

This patient had developed metachronous common iliac artery aneurysms after aorto-bi-iliac graft placement of a AAA a decade ago. This is not infrequent occurence in a significant number of patients with aneurysmal degeneration seen in the thoracic or visceral segment abdominal aorta, iliac arteries, and popliteal arteries, years after a primary AAA repair. The patients are often older than they were at the original repair, with concomitant risk factors, and so a minimally invasive option is preferred.
Right CIAA -vulnerable tissue

The teaching during my fellowship was that aorto-iliac bypasses for aneurysmal disease were to be taken to the iliac bifurcation to go around vulnerable tissues. These tissues vulnerable to aneurysmal degeneration were infrarenal aorta up to the renal artery origins, common iliac and internal iliac arteries, and popliteal arteries. An anastomosis to the iliac bifurcation however normal appearing may degenerate given enough time. This patient developed a saccular aneurysm on the right iliac bifurcation and a small internal iliac artery aneurysm (1.5cm).

This was treated with coil embolization and stent graft from the right iliac limb to the external iliac artery.

This is the standard endovascular therapy for common iliac artery aneurysms, and acceptable in the setting of unilateral disease, and in a staged fashion has been considered acceptable for bilateral disease, acknowledging there is a 10-40% incidence of buttock claudication and when the contralateral hypogastric is occluded or when the patient is diabetic, the risk of buttock or colorectal necrosis is not insignificant. The patient had transiently some buttock claudication and hip and thigh neuralgia with walking but this improved in the weeks leading up to treating his left common iliac artery aneurysm.
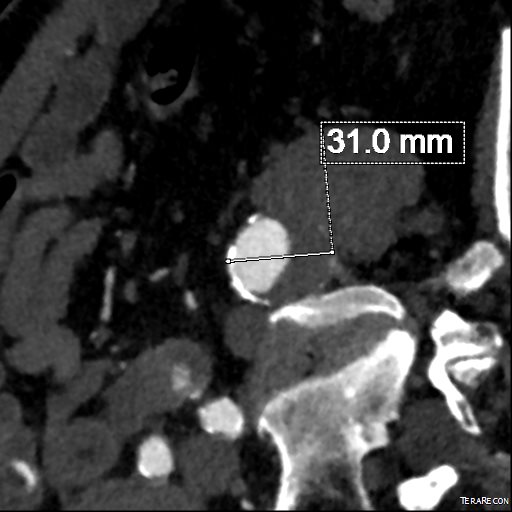
Left CIAA
The left common iliac artery bifurcation is sometimes challenging to access from a midline incision and exposure requiring a separate sigmoid mobilization. In men, the narrow pelvis can increase the challenge, so it is without fault that sometimes common iliac artery is left behind. This is what became aneurysmal, developing into a 3.0cm fusiform aneurysm beyond the left limb of the graft.
The internal iliac artery had a moderate 50-75% stenosis at its origin but was not aneurysmal, and I chose to revascularize this. The patient was sexually active and walked for exercise. My options included proceeding with left hypogastric embolization and stent grafting, mirroring the right but with a significant risk for buttock claudication, sexual dysfunction, and a small risk for colorectal ischemia. Other option is an external iliac or common femoral to internal iliac artery bypass which is an excellent option in good risk patients.
Endovascular options
Iliac branched stent grafts are undergoing trial. My center is participating in both available industrial FDA approval trials (disclosure, I am site PI for the Gore trial), but this patient’s presentation and anatomy exclude him from the trials. The final option is placing a parallel stent grafts -one to the internal iliac artery and the other to the external iliac artery from a large common iliac stent graft. While not ideal, until branched grafts become available, this remains a viable option. The principle is to size the grafts to minimize potential gutters between the grafts, and have long seal zones to minimize the impact of the gutters. Access from two points is required to get two grafts into position. With the acute angle of the aortobi-iliac graft, up and over access is generally not possible. The 10mm Viabahn graft that I chose to place in the hypogastric requires a 12Fr sheath, which cannot be placed from the brachial artery, so I prepped for an axillary cutdown. The left common femoral access was percutaneous.

The left CFA access allowed placement of a 16mmx10cm Excluder iliac graft limb to cover the aneurysm down to the iliac bifurcation. The left axillary arterial cutdown access allowed placement of a 12Fr sheath (Flexor) to allow access of the left internal iliac artery and safe delivery of a 10mm Viabahn stent graft. The left external iliac artery was sealed with a 13mm Viabahn stent graft that was deployed simultaneously. Ballooning was performed to both.
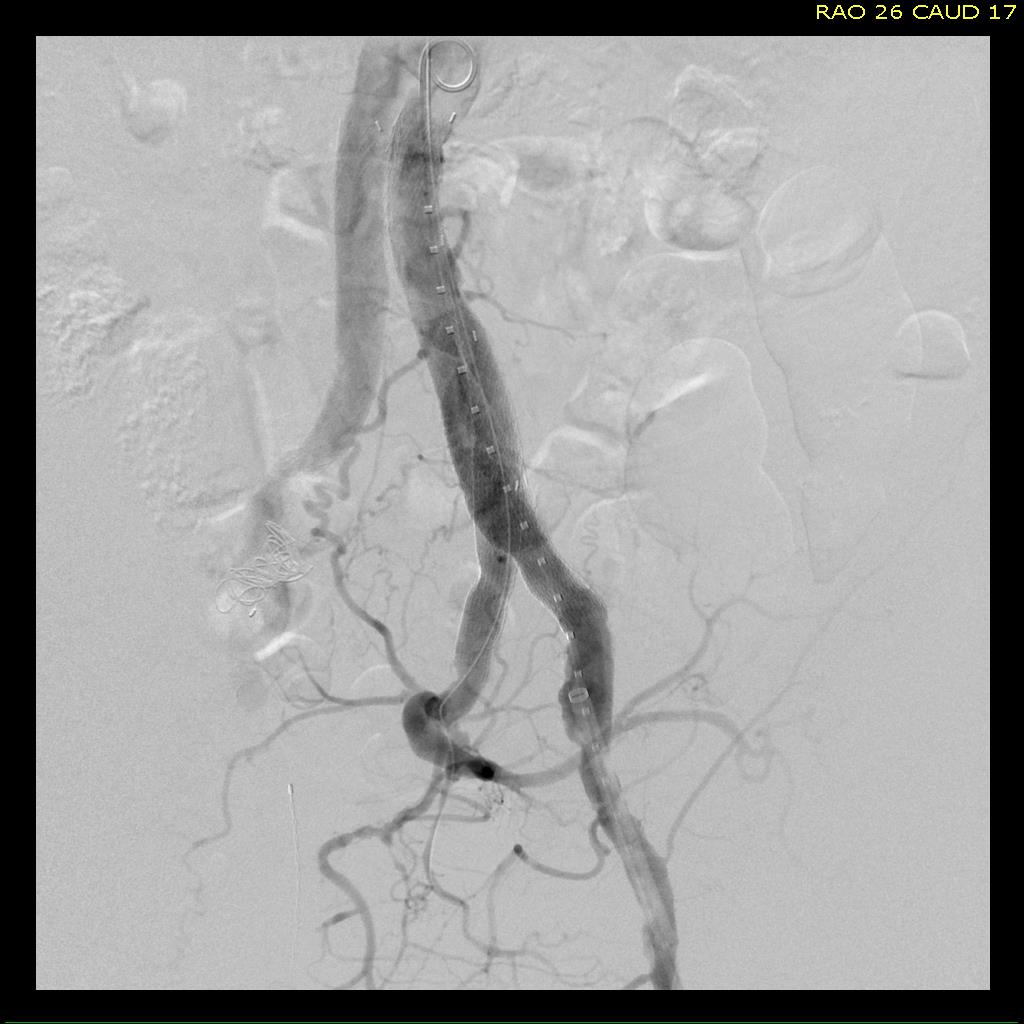
No leak was seen. The axillary access was repaired directly and the CFA access was repaired with two Perclose S devices.
Discussion
Despite initial acceptance of bilateral hypogastric occlusion, even staged, it can be the cause of significant disability aside from buttock claudication, which sometimes does not remit with exercise. Ischemia of the pelvis can drive a plexopathy that can result in motor and sensory neuropathy and disability. Death can occur. Preserving one of the hypogastrics can go a long way to preventing these complications, and everyone eagerly awaits adding iliac branched grafts to the armamentarium.
