
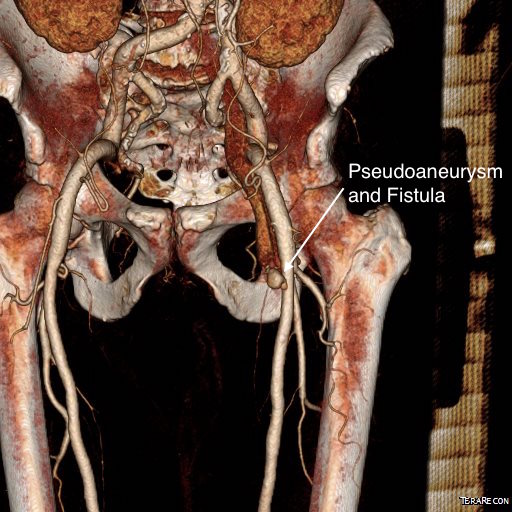
The patient is a middle aged man who after an interventional procedure was referred to my clinic with an expanding hematoma due to a pseudoaneurysm complicated by an arteriovenous fistula. He was a week out from his procedure and had grown a hematoma roughly the size of a hard boiled egg in his left groin which caused him pain. A duplex scan showed a pseudoaneurysm (below) with fistula flow.
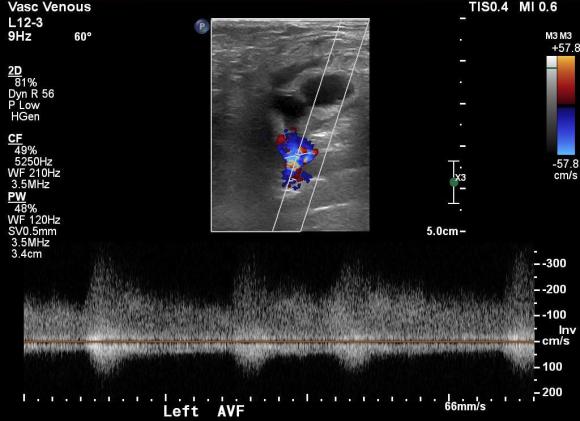
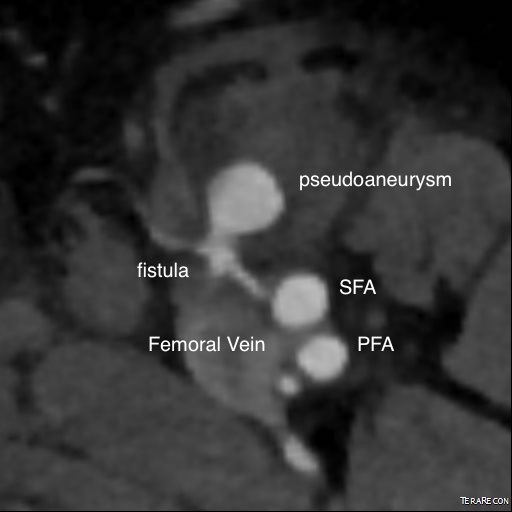
On examination, he had this well circumscribed indurated hematoma of hard boiled egg size with tenderness. There was a bruit on auscultation. Duplex showed a small chamber of flow adjacent to the proximal superficial femoral artery emptying into the femoral vein. Doppler in the common femoral vein showed relatively high fistula flow, and this is reported to be associated with failure of thrombin injection. CTA (top) demonstrated flow of contrast from femoral artery to vein through a pseudoaneurysm chamber that laid between. Angulation to an axial orientation showed this better (below).


Arteriography showed much of the contrast from injection of the pseudoaneurysm to preferentially go to the artery which made me worry less about creating a DVT/PE. With balloon inflated (below), thrombin was injected and balloon inflation held for about 30 seconds.

There was resolution of flow in the pseudoaneurysm and in the fistula. Before and after duplexes are composited below.
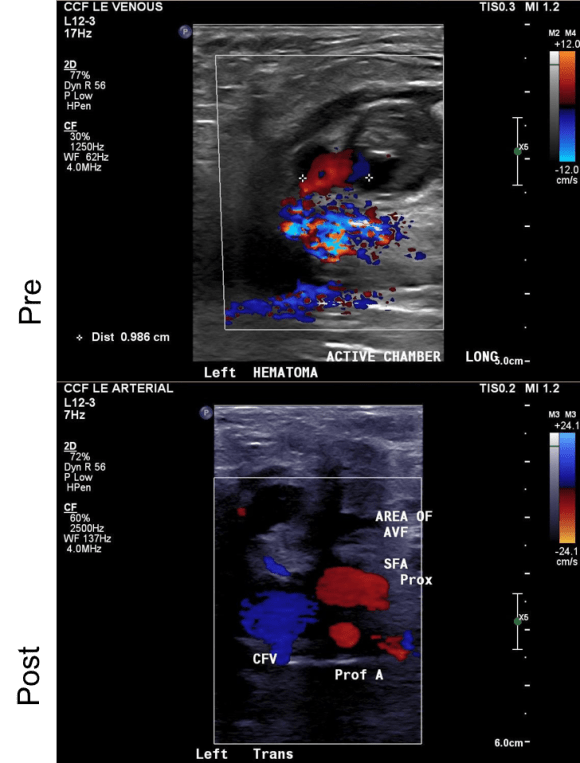
Repeat duplex on the following day showed resolution of the pseudoaneurysm and arteriovenous fistula.
In the days before ultrasound guided thrombin injection of pseudoaneurysms, open surgical repair of these was fraught with complications. First, these patients typically had cardiac disease. Second, they were usually anticoagulated often with multiple agents. And finally, they were many times obese, making not only the operation fraught with complexity, but the ultimate wound healing a delicate and rare phenomena. Even now, we get emergency repairs when access hemostasis fails, and these patients are typically high risk. With hematoma evacuation, inflammation, lymph leaks, and infections may follow; the patient was correct in his enthusiasm for agreeing to proceed with a minimally invasive effort.
As to the techniques, they are all well established in the vascular surgeon’s toolbox. Ultrasound guided access of the pseudoaneursm should be obtained before arterial occlusion. This was facilitated by general anesthesia which kept the patient from moving. Having access to excellent ultrasound and angiographic imaging made this possible. The patient felt much better and was discharged home the next day after his confirmatory duplex.
