This was presented at Dia De La Patología Aortíca Marbella organized by Dr. Fernando Gallardo.
Here is the link.
 A Surgeon's Notes
A Surgeon's NotesThis was presented at Dia De La Patología Aortíca Marbella organized by Dr. Fernando Gallardo.
Here is the link.

I recently had to remove a stent graft for infection and got to thinking about how the number of people who could comfortably and confidently manage that has thinned out in the world through the unintended consequence of the medical device market place. In every surgical specialty over the past twenty years, many open procedures were replaced with a minimally invasive option which generally involved adoption of new technology and large costs to the hospital. These newer procedures were touted as easier on the patient while being easier to perform for the average physician than the open procedure that they were replacing. That was the other selling point -that one could do several of these operations in the time it took one open procedure. In most cases, they were at best almost as good as the open procedure but at higher cost.
In the marketplace, minimally invasive always wins. In many specialties it became untenable to practice without marketing these “advanced minimally invasive” skills. Hence, the wide adoption of robotics in urology outside major academic centers -during those years of rapid adoption the surgeons would get flown to a course, work on an animal model, then for their first case a proctor would be flown out and voila -a minimally invasive specialist is born. The problem comes when learning these skills displaces the learning of traditional open surgical skills. In general surgery, it is not uncommon to hear of residents graduating without having ever having done an open cholecystectomy. It is also the case that many vascular trainees graduate with but a few if any open aortic cases. What happens when minimally invasive options run out? Who will do my carotid endarterectomy or open AAA repair?
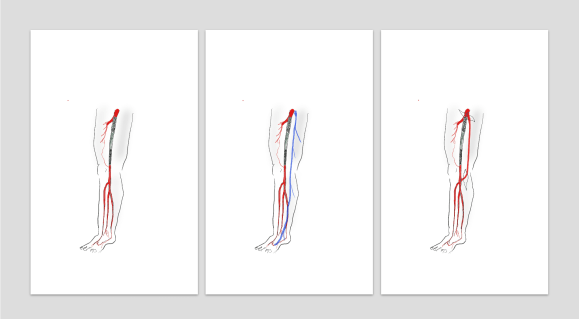
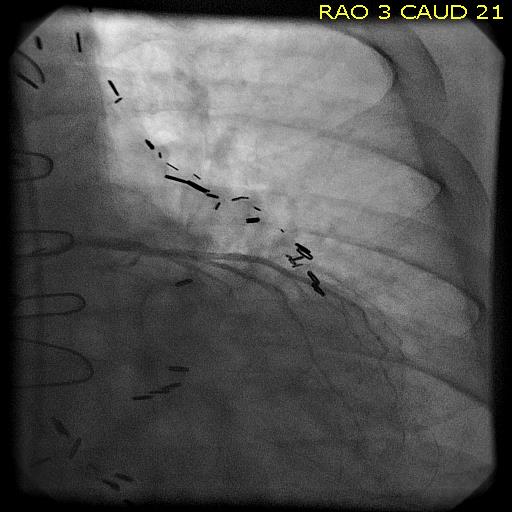
The first case is an elderly man with an enlarging AAA sac despite having had EVAR about seven years prior. No endoleak was demonstrated but the proximal seal was short on CT. Also, it was a first generation graft which is prone to “peek a boo” endoleaks from graft junctions and stent anchoring sutures. On that last point, I use the analogy of a patio umbrella -after seven seasons, they can leak where cloth is sewn to the metal struts. It is very hard to demonstrate leak of this kind on CTA or duplex ultrasound because they are small. The patient had his EVAR because he was considered high risk for open repair at the time of his operation -moderate COPD, mild cardiac dysfunction. His sac had enlarged to over 6cm in a short time, and therefore open conversion was undertaken. No clinical signs of infection were present. A retroperitoneal approach was undertaken. After clamps were positioned, the sac was opened.
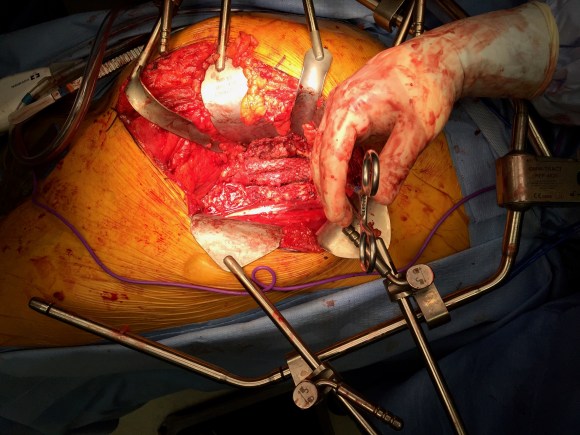
The picture does not show it, but a leak from the posterior proximal seal zone was seen with clamp off. The clamp was reapplied and the graft transected flush to the aortic neck. A bifurcated graft was sewn to this neck incorporating the main body stent graft and aortic neck in a generous running suture. The left iliac limb came out well and the new graft limb sewn to the iliac orifice, the right iliac limb was harder to clamp and therefore I clamped the stent graft and sewed the open graft to the stent graft.
The patient recovered well and went home within the week. He was relieved at no longer needing annual CT scans.
Who needs annual CT scans? Patients with metastatic cancer in remission.
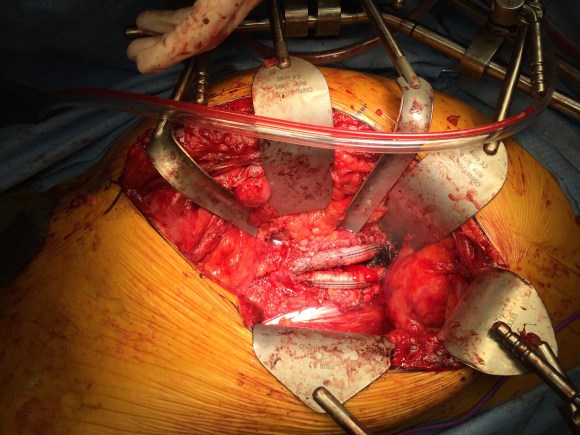
The second patient was an older man referred for enlarging AAA sac without visible endoleak. The aneurysm had grown over 7cm and was causing discomfort with bending forward. He too had been deemed high risk for open repair prior to his EVAR. If he had had an early generation Excluder graft, the possibility of ultrafiltration would be more likely and relining the graft would be reasonable (link). This was again a cloth and metal stent graft which can develop intermittent bleeding from graft to stent sutures, and I don’t think relining will help.
The patient was taken for open repair (above), and on opening the AAA sac, bleeding could be seen coming from the flow divider. It stopped with pressure, but I replaced the graft in a limited fashion from the neck to the iliac limbs as in the first case. This patient did very well and was discharged home under a week.
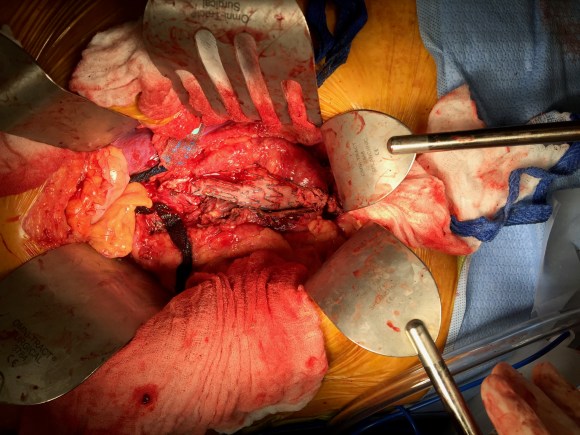
The third patient was another fellow referred from outside who had an EVAR for a very short and angulated neck, and a secondary procedure with an aortic extension in an attempt to seal the leak had been done. This failed to seal the type Ia leak. This patient too was deemed too high risk for open surgery of what was basically a juxtarenal AAA with very tortuous anatomy.
The patient was taken for open repair, and the stent grafts slid out easily (below).

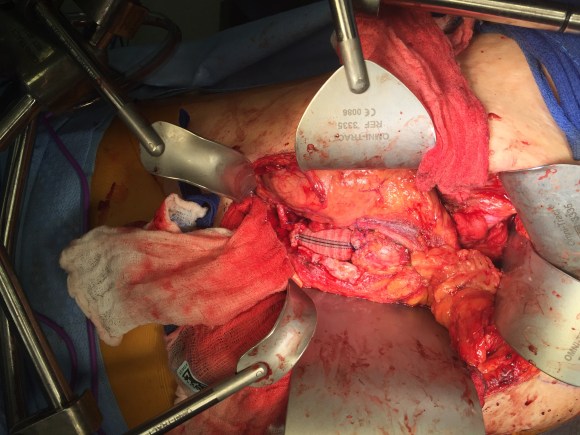
A tube graft was sewn to the short aortic neck and distally anastomosed to the main body of the stent graft -with pledgets because of the thin PTFE graft material in this particular graft. This patient did well and went home within a week.
All three cases are patients who were deemed originally too high risk for open repair, who underwent EVAR, then underwent explantation of their failing stent graft. Only one involved a patient whose graft was placed off the IFU (short angled neck), but the rationale was that he was too high risk.
What is high risk? In non-ruptured, non-infected explantation of failing stent graft, the mortality is 3% (ref 2) from an earlier series from Cleveland Clinic. With stent graft infection, the 30-day mortality of surgical management from a multi-institutional series was 11% (ref 3) when there was no rupture. From a Mayo Clinic series, stent graft resection for infection came with a 4% 30-day mortality (ref 4). These were nominally all high risk patients at the time of the original EVAR.
Real world risk is a range at the intersection of patient risk and the expertise of the operating room, critical care, and hospital floor teams. The constant factor is the surgeon.
Endografts for AAA disease (EVAR, endovascular aortic aneurysm repair), makes simple work of a traditionally complex operation, the open aortic aneurysm repair. The issue has been the cost and risks of long term followup as well as endograft failure and aneurysm rupture. The Instructions For Use on these devices recommend a preop, a followup 1 month, 6 month, and 12 month CTA (with contrast) and annual followup with CTA for life. These devices were meant to treat high risk patients but high risk patients with limited life spans do not benefit from EVAR (ref 1, EVAR-2 Trial). These have lead the NHS in the UK to propose that EVAR has no role in the elective repair of abdominal aortic aneurysms in their draft proposal for the NICE guidelines for management of AAA (link). While this is a critical discussion, it is a discussion that is coming at least ten years too late. A generation of surgeons have been brought up with endovascular repair, and to suddenly announce that they must become DeBakey’s, Wiley’s, Imperato’s, and Rutherford’s is wishful thinking at best or wilful rationing of services at worst.
In 2006, Guidant pacemakers were recalled because of a 1000 cases of possible capacitor failure out of 28,000 implants for a failure rate of 3.7% -there were 2 deaths for a fatality rate of 0.00007%. EVAR-1 Trial’s 8 year result (ref 5) reported 16 aneurysm related deaths out of 339 patients (1.3%) in the EVAR group compared to 3 aneurysm related deaths out of 333 patients (0.2%) in the OPEN group.
Academic medical centers, behemoths though they are, serve a critical function in that they are critical repositories of human capital. The elders of vascular surgery, that first and second generation of surgeons who trained and received board certification, are still there and serving a vital role in preserving open aortic surgery. My generation -the ones who trained in both open and endovascular, are still here, but market forces have pushed many of my colleagues into becoming pure endovascularists. The younger generation recognizes this and last year, I sat in on an open surgical technique course at the ESVS meeting in Lyons organized by Dr. Fernando Gallardo and colleagues. It was fully attended and wonderfully proctored by master surgeons. This is of critical importance and not a trivial matter. As in the 2000’s when endovascular training was offered as a postgraduate fellowship in centers of excellence, there is no doubt in my mind that today, exovascular fellowships need to be considered and planned and that current training must reinvigorate and reincorporate their open surgical components.
References
During our daily morning huddles, peopled by cardiologists and cardiac surgeons, one thing impresses me more than anything else. The assembled interventional cardiologists, world class and renown, they who can place a stent in any part of the body, will defer to the unassailable superiority of the LIMA to LAD bypass over any existing intervention. I am always a little sad that the analog for this, the vein bypass in the leg does not get the same love. The open surgical bypass of the leg is the great straw man at international symposia. It is fast becoming a diminishing and curious habit of a fading generation.
The acknowledged superior hemodynamics and patency of the bypass is diminished in the literature by pooling patency loss with other factors such as amputation, heart attacks, and death. Some vascular surgeons dogmatically cling to habits learned in training that favor complications, making themselves their own worst enemies both in the literature and in the marketplace. These bad habits involve long incision length, closure techniques that do not anticipate edema, and wound orientation that makes failure more likely.
Operations require far more support and resources to succeed than do interventions that soon go home. Brilliant operations alone will not heal the patient. It is pathways and postoperative care infrastructure and staff that prevent these secondary complications -the very complications that keep the leg vein bypass from being as respected, if not loved, as the LIMA to LAD.
The postoperative care of these patients devolves to management of leg edema. No medical or nursing school adequately teaches the basic science nor management of edema, which is the most common vascular condition
The incisions are too long in the classic vein bypass. When you create and then close an incision, the inflammation drives the accumulation of fluid in the extracellular space – creating edema. This postoperative edema, poorly managed, results in complications that leave the patient hobbled with time lost to healing wound complications, pain, and excess limb weight. Additionally, vein bypasses usually involve groin exposure and the delicate lymphatics that coalesce there are perturbed or destroyed during exposure. Postop, this damage and the inflammation rapidly overcomes the capacity of a lymphatic system. The traditional vein harvest also involves cutting through deep layers of fat. The fat is typically closed by broad sutures that create areas of fat necrosis -potential fodder for bacteria. The best ways the complications of long and deep incisions is to avoid them altogether. The calculus of the operative moment – “I must see the vein,” must include the vision of a patient losing months to wound therapies to heal a gaping, necrotic, infected wound. I recommend skip incisions or adopting in-situ bypass technique with endovascular management of fistulae. Or corral your cardiac PA to harvest the vein segment in the thigh after mobilizing the vein in the leg with the endoscope.
The incisions are often closed with Nylon sutures and skin clips which can become potential foci of infection. With edema, they create zones of ischemia around them, killing skin and creating entry points for skin flora as the skin expands under an unyielding clip or suture. Placed under a pannus, these sutures or clips fester in an anaerobic environment. Closure should adhere to anatomy. The body relies on connective tissue planes to keep itself together. In the groin, these are Scarpa’s layer and the dermis. They should be closed with absorbable monofilament in a buried interrupted fashion at the dermis with a final running subcuticular layer of 4-0 absorbable monofilament. Steristrips or glue at the skin finishes the job. If you use sutures, particularly at the distal anastomotic site, take care to realize that you have about 12 hours before the skin dies in the best of circumstances, and less with microangiopathy of diabetes and ESRD. Squeezing out the edema before closure with a sterile Esmarch or short counterincisions or even a large one to allow for tension free closure over an anastomosis will prevent wound complications over your graft.
The classic longitudinal groin incisions that cut across the inguinal crease divides a tension point -that crease is like a cord that supports the pannus that is slung over it and when divided and then closed with a stitch, that stitch then bears the weight of that pannus every time the patient sits up or stands. If you are observant, wound necrosis typically starts at the groin crease under a surgical clip or suture. Incisions in the groin should be obqlique and parallel to this crease, or if you can, even inside this crease. When these wounds are closed, the natural lines of tension are in line with the incision rather than orthogonal to it. The natural forces keep the wound shut.
This is only the first step. The next is keeping the wound clean and dry for at least 5 days. At the Mayo Clinic, where I trained, the nurses up on 5 Mary Brigh were trained to blow dry the groin wounds every few hours on cool setting and redressing the wound with dry gauze. You can get something close to it by ensuring the wounds painted with betadine, allowed to air dry, and dressed with dry gauze. If there is a constant leak of fluid, you have a serious problem as there is too much edema in the leg, or the wound isn’t closed, or there is a lymph leak. It needs to be actively dried out or you get a wet, macerated, infected wound like a grenade went off in the groin.

They don’t teach compression wrap techniques in medical or nursing school
The simplest thing to avoid lymph leaks is to not make them. Cutting near lymph nodes is hazardous, and once below Scarpa’s you have to orient your dissection directly over the femoral artery. Stray horizontally and you will undoubtedly cut one of the 4 to 10 invisible lymph channels.
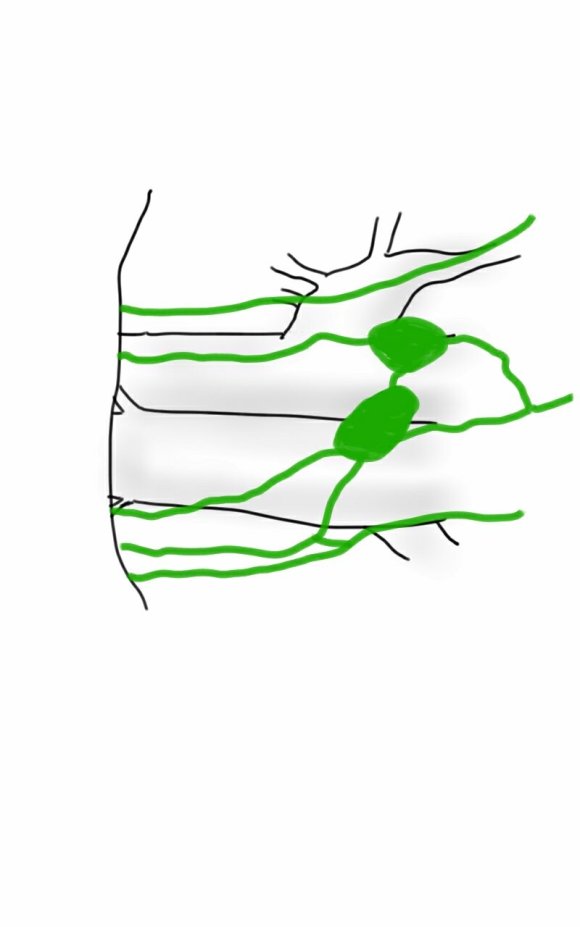
They are invisible but detectable -after you break them, you will see a constant wetness in the wound. Think about injecting a cc or two of Lymphazurin (Isosulfan Blue, for those not allergic to Sulfa) into the intertriginous space on the same foot and you will see the lymph channel in bright blue, or stare carefully at the likely spots for a lymph leak and clip it, burn it, Ligasure or Harmonic scalpel it.


So how did we get to a rather dry discussion about edema? Wound complications are tremendously debilitating and offset any benefit from vein bypass operations. These long incisions become terrible big wounds if not prevented. It takes the concerted effort of a team and particularly nursing in actively managing edema. And at the end, the patient too must be included in this discussion. For the vein bypass of the leg to get the same respect and love as the LIMA to LAD bypass, surgical wound complications must become never events.
Something that I recently promised Dr. James S.T. Yao, I will be working to publish on my stent removal and extended remote endarterectomy cases and techniques. Meanwhile, here is a talk.

Case Report
Patient is a 43 year old woman who had been having bouts of severe left sided abdominal pain for several years with worsening episodes of nausea and vomiting resulting in several visits to the emergency room. She has also had microscopic hematuria. Gastrointestinal workup including gastric emptying study, esophagogastroduodenoscopy and colonoscopy were negative, as was a workup for kidney stones. Eventually she was referred to my clinic for management of nutcracker syndrome. She denied lower abdominal pain nor excessive menstrual bleeding.
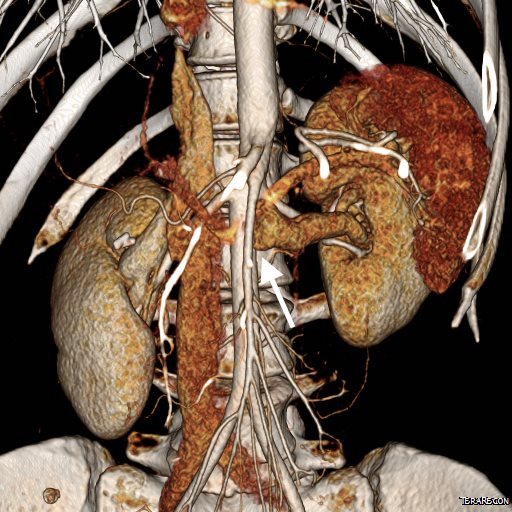
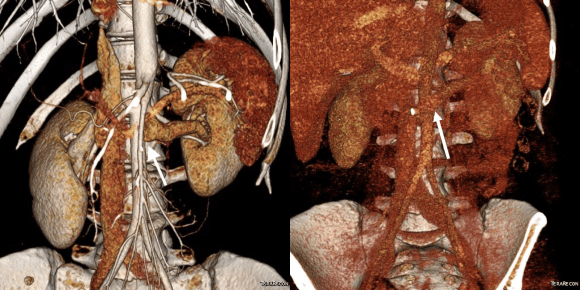
On examination, she was tender over the left kidney and flank. Laboratory examination was positive for microscopic hematuria. CT venography (below) showed an obstruction of her left renal vein by the superior mesenteric artery. Drainage via gonadal vein was not demonstrated, and no pelvic varices or complex of retroperitoneal veins was apparent.
Duplex showed the narrowing in the left renal vein and spectral Doppler showed elevated velocities across the compression caused by the superior mesenteric artery (below). The collecting system was not obstructed.


Treatment options included endovascularization with a large stent in the left renal vein, left renal vein transposition to a lower position on the inferior vena cava, left renal autotransplantation, and left nephrectomy. Stent placement comes with a degree of risk for cardiopulmonary embolism which may require a sternotomy to fish out an errant stent. The risk for this in the US is because the largest nitinol stents available are 14mm in diameter which might result in undersizing in a vein that could easily dilate to well over 20mm. Larger nitinol stents for venous applications are available in Europe but currently are not approved in the US (yet). Wall stents, while certainly wide enough, have the problem of being long and stiff when not fully deployed. A 22×35 Wall stent may be 50mm long if deployed inadvertently into a tributary vein or contrained at the narrowing. Because it slides easily, passing balloons in or out can cause it to slip out of position. Because this stent elongates when compressed and packed, deployment is challenging and it is prone to “watermelon seeding,” a set up for embolism. It does have the virtue of easy reconstraining.
My friend and recent host for Midwest Vascular Surgery Society Travelling Fellowship, Dr. John V. White, in Chicago, seems to have solved this problem by a multistep process of predeploying a temporary suprarenal IVC filter, deploying a stent (whatever fits), leaving the filter as a protection against stent migration for 4 weeks until the stent permanently seats itself through scarring/intimal ingrowth, then removing the filter.
I chose to perform venography and renal vein transposition. The patient was placed in a supine position on a hybrid angiographic operating room table and her right femoral vein was accessed. She was placed in 15 degrees reverse Trendelenberg which is about the upper limit possible. Venography below.

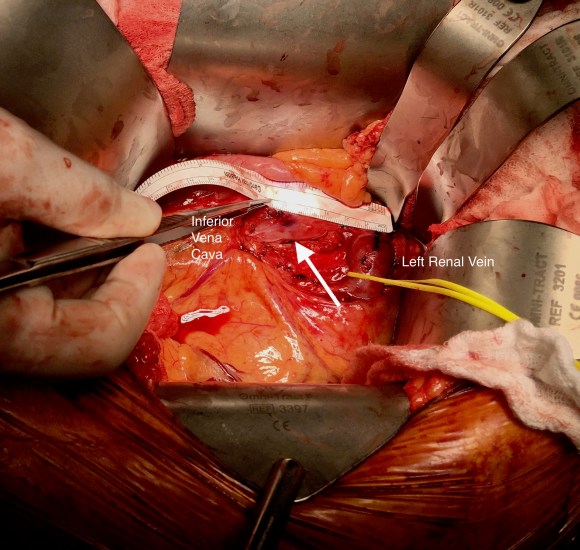
After heparinizing and clamping, the renal tributary was taken with a 5mm cuff –this would ensure proper length without narrowing the IVC.

The vein was anastomosed and flow was excellent by pulse Doppler.

She recovered well but had a longer stay because of an ileus, being discharged on day 5. Because she lived at a distance, and came back for followup the following week prior to boarding a plane for home. She no longer had the left sided abdominal pain and there was no hematuria. CT showed excellent drainage through the transposed vein.
Followup will be periodic (6 monthly) renal venous duplex from home. Given that there was minimal tension on the repair, I expect this to do well.
Discussion:
Nutcracker syndrome is one of the many unfortunate consequences of our bipedal lifestyle. The small intestines hang like baggy sausages off the branched stems of the superior mesenteric artery (SMA), and in some individuals, the SMA compresses the left renal vein against the aorta. The left renal vein receives up to 12-15% of cardiac output via the left kidney, and with outflow obstruction, drains the blood through small collaterals. The renal venous hypertension results in swelling of the left kidney with subsequent left renal colic -with flank and abdominal pain, nausea, and vomiting. There is hematuria which can be gross or microscopic. With drainage via an incompetent gonadal vein, varicoceles can occur with discomfort in men and pelvic varices with pelvic congestion syndrome can occur in women.
Diagnosis is challenging because it is one of the relatively rare non-gastrointestinal causes of abdominal pain (table).
A history of left sided abdominal pain, flank pain, nausea, vomiting, associated pelvic pain, and episodes of hematuria are diagnostic. Examination is typically positive for left renal tenderness and flank tenderness. Laboratory examination include urinalysis for hematuria. Duplex, while technically challenging, will show renal venous compression with velocity elevation or loss of respirophasicity, CTA will typically show obstruction of the left renal vein with filling of collaterals, as will MRV.
Venography should be done in a stepwise manner (White protocol) to fully demonstrate the maldistribution of blood. That is the key word, maldistribution. I learned from my fellowship with Dr. White that performing venography in as upright a position as possible recreated the pathophysiology, the physics, particularly for pelvic congestion and nutcracker. Remember, this is a disease of bipedalism, of upright posture. Many negative studies done supine become positive, as the contrast will fall to where it prefers to go. As I have stated in the past, on the venous side, demonstrating drainage has different imaging needs than demonstrating flow. Pathologic venous drainage has three characteristics:
While pressure gradients are nice if they are large, they are difficult to assess when they narrow to 1-2mmHg, particularly if they vary with cardiac cycle and respiration. Because we are assessing drainage, the distribution of contrast and the direction it goes is particularly important, and far more sensitive than pressure measurements.
Venography was done per a modification of Dr. White’s protocol for pelvic congestion:
I have started transposing gonadal veins when they have enlarged from chronic reflux (link, ref 2). Renal vein transposition was chosen because her ovarian vein was competent and too small to transpose (ref 1-3). While the patency rate of stents in veins seems to be acceptable, long term data is unavailable. Also, venographic appearances are deceiving -see the in-vivo measurement of the left renal vein after dissection:

References:
A case report co-authored by my recently graduated trainees, Drs. Roy Miler and Eric Shang. An update to be presented at Midwest Vascular Surgery Society Meeting in Chicago.

History
The patient is an 80 year old woman with lung cancer who was getting a port placed at her home institution. It was to be a left subclavian venous port, but when access was not gained, a left internal jugular venous port was attempted, but after the intitial stick and sheath placement, pulsatile bleeding was recognized and the sheath removed. Hemostasis was achieved with clips and the wound closed and a right internal jugular venous port was placed. The postprocedural CXR shown above showed tracheal deviation and numerous clips from the initial port placement attempt, and a CT scan with contrast (unavailable) showed a carotid pseudoaneurysm of 3cm projecting posteriorly behind the pharynx/esophagus. She was kept intubated and sedated, and transferred for management.
On examination, her vital signs were stable. She had 2cm of tracheal deviation and swelling was apparent at the base of the neck. While my trainees may be better versed at this than I at the particulars of this, my old general surgery trauma training kicked in, as she had a Zone I neck carotid injury,  which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
Open Repair
Open repair is the approach of choice for zone 2 injuries because aerodigestive tract injuries can also be addressed and the exposure is straightforward. For Zone 1 injury, the exposure is potentially possible from a neck exposure, but in my experience, jumping into these without prepping for a sternotomy puts you into a situation without a plan B. The exposure of the carotid artery at this level becomes challenging with hemorrage from the artery once the compression from the hematoma or pseudoaneurysm is released. A sternotomy in this elderly woman, while not optimal, may be necessary if open control is required, but the best plan is to avoid this.
Endovascular Options
This should be a straightforward repair from an endovascular approach, even with the larger sheath required for the covered stents. A purely endovascular approach is problematic for two reasons. One, cerebral protection devices are built for bare carotid stents and not peripheral stent grafts, but this is not prohibitive -it should be fine. Without a planned drainage, the hematoma would be left behind which could cause prolonged intubation and problems with swallowing -both an issue for an elderly patient battling lung cancer. Endovascular access could provide proximal control for an open attempt from above, but instrumenting from the arch in an 80 year old has a known 0.5-1% stroke rate.
Hybrid Repair
A hybrid open approach with exposure at the carotid bifurcation offers several advantages. With control of the internal carotid artery, cerebral protection is assured while the carotid artery is manipulated. At the end of the procedure, the internal carotid can be backbled through the access site with the common carotid artery clamped. The hematoma could be avoided until the stent graft is deployed. An unprotected maniplation in the arch can be avoided. Once the stent graft is deployed, drainage of the hematoma can be performed.
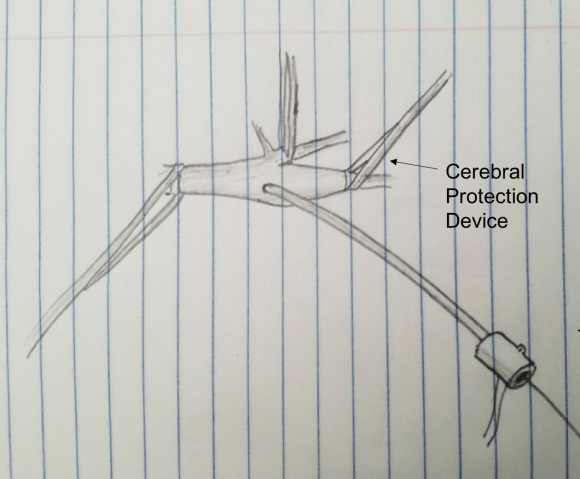
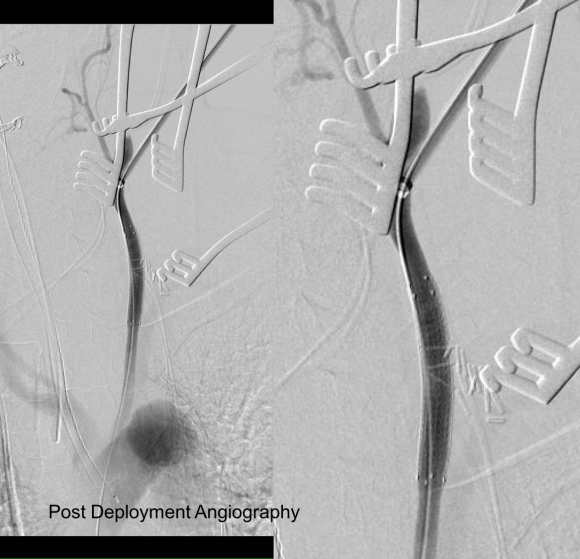
This required setting up a table off the patient’s left that allowed the wire to lie flat to be manipulated by my right hand. The carotid bifurcation was accessed through a small oblique skin line incision and the common, internal, and external carotid arteries, which were relatively atherosclerosis free, were controlled with vessel loops. The patient was heparinized. The internal carotid was occluded with the loop, and the common carotid below the bifurcation was accessed and an 8F sheath with a marker tip inserted over wire. Arteriography showed the injury and pseudoaneurysm.

The location of the injury based on CT and on this angio would have baited a younger me into directly exposing it, but experience has taught me that which occasionally you can get away with it, the downsides -massive hemorrhage, stroke, need for sternotomy, just aren’t worth it. The sheath was brought across the injury and a Viabahn stent graft was deployed across the injury.
The hemorrhage was controlled and the hematoma was then exposed and drained -the cavity was relatively small and accepted the tip of a Yankauer suction easily. A Jackson-Pratt drain was placed. The access site was repaired after flushing and retrograde venting as described.
She recovered rapidly after extubation postop. She was able to breath and swallow without difficulty and had suffered neither stroke nor cranial nerve injury. The drain was removed on postop day 2.
The patient recently returned for a 6 month followup. Duplex showed wide patency of her stent.

More gratifyingly, her port was removed as her cancer was controlled with an oral regimen.
Discussion
Let me start with my bias that all penetrating trauma should be approached in a hybrid endovascular OR. It is a natural setting for trauma and this case illustrates that. In a hybrid operating room, central aortic and venous injuries can be controlled endovascularly while open repair, including salvage packing, can be done. Excess morbidity of central vascular exposures can be avoided. Temporary IVC filters can be placed if indicated (becoming rarer and rarer). Cardiopulmonary bypass can be started.
In this patient, hybrid therapy brought the best of both techniques and avoided many of the pitfalls of the purely open or endovascular approach. For stable zone I penetrating injuries of the neck, it is clear that this is a reasonable approach.

The principles of salvage are in rescuing valuable undamaged goods in the setting of catastrophe. This guided me when a patient was flown in from an outside institution to our ICU with a saline soaked OR towel in his right groin -he had had an aorto-bifemoral bypass for aorto-iliac occlusive disease a year prior, but had never properly healed his right groin wound which continued to drain despite VAC therapy and wound care. On revealing his groin, this is what I saw:

A CT scan was sent with the patient but has been lost to time, and it showed a patent aorto-bifemoral bypass send flow around an occluded distal aorta and iliac arteries. The graft did not have a telltale haze around it nor a dark halo of fluid which signaled to me that it was likely well incorporated and only sick in the exposed part. The patient was not septic, but had grown MRSA from the wound which was granulating from the extensive wound care that had been delivered.
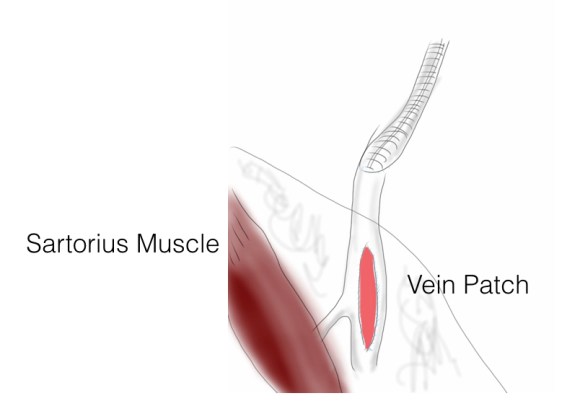
I felt that it would be possible to move his anastomosis point more proximally on the external iliac in a sterile field (figure above), and then close, then endarterectomize the occluded external iliac artery after removing the distal graft, then after vein patching, cover the repair with a sartorius muscle flap. It would salvage the remaining graft and avoid a much larger, more intense operation which was plan B. To prepare for that, I had his deep femoral veins mapped.
The patient was prepped and draped, the groin was excluded by placing a lap pad soaked in peroxide/betadine/saline solution (recipe for “brown bubbly” liter saline, a bottle of peroxide, a bottle of betadine), and covering with an adesive drape. The rest of the abdomen was then draped with a second large adhesive drape. A retroperitoneal (transplant-type) right lower quadrant incision was made (below) and the external iliac artery and graft were exposed. As predicted on CT, the graft was well incorporated.

The external iliac artery was opened and focally endarterectomized of occlusive plaque (image below). The adventitia had good quality despite the longstanding occlusion.

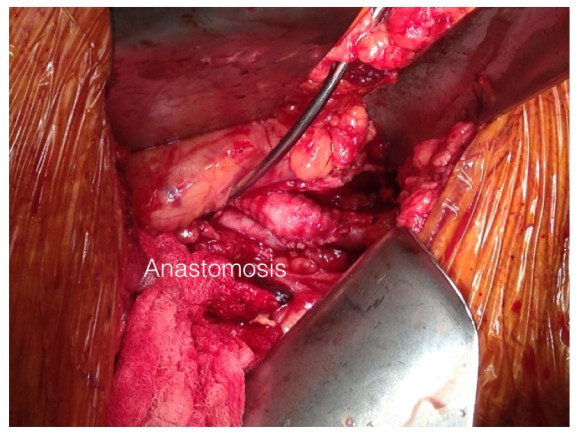
The graft was mobilized and transected and anastomosed end to side to this segment of artery (below). Dissecting was made difficult by how well incorporated it was.
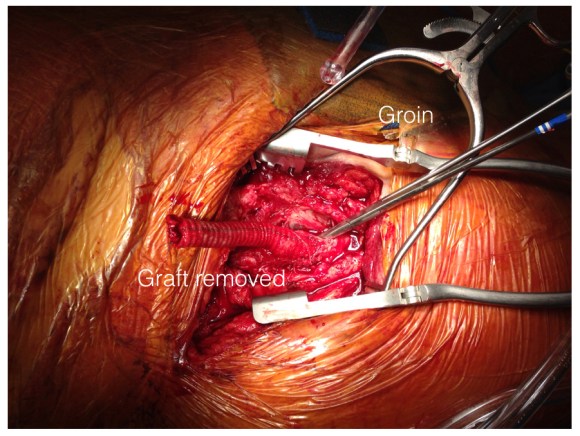
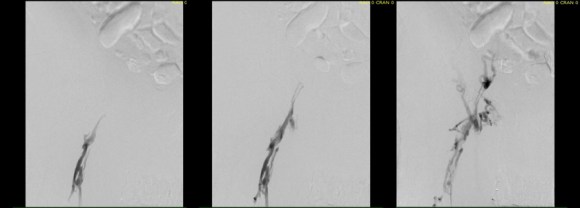
The wound was irrigated (with brown bubbly) and closed, dressed, and sealed over with the adhesive drape. The groin wound was then revealed and the graft pulled out (below).
Remote endarterectomy using a Vollmer ring was used -in this case I didn’t use fluoroscopy given the short distance to the terminus of the plaque which i had mobilized in the pelvis.

The plaque came out easily and was not infected appearing. It is shown below ex vivo.

A segment of saphenous vein was harvested from the patient medially and the arteriotomy was patched. The sartorius muscle was mobilized and applied as a flap over this. The wound was irrigated with brown bubbly and packed open with the intention of VAC application.
The patient healed very rapidly and remains infection free. I had used this approach on several occasions in the past and twice more recently. It truly is salvage as it preserves the uninfected graft while never exposing it to the infection in the process of operating. It avoids having to remove the whole graft which then damages the left side -I have seen other surgeons take this approach elsewhere taking a all-or-nothing approach to graft infection to considerable morbidity to the patient. It avoids having to harvest deep femoral vein -another large operation to which the body responds truculently. The patient recently came by for his 4 year followup, still smoking, but legs preserved.
Followup At 4 Years

The patient came back in followup -it has been 4 years since his infection was repaired. He was complaining of short distance claudication. His wound healed well and remains closed. CTA shows along with his short segment SFA occlusion which we will treat, a widely patent R. EIA (below).

The remote endarterectomy of the external iliac artery remains patent. Compare this to the preop CTA which I found and wasn’t available when I posted this case originally:
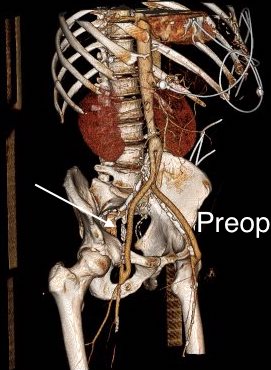
The chronically occluded EIA can be readily seen. The artery shown in the current CTA is that recanalized artery.

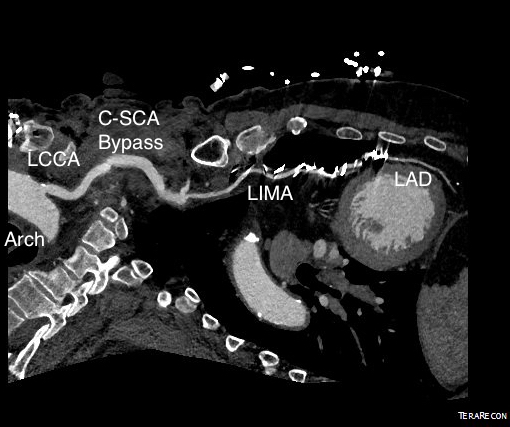
Patient is a 77 year old man with history of HTN, hyperlipidemia, former smoking, and CAD with CABGx5 and bilateral lower extremity bypasses who developed unstable angina consisting of neck and throat pain. He underwent catheterization at an outside hospital and found to have 100% LAD occlusion, a diseased, small patent left main and left circumflex (the profunda femoral artery of the heart!), 100% RCA occlusion, a patent but diseased SVG to distal RCA, and a patent LIMA graft to distal LAD but with severe plaque and near occlusion of his proximal left subclavian artery.

He had an NSTEMI. His vitals signs stabilized in the coronary care unit and he was sent to a telemetry floor. Whenever he walked, he would get the jaw pain, and this would also occur sporadically while recumbent.
On examination, he had no left brachial pulse, only a monophonic signal there, and bounding femoral pulses where there were the origins of bilateral femoral-tibial bypasses. His radial artery pulse was diminished on the right and absent on the left. Both saphenous veins had been harvested as were arm veins for the left leg bypass.
CTA shows the left subclavian artery to be occluded at its origin.


Cardiac surgery, interventional cardiology, and vascular surgery were called in for consultation. Cardiology consultation (Drs. Kapadia and Shisheboor) felt, and I agreed, that the left subclavian lesion was a poor candidate for recanalization and stenting. CT Surgery (Dr. Faisal Bakaeen) and I had a long discussion regarding alternate conduits, as he had unknown radial but likely radial artery disease, and had all usable veins previously harvested. I brought up a free RIMA graft -I had worked with Dr. Daniel Swistel, in NYC as a resident, who was Dr. George Green’s protege, and as a medical student at P&S I scrubbed Dr. Green’s final cardiac case. He routinely performed bilateral ITA bypasses decades before all-arterial revascularizations were routine. I get enthusiastic talking about cardiac disease! Walking through all the options -does anyone use deep femoral vein as coronary bypass conduit -we agreed ultimately that the best option would be a carotid-subclavian bypass with plenty of backup.

At its heart, it would be this vascular surgeon’s attempt at an off-pump single vessel CABG (above). Preparations were made with cardiac anesthesia and cardiac surgery to place an IABP (intra-aortic balloon pump) if he became unstable. For my part, the operation was straightforward, but I was going to have to go about it efficiently. I also figured that with a clamp beyond the LIMA takeoff, no significant change would occur to the coronary flow from the LIMA graft. So I hoped as I worked very deliberately. We kept him on the hypertensive side during the case.
The operation went well. The patient’s angina resolved and a followup CT showed the patent bypass feeding the LIMA and LAD.

His resting angina resolved. He followed up a month later and was very pleased. Moreover, he had a brachial and radial artery pulse and a general weakness of the left arm that he never complained about before lifted.
Discussion
The carotid subclavian bypass is something that really needs to be in the armamentarium of a modern vascular surgeon. Though out of print, Wylie’s Atlas (the unabridged, multivolume version) is available used through online sellers, and is useful for elucidating the anatomy which boils down to avoiding cutting the important structures -the phrenic nerve, the vagus nerve, the brachial plexus, branches of the subclavian including the vertebral artery, while cutting away muscles -lateral head of sternocleidomastoid, any part of the omohyoid, the anterior scalene muscle. And dividing the lymphatic duct if encountered. And tunneling under the jugular vein. And minding the buttery fragility of the SCA. The best technical paper out there is by Dr. Mark Morasch and it mostly deals with carotid-subclavian transposition (reference 1) but has excellent figures on bypass as well. I do both transposition and bypass, but for brevity, I prefer bypass.
This is not a unique problem, having been reported in the literature. An unusual variant of this is coronary sbuclavian steal syndrome (reference 2), which refers to reversal of flow in the LIMA bypass in the setting of subclavian artery occlusion and left arm exertion -which was not the case here, but interesting enough to mention. Here, it was a straightforward case of managing the hemodynamics. The key point of operating on such a patient was having the surety of quick response in the case of ischemic heart failure -we operated in the cardiovascular operating rooms with rows of perfusion pumps and balloon pumps and VADs and ECMOs at the ready. Indeed, this result could not have been so straightforward and routine seeming without the combined effort and experience of the whole Heart and Vascular Institute from nursing to consultant staff.
Reference

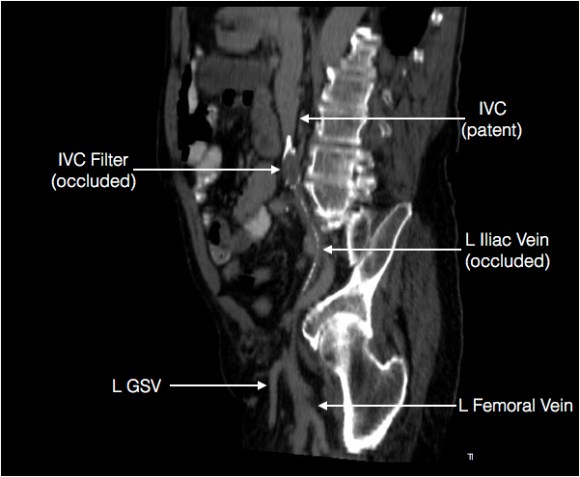
The patient is a gentleman from out of state who had called about problems he was having with walking and with leg ulcers that wouldn’t heal. He is in his seventies and has a pacemaker for an arrhythmia for which he was on Xarelto. He also had type II diabetes. He had bilateral lower extremity deep venous thromboses 6 years prior requiring IVC filter placement. The filter occluded, and it resulted in sudden sharp and debilitating pain in both legs with walking short distances -some days only 50 paces.He described it as an unbearable pain in calves and thighs that felt like his legs were going to burst. He also had ulcers on his legs that would heal with ministration but soon recur. This was all despite being quite active, with regular workouts, and being fit. He was compliant with compression. He sent a CT scan done last year (below).

It showed an Optease retrievable vena cava filter that was occluded and the iliac systems bilaterally (right above and left below) were chronically occluded with patent vena cava above and femoral confluences bilaterally below.
He had no hypercoagulability nor ongoing recent DVT’s. I thought there was a good chance that we would be able to recanalize the occluded iliocaval segment and he flew in for a consultation, and he was pencilled into the schedule ahead of his visit.
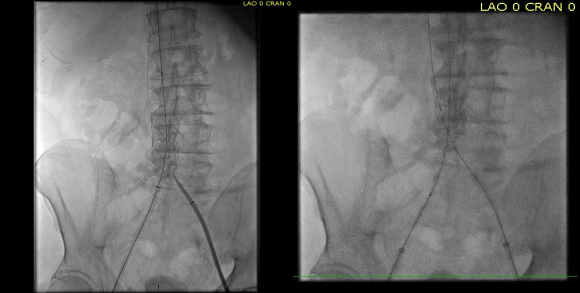
Examination revealed a fit and trim man in his 70’s in no apparent distress. He had bilateral leg edema that was moderate with small superficial and tender ulcers of the right posterior distal calf. Pulses were normal. He was taken to our hybrid suite and venography from femoral vein access in the proximal thigh in the supine position revealed his right and left iliac venous systems to be occluded (below figures).

Wire access into the iliac systems was performed with Glidewire and Glidecatheter periodic venography to confirm that I had not exited the vein. Unlike the arterial system, extravasation from being extravenous does not have the consequence of bleeding, hematoma development, and pseudoaneurysm formation because of the low pressure, but it can be a long procedure and uncomfortable as well so these are done under general anesthesia.

Once position confirmed to be in the iliac vein, the vein was dilated to allow for greater ease of movement. In the case of the uncrossable filter, I switched to access from above via a right internal jugular vein access.

Once the wire crossed into the iliac vein from above, it was captured and brought out. While ballooning by itself is inadequate for revascularization, it greatly eases wire capture and on the right, it was done simply by driving the wire from above into the sheath. Wire capture wins access across the iliocaval and IVC filter occlusion from below.

Once wire access is done, ballooning across the filter is done from both sides. A large sheath is them delivered across the IVC filter. Finally, a Palmaz stent mounted on a large balloon is delivered and deployed. I chose to do this from the right access, and retracted the wire on the left -something done with some trepidation because of the great difficulty gaining this access, but with with prior balloon dilatation, reaccess is made easier. Also, plan B would be reaccess from above.

When this is accomplished, the left sided wire is reaccessed across this stent. This is the venous side analogue to gate access in EVAR (below).
Once this is done, the iliac veins are dilated to 14mm from the IVC to the common femoral arteries. large 18mm Wall stents are deployed in a kissing fashion from the caval stent into both iliac systems and dilated to 18mm.

After deployment, the Wall Stents are ballooned to 18mm. These stents were extended into the common femoral artery with 14mm nitinol stents.

Completion venography suggested successful iliocaval recanalization and revascularization but these procedures are not done without a final intravascular ultrasound (IVUS).

Intravascular ultrasound revealed incomplete expansion of the right common femoral stent. This was treated with another stent and ballooning with the result on the right.
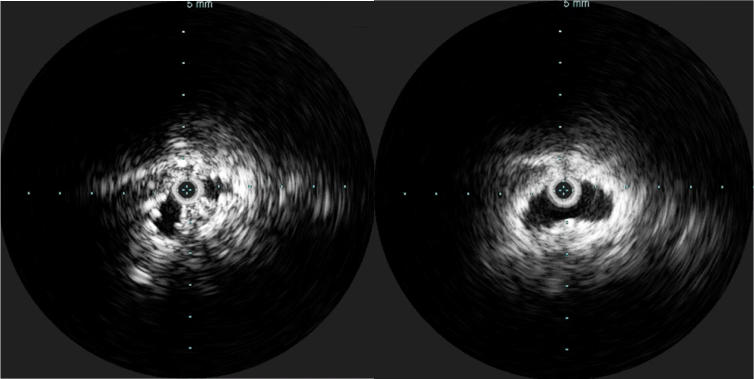
Venography alone is insufficient in determining patency. As illustrated, IVUS ensures a durable outcome.
The leg ulcer was treated with an Unna’s boot. A word about the venerable Unna’s boot –it works. The dressing dries and compresses while the Zinc Oxide prevents bacterial growth. It is interesting that the dressing is so infrequently used nowadays but not so when you consider that it isn’t reimbursed. And patients generally hate it.
This revascularization has an excellent chance at working as the patient has no hypercoagulability and had a patent common femoral confluence bilaterally. As I had mentioned in a prior post, the idea in venous revascularization is connecting confluences that serve as inflow and outflow.

This will require followup, consisting of duplex, and it is advantageous that he is anticoagulated for his arrhythmia. It is becoming more apparent that those languishing with chronic venous insufficiency and its complications need the IVC and iliac veins interrogated with a duplex. When an obstruction is found, they should be treated with these techniques as a first line therapy.
