breaking out 1% of patients who had conduit or direct puncture access.
Matched analyses of comorbidities revealed that patients requiring [conduit or direct access] had higher perioperative mortality (6.8% vs. 2.3%, P = 0.008), cardiac (4.8% vs. 1%, P = 0.004), pulmonary (8.8% vs. 3.4%, P = 0.006), and bleeding complications (10.2% vs. 4.6%, P = 0.016).
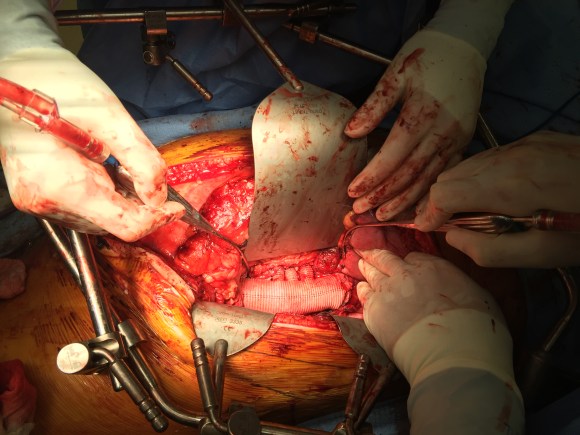
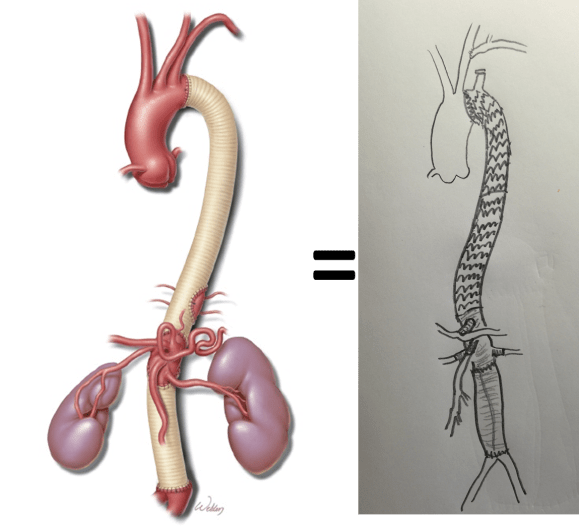
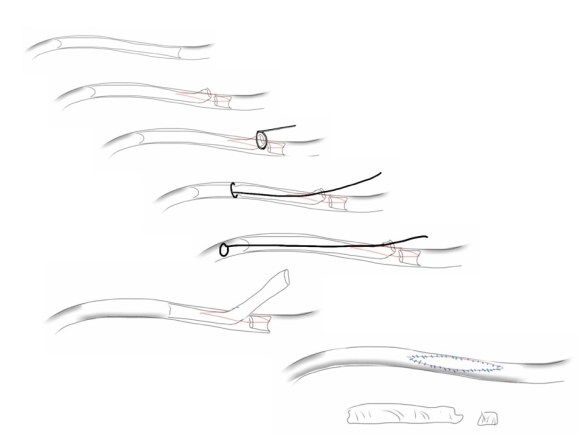
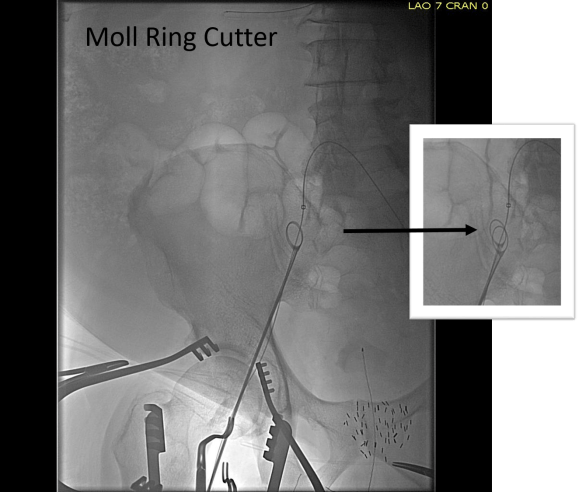
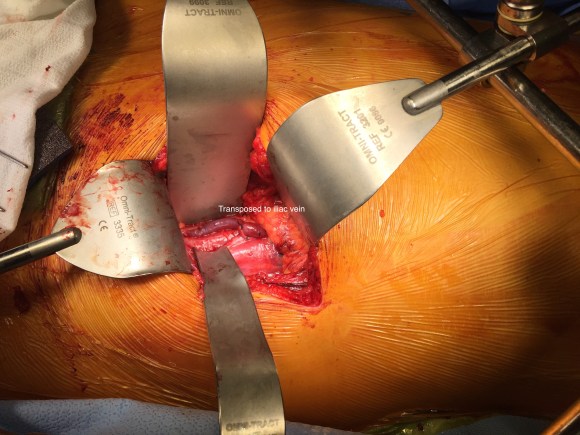
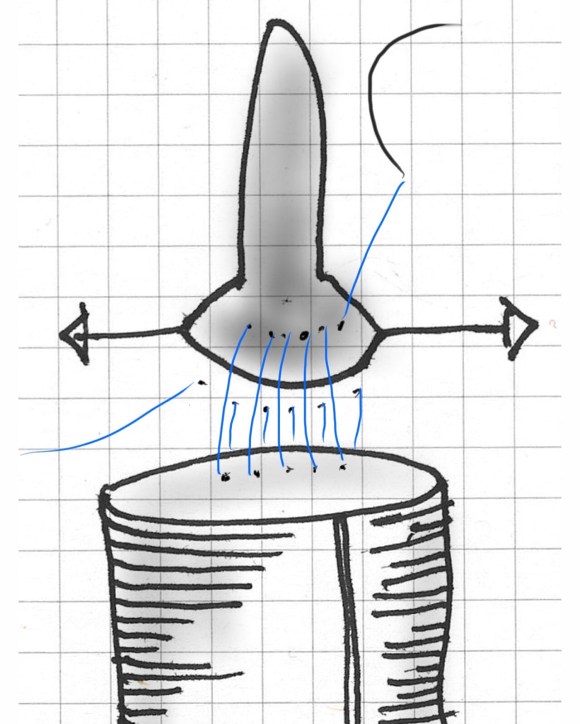
Despite these risks, I have performed AUI-FEM-FEM with good results with the modification of deploying the terminus of the stent graft across an end to end anastomosis of the conduit graft to the iliac artery (below), resulting in seal and avoiding the problems of bleeding from the usually heavily diseased artery

The iliac limbs of some stent graft systems will have proximal flares and can be used in a telescoping manner to create an aorto-uni-iliac (AUI) configuration in occlusive disease. The Cook RENU converter has a 22mm tall sealing zone designed for deployment inside another stent graft and would conform poorly to this kind of neck as a primary AUI endograft which this was not designed to act as. The Endurant II AUI converter has a suprarenal stent which I preferred to avoid in this patient as the juxtarenal neck likely was aneurysmal and might require future interventions
I chose to perform a right sided common femoral cutdown and from that exposure, perform an iliofemoral remote endarterectomy of the right external iliac to common femoral artery. This in my experience is a well tolerated and highly durable procedure (personal data). Kavanagh et al (ref 3) presented their experience with iliofemoral EndoRE and shared their techniques. This would create the lumenal diameter necessary to pass an 18F sheath to deliver an endograft. I chose the Gore Excluder which would achieve seal in the hourglass shaped neck and allow for future visceral segment intervention if necessary without having a suprarenal stent in the way. I planned on managing the left common iliac artery via a percutaneous recanalization.
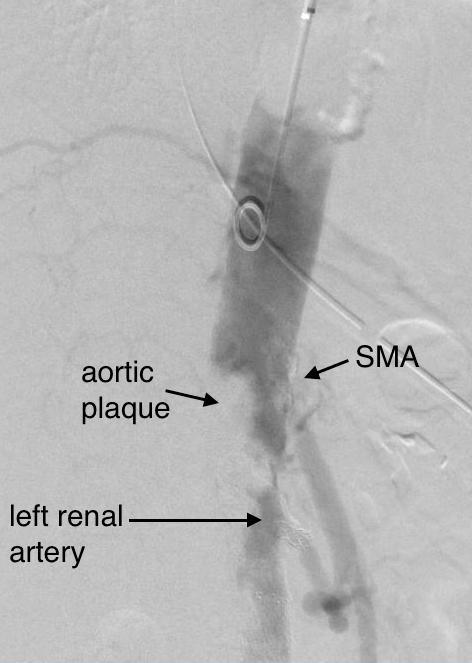
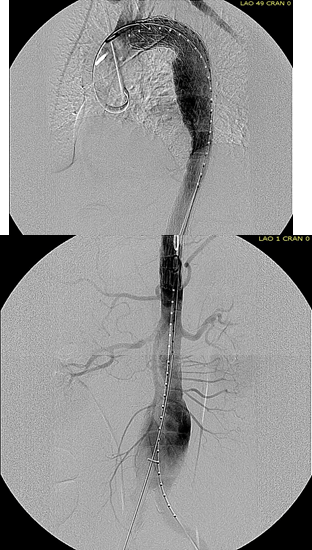
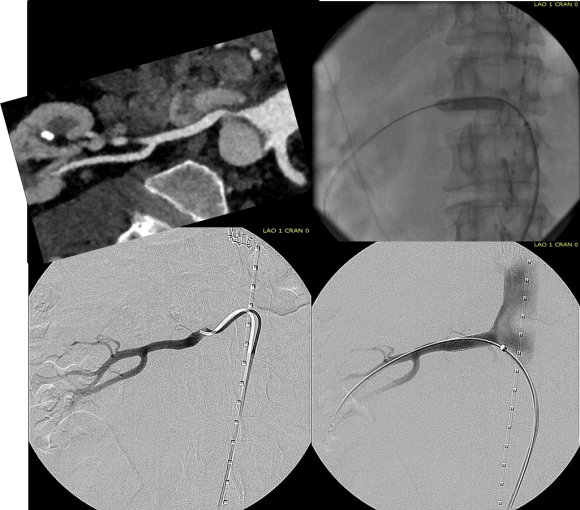
The patient’s right common femoral artery was exposed in the usual manner. Wire access across the occluded external iliac artery was achieved from a puncture of the common femoral artery. Remote endarterectomy (EndoRE) was performed over a wire from the common femoral artery to the external iliac artery origin (pictures below).
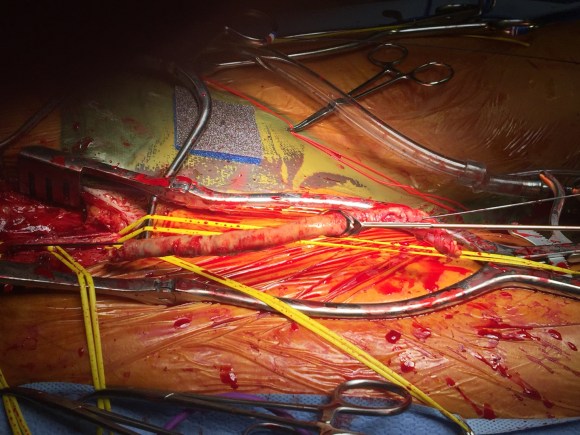
The 18F sheath went up with minimal resistance, and the EVAR was performed in the usual manner. The left common iliac artery occlusion was managed percutaneously from a left brachial access. The stent graft on the left was terminated above the iliac bifurcation and a self expanding stent was used to extend across the iliac bifurcation which had a persistent stenosis after recanalization.
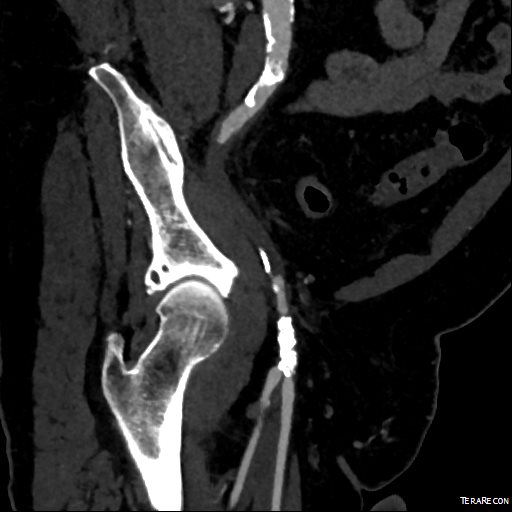
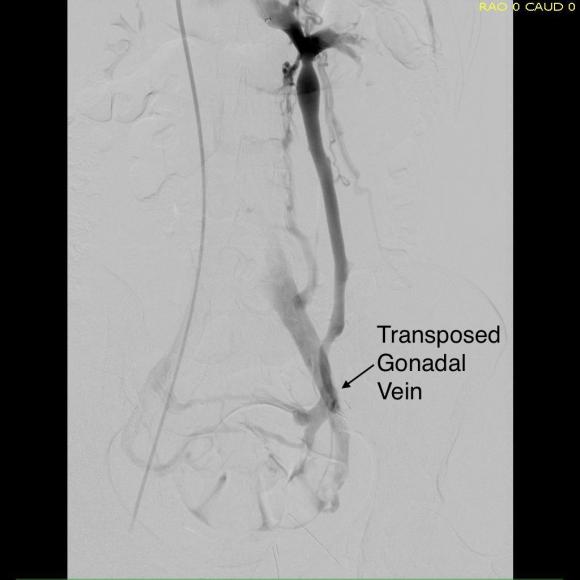
The patient recovered well and was sent home several days postprocedure. He returned a month later with healed wounds and palpable peripheral pulses. He no longer had claudication and CTA showed the aneurysm sac to have no endoleak (figures below).


Discussion
I have previously posted on using EndoRE (remote endarterectomy) for both occlusive disease and as an adjunct in EVAR. Iliofemoral EndoRE has excellent patency in the short and midterm, and in my experience has superior patency compared to the femoropopliteal segment where EndoRE is traditionally used. This case illustrates both scenarios. While the common iliac artery occlusions can be expected to have acceptable patencies with percutaneous interventions, the external iliac lesions typically fail when managed percutaneously especially when the stents are extended across the inguinal ligament. The external iliac artery is quite mobile and biologically, in my opinon, behaves much as the popliteal artery and not like the common iliac. Also, the common femoral arterial plaque is contiguous with the external iliac plaque, making in my mind, imperative to clear out all the plaque rather than what can just be seen through a groin exposure.
On microscopy, the external iliac artery is restored to a normal patent artery -I have sent arterial biopsies several months after endarterectomy and the artery felt and sewed like a normal artery and had normal structure on pathology. This implies that the external iliac can be restored to a near normal status and patients that are turned down for living related donor transplantation of kidneys can become excellent recipients. In this case, this hybrid approach effectively treated his claudication but also sealed off his moderate sized AAA while not precluding future visceral segment surgery or intervention with a large suprarenal stent.
Reference
- Hollier LH et al. J Vasc Surg 1986; 3:712-7.
- Nzara R et al. Ann Vasc Surg. 2015 Nov;29(8):1548-53
- Kavanagh CM et al. J Vasc Surg 2016;64:1327-34
 The inflow graft area is taken from its measured diameter. Then usually one or the other artery has an obligate size -a size the graft has to be while the other has more “wiggle room.” The other thing that comes from experience is that the AFX graft’s iliac limb extension don’t get the B-infolding that can affect an oversized stent graft placed in a small artery and it accomodates a neighbor well.
The inflow graft area is taken from its measured diameter. Then usually one or the other artery has an obligate size -a size the graft has to be while the other has more “wiggle room.” The other thing that comes from experience is that the AFX graft’s iliac limb extension don’t get the B-infolding that can affect an oversized stent graft placed in a small artery and it accomodates a neighbor well.



































 His operation was performed via an anterior approach with the patient supine. A tube graft repair was performed expeditiously and included resecting the dissection flap up to the clamp. Care was taken to avoid injury to the renal stent. The proximal anastomosis went well – the dilated aorta yet had strong tissue strength. A felt strip was used to buttress the aortic side of the anastomosis. The estimated risk of paralysis was less than 1% and risk of death was less than 2%. The patient recovered uneventfully and went home on POD 5.
His operation was performed via an anterior approach with the patient supine. A tube graft repair was performed expeditiously and included resecting the dissection flap up to the clamp. Care was taken to avoid injury to the renal stent. The proximal anastomosis went well – the dilated aorta yet had strong tissue strength. A felt strip was used to buttress the aortic side of the anastomosis. The estimated risk of paralysis was less than 1% and risk of death was less than 2%. The patient recovered uneventfully and went home on POD 5.