The patient is a man over 70 years of age who came to the hospital with severe pain of his right foot and leg with walking short distances and at night while recumbent. He had a history of hypertension, diabetes, and coronary artery disease, and several years ago had his left common iliac artery stented. On examination, he had no lesions of his foot, and his pulses were only palpable (barely) in the femoral arteries only. He did have strong monophasic signals in the anterior tibial arteries bilaterally.
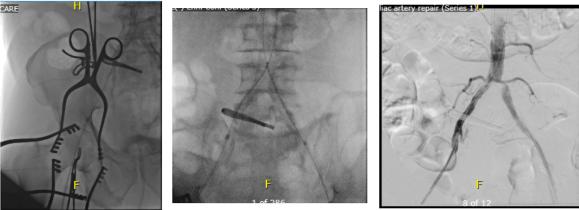
Initial vascular lab testing showed only mildly depressed ankle brachial (above), with dampened waveforms consistent with inflow and femoropopliteal disease on the right. He underwent arteriography by our vascular medicine specialist and cardiologist Dr. Faisal Hasan, and it showed bilateral common iliac stenoses, a severely calcified and nearly occlusive plaque in the right common femoral artery, and a long segment occlusion in the superficial femoral artery with diffuse calcified plaque extending into the popliteal artery. There was diseased but patent 3 vessel tibial runoff.


To Act As A Unit are the Cleveland Clinic’s words and it shows the Clinic’s roots as an US Army field hospital on the vasty fields of World War I France a little over a century ago, and we take it seriously. It may come as a surprise to some that a cardiologist referred me this patient after mutually deciding that the common femoral disease and the TASC D SFA occlusive disease, but we both decided that a surgical approach was the best one. The question then is how much more flow?
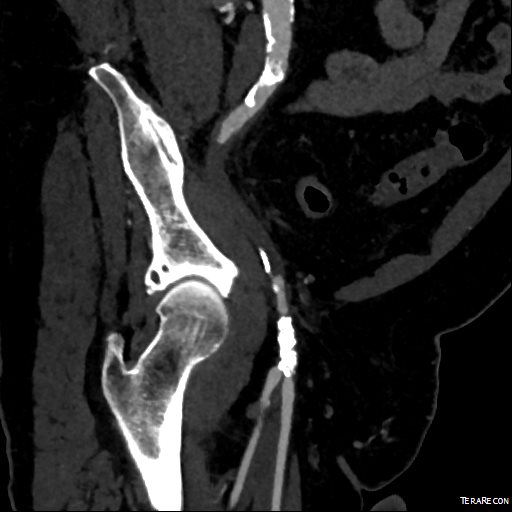
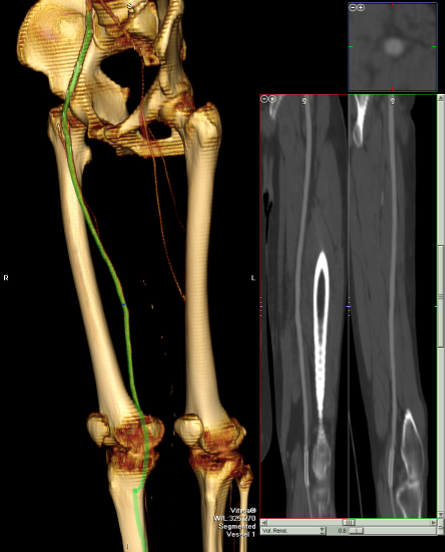
I ordered a CTA (CT angiogram) particularly for endarterectomies as I find it imperative to know the actual end point of plaque. Arteriography only hints at it, and while a 5mm lumen may look large and patent, it may be a channel in a 10mm wide plaque that when a stent terminates within it, breaks and becomes biologically active as intimal hyperplasia at best or embolizes at worst. CTA shown below revealed the plaque where contrast angio showed only the lumena of the vessels.



The 3D reconstruction function also allowed me to see and plan the operative approach and predict the lack of saphenous vein confirmed on duplex ultrasound.
For the students reading this, ischemic rest pain is often simpler to treat because it requires only a little more blood flow. There is a neurologic ischemia component that is not well studied, particularly in diabetics, as ischemia may result in anesthesia in someone who has underlying diabetic neuropathy, but that is not an indication for revascularization while rest pain is, and someone should investigate this. This little more blood flow in the form of treating inflow disease only may be sufficient in relieving rest pain while avoiding interventions on the superficial femoral, popliteal and tibial arteries which have limited longevity.
The common femoral artery on the other hand is the throttle of inflow and as a principle, inflow can be considered as the infrarenal aorta to profunda femoral artery, and repairing the common femoral necessitates an operation. There is no durable or laudable endovascular procedure for occlusive disease of the common femoral artery, a feature shared with the subclavian artery at the thoracic outlet and the celiac axis at the median arcuate ligament. All three are externally compressed by hard structures and revascularization must be ever mindful of the inguinal ligament, the thoracic outlet, and median arcuate ligament. The only exception to the “you must operate” rule of the CFA is calcified atherosclerotic disease in high risk individuals, and I make careful exception here with rotational atherectomy devices.
Claudication is another thing entirely. Claudication limits lifestyle and can be corrected by changing lifestyle -either with more exercise or limiting exercise. The thing is, when a patient has reached a certain age, that lifestyle may be walking slowly from chair to commode, and if that activity is limited, no amount of haranguing may be able to induce that person to embark on an ambitious exercise program. Sometimes, you have to be realistic about telling a frail old man to go for a 60 minute walk. But if that person has difficulty getting to the bathroom because of leg cramps, then either they have to get assistance or more bloodflow, and ironically, a little more blood flow represented by improving inflow, may not be enough.
That was what I was thinking when I was planning this operation. Improve the inflow with stents to the common iliacs and a right CFA endarterectomy, but use the opportunity of surgical exposure to extend the endarterectomy to the distal external iliac and through the entire SFA.
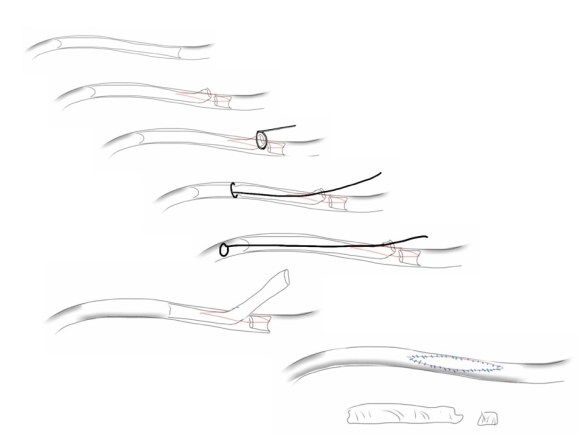
My fondness of remote endarterectomy is well known from my many blog posts on it (link). It is a modern update on a very old procedure -the ring endarterectomy, done since the middle of the last century when bypass grafts were unavailable. The occlusive plaque is removed, and an end-point reached and cut with a scissor like device (available from LeMaitre). It is the ultimate hybrid operation (below) requiring open and endovascular skills. I tell prospective trainees to judge training programs by how facile are the surgeons and how many are the procedures with and involving a hybrid approach, because any program can have few (getting fewer) old surgeons doing only open surgery and a lot of young surgeons doing only endovascular procedures, but a rare few will do a lot of hybrid procedures. 
I chose to add femoral EndoRE. This would bring the extra blood flow needed to kickstart any walking program, barring cardiopulmonary limitations.
The patient was brought to our hybrid operating theatre and prepped from nipples to toes. The right common femoral artery was exposed for endarterectomy, and accessed then with a sheath along with a left femoral sheath for kissing balloon angioplasty and stenting of the common iliac artery stenoses (below).
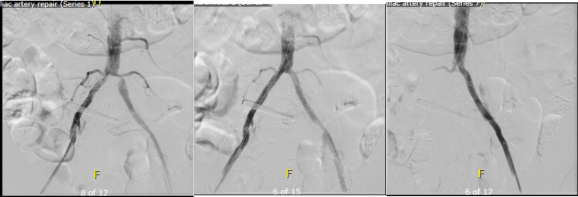
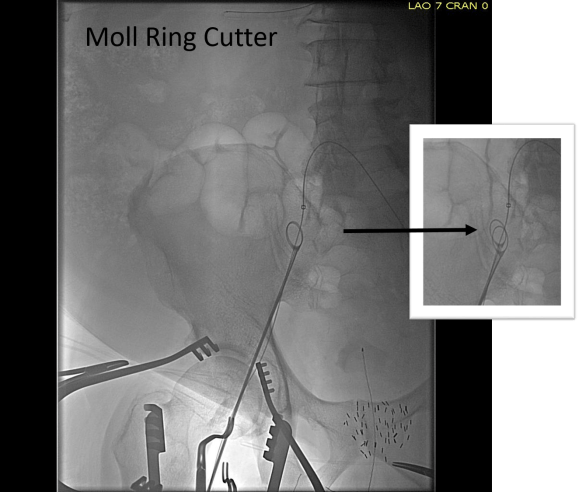
Afterword, the CFA was opened and endarterectomized, and the SFA was remote endarterectomized (below).


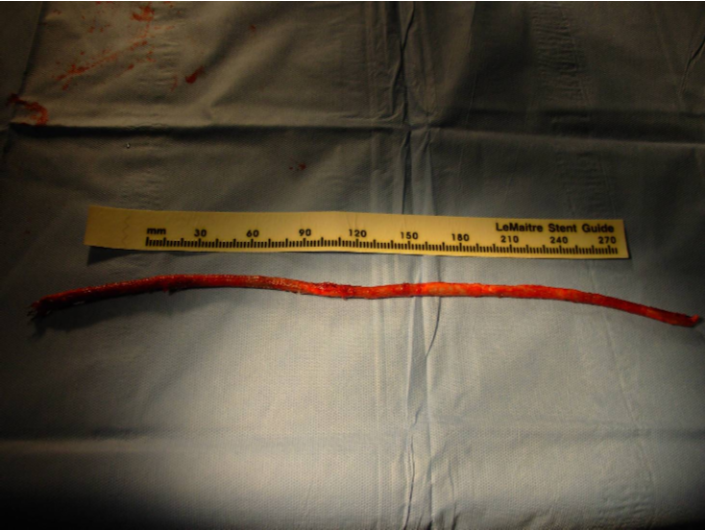
The endpoint was chosen in the above knee popliteal artery to avoid having to stent the dissected end point plaque well into the popliteal artery. If I wanted to go all the way to the below knee popliteal artery, I would have to open it to manage the plaque and artery at the so-called trifurcation, typically with a patch angioplasty. The plaque came out in one piece (below):


The terminus of the plaque in the POP where it was cut has to be managed with a stent, unless you open and complete the endarterectomy and patch the artery. I was able to cross the dissection (no small feat) and plaque a stent. The artery was widely patent and even the small branches off the previously occluded SFA were now reopened.


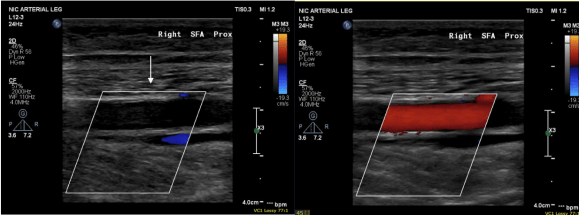
His pulse volume recording done after intervention reflects the improved flows (below).

His rest pain resolved, but more gratifyingly, he has regained the confidence to walk and exercise, which he now does without limitation up to 45 minutes a day. In two month followup, we performed a duplex which showed his right SFA to be basically normal (below), including an intimal stripe and media. This is not an anomaly. When I took a punch out of restored artery to perform an anastomosis (from this case link), I sent it. Previously it had been an artery that was obstructed for nearly a decade, but after EndoRE, had become an elastic, compliant vessel. The pathology returned as “normal artery.”
When these fail, they typically do so a random points on the endarterectomized vessel and on the stent. While stent grafting may have better outcomes with regard to restenosis, doing so covers collateral vessels and PTFE grafts behave poorly by embolizing while clotting off, and PTFE stent grafts are no different. Data from over a decade ago suggests that EndoRE of the SFA while inferior in patency to vein grafts, are equivalent to PTFE [reference 1] and superior to endovascular revascularization [reference 2] in terms of primary patency. When they occlude, they achieve a “soft landing” without the furious acute ischemia and embolization seen with PTFE bypasses.
I think these handful of cases I performed here in the UAE represent the first in the region. The main difference here is that the arteries tend to be smaller by about 20%, and in one instance, the smallest Vollmer ring was too large for the vessel in a case where I abandoned the SFA revascularization -the profunda and inflow revascularization proved sufficient in reversing rest pain. The intriguing property of endarterectomy is something that we all try to do with surgery but rarely achieve -a restoration to an earlier time. I believe this patient’s right femoral artery is now back to a youthful state.
References:
-
Eur J Vasc Endovasc Surg 2009;37: 68-76
- J Vasc Surg 2012;56:1598-605.