Generated from my prior posts on the biomechanical problems generated by a bipedal lifestyle, this podcast discusses those issues. This was discussed by Dr. Elen Feurriegel on her lecture series “Big Mysteries of Human Evolution” available on Audible where she describes the human spine as a stack of teacups and saucers supporting a bowling ball.
In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.
Median arcuate ligament syndrom (MALS), also known as celiac axis compression syndrome (CACS) and its eponym Dunbar Syndrome, is manifest as epigastric abdominal pain and a compendium of symptoms, arising from chronic compression and inflammation resulting from compression of the celiac plexus between the median arcuate ligament and the celiac axis.
Graphic showing the pathoanatomy of neurogenic MALS (from ref 1). The repeated trauma to the celiac plexus results in inflammation and nerve injury with transmission of pain and neuropathic sensations.
The diaphragm muscle descends from the neck during development (the phrenic nerve originates from C3-C5 nerve roots), and in perhaps up to 25 percent of individuals, drapes across the origin of the celiac axis, and sometimes anchors further down impinging on the SMA or renal artery origins.
While a significant number of patients have this coverage of the celiac axis origin, not everyone has pain. Some whose celiac axis is compressed develop post-stenotic dilatation. For some of these, there is damage to the celiac axis resulting in intimal injury, dissections, thromboses, webs. Turbulent flow causing post-stenotic dilatation in the celiac axis can proceed to aneurysm formation. Downstream in the splenic and hepatic artery and its branches, turbulent flow can engender tortuosity (lengthening) and aneurysms (widening). This disease subset of celiac axis compression should be termed aMALS (arterial median arcuate ligament syndrome).
A question was asked at this year’s VEITH Symposium as to whether post-stenotic dilatation due to median arcuate ligament compression could be considered an aneurysm. The answer given was no, but I think it would be yes in the above example.
Both arterial and neurogenic manifestations of celiac axis compression are under the same ICD code of I77.4, referring to both celiac axis compression syndrome and median arcuate ligament syndrome. While I would never suggest more ICD codes, there should be a differentiation similar to the other compression syndrome, thoracic outlet syndrome (TOS). The pain-based syndrome, which is more common, should be termed neurogenic MALS, or nMALS, and the arterial disease secondary to celiac axis compression should be termed arterial MALS or aMALS. The treatment of nMALS is surgical ablation of the celiac plexus along with median arcuate ligament release, done via open, laparoscopic, and robotic techniques. The treatment of aMALS is the treatment of the arterial complications of celiac axis compression and should involve median arcuate release and treatment of the arterial pathology with either open or endovascular techniques.
Case Presentation
The patient is a middle-aged man with several months of right sided abdominal pain, mostly in the right midaxillary line at the costal margin, right upper quadrant abdominal pain, and right sub-scapular pain. He did not have gallstones, and had no gastrointestinal complaints. He is hypertensive and was on a single agent which he took in the mornings. His pain began during the day and crescendoed in the evening. His prior visits to the emergency room had revealed a hepatic artery aneurysm and celiac axis aneurysm. In the ED, his examination was significant for pain and mild tenderness in the right upper quadrant of his abdomen. He underwent a CT scan.
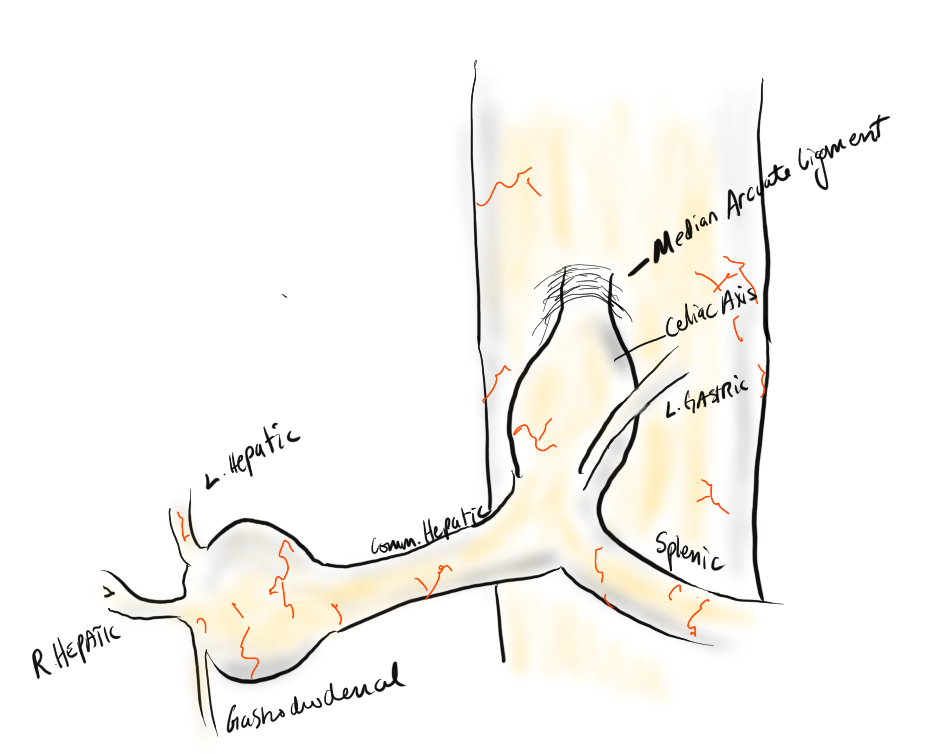
Common Hepatic Artery Aneurysm, 2.4cm with celiac axis ectasia to 14mm, median arcuate ligament compression of celiac axis
The CTA showed compression of the first centimeter of the celiac axis by the median arcuate ligament of the diaphragm and mild post-stenotic dilatation to 14mm. At the terminus of the common hepatic artery, where the hepatic bifurcated was a 2.4cm aneurysm with mural thrombus. With blood pressure control, his pain remitted.
The trainees and I had a lively discussion as to indications for repair and whether this constituted a symptomatic aneurysm. As I have stated in past posts, all pain has a nerve and a mechanism for pain. Abdominal pain and its points of referral are well known going back to the 19th century and encapsulated in Cope’s Early Diagnosis of the Acute Abdomen, whose most recent steward, Dr. William Silen just passed this September. Processes involving the gallbladder and nearby hepatic artery refer to the right upper quadrant abdomen, right chest, right shoulder and scapula which was where the patient’s pain was. And it improved with controlling his hypertension. There was no question to me the aneurysm was symptomatic, likely from strain on the aneurysm.
The question then devolves to whether this is to be done endovascularly or open. While it seems straightforward for me, I have realized at large meetings there will always be some endovascularist proposing something. For me, to exclude pressure from the aneurysm and avoid rupture, the aneurysm had to be isolated from the blood flow and pressure. Ideally, this would be done with tiny covered stents. There are no 7mm x 4mm stents bifurcation stents.
Hypothetical bifurcated small stent system -does not exist, would not work.
Embolization of the hepatic aneurysm, which is done for the splenic, offers hazard of hepatic ischemia. Despite what is written in the textbooks about the portal venous system providing most of the perfusion of the liver, you have to remember there is only portal flow when there is food. Acutely losing one of the hepatics, even clamping it for a time, reverberates as a spike in the LFTs, along with attendant systemic inflammatory response. While the liver, like spleen, can recover and regrow, you mess with it at your great peril. Based on the CTA, closing the hepatic artery with coils and plugs will likely be tolerated as hepatic flow would continue via the gastroduodenal artery which is not small, but there is no guarantee that the aneurysm wouldn’t be pressurized yet by the prominent GDA (if you disagree please feel free to comment).
He was prepared for surgery with echocardiography (normal) and lab testing (normal LFT’s, CBC, BMP, INR), and taken to the OR. A chevron incision was made to broadly expose the area. The median arcuate ligament was exposed and released -there was dense tissues proximal to the dilated celiac axis. The aneurysm was dissected out and the small branches were carefully dissected out and controlled. It is easy to injure the branch hepatic arteries which can constrict on dissection.
A suitable length of saphenous vein was harvested and prepared. The three vessels diagrammed above did not present themselves suitable for a single Carrel patch so I sewed end to end to a patch incorporating the right hepatic and gastroduodenal arteries, and performed a sequential side to end anastomosis to the left gastric artery.
The patient recovered well and was discharged home on POD#5, and in followup had no further symptoms.
Discussion:
The differentiation of arterial and neurogenic manifestations of MALS is an important refinement of our understanding of this disease, which I believe to be a byproduct of our bipedal lifestyle. The lordotic curvature of the spine, necessary to balance our upper torso on a vertical spine, pushes the spine forward and applies tension to the median arcuate ligament, along with other structures such as the duodenum and left renal vein in superior mesenteric artery syndrome and nutcracker syndrome, and the left iliac vein in May-Thurner Syndrome.
This compression is not only enough to narrow the celiac, but injure the artery by crushing. Stenting here does not do well because of the external compression and even after release, the artery may be damaged and require repair.
The chevron exposure heals well and is well tolerated and offers perfect exposure. While I was doing it, it occurred to me that a laparoscopic bypass is technically possible, and may be preferred to the long incision. Recent multi-institution study of MALS treatment would suggest laparoscopic approach offers a lower complication rate compared to open surgery (ref 2.)
The critical thing is having more surgeons recognize the compression that occurs in the abdomen and manifests in disparate and unconventional ways. The key is tying pain to a lesion, a mechanism, a nerve, just the way Cope’s does.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
DeCarlo C, Woo K, van Petersen AS, Geelkerken R, Chen AJ, Yeh SL, Kim GY, Henke PK, Tracci MC, Schneck MB, Grotemeyer D, Meyer B, DeMartino RR, Wilkins PB, Iranmanesh S, Rastogi V, Aulivola B, Korepta LM, Shutze WP, Jett KG, Sorber R, Abularrage CJ, Long GW, Bove PG, Davies MG, Miserlis D, Shih M, Yi J, Gupta R, Loa J, Robinson DA, Gombert A, Doukas P, de Caridi G, Benedetto F, Wittgen CM, Smeds MR, Sumpio BE, Harris S, Szeberin Z, Pomozi E, Stilo F, Montelione N, Mouawad NJ, Lawrence P, Dua A. Factors Associated With Successful Median Arcuate Ligament Release in an International, Multi-Institutional Cohort. J Vasc Surg. 2022 Oct 25:S0741-5214(22)02443-0. doi: 10.1016/j.jvs.2022.10.022. Epub ahead of print. PMID: 36306935.
Absolute Neutral Position is suprisingly universal
A body floating in space, a fetus in the womb, a dad lounging in his favorite chair, share the feature of weightlessness and represent the absolute neutral position (figure above) of the human which is the position of a relaxed supine quadruped -a dead mouse. Anything else is a stress position, including standing. Repeating motions outside of this relaxed pose or holding those positions away from this absolute neutral for long periods of time is a nidus for injury and pain. That is why most land animals sleep flat on the ground.
The Pain Operations
Operations to relieve pain are often the most gratifying to both patient and surgeon to perform successfully. This circumstance applies to the commonly performed procedures such as spine surgery, endometrial ablations, and varicose vein resections. When the pain is due to a rare set of circumstances, things are not so easy. Typically for rarer pain syndromes, two things need to coincide for the successful operation to happen. First is the patient must suffer while more common and potentially life threatening diseases are ruled out and even treated if these are found. This may take months or years. The second necessary condition is finding a physician who has seen the particular pain syndrome before and understand how to test for it and treat it. That meant the majority of people never get treated, or are shunted into the circle of shame as malingering, drug seeking, and mentally unstable. The opioid epidemic creates double jeopardy for these patients -they can become addicts as their pain is never successfully diagnosed and treated and they get labeled as drug seeking.
A random list of conditions that cause pain that should be on the mind after the usual things are ruled out. Also, vasculitis, autoimmune disorders, and foreign body reactions
All pain syndromes that can be successfully treated share common features that give you a degree of surety about the diagnosis, but at the end, there is a leap of faith on the part of both patient and practitioner because many of these operations have a failure rate ranging from 5-20 percent. First, the symptoms must be associated with sensory nerves, somatic or visceral. Second, there is a physical mechanism for that nerve to be inflamed from compression, swelling, or irritation that can be accounted for through history, physical examination, and imaging studies. Third, though not a constant, a major nerve trunk will be associated with a blood vessel, typically and artery, that is also affected by compression. Fourth, when swollen veins are the cause of pain, it has to be recognized that at an end stage the organ that the veins drain can also be affected.
The Pain Must Have a Testable Anatomic Basis
The somatic sensory nerves in the periphery are well mapped out and known since even classical times. The described pain should be consistent with a nerve. The best and easiest example is a neuroma that forms in an amputation stump. It triggers pain in its former distribution. It is palpable as a nodular mass. It is visible under ultrasound or cross sectional imaging. And it is easy to turn off temporarily with an injection of lidocaine, either under palpation or image guidance. If you can turn off the nerve and relieve the pain, it is likely that ablating or relieving the nerve of irritation will also relieve the pain. Such is the case in median arcuate ligament syndrome (figure below). The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
Tight Spaces Impinging Nerves, Arteries, and Veins
Many of the tight spaces involving the nerves have accompanying arteries that are compressed. This results in injury to the artery in the form of intimal hyperplasia, post stenotic dilatation, aneurysm formation, and thromboembolism. Shared tight spaces that cause problems for nerves and arteries have the common features of fixed ligaments, adjacent bones and muscles, inflammation, and motion. These include the thoracic outlet, antecubital fossa, cubital canal, diaphragmatic hiatus at median arcuate ligament, inguinal ligament, popliteal fossa, carpal tunnel, obturator canal, mediastinum, retroperitoneum -basically anywhere nerve, compression, and motion occur. In some instances of median arcuate ligament syndrome, postures and breathing trigger the pain. Holding a child in an arm may trigger pain in neurogenic thoracic outlet. Or sitting while wearing tight jeans may trigger a burning pain in meralgia paresthetica. It is not uncommon to find damaged arteries in median arcuate ligament syndrome, thoracic outlet syndrome, and popliteal entrapment or thrombosed veins in nutcracker syndrome, May-Thurner Syndrome, and Paget-von Schroetter Syndrome. Because nerves are typically difficult to visualize, their compression may only be inferred by testing for compression in their adjacent arteries.
Dilated Veins and Swollen Organs and Visceral Pain
Venous hypertension is most commonly conceived of as varicose and spider veins of the legs and offer a model of pain when applied to other pain caused by venous dissension. The visceral sensory fibers veins and arteries trigger a very intense pain that localizes to the trigger. I have often witnessed this when I manipulate a blood vessel during local anesthesia cases. Visceral pain from swelling has a dull achiness that is localizable to my spider veins after a long day standing like a bruise (below). The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
Actual Slide From Midwest Vascular Surgery Traveling Fellowship talk 2017, Chicago, IL, USA
When a limb is swollen from a thrombosis, the veins hurt and is similar to a bone pain from a fracture or a pulled muscle -that is how the brain processes the pain, but when the muscles and skin get tight from edema, the pain is sharp and dire. This is the same kind for pain from a distended left kidney from nutcracker syndrome or a spleen from a splenic vein thrombosis. These conditions can be modeled and predicted based on history and correct differential and confirmed with proper imaging -always.
Build a theory of the pain based on a testable proposition and set of nerves
That is the final message. These pain syndrome require some imagination and empathy to map and model. Predictive tests then can be performed on physical examination, functional testing, or imaging. Often, the adjacent artery is the only thing that can be reliably visualized and tested, knowing that it is the nerve that is compressed. Turning off the offending nerve with a block and relieving the pain is the most powerful argument for operating. It is building the argument for an operation that requires these objective data, but at the end, it does require some experience and faith. You have to believe in your patient and the science and when they coincide, you have to act.
Patient is a 43 year old woman who had been having bouts of severe left sided abdominal pain for several years with worsening episodes of nausea and vomiting resulting in several visits to the emergency room. She has also had microscopic hematuria. Gastrointestinal workup including gastric emptying study, esophagogastroduodenoscopy and colonoscopy were negative, as was a workup for kidney stones. Eventually she was referred to my clinic for management of nutcracker syndrome. She denied lower abdominal pain nor excessive menstrual bleeding.
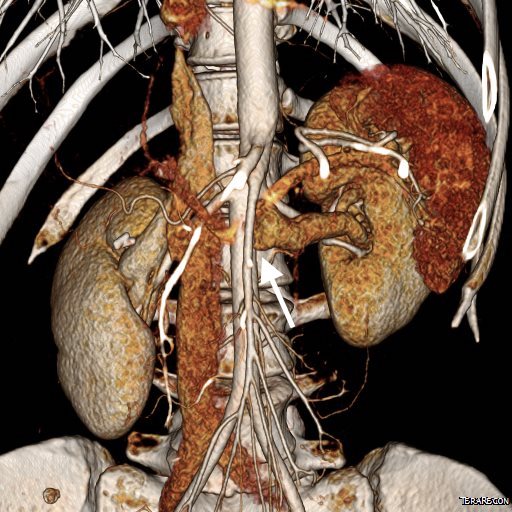
On examination, she was tender over the left kidney and flank. Laboratory examination was positive for microscopic hematuria. CT venography (below) showed an obstruction of her left renal vein by the superior mesenteric artery. Drainage via gonadal vein was not demonstrated, and no pelvic varices or complex of retroperitoneal veins was apparent.
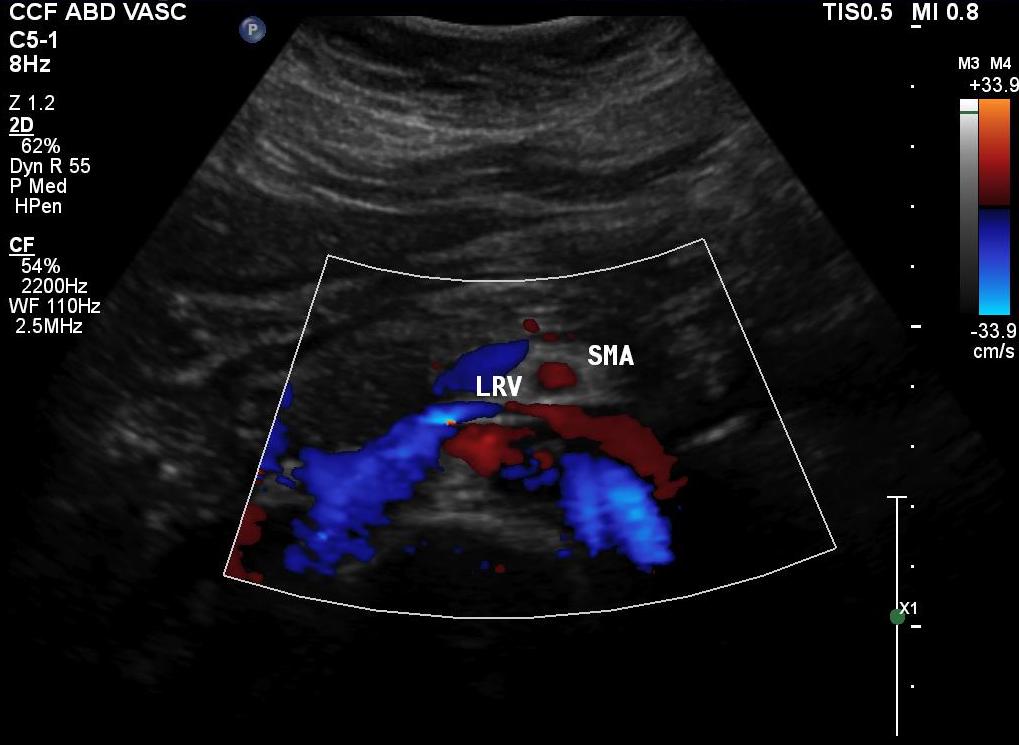
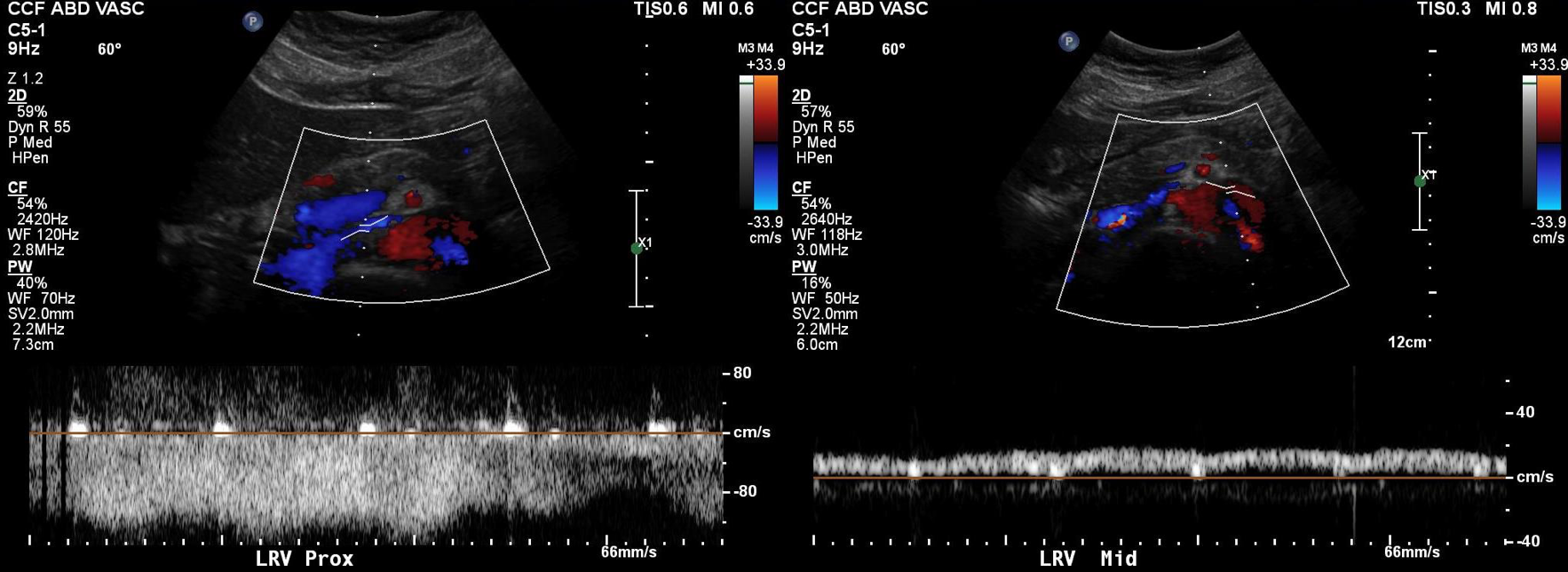
Duplex showed the narrowing in the left renal vein and spectral Doppler showed elevated velocities across the compression caused by the superior mesenteric artery (below). The collecting system was not obstructed.
Treatment options included endovascularization with a large stent in the left renal vein, left renal vein transposition to a lower position on the inferior vena cava, left renal autotransplantation, and left nephrectomy. Stent placement comes with a degree of risk for cardiopulmonary embolism which may require a sternotomy to fish out an errant stent. The risk for this in the US is because the largest nitinol stents available are 14mm in diameter which might result in undersizing in a vein that could easily dilate to well over 20mm. Larger nitinol stents for venous applications are available in Europe but currently are not approved in the US (yet). Wall stents, while certainly wide enough, have the problem of being long and stiff when not fully deployed. A 22×35 Wall stent may be 50mm long if deployed inadvertently into a tributary vein or contrained at the narrowing. Because it slides easily, passing balloons in or out can cause it to slip out of position. Because this stent elongates when compressed and packed, deployment is challenging and it is prone to “watermelon seeding,” a set up for embolism. It does have the virtue of easy reconstraining.
My friend and recent host for Midwest Vascular Surgery Society Travelling Fellowship, Dr. John V. White, in Chicago, seems to have solved this problem by a multistep process of predeploying a temporary suprarenal IVC filter, deploying a stent (whatever fits), leaving the filter as a protection against stent migration for 4 weeks until the stent permanently seats itself through scarring/intimal ingrowth, then removing the filter.
I chose to perform venography and renal vein transposition. The patient was placed in a supine position on a hybrid angiographic operating room table and her right femoral vein was accessed. She was placed in 15 degrees reverse Trendelenberg which is about the upper limit possible. Venography below.
Arrow points to left ascending lumbar vein which is taking most of the reflux. It drains the left kidney across the midline via retroartic channels to the IVCThe films showed left renal vein compression by the superior mesenteric artery with outflow via the ascending lumbar vein, both supra and infrarenal tributaries. A midline exposure was performed and the retroperitoneum opened as in an transabdominal aortic exposure. The vena cava was exposed, and the left renal vein was mobilized by ligating and dividing its tributaries. A point 5cm below the tributary point was marked on the IVC, and this was the target for transposition.
After heparinizing and clamping, the renal tributary was taken with a 5mm cuff –this would ensure proper length without narrowing the IVC.
The vein was anastomosed and flow was excellent by pulse Doppler.
She recovered well but had a longer stay because of an ileus, being discharged on day 5. Because she lived at a distance, and came back for followup the following week prior to boarding a plane for home. She no longer had the left sided abdominal pain and there was no hematuria. CT showed excellent drainage through the transposed vein.
Followup will be periodic (6 monthly) renal venous duplex from home. Given that there was minimal tension on the repair, I expect this to do well.
Discussion:
Nutcracker syndrome is one of the many unfortunate consequences of our bipedal lifestyle. The small intestines hang like baggy sausages off the branched stems of the superior mesenteric artery (SMA), and in some individuals, the SMA compresses the left renal vein against the aorta. The left renal vein receives up to 12-15% of cardiac output via the left kidney, and with outflow obstruction, drains the blood through small collaterals. The renal venous hypertension results in swelling of the left kidney with subsequent left renal colic -with flank and abdominal pain, nausea, and vomiting. There is hematuria which can be gross or microscopic. With drainage via an incompetent gonadal vein, varicoceles can occur with discomfort in men and pelvic varices with pelvic congestion syndrome can occur in women.
Diagnosis is challenging because it is one of the relatively rare non-gastrointestinal causes of abdominal pain (table).
Mesenteric ischemia
Median arcuate ligament syndrome
Nutcracker syndrome
Neuromuscular
Urolithiasis
Inflammatory aortitis/arteritis
Hypersplenism
Portal hypertension
Arterial aneurysm
Infections
Pelvic Congestion Syndrome
Endometriosis
Hernias
A history of left sided abdominal pain, flank pain, nausea, vomiting, associated pelvic pain, and episodes of hematuria are diagnostic. Examination is typically positive for left renal tenderness and flank tenderness. Laboratory examination include urinalysis for hematuria. Duplex, while technically challenging, will show renal venous compression with velocity elevation or loss of respirophasicity, CTA will typically show obstruction of the left renal vein with filling of collaterals, as will MRV.
Venography should be done in a stepwise manner (White protocol) to fully demonstrate the maldistribution of blood. That is the key word, maldistribution. I learned from my fellowship with Dr. White that performing venography in as upright a position as possible recreated the pathophysiology, the physics, particularly for pelvic congestion and nutcracker. Remember, this is a disease of bipedalism, of upright posture. Many negative studies done supine become positive, as the contrast will fall to where it prefers to go. As I have stated in the past, on the venous side, demonstrating drainage has different imaging needs than demonstrating flow. Pathologic venous drainage has three characteristics:
Varicose veins develop as an end stage process
Reversal of flow or reflux is demonstrated, particularly into small tributary veins
The midline is crossed in these usually small, now larger, collateral veins
While pressure gradients are nice if they are large, they are difficult to assess when they narrow to 1-2mmHg, particularly if they vary with cardiac cycle and respiration. Because we are assessing drainage, the distribution of contrast and the direction it goes is particularly important, and far more sensitive than pressure measurements.
Venography was done per a modification of Dr. White’s protocol for pelvic congestion:
Steep reverse Trendelenberg
Hand injection 10mL half diluted contrast, gently as to not create false reflux
Runs with catheter in left EIV, right EIV, left renal vein, right renal vein
With pelvic congestion workup, add selective bilateral gonadal and internal iliac veins.
I have started transposing gonadal veins when they have enlarged from chronic reflux (link, ref 2). Renal vein transposition was chosen because her ovarian vein was competent and too small to transpose (ref 1-3). While the patency rate of stents in veins seems to be acceptable, long term data is unavailable. Also, venographic appearances are deceiving -see the in-vivo measurement of the left renal vein after dissection:
Left renal vein at widest is 22mm, with expansion, possibly up to 28mm, but is relatively short. Do you see the SMA?The variability in diameter and length of the Wallstent in the 22-24mm diameter range makes this a challenging deployment. Given that I would not be able to closely follow this young patient, I felt compelled to recommend a durable solution (ref 4).
References:
White, J. et al, Left ovarian to left external iliac vein transposition for the treatment of nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2016;4:114–118.
Miler R, Shang E, Park W. Gonadal Vein Transposition for the Treatment of Nutcracker Syndrome. Annals of Vascular Surgery 2017, July 6. in press. http://dx.doi.org/10.1016/j.avsg.2017.06.153
Markovic J, Shortell C. Right gonadal vein transposition for the treatment of anterior nutcracker syndrome in a patient with left-sided inferior vena cava. J Vasc Surg Venous Lymphat Disord.2016 Jul;4(3):340-2. doi: 10.1016/j.jvsv.2015.09.002.
A case report co-authored by my recently graduated trainees, Drs. Roy Miler and Eric Shang. An update to be presented at Midwest Vascular Surgery Society Meeting in Chicago.
The patient is a young woman in her twenties who developed severe right sided abdominal and back pain about 4 months prior to presentation associated with bouts of bloody urine. Activity and standing exacerbated her pain and inactivity and recumbency relieved it. She gained 15 pounds because of her inactivity. Examination was significant for tenderness over her left kidney. Urinanalysis showed positive proteinuria and hemaglobinuria.
Prior to consultation with me she had had an MR venogram showing compression of her left renal vein by the superior mesenteric artery (nutcracker phenomena). The presence of hematuria, proteinuria, and pain (albeit atypically right sided) made it nutcracker syndrome.
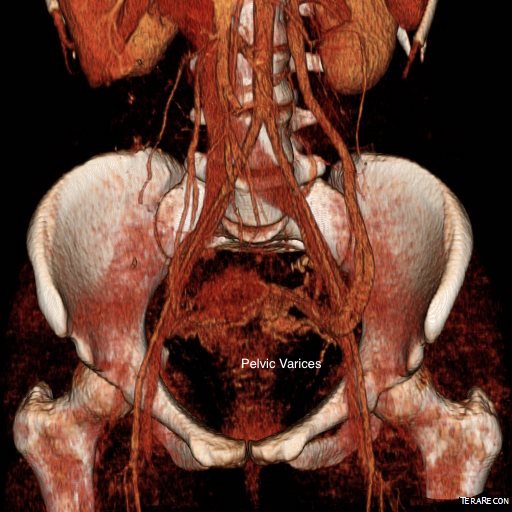
Dilated left gonadal vein and pelvic varices indicate left renal vein (LRV) ouflow obstruction by the superior mesenteric artery (SMA)
I ordered a renal duplex and a CT venogram for procedural planning.
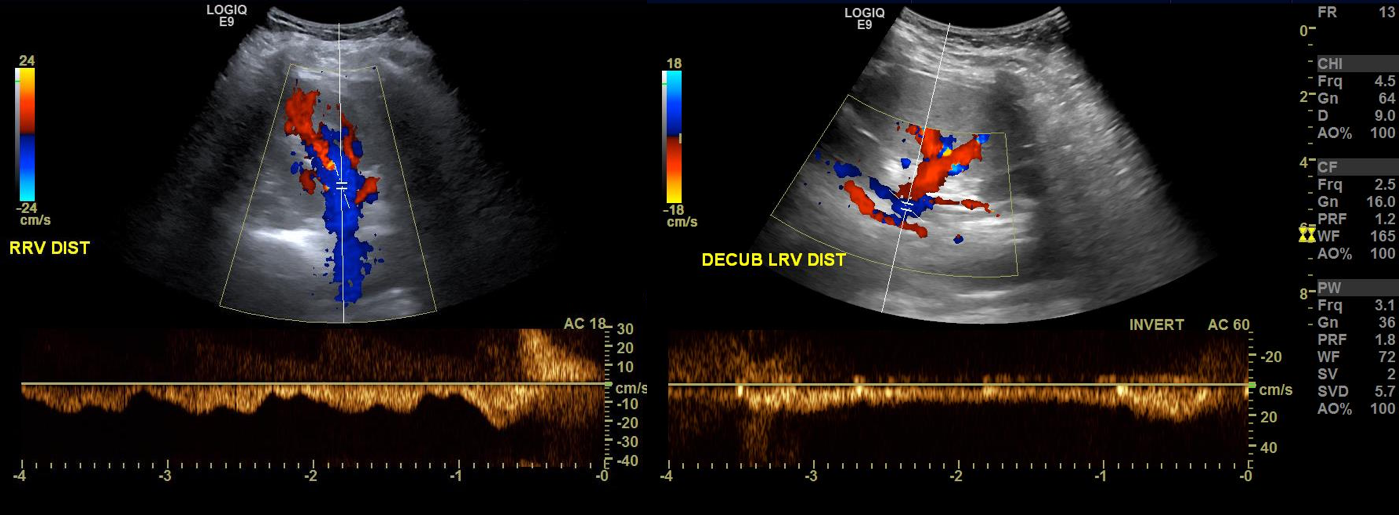
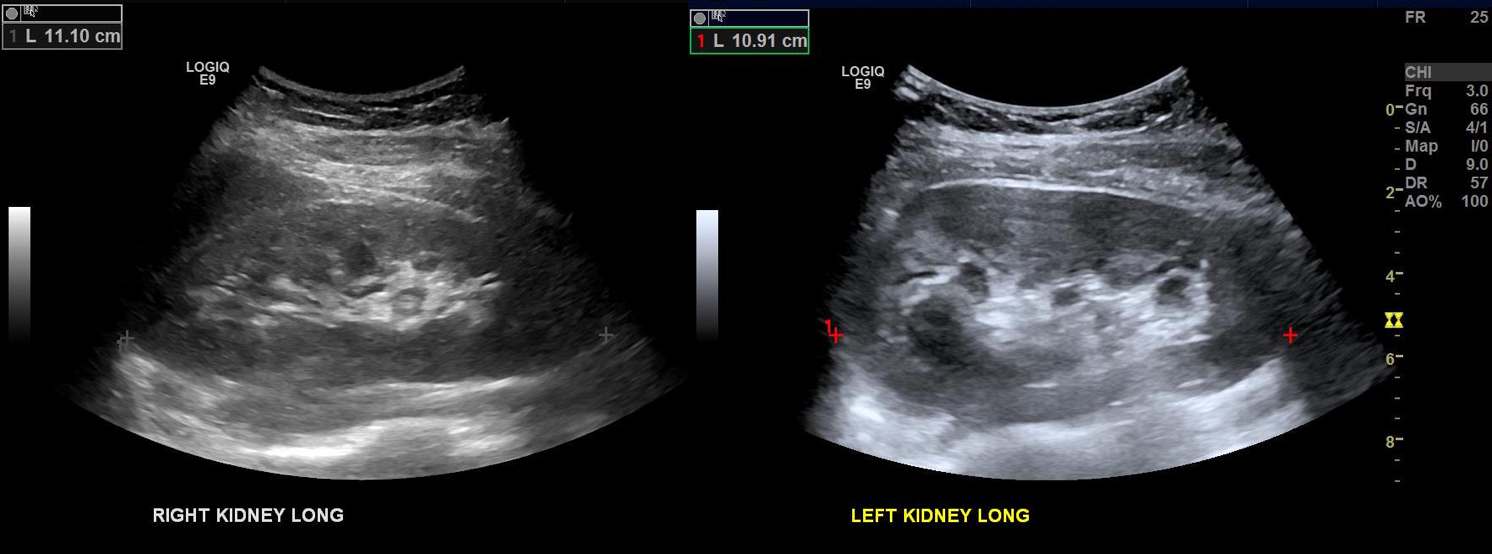
On the duplex, the proximal left renal vein (LRV) was not visualized. The right kidney had normal parenchymal appearance and blood flows, while the left, the kidney appeared distended and had flows consistent with outflow obstruction.
Spectral Doppler flows show respirophasicity in right renal vein(RRV), outflow obstruction on left renal vein (LRV)
The left kidney is swollen and tender.
CT Venography showed the gonadal vein to be an important outflow vessel to the left renal vein with dilated proximal segment and reflux into pelvic varices.
A left gonadal vein to iliac vein transposition was planned via a left lower quadrant retroperitoneal exposure. On the table, a venogram was performed with selective access of the left renal vein.
The injection from the LRV showed severe compression of the LRV with a channel only slightly larger than the sheath and avid reflux into the gonadal vein. Selective access into the gonadal vein and venography from a confluence in the pelvis showed that flow was one way from the LRV into the gonadal vein and this filled a large region of pelvic varices.
The gonadal vein was large caliber and refluxed into two large veins in the pelvis. The one that fed the varices was not selected for transposition, but rather the longer straighter tributary. A catheter was left for easier identification during the dissection.
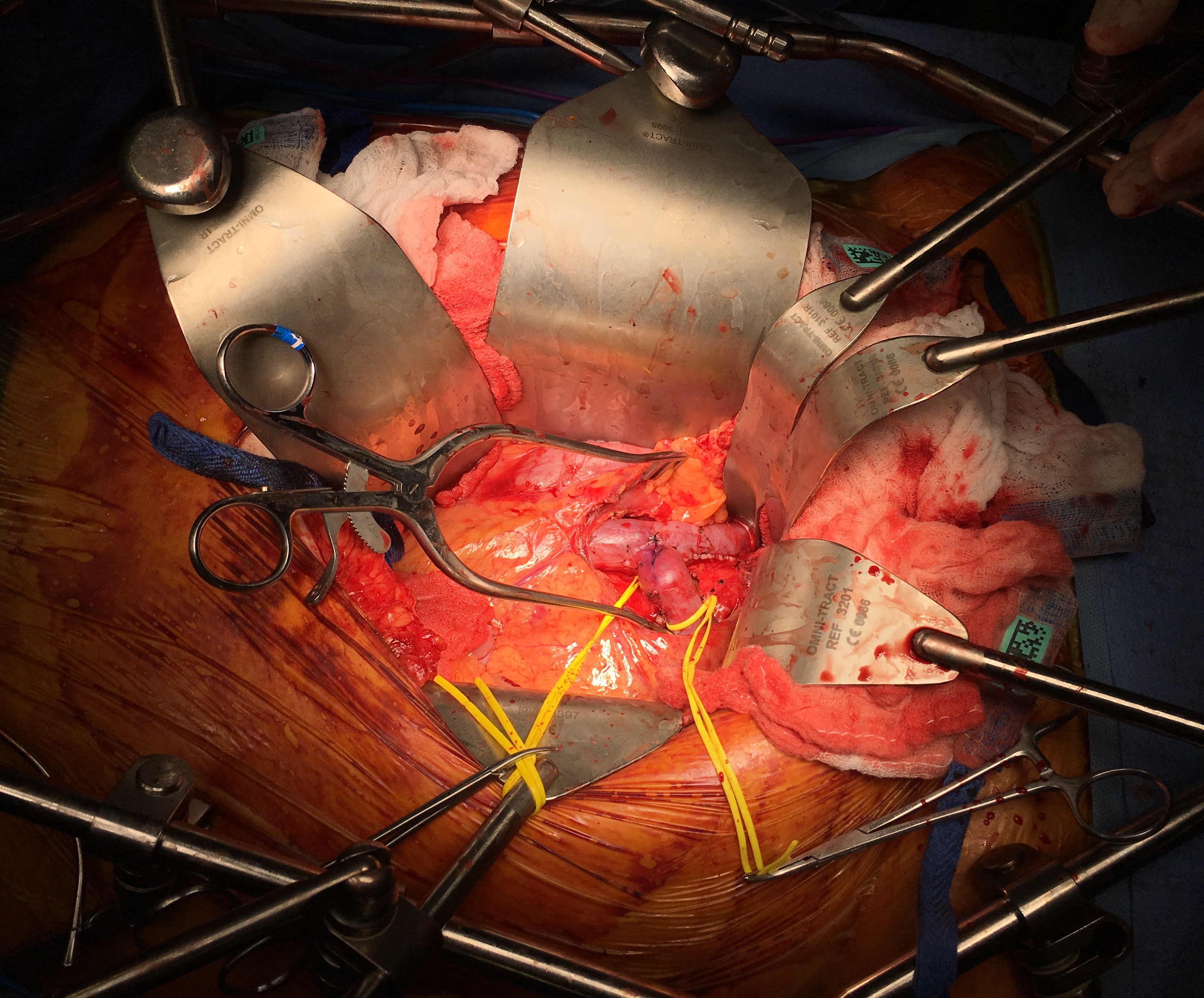
A left lower quadrant incision was made and a retroperitoneal dissection performed exposing the gonadal vein and iliac vein.
Prior to ligation of the tributaries, a sheath was inserted and through this a LeMaitre valvulotome was brought up to the left renal vein and carefully deployed and pulled back, cutting the valves. This greatly increased the outflow from the vein as evidenced by the height of the blood spout from the vein when the sheath was removed. The varices were ligated at their root -treating them definitively. Transposition was to the external iliac vein, and I could see the feasibility of a laparoscopic or robotic approach to this operation (ref 3).
Completion venography showed excellent flow from the LRV down the gonadal vein into the iliac venous system.
The patient lost less than 10mL of blood and was discharged on postop day 2. Gratifyingly, all of her preoperative pain resolved and her UA showed no more hemoglobinuria or proteinuria.
Discussion
The described treatment options for nutcracker syndrome include (ref 1):
Medical therapy aimed at decreasing renal venous hypertension (for hematuria)
Renal autotransplantation
Left renal vein transposition
Left renal vein to vena cava bypass (autologous or PTFE)
SMA transposition
Nephrectomy
Gonadal vein to IVC bypass
Exovascular stenting (wrap of renal vein with ringed PTFE graft)
Endovascular stenting
Many of the operations are of historic interest. Stenting deserves some comment. The patient self referred because she had read multiple reports of cardioembolization on internet support group comments. The largest nitinol stent (self expanding) available is 14mm. Wall stents in larger diameters are available, but are stiff, poorly conformable, and will elongate if constrained by a non-dilating stenosis like the external compression by the SMA. While acceptable results have been reported, the long term results (20-70 years) for younger patients is unknown. Migration is highly morbid, and usually to the heart, requiring sternotomy and cardiotomy to retrieve the stent. Optimally, a conforming 16-28mm self expanding stent should eventually become available, but conformability is typically inversely proportional to radial strength, and it is the less conformable stents that migrate. Work is ongoing to bring larger diameter nitinol stents for venous indications. The difference between May-Thurner Syndrome and Nutcracker syndrome isn’t merely the size of the veins and stents. The iliocaval confluence is relatively static with some movement of the lumbosacral joints and well suited for treatment with the relatively nonconforming Wall Stents. The left renal vein under the SMA is a very dynamic environment with motion of the SMA and the kidneys with respiration, ambulation, and activity leaving stents vulnerable early to migration and later to fracture.
The left renal vein transposition to the IVC is a nice operation with a good track record (ref 2). The downside is the long midline incision required with transperitoneal exposure. There is bleeding risk and postoperative complications of ileus, wound infection, and small bowel obstruction. Looking at the CTV, it seems obvious that the gonadal vein crosses over the iliac vein in the pelvis and would be a straightforward, less morbid, less invasive option. A review of the literature reveals only a single reference discussing three cases of left renal vein transposition (ref 3), and it was done with a surgical robot. I think that a laparoscopic approach would be simpler and less invasive and will consider developing this if volumes justify it. That said, the open retroperitoneal approach is very straightforward and well used exposure. Using venography to set up and then confirm the results of the transposition was helpful. I don’t think that measuring pressures and diameters and taking calipers to calculate stenoses is all that useful and in some instances a harmful method of justifying endovascular treatment of nutcracker phenomena in the absence of serious symptoms and a careful deliberate workup which includes a good history and physical, a UA, a duplex and CTV.
Intervening on the gonadal vein to iliac vein anastomosis should be straightforward from a groin or thigh venous access on the ipsilateral side. This operation doesn’t preclude any future interventions on the LRV. The pelvic varices were treated with direct ligation. The patient’s pain was successfully relieved in the short term.
Conclusion: Open retroperitoneal left gonadal vein to iliac vein transposition with gonadal vein valvulotomy is effecting in treating nutcracker syndrome.
References
Kurklinsky AK, Rooke TW. Mayo Clin Proc. 2010 Jun; 85(6): 552–559.
Reed NR et al. J Vasc Surg. 2009 Feb;49(2):386-93;













 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).