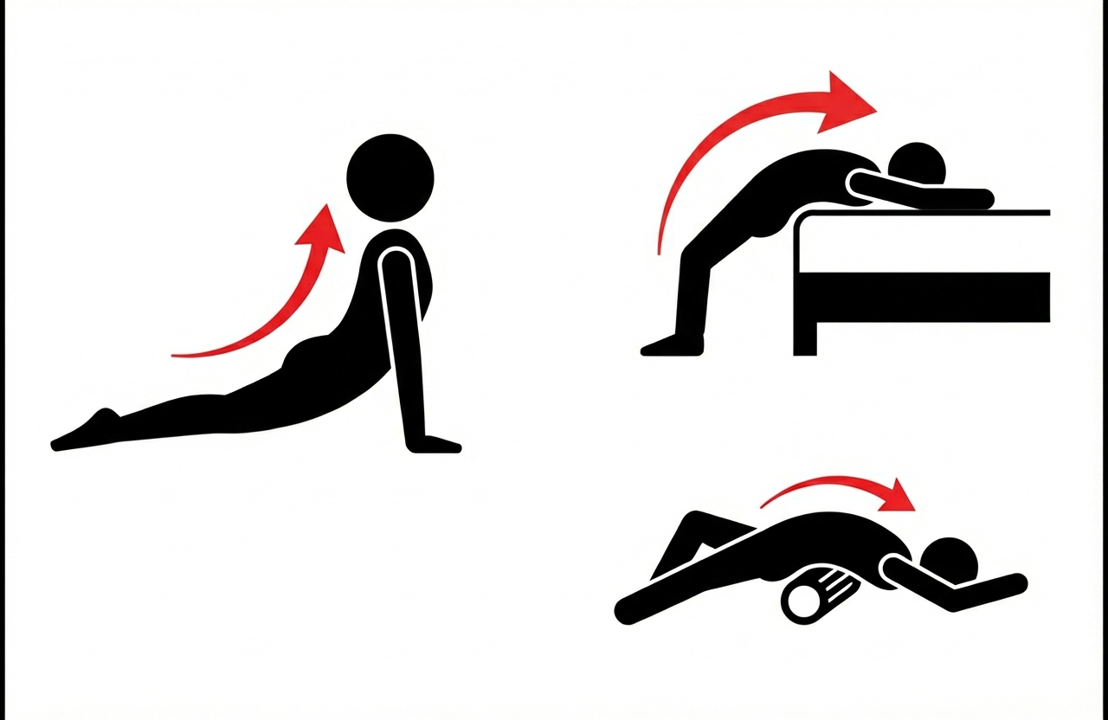
When you sprain your ankle and its on the mend, you instinctively start stretching to retain and regain range of motion, or you end up limping. The fibrosis seen in many pathology specimen of median arcuate ligaments resected surgically suggest the need to do the same -range of motion needs to be entrained with these stretches and with deep inspiration and breath holds. It should feel a bit uncomfortable.
The anecdotal evidence goes back over a decade where a patient I had performed laparoscopic MALS surgery on developed recurrent pain. He had a blockage of his celiac axis and was told to get a stent. I spoke with him in detail and given his pain with breathing and moving, I suggested starting stretches while I made inquiries about stenting where he lived (far away). He reported back after a month that these stretches relieved his pain and he no longer needed angioplasty. He is a physician and I still followup.
The other anecdote has to do with a patient I saw in Abu Dhabi who was an expat. She had classic MALS pain but her insurance would not cover surgery at CCAD and she was scheduled to return to her home country which did not have surgeons knowledgeable in MALS. I recommended stretching and eating standing up. Eating standing up relieves the pressure under the ligament and relieves any kinking of the celiac axis. She found substantial relief with these alone and left for home having regained some of her lost weight and managing her symptoms.
I recommend these stretches postoperatively to start the process of establishing a broad range of motion of the diagphragm as scarring starts on day one. The scarring is a healing process that rebuilds a median arcuate ligament much in the way that a severed Achilles tendon with regrow in a boot.
Generated from my prior posts on the biomechanical problems generated by a bipedal lifestyle, this podcast discusses those issues. This was discussed by Dr. Elen Feurriegel on her lecture series “Big Mysteries of Human Evolution” available on Audible where she describes the human spine as a stack of teacups and saucers supporting a bowling ball.
This article went up earlier this year and it was an oversight to not post it here on my blog. It is an article explaining MALS for the lay public drawn from my clinical experience going back ten years. Our approach is still a work in progress as each patient is comes with a unique presentation. Here is the link
Median arcuate ligament syndrom (MALS), also known as celiac axis compression syndrome (CACS) and its eponym Dunbar Syndrome, is manifest as epigastric abdominal pain and a compendium of symptoms, arising from chronic compression and inflammation resulting from compression of the celiac plexus between the median arcuate ligament and the celiac axis.
Graphic showing the pathoanatomy of neurogenic MALS (from ref 1). The repeated trauma to the celiac plexus results in inflammation and nerve injury with transmission of pain and neuropathic sensations.
The diaphragm muscle descends from the neck during development (the phrenic nerve originates from C3-C5 nerve roots), and in perhaps up to 25 percent of individuals, drapes across the origin of the celiac axis, and sometimes anchors further down impinging on the SMA or renal artery origins.
While a significant number of patients have this coverage of the celiac axis origin, not everyone has pain. Some whose celiac axis is compressed develop post-stenotic dilatation. For some of these, there is damage to the celiac axis resulting in intimal injury, dissections, thromboses, webs. Turbulent flow causing post-stenotic dilatation in the celiac axis can proceed to aneurysm formation. Downstream in the splenic and hepatic artery and its branches, turbulent flow can engender tortuosity (lengthening) and aneurysms (widening). This disease subset of celiac axis compression should be termed aMALS (arterial median arcuate ligament syndrome).
A question was asked at this year’s VEITH Symposium as to whether post-stenotic dilatation due to median arcuate ligament compression could be considered an aneurysm. The answer given was no, but I think it would be yes in the above example.
Both arterial and neurogenic manifestations of celiac axis compression are under the same ICD code of I77.4, referring to both celiac axis compression syndrome and median arcuate ligament syndrome. While I would never suggest more ICD codes, there should be a differentiation similar to the other compression syndrome, thoracic outlet syndrome (TOS). The pain-based syndrome, which is more common, should be termed neurogenic MALS, or nMALS, and the arterial disease secondary to celiac axis compression should be termed arterial MALS or aMALS. The treatment of nMALS is surgical ablation of the celiac plexus along with median arcuate ligament release, done via open, laparoscopic, and robotic techniques. The treatment of aMALS is the treatment of the arterial complications of celiac axis compression and should involve median arcuate release and treatment of the arterial pathology with either open or endovascular techniques.
Case Presentation
The patient is a middle-aged man with several months of right sided abdominal pain, mostly in the right midaxillary line at the costal margin, right upper quadrant abdominal pain, and right sub-scapular pain. He did not have gallstones, and had no gastrointestinal complaints. He is hypertensive and was on a single agent which he took in the mornings. His pain began during the day and crescendoed in the evening. His prior visits to the emergency room had revealed a hepatic artery aneurysm and celiac axis aneurysm. In the ED, his examination was significant for pain and mild tenderness in the right upper quadrant of his abdomen. He underwent a CT scan.
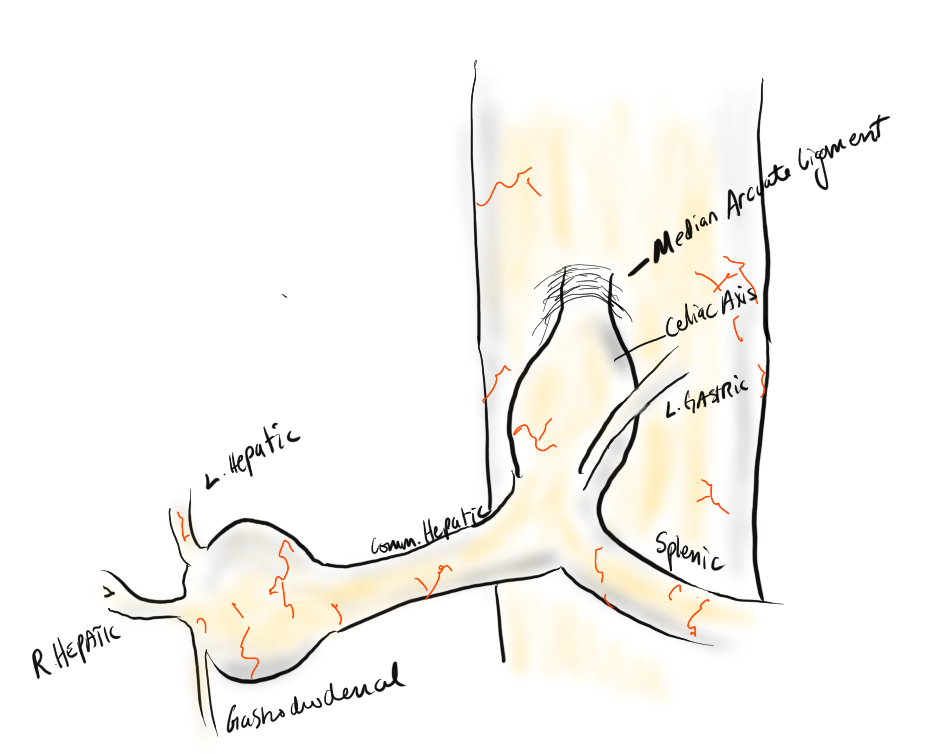
Common Hepatic Artery Aneurysm, 2.4cm with celiac axis ectasia to 14mm, median arcuate ligament compression of celiac axis
The CTA showed compression of the first centimeter of the celiac axis by the median arcuate ligament of the diaphragm and mild post-stenotic dilatation to 14mm. At the terminus of the common hepatic artery, where the hepatic bifurcated was a 2.4cm aneurysm with mural thrombus. With blood pressure control, his pain remitted.
The trainees and I had a lively discussion as to indications for repair and whether this constituted a symptomatic aneurysm. As I have stated in past posts, all pain has a nerve and a mechanism for pain. Abdominal pain and its points of referral are well known going back to the 19th century and encapsulated in Cope’s Early Diagnosis of the Acute Abdomen, whose most recent steward, Dr. William Silen just passed this September. Processes involving the gallbladder and nearby hepatic artery refer to the right upper quadrant abdomen, right chest, right shoulder and scapula which was where the patient’s pain was. And it improved with controlling his hypertension. There was no question to me the aneurysm was symptomatic, likely from strain on the aneurysm.
The question then devolves to whether this is to be done endovascularly or open. While it seems straightforward for me, I have realized at large meetings there will always be some endovascularist proposing something. For me, to exclude pressure from the aneurysm and avoid rupture, the aneurysm had to be isolated from the blood flow and pressure. Ideally, this would be done with tiny covered stents. There are no 7mm x 4mm stents bifurcation stents.
Hypothetical bifurcated small stent system -does not exist, would not work.
Embolization of the hepatic aneurysm, which is done for the splenic, offers hazard of hepatic ischemia. Despite what is written in the textbooks about the portal venous system providing most of the perfusion of the liver, you have to remember there is only portal flow when there is food. Acutely losing one of the hepatics, even clamping it for a time, reverberates as a spike in the LFTs, along with attendant systemic inflammatory response. While the liver, like spleen, can recover and regrow, you mess with it at your great peril. Based on the CTA, closing the hepatic artery with coils and plugs will likely be tolerated as hepatic flow would continue via the gastroduodenal artery which is not small, but there is no guarantee that the aneurysm wouldn’t be pressurized yet by the prominent GDA (if you disagree please feel free to comment).
He was prepared for surgery with echocardiography (normal) and lab testing (normal LFT’s, CBC, BMP, INR), and taken to the OR. A chevron incision was made to broadly expose the area. The median arcuate ligament was exposed and released -there was dense tissues proximal to the dilated celiac axis. The aneurysm was dissected out and the small branches were carefully dissected out and controlled. It is easy to injure the branch hepatic arteries which can constrict on dissection.
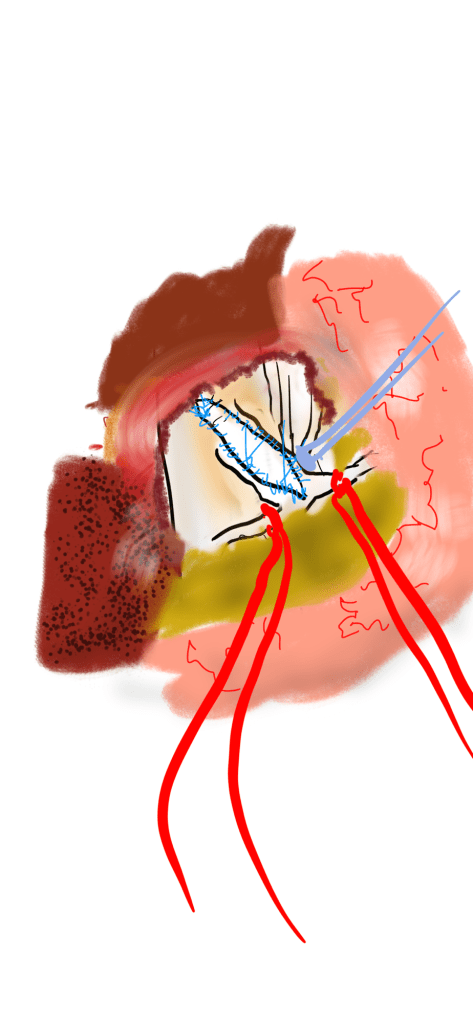
A suitable length of saphenous vein was harvested and prepared. The three vessels diagrammed above did not present themselves suitable for a single Carrel patch so I sewed end to end to a patch incorporating the right hepatic and gastroduodenal arteries, and performed a sequential side to end anastomosis to the left gastric artery.
The patient recovered well and was discharged home on POD#5, and in followup had no further symptoms.
Discussion:
The differentiation of arterial and neurogenic manifestations of MALS is an important refinement of our understanding of this disease, which I believe to be a byproduct of our bipedal lifestyle. The lordotic curvature of the spine, necessary to balance our upper torso on a vertical spine, pushes the spine forward and applies tension to the median arcuate ligament, along with other structures such as the duodenum and left renal vein in superior mesenteric artery syndrome and nutcracker syndrome, and the left iliac vein in May-Thurner Syndrome.
This compression is not only enough to narrow the celiac, but injure the artery by crushing. Stenting here does not do well because of the external compression and even after release, the artery may be damaged and require repair.
The chevron exposure heals well and is well tolerated and offers perfect exposure. While I was doing it, it occurred to me that a laparoscopic bypass is technically possible, and may be preferred to the long incision. Recent multi-institution study of MALS treatment would suggest laparoscopic approach offers a lower complication rate compared to open surgery (ref 2.)
The critical thing is having more surgeons recognize the compression that occurs in the abdomen and manifests in disparate and unconventional ways. The key is tying pain to a lesion, a mechanism, a nerve, just the way Cope’s does.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
DeCarlo C, Woo K, van Petersen AS, Geelkerken R, Chen AJ, Yeh SL, Kim GY, Henke PK, Tracci MC, Schneck MB, Grotemeyer D, Meyer B, DeMartino RR, Wilkins PB, Iranmanesh S, Rastogi V, Aulivola B, Korepta LM, Shutze WP, Jett KG, Sorber R, Abularrage CJ, Long GW, Bove PG, Davies MG, Miserlis D, Shih M, Yi J, Gupta R, Loa J, Robinson DA, Gombert A, Doukas P, de Caridi G, Benedetto F, Wittgen CM, Smeds MR, Sumpio BE, Harris S, Szeberin Z, Pomozi E, Stilo F, Montelione N, Mouawad NJ, Lawrence P, Dua A. Factors Associated With Successful Median Arcuate Ligament Release in an International, Multi-Institutional Cohort. J Vasc Surg. 2022 Oct 25:S0741-5214(22)02443-0. doi: 10.1016/j.jvs.2022.10.022. Epub ahead of print. PMID: 36306935.
Absolute Neutral Position is suprisingly universal
A body floating in space, a fetus in the womb, a dad lounging in his favorite chair, share the feature of weightlessness and represent the absolute neutral position (figure above) of the human which is the position of a relaxed supine quadruped -a dead mouse. Anything else is a stress position, including standing. Repeating motions outside of this relaxed pose or holding those positions away from this absolute neutral for long periods of time is a nidus for injury and pain. That is why most land animals sleep flat on the ground.
The Pain Operations
Operations to relieve pain are often the most gratifying to both patient and surgeon to perform successfully. This circumstance applies to the commonly performed procedures such as spine surgery, endometrial ablations, and varicose vein resections. When the pain is due to a rare set of circumstances, things are not so easy. Typically for rarer pain syndromes, two things need to coincide for the successful operation to happen. First is the patient must suffer while more common and potentially life threatening diseases are ruled out and even treated if these are found. This may take months or years. The second necessary condition is finding a physician who has seen the particular pain syndrome before and understand how to test for it and treat it. That meant the majority of people never get treated, or are shunted into the circle of shame as malingering, drug seeking, and mentally unstable. The opioid epidemic creates double jeopardy for these patients -they can become addicts as their pain is never successfully diagnosed and treated and they get labeled as drug seeking.
A random list of conditions that cause pain that should be on the mind after the usual things are ruled out. Also, vasculitis, autoimmune disorders, and foreign body reactions
All pain syndromes that can be successfully treated share common features that give you a degree of surety about the diagnosis, but at the end, there is a leap of faith on the part of both patient and practitioner because many of these operations have a failure rate ranging from 5-20 percent. First, the symptoms must be associated with sensory nerves, somatic or visceral. Second, there is a physical mechanism for that nerve to be inflamed from compression, swelling, or irritation that can be accounted for through history, physical examination, and imaging studies. Third, though not a constant, a major nerve trunk will be associated with a blood vessel, typically and artery, that is also affected by compression. Fourth, when swollen veins are the cause of pain, it has to be recognized that at an end stage the organ that the veins drain can also be affected.
The Pain Must Have a Testable Anatomic Basis
The somatic sensory nerves in the periphery are well mapped out and known since even classical times. The described pain should be consistent with a nerve. The best and easiest example is a neuroma that forms in an amputation stump. It triggers pain in its former distribution. It is palpable as a nodular mass. It is visible under ultrasound or cross sectional imaging. And it is easy to turn off temporarily with an injection of lidocaine, either under palpation or image guidance. If you can turn off the nerve and relieve the pain, it is likely that ablating or relieving the nerve of irritation will also relieve the pain. Such is the case in median arcuate ligament syndrome (figure below). The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
Tight Spaces Impinging Nerves, Arteries, and Veins
Many of the tight spaces involving the nerves have accompanying arteries that are compressed. This results in injury to the artery in the form of intimal hyperplasia, post stenotic dilatation, aneurysm formation, and thromboembolism. Shared tight spaces that cause problems for nerves and arteries have the common features of fixed ligaments, adjacent bones and muscles, inflammation, and motion. These include the thoracic outlet, antecubital fossa, cubital canal, diaphragmatic hiatus at median arcuate ligament, inguinal ligament, popliteal fossa, carpal tunnel, obturator canal, mediastinum, retroperitoneum -basically anywhere nerve, compression, and motion occur. In some instances of median arcuate ligament syndrome, postures and breathing trigger the pain. Holding a child in an arm may trigger pain in neurogenic thoracic outlet. Or sitting while wearing tight jeans may trigger a burning pain in meralgia paresthetica. It is not uncommon to find damaged arteries in median arcuate ligament syndrome, thoracic outlet syndrome, and popliteal entrapment or thrombosed veins in nutcracker syndrome, May-Thurner Syndrome, and Paget-von Schroetter Syndrome. Because nerves are typically difficult to visualize, their compression may only be inferred by testing for compression in their adjacent arteries.
Dilated Veins and Swollen Organs and Visceral Pain
Venous hypertension is most commonly conceived of as varicose and spider veins of the legs and offer a model of pain when applied to other pain caused by venous dissension. The visceral sensory fibers veins and arteries trigger a very intense pain that localizes to the trigger. I have often witnessed this when I manipulate a blood vessel during local anesthesia cases. Visceral pain from swelling has a dull achiness that is localizable to my spider veins after a long day standing like a bruise (below). The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
Actual Slide From Midwest Vascular Surgery Traveling Fellowship talk 2017, Chicago, IL, USA
When a limb is swollen from a thrombosis, the veins hurt and is similar to a bone pain from a fracture or a pulled muscle -that is how the brain processes the pain, but when the muscles and skin get tight from edema, the pain is sharp and dire. This is the same kind for pain from a distended left kidney from nutcracker syndrome or a spleen from a splenic vein thrombosis. These conditions can be modeled and predicted based on history and correct differential and confirmed with proper imaging -always.
Build a theory of the pain based on a testable proposition and set of nerves
That is the final message. These pain syndrome require some imagination and empathy to map and model. Predictive tests then can be performed on physical examination, functional testing, or imaging. Often, the adjacent artery is the only thing that can be reliably visualized and tested, knowing that it is the nerve that is compressed. Turning off the offending nerve with a block and relieving the pain is the most powerful argument for operating. It is building the argument for an operation that requires these objective data, but at the end, it does require some experience and faith. You have to believe in your patient and the science and when they coincide, you have to act.
The patient is a young woman from overseas who was referred to the clinic for abdominal and chest pain that persisted after diagnosis and treatment of Takayasu’s Arteritis affecting her visceral (middle) aorta. A year prior to presentation, she had been having severe abdominal pain, 30 pound weight loss, and weakness. Laboratory findings included elevated inflammatory markers. CT scan showed inflammation around her celiac axis and superior mesenteric artery. She was treated with prednisone but only responded ultimately to immunosuppressives. Her pain remitted for a while and she regained weight and strength, but eventually in the months prior to consultation, symptoms of postprandial abdominal pain and nausea set in with concomitant constant midsternal chest pain which at times was incapacitating.
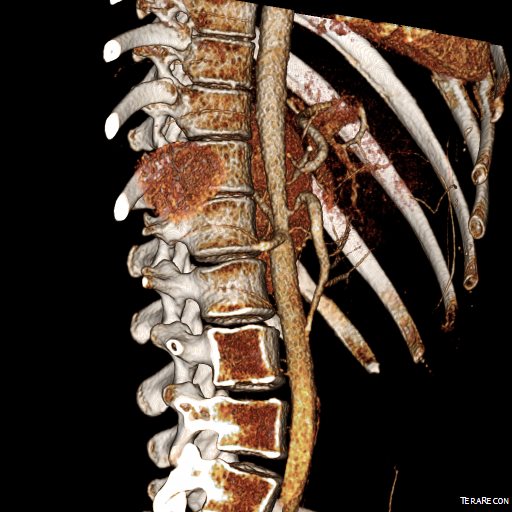
Examination was remarkable for a well nourished young woman in distress with epigastric tenderness. Inflammatory markers were normal and she was on methotrexate and tocilizumab. CTA (above) and duplex showed severe stenoses affecting the origins of the celiac axis and superior mesenteric artery. A composite of the centerlines through these showed the arteries to be critically narrowed at their origins (below), along with a mild to moderate stenosis of the aorta (above). No active inflammation could be seen.
The anterior view of the 3DVR images of her CT showed an absence of collateralization via the inferior mesenteric artery and Arc of Riolan.
This could account for her postprandial abdominal pain which was midabdominal, but the midsternal chest pain was difficult to explain. A cardiac cause had been ruled out at her home institution. It was on the lower part of the sternum and bordered the epigastrium. Through my work with median arcuate ligament syndrome, it was not unusual to have chest pain be part of the pain syndrome which comes about through the compression of the celiac plexus by the median arcuate ligament (reference), and treated effectively with the division of the median arcuate ligament and celiac plexus neurolysis.
I did feel that revascularizing the SMA was likely to improve her postprandial symptoms, given the paucity of circulation to the gut. I had a discussion about her chest pain and the thought that this was a celiac plexus neuropathy as the result of compression of the celiac plexus by her Takayasu’s disease. Typically, for younger people, I perform a bifurcated graft to the celiac axis and SMA from the distal descending thoracic aorta for younger patients, but I had no intention of replacing her aorta at this time, and wanted to reserve any definitive revascularization of her visceral vessels for a later time if it became necessary. Her pulses were full in the legs and she had no hypertension, renal insufficiency, or claudication. I therefore planned a ilio-mesenteric bypass, as it would preserve planes for a later more definitive operation if necessary, and would address her mesenteric ischemia.
I also proposed taking down the median arcuate ligament and lysing her celiac plexus to treat her chest pain symptoms. While I knew this would be fraught with some hazard because of the inflammation that had been there, it would be the best chance at treating this symptom that was debilitating her. I did not think the constant chest/epigastric pain had a vascular etiology. Normally, I would test this with a celiac plexus block, but given the likely inflammation involved, a failed block would not be helpful, and a positive one achieved with some difficulty.
The patient thought this was reasonable and agreed. She underwent a midline laparotomy and I exposed both the SMA and right common iliac artery in the retroperitoneum and tunneled a PTFE graft in a C-pattern in the retroperitoneum. The SMA was diseased proximally under the pancreas and affected by inflammatory scar tissue, and the vessel was thickened as well. The iliac pulse was normal and full and provided excellent inflow.
Going into the lesser sac, the crurae of the diaphragm were heavily scarred near the celiac axis. Division of these fiber was taken slowly and with the aid of both loupe magnification and a hook cautery (borrowed from laparoscopic surgery). The aorta was cleared of tissue first -it was also encased in scar tissue. The dissection going distally was made difficult by inflammatory scar tissue as well, but several large nerve trunks were encountered and divided. The celiac axis was atretic and small within this scar tissue, but was released down to the trifurcation.
The recovery was notable for remission of her chest pain and her ability to resume eating without pain or nausea. A CTA done before discharge showed a patent bypass.
Followup communication has revealed continued remission of her presenting symptoms months after her operation.
We are working on presenting a followup to our recent paper on MALS. Increasingly, it is apparent that consideration of celiac plexus compression as an etiology of epigastric abdominal pain unexplained by more common gastrointestinal causes provides solutions for patients given no explanation for their debilitating pain. This pain can also affect the chest, and flanks and back in the distal thoracic dermatomes, and mimic the some of the symptoms of mesenteric ischemia. In those with recurrent MALS after a successful ligament release and interval of symptom remission, even in the absence of celiac axis compression, a positive response to a celiac plexus block points to the presence of either remnant plexus fibers or compression by scar tissue of the cut nerve endings (neuromata) and reoperation has been successful. Extrapolating this experience to this patient with inflammatory compression of the celiac plexus secondary to Takayasu’s Arteritis made sense and celiac neurolysis appears effective.
Reference
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median arcuate ligament syndrome is not a vascular disease. Ann Vasc Surg. 2016 Jan;30:22-7.
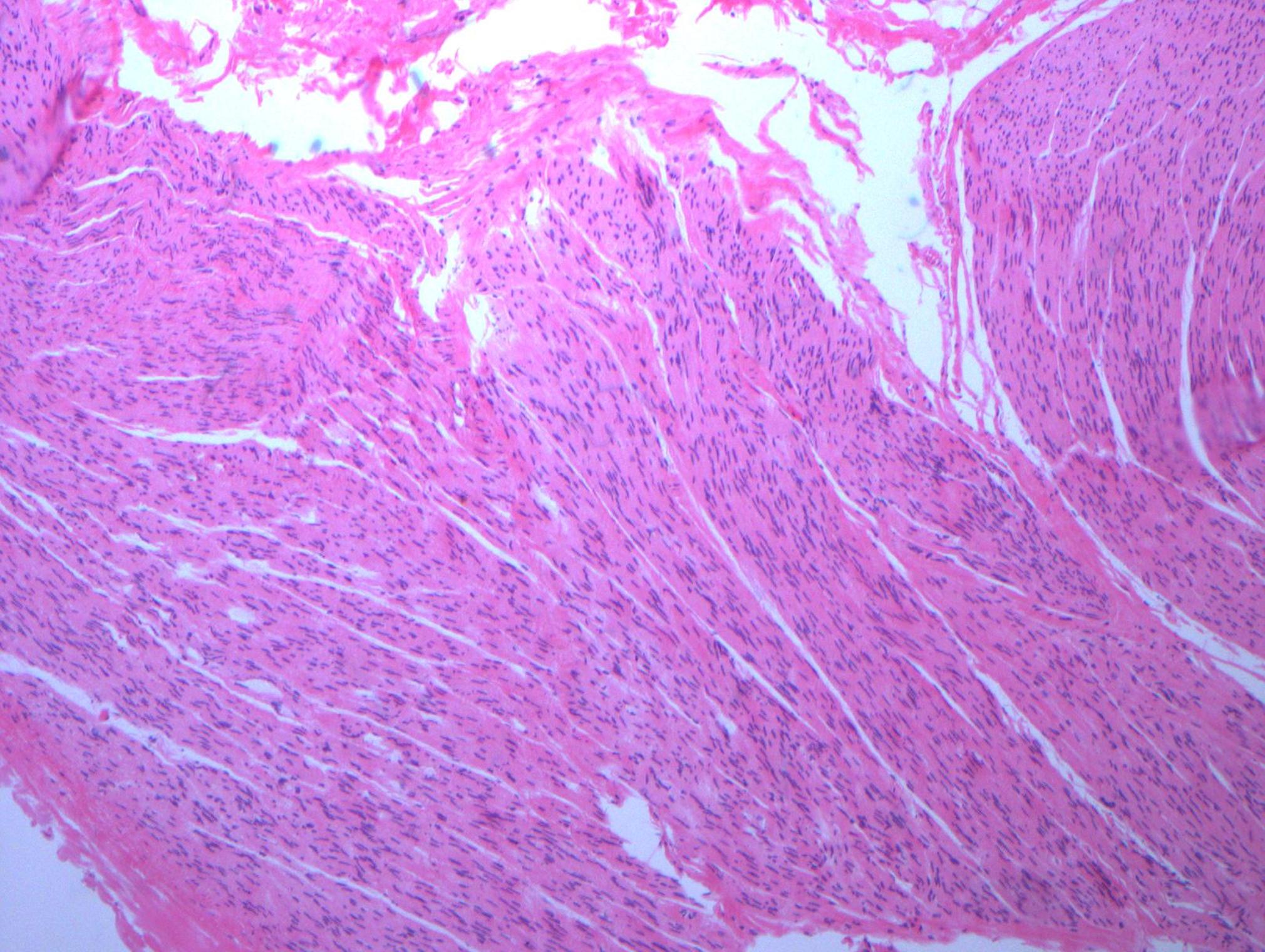
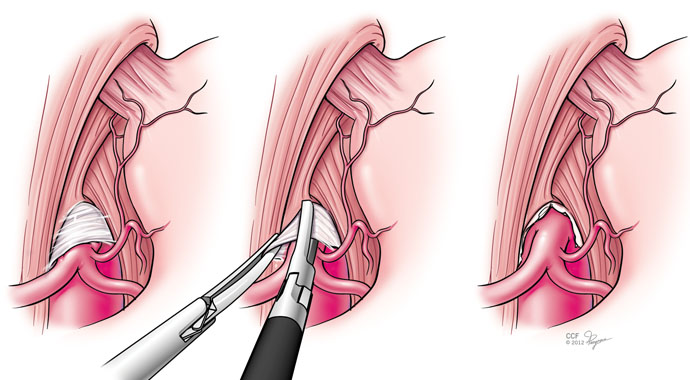
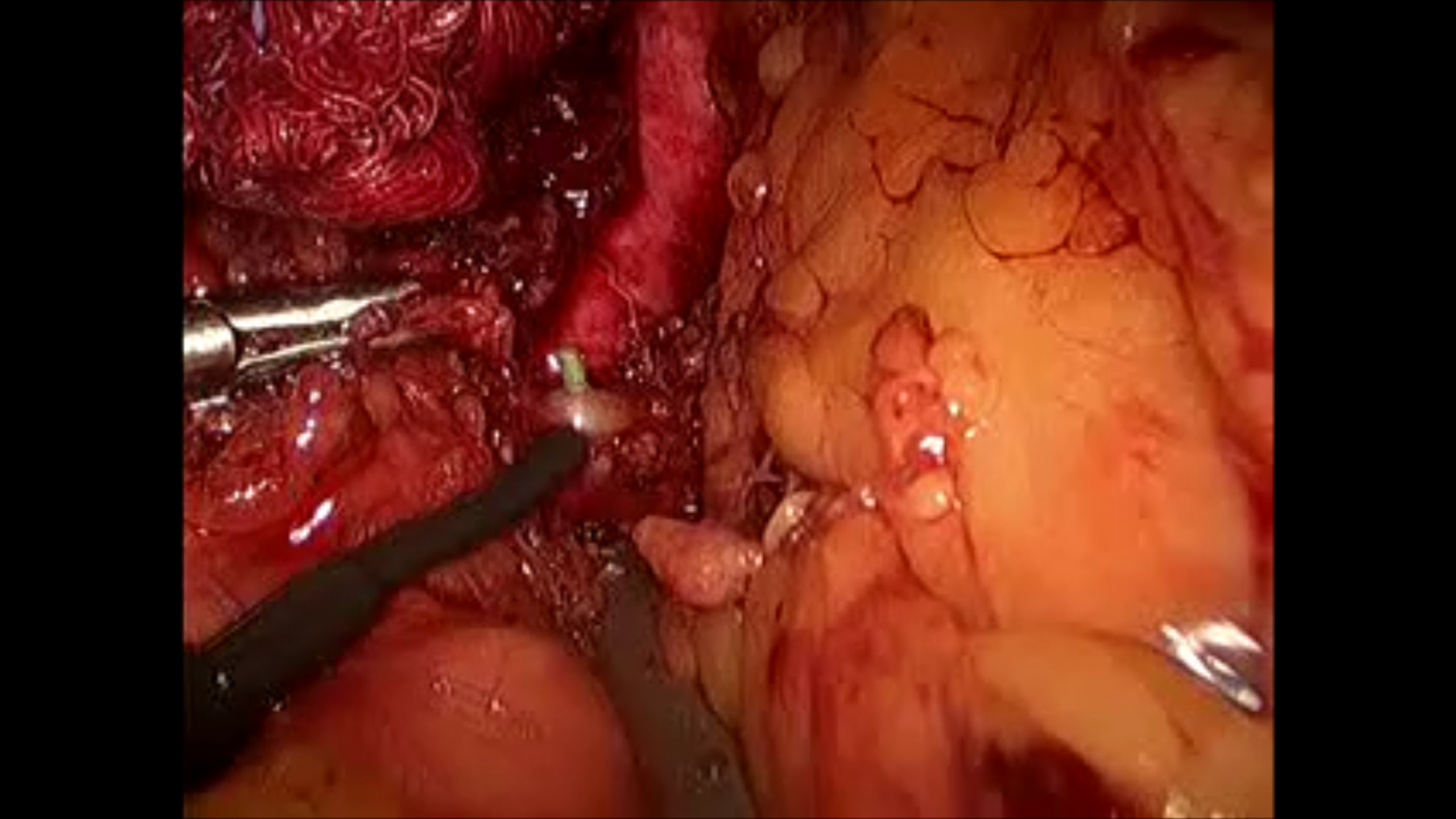
This was removed during a laparoscopic median arcuate ligament release. It was a hard white band compressed under the ligament and itself compressing the celiac axis. During the release, I grabbed a piece of these fibers and sent it for pathology under the preliminary diagnosis of celiac plexus, and it was. Described as “typical for a peripheral nerve…mostly Schwann cell nuclei in between nerve fiber.” Other micrographs in the specimen had ganglionic fibers but our pathologist wasn’t able to locate it. This is an important piece of the pathoanatomy because I believe that this is the nidus of the pain associated with median arcuate ligament syndrome, not a regional ischemia that can only occur if the celiac axis is an end artery, which can really only happen after a major exenteration like a Whipple procedure.
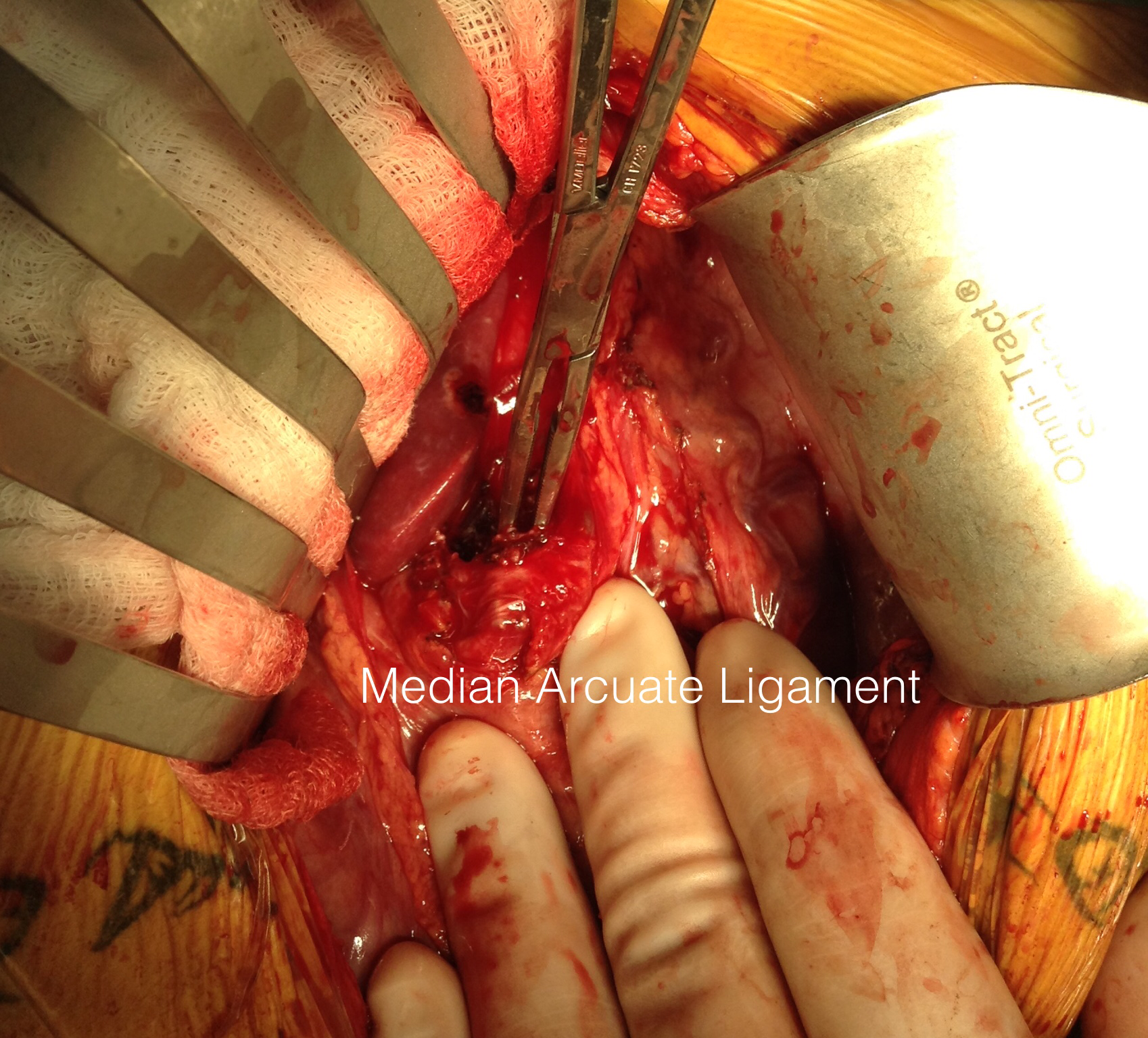
This is a picture from several years ago when I released the median arcuate ligament with open surgery. Seen tented up by the right angle clamp is the fibromuscular tissue over the celiac axis. You can also see a cord of celiac plexus, which gives the foregut somatic sensory innervation. It is becoming clearer that MALS is a nerve compression syndrome in the same way that carpal tunnel compression of the median nerve or thoracic outlet compression of the brachial plexus causes pain. Like nTOS, the arterial compression is a bystander, but a necessary finding in the diagnosis. The celiac axis and median arcuate ligament acts as a nerve compressor. This is why people with MALS respond to celiac plexus block and why it makes sense they don’t have mesenteric ischemia.
Median arcuate ligament syndrome has some disrepute among vascular surgeons because it does not make intrinsic sense that an isolated celiac axis stenosis, an intermittent one at that, would cause a regional mesenteric ischemia in a population that is in the literature, generally younger than the classic population seen for chronic mesenteric ischemia. And it shouldn’t, because no exceptions to the physiology and anatomy of mesenteric ischemia can be made.
The finding that some younger patients present with post prandial upper abdominal pain with associated compression of the celiac axis by the median arcuate ligament of the diaphragm dates to the 1960’s. These patients lose weight and find relief by leaning forward, standing, and crouching. They resort to small volume liquid diets in extreme cases, and more than 50 pounds of weight loss is seen.
During my fellowship, we treated these with operative release of the median arcuate ligament and there would be fibrosis and the celiac plexus, nerves mediating somatic pain from the foregut, would be ablated during the dissection. Inevitably, the celiac axis would undergo a patch or bypass because of the chronic scarring on the artery due to the compression. For the past two years, in collaboration with Drs. Matthew Kroh and Kevin El-Hayek (now in CCF Abu Dhabi), these releases have been performed laparoscopically, and celiac stents are hardly ever used.
John Weber, our vascular surgery chief resident, has prepared this data and we have submitted it to the PVSS for the meeting in February. Not thinking of this as a vascular disease, but rather a nerve compression disease, much like neurogenic thoracic outlet syndrome or carpel tunnel syndrome, the pathoanatomy and clinical presentation make far more sense. There is inflammation typically and nerves are ablated, and celiac plexus block, it turns out, is an excellent screening tool when the classic presentation is not present. It is analogous to using a scalene block in neurogenic thoracic outlet syndrome. Redo operation is feasible if the original procedure fails to relieve pain completely, if the celiac plexus block works to block the pain.













 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).