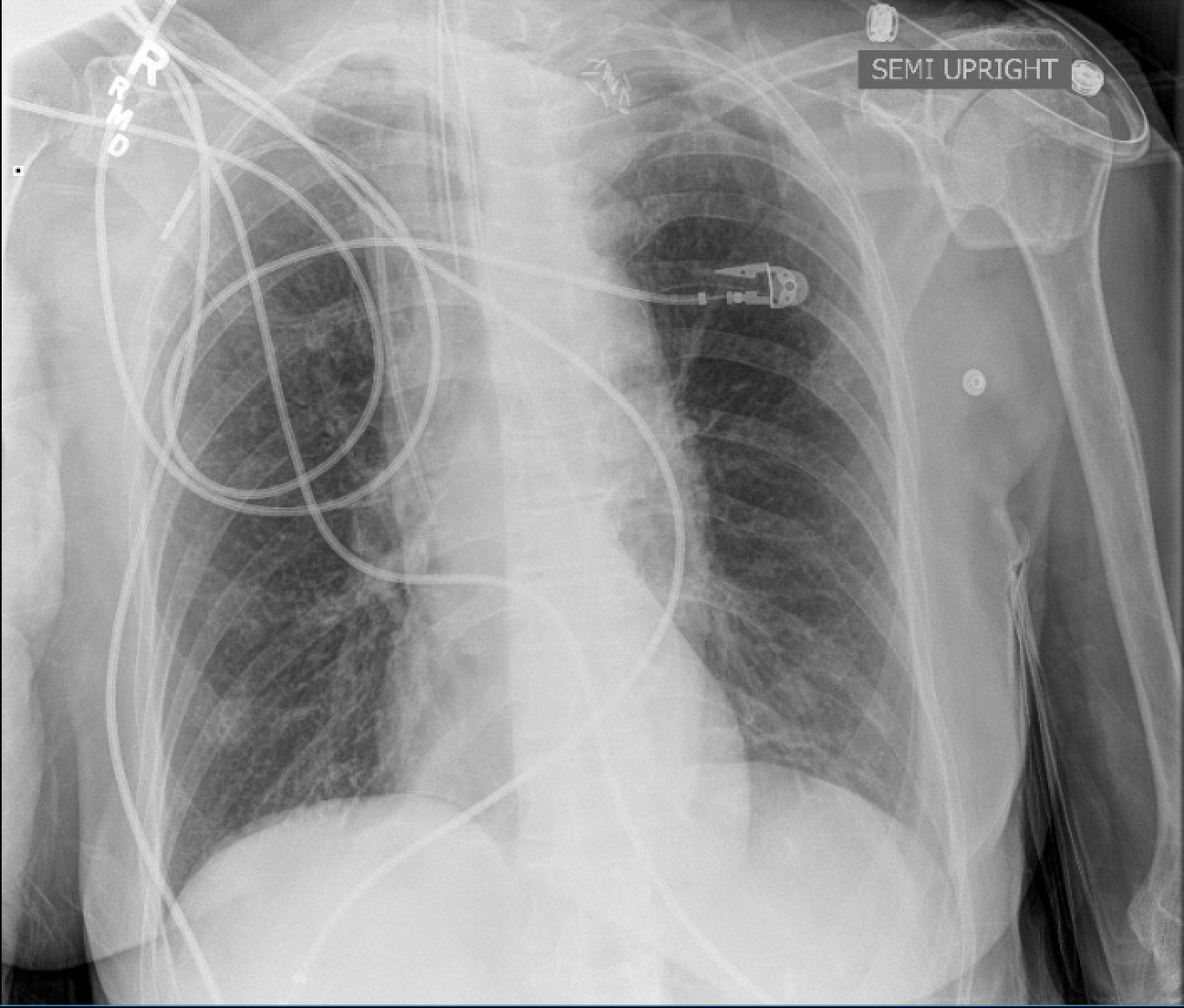
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
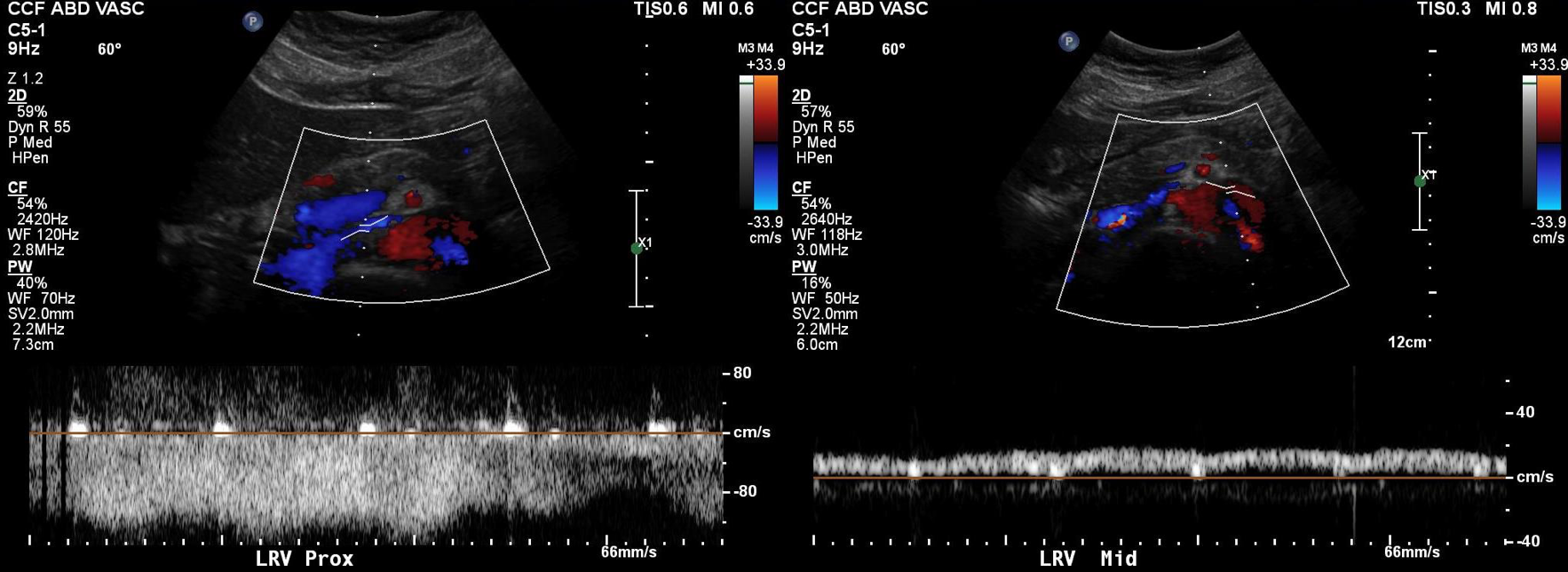
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
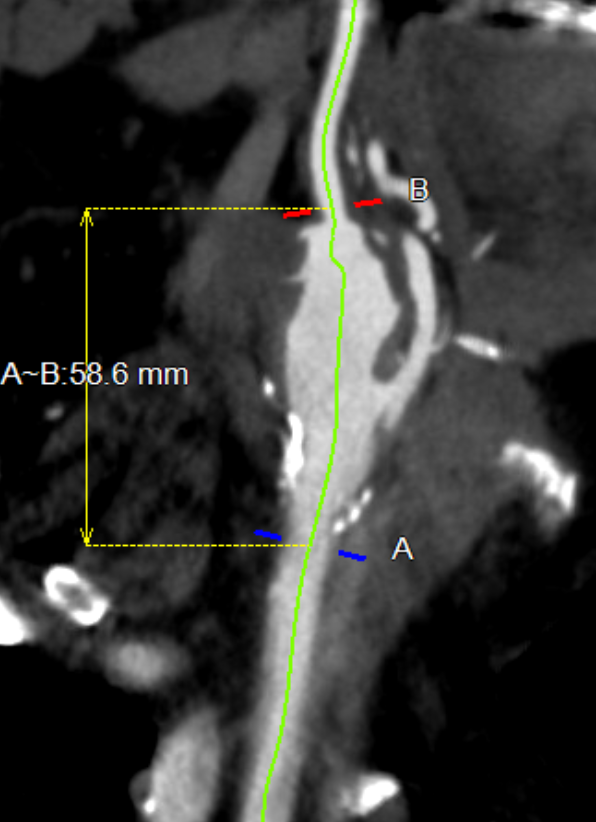
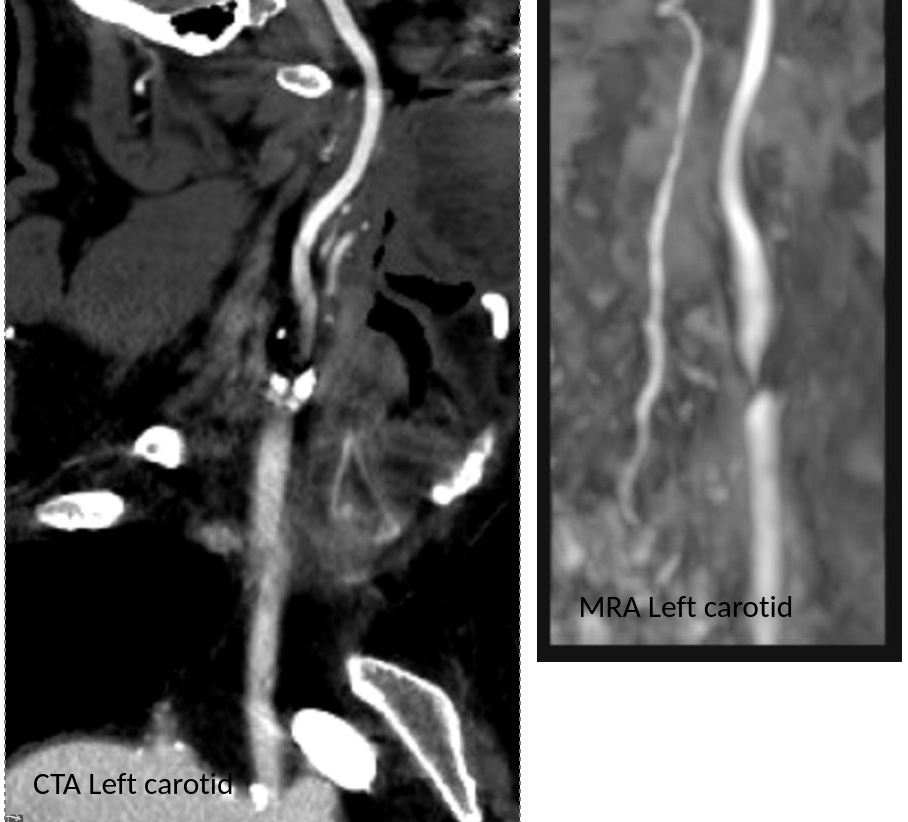
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
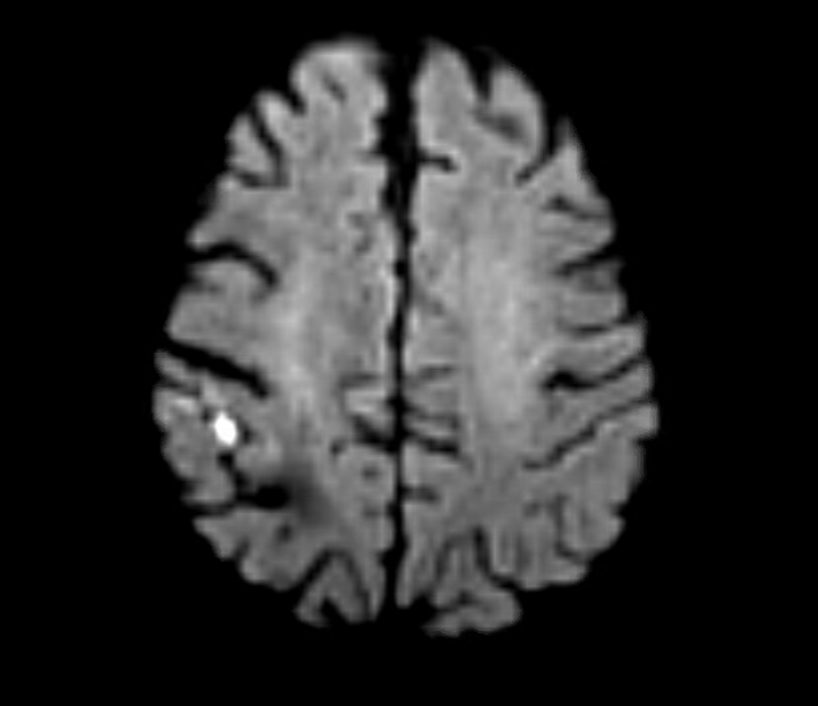
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
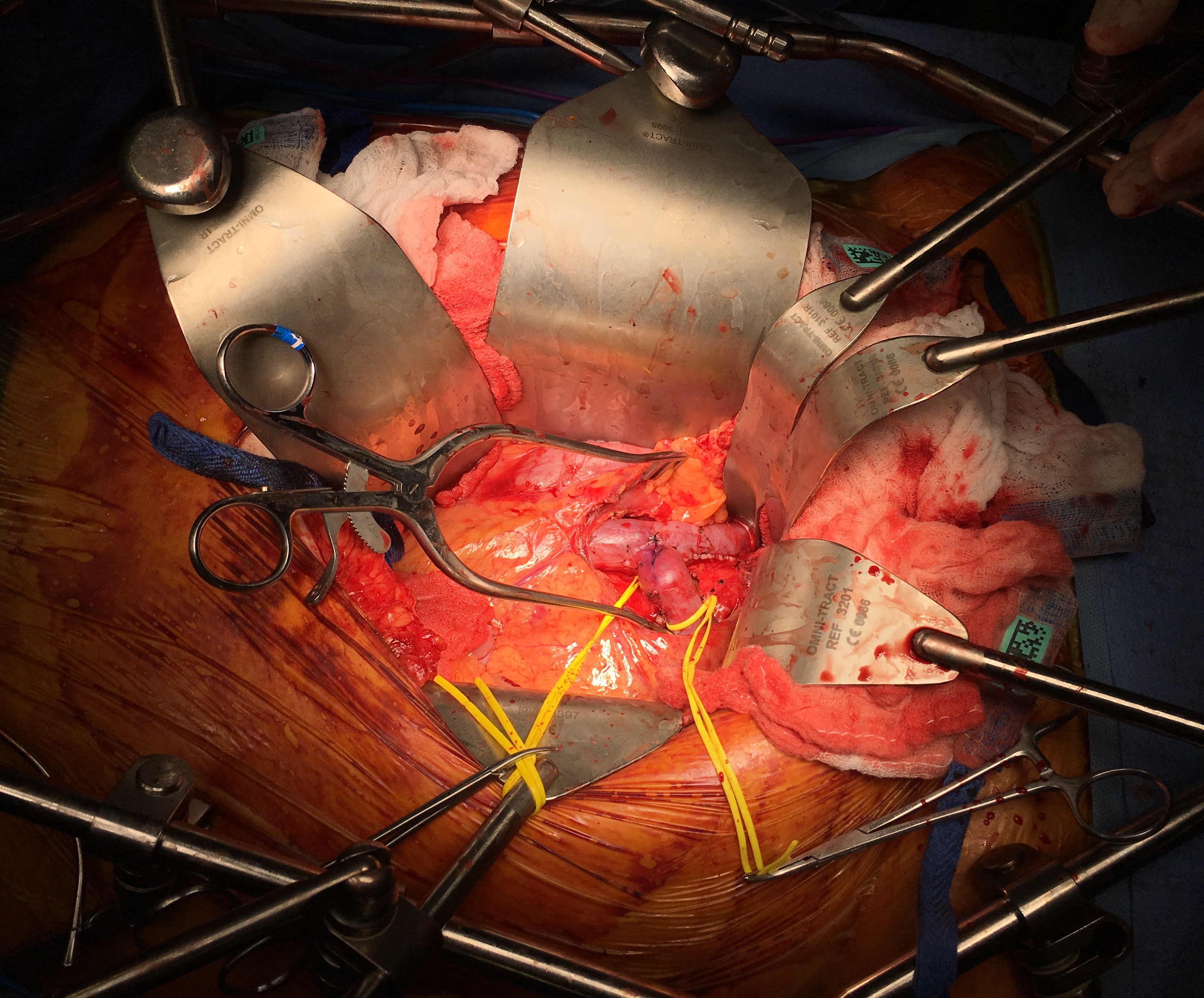
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
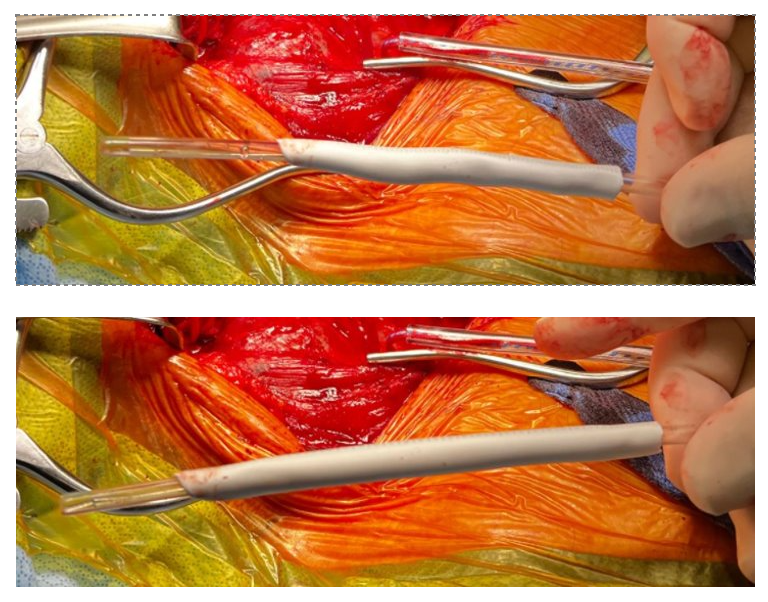
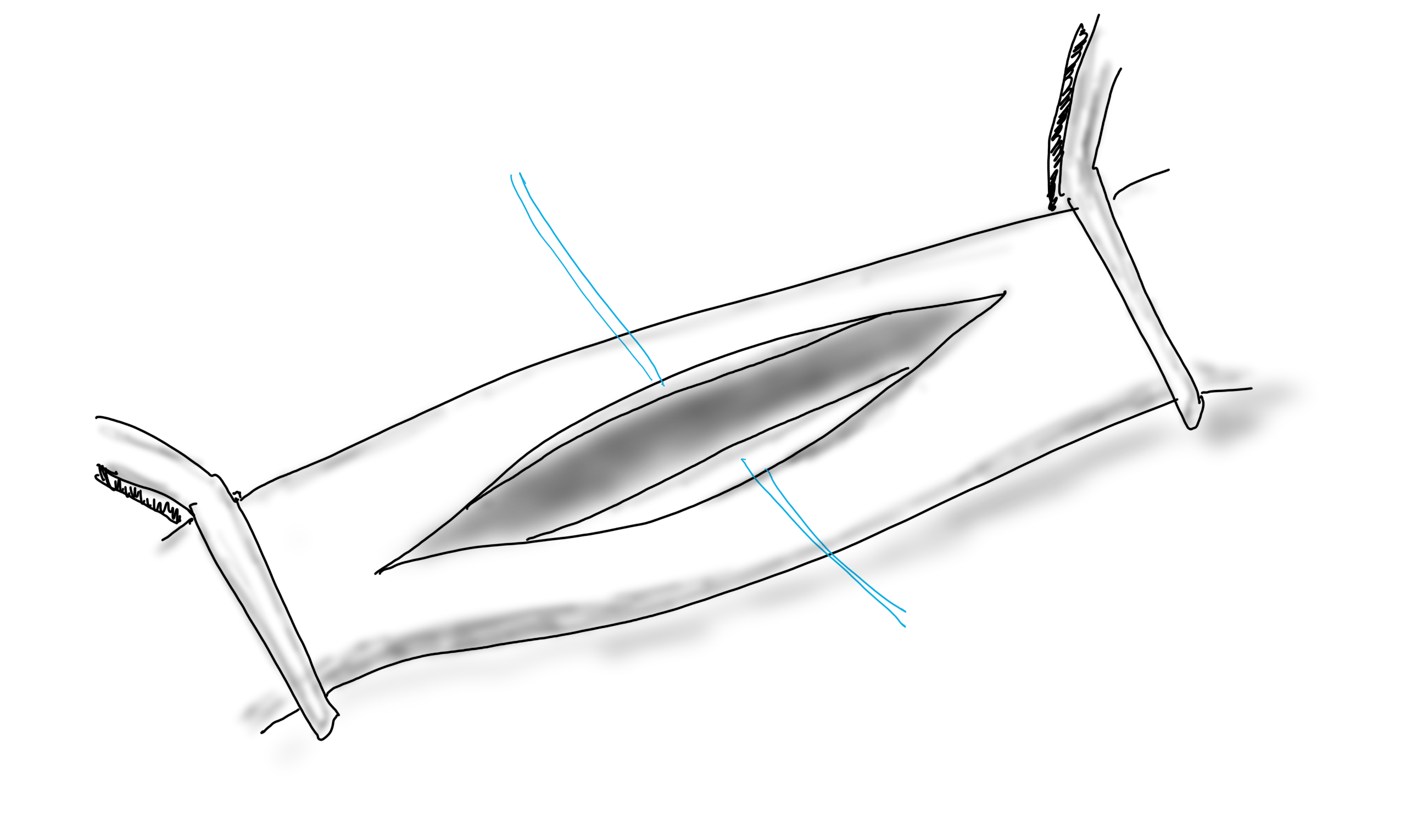
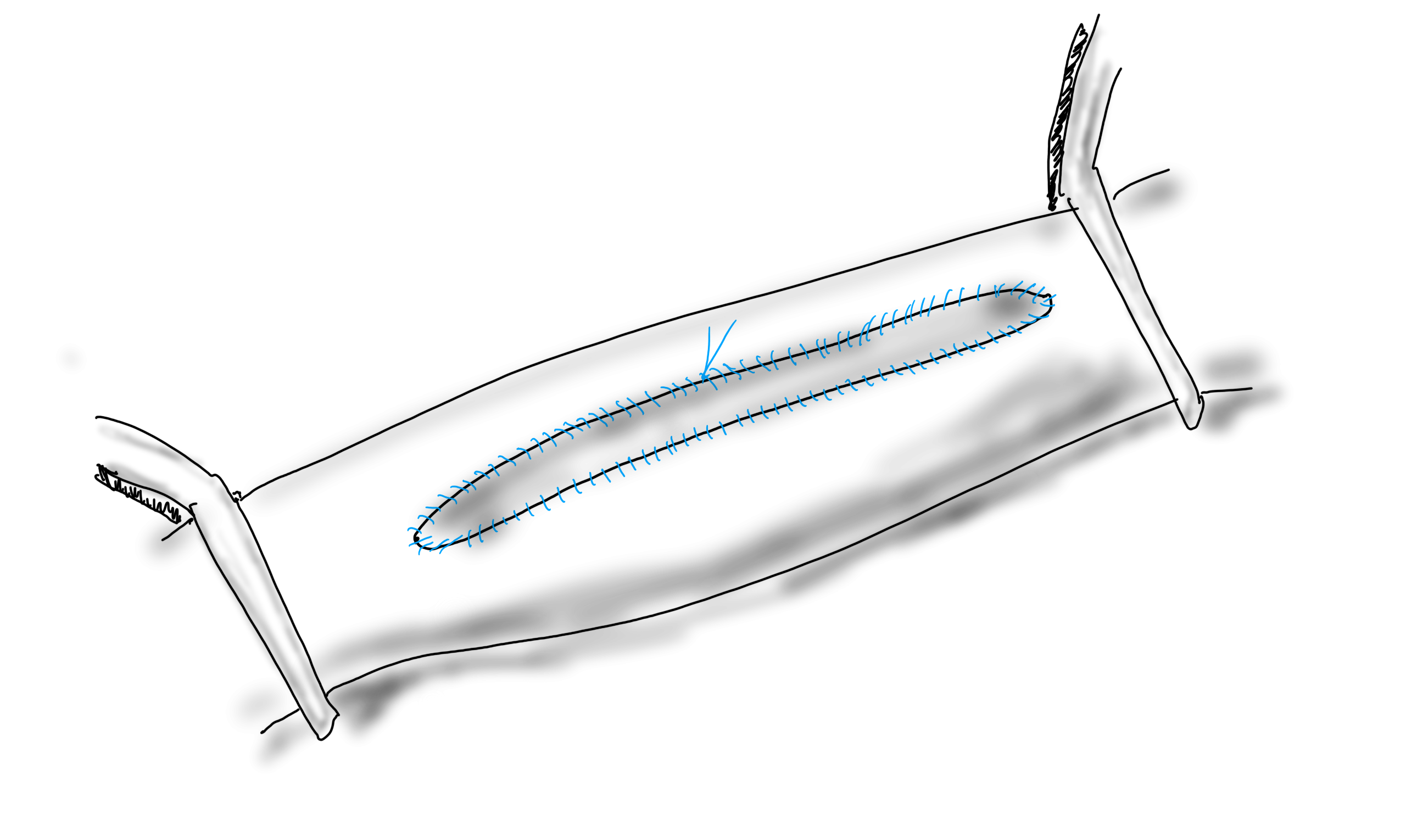
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
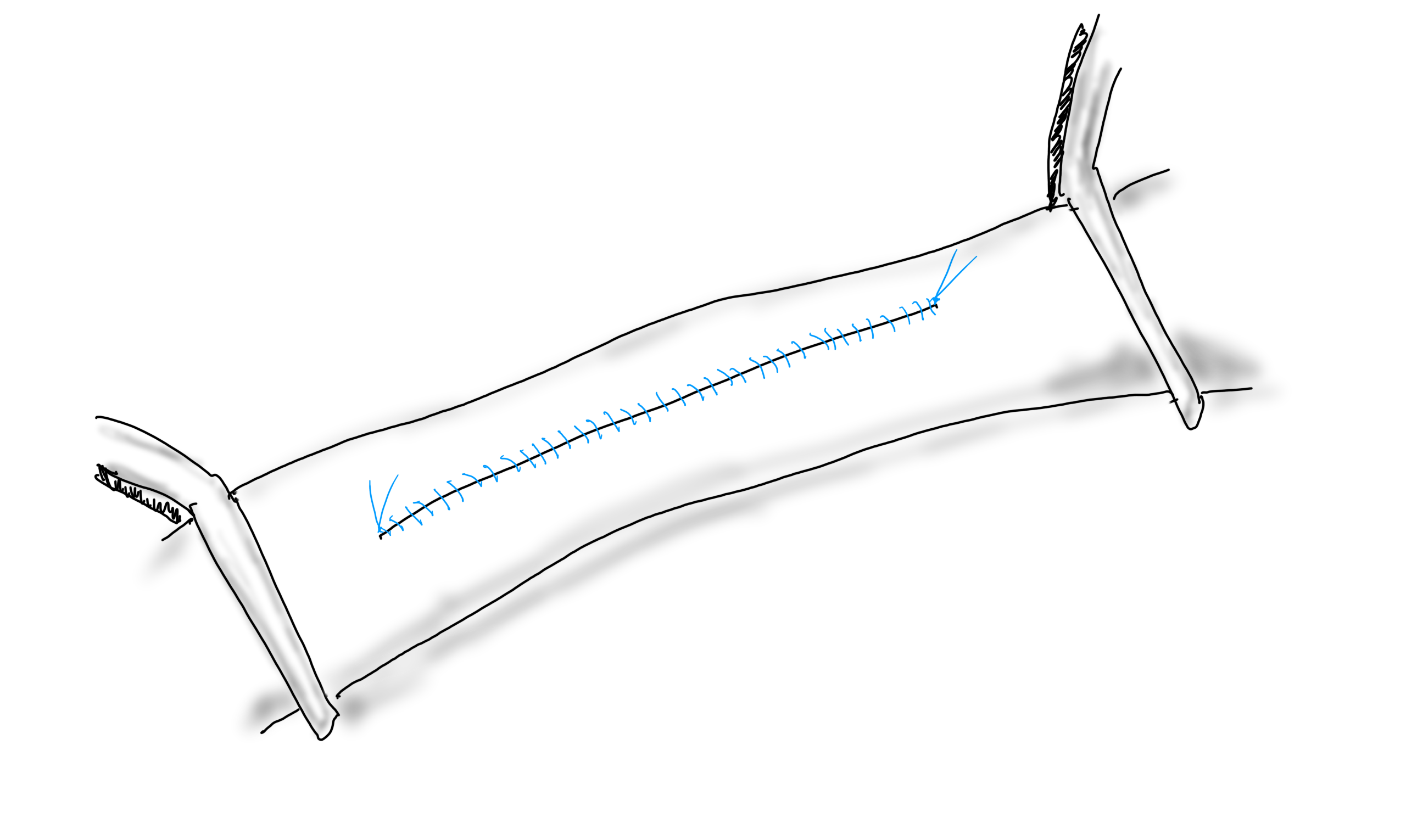
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
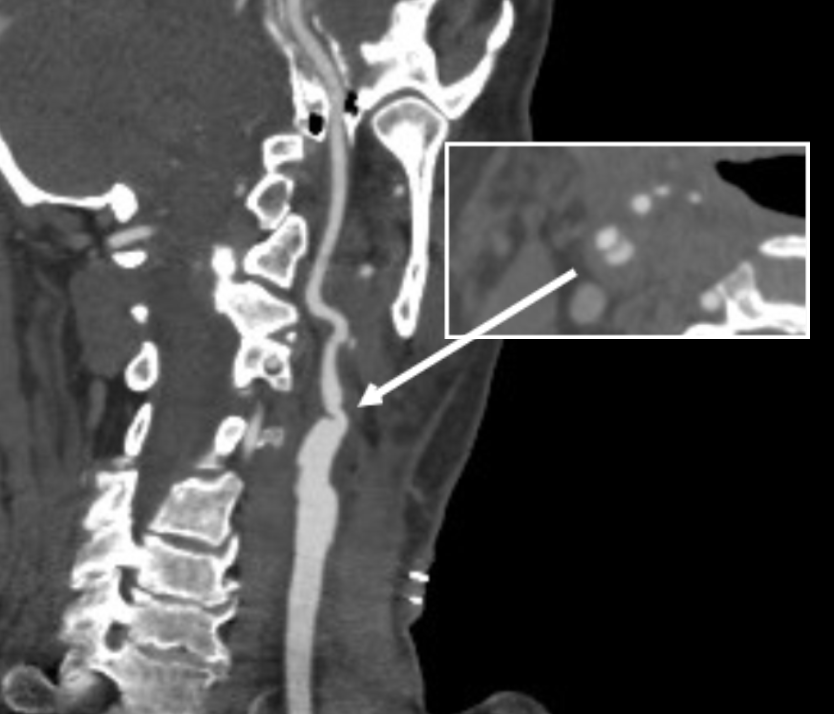
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
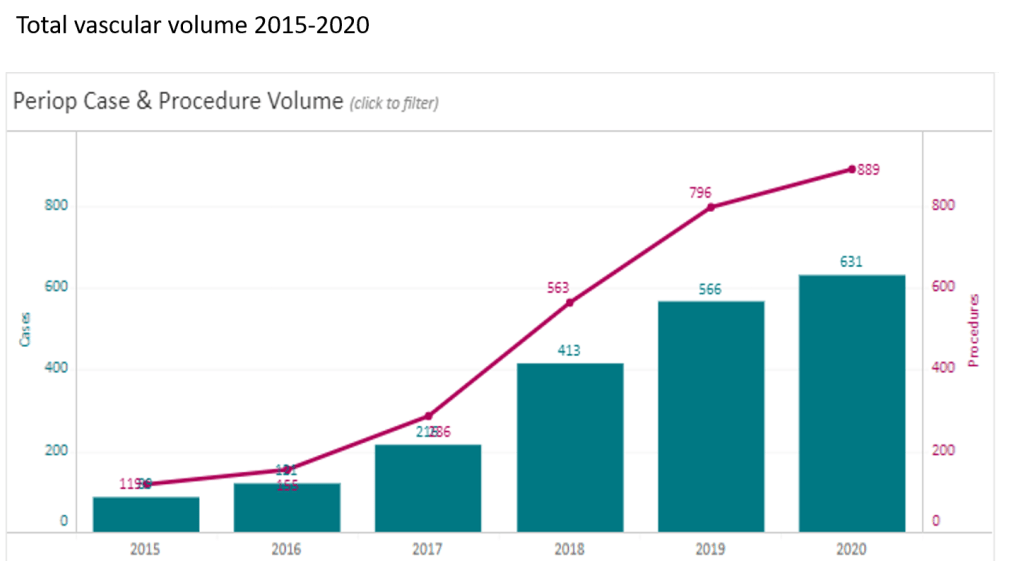
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
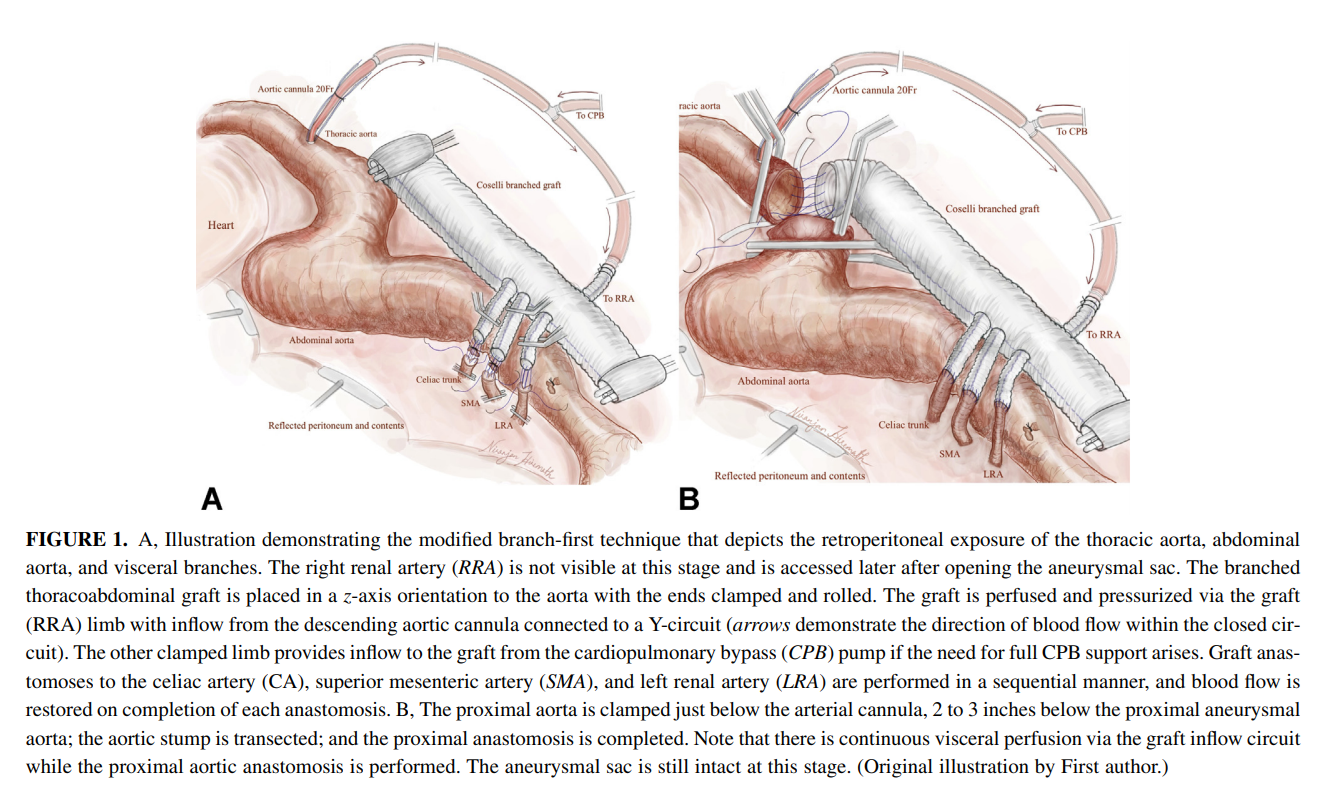
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
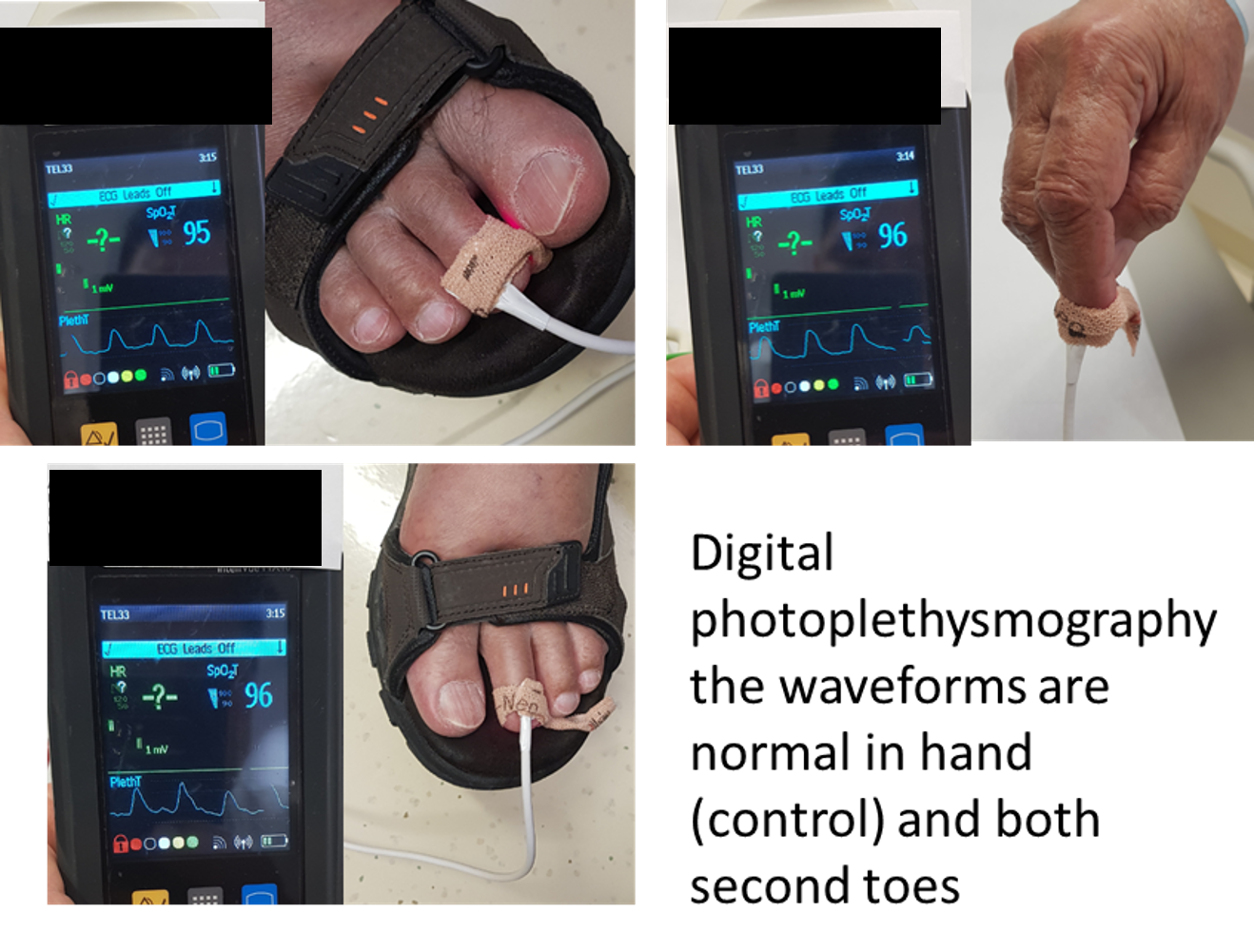
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.
This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).
an abnormal DPPG captured with a hospital ICU pulse oximeter
We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).
At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).
The distal perfusion cannula is in the dorsalis pedis artery
This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery
The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).
Pulmonary artery staple line bleeding controlled, ready for suturing.
In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.
A long time ago, there was the IVC clip which survives today as a vestigial CPT code. Then in the 1980’s, the Greenfield filter was introduced and changed the management of thromboembolism (reference). The explosive adoption of endovascular technology in the late nineties and early 2000’s drove the growth in implantation of newer generations of IVC filters that were designed to be retrievable. The people requesting the filters -the physicians, surgeons, and even patients looking to stop taking anticoagulation, were basing their decision on common sense –“sometimes, people are vulnerable to pulmonary embolism and are at risk of hemorrhage with anticoagulation, so an IVC filter makes sense.” There was frankly a data gap -a breach into which multiple companies jumped in with their own flavor of filter. Many interventionists saw no need to be selective -these were easy to place, and easy to remove, and if they stayed in there was the excellent long term results of the Greenfield filter to cite, and their referring docs asked for it. There was also the high revenue density (revenue/time) that gave filters a gravitational pull. There were several problems with this endo-enthusiasm (like in so many other cases). In the absence of data and with the aggressive marketing, too many filters went in for weak indications. We now know that most of these filters do not behave like the Greenfield, which itself is not completely innocent. Unless followup is part of a process, many patients neglected to have their filters removed. And finally, the data caught up and failed several filters which are no longer on the market and the indication for these filters is now quite narrow.
In 2009, I was asked to consult on a young man who was hospitalized for upper GI bleeding. The EGD revealed the tines of an IVC filter poking through (the jpg is somewhere I swear). The prior year, he had been in a bad car accident and had a filter placed but never had it removed. The filter had migrated out of the IVC into the duodenum and into the spine and aorta. I removed it operatively, and that was the beginning of a series of cases, about 1-2 annually in my general vascular practice, of filters that had eroded through the IVC and was causing symptoms of bleeding or pain. The pain typically was associated with a tine touching on or eroding into the spine. Biomechanically, the IVC is a collapsible tube and all the viscera on top of it weighs about as much as an equivalent sack of uncooked chitterlings when recumbent and grinds on the filter and any sharp parts. Imagine unbending a paperclip (figure) and putting it in the belly. Over time, that clip will poke a hole in something. Why would we not expect an IVC filter to behave otherwise?
An Iliocaval Thrombosis Below a TrapEase Filter
The patient is a younger man who over a decade ago had a TrapEase permanent IVC filter placed when he had a pulmonary embolism while having multiorgan failure. He was on coumadin briefly, but in the 17 years since filter placement, never had another venous thromboembolic event, but did develop venous insufficiency and varicose veins that were successfully treated. Several days prior to admission, he had been working out and developed back pain. After trying to sleep it off, he woke with severely swollen and painful legs. On admission, he was found to have no lower extremity DVTs, but had slow flow suggesting central occlusion. An abdominal x-ray showed the TrapEase filter (image below).
CT scanning and MRV showed the occlusion of the patient’s iliac veins and erosion of the struts of the filter outside the IVC (axial images below).
On heparin infusion and bedrest, his swelling improved and we had a chance to go over our treatment options. They included
Catheter directed thrombolysis
Angiojet thrombectomy
Large sheath thrombectomy (link)
–with one of the following–
Surgical resection of filter
Endovascular retrieval of filter
Balloon venoplasty and stent exclusion of the filter (link)
Catheter directed thrombolysis of such a large volume of clot in the absence of a good flow channel usually necessitates multiple days of thrombolysis with return for venography and adjustment, with a small but not zero chance of fatal or disabling hemorrhage. It is expensive -multiple ICU days, return trips to the OR angiosuite. Angiojet thrombectomy is useful for clearing smaller vessels and grafts but due to the pulsing of the jet, it has a good chance at creating pulmonary emboli if the filter’s occlusion is not complete. Plus it is expensive and limited by the volume of fluid necessary to create the suction. Large sheath thrombectomy has worked for me in the past (link), but I worry about leaving behind thrombus that would embolize when the filter is removed or pushed aside.
Endovascular removal of the filter is always an option -I have removed a Greenfield filter over two decades in. I have never been able to remove an OptEase or TrapEase filter -there is nothing easy about these. I have a picture somewhere sent to me by a trainee who was consulted on a patient whose IVC was transected during the attempt to remove one of these endovascularly. That said, both my partners Houssam Younes here in Cleveland Clinic Abu Dhabi and Christopher Smolock at Cleveland Clinic Main Campus suggested trying with a two-team approach with a 16F sheath and wire from above and a 12F sheath and wire from below. That would be contingent on being able to clear the thrombus adequately.
Surgery to remove the filter is something I am comfortable with. It sometimes is the only option (link). Several times a year, I scrub in with urologists and oncologic surgeons to remove tumor from the retroperitoneum or IVC and the exposure is straightforward. When I only need control of the IVC, I make a transverse incision slightly above the umbilicus and mobilize the retroperitoneum leaving the kidney down to expose the IVC. For the IVC and iliacs, a midline laparotomy with a Cattell maneuver allows for broad control. Surgical thrombectomy would be great if the thrombus was all fresh, but challenging if there were differing amounts of fresh and chronic occlusion. The CT scan, showing the iliac veins and IVC to be swole with clot, suggesting most of it was fresh. Neither CT nor MRV could tell me if the IVC below the renal confluence was occluded. I had to be certain.
I went over these issues in detail with the patient and we agreed to proceed with diagnostic venography to check out the clot. The verbiage of clot, tofu, and cheese (link) worked well in communicating the information needed to achieve our goal of getting the filter out and the IVC and iliac veins cleared of thrombus. I sent a hypercoagulability study (even on heparin, the genetic component is useful information) which returned negative.
The diagnostic venogram is much more than just the pictures. For me, so much information is transmitted from the tip of a Glidewire as it passes through an obstruction or clot. Venography (image below) showed the thrombus but more importantly, the wire passed effortlessly in either side, got caught up in the bottom of the filter, but I was able to get through and the 5cm of IVC below the renal confluence turned out to be patent. The wire looped easily on both sides to the full extant of the dilated vein suggesting no chronic component.
I recommended surgery in our hybrid angiography suite. It would avoid multiple days of thrombolysis and its attendant risks. It would avoid subtotal clearance of thrombus. It would avoid failed filter retrieval and bailing out by stenting the filter (link), something acceptable in an older higher risk patient but not in an active young man. It would avoid surgery after several days of failed thrombolysis. The ability to perform venography and sonography with a clamp on the IVC ensured the ability to fully clear clot. And we had cell saver. After laying out my thoughts and concerns, the patient agreed.
The patient was opened via a generous midline laparotomy. I recruited the assistance of my friend Waleed Hassen, master urologic surgeon here at CCAD, in exposing the IVC. The vessel loop in the picture (below) is around the ureter. Green arrows on the right image show the anterior struts (there are three posterior struts). I had just assisted Waleed recently in removing a metastatic testicular tumor off the IVC, aorta, and mesenteric arteries through the same exposure.
The surprising finding was the anterior hooks of the TrapEase filter had penetrated the serosa of the overlying duodenum. While not perforating, it eventually would have, as the struts had eroded through the wall of the IVC and were outside the adventitial. After heparinizing the patient, the cava was clamped above the filter and I opened the cava lontitudinally along the anterior most strut. I got the sternal wirecutters and removed the anterior three struts along with their hooks. There were large draining lumbar veins which were acting as collaterals that were ligated. The filter was removed internally in pieces leaving the posterior three struts behind as they were outside the IVC lumen. The lower cone can be seen with tissue ingrowth and chronic thrombus. It was dangerous and bloody behind the IVC and I chose to leave these struts behind as they would no longer be pressing into the spine with the filter mostly out. (image below).
The initial thrombectomy was done manually by massaging the vein from either side and up the cava -the thrombus (image below) in the basin on the left expelled as a unit with a spout of blood. Thrombectomy with a #5 Fogarty proved ineffective in the large vessel, and I resorted to using a Foley catheter, directing it left and right, with removal of some more thrombus.
Duplex demonstrated clearance of thrombus from the right iliac vein but adherent thrombus on the left. I placed an 18F sheath into the left femoral vein over a wire I had directed up and over into the right iliac system and advanced the sheath while suctioning -this collapsed the vein and allowed the sheath to scrape the walls of the vein, retrieving the final clot material in the right basin. Duplex confirmed the absence of clot in the left iliac vein. The venotomy was then closed primarily and a completion venogram was performed (below).
The patient recovered and was sent home after a duplex confirmed patency of his leg and iliac veins and IVC. He will be on 3 months of a NOAC for provoked DVT.
Discussion:
Most of these filters can be retrieved with endovascular techniques. The principle is of gaining control of the top of the cone and collapsing it like an umbrella. For the Cordis TrapEase and OptEase filters, both cones have to be collapsed, and the struts which will have grown into the walls of the IVC have to be be stripped away from the IVC. I had attempted removal of an OptEase with control from above when I was in Ohio, but like in this case, the filter had tissue ingrowth on the lower cone making looping and control of the filter difficult as the hook was encased. While I was able to collapse the filter into a 16F sheath supported through an 18F sheath, it was clear the IVC was invaginating into the sheath and with enough force, I would tear the IVC. It is not the worst thing, perforating the IVC, as it is a low pressure system, and a small perforation is tolerated, but a large one needs operative repair. This can be avoided with surgical removal of the filter.
Performing this in the hybrid suite allowed for complete clearance of thrombus. That said, the thrombus in the internal iliac veins likely did not come out, nor did I seek to clear them. Rather, I will rely on systemic anticoagulation to do this for me.
I use duplex sonography intraoperatively liberally during my procedures. During EVAR, transabdominal ultrasound is sufficient in ruling out or specifying endoleaks. During complex kidney transplantation which I sometimes participate in, duplex is a critical tool for evaluating flow. In this case, images showing a cleared vein (will post, currently stuck in portable ultrasound memory) assured me that I could open the clamps with confidence that pulmonary embolism could be avoided. Gratifyingly, the patient had immediate reduction of leg swelling and can be expected to avoid problems as nothing (such as stents) was left behind in the vena cava lumen.
The rise of cardiopulmonary bypass life support has also given a rise to the need to keep large, obstructive cannulas in femoral arteries. ECMO cannulas are often kept in for days, and it is not uncommon to discover limb ischemia and infarction relatively late. This can be avoided by placing a distal perfusion cannula to shunt blood to the leg early in the ECMO process. The ECMO cannulas have a convenient side port to send a little flow to a 6F sheath placed in the femoral or popliteal artery. This is an established technique (reference 1, sketch below), and it works despite the modest flows achieved because it does not take much to keep the leg alive. These patients are not walking, nor are they need to heal leg wounds, so just enough blood flow means something just a little more than what they get when the common femoral artery is completely occluded by the life support cannulas. What is fascinating to me is that these shunts can pptentially help to save limbs when used as temporary extracorporeal bypasses when definitive vascular surgical care is not immediately available.
When I was a medical student, I took on a research project after my first year where I had a Langendorff preparation of a rat heart (below).
an isolated, perfused, beating rat heart placed in a superconducting magnet for NMR spectra acquisition
My project was to take a rat heart and keep it alive, beating, and even working, through a perfusion apparatus and place this inside a superconductive magnet to obtain Phosphorus nuclear magnetic resonance spectra -intracellular metabolism data including concentration of ATP, intracellular pH, and ATP/ADP ratio. While the project was successful -I am quite proud to have been the only person at Columbia to have successfully acquired NMR-S data with living beating heart, I moved on to other interests and took away this concept: with oxygenated, glucose enriched, isoosmolar fluid perfused at arterial pressure, any organ can be kept alive, possibly indefinitely, including a brain which only recently others have found possible (reference 2) in reputable scientific circles, but the the Nature publishing Yalies were scooped by the Simpsons decades ago (below), and maybe Mary Shelley centuries before,
This is the simple idea. Revascularization is keeping the target vascular bed alive by delivering oxygenated blood. With a shunt, it could be little, it could be a lot, but it certainly is better than zero, and even a little can buy you time.
The breakthrough that I had was several years ago, a patient arrived from another hospital with an Impella pump which did not have a side port like an ECMO cannula. It is a large catheter that augments cardiac output and in the patient that I was asked to see this patient as their leg was cold and pulseless. Their cardiac output was very poor, and they were sustaining an augmented systolic pressure in the 90’s. There was no way to get this patient to the operating room for a revascularization of any sort. It did strike me that the patient had the misfortune of having catastrophic heart failure in the absence of significant athersclerosis and had normal brachial arteries. After discussing the ramifications with the ICU and family, I placed a brachial artery 5F cannula, and connected it to a 5F sheath I placed in the superficial femoral artery below the occlusive common femoral sheath (figure below). A doppler on the tubing connecting the two cannulas confirmed flow and the patient’s left hand maintained a pulsatile oximetry waveform. The leg pinked up and eventually there was a signal in the foot. This managed to perfuse the leg which did better than the patient who succumbed to multiorgan failure from heart failure. The leg did great.
Which leads me to these thoughts. Most hospitals are good at diagnosing large vessel occlusion via CTA. Most hospitals have doctors who can place arterial lines with ultrasound guidance. In the instance of aortoiliac occlusion or femoral occlusion from thromboemboliem, time is a critical limiting factor to limb salvage. Many hospitals do not have vascular surgeons. Many hospitals transfer these patients with a heparin drip but in the ischemic condition. Transfer arrangements may take hours. Why not ameliorate this situation by having an appropriate physician -an anesthesiologist, an intensivist, an EM physician, place an ultrasound guided radial or brachial arterial line, connect to arterial line tubing to a dorsalis pedis arterial line. Tape it all down on the patient after confirming flow (crude sketch below). This would be better than the three extra hours of ischemia the patient gets hit with on transfer. No one would transport a donor kidney without adequate perfusion and protection, but dying legs get transferred all the time with established warm ischemia. If done well, it might turn an emergency procedure into an urgent, semi-elective one. Have the vascular surgeon video conference in to confirm the absence of blood flow and appropriateness of temporary shunting.
radial artery to dorsalis pedis artery shunt
If we are to live in a world with less vascular surgeons, then the radius of survival has to be extended with use of technology and simple ideas such as this. Comments are welcome.
Reference
1. Foltan M, Philipp A, Göbölös L, Holzamer A,
Schneckenpointner R, Lehle K, Kornilov I, Schmid C, Lunz D. Quantitative assessment of peripheral limb perfusion using a modified distal arterial cannula in venoarterial ECMO settings. Perfusion. 2019 Mar 13:267659118816934. doi: 10.1177/0267659118816934.
2. Vrselja, Z., Daniele, S. G., Silbereis, J., Talpo, F., Morozov, Y. M., Sousa, A. M. Mario, S., Mihovil, P., Navjot, K., Zhuan, Z. W., Liu, Z., Alkawadri, R., Sinusas, A. J., Latham, S.R., Waxman, S. G., & Sestan, N. (2019). Restoration of brain circulation and cellular functions hours post-mortem. Nature, 568(7752), 336–343.
The patient is a man over 70 years of age who came to the hospital with severe pain of his right foot and leg with walking short distances and at night while recumbent. He had a history of hypertension, diabetes, and coronary artery disease, and several years ago had his left common iliac artery stented. On examination, he had no lesions of his foot, and his pulses were only palpable (barely) in the femoral arteries only. He did have strong monophasic signals in the anterior tibial arteries bilaterally.
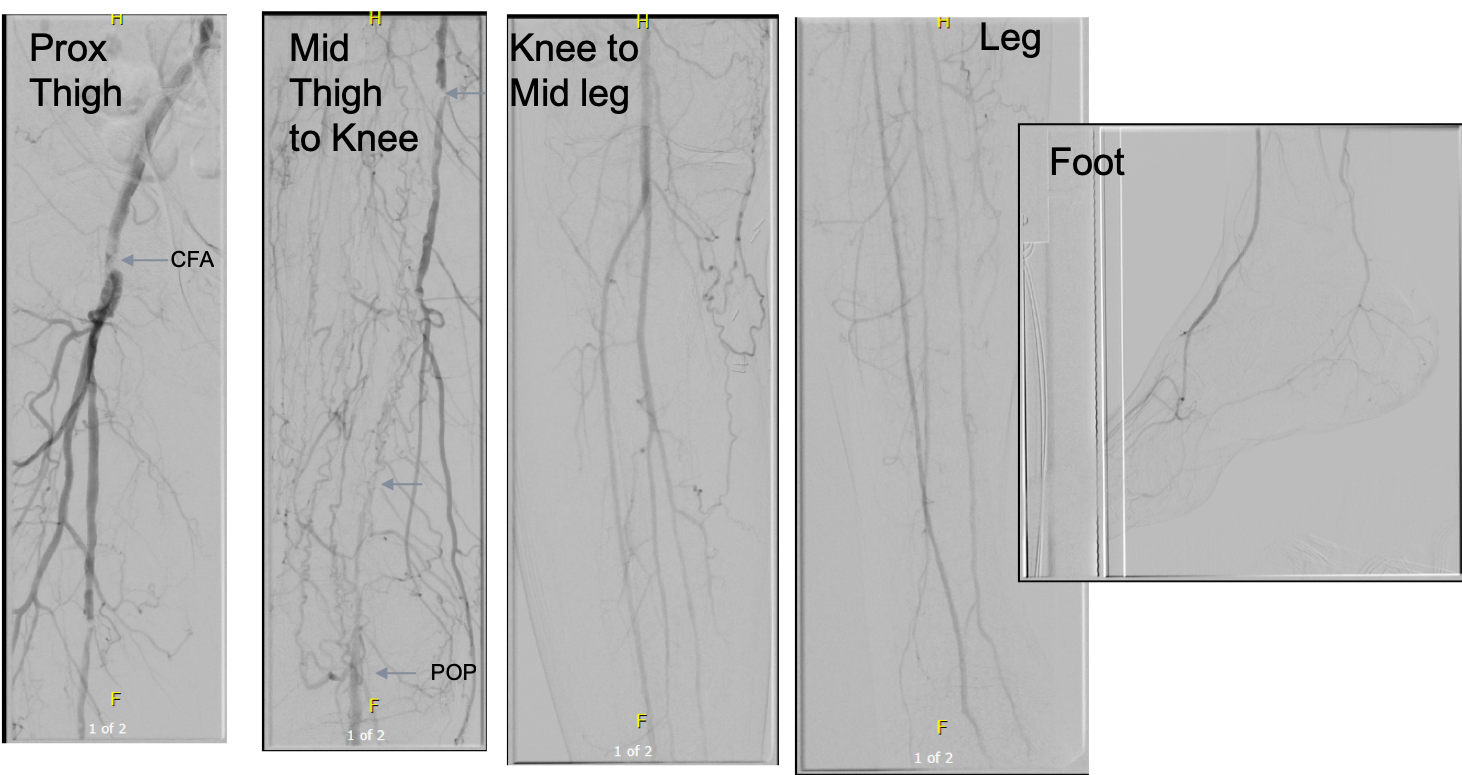
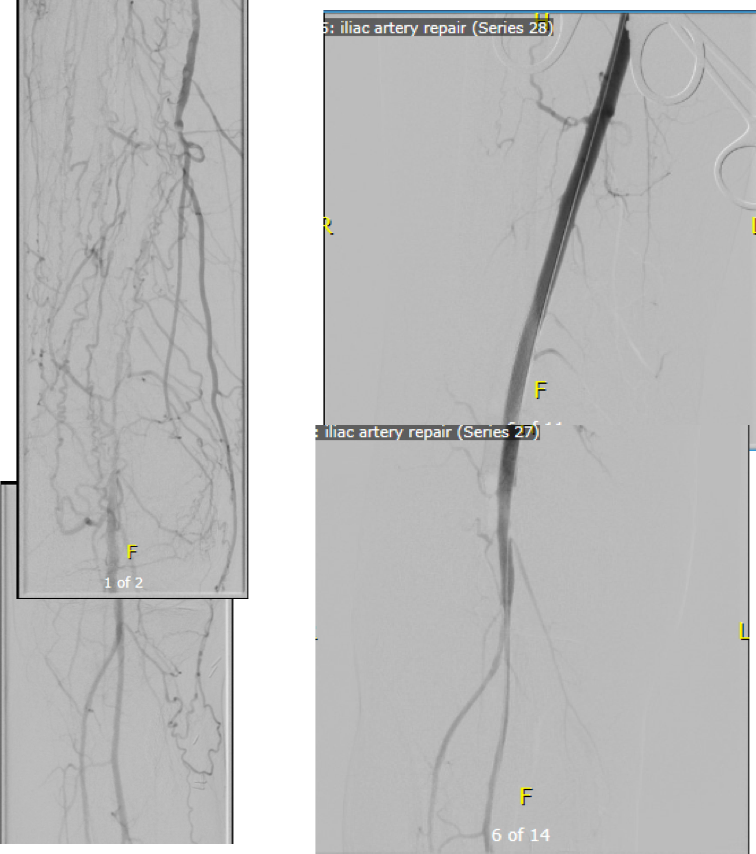
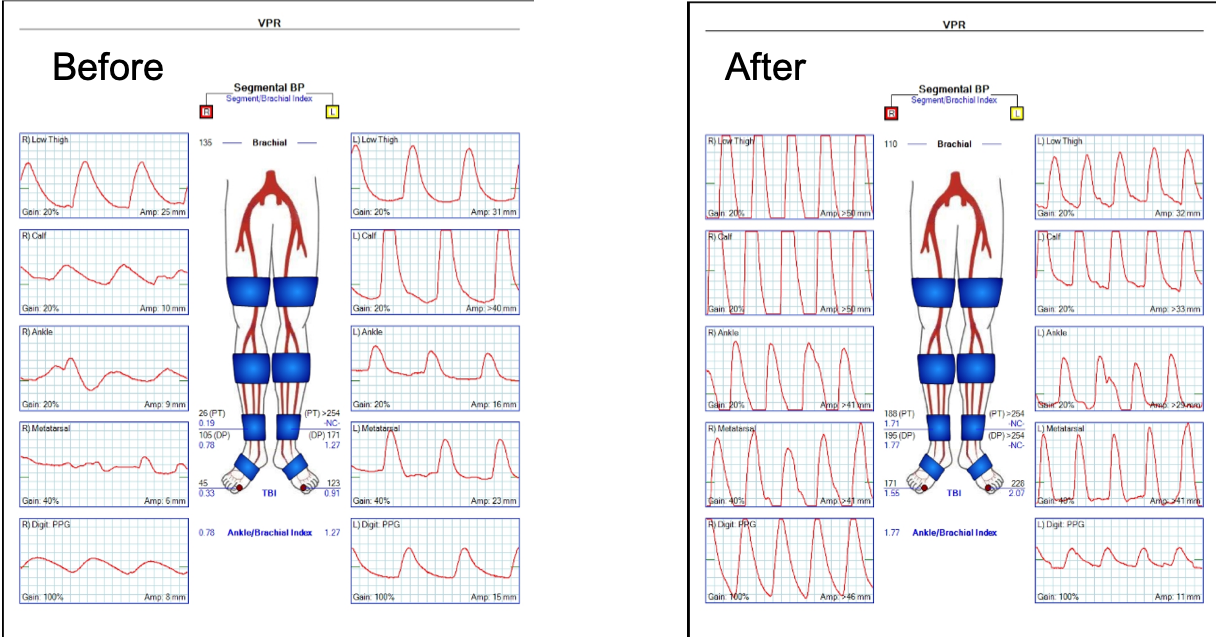
Initial vascular lab testing showed only mildly depressed ankle brachial (above), with dampened waveforms consistent with inflow and femoropopliteal disease on the right. He underwent arteriography by our vascular medicine specialist and cardiologist Dr. Faisal Hasan, and it showed bilateral common iliac stenoses, a severely calcified and nearly occlusive plaque in the right common femoral artery, and a long segment occlusion in the superficial femoral artery with diffuse calcified plaque extending into the popliteal artery. There was diseased but patent 3 vessel tibial runoff.
To Act As A Unit are the Cleveland Clinic’s words and it shows the Clinic’s roots as an US Army field hospital on the vasty fields of World War I France a little over a century ago, and we take it seriously. It may come as a surprise to some that a cardiologist referred me this patient after mutually deciding that the common femoral disease and the TASC D SFA occlusive disease, but we both decided that a surgical approach was the best one. The question then is how much more flow?
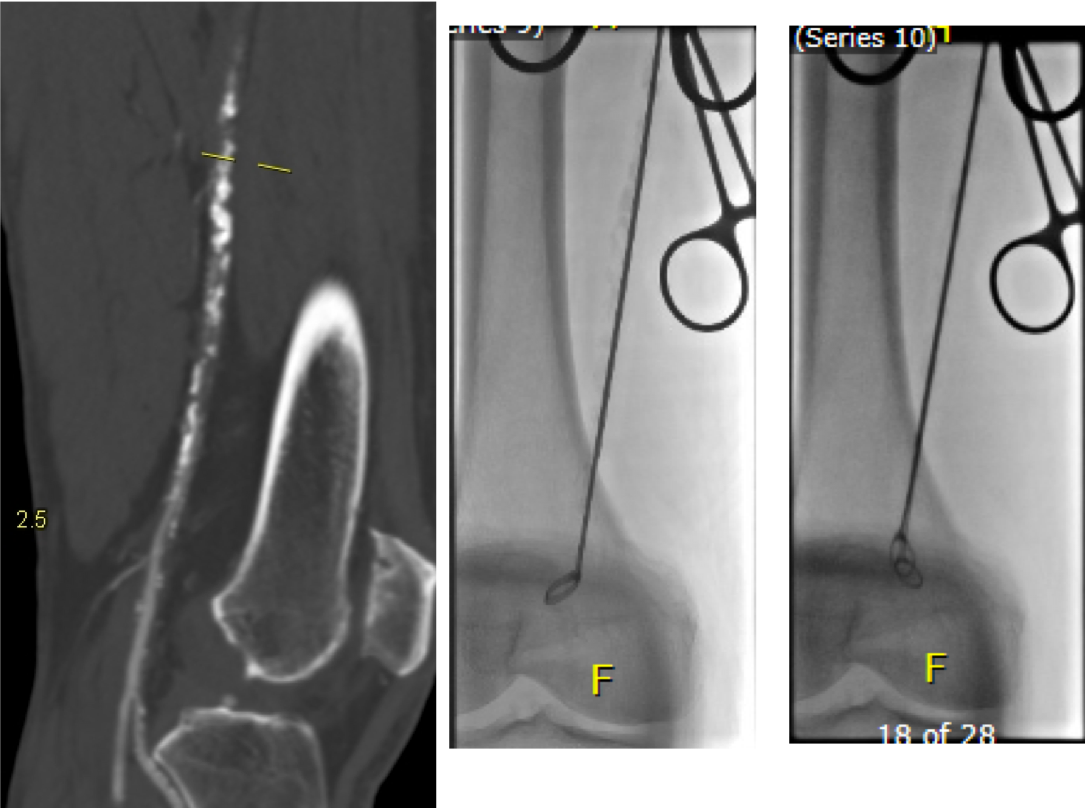
I ordered a CTA (CT angiogram) particularly for endarterectomies as I find it imperative to know the actual end point of plaque. Arteriography only hints at it, and while a 5mm lumen may look large and patent, it may be a channel in a 10mm wide plaque that when a stent terminates within it, breaks and becomes biologically active as intimal hyperplasia at best or embolizes at worst. CTA shown below revealed the plaque where contrast angio showed only the lumena of the vessels.
The 3D reconstruction function also allowed me to see and plan the operative approach and predict the lack of saphenous vein confirmed on duplex ultrasound.
For the students reading this, ischemic rest pain is often simpler to treat because it requires only a little more blood flow. There is a neurologic ischemia component that is not well studied, particularly in diabetics, as ischemia may result in anesthesia in someone who has underlying diabetic neuropathy, but that is not an indication for revascularization while rest pain is, and someone should investigate this. This little more blood flow in the form of treating inflow disease only may be sufficient in relieving rest pain while avoiding interventions on the superficial femoral, popliteal and tibial arteries which have limited longevity.
The common femoral artery on the other hand is the throttle of inflow and as a principle, inflow can be considered as the infrarenal aorta to profunda femoral artery, and repairing the common femoral necessitates an operation. There is no durable or laudable endovascular procedure for occlusive disease of the common femoral artery, a feature shared with the subclavian artery at the thoracic outlet and the celiac axis at the median arcuate ligament. All three are externally compressed by hard structures and revascularization must be ever mindful of the inguinal ligament, the thoracic outlet, and median arcuate ligament. The only exception to the “you must operate” rule of the CFA is calcified atherosclerotic disease in high risk individuals, and I make careful exception here with rotational atherectomy devices.
Claudication is another thing entirely. Claudication limits lifestyle and can be corrected by changing lifestyle -either with more exercise or limiting exercise. The thing is, when a patient has reached a certain age, that lifestyle may be walking slowly from chair to commode, and if that activity is limited, no amount of haranguing may be able to induce that person to embark on an ambitious exercise program. Sometimes, you have to be realistic about telling a frail old man to go for a 60 minute walk. But if that person has difficulty getting to the bathroom because of leg cramps, then either they have to get assistance or more bloodflow, and ironically, a little more blood flow represented by improving inflow, may not be enough.
That was what I was thinking when I was planning this operation. Improve the inflow with stents to the common iliacs and a right CFA endarterectomy, but use the opportunity of surgical exposure to extend the endarterectomy to the distal external iliac and through the entire SFA.
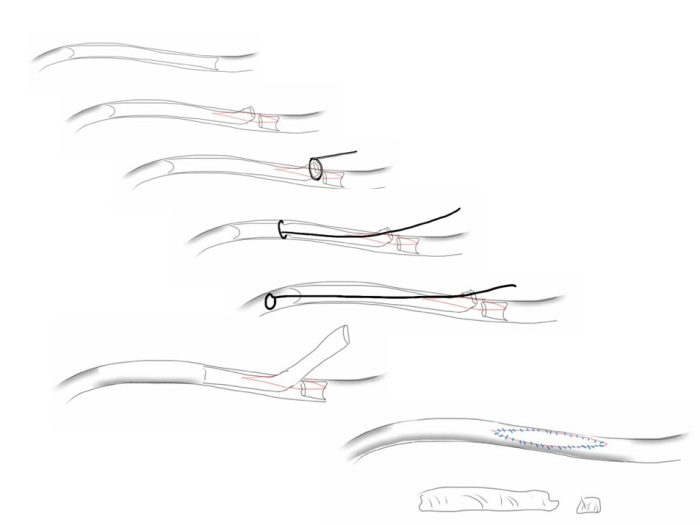
My fondness of remote endarterectomy is well known from my many blog posts on it (link). It is a modern update on a very old procedure -the ring endarterectomy, done since the middle of the last century when bypass grafts were unavailable. The occlusive plaque is removed, and an end-point reached and cut with a scissor like device (available from LeMaitre). It is the ultimate hybrid operation (below) requiring open and endovascular skills. I tell prospective trainees to judge training programs by how facile are the surgeons and how many are the procedures with and involving a hybrid approach, because any program can have few (getting fewer) old surgeons doing only open surgery and a lot of young surgeons doing only endovascular procedures, but a rare few will do a lot of hybrid procedures.
I chose to add femoral EndoRE. This would bring the extra blood flow needed to kickstart any walking program, barring cardiopulmonary limitations.
The patient was brought to our hybrid operating theatre and prepped from nipples to toes. The right common femoral artery was exposed for endarterectomy, and accessed then with a sheath along with a left femoral sheath for kissing balloon angioplasty and stenting of the common iliac artery stenoses (below).
Afterword, the CFA was opened and endarterectomized, and the SFA was remote endarterectomized (below).
The endpoint was chosen in the above knee popliteal artery to avoid having to stent the dissected end point plaque well into the popliteal artery. If I wanted to go all the way to the below knee popliteal artery, I would have to open it to manage the plaque and artery at the so-called trifurcation, typically with a patch angioplasty. The plaque came out in one piece (below):
The terminus of the plaque in the POP where it was cut has to be managed with a stent, unless you open and complete the endarterectomy and patch the artery. I was able to cross the dissection (no small feat) and plaque a stent. The artery was widely patent and even the small branches off the previously occluded SFA were now reopened.
His pulse volume recording done after intervention reflects the improved flows (below).
His rest pain resolved, but more gratifyingly, he has regained the confidence to walk and exercise, which he now does without limitation up to 45 minutes a day. In two month followup, we performed a duplex which showed his right SFA to be basically normal (below), including an intimal stripe and media. This is not an anomaly. When I took a punch out of restored artery to perform an anastomosis (from this case link), I sent it. Previously it had been an artery that was obstructed for nearly a decade, but after EndoRE, had become an elastic, compliant vessel. The pathology returned as “normal artery.”
When these fail, they typically do so a random points on the endarterectomized vessel and on the stent. While stent grafting may have better outcomes with regard to restenosis, doing so covers collateral vessels and PTFE grafts behave poorly by embolizing while clotting off, and PTFE stent grafts are no different. Data from over a decade ago suggests that EndoRE of the SFA while inferior in patency to vein grafts, are equivalent to PTFE [reference 1] and superior to endovascular revascularization [reference 2] in terms of primary patency. When they occlude, they achieve a “soft landing” without the furious acute ischemia and embolization seen with PTFE bypasses.
I think these handful of cases I performed here in the UAE represent the first in the region. The main difference here is that the arteries tend to be smaller by about 20%, and in one instance, the smallest Vollmer ring was too large for the vessel in a case where I abandoned the SFA revascularization -the profunda and inflow revascularization proved sufficient in reversing rest pain. The intriguing property of endarterectomy is something that we all try to do with surgery but rarely achieve -a restoration to an earlier time. I believe this patient’s right femoral artery is now back to a youthful state.
Patient is a 43 year old woman who had been having bouts of severe left sided abdominal pain for several years with worsening episodes of nausea and vomiting resulting in several visits to the emergency room. She has also had microscopic hematuria. Gastrointestinal workup including gastric emptying study, esophagogastroduodenoscopy and colonoscopy were negative, as was a workup for kidney stones. Eventually she was referred to my clinic for management of nutcracker syndrome. She denied lower abdominal pain nor excessive menstrual bleeding.
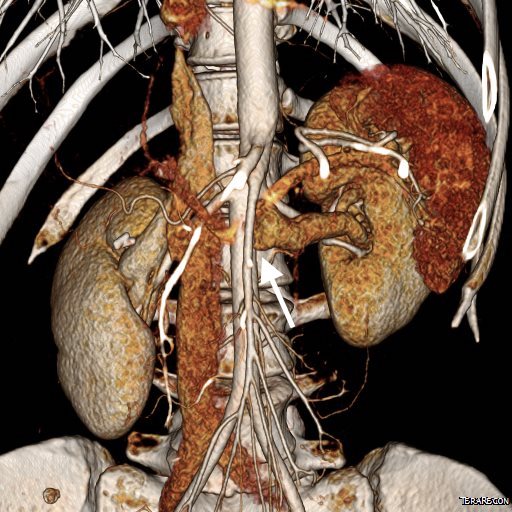
On examination, she was tender over the left kidney and flank. Laboratory examination was positive for microscopic hematuria. CT venography (below) showed an obstruction of her left renal vein by the superior mesenteric artery. Drainage via gonadal vein was not demonstrated, and no pelvic varices or complex of retroperitoneal veins was apparent.
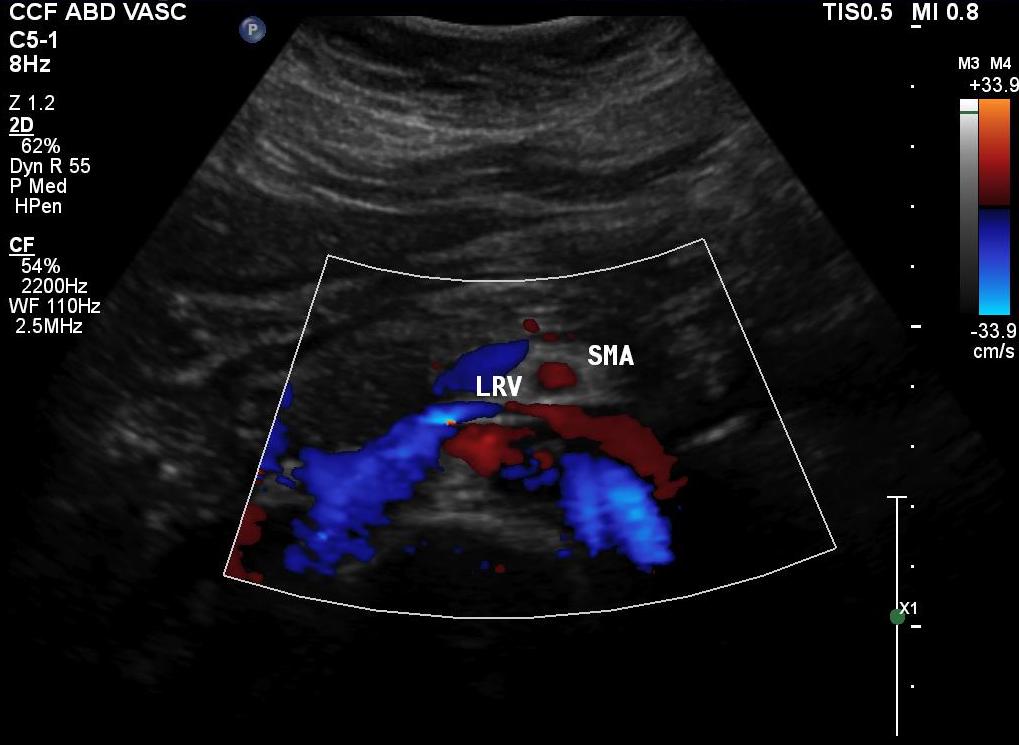
Duplex showed the narrowing in the left renal vein and spectral Doppler showed elevated velocities across the compression caused by the superior mesenteric artery (below). The collecting system was not obstructed.
Treatment options included endovascularization with a large stent in the left renal vein, left renal vein transposition to a lower position on the inferior vena cava, left renal autotransplantation, and left nephrectomy. Stent placement comes with a degree of risk for cardiopulmonary embolism which may require a sternotomy to fish out an errant stent. The risk for this in the US is because the largest nitinol stents available are 14mm in diameter which might result in undersizing in a vein that could easily dilate to well over 20mm. Larger nitinol stents for venous applications are available in Europe but currently are not approved in the US (yet). Wall stents, while certainly wide enough, have the problem of being long and stiff when not fully deployed. A 22×35 Wall stent may be 50mm long if deployed inadvertently into a tributary vein or contrained at the narrowing. Because it slides easily, passing balloons in or out can cause it to slip out of position. Because this stent elongates when compressed and packed, deployment is challenging and it is prone to “watermelon seeding,” a set up for embolism. It does have the virtue of easy reconstraining.
My friend and recent host for Midwest Vascular Surgery Society Travelling Fellowship, Dr. John V. White, in Chicago, seems to have solved this problem by a multistep process of predeploying a temporary suprarenal IVC filter, deploying a stent (whatever fits), leaving the filter as a protection against stent migration for 4 weeks until the stent permanently seats itself through scarring/intimal ingrowth, then removing the filter.
I chose to perform venography and renal vein transposition. The patient was placed in a supine position on a hybrid angiographic operating room table and her right femoral vein was accessed. She was placed in 15 degrees reverse Trendelenberg which is about the upper limit possible. Venography below.
Arrow points to left ascending lumbar vein which is taking most of the reflux. It drains the left kidney across the midline via retroartic channels to the IVCThe films showed left renal vein compression by the superior mesenteric artery with outflow via the ascending lumbar vein, both supra and infrarenal tributaries. A midline exposure was performed and the retroperitoneum opened as in an transabdominal aortic exposure. The vena cava was exposed, and the left renal vein was mobilized by ligating and dividing its tributaries. A point 5cm below the tributary point was marked on the IVC, and this was the target for transposition.
After heparinizing and clamping, the renal tributary was taken with a 5mm cuff –this would ensure proper length without narrowing the IVC.
The vein was anastomosed and flow was excellent by pulse Doppler.
She recovered well but had a longer stay because of an ileus, being discharged on day 5. Because she lived at a distance, and came back for followup the following week prior to boarding a plane for home. She no longer had the left sided abdominal pain and there was no hematuria. CT showed excellent drainage through the transposed vein.
Followup will be periodic (6 monthly) renal venous duplex from home. Given that there was minimal tension on the repair, I expect this to do well.
Discussion:
Nutcracker syndrome is one of the many unfortunate consequences of our bipedal lifestyle. The small intestines hang like baggy sausages off the branched stems of the superior mesenteric artery (SMA), and in some individuals, the SMA compresses the left renal vein against the aorta. The left renal vein receives up to 12-15% of cardiac output via the left kidney, and with outflow obstruction, drains the blood through small collaterals. The renal venous hypertension results in swelling of the left kidney with subsequent left renal colic -with flank and abdominal pain, nausea, and vomiting. There is hematuria which can be gross or microscopic. With drainage via an incompetent gonadal vein, varicoceles can occur with discomfort in men and pelvic varices with pelvic congestion syndrome can occur in women.
Diagnosis is challenging because it is one of the relatively rare non-gastrointestinal causes of abdominal pain (table).
Mesenteric ischemia
Median arcuate ligament syndrome
Nutcracker syndrome
Neuromuscular
Urolithiasis
Inflammatory aortitis/arteritis
Hypersplenism
Portal hypertension
Arterial aneurysm
Infections
Pelvic Congestion Syndrome
Endometriosis
Hernias
A history of left sided abdominal pain, flank pain, nausea, vomiting, associated pelvic pain, and episodes of hematuria are diagnostic. Examination is typically positive for left renal tenderness and flank tenderness. Laboratory examination include urinalysis for hematuria. Duplex, while technically challenging, will show renal venous compression with velocity elevation or loss of respirophasicity, CTA will typically show obstruction of the left renal vein with filling of collaterals, as will MRV.
Venography should be done in a stepwise manner (White protocol) to fully demonstrate the maldistribution of blood. That is the key word, maldistribution. I learned from my fellowship with Dr. White that performing venography in as upright a position as possible recreated the pathophysiology, the physics, particularly for pelvic congestion and nutcracker. Remember, this is a disease of bipedalism, of upright posture. Many negative studies done supine become positive, as the contrast will fall to where it prefers to go. As I have stated in the past, on the venous side, demonstrating drainage has different imaging needs than demonstrating flow. Pathologic venous drainage has three characteristics:
Varicose veins develop as an end stage process
Reversal of flow or reflux is demonstrated, particularly into small tributary veins
The midline is crossed in these usually small, now larger, collateral veins
While pressure gradients are nice if they are large, they are difficult to assess when they narrow to 1-2mmHg, particularly if they vary with cardiac cycle and respiration. Because we are assessing drainage, the distribution of contrast and the direction it goes is particularly important, and far more sensitive than pressure measurements.
Venography was done per a modification of Dr. White’s protocol for pelvic congestion:
Steep reverse Trendelenberg
Hand injection 10mL half diluted contrast, gently as to not create false reflux
Runs with catheter in left EIV, right EIV, left renal vein, right renal vein
With pelvic congestion workup, add selective bilateral gonadal and internal iliac veins.
I have started transposing gonadal veins when they have enlarged from chronic reflux (link, ref 2). Renal vein transposition was chosen because her ovarian vein was competent and too small to transpose (ref 1-3). While the patency rate of stents in veins seems to be acceptable, long term data is unavailable. Also, venographic appearances are deceiving -see the in-vivo measurement of the left renal vein after dissection:
Left renal vein at widest is 22mm, with expansion, possibly up to 28mm, but is relatively short. Do you see the SMA?The variability in diameter and length of the Wallstent in the 22-24mm diameter range makes this a challenging deployment. Given that I would not be able to closely follow this young patient, I felt compelled to recommend a durable solution (ref 4).
References:
White, J. et al, Left ovarian to left external iliac vein transposition for the treatment of nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2016;4:114–118.
Miler R, Shang E, Park W. Gonadal Vein Transposition for the Treatment of Nutcracker Syndrome. Annals of Vascular Surgery 2017, July 6. in press. http://dx.doi.org/10.1016/j.avsg.2017.06.153
Markovic J, Shortell C. Right gonadal vein transposition for the treatment of anterior nutcracker syndrome in a patient with left-sided inferior vena cava. J Vasc Surg Venous Lymphat Disord.2016 Jul;4(3):340-2. doi: 10.1016/j.jvsv.2015.09.002.
Tracheal deviation due to iatrogenic carotid pseudoaneurysm
History
The patient is an 80 year old woman with lung cancer who was getting a port placed at her home institution. It was to be a left subclavian venous port, but when access was not gained, a left internal jugular venous port was attempted, but after the intitial stick and sheath placement, pulsatile bleeding was recognized and the sheath removed. Hemostasis was achieved with clips and the wound closed and a right internal jugular venous port was placed. The postprocedural CXR shown above showed tracheal deviation and numerous clips from the initial port placement attempt, and a CT scan with contrast (unavailable) showed a carotid pseudoaneurysm of 3cm projecting posteriorly behind the pharynx/esophagus. She was kept intubated and sedated, and transferred for management.
On examination, her vital signs were stable. She had 2cm of tracheal deviation and swelling was apparent at the base of the neck. While my trainees may be better versed at this than I at the particulars of this, my old general surgery trauma training kicked in, as she had a Zone I neck carotid injury, which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
Open repair
Endovascular repair from femoral access
Hybrid repair
Open Repair
Open repair is the approach of choice for zone 2 injuries because aerodigestive tract injuries can also be addressed and the exposure is straightforward. For Zone 1 injury, the exposure is potentially possible from a neck exposure, but in my experience, jumping into these without prepping for a sternotomy puts you into a situation without a plan B. The exposure of the carotid artery at this level becomes challenging with hemorrage from the artery once the compression from the hematoma or pseudoaneurysm is released. A sternotomy in this elderly woman, while not optimal, may be necessary if open control is required, but the best plan is to avoid this.
Endovascular Options
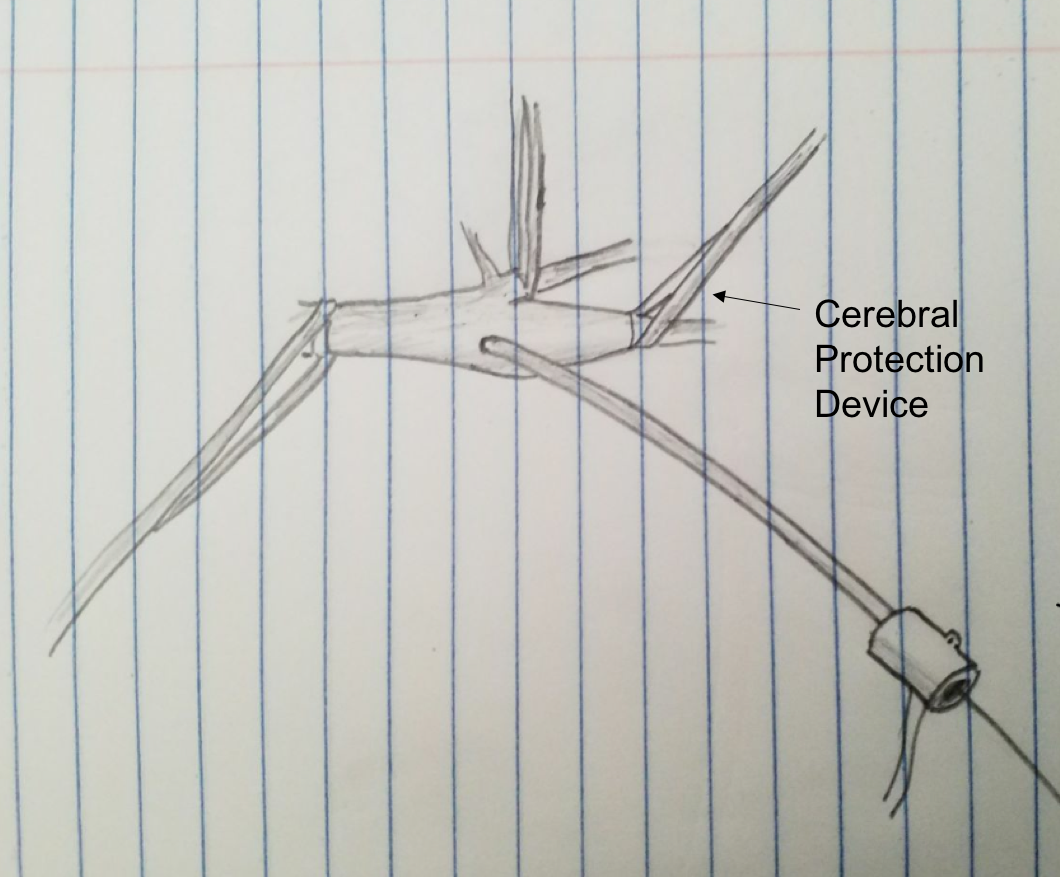
This should be a straightforward repair from an endovascular approach, even with the larger sheath required for the covered stents. A purely endovascular approach is problematic for two reasons. One, cerebral protection devices are built for bare carotid stents and not peripheral stent grafts, but this is not prohibitive -it should be fine. Without a planned drainage, the hematoma would be left behind which could cause prolonged intubation and problems with swallowing -both an issue for an elderly patient battling lung cancer. Endovascular access could provide proximal control for an open attempt from above, but instrumenting from the arch in an 80 year old has a known 0.5-1% stroke rate.
Hybrid Repair
A hybrid open approach with exposure at the carotid bifurcation offers several advantages. With control of the internal carotid artery, cerebral protection is assured while the carotid artery is manipulated. At the end of the procedure, the internal carotid can be backbled through the access site with the common carotid artery clamped. The hematoma could be avoided until the stent graft is deployed. An unprotected maniplation in the arch can be avoided. Once the stent graft is deployed, drainage of the hematoma can be performed.
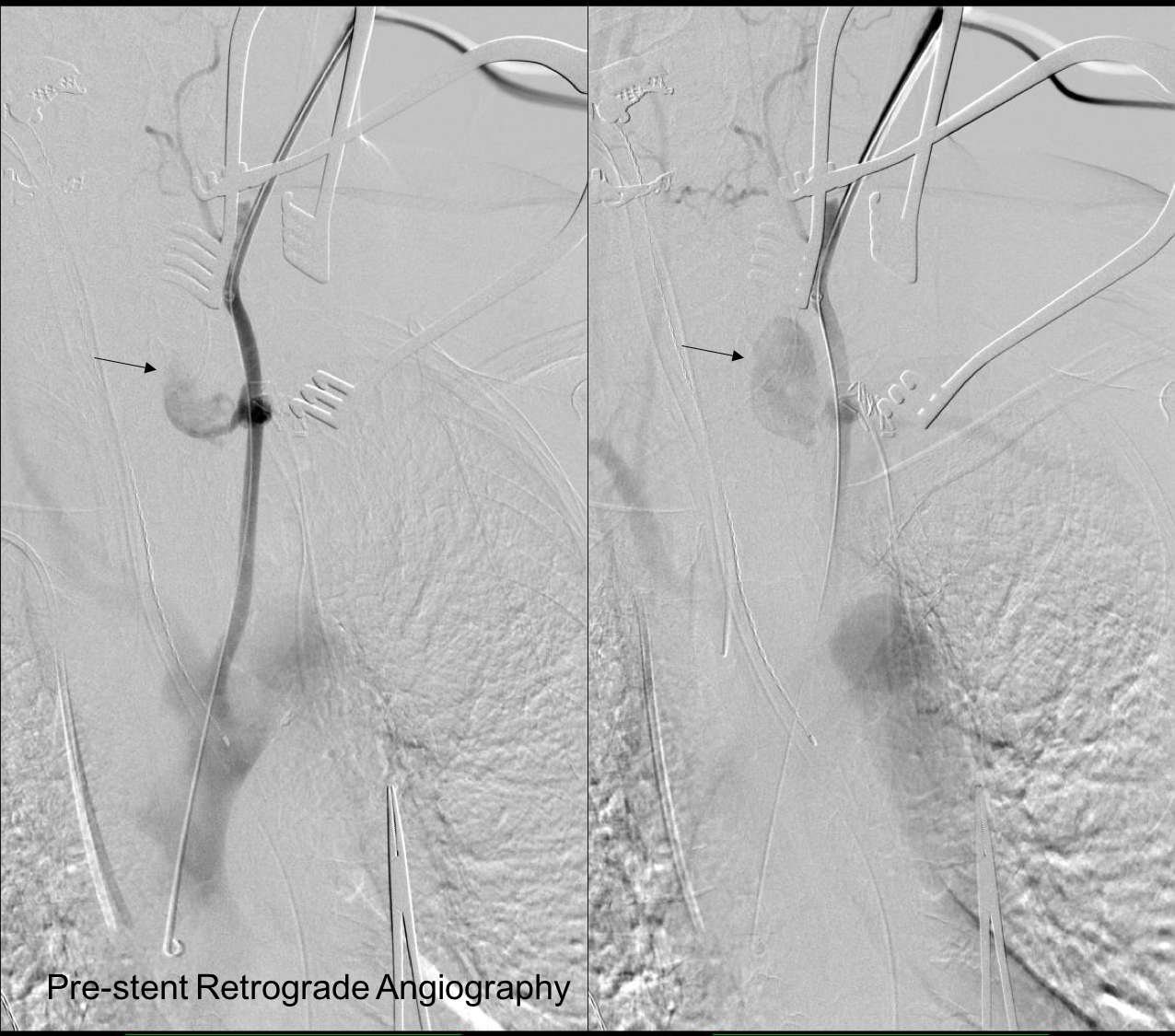
This required setting up a table off the patient’s left that allowed the wire to lie flat to be manipulated by my right hand. The carotid bifurcation was accessed through a small oblique skin line incision and the common, internal, and external carotid arteries, which were relatively atherosclerosis free, were controlled with vessel loops. The patient was heparinized. The internal carotid was occluded with the loop, and the common carotid below the bifurcation was accessed and an 8F sheath with a marker tip inserted over wire. Arteriography showed the injury and pseudoaneurysm.
The location of the injury based on CT and on this angio would have baited a younger me into directly exposing it, but experience has taught me that which occasionally you can get away with it, the downsides -massive hemorrhage, stroke, need for sternotomy, just aren’t worth it. The sheath was brought across the injury and a Viabahn stent graft was deployed across the injury.
The hemorrhage was controlled and the hematoma was then exposed and drained -the cavity was relatively small and accepted the tip of a Yankauer suction easily. A Jackson-Pratt drain was placed. The access site was repaired after flushing and retrograde venting as described.
She recovered rapidly after extubation postop. She was able to breath and swallow without difficulty and had suffered neither stroke nor cranial nerve injury. The drain was removed on postop day 2.
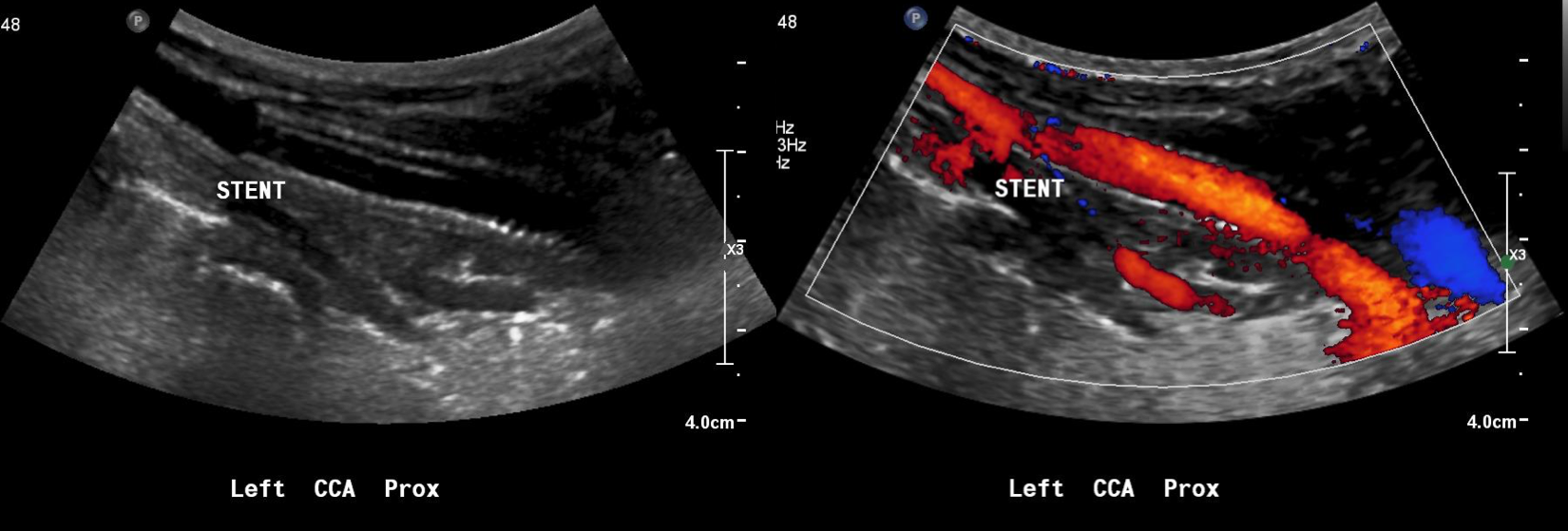
The patient recently returned for a 6 month followup. Duplex showed wide patency of her stent.
More gratifyingly, her port was removed as her cancer was controlled with an oral regimen.
Discussion
Let me start with my bias that all penetrating trauma should be approached in a hybrid endovascular OR. It is a natural setting for trauma and this case illustrates that. In a hybrid operating room, central aortic and venous injuries can be controlled endovascularly while open repair, including salvage packing, can be done. Excess morbidity of central vascular exposures can be avoided. Temporary IVC filters can be placed if indicated (becoming rarer and rarer). Cardiopulmonary bypass can be started.
In this patient, hybrid therapy brought the best of both techniques and avoided many of the pitfalls of the purely open or endovascular approach. For stable zone I penetrating injuries of the neck, it is clear that this is a reasonable approach.
The patient is a gentleman from out of state who had called about problems he was having with walking and with leg ulcers that wouldn’t heal. He is in his seventies and has a pacemaker for an arrhythmia for which he was on Xarelto. He also had type II diabetes. He had bilateral lower extremity deep venous thromboses 6 years prior requiring IVC filter placement. The filter occluded, and it resulted in sudden sharp and debilitating pain in both legs with walking short distances -some days only 50 paces.He described it as an unbearable pain in calves and thighs that felt like his legs were going to burst. He also had ulcers on his legs that would heal with ministration but soon recur. This was all despite being quite active, with regular workouts, and being fit. He was compliant with compression. He sent a CT scan done last year (below).
Right iliocaval centerline projection
It showed an Optease retrievable vena cava filter that was occluded and the iliac systems bilaterally (right above and left below) were chronically occluded with patent vena cava above and femoral confluences bilaterally below.
Left iliocaval system showing chronic occlusion on centerline projection
He had no hypercoagulability nor ongoing recent DVT’s. I thought there was a good chance that we would be able to recanalize the occluded iliocaval segment and he flew in for a consultation, and he was pencilled into the schedule ahead of his visit.
Examination revealed a fit and trim man in his 70’s in no apparent distress. He had bilateral leg edema that was moderate with small superficial and tender ulcers of the right posterior distal calf. Pulses were normal. He was taken to our hybrid suite and venography from femoral vein access in the proximal thigh in the supine position revealed his right and left iliac venous systems to be occluded (below figures).
Right injection from femoral sheath showing occluded iliac vein with collaterals
Left injection
Wire access into the iliac systems was performed with Glidewire and Glidecatheter periodic venography to confirm that I had not exited the vein. Unlike the arterial system, extravasation from being extravenous does not have the consequence of bleeding, hematoma development, and pseudoaneurysm formation because of the low pressure, but it can be a long procedure and uncomfortable as well so these are done under general anesthesia.
Advancing wire and sheath into iliac vein, crossing filter resulted in extravasation of contrast
Once position confirmed to be in the iliac vein, the vein was dilated to allow for greater ease of movement. In the case of the uncrossable filter, I switched to access from above via a right internal jugular vein access.
Dilating vein (left) for greater mobility, and crossing from above (R. IJV access)
Once the wire crossed into the iliac vein from above, it was captured and brought out. While ballooning by itself is inadequate for revascularization, it greatly eases wire capture and on the right, it was done simply by driving the wire from above into the sheath. Wire capture wins access across the iliocaval and IVC filter occlusion from below.
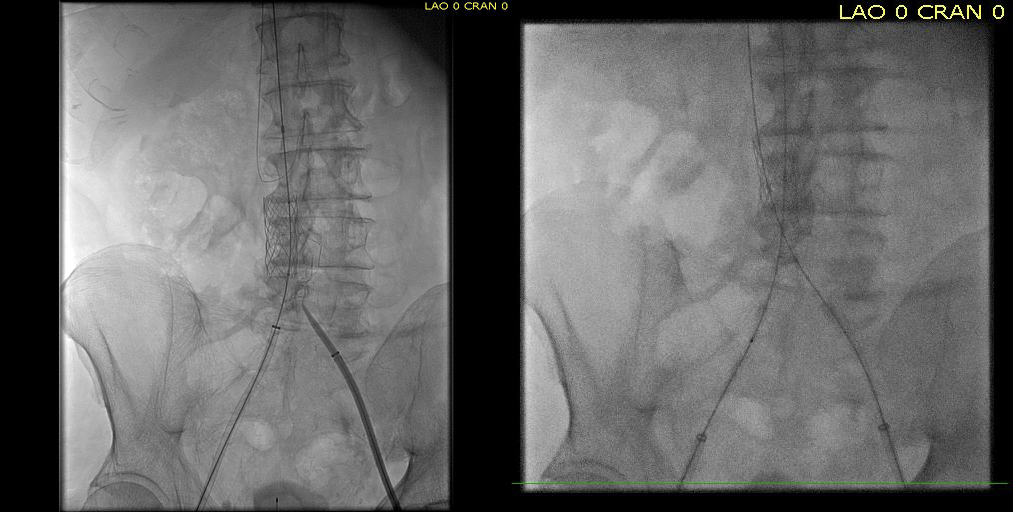
Wire passage across IVC filter into right and left systems
Once wire access is done, ballooning across the filter is done from both sides. A large sheath is them delivered across the IVC filter. Finally, a Palmaz stent mounted on a large balloon is delivered and deployed. I chose to do this from the right access, and retracted the wire on the left -something done with some trepidation because of the great difficulty gaining this access, but with with prior balloon dilatation, reaccess is made easier. Also, plan B would be reaccess from above.
After balloon dilatation of occlusion typically to 8mm from both sides, a sheath placed and Palmaz stent deployed across filter on a large 24mm balloon
When this is accomplished, the left sided wire is reaccessed across this stent. This is the venous side analogue to gate access in EVAR (below).
Reaccess of the left iliac venous wire across Palmaz stent
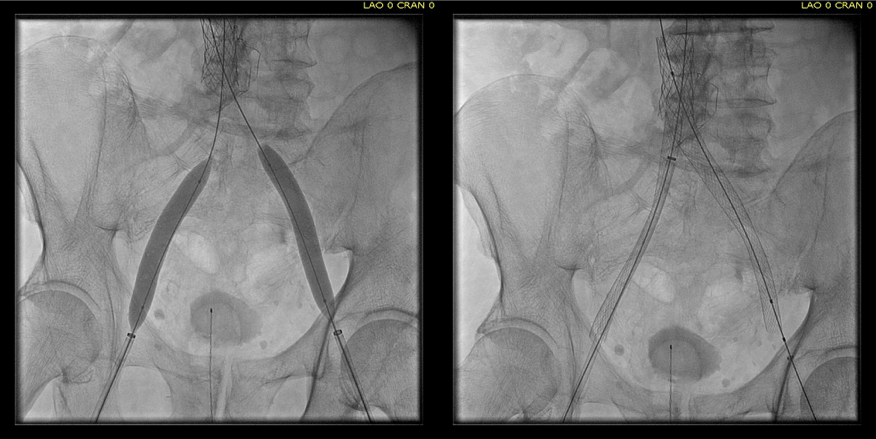
Once this is done, the iliac veins are dilated to 14mm from the IVC to the common femoral arteries. large 18mm Wall stents are deployed in a kissing fashion from the caval stent into both iliac systems and dilated to 18mm.
Predilatation of iliac venous systems with ever larger balloons, deployement of bilateral 18mm Wall Stents
After deployment, the Wall Stents are ballooned to 18mm. These stents were extended into the common femoral artery with 14mm nitinol stents.
Ballooning 18 mm Wall Stents with 18mm Atlas balloons, then extending to CFA with nitinol stents of 14mm
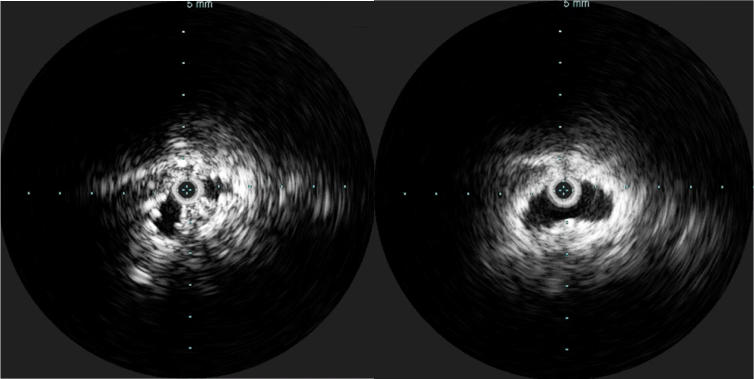
Completion venography suggested successful iliocaval recanalization and revascularization but these procedures are not done without a final intravascular ultrasound (IVUS).
Looks done, but needed final intervention after IVUS.
Intravascular ultrasound revealed incomplete expansion of the right common femoral stent. This was treated with another stent and ballooning with the result on the right.
Stent compression on IVUS treated with second stent
Venography alone is insufficient in determining patency. As illustrated, IVUS ensures a durable outcome.
The leg ulcer was treated with an Unna’s boot. A word about the venerable Unna’s boot –it works. The dressing dries and compresses while the Zinc Oxide prevents bacterial growth. It is interesting that the dressing is so infrequently used nowadays but not so when you consider that it isn’t reimbursed. And patients generally hate it.
This revascularization has an excellent chance at working as the patient has no hypercoagulability and had a patent common femoral confluence bilaterally. As I had mentioned in a prior post, the idea in venous revascularization is connecting confluences that serve as inflow and outflow.
This will require followup, consisting of duplex, and it is advantageous that he is anticoagulated for his arrhythmia. It is becoming more apparent that those languishing with chronic venous insufficiency and its complications need the IVC and iliac veins interrogated with a duplex. When an obstruction is found, they should be treated with these techniques as a first line therapy.
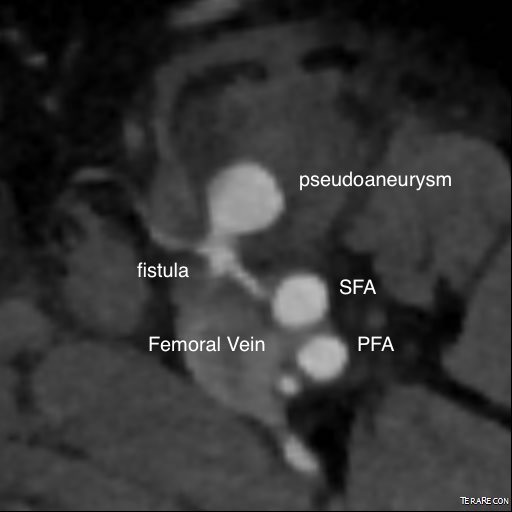
The patient is a middle aged man who after an interventional procedure was referred to my clinic with an expanding hematoma due to a pseudoaneurysm complicated by an arteriovenous fistula. He was a week out from his procedure and had grown a hematoma roughly the size of a hard boiled egg in his left groin which caused him pain. A duplex scan showed a pseudoaneurysm (below) with fistula flow.
On examination, he had this well circumscribed indurated hematoma of hard boiled egg size with tenderness. There was a bruit on auscultation. Duplex showed a small chamber of flow adjacent to the proximal superficial femoral artery emptying into the femoral vein. Doppler in the common femoral vein showed relatively high fistula flow, and this is reported to be associated with failure of thrombin injection. CTA (top) demonstrated flow of contrast from femoral artery to vein through a pseudoaneurysm chamber that laid between. Angulation to an axial orientation showed this better (below).
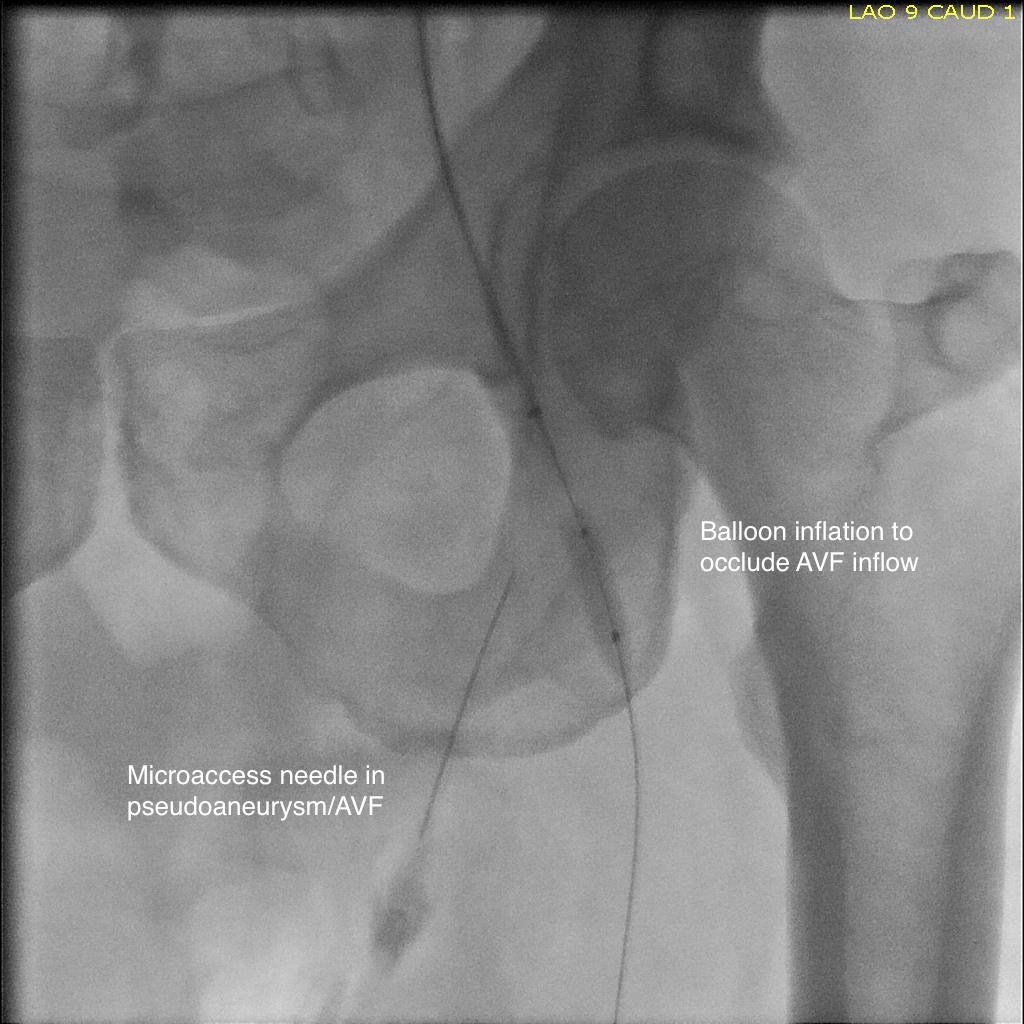
Contrast flows from femoral artery (right) to the fistula chamber, then into the femoral vein. Axial MPROperation was planned, but in the days leading up to the operation, I had a thought -the primary reason why ultrasound guided thrombin injection would fail is the AVF. It would be simple to fluoroscopically guide an angioplasty balloon on the arterial side to occlude the fistula inflow. The next step would be to get access to the pseudoaneurysm with a needle under ultrasound guidance, confirm location with a contrast injection. Once confirmed, the balloon is inflated and a small volume of thrombin would be injected. I discussed this with the patient in detail and he was enthusiastic about trying this before proceeding with an open repair.
Schematic of procedureThe procedure went as planned. Ultrasound guided access is aided with dual live display of B-mode and color flow (below)
Arteriography showed much of the contrast from injection of the pseudoaneurysm to preferentially go to the artery which made me worry less about creating a DVT/PE. With balloon inflated (below), thrombin was injected and balloon inflation held for about 30 seconds.
There was resolution of flow in the pseudoaneurysm and in the fistula. Before and after duplexes are composited below.
Repeat duplex on the following day showed resolution of the pseudoaneurysm and arteriovenous fistula.
In the days before ultrasound guided thrombin injection of pseudoaneurysms, open surgical repair of these was fraught with complications. First, these patients typically had cardiac disease. Second, they were usually anticoagulated often with multiple agents. And finally, they were many times obese, making not only the operation fraught with complexity, but the ultimate wound healing a delicate and rare phenomena. Even now, we get emergency repairs when access hemostasis fails, and these patients are typically high risk. With hematoma evacuation, inflammation, lymph leaks, and infections may follow; the patient was correct in his enthusiasm for agreeing to proceed with a minimally invasive effort.
As to the techniques, they are all well established in the vascular surgeon’s toolbox. Ultrasound guided access of the pseudoaneursm should be obtained before arterial occlusion. This was facilitated by general anesthesia which kept the patient from moving. Having access to excellent ultrasound and angiographic imaging made this possible. The patient felt much better and was discharged home the next day after his confirmatory duplex.













































 which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were: