Context
Despite all the advances in endovascular repair of thoracoabdominal aortic aneurysms, no data shows their superiority in the mid to long term compared to open repair. That is why branched stent graft programs occur hand-in-hand with robust open surgical programs, to offer durable open solutions to younger healthier patients while mitigating risk in older sicker patients by going with a branched or fenestrated device. Despite these advances, clamp time and visceral ischemia persists as a challenge to safe performance of open thoracoabdominal aortic surgery. Even a straightforward group IV requires the surgeon to be swift. Time on an thoracic aortic clamp results in visceral ischemia with a predictable response of coagulopathy, acidosis, systemic inflammation, and renal insufficiency. Adding cardiopulmonary bypass mitigates some things (distal ischemia, normothermia, hypertension) but brings on other complexities (cannulation, circuitry, coagulopathy). Sewing to a Carrel patch allows one to perform one large anastomosis rather than four individual ones, gaining speed and time, but compromises by leaving aneurysmal tissue which could progress to a troublesome patch aneurysm. TAAA is a condition that demands referral to high volume centers. It is in high volume centers that these apex predator surgical conditions can be subdued. It is in these centers that branched/fenestrated stent graft programs can offer treatment for patients high risk for open repair. It is in these centers that patients can avoid compromises such as snorkels and chimneys. Unfortunately, these centers are long air flights away and the means of the patients may not match the desires. Out here in Abu Dhabi, half a world away from Cleveland, Rochester, Houston, Boston, Chapel Hill, New York, and Seattle, and over six hours from major centers in Europe, we usually have to find our own way. Thankfully, we have the resources in experienced staff and abundant materiel.
During my time at the main campus of Cleveland Clinic, I came to appreciate the hospital as a highly evolved tool for healing, but for open repair of TAAA, it still falls on the operating surgeon and the choices made that shaped the outcome. In this most invasive of operations, simplicity and efficiency translating to speed offers the only consistent path to success. My partner, Dr. Houssam Younes, who trained in Houston, mentioned that Dr. Joseph Coselli, has clamp times approaching 30 minutes for group II TAAA -an almost inhuman speed achieved by doing these cases every day. For this reason, stent grafts are popular because repair of aortic aneurysms can be achieved by more practitioners in widely distributed settings. Because of the marketing of all things minimally being better, patients come asking for endovascular.
Case
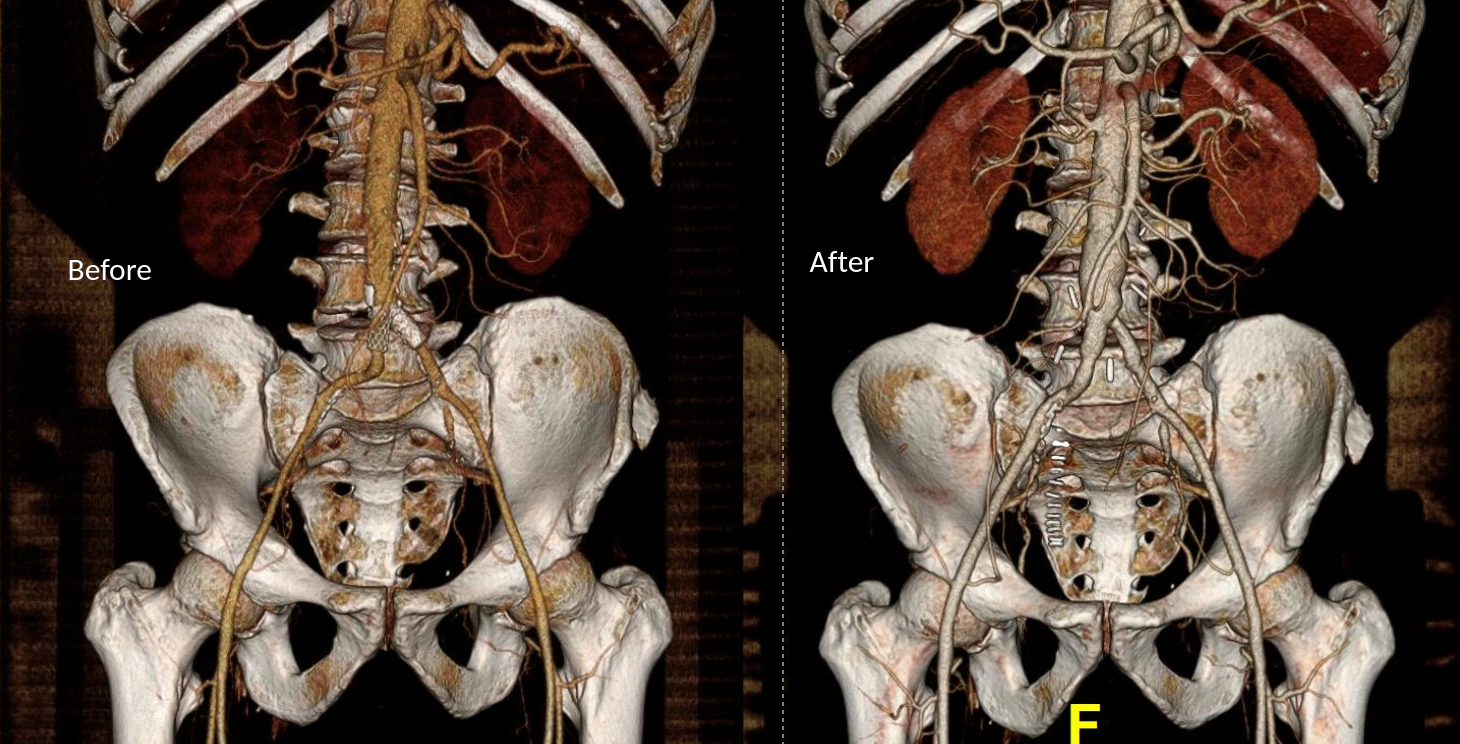
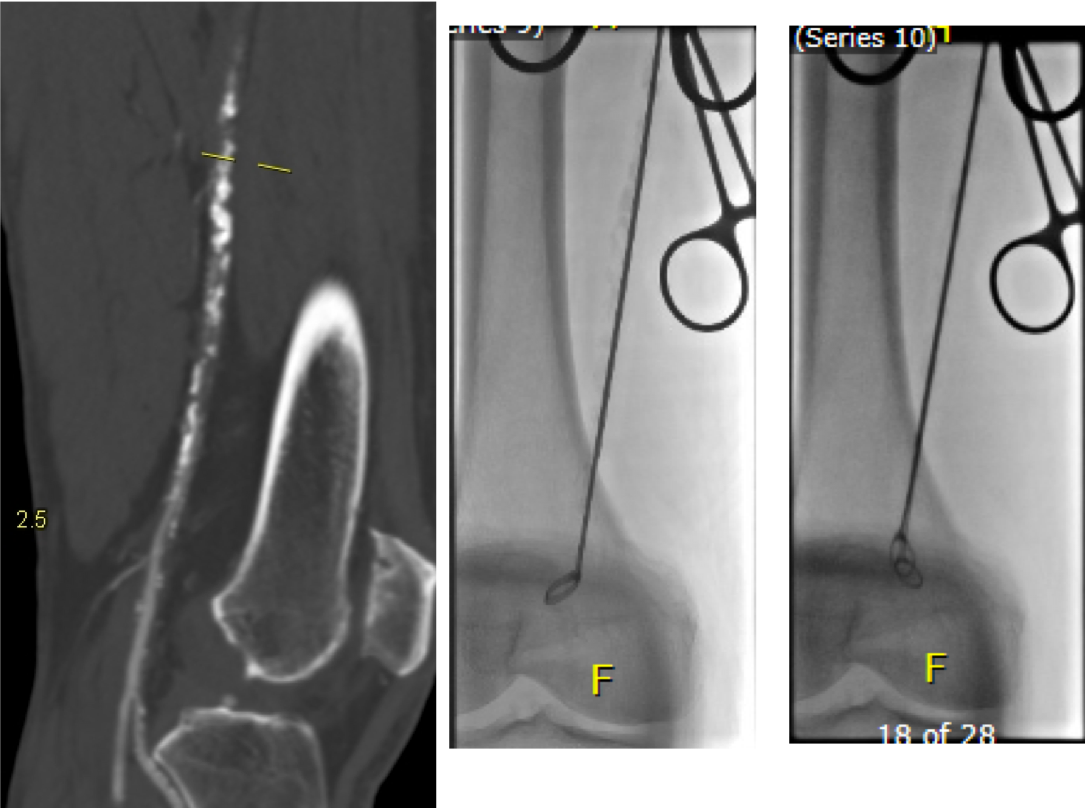
The patient is a fifty-something smoker who had a prior type B aortic dissection nearly a decade past who presented with substernal chest pain radiating to the back. He was found on CTA (figure below) to have a 6.5cm extant V TAAA starting above the diaphragm and ending at the level of the renal arteries.
Closer inspection revealed it to be aneurysmal degeneration of the aorta at a large false lumen fenestration. The aneurysm had grown eccentrically into the patient’s right chest and retroperitoneum. The remaining dissection above to the left subclavian artery and to the aortic bifurcation was chronic and thrombosed. His pain waxed and waned with hypertension which initially had to be controlled with parenteral agents. His cardiac workup revealed normal ejection fraction and valve function, and no critical coronary artery disease on coronary CTA. Pulmonary consultation deemed him a low pulmonary risk for major surgery. I offered him open repair, and initially the patient balked, asking for an endovascular repair, but I carefully walked him through the concepts, principles, and data guiding my recommendation. Yes, in a rupture, I have stented and followed with visceral debranching (link) and we have placed multiple snorkels in a very high risk octogenarian with a rupture, but who would offer endovascular repair to an otherwise good risk 50 year old?
The operation was initially planned in the standard way with cell salvage, plan for clamping in the transition point where the descending thoracic aorta took a rightward turn. The sequence of operation was for proximal anastomosis, right renal anastomosis, cooling the left kidney, celiac axis (CA), superior mesenteric artery (SMA), left kidney, and finally distal anastomosis with reimplantation of any prominent intercostal vessels. Preop imaging suggested the one at the T12 level was large. CT surgery was asked to be available for cardiopulmonary bypass via left atrium and femoral vein. Cardiac anesthesia and I had a discussion about intraoperative monitoring and management. Plans were made for CSF drainage -despite recent papers suggesting as much harm as benefit from these drains, I still feel critical time is lost if the patient is ventilated for a prolonged period postop and motor evoked potential monitoring is not available. The culture of CCAD mirrors that of Cleveland Clinic’s main campus in Ohio, and collaboration is ingrained. It was also serendipitous that one of the clinical associates, Dr. Niranjan Hiremath, had a particular interest and training in aortic surgery and suggested something amazing.
The Game is Changed
Dr. Hiremath trained in both vascular surgery and cardiothoracic surgery in Melbourne under Dr. Matalanis. Drs. Matalanis and Ch’ng published a series of 5 patients done with a separate branched bypass to the visceral vessels fed from the cardiopulmonary bypass circuit (reference). A separate aortic bypass was then performed and this truncal visceral graft was anastomosed to the main aortic graft. It was a visceral branch application of what is commonly done for the aortic arch great vessels. It was clear to me that this concept eliminated the need for desperate speed, and minimized clamp time to the 5-15 minutes required for each visceral branch anastomosis. A game changer.
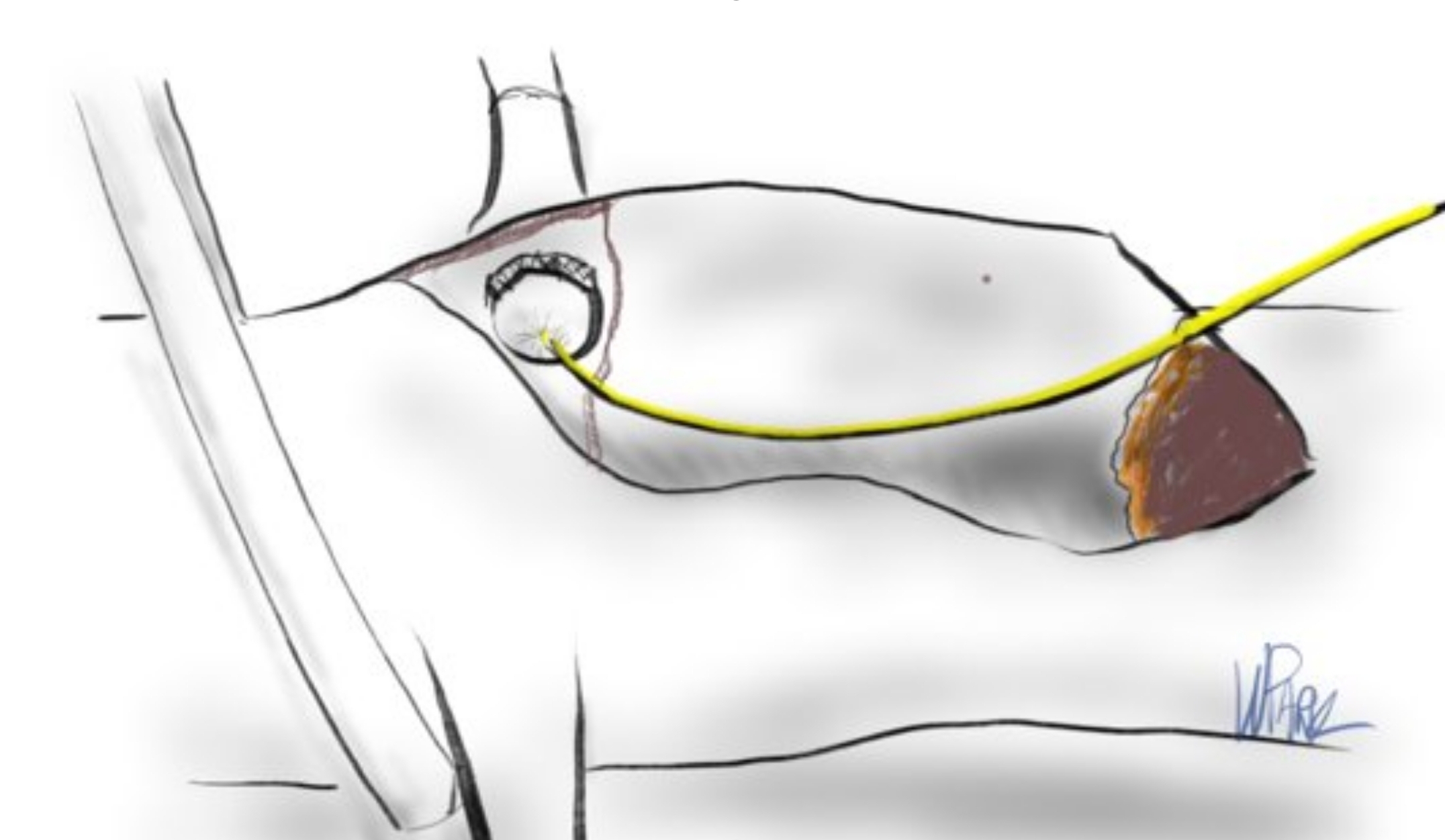
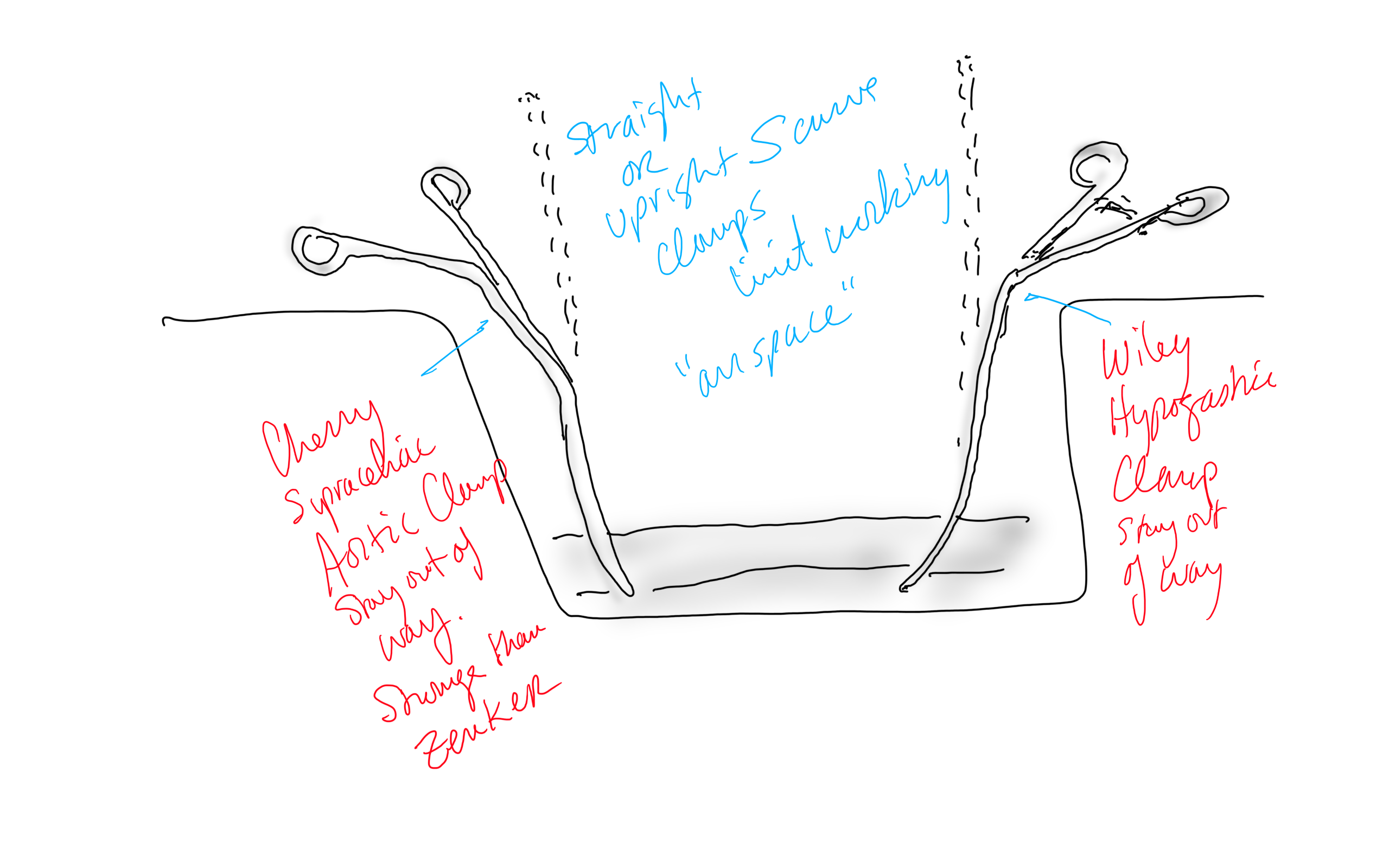
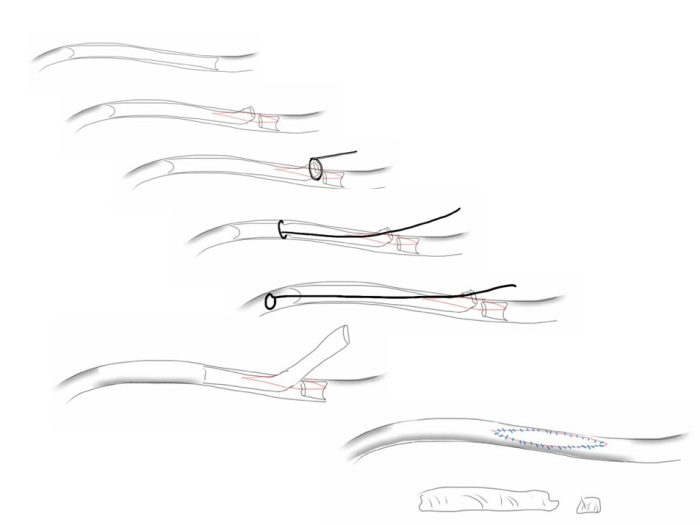
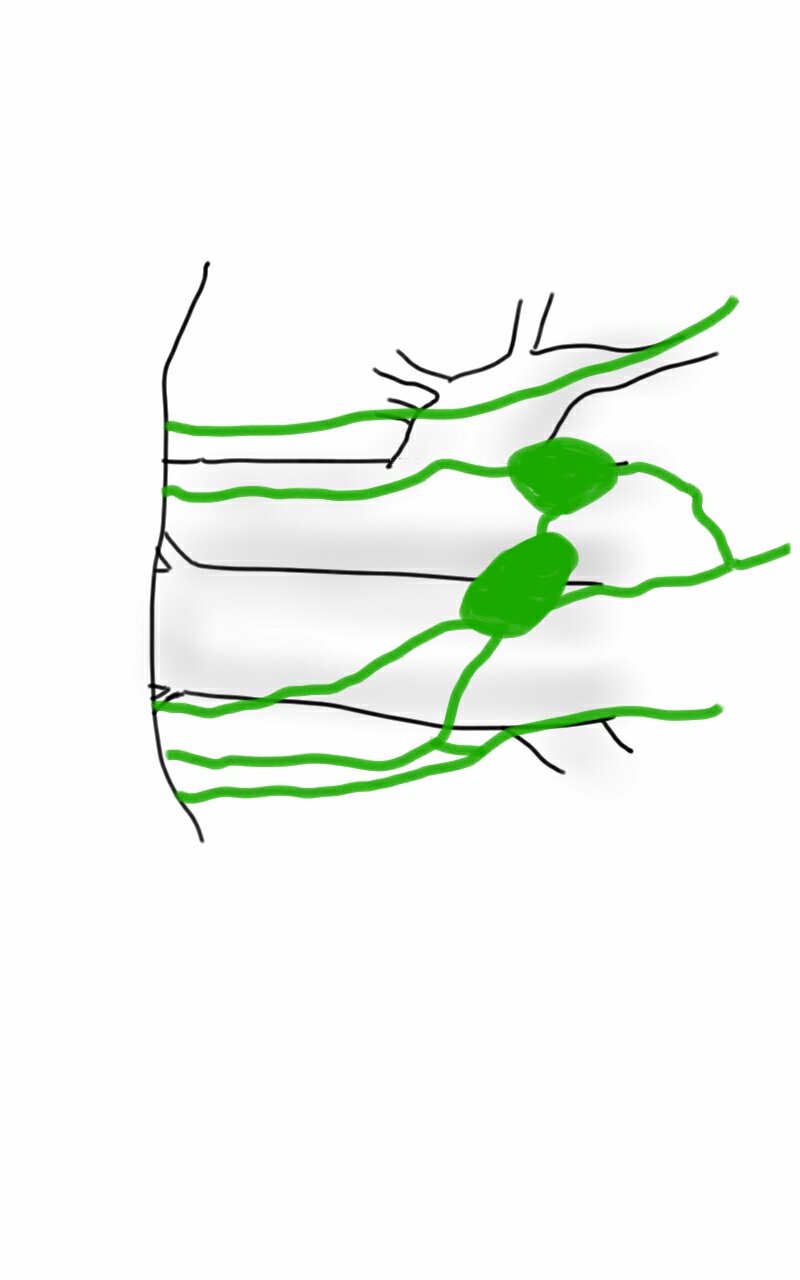
My process for incorporating new concepts to an operation requires comfort and familiarity. The familiarity with this modification had everything to do with my extensive use of shunts during peripheral bypass surgery. Placing the shunt into one of the renal branches of a 4 branch Coselli graft turns this graft into a live blood vessel. By fixing the proximal and distal ends of the graft in the correct orientation and position relative to the branches, each of the visceral branches could be anastomosed to the graft one at a time while the patient’s aorta remained unclamped. This is best described with the sketches I put together for the preop huddle (gif and figure below).


Even though I have done many of these operations, because of the smaller population at risk, thoracoabdominal aortic aneurysms are a relatively low frequency disease and no assumptions can be made. The fact was, it took very little convincing for me to understand this concept as a game changer, but I took the liberty of modifying it for the particular situation of the patient. Every operation is ultimately another quantum of experience for the people involved to take away priceless information for the next one which will always be unique. We must take these as opportunities for improvement. For once in a long time, I felt this would be a big improvement.
Day of Surgery
Our operations always start with a huddle, but this one was different because of the numbers of people involved. There were the cardiac anesthesiologists, some of the best I have ever worked with in my career led by Dr. Dominique Prudhomme. The cardiac surgeons, Dr. Tareq Aleneiti and Hiremath, who planted this idea, along with the perfusion team, cardiovascular nursing team, and my partner Dr. Younes walked through the steps of the operation with me, with bailout points and plans B and C (CPB with hypothermia and circulatory arrest as a last resort for any unforeseen uncontrollable bleeding). I felt like I was the ringleader in a heist movie, only in this case, rather than jewels, we were grabbing something actually priceless (figure 3).

The patient was placed in the right lateral decubitus position across the table break in the golf backswing position with pelvis relatively flat to the shoulders which were upright. The incision extended from the top of the sixth rib into the abdomen. This dissection is really two -the thoracotomy and separation of the peritoneum from the retroperitoneum linked by the takedown of the diaphragm and cutting of the costal margin. It is a tactile portion of the operation -only the hands really understand when to pull down and separate the two layers. The celiac and SMA are entangled in myenteric plexus which had to be cut to exposure sewable lengths of both. The left renal artery was also tricky in that the prior inflammation of the dissection resulted in stickiness of the tissues. It goes quickly and we have this exposure (figure 4).

Heparinized
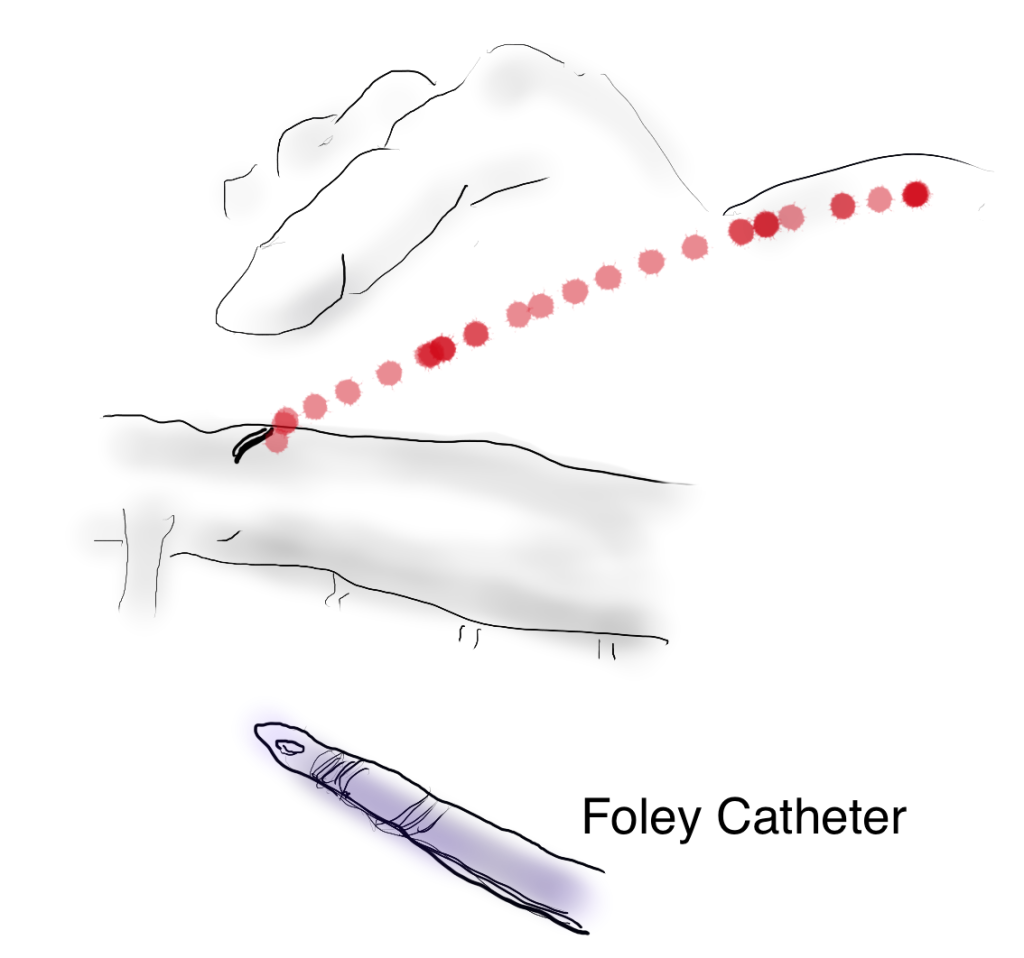
The patient is heparinized with a goal ACT around 250. Not enough for CPB, but good enough for rock and roll. The cardiac surgeons placed a cannula within a double ring of advential sutures, cinched with Rummel tourniquets and secured with an 0 silk tie -a maneuver I did many times myself during my cardiac rotations in residency. This was placed on a Y connector, one branch going to the CPB pump in case of a need to go to plan C, and the other to a tubing connector inserted into the right renal artery branch of the Coselli graft -a slight modification of the original plan (figure 5).
The other branches were simply clamped and the aortic ends of the graft were rolled up with a straight Kelly and secondarily clamped with aortic clamps -this gave weight to the ends letting them be positioned in a way that kept the branches oriented properly. There is need for precision and prediction as everything rotates back 45-90 degrees and the viscera sit on the grafts and the anastomoses. That is why keeping some length is crucial -this length accommodates this rotation. The Coselli graft is opened to systemic pressure by releasing the shunt. The proximal and distal ends of the main graft are twisted and double clamped to position the graft branches in the correct radial and z-axis orientation.
The aortic and branch exposure with takedown of the diaphragm is a standard exposure. One technical difference for this procedure is the need to expose about 2cm of the CA and SMA. Typically, only enough to clamp the vessel is necessary in standard surgery as these vessels are prepared with aortic buttons or anastomosed as an island patch. These vessels are surrounded by myenteric nerve plexus which feels like fascia or scar tissue but can be divide. Use of a hook cautery typically used in laparoscopic surgery along with a Ligasure speeds dissection.
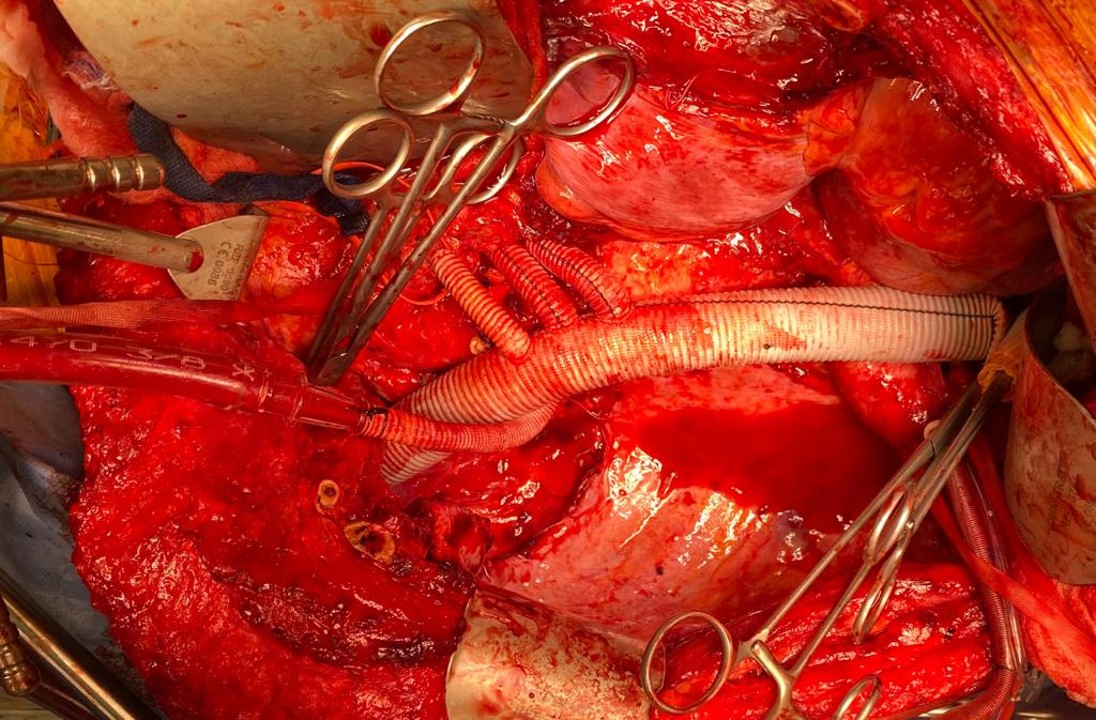
These arteries, starting with the left renal artery, are ligated at the origin and divided for end to end anastomoses to the Coselli graft branches. As these arteries are only briefly clamped for the anastomosis while the remainder are getting flow from the aorta or the shunted Coselli graft, visceral ischemia is minimized. I still chilled the kidneys with manual injections of cold Ringer’s Lactate via large syringes and Stoney injector tips. The final product is shown on figure 6.

The operation no longer felt like a sprint. The atmosphere was lively and relaxed -something that does not happen in these cases even at closing as exhausted residents or fellows focus on stitching together all the separated layers of the patient’s chest and abdomen. I played a soundtrack of classic Bollywood tracks, alternating between mellow and lively.
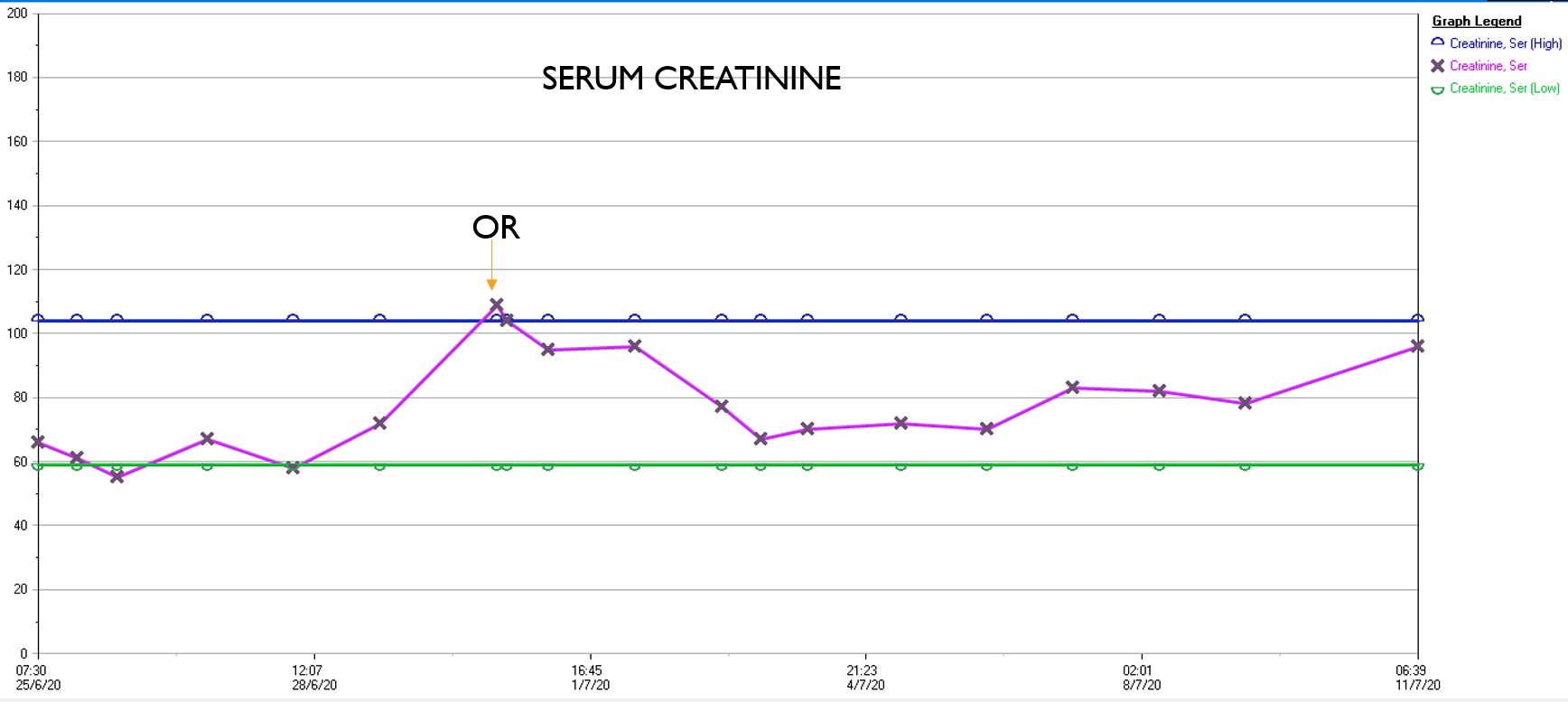
What was striking was the absence of the need for blood transfusion -about a liter and half ended up in the cell saver, and the patient received 2 units of plasma, out of tradition. The patient had a minimal brief plasma lactate elevation which did not persist. He was closed with a chest tube and brought to the cardiac intensive care unit, stable, not on pressors. He was extubated that night, and moved all of his limbs to command. The chest tube was removed on POD#2, and he left the unit to recuperate on the floor. Amazingly, his serum creatinine did not rise significantly. Prior to clamping he received the usual cocktail of mannitol but it was likely unnecessary. Most of these patients, even with revascularizing first after the proximal aortic anastomosis in the fastest of hands, there is at least 30 minutes of ischemia manifest postoperatively as a rise in the creatinine with recovery in most. This rise was brief and transient (graph).
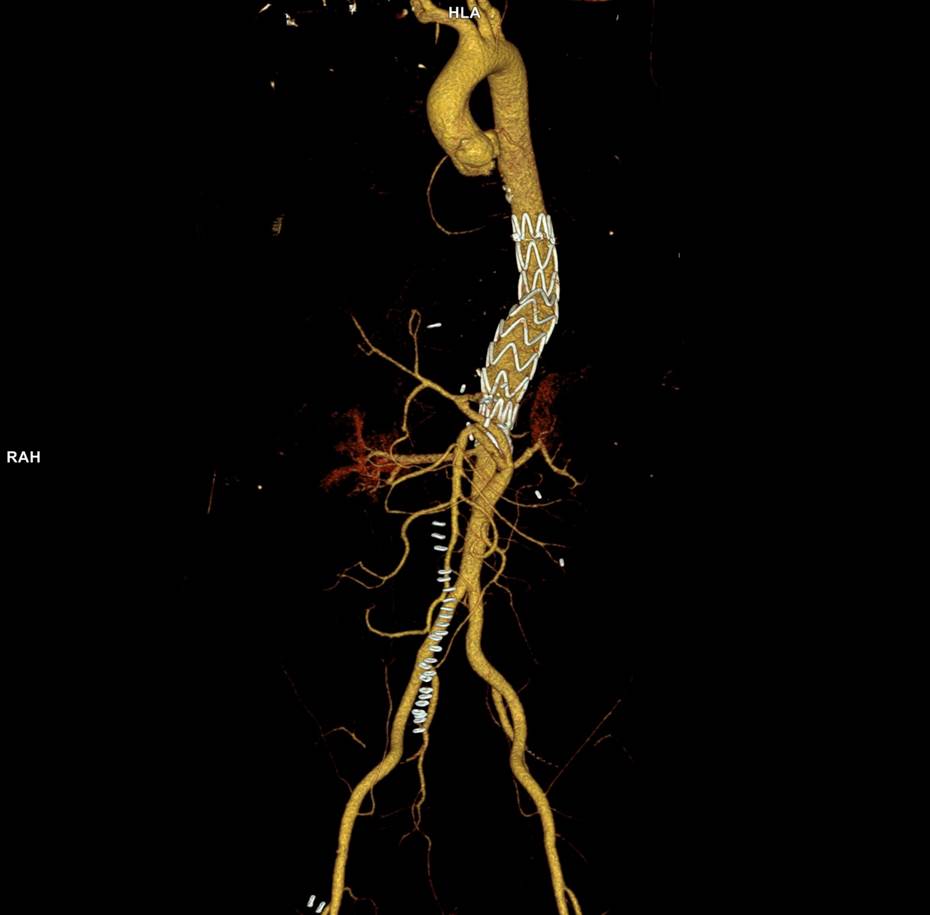
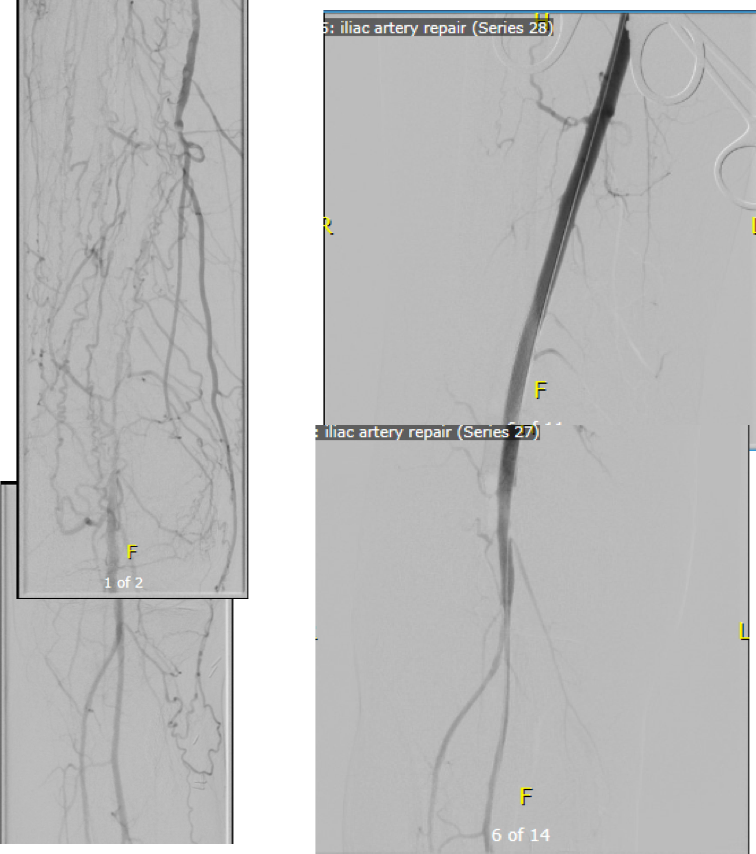
In the visceral circulation, the ischemia in the normal open repair is manifest postoperatively as systemic inflammation requiring pressors, persistent lactic acidosis, and coagulopathy, which at best is transient but at worst, fatal. This patient had no significant shift in any of these parameters. He had his CSF drain removed POD#2 after clamping for 24 hours, and was discharged home POD#11, having to recover from right chest atelectasis and a blood patch placed for persistent headache. CTA prior to discharge showed a good result. The left renal graft had been on stretch but was rendered redundant on repositioning of the viscera. No stenoses were noted.

Aftermath
Of course we are writing this case up, but case reports by their form cannot be overly enthusiastic whereas on my personal blog I can be excited. The normal course of postoperative recovery, the ebb and flow taught in surgical critical care books, is a result of ischemia, blood loss and replacement, fluid resuscitation, and cardiopulmonary support. Add to that cardiopulmonary bypass and you get an additional hurdle for the patient to recover from. This technique of shunting reminds me most of the temporary axillofemoral bypass. When I was a fellow at Mayo, I assisted Audra Noel in taking an elderly patient with a 25% ejection fraction through open aortic surgery with nearly miraculous recovery largely by avoiding the factors that trigger the ebb and flow. This technique is easier but mandates a strong normal segment of thoracic aorta to serve as inflow, otherwise an axillary artery will need to be cannulated.
Spinal cord protection is made easier with this technique by avoiding the massive fluid shifts, the pressors, and the acidosis in a typical thoracoabdominal aortic aneurysm repair. The blood pressure and cardiac output were never seriously perturbed. Several large intercostals and lumbar arteries were encountered and they backbled so avidly, after the short operation that I really felt there was no need to revascularize them. The spinal drain was kept open only for a day, and kept another day clamped to ensure that it would not be needed before removing it.
If you accept that spinal cord ischemia is multifactorial, we had avoided those factors. The absence of massive blood loss, negligible pressor use, no fluid shifts, minimal ischemia, no significant acidosis, no prolonged OR and clamp times, no blood transfusions, and the presence of avid back bleeding suggesting strong collateralization, compelled me to end the operation without revascularizing these intercostal vessels.
The patient recuperated for an ten days after his operation but was walking from postoperative day #1. He had atelectasis due to mucus plugging in his right lung base and was treated for aspiration, but clinically did not have a pneumonia and his atelectasis cleared with chest physiotherapy and nebulizers and was discharged home. Gratefully, he has given us permission to discuss and study his case.
There is no success in these cases without a team, and we are blessed with talented caregivers. This technique greatly reduces the physiologic impact of this surgery on the patient, reducing the injury to the equivalent of a broad sword cut from chest to abdomen that missed all the vital organs and vessels. In the right hands, this concept will broaden the appeal of open repair of these challenging aneurysms.
Reference
Matalanis G, Ch’ng SL. Semin Thoracic Surg 31:8:708-12.