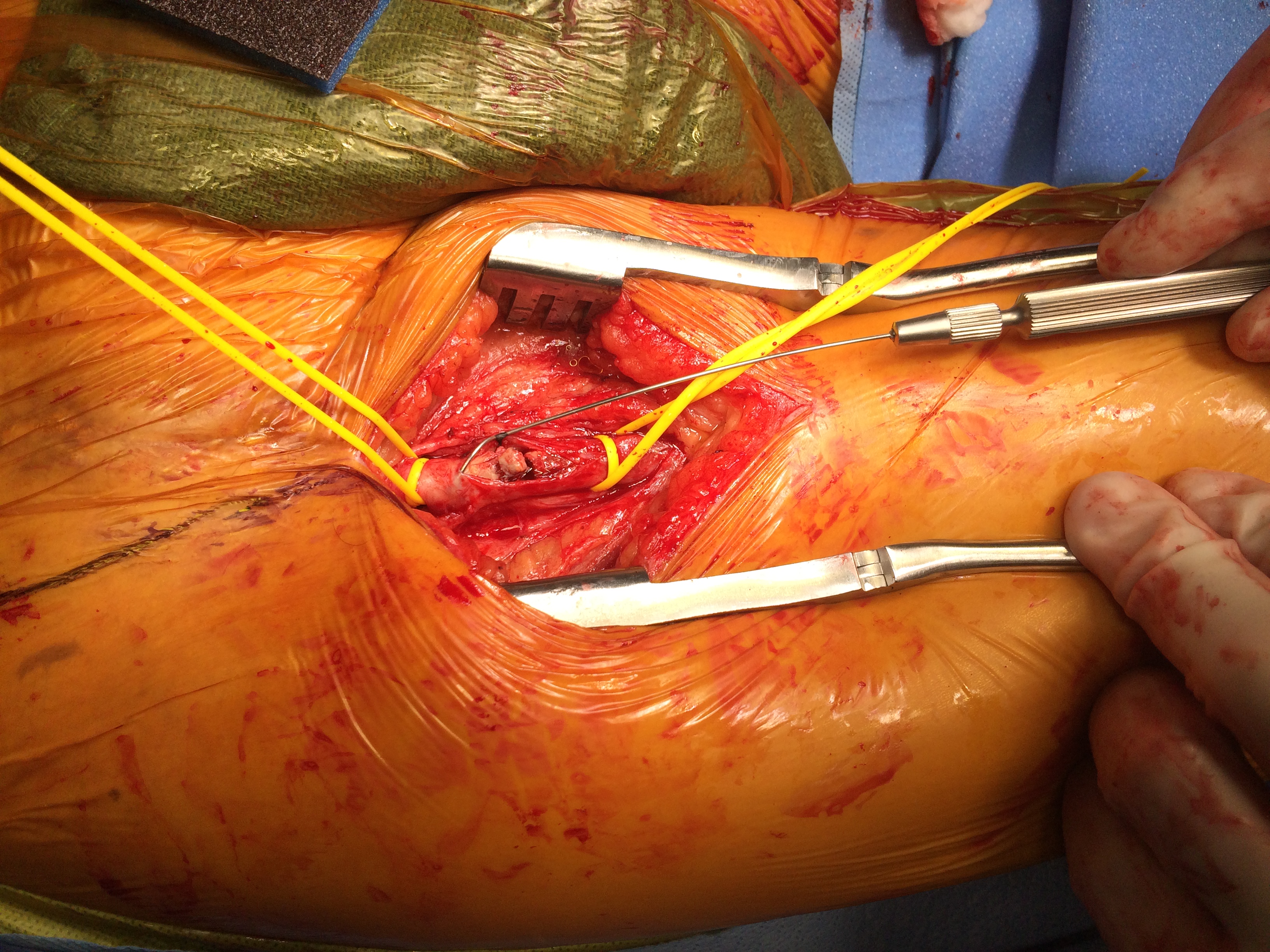
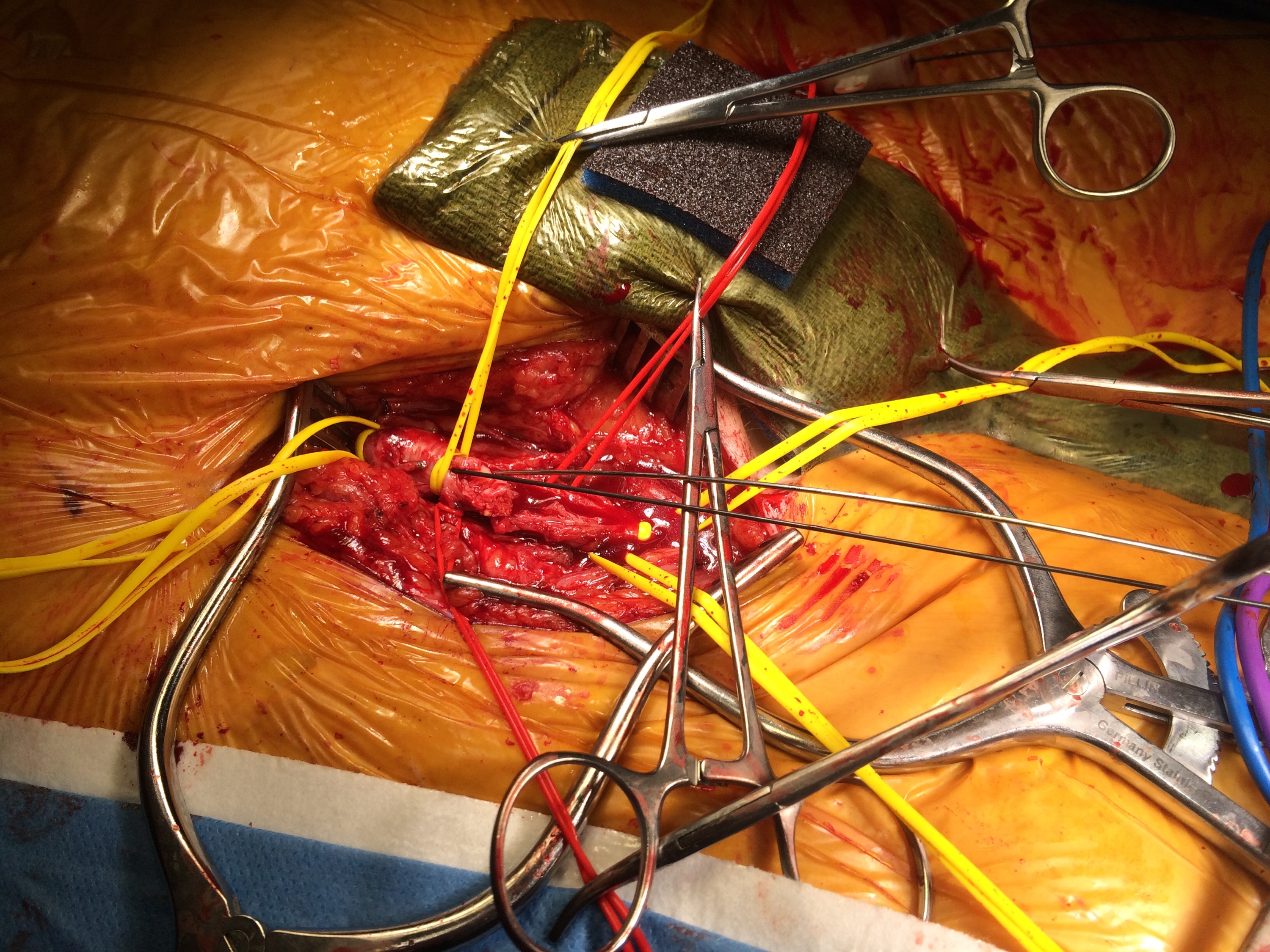
The principles of salvage are in rescuing valuable undamaged goods in the setting of catastrophe. This guided me when a patient was flown in from an outside institution to our ICU with a saline soaked OR towel in his right groin -he had had an aorto-bifemoral bypass for aorto-iliac occlusive disease a year prior, but had never properly healed his right groin wound which continued to drain despite VAC therapy and wound care. On revealing his groin, this is what I saw:

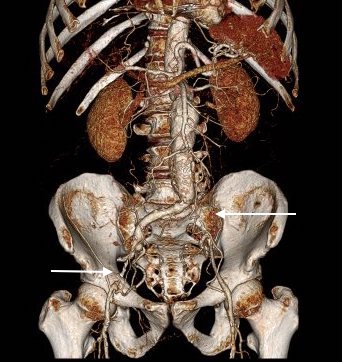
A CT scan was sent with the patient but has been lost to time, and it showed a patent aorto-bifemoral bypass send flow around an occluded distal aorta and iliac arteries. The graft did not have a telltale haze around it nor a dark halo of fluid which signaled to me that it was likely well incorporated and only sick in the exposed part. The patient was not septic, but had grown MRSA from the wound which was granulating from the extensive wound care that had been delivered.
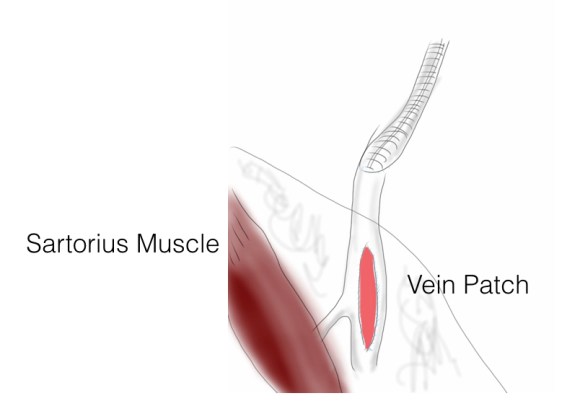
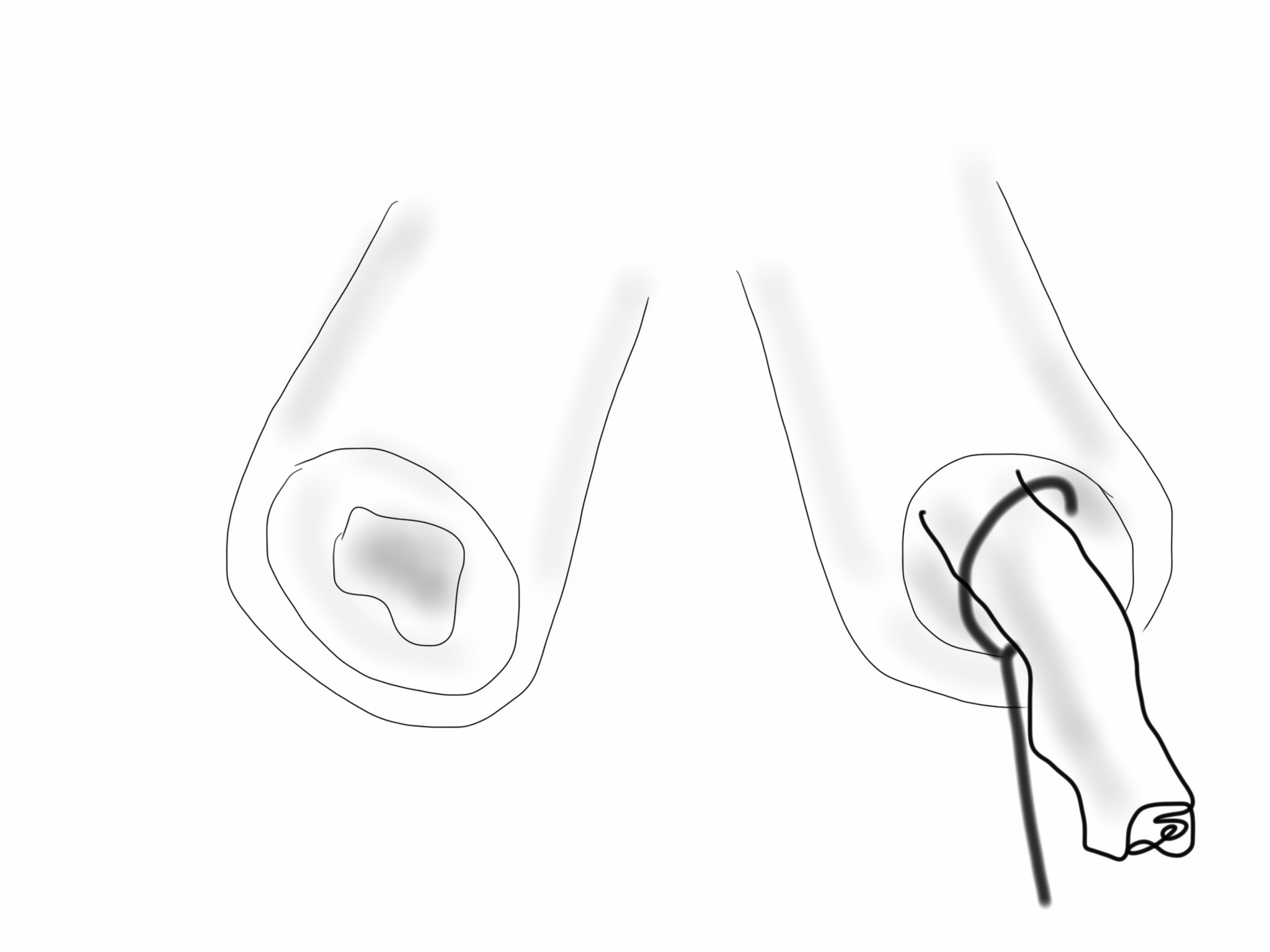
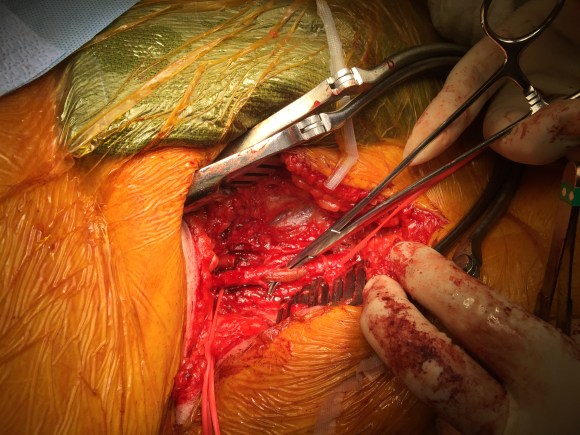
I felt that it would be possible to move his anastomosis point more proximally on the external iliac in a sterile field (figure above), and then close, then endarterectomize the occluded external iliac artery after removing the distal graft, then after vein patching, cover the repair with a sartorius muscle flap. It would salvage the remaining graft and avoid a much larger, more intense operation which was plan B. To prepare for that, I had his deep femoral veins mapped.
The patient was prepped and draped, the groin was excluded by placing a lap pad soaked in peroxide/betadine/saline solution (recipe for “brown bubbly” liter saline, a bottle of peroxide, a bottle of betadine), and covering with an adesive drape. The rest of the abdomen was then draped with a second large adhesive drape. A retroperitoneal (transplant-type) right lower quadrant incision was made (below) and the external iliac artery and graft were exposed. As predicted on CT, the graft was well incorporated.

The external iliac artery was opened and focally endarterectomized of occlusive plaque (image below). The adventitia had good quality despite the longstanding occlusion.

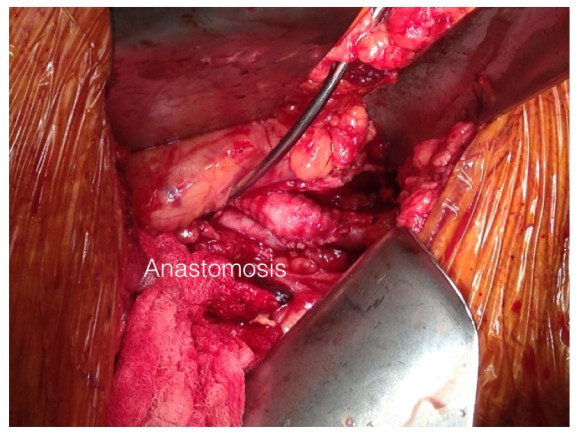
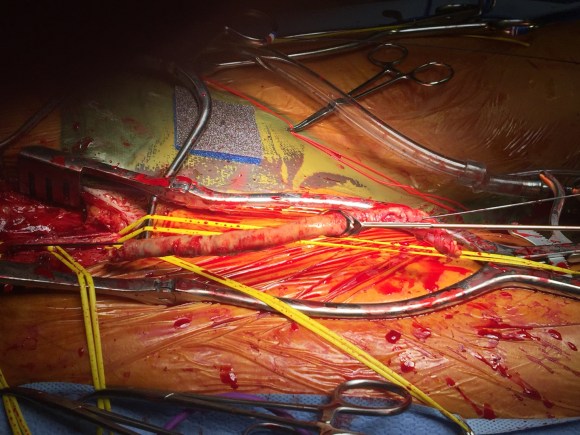
The graft was mobilized and transected and anastomosed end to side to this segment of artery (below). Dissecting was made difficult by how well incorporated it was.
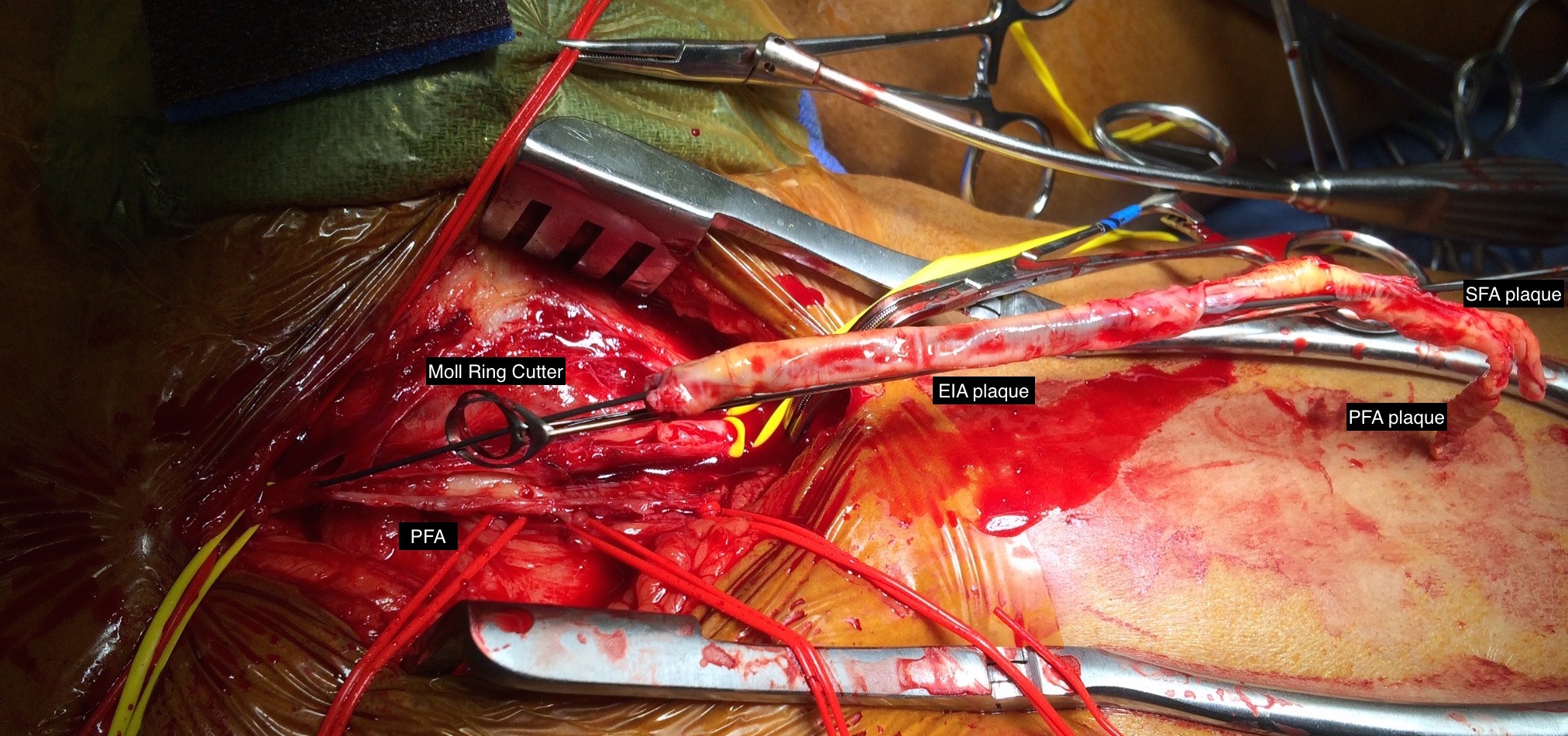
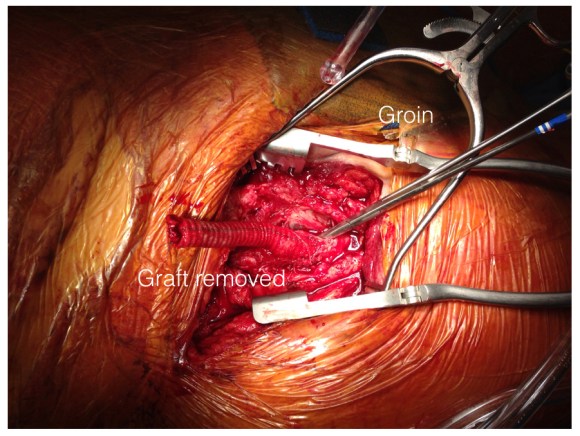
The wound was irrigated (with brown bubbly) and closed, dressed, and sealed over with the adhesive drape. The groin wound was then revealed and the graft pulled out (below).
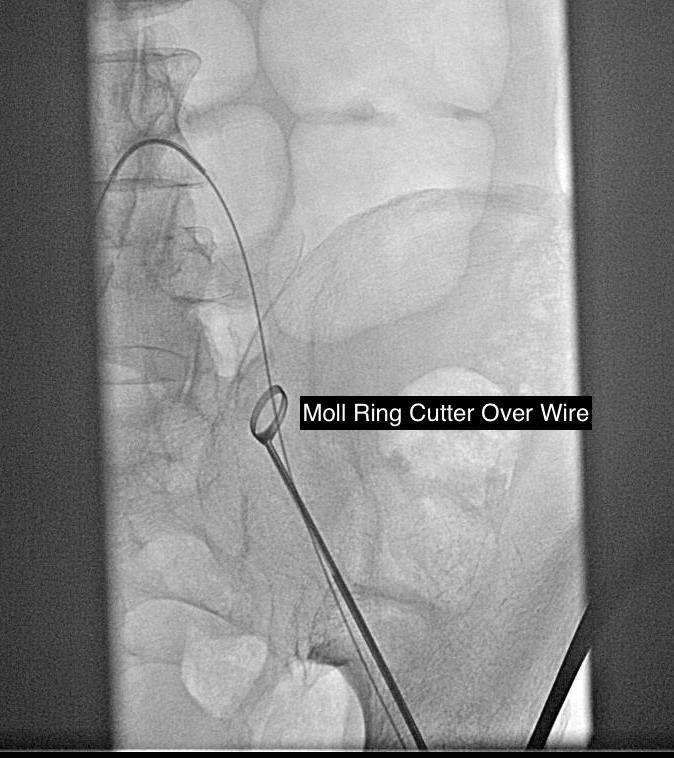
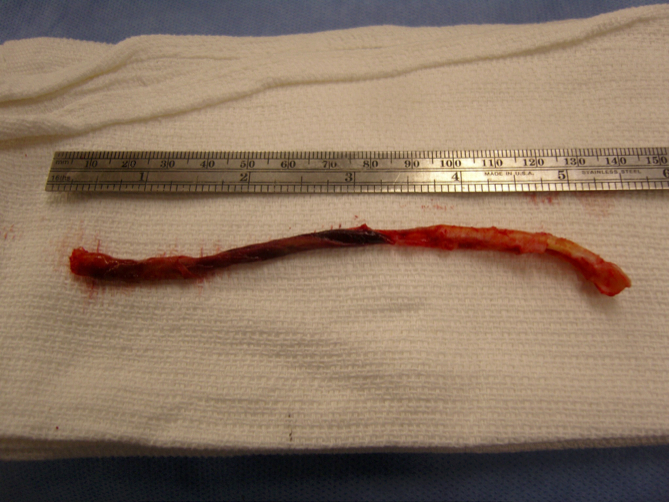
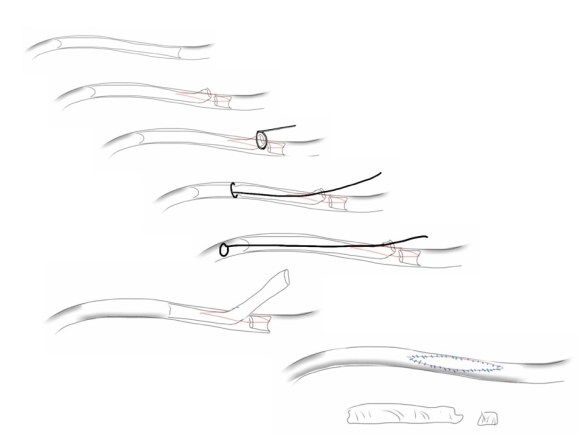
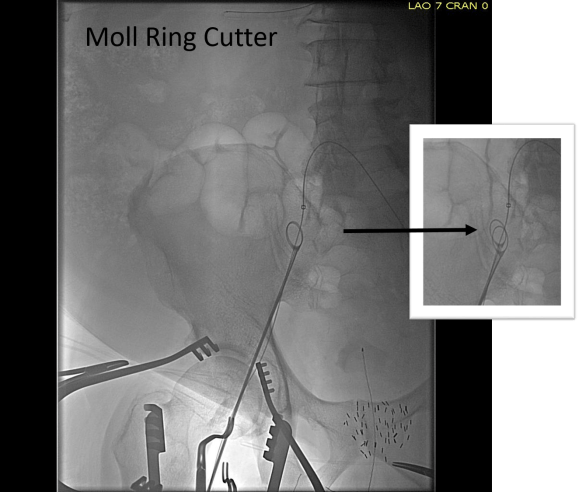
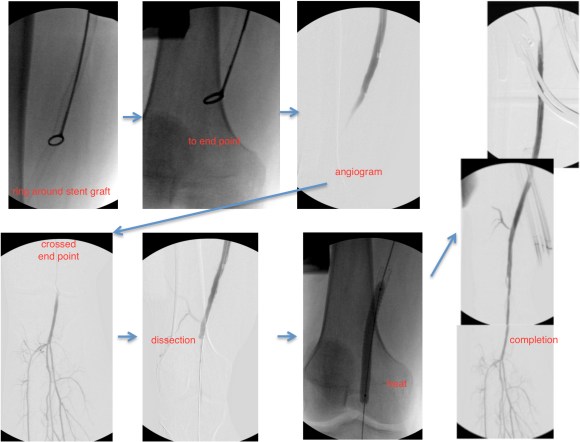
Remote endarterectomy using a Vollmer ring was used -in this case I didn’t use fluoroscopy given the short distance to the terminus of the plaque which i had mobilized in the pelvis.

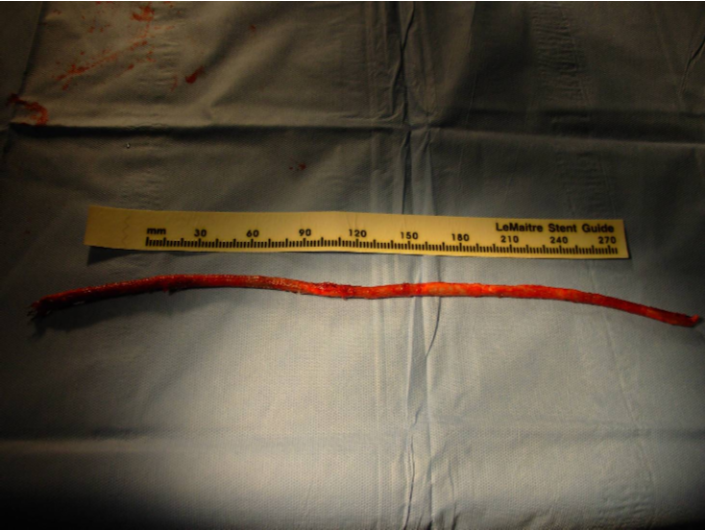
The plaque came out easily and was not infected appearing. It is shown below ex vivo.

A segment of saphenous vein was harvested from the patient medially and the arteriotomy was patched. The sartorius muscle was mobilized and applied as a flap over this. The wound was irrigated with brown bubbly and packed open with the intention of VAC application.
The patient healed very rapidly and remains infection free. I had used this approach on several occasions in the past and twice more recently. It truly is salvage as it preserves the uninfected graft while never exposing it to the infection in the process of operating. It avoids having to remove the whole graft which then damages the left side -I have seen other surgeons take this approach elsewhere taking a all-or-nothing approach to graft infection to considerable morbidity to the patient. It avoids having to harvest deep femoral vein -another large operation to which the body responds truculently. The patient recently came by for his 4 year followup, still smoking, but legs preserved.
Followup At 4 Years

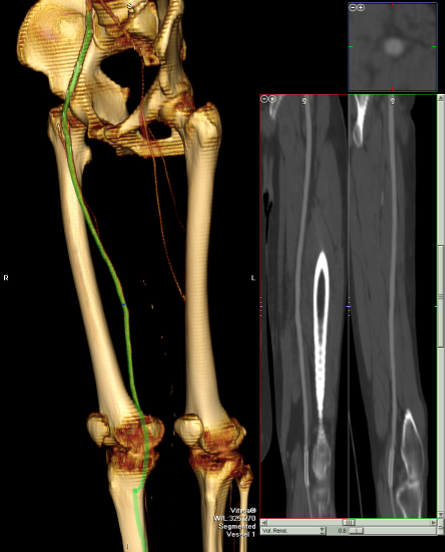
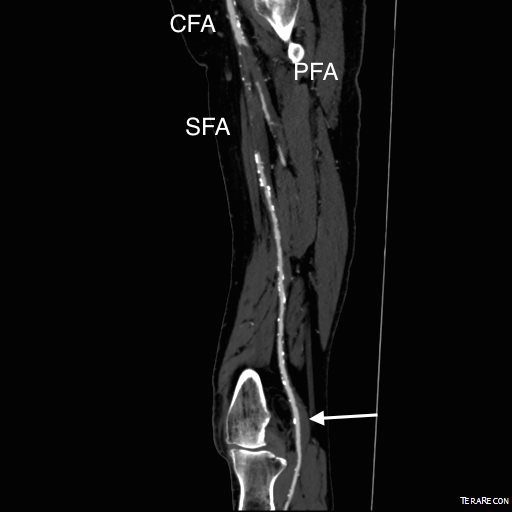
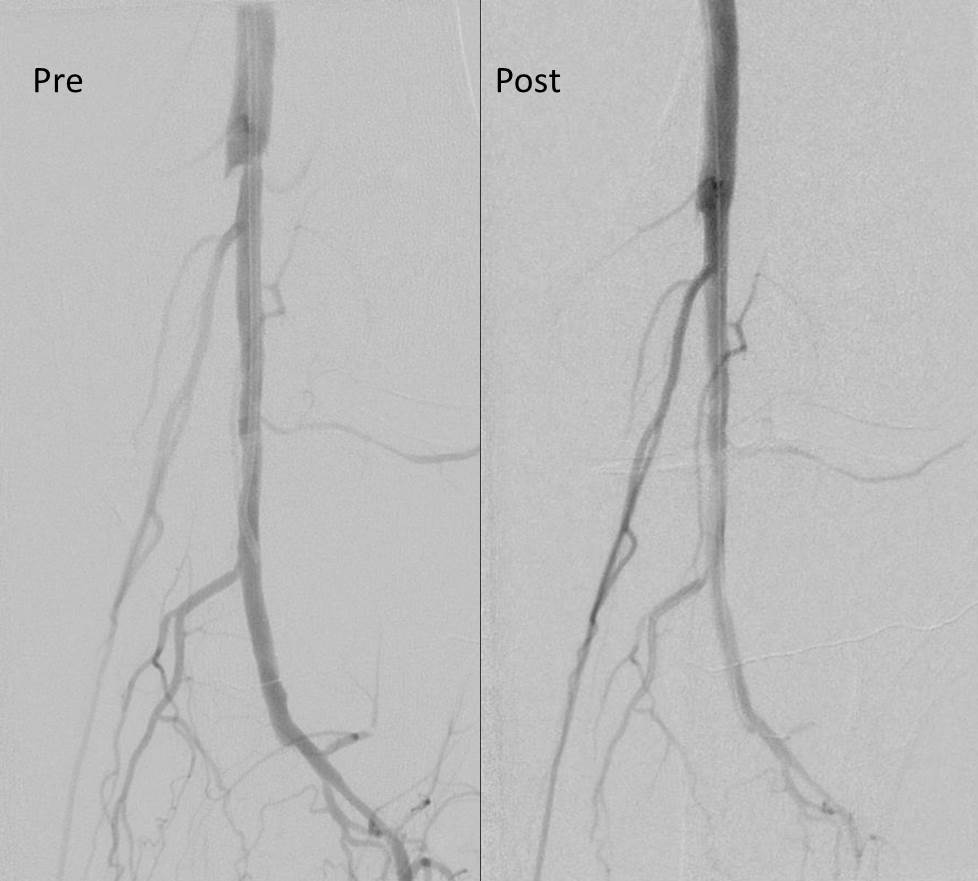
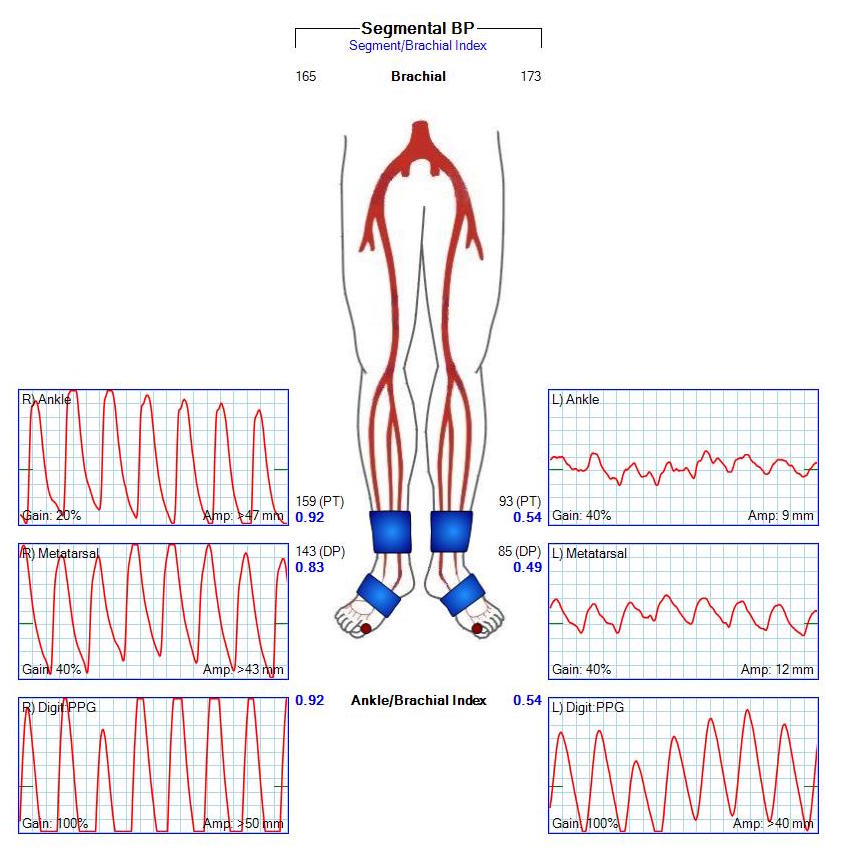
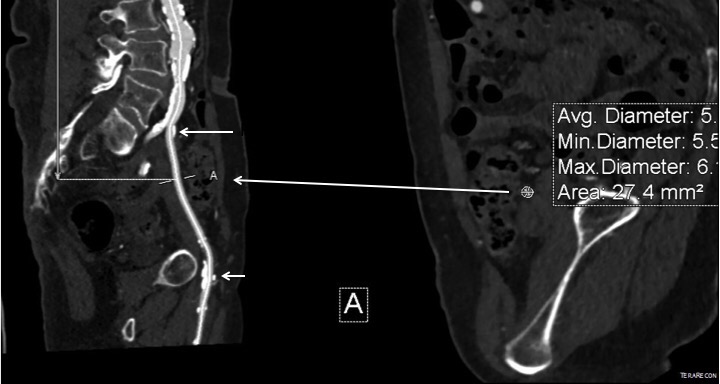
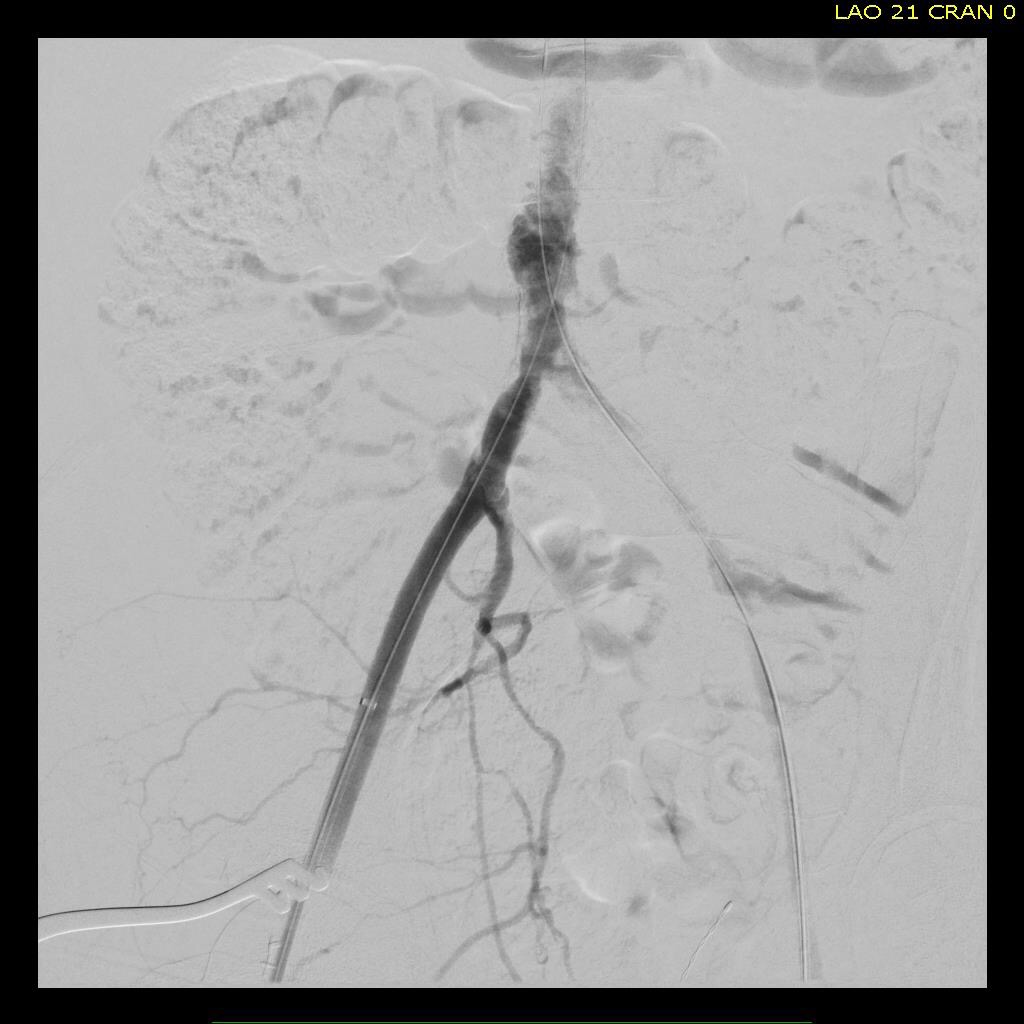
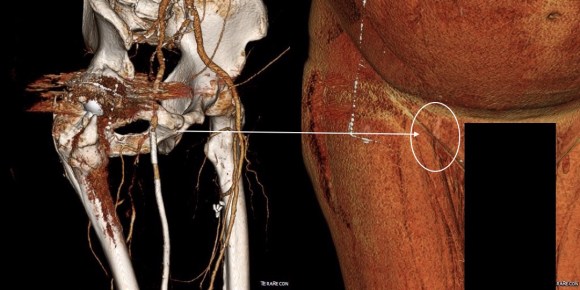
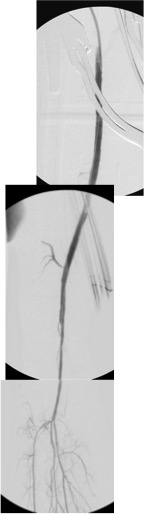
The patient came back in followup -it has been 4 years since his infection was repaired. He was complaining of short distance claudication. His wound healed well and remains closed. CTA shows along with his short segment SFA occlusion which we will treat, a widely patent R. EIA (below).

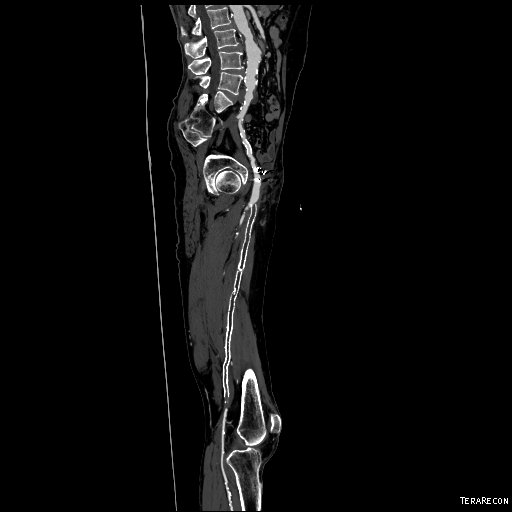
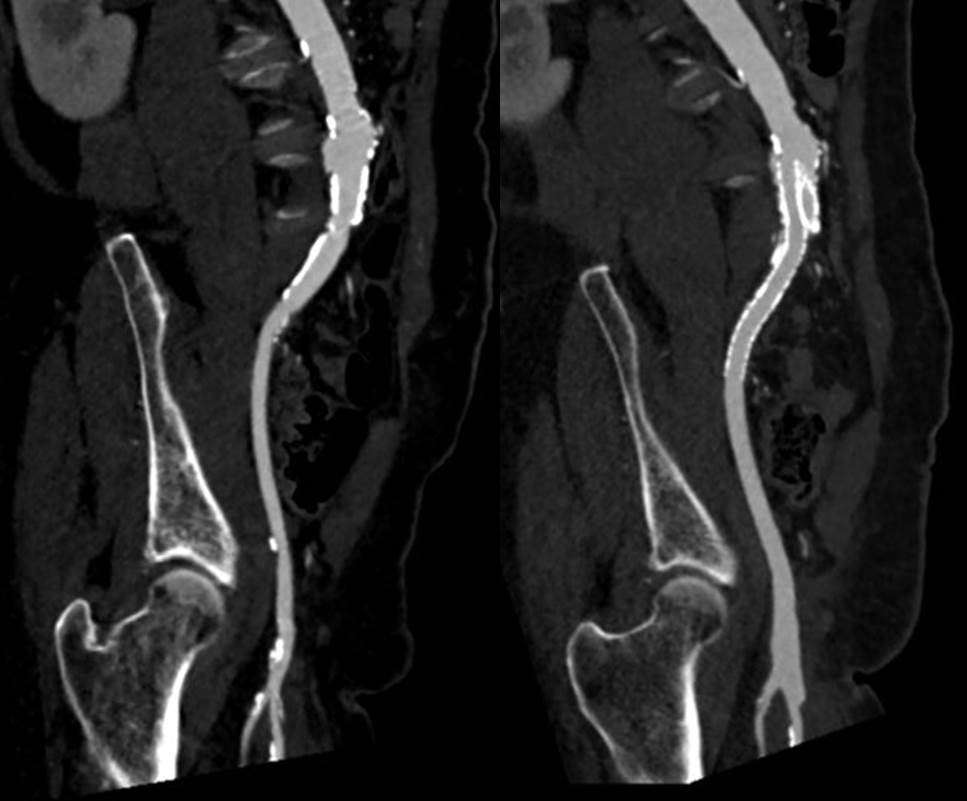
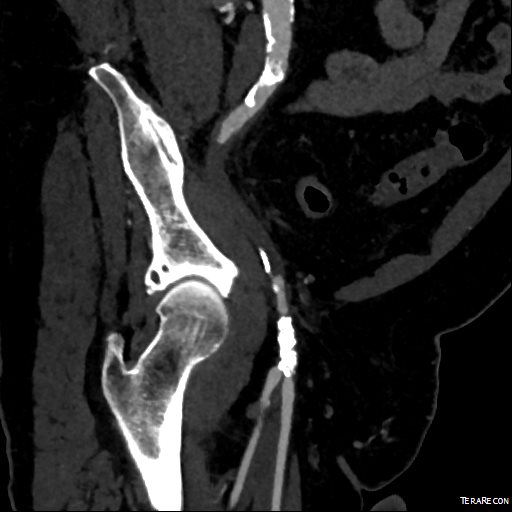
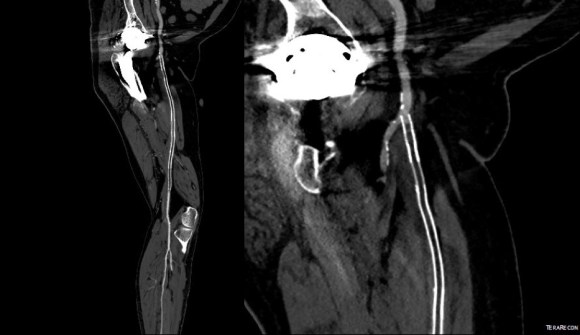
The remote endarterectomy of the external iliac artery remains patent. Compare this to the preop CTA which I found and wasn’t available when I posted this case originally:
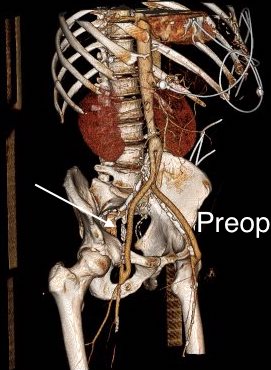
The chronically occluded EIA can be readily seen. The artery shown in the current CTA is that recanalized artery.













 The patient regained palpable pulses in his right foot and recovered well, being discharged home after a 4 day stay.
The patient regained palpable pulses in his right foot and recovered well, being discharged home after a 4 day stay.