George W. LeMaitre, Chairman and Chief Executive Officer, LeMaitre Vascular, Inc.
Dear George,
If you go to the LeMaitre Vascular website, there is a link to the story about the company’s founding by your father, Dr. George Lemaitre, which I heard first hand over dinner hosted by him and your mother many years ago. The original LeMaitre Valvulotome has followed me through my career from surgery residency in the 90’s to a recently closed tenure as vascular chief at Cleveland Clinic Abu Dhabi. There is no in-situ bypass that I perform where I am not struck by your father’s story and by the ideals passed by him into the company he founded which had at its core the desire to help vascular surgeons take care of their patients. There are so many other companies, most of them in fact, in this vascular space who are investor-first when it comes to decisions about what diseases, procedures, and specialties to support, but LeMaitre Vascular has always felt different.
For decades, LeMaitre Vascular seemed focused on helping vascular surgeons care for their patients with unique, purpose-designed solutions. Engineering at its finest. It gave life to many ingenious products like Anastoclip, Unballoon, and LeverEdge, that seemed to spring from the minds of working surgeons and physicians directly into their hands, much like the valvulotome. The best ones appealed to the many surgeons who wanted to advantage their patients and their institutions with both lower cost, time efficiency, and equivalent or better outcomes to the usual way things are done. Unfortunately, we live in a universe where the incredibly potent gravitational pull of the investor interests is for high volume, high margin items. This pull greatly exceeds that of the bright yet smaller stars and moons that are common sense, durability, and sustainability. Items that drop out of peel packs, are used once, and thrown into a landfill, have become everything used in healthcare. The sudden absence of EndoRE (remote endarterectomy) on the LeMaitre product page speaks volumes to this. Something that is low volume, durable, subject to repeat use like a set of Vollmar Rings, which are purchase once and used for a long time, must have little appeal to those who author investor reports. It is in such an decision environment that EndoRE the product must have been cancelled from the LeMaitre Vascular web page (link). I wouldn’t think that LeMaitre would give up manufacturing the eponymous valvulotome for low sales figures, but it did give up on remote endarterectomy for that reason.
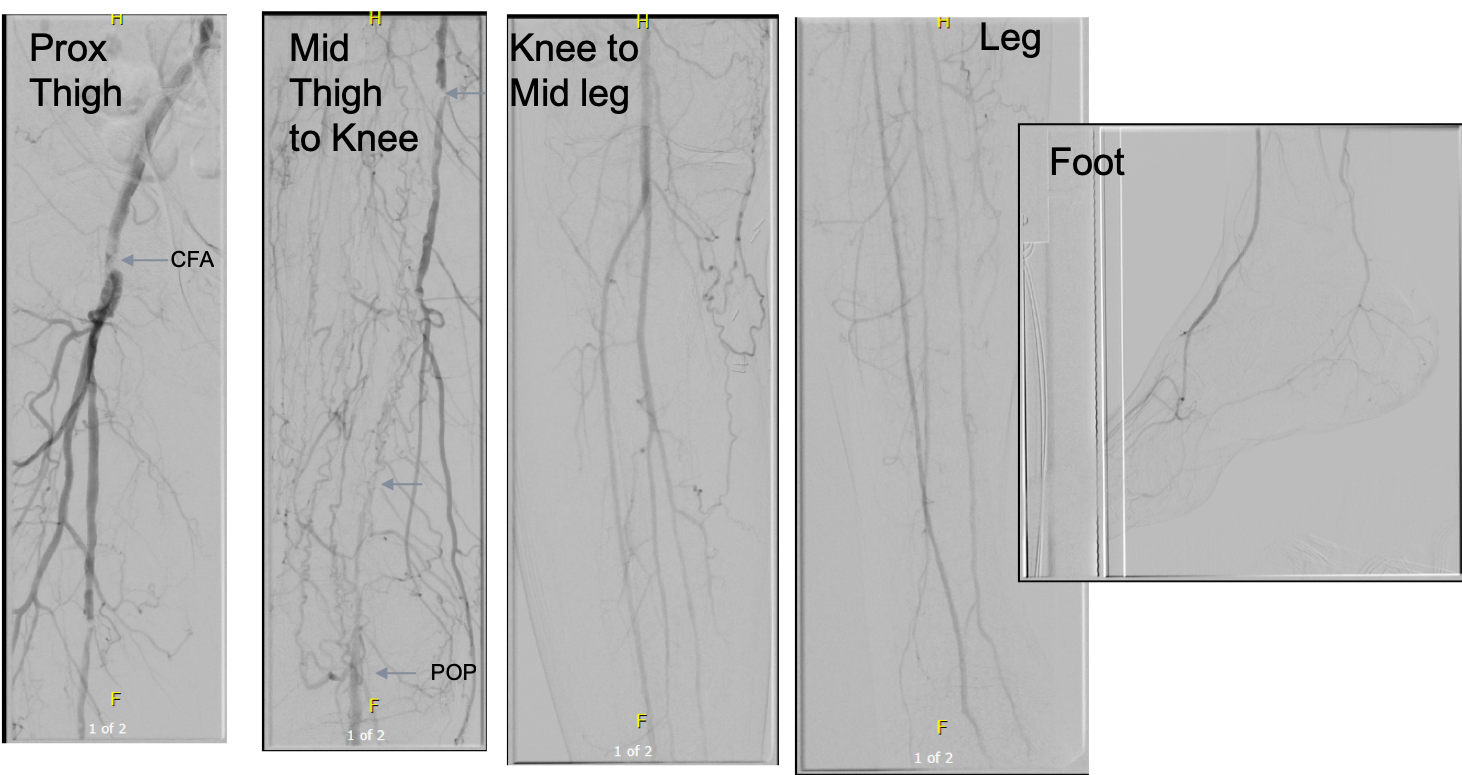
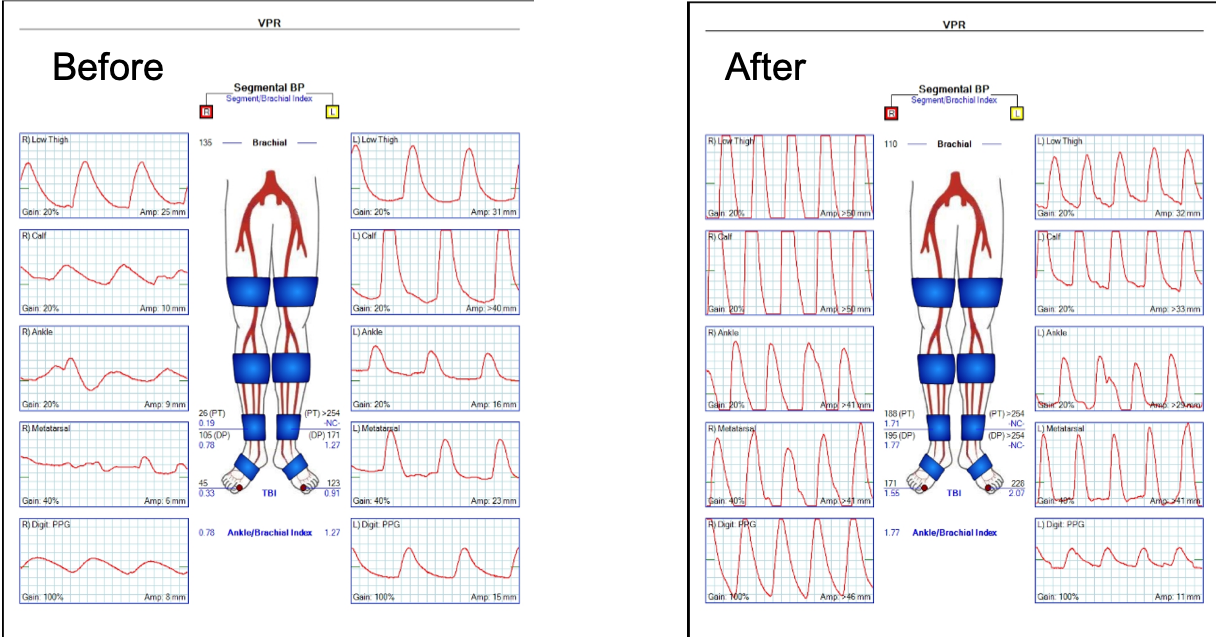
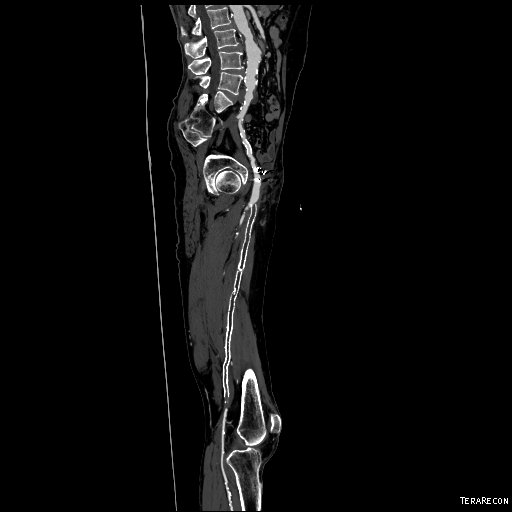
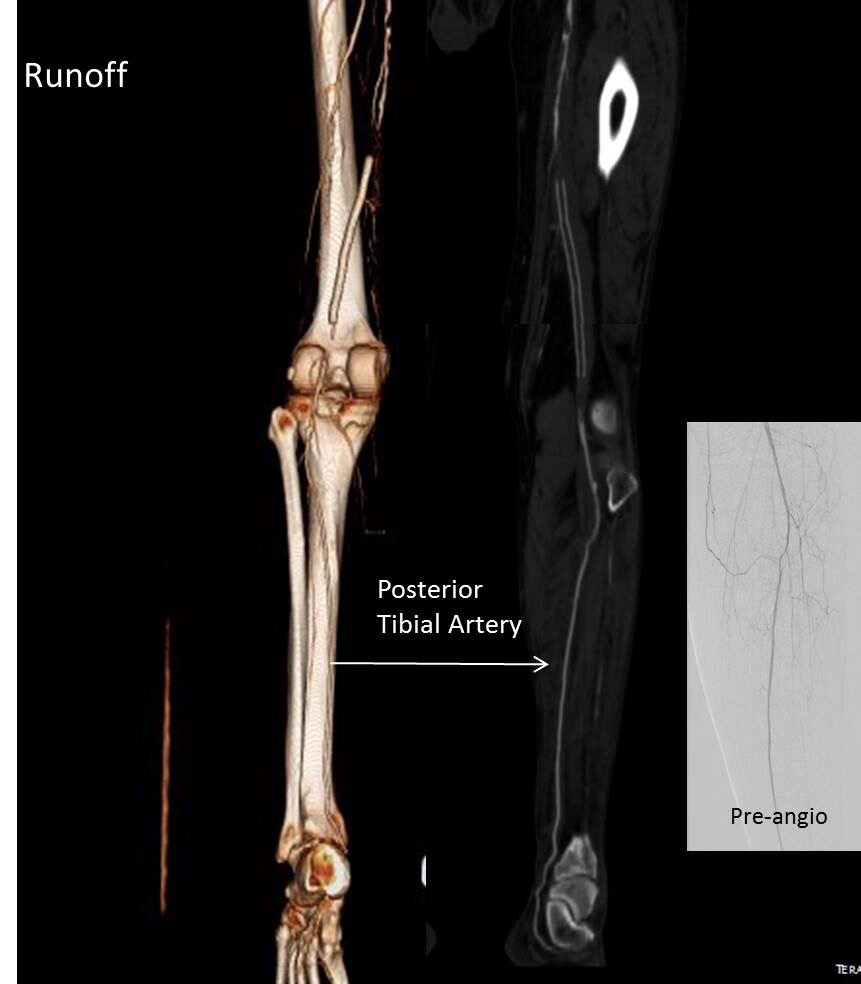
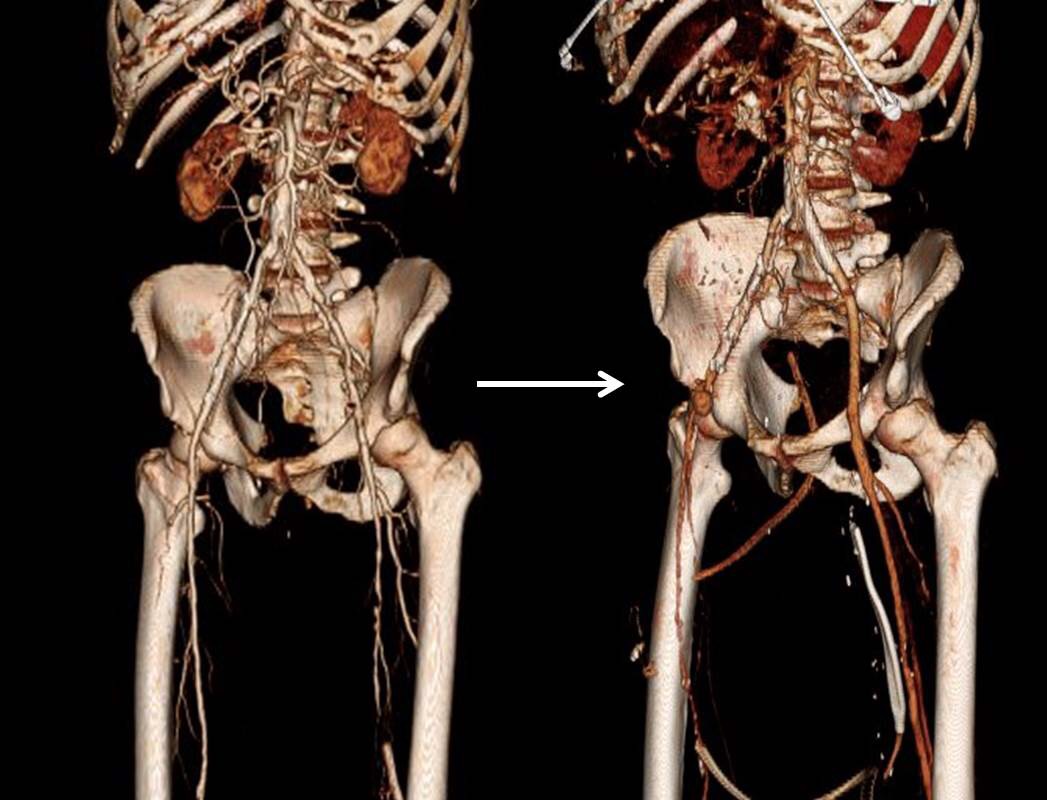
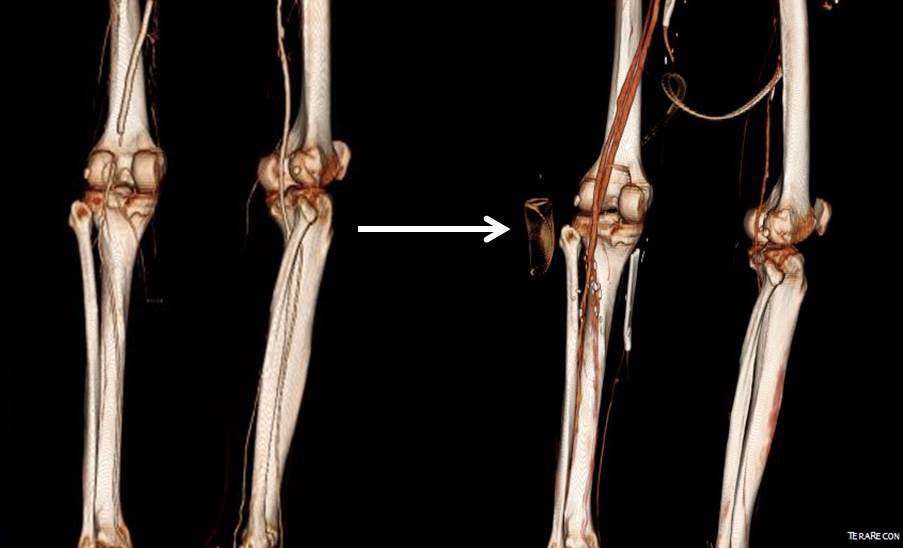
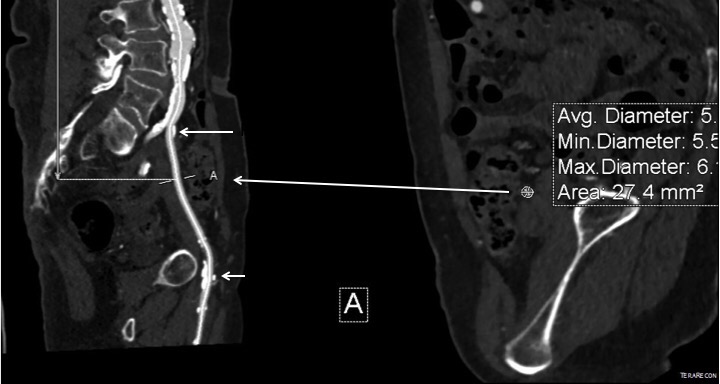
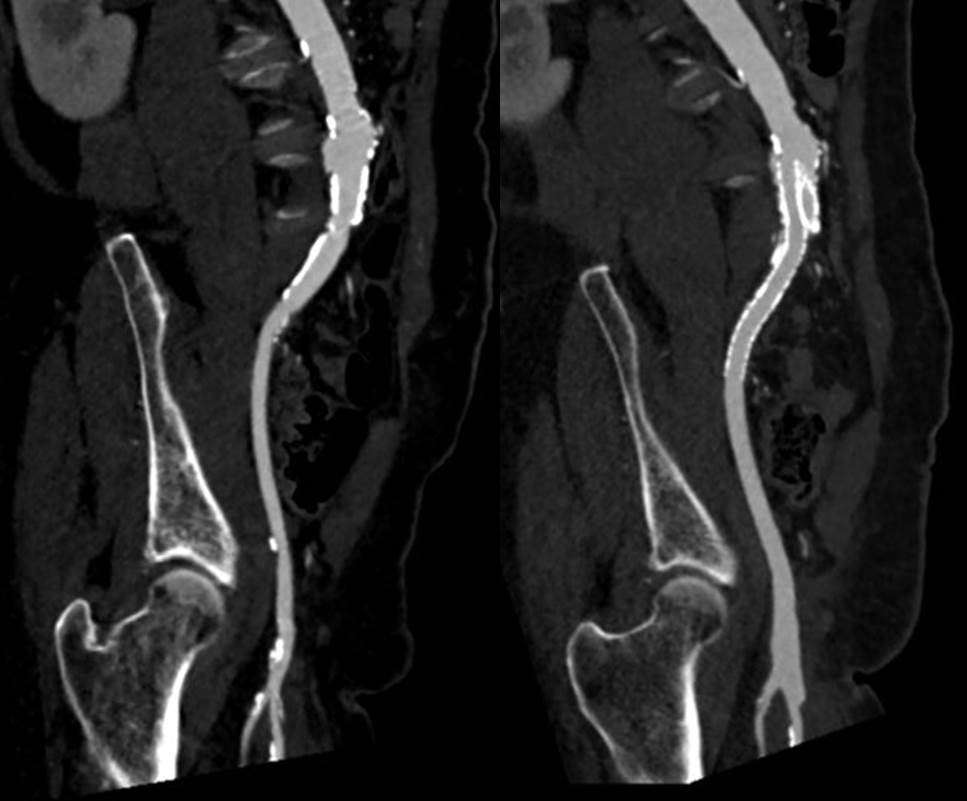
Let me show you one of the first cases I did after returning to Cleveland. I am now practicing at Fairview and Avon Hospitals, premier flagship hospitals in the Cleveland Clinic fleet, on Cleveland’s west side, and a patient arrived while I was on call with sudden onset of pain in his leg from a lack of blood flow. He had occlusive atherosclerotic plaque extending from his external iliac artery to the above knee popliteal artery causing ischemic rest pain.

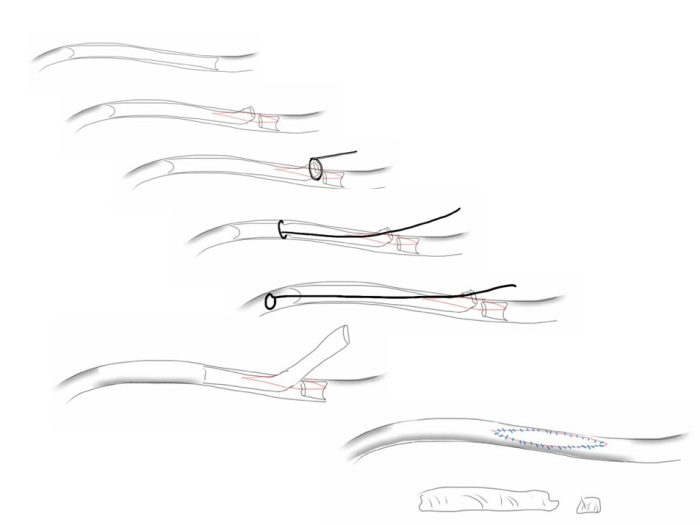
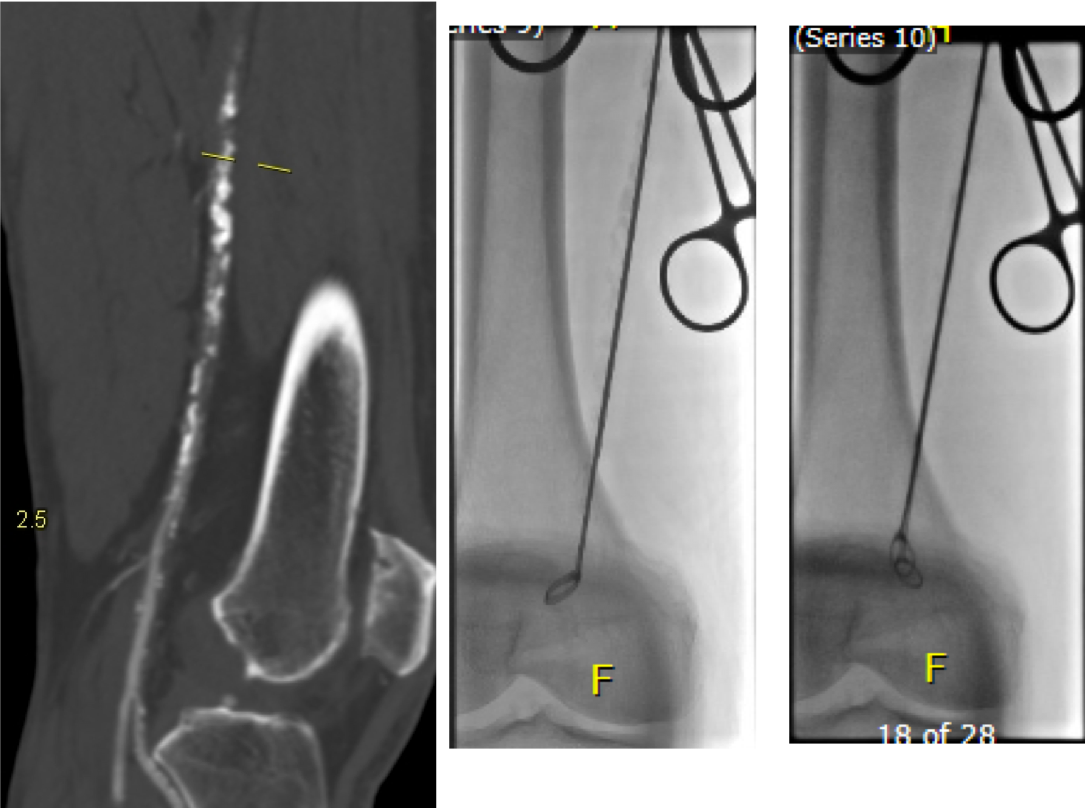
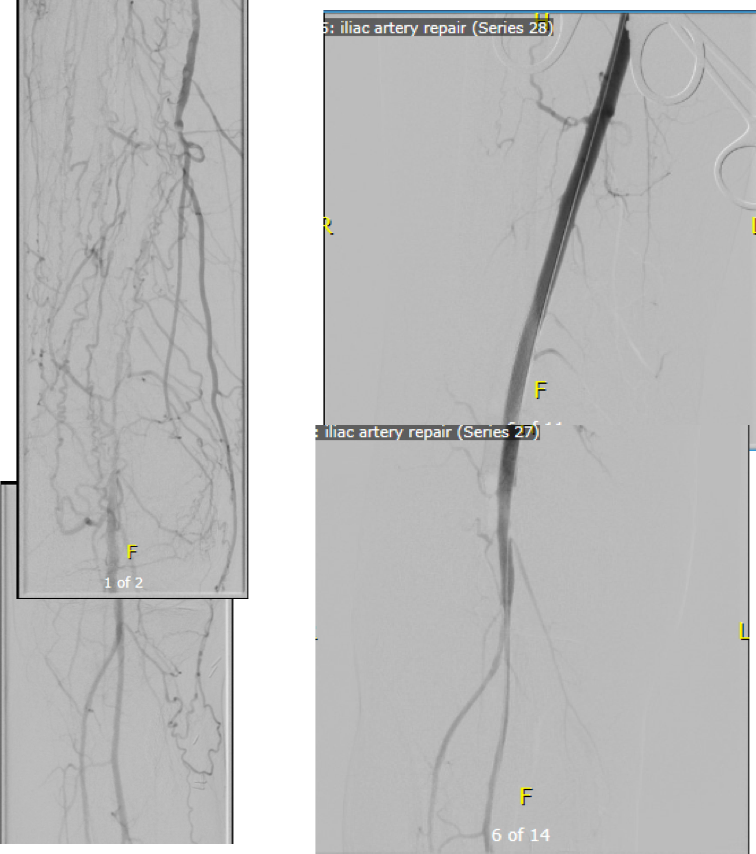
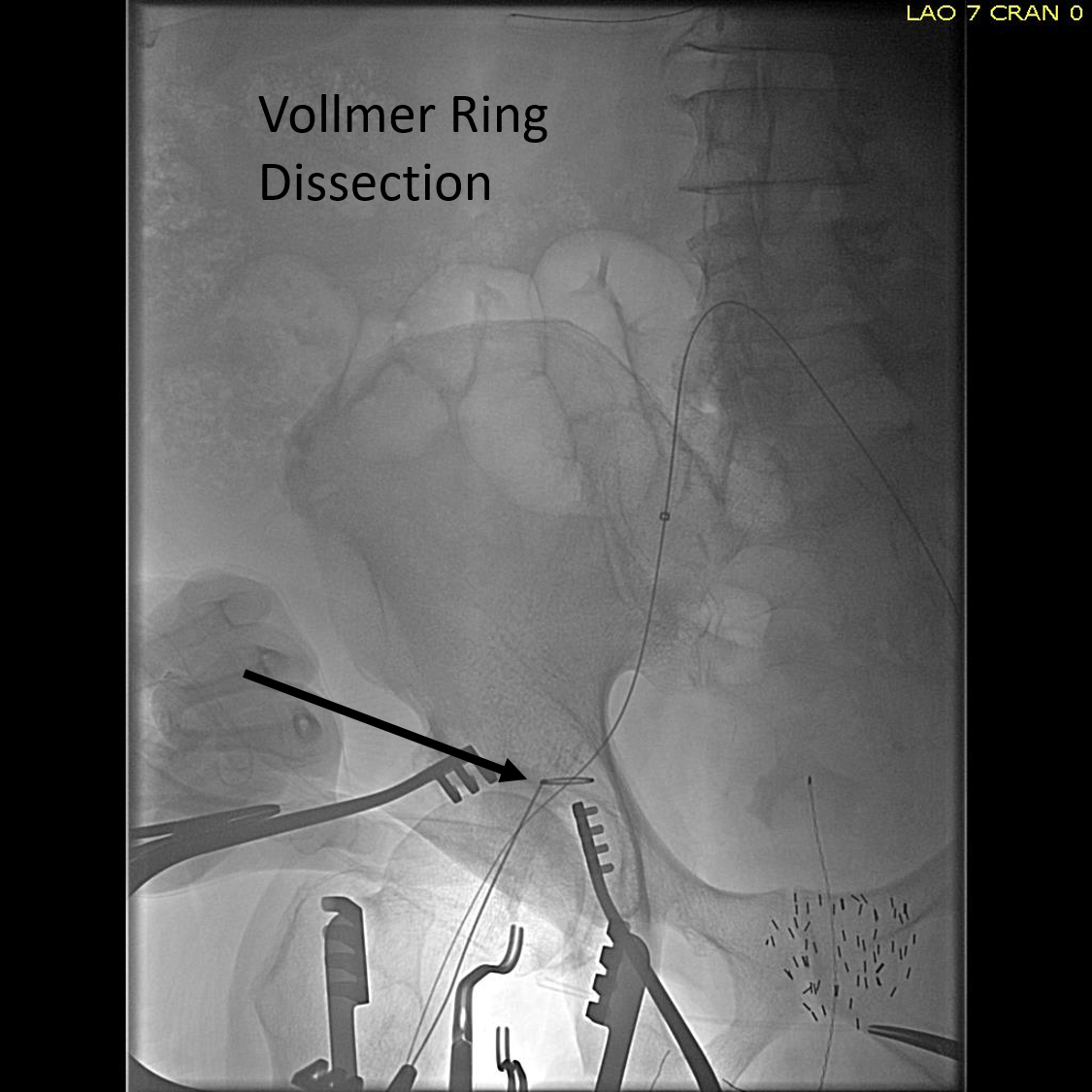
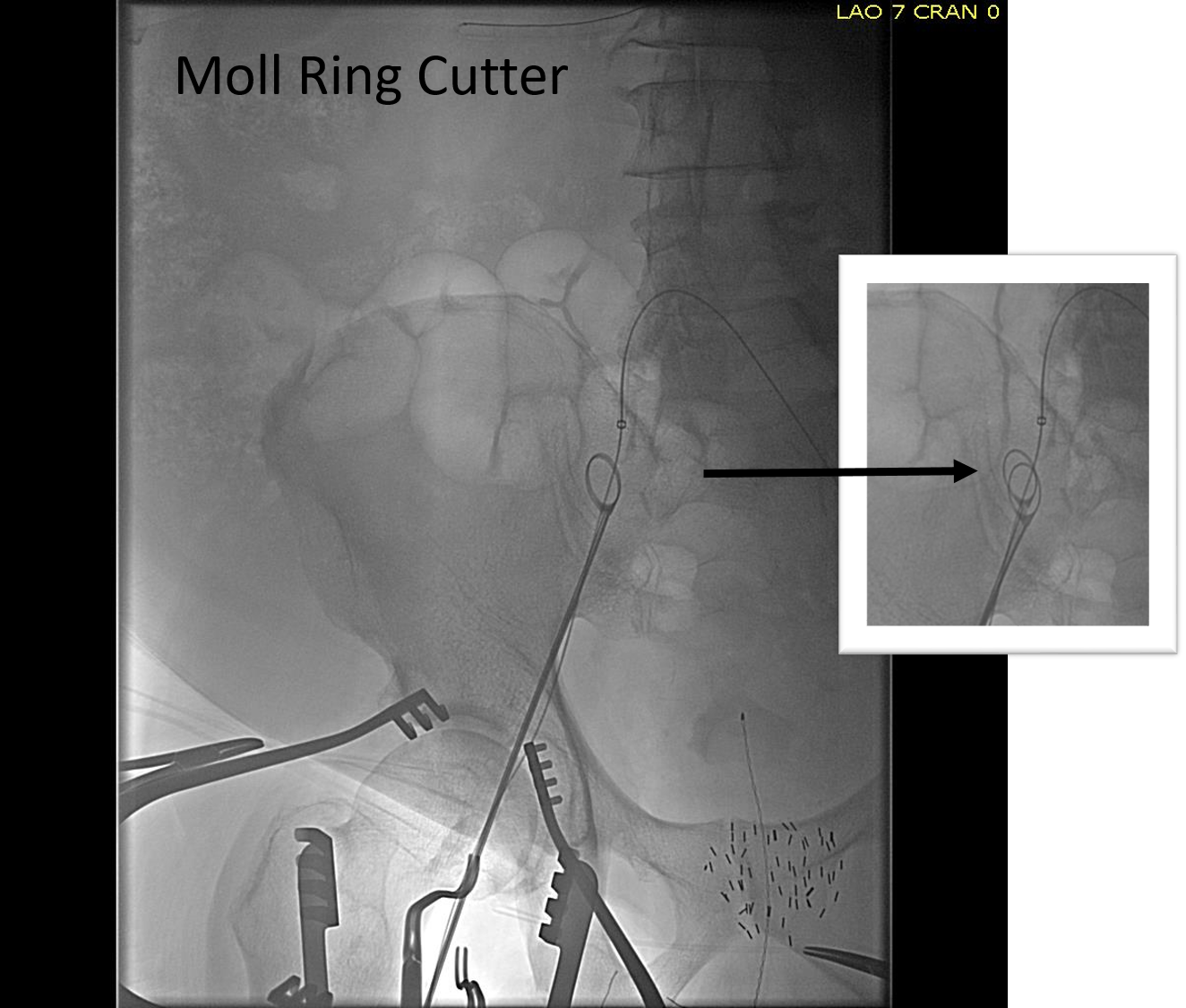
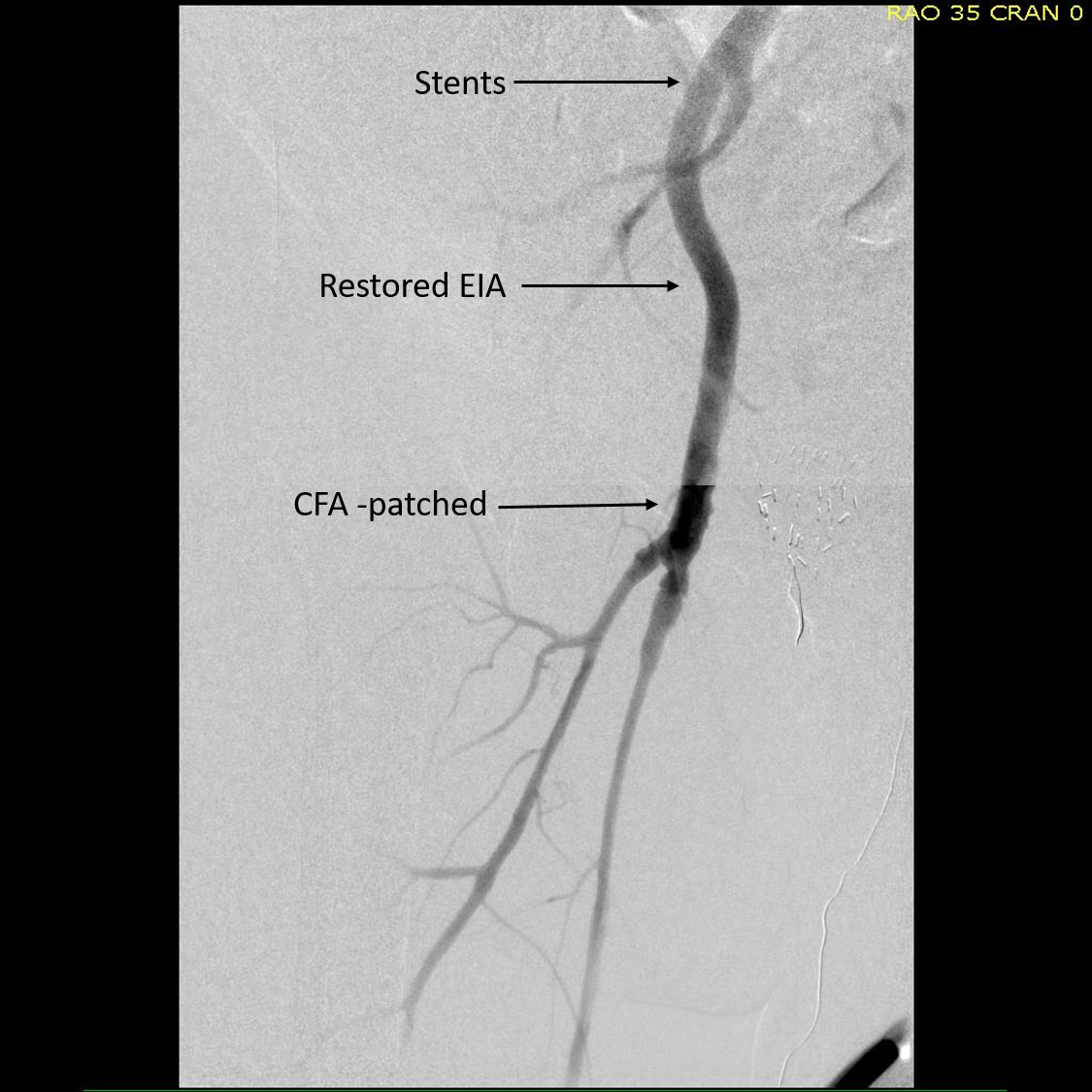
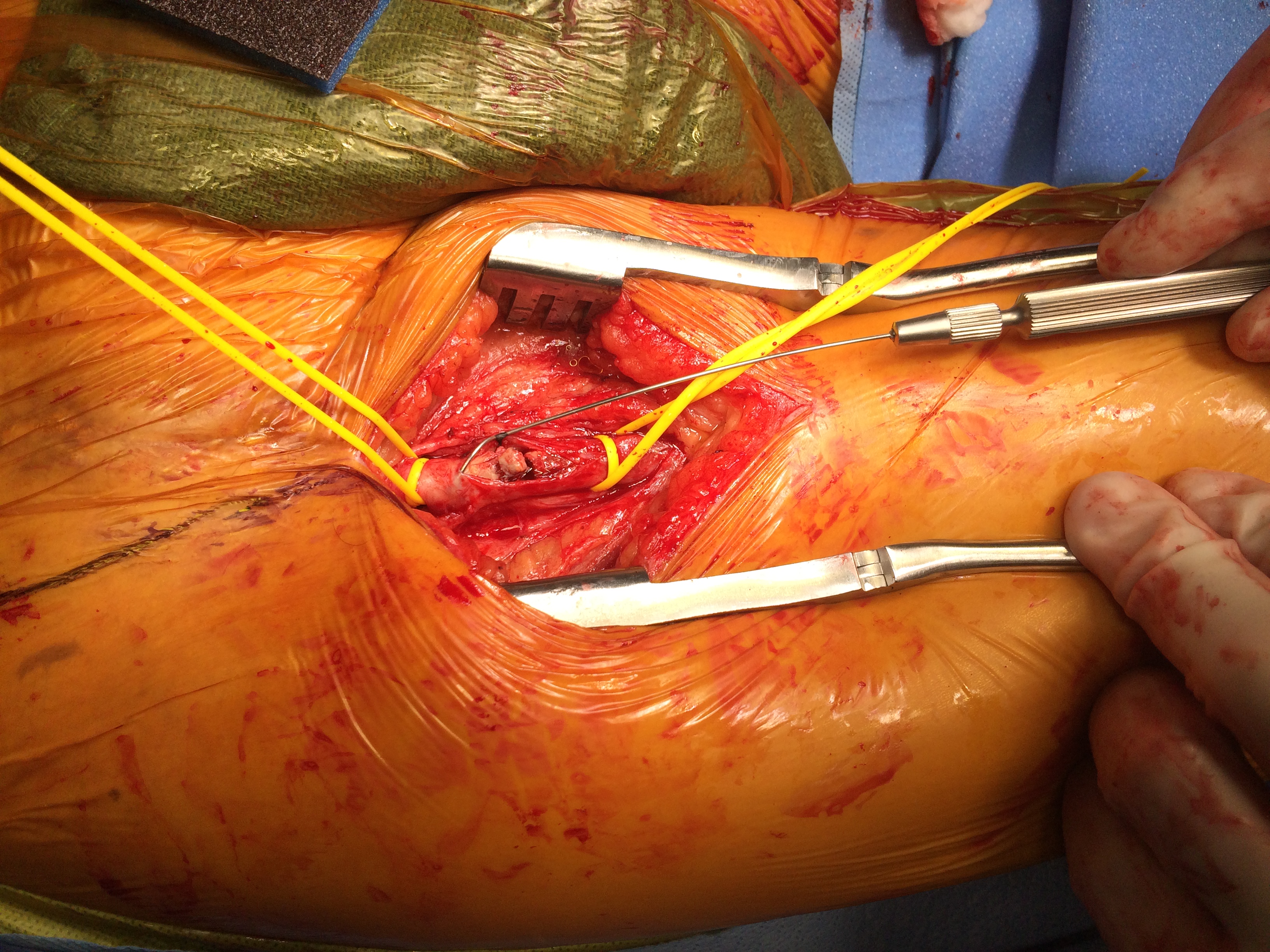
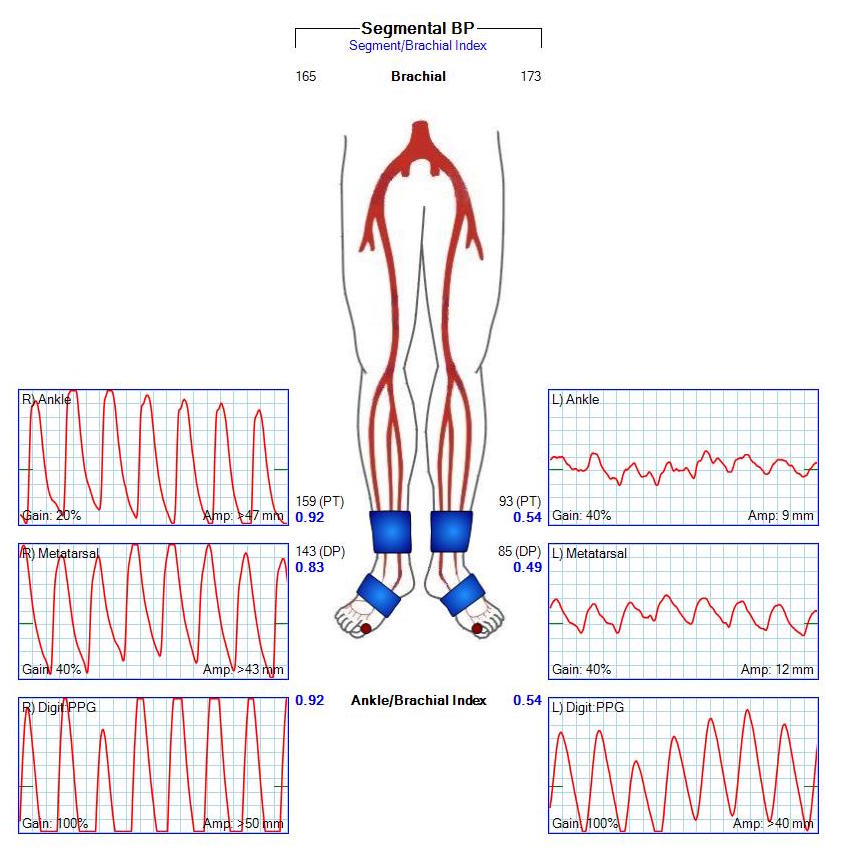
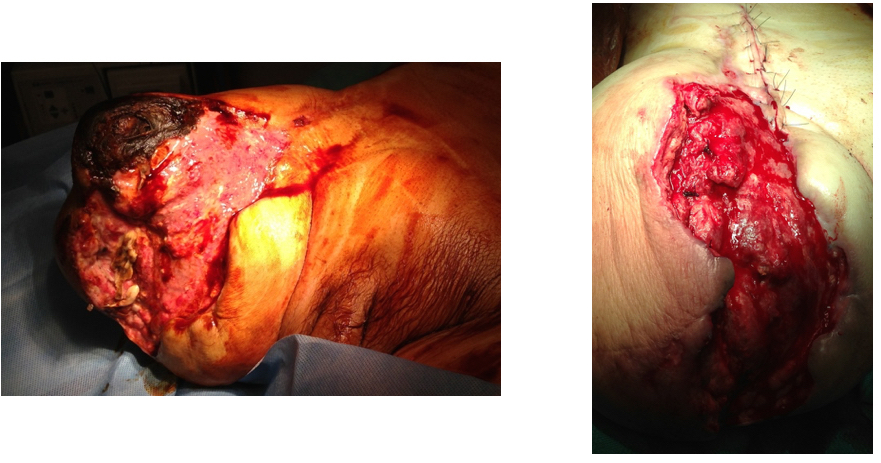
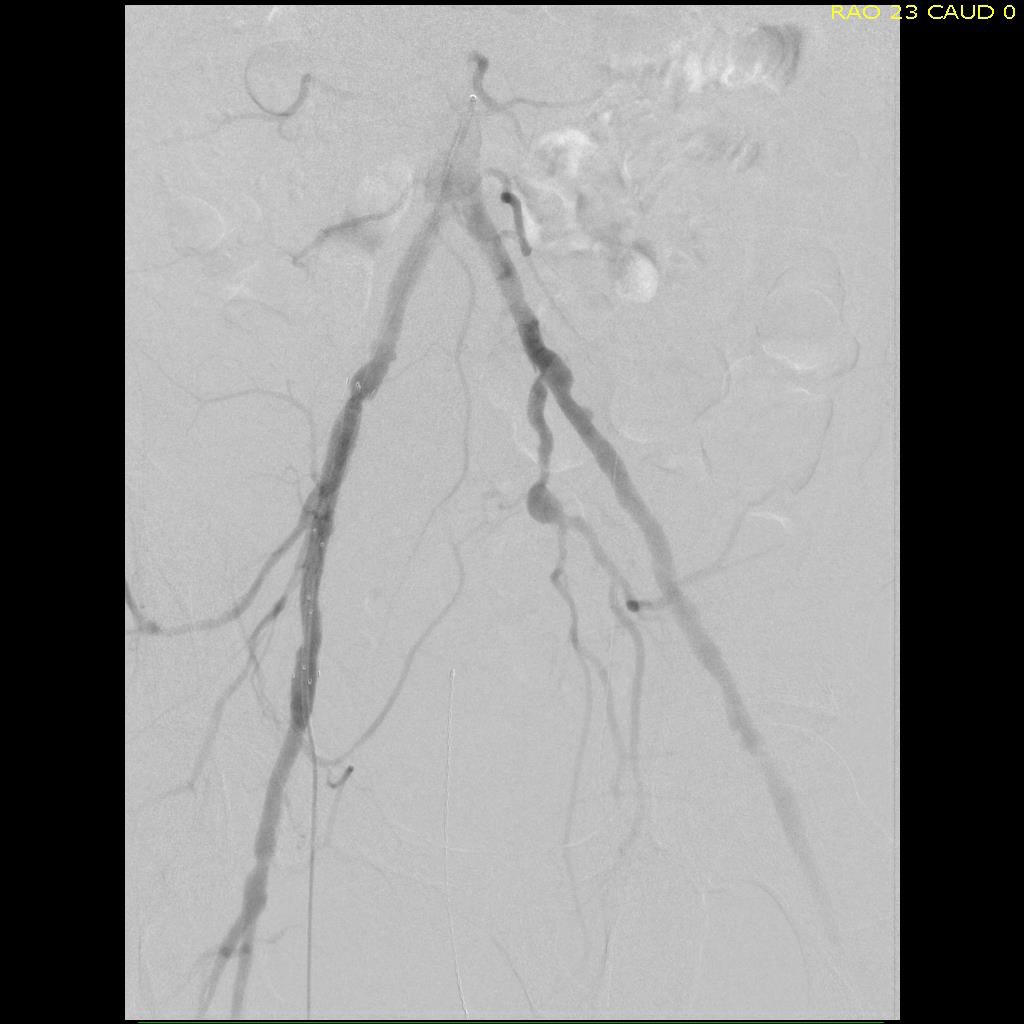
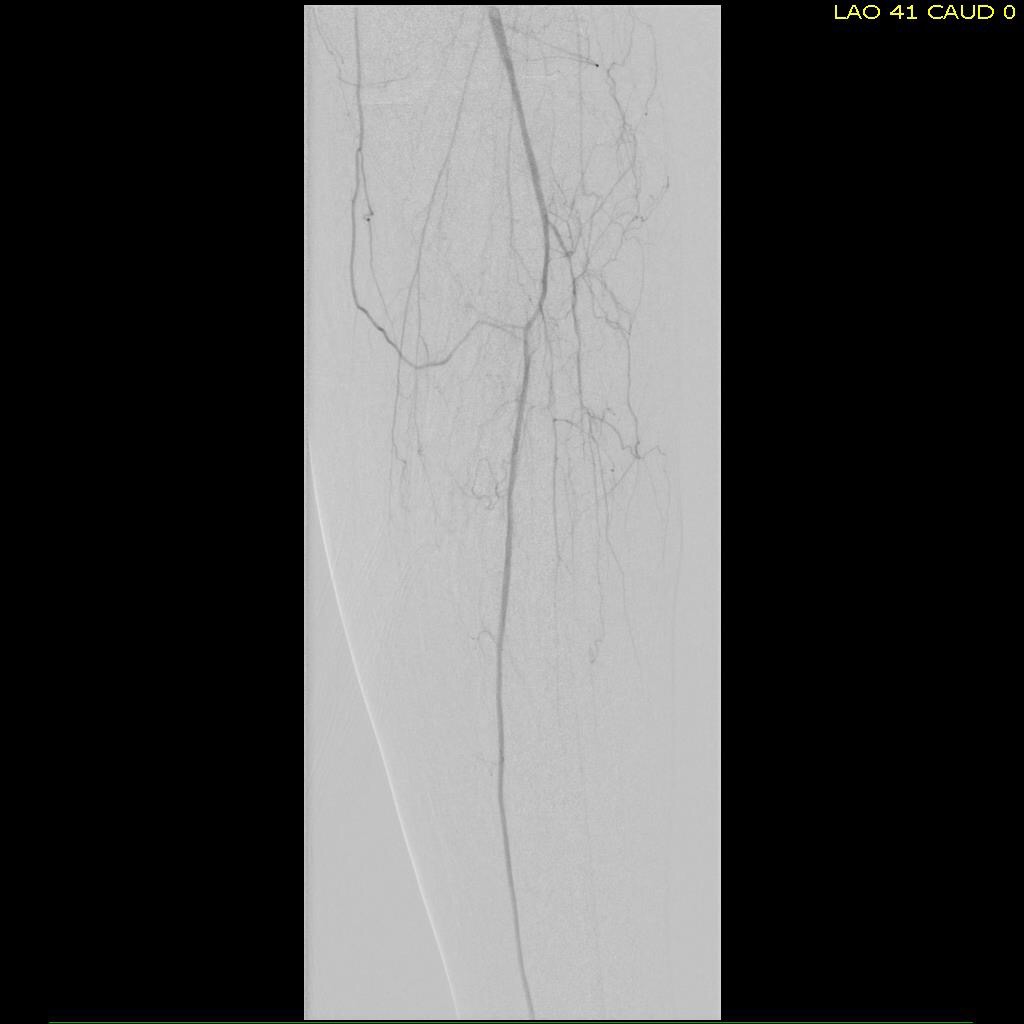
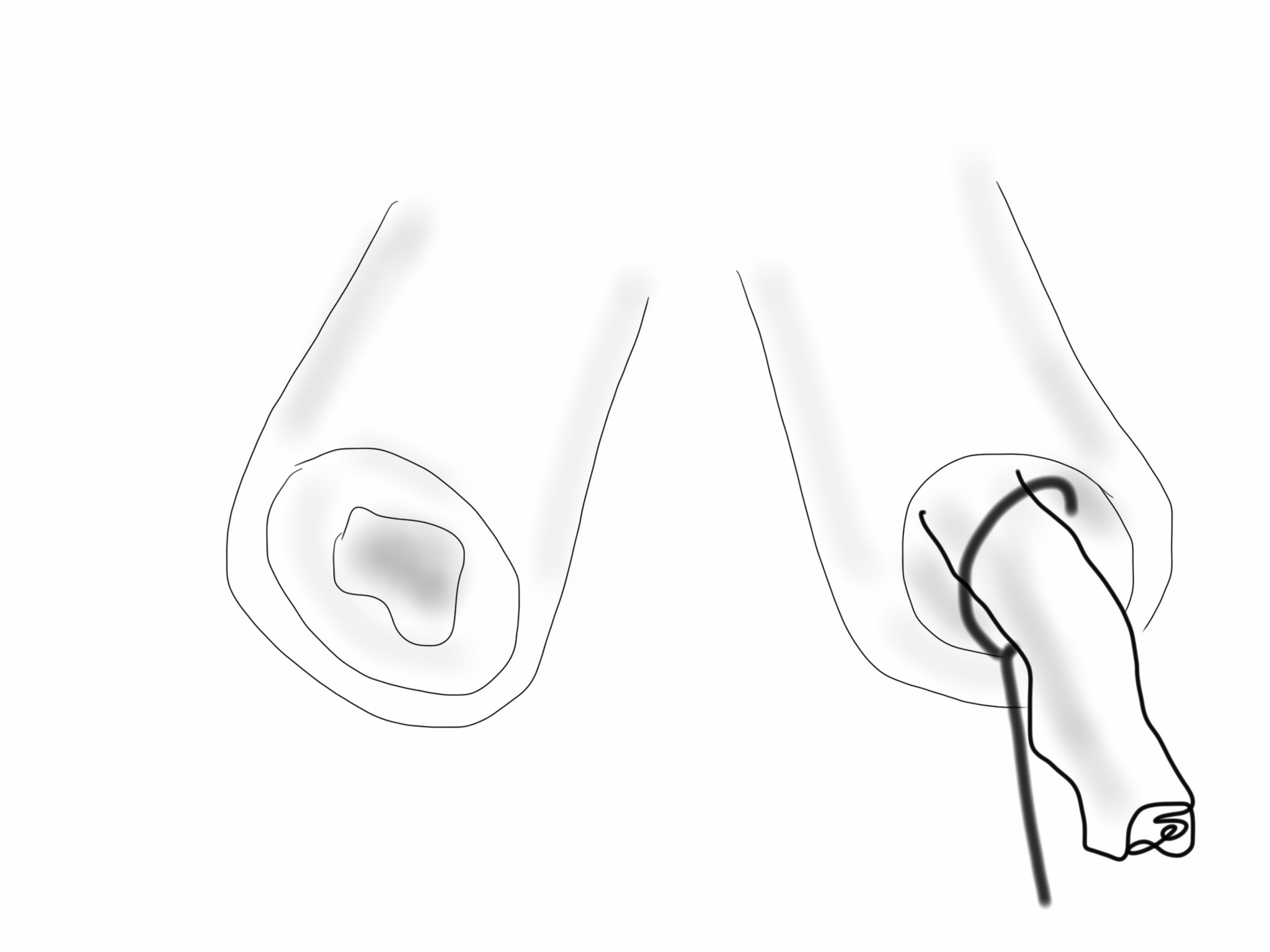
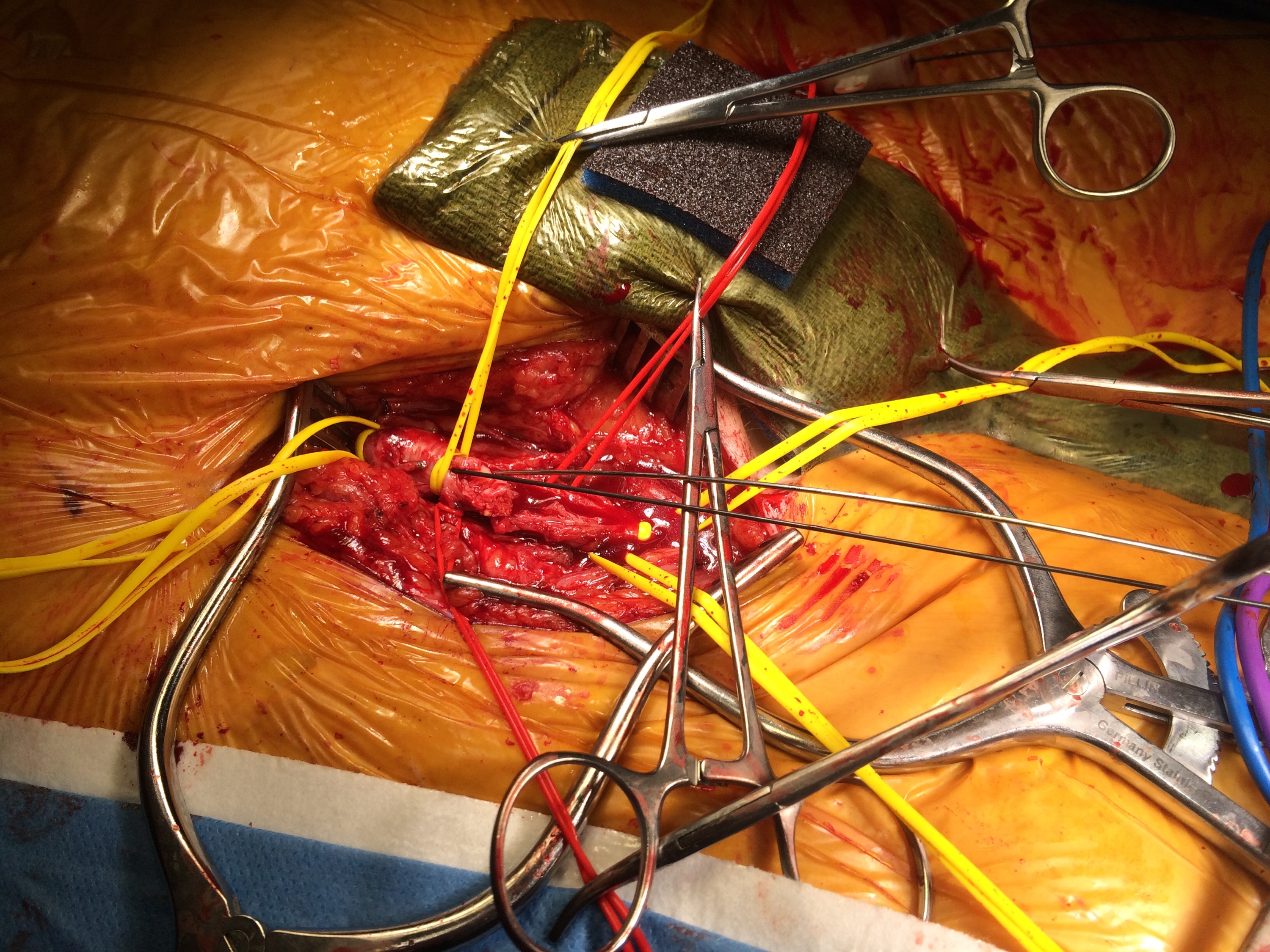
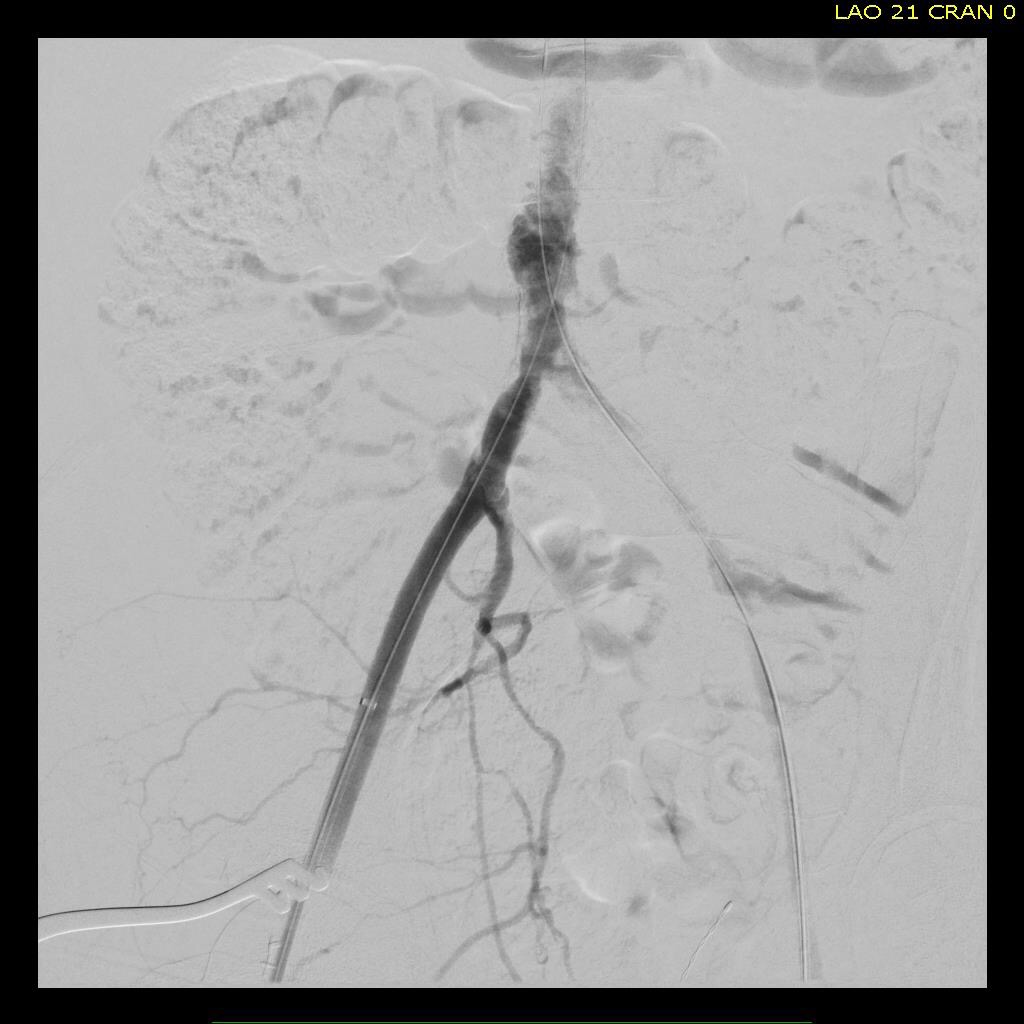
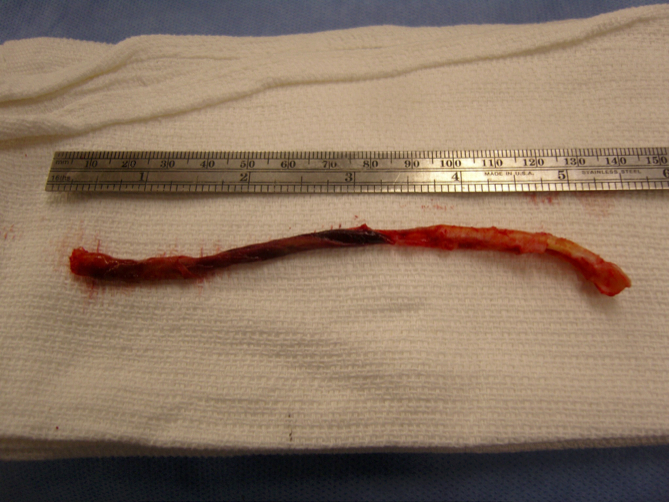
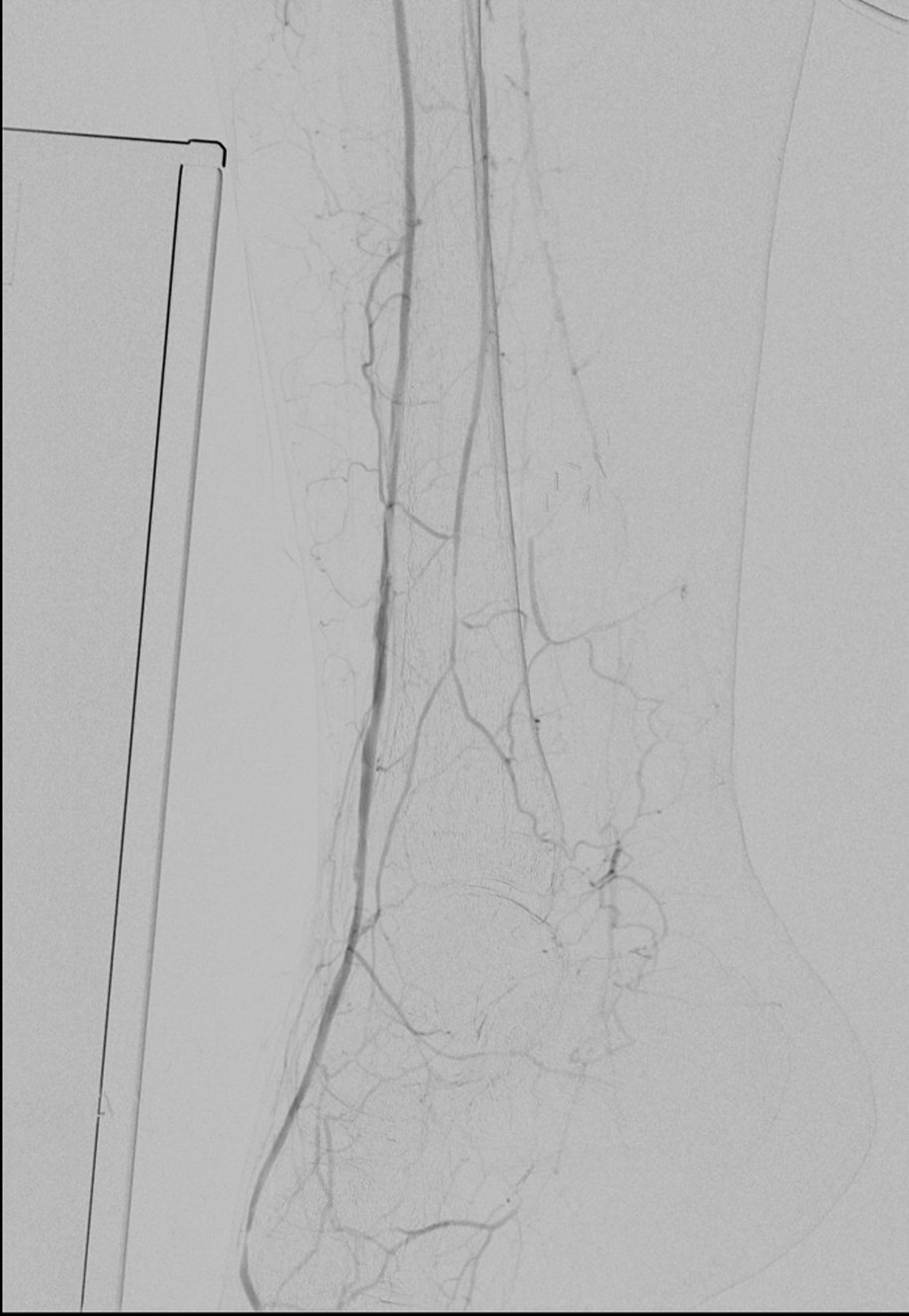
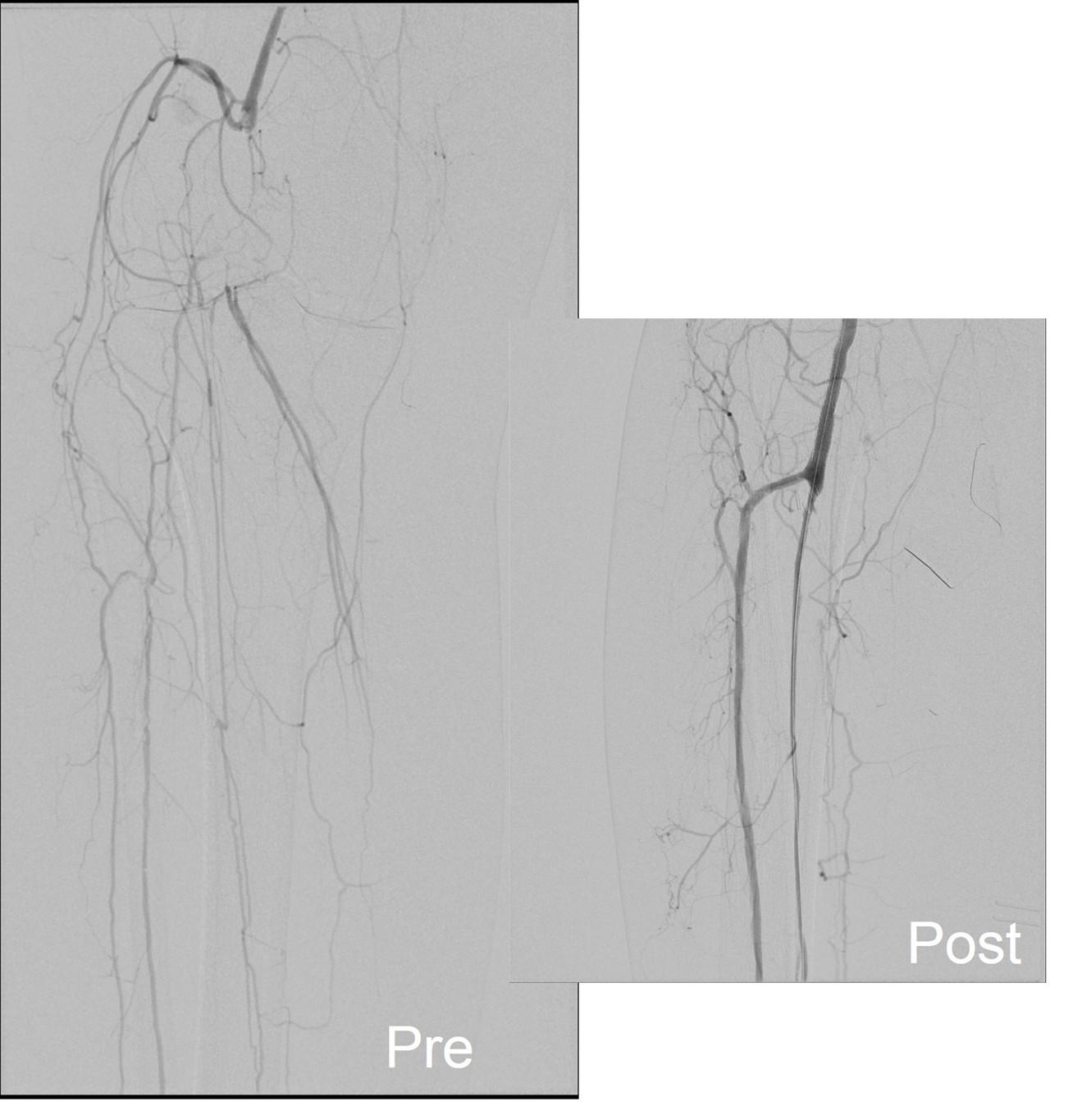
I contacted LeMaitre Vascular and got in touch with your representative, L. Fisher, who promptly sent the Moll Ring Cutters I needed to perform a remote endarterectomy of the patient’s occlusive external iliac and superficial femoral artery plaque. The technical details of remote endarterectomy are have been covered in my blog (https://vascsurg.me/?s=endore), but in the end, through a 7cm incision in the groin (don’t believe the hype, this is minimally invasive), I restored his arteries to their original open condition. Shown below are the results. It was with great sadness that I heard that the LeMaitre Vascular equipment being sent were the last of the stock available in North America. The patient did very well, with the operation completed well before lunch, and is recovering rapidly from his small wound and big rescue. He gets to walk out of the hospital on two legs, but also with the surety that he avoided a major bypass operation, and avoided the short term gains of stenting from the aorta to the profunda -more peel packs and landfill items and a dubious long term durability. Hey, I even used a XenoSure patch on the common femoral.



Endarterectomy is foundational to vascular surgery going back to the work of Professors J. Cid Dos Santos and E. Jack Wiley. Through Dr. Kenneth J. Cherry, who trained under Dr. Wiley, and who trained me, I can claim two degrees of separation from the originator of endarterectomy, and this drives my passion for preserving this critical tool in our vascular kit. The basic tools, the endarterectomy rings, are as old as vascular surgery itself. To lose a critical supplier, particularly in a time when the pendulum to open surgery is swinging back, when the best results come from combining traditional surgery and cutting edge endovascular techniques in hybrid procedures such as EndoRE, when the coming healthcare cost-apocalypse will cause everyone to question the value of thousand dollars-plus items dropped from peel packs, is devastating.
I get it that the aSpire stent never panned out, and that disposable dissector/cutters never moved that well, and that you run a business, not a charity. But I do believe that best companies reflect the best values of their people, such as the prompt action and followup of your rep L. Fisher who by getting us the rare supplies, helped in achieving this patient’s excellent results. While I believe there is a business case to be made in preserving and relaunching EndoRE, as endarterectomy has proved to be future proof for nearly a century, I believe more strongly that it is the right thing to do.
Sincerely
W. Michael Park