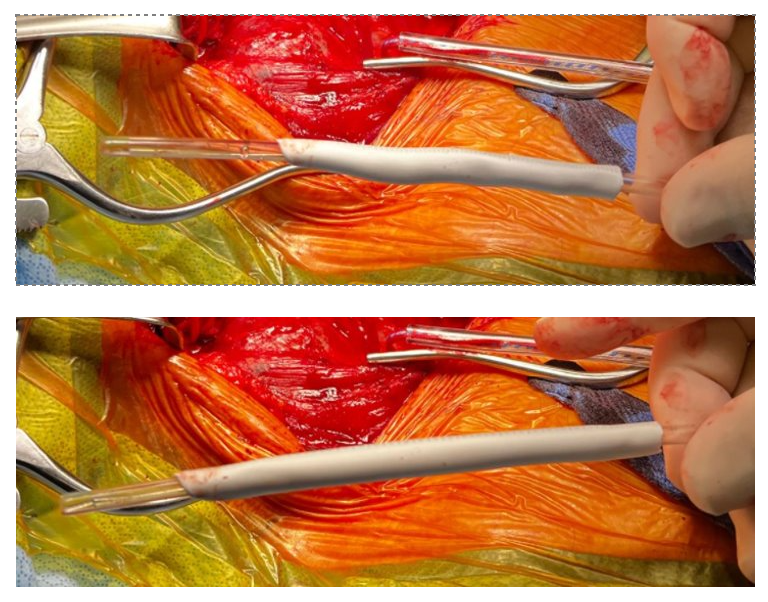
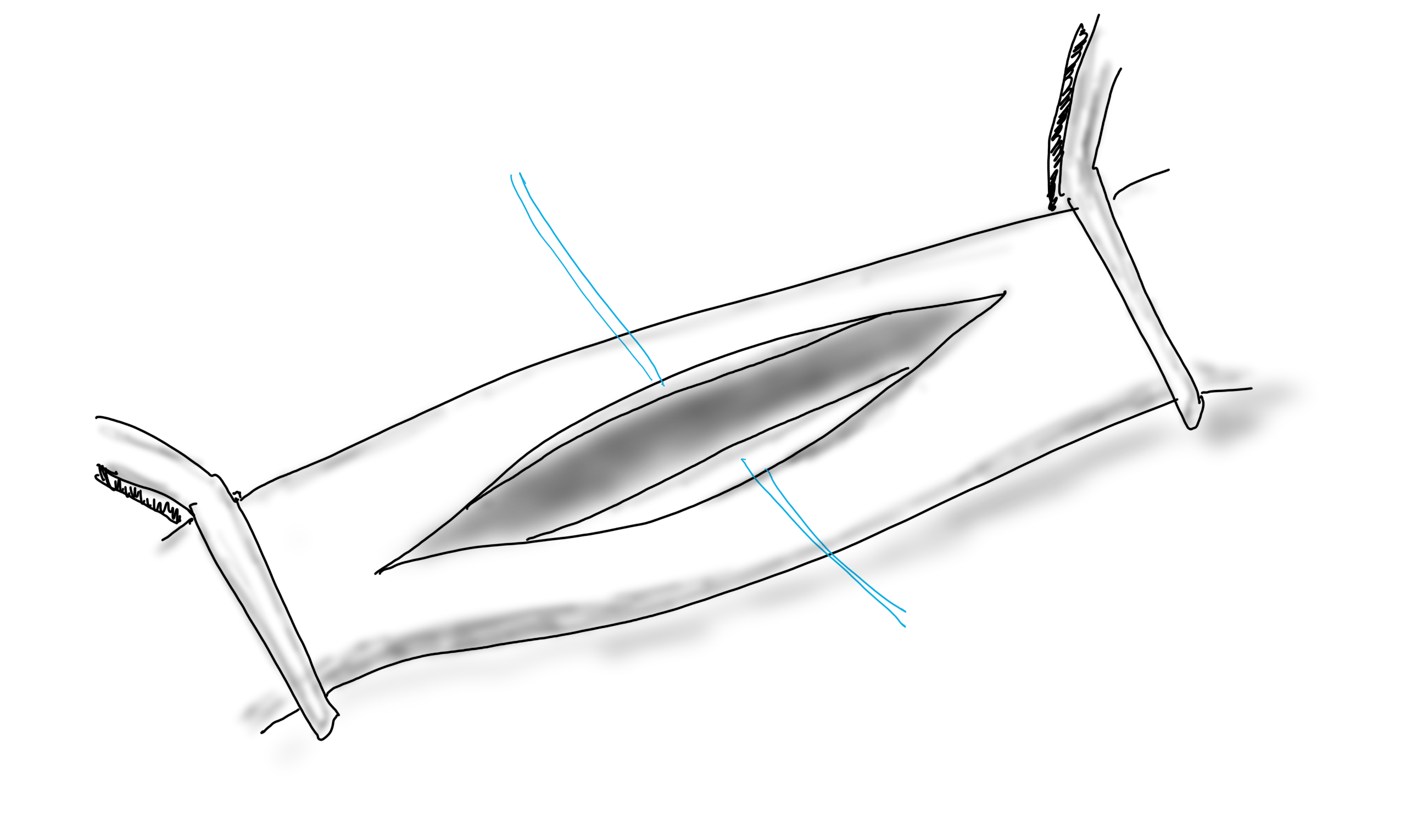
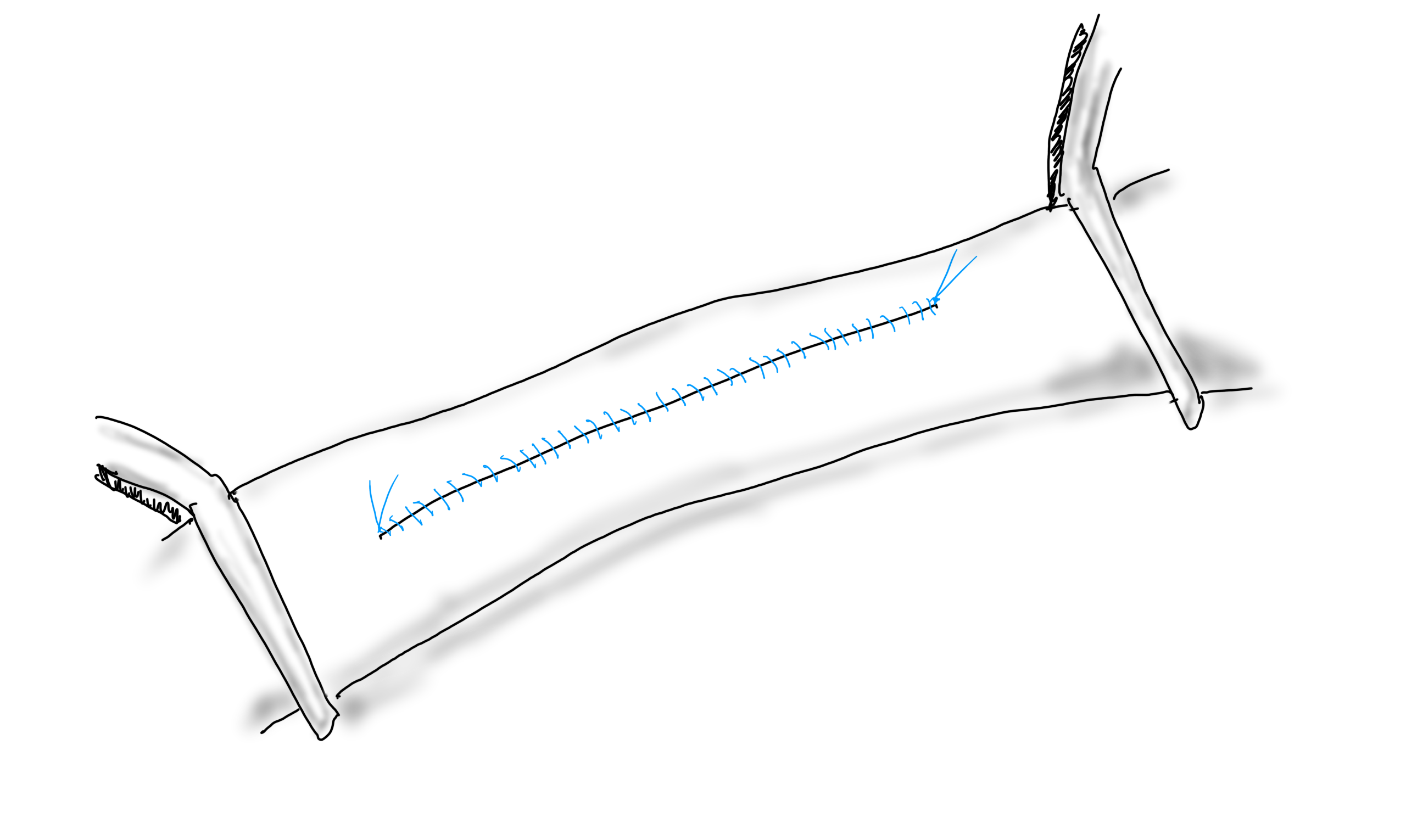
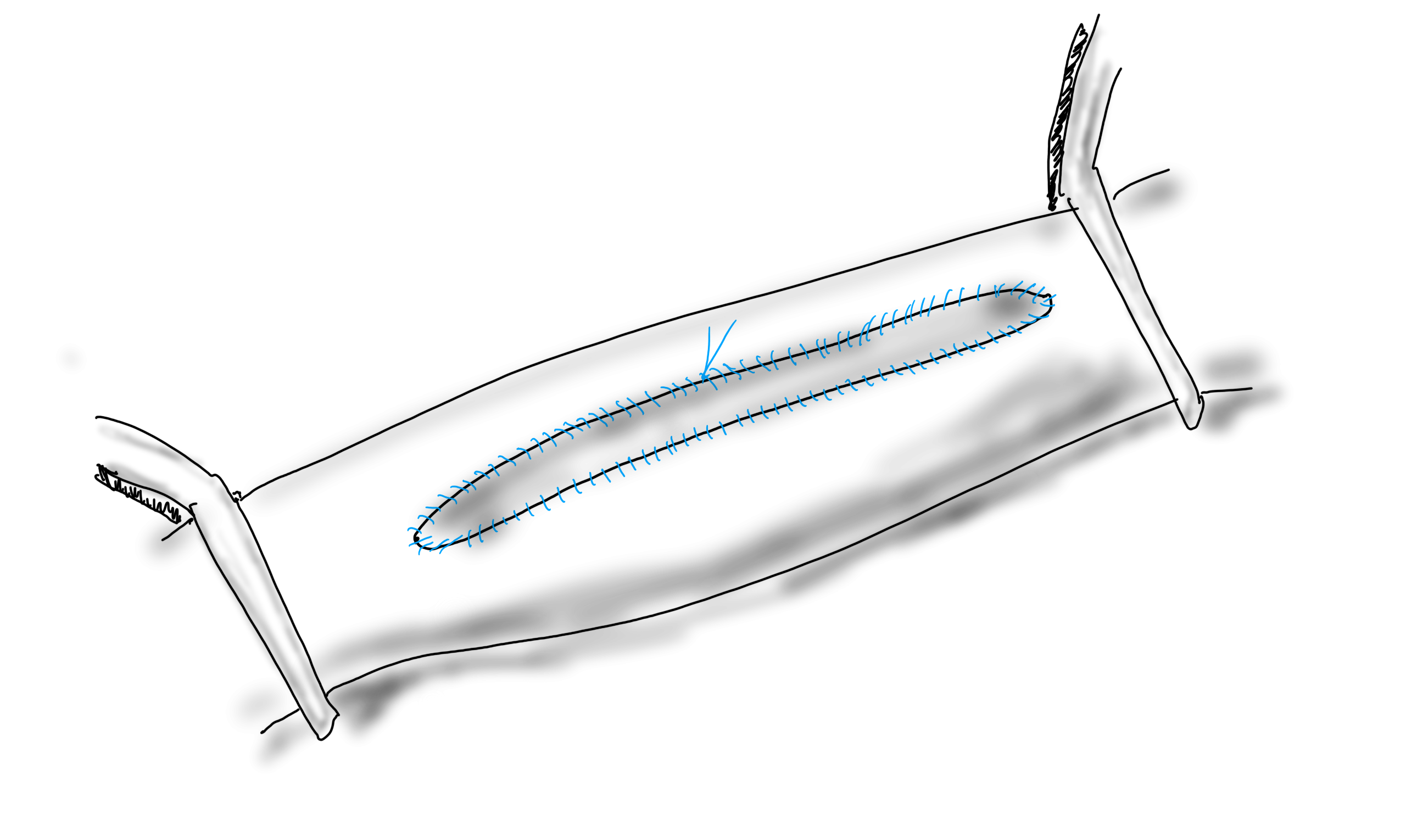
PTFE bypass to a smaller tibial artery with Taylor vein patch
One of the conclusions of the BEST-CLI trial (ref 1) was that of equivalency between alternate bypass conduits and interventions when a single saphenous vein is not available. I recently contacted Dr. Matt Menard to see if there had been subgroup analysis of these bypasses which represents a heterogeneous group of conduits including PTFE, PTFE with vein patch, spliced vein, composite vein, and even possibly allograft. The results from the abstract were intriguing -“83 of 194 patients (42.8%) in the surgical group and in 95 of 199 patients (47.7%) in the endovascular group (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; P = 0.12) after a median follow-up of 1.6 years” with the primary MALE endpoint. If this was a football game, there would be a video review of the call. And they are looking at this, I was assured by Matt, but we would all have to wait for this year’s SVS VAM. Dr. Matt Menard is coming to speak at our 12th Annual Vascular Disease Update (link) which I highly encourage you to register and attend (addendum).
The Cohort 1 from BEST-CLI is an illustration of the vascular surgeons’ LIMA to LAD. It’s something we already knew from years of experience, but laid out in level 1 data (below).
The BEST-CLI paper is short on detail about cohort 2. This is where a lot of clinical decisions get made, and I suspect the vast majority of patients are getting interventions because fewer surgeons are facile with leg bypasses and vein patches.
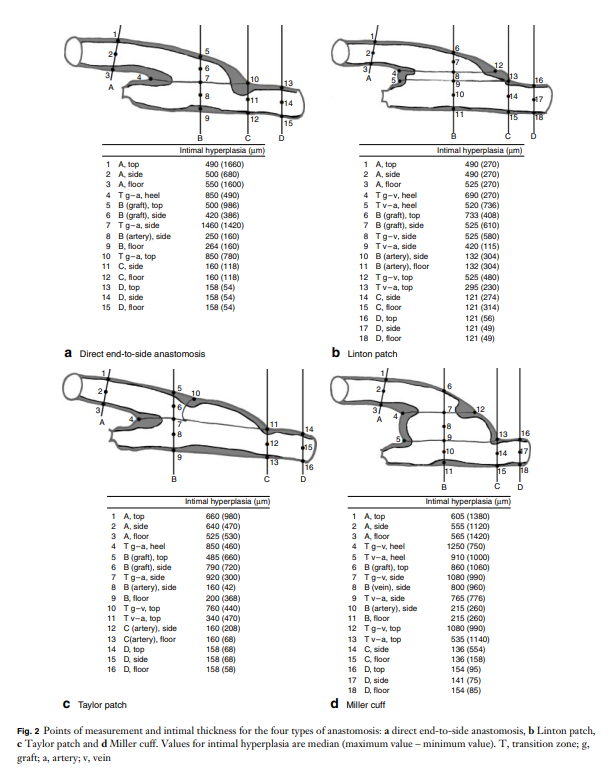
Why the vein patch? While not a panacea for the lack of vein, from its inception, it has proved a worthy adjunct in limb salvage. Decades before endovascular therapies showed good limb salvage with modest to poor patency rates, Dr. Frank Veith showed that infrageniculate PTFE bypasses showed good limb salvage with poor patency (reference 2). Vein patches, such as the Taylor patch illustrated at the top, showed good patencies (reference 3) in an era where DOACS, DAPT, and statins were not available.
Results of the Taylor Patch from Mr. RS Taylor.
Why a patch works is debated. Some feel it is the modification of the end to side anastomosis that creates an optimal shape for containing turbulence which leads to intimal hyperplasia. This was the concept behind the Distaflo graft which I tried but have abandoned for not improving patency in my personal experience.
The Distaflow Mini-Cuff which applies the concept of flow optimization by the shape of the anastomosis achieved by vein cuffs.
The best explanation of why vein cuffs work is from an animal study from Vienna. Intimal hyperplasia is best explained as a foreign body reaction and the reaction is worse with a true foreign body than with autologous materials. A simple anastomosis with PTFE to tibial artery creates a ring of hyperplasia. Vein patching moves this severe foreign body reaction off of the artery, leaving a gentler vein to artery reaction to occur on the outflow (reference 4).
My final point is that these surgical papers used to be the mainstay of podium presentation in the 90’s and ’00’s, but are now infrequent as the bulk of the time at these meetings is devoted to gadgets which almost always involves purchasing a box and contracting for disposables (the printer and ink business model). I am going to review our institutional results of these PTFE bypasses, and hope to see more from other groups. I look forward to the BEST-CLI papers to come, and other trials.
References
Farber A, Menard MT, et al. BEST-CLI Investigators. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N Engl J Med. 2022 Dec 22;387(25):2305-2316. doi: 10.1056/NEJMoa2207899. Epub 2022 Nov 7. PMID: 36342173.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
Taylor RS, Loh A, McFarland RJ, Cox M, Chester JF. Improved technique for polytetrafluoroethylene bypass grafting: long-term results using anastomotic vein patches. Br J Surg. 1992 Apr;79(4):348-54. doi: 10.1002/bjs.1800790424. PMID: 1576506.
Trubel W, Schima H, Czerny M, Perktold K, Schimek MG, Polterauer P. Experimental comparison of four methods of end-to-side anastomosis with expanded polytetrafluoroethylene. Br J Surg. 2004 Feb;91(2):159-67. doi: 10.1002/bjs.4388. PMID: 14760662.
Addendum
The Annual Vascular Update at University Hospital has something for everyone, including a presentation on IRAD by Dr. Santi Trimarchi, and BEST-CLI by Dr. Matthew Menard. Local faculty from Cleveland are also featured in a broad review of vascular medicine and surgery chaired by Drs. Mehdi Shishehbor, Heather Gornik, and our chair in vascular surgery, Dr. Jae Sung Cho. Link. I will be presenting on neurovascular compression syndromes and renal failure/heart failure.
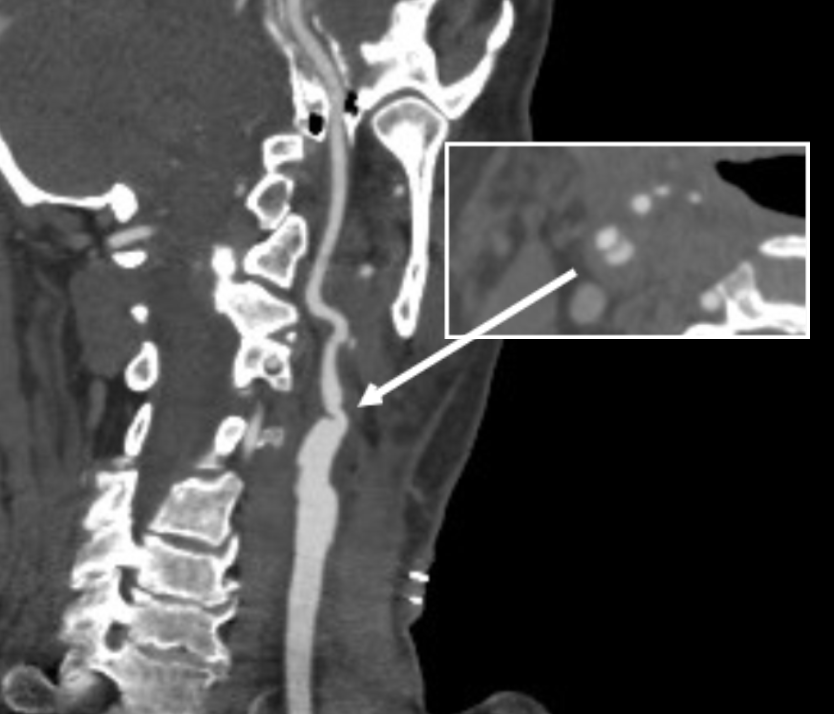
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
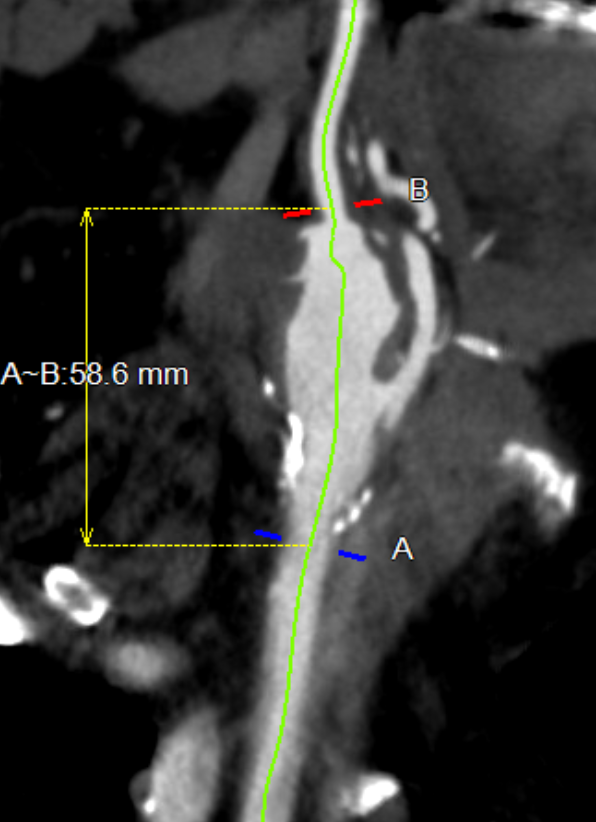
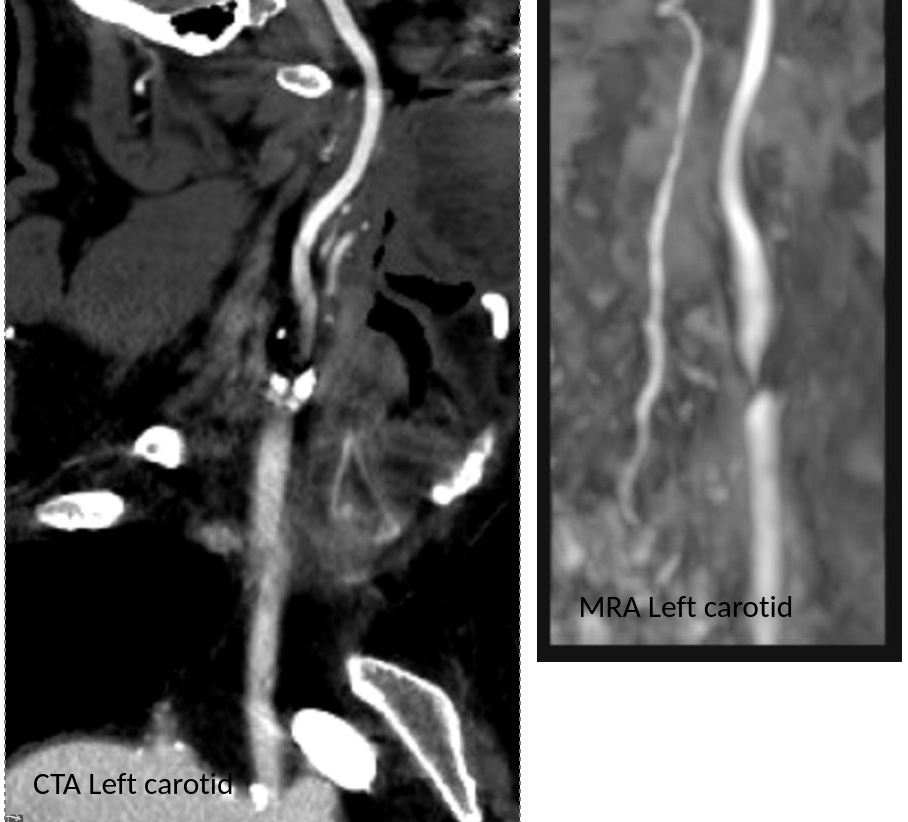
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
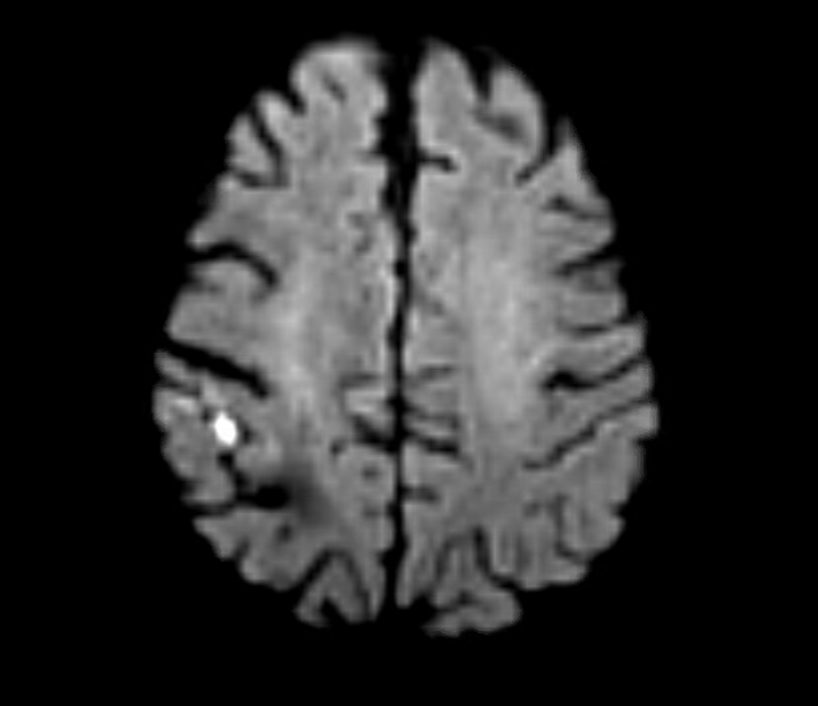
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
The patient is a 70 year old man with risk factors of cigarette smoking, type II diabetes mellitus, hypertension, and hypercholesterolemia who presents with rest pain and gangrene of the tip of his left great toe. Several weeks prior to this, he went to his pharmacy and received a flu vaccination and picked up over the counter topical medication for an ingrown toenail. who developed pain from an ingrown toenail. Several weeks later, the tip of his toe blackened and the pain became unbearable and he came to the hospital.
No pulses, dry gangrene of tip of toe
Physical examination was notable for the dry gangrene affecting the distal phalanx of the left hallux. There was a left femoral pulse, but nothing was palpable below. His forefoot was cool and painful and this pain was relieved with dependency.
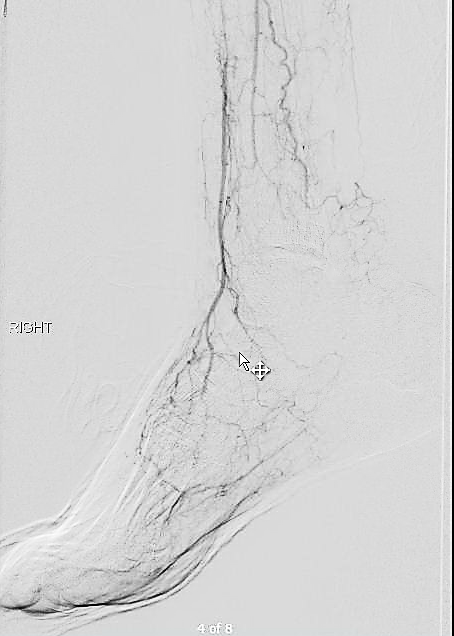
Pulse volume recording showed a drop in flow across the left knee and flate waveforms at the ankle, foot, and digits. The ABI was zero. WIfI 2 3 2, Stage 4, potential benefit of revascularization high (reference 1). CTA was performed and revealed patent aortoiliac segment, patent common femoral and profunda femoral arteries, with occlusion of the mid to distal SFA, reconstitution of the above knee popliteal artery with 2 vessel runoff via a patent posterior tibial and peroneal arteries.
CTA VR Reconstruction Shows Reconstitution of AK POP and 2V Runoff via PT and Peroneal Arteries
The centerline reconstructions, adapted from aortic planning, lets me determine the character of the arteries for size, calcification, stiffness, collateralization, and length of occlusion. This was had low density and given the timecourse of the events -from claudication to gangrene, and the lack of collaterization implying an acute process possibly on a chronic lesion, I felt there was likely to be some thrombus burden over a chronic plaque across Hunter’s Canal with occlusion of the geniculate arteries. Usually, when the occlusion is chronic, femoropopliteal occlusions of this type come with an ABI of 0.5-0.7, not 0.
Global Limb Anatomical Staging System (GLASS) Classification of CLTI (reference 2) through the easy to use SVS calculator came out Stage II: Intermediate Complexity. I had the good fortune of being in the audience when GLASS was presented to a rapt audience in Lyons, France, by Dr. John White in 2017, at the ESVS meeting. I include it because Dr. Devin Zarkowsky on a tweet that generated this post wanted WIfI and GLASS. WIfI I find helpful. GLASS I am still figuring out, because it tends to tell me what I already know: this is a lesion of intermediate complexity that could go either way to open or endovascular.
Treatment options include:
Endovascular -starting with POBA and escalating to various additional therapies such as stents, covered stents, DCB, drug coated stents, atherectomy, thrombectomy, thrombolysis (then any of the previously mentioned).
Bypass with PTFE
Bypass with vein
White Arrows Show the Excellent GSV
The data tells us so far that open or endovascular is broadly equivalent, but experience guides me. For rest pain, any incremental increase of flow will do, and it does not necessarily have to be in-line. For healing major tissue loss, there really can’t be enough flow. Bypasses with good runoff deliver a lot of flow. Bypasses with vein have great longevity and the shorter they are, the longer they last.
So is long patency important? Numerous studies have shown that patency does not impact limb salvage or amputation free survival, going to BASIL Trial (reference 3), but even stretching back to Dr. Frank Veith’s advocacy of PTFE bypass to infrageniculate targets (reference 4), patency does not add to limb salvage beyond the initial wound healing. The patency of a PTFE bypass to a tibial target is less than 20% at 5 years, but the limb salvage rate is a laudable 80% plus, and this is repeated in numerous evaluations of POBA, stents, and every new technology that has accrued in the nearly 4 decades since that paper.
What does patency buy you? Less reinterventions. There is nothing worse to me than having to reintervene within a year or two of an intervention. When a bypass works well, the patients just come for a hello-how-do-you-do for years. The BASIL trial concluded that bypass operations were more expensive, and I dispute this. In 2021, operations were far less expensive than the latest energy weapon, their box you have to purchase, and the catheters you use once and throw away. The argument given by interventionalists is that bypass operations are disfiguring and ridden with complications and that argument holds water as there are many points where vascular surgeons fail or have largely stopped work on investigating and optimizing open surgery. What if bypass surgery could be brought to the level of dialysis access surgery in terms of invasiveness? What if groin complications could be minimized? What if long filleting-type incisions of the thigh and leg could be eliminated entirely? What if edema could be prevented or minimized postoperatively to prevent serous drainage and infections? If you focus on the art of bypass surgery and choose patients well, you can get a quick, minimally invasive bypass with the overall physiologic impact of a Brescia-Cimino AV fistula. After considering endovascular, I chose bypass.
This patient had on mapping excellent saphenous vein between 3-5mm in diameter. He had excellent skin and was not obese. A vertical groin incision could be avoided by making a skin line incision over the saphenofemoral junction and transposing it to the adjacent SFA which was patent. Skin line oblique incisions in the groin heal much better than the standard vertical incisions, and it is possible to mobilize and expose the saphenous vein using an appendiceal retractor and clipping the generous proximal thigh tributary. In this patient, the most proximal incision was well away from the inguinal crease, the generator of wound infections in the groin. Essentially, if there is no groin incision there can be no groin complication.
The distal vein is mobilized first before dropping on the above knee popliteal artery which is exposed through a separate incision. This is because the AK POP space is best exposed over the sartorius, and the vein in this patient was well below (posterior) to the sartorius. The vein was tunneled under the sartorius to the AK POP. With the in-situ technique, the proximal anastomosis is completed, then the valves lysed with a retrograde LeMaitre valvulotome. Doing, after two or three passes, the pulse was strong, and the flow strong enough to fling the blood beyond the foot -a key step. If there is no such flow, if there is a weak pulse, or poor blood flight, I do one more pass of the valvulotome then duplex for any large diverting tributaries and tie them off one by one until good flow is achieved.
I do not mobilize the entire vein (and tie off every collateral) unless I cannot do an in-situ technique. It defeats the purpose of this beautiful minimally invasive procedure.
Femoral artery to above knee popliteal bypass with in-situ vein
He recovered rapidly and was discharged home after a partial hallux amputation by podiatry. In followup, he was feeling better. All of his surgical wounds had healed. Duplex and ABI did find this:
Retained valve, very hard to see but present on B-mode, causing a hemodynamically significant stenosis, with ABI of 0.57
I took him to the angiosuite for repair of this retained valve. Rarely, retained valves occur after in-situ bypasses, but require generally unsatisfactory solutions involving either open valvulectomy and patch venoplasty or stenting of a virgin vein. Valvulotomy is possible, but generally described as an open procedure as well, but I had other plans.
Downstream of this retained valve were tributaries which could be seen on duplex, and therefore accessible with a micropuncture needle. This would then allow for placement of a 4F sheath, through which the LeMaitre valvulotome would pass unhindered, allowing for valvulotomy. I would use this session in the angiosuite to deliver embolization coils to the diverting tributaries as well.
Arteriography reveals a retained valve and diverting AVF’sRetained valve catches the catheter sent up and over from the other side
LeMaitre is a unique company in that it focuses on vascular surgical operations and arises from the original product and reason for the company the eponymous valvulotome. Because it comes sheathed in a low profile catheter, it is immediately familiar to modern surgeons even though it was made in another century.
Cutting of retained valve with LeMaitre valvulotome using ultrasound guidance
Cutting the valves involved passing the valvulotome several under fluoroscopy through a 4F sheath placed through the tributary seen above. After the valvulotomy, the diverting tributaries, only one of which drained quickly into a deep vein, were coiled. At the end of the procedure, a manual cuff was found and an ABI checked. It was now 1.05.
Diverting tributaries coiled
In 2015, the Oxford English Dictionary added McGyver as a verb -“Make or repair (an object) in an improvised or inventive way, making use of whatever items are at hand.” A television show from the 80’s and early 90’s, the main character, McGyver, was able to make useful tools out of what was available, allowing him to come out victorious, but usually just survive. It is a useful concept that is a must have in managing complex and dynamic situations. Just because it hasn’t been done before to your knowledge doesn’t mean that it isn’t a simple solution. I have only one ask that LeMaitre flip their blades around and design an ante grade valvulotome. Those who know what I’m getting at know what I am getting at.
The LeMaitre valvulotome allows for in-situ saphenous vein bypass, a prototypical hybrid vascular procedure from the 80’s that portended the endovascular revolution that followed. It is meant to be used intraoperatively, but because of its low profile, it can be applied.
I will allow that this second procedure likely makes any argument to cost moot, but numerous incisions and extra time in the OR is avoided. The patient now has a vein bypass that could last many years which diminishes the need for follow up procedures to maintain assisted patency.
We will be arguing this point for years even after BEST-CLI is presented. BASIL-2 just closed enrollment. Hopefully we will get some clarity.
Reference
Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014 Jan;59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12. PMID: 24126108.
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28. Erratum in: J Vasc Surg. 2019 Aug;70(2):662. PMID: 31159978; PMCID: PMC8365864.
Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005 Dec 3;366(9501):1925-34. doi: 10.1016/S0140-6736(05)67704-5. PMID: 16325694.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
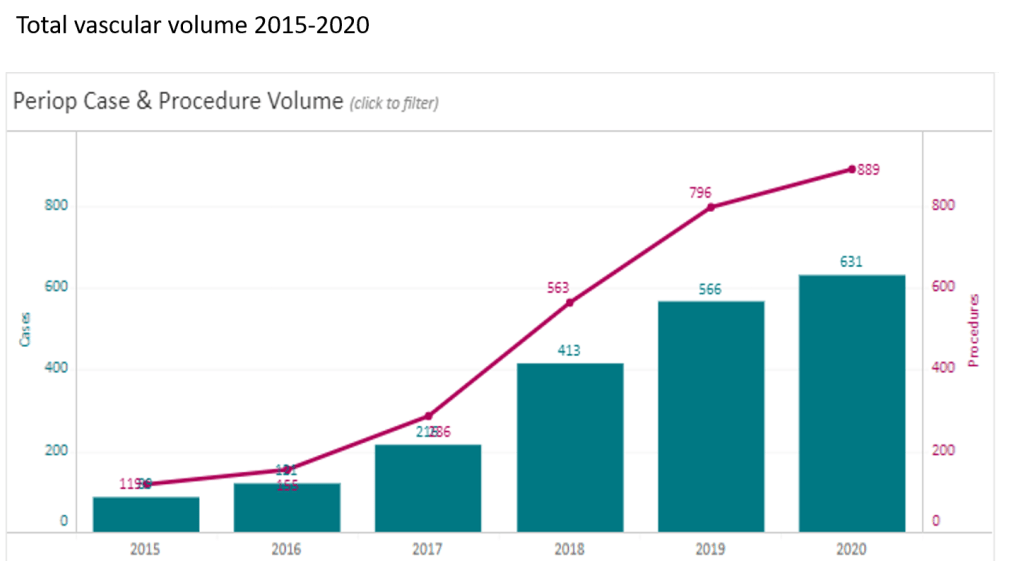
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
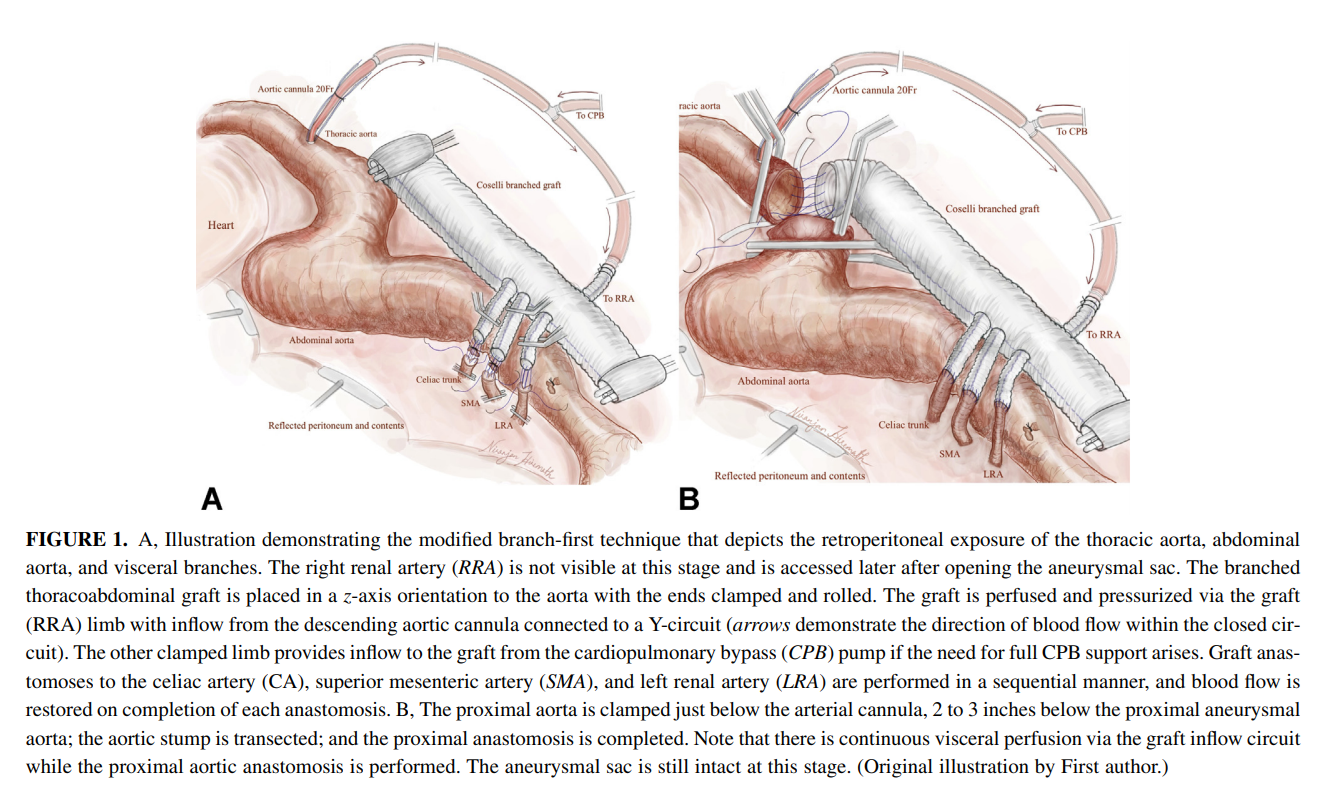
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
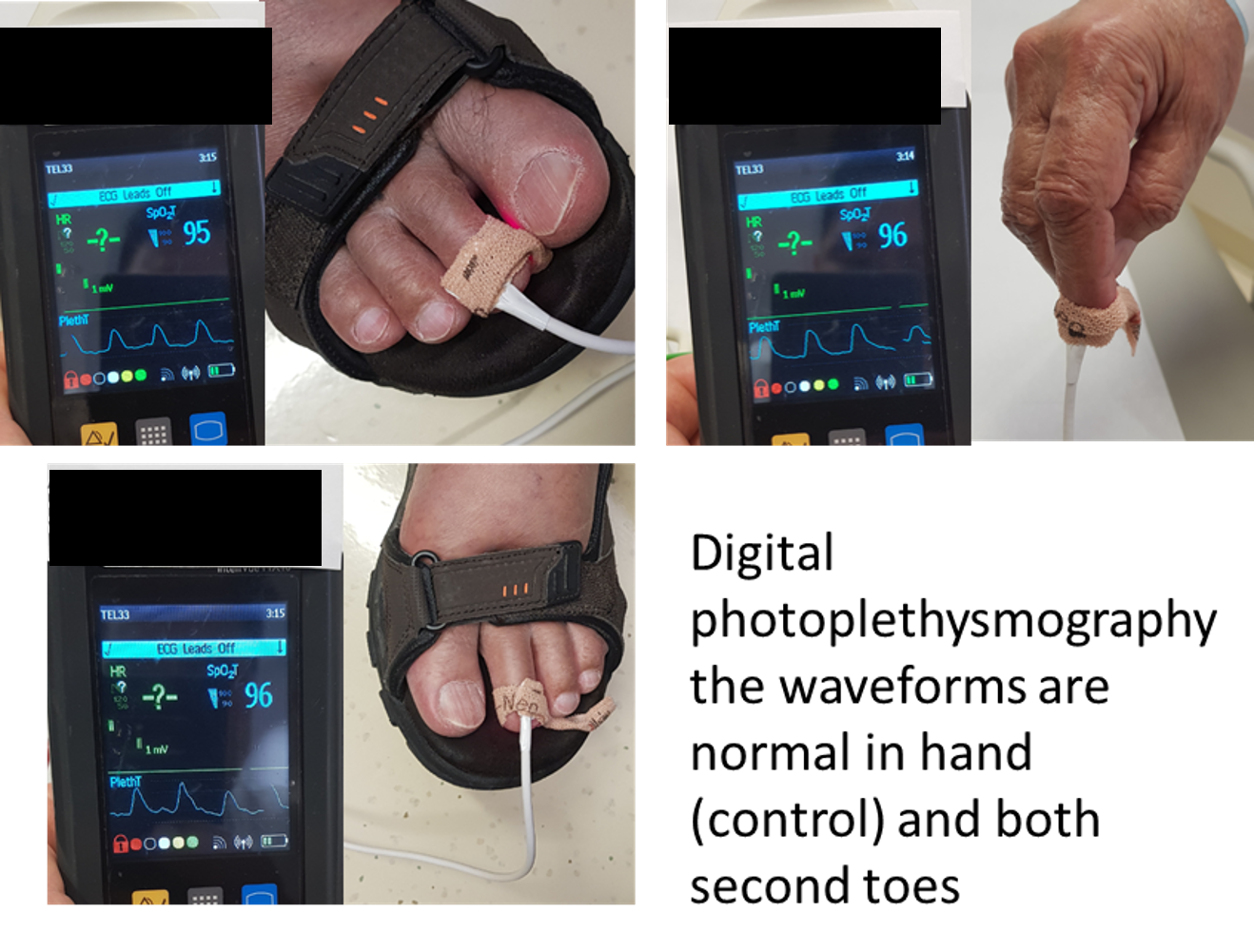
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.
This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).
an abnormal DPPG captured with a hospital ICU pulse oximeter
We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).
At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).
The distal perfusion cannula is in the dorsalis pedis artery
This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery
The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).
Pulmonary artery staple line bleeding controlled, ready for suturing.
In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.
View out of my balcony, sometimes you need many pieces to assemble a beautiful whole
Innovating Our Way Out of Not Having Enough Vascular Surgeons
This year’s SVS meeting featured a sobering assessment about the vascular manpower deficit affecting North America at the E. Stanley Crawford Critical Issues Forum, moderated by Dr. Michel Makaroun, MD, president-elect of the SVS. 35-45% of practicing vascular surgeons plan on retiring in the next decade by conservative estimates. We are not attracting enough candidates for the training programs. The solutions, including decreasing the length of training, public relations campaigns, and incentivizing retention have had mixed results, but we have yet to see a sustainable rise in vascular surgeon numbers.
Burnout driven by lack of work-life balance, the advent of electronic medical records optimized for billing, the passing of the private practice era, and the constant need to adapt to new techniques, create a persistent downdraft on staffing. So as some hospital face the reality of having to contract services, little attention is given to delivering best care with the staffing that we have. Changing how we practice is the only viable solution.
There are an estimated 3000 active vascular surgeons in the US. Imagine if all the cheese needs of this country could only be met by 3000 artisanal cheesemakers who make cheeses one at a time and want to live in places with international airports, BMW dealerships, and major league sports teams, and must have 3-4 partners to share cheese call. If you are a rural hospital in dire need of vascular surgery services and your one vascular surgeon is retiring, you are probably SOL.
When I was training, vascular surgery was oft touted as a primary care specialty. And that is how many of us still practice, managing risk factors, monitoring mild disease, as well as planning and performing interventions and operations. As much as I enjoy that kind of interaction, the half hour to an hour visit for a head to toe cardiovascular survey and discussion, educating patients and families about pipes and pumps, is incredibly inefficient. A healthcare system, a hospital, facing a staffing shortfall, has to do everything possible keep that vascular surgeon in the OR during work hours.
What is the core function of a vascular surgeon? Making good decisions and executing plans well. Decisions require data. What is this data? We laud the history and physical examination, but this is a throwback to another era. If you look at the diagnosis of myocardial infarction, it is not standard practice for a cardiologist to come and get a history, examine the patient, and declare that the patient is having a heart attack based solely on history and physical examination. It is a triage nurse in the ED who draws labs and orders an EKG which is read by a machine. These data points will tell you if heart muscle is being damaged. A process is started which triggers a team to come and take care of this patient. The hospitals focused on this actually drill their cath lab teams like pit crews. A stopwatch starts with the goal of revascularization under an hour.
Not so with peripheral vascular disease. The ischemic foot might have only a few hours depending on its presentation before it is irretrievably lost, but no matter -they sit in the ED until a vascular surgeon comes to speak to the patient and family, examine them, and then order tests, admission, consults, and operating room -typically all by themselves. Getting these patients into the operating room is in many places hampered by the lack of dedicated OR staffing, radiology techs, anesthesiologists, space, equipment, and critical care capacity. During work hours, there are scheduled cases that have to be delayed or canceled for another time, which takes time to do. After hours, the patient may have too many comorbidities to handle safely with the available staff. The vascular surgeon may have to bargain and cajole, to align several factions whose attention is demanded by many equally important concerns. If you decide to hold a lavish dinner party of twenty important guests -reserving space, calling caterers, inviting guests, arranging transportation – on short notice, you might pull it off once, but if you do this regularly, you are a masochist of the first order.
In the heart attack model, the history and physical examination is relegated to a series of yes/no or how long questions, and positive responses trigger a series of coordinated actions of a system -a reflex. In the leg attack model, there is no such system. I have to blame the vascular surgeons for preserving the current model. Vascular surgeons are organized as a guild. Guilds are protective of their monopolies on skills and markets and fiercely resist change. Most vascular surgeons are terrified by loss of control, and cling to the notion of being misunderstood and unappreciated saviors. We can do better.
The area that needs streamlining is at the point of referral. The majority of time of a vascular surgeon is spent working up normal blood vessels, varicose and spider veins, leg edema and pain, and mild and moderate arterial atherosclerosis. This work initially does not require a vascular surgeon but rather a focused set of policies and initial diagnostic studies that can be administered or ordered by any caregiver. Reducing the need for vascular surgeons at this point in vascular care will go a long way in extending the vascular work force at hand.
Point of Care Blood Flow Evaluation
Finding and declaring blood vessels to be normal is challenging and too often time consuming. Streamlining this will go a long way in freeing vascular surgeons to take care of disease.
The average caregiver is an inconsistent pulse taker. The palpable pulses are not always easy to find. Asking over the phone or as policy for someone to examine pedal pulses -the posterior tibial artery and dorsalis pedis artery pulses, is challenging. A positive is just as likely to be true or false as a negative. No cardiologist would ask a similarly detailed and technical question about an MI. In fact, they can’t ask, “Is there a pulse in the LAD?” Cardiologists make do with tests easy to obtain and interpret with certainty -the plasma troponin level and the EKG. The EKG is read by an algorithm so established and so tested, that it should stand as an example of early machine intelligence taking over a human job -but I digress.
What is our EKG? It is not the ABI -the ankle brachial index, because it is terrible at identifying disease, and is difficult to obtain reliably without practice. The closest thing to an EKG we have in terms of simplicity and accuracy is the pulse volume recording, the PVR (figure below). A FloLab machine, the machine used to obtain PVRs, will basically run itself once the cuffs are correctly applied on the leg, and the tracings are very easy to interpret. Unlike an EKG, there are no electrodes whose locations you must memorize. If the closest vascular surgeon is an hour away by ambulance, the transfer of a patient with flat waveforms and ischemic foot does not require a consultation on site. The patient would go to the vascular surgeon with no time wasted and no kidneys injured by CTA’s that too often fail to travel with the patient. Unlike an EKG which can be performed by many caregivers, a PVR requires both the equipment and a vascular technologist. A vascular technologist is not available 24-7 in most hospitals, and FloLab machines purchased for vascular labs are not meant to be dragged around the hospital.
So let’s think out of the box about another box in every triage nurse’s cell, every ER and ICU bed, and on every hospital nursing floor. These are pulse oximeters with a digital tracing, and bonus points, some come with strip printers! Placing a pulse oximeter probe on the second toe and comparing to an erstwhile normal wave signal such as on an index finger can provide qualitative information about normality and disease. Normal waveforms and abnormal ones can be easily discerned. A flat line is another obvious finding when in comparison, a finger or an ear on the same patient has normal signals.
How much better would a vascular surgeon feel about a transfer call that has this information, “digital waveforms are flat in this patient with rest pain and a bruised toe.” How much better would a vascular surgeon feel about a call about a patient with “digital wave forms are normal in this patient with toe pain and a bruised toe. We got an x-ray and there was a fracture.” The communication can be quite detailed and refined. For example: “The patient had no pulses, we think. Digital wave forms were dampened but pulsatile in a patient with a bruised toe, we’ll send to vascular clinic in the morning.”
A study comparing pulse oximetry signals and ABI in type 2 Diabetes Mellitus found the following results (link).[i]
Method
Sensitivity
Specificity
PPV
NPV
Pulse oximetry
74.1%
95.7%
83.3%
92.7%
ABI
70.3%
87.1%
61.3%
91.0%
These data suggests pulse oximetry signal is equal to and somewhat better than ABI. Why is this important? Cost. This information is better than asking unsure people, “Is there a pulse?” A vascular technologist need not be on call 24/7. Extra FloLabs for ED, ICU, and floors need not be purchased. The pulse oximeter with waveform tracing is nearly ubiquitous wherever patient’s oxygenation needs to be assessed in most hospitals. While not perfect, it has great potential for serving as vascular surgery’s EKG machine for critical limb ischemia. Policies and algorithms can be built out in collaboration with Emergency Departments and nursing departments that can effectively determine if blood flow is normal or abnormal at point of care. Effective emergency responses to critical limb ischemia can be authored triggered by abnormal findings. Acute limb ischemia protocols based on time sensitive responses can be initiated. All of these can flow from referring entities being able to determine objectively normal or abnormal blood flow.
Clinic
The vascular clinic is a sorting process where patients are determined to be normal or have mild, moderate, or severe disease. The vast majority of the time spent in clinic can be spent in triage by trained nurses and testing by technologists. Clear pathways and guidelines can dictate the ordering of vascular laboratory tests obviating the need for vascular consultation at this stage. Patients with normal blood vessels and vascular function are sent back to their physicians with the normal report. Patients with mild disease and moderate disease are sent to a physician with specialization in cardiovascular medicine for management of risk factors and periodic surveillance. At any point in the process, a vascular surgeon can be called to provide guidance and direct patients to different tests and consultations. The patients needing operations, based on correct indications and imaging are sent to a focused clinic where the surgeon and interventional team can review films, determine the urgency of indications balanced against risk, and plan and schedule procedures. Currently, vascular surgeons do all of this by themselves, as well as make hospital rounds, perform procedures, and interpret vascular laboratory studies, seeing one patient at a time.
In introductory computer sciences courses, search algorithms are taught to be brute force if you look at one item at a time for the thing you want, and to be efficient if you have presorted those items because every time you look, you can exclude part of the data set, ever shrinking the pool in which you search, making the search shorter and faster
The shortfalls in vascular surgeon numbers have as much to do with this dependence on the star chef cooking up one meal at a time, rather than a team working off recipes, with the chef directing the flow and occasionally jumping by the fire to make the most difficult of dishes. The first restaurant can seat three parties. The latter, easily ten times the number. Everyone gets fed.
Only asking how many vascular surgeons you need misses the big picture because there are many equally important questions. How many vascular technologists do you need? An accredited laboratory provides the critical diagnostics upon which decisions are made, and the surgeon should oversee but not be directly involved in the initial screening. Nurses trained to triage and order vascular laboratory tests and even perform the simpler ones is the second need. Third, is the cardiovascular medicine physician who manages those patients discovered to have mild to moderate disease, and depending on symptoms, refers severely symptomatic moderate disease and severe disease to a scheduling clinic. The scheduling clinic is composed of both interventionalists and vascular surgeons who plan interventions and operations.
Surgeons must be in the operating room to be effective. A well thought out and organized system, with interlocking teams, and well disseminated basic knowledge and awareness of vascular diseases reduces the need for a vascular surgeon to be present all the time in many places and ultimately increases the effectiveness of the vascular surgeons that are available by keeping them in the operating room. The system needs to be set up by the surgeon to allow clinic to be a setting mostly for consenting the patient for an operation or a discussion of treatment options.
Finally, vascular surgeons must be aligned with all the resources of the hospital including the considerable numbers of interventional cardiologists and radiologists, neurologists, and nephrologists. There is no reason someone should wait a month to get on the OR list for an iliac angioplasty and stent if an equally skilled and privileged cardiologist or radiologist has an opening the next day. The surgeon’s special talent should be open surgery and hybrid surgery -that which mixes open surgery and intervention in optimal measures which is not possible from a purely percutaneous approach. The key is frequent and easy communication between specialities and trust built by being in one shared cardiovascular institute.
Execution
There is a critical need of good operators. The acuity of disease and their solutions demand the continued presence and availability of open surgery. The fact is, many solutions are optimal in a hybrid fashion and for peripheral vascular disease, these options can only be offered via a vascular surgeon trained in both open surgery and peripheral interventions, or in a combined effort of open surgeon and interventionalist. And many disease categories can only be managed by open surgery.
The reality is that silos, economics, and practice patterns prevent this kind of combined effort. Market forces have pushed the training of vascular surgeons forcefully into the interventional realm at the cost of open surgical training. Some of the geographic maldisdribution of vascular surgeons has to do with younger vascular surgeons flocking to established practices where there are senior surgeons more comfortable in opening a belly or chest (or both). The trap they and hospital systems fall into is then allowing these new recruits to become the interventional specialist of that group, relegating the aging open surgeon to a narrow role, and then finding that the hospital has a problem when that surgeon announces retirement at 60. Every year, millennia of surgical experience retires to beaches and golf courses. The hospital systems should recognize this brain drain as a crisis and create work arounds that keep these skills going. The other opportunity lost is close coordination with interventional cardiologists, radiologists, and nephrologists who in many cases compete with vascular surgeons for the same patients but treat the patients based on their training and skill sets to the exclusion of potentially better operations offered by surgeons. This disjointed care creates both suboptimal outcomes for patients and high costs for hospital systems.
Commerce should never dictate the fate of a patient. A particular point is where competencies and privileging overlap, and guidelines recommend intervention over surgery as in the case of a TASC A or B iliac artery lesion. A patient should not be kept waiting weeks for a spot on a busy surgeon’s OR schedule when an open interventional cardiologist or radiologist slot is available for a iliac stent the next day. It should be a matter of practice that these cases are discussed and distributed, optimally in a shared indication clinic or rounds. Patients bumped off of a surgeon’s elective schedules for emergencies who could be cared for by an interventional partner without an added delay should be given that option. This kind of change requires a commitment to continual reorganization and optimization into a vascular institute.
Conclusion
The perfect vascular surgeon is a unicorn -well skilled, and experienced in open vascular surgery, but also versatile, innovative, and skillful in wielding a wire. I can name just a handful of unicorns. An apt analogy from the book Moneyball is the signing of superstars in baseball on the free agent market. The upshot of that book is that you can arbitrage for the valued metrics through signing several utility players with an aptitude for one thing or another which in sum equals or exceeds that superstar and get the final result -wins, in the same proportions as overspending on a superstar. Rather than searching for that unicorn, it is more important to set up the right system. Screening, testing, and management of mild vascular disease by a nurses and cardiovascular medicine physicians, while directing operations and interventions to vascular surgeons, cardiologists, and interventional radiologists should be the next step in the evolution of vascular care systems. There will never be enough vascular surgeons in the current system. The critical and rare competency is open vascular surgical skill. A surgeon who performs only interventions is not an “advanced minimally invasive practitioner” but rather someone equally privileged as an interventional cardiologist or radiologist, and therefore easily replaceable by an interventional cardiologist or radiologist specializing in peripheral vascular disease. A surgeon skilled in open vascular surgery is becoming rarer every year, but they are still out there, looking at brochures of real estate in sunny places. A team consisting of a cardiovascular medicine physician, many vascular technologists, nurses specializing in vascular diseases, several interventionalists, and a vascular surgeon skilled in open vascular surgery working as a single unit, is far more easy to assemble than finding and recruiting a herd of unicorns.
The patient is a gentleman from out of state who had called about problems he was having with walking and with leg ulcers that wouldn’t heal. He is in his seventies and has a pacemaker for an arrhythmia for which he was on Xarelto. He also had type II diabetes. He had bilateral lower extremity deep venous thromboses 6 years prior requiring IVC filter placement. The filter occluded, and it resulted in sudden sharp and debilitating pain in both legs with walking short distances -some days only 50 paces.He described it as an unbearable pain in calves and thighs that felt like his legs were going to burst. He also had ulcers on his legs that would heal with ministration but soon recur. This was all despite being quite active, with regular workouts, and being fit. He was compliant with compression. He sent a CT scan done last year (below).
Right iliocaval centerline projection
It showed an Optease retrievable vena cava filter that was occluded and the iliac systems bilaterally (right above and left below) were chronically occluded with patent vena cava above and femoral confluences bilaterally below.
Left iliocaval system showing chronic occlusion on centerline projection
He had no hypercoagulability nor ongoing recent DVT’s. I thought there was a good chance that we would be able to recanalize the occluded iliocaval segment and he flew in for a consultation, and he was pencilled into the schedule ahead of his visit.
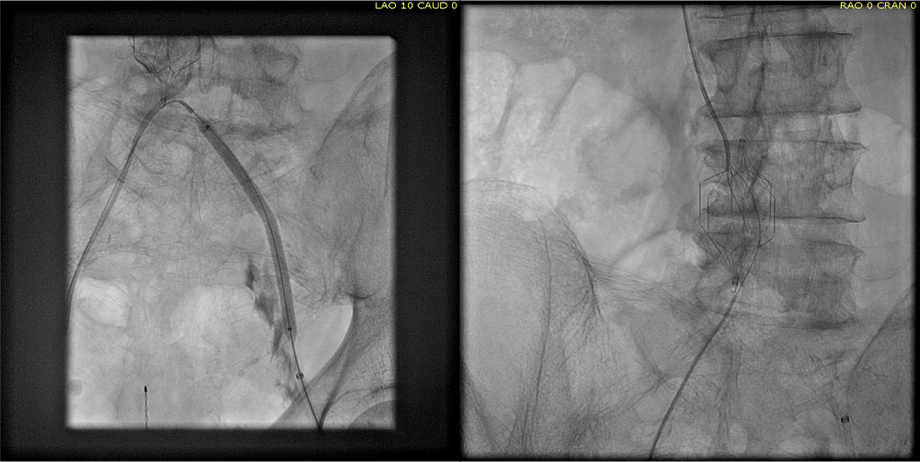
Examination revealed a fit and trim man in his 70’s in no apparent distress. He had bilateral leg edema that was moderate with small superficial and tender ulcers of the right posterior distal calf. Pulses were normal. He was taken to our hybrid suite and venography from femoral vein access in the proximal thigh in the supine position revealed his right and left iliac venous systems to be occluded (below figures).
Right injection from femoral sheath showing occluded iliac vein with collaterals
Left injection
Wire access into the iliac systems was performed with Glidewire and Glidecatheter periodic venography to confirm that I had not exited the vein. Unlike the arterial system, extravasation from being extravenous does not have the consequence of bleeding, hematoma development, and pseudoaneurysm formation because of the low pressure, but it can be a long procedure and uncomfortable as well so these are done under general anesthesia.
Advancing wire and sheath into iliac vein, crossing filter resulted in extravasation of contrast
Once position confirmed to be in the iliac vein, the vein was dilated to allow for greater ease of movement. In the case of the uncrossable filter, I switched to access from above via a right internal jugular vein access.
Dilating vein (left) for greater mobility, and crossing from above (R. IJV access)
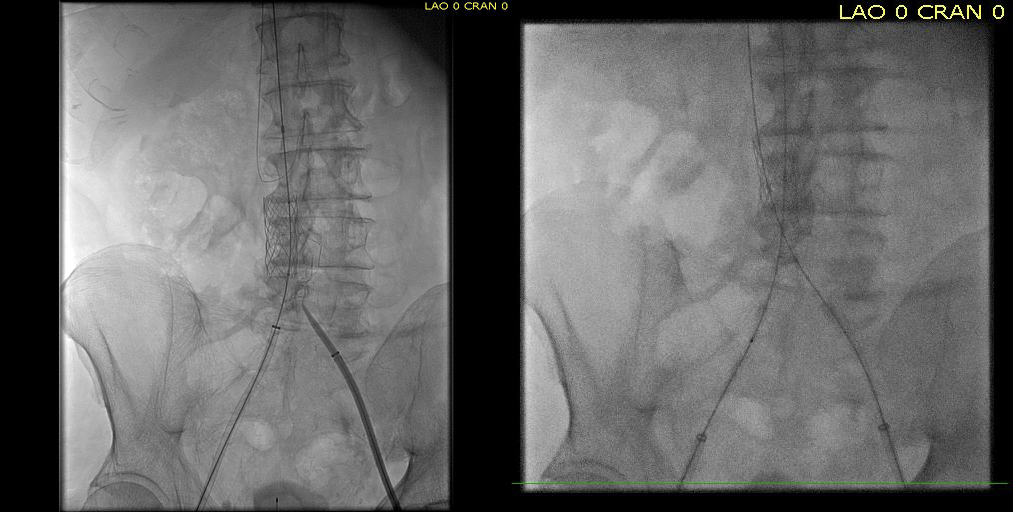
Once the wire crossed into the iliac vein from above, it was captured and brought out. While ballooning by itself is inadequate for revascularization, it greatly eases wire capture and on the right, it was done simply by driving the wire from above into the sheath. Wire capture wins access across the iliocaval and IVC filter occlusion from below.
Wire passage across IVC filter into right and left systems
Once wire access is done, ballooning across the filter is done from both sides. A large sheath is them delivered across the IVC filter. Finally, a Palmaz stent mounted on a large balloon is delivered and deployed. I chose to do this from the right access, and retracted the wire on the left -something done with some trepidation because of the great difficulty gaining this access, but with with prior balloon dilatation, reaccess is made easier. Also, plan B would be reaccess from above.
After balloon dilatation of occlusion typically to 8mm from both sides, a sheath placed and Palmaz stent deployed across filter on a large 24mm balloon
When this is accomplished, the left sided wire is reaccessed across this stent. This is the venous side analogue to gate access in EVAR (below).
Reaccess of the left iliac venous wire across Palmaz stent
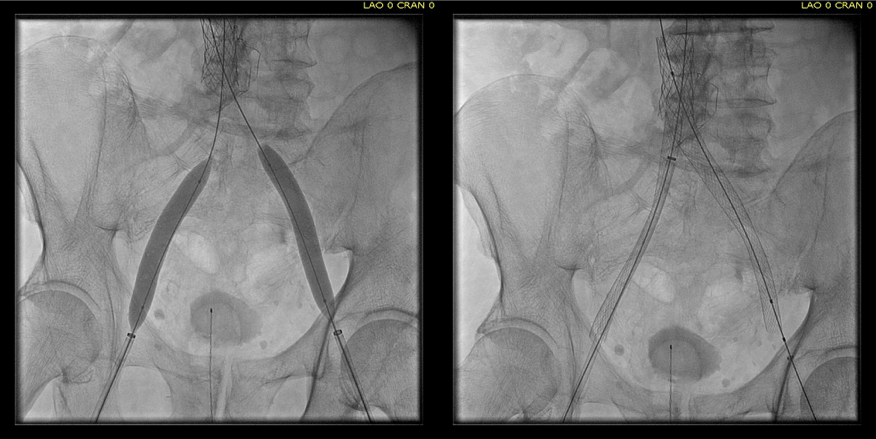
Once this is done, the iliac veins are dilated to 14mm from the IVC to the common femoral arteries. large 18mm Wall stents are deployed in a kissing fashion from the caval stent into both iliac systems and dilated to 18mm.
Predilatation of iliac venous systems with ever larger balloons, deployement of bilateral 18mm Wall Stents
After deployment, the Wall Stents are ballooned to 18mm. These stents were extended into the common femoral artery with 14mm nitinol stents.
Ballooning 18 mm Wall Stents with 18mm Atlas balloons, then extending to CFA with nitinol stents of 14mm
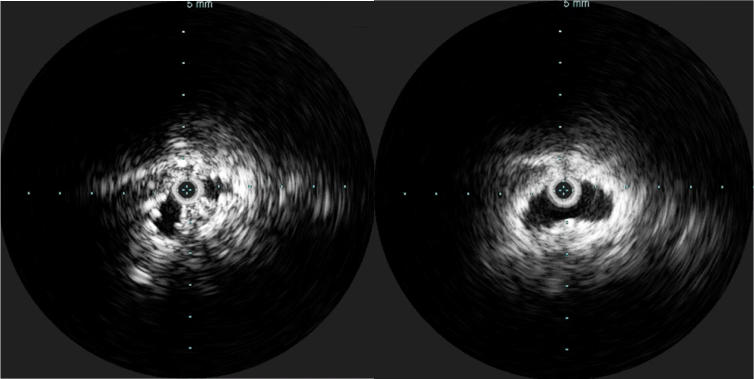
Completion venography suggested successful iliocaval recanalization and revascularization but these procedures are not done without a final intravascular ultrasound (IVUS).
Looks done, but needed final intervention after IVUS.
Intravascular ultrasound revealed incomplete expansion of the right common femoral stent. This was treated with another stent and ballooning with the result on the right.
Stent compression on IVUS treated with second stent
Venography alone is insufficient in determining patency. As illustrated, IVUS ensures a durable outcome.
The leg ulcer was treated with an Unna’s boot. A word about the venerable Unna’s boot –it works. The dressing dries and compresses while the Zinc Oxide prevents bacterial growth. It is interesting that the dressing is so infrequently used nowadays but not so when you consider that it isn’t reimbursed. And patients generally hate it.
This revascularization has an excellent chance at working as the patient has no hypercoagulability and had a patent common femoral confluence bilaterally. As I had mentioned in a prior post, the idea in venous revascularization is connecting confluences that serve as inflow and outflow.
This will require followup, consisting of duplex, and it is advantageous that he is anticoagulated for his arrhythmia. It is becoming more apparent that those languishing with chronic venous insufficiency and its complications need the IVC and iliac veins interrogated with a duplex. When an obstruction is found, they should be treated with these techniques as a first line therapy.
Max Wohlauer, a recent graduate, is now Assistant Professor of Surgery at the Medical College of Wisconsin in the Division of Vascular Surgery. He sent along a case which is published with his patient’s and department’s permission.
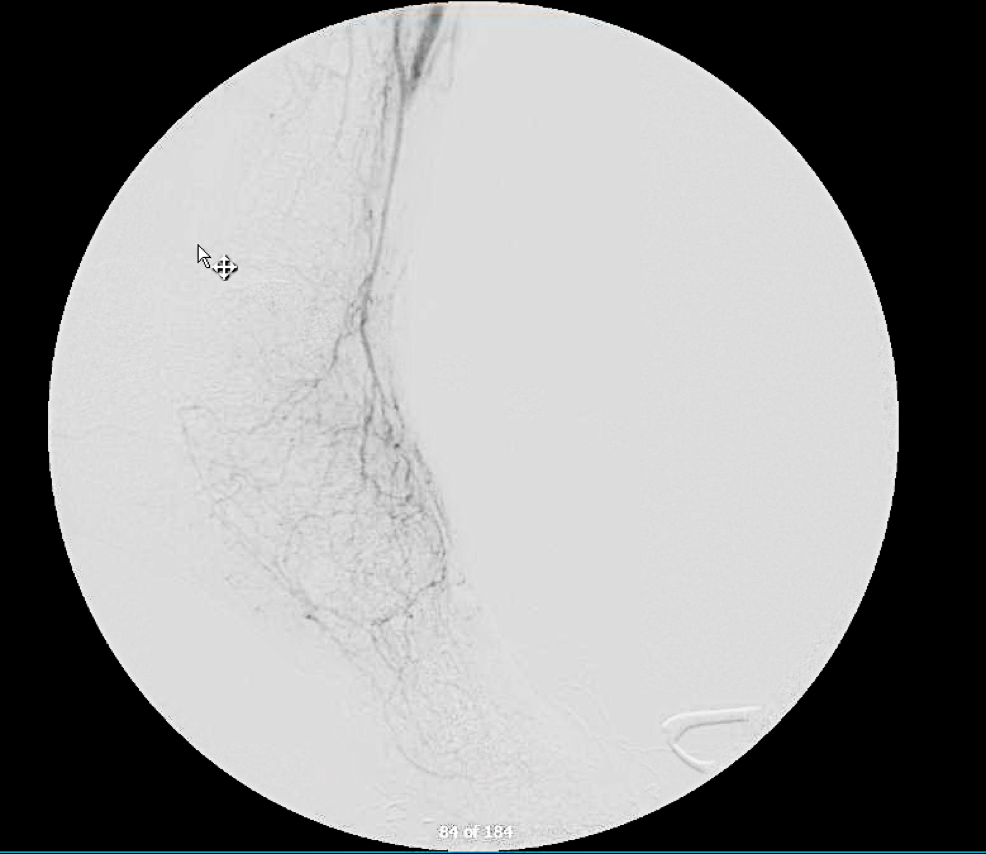
The patient is an 80 year old man with diabetes mellitus, CHF, and pulmonary fibrosis, who presents with right foot toe ulcers. He had an inflow procedure earlier in the year, but it failed to heal the ulcers. An attempt at crossing a CTO of the SFA/POP failed. Angiogram (above), showed a distal anterior tibial artery target.
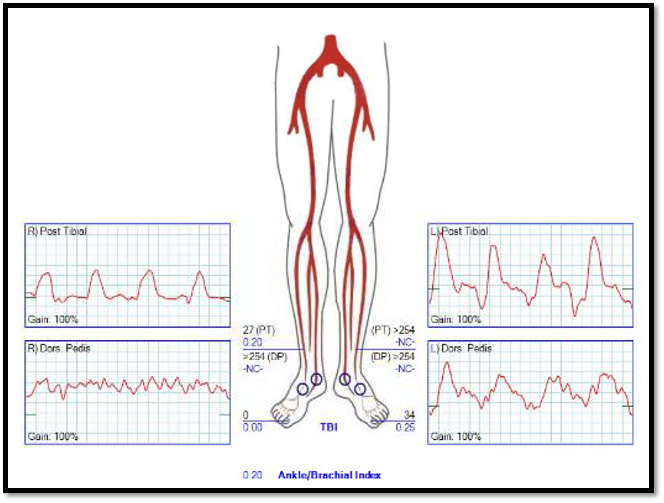
Preop ABI, TBI’s, toe waveforms, and pulse Dopplers are shown. are as shown.
All point to likely limb loss. The TBI is 0 and the ABI is incompressible. Max planned for bypass. The saphenous vein was mapped and shown to be adequate.
Max comments:
Compromised runoff on angio. Cutdown on AT and determined it was adequate target at start of case
Right fem-AT bypass
Re-do groin exposure
Translocated non-reversed GSV
Subcutaneous tunnel
The operation went well. Completion angiography was performed showing a patent bypass and distal anastomosis with good runoff.
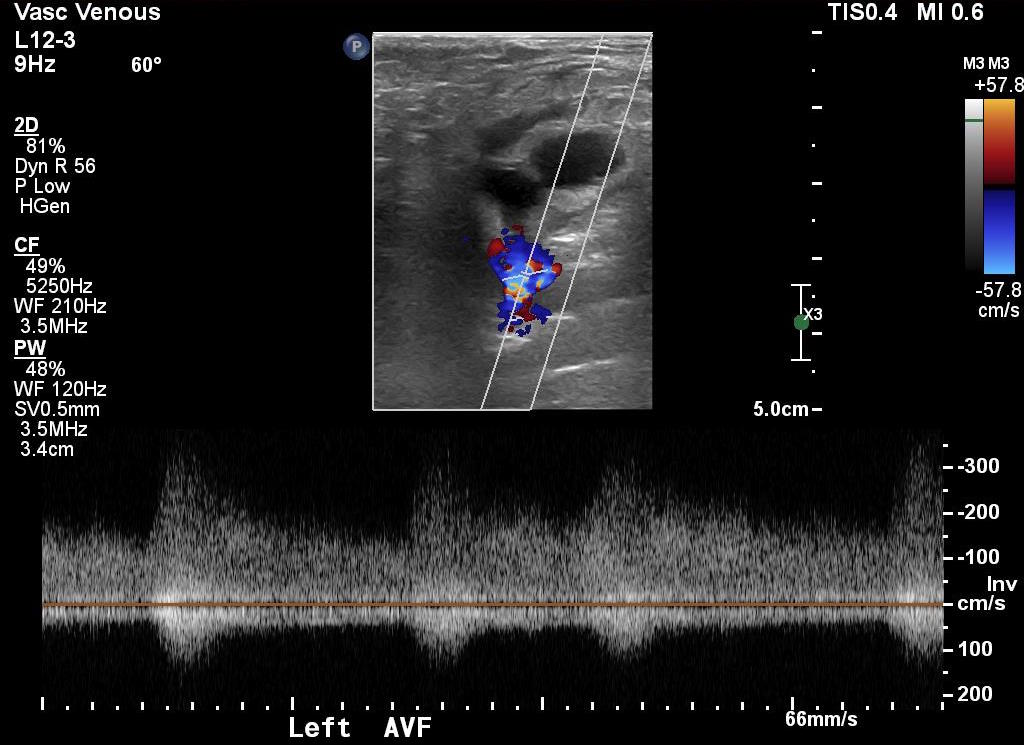
A followup duplex showed patency of the graft.
Postop ABI’s showed excellent results:
Commentary from Park
Bypasses work and are possible even in high risk individuals with good anesthesia and postoperative care. Because open vascular surgical skills are not well distributed while endovascular skills are more widely distributed, there is bias both in the popular mind and even among some catheter based specialists that bypass surgery is a terrible, no good thing. The fact is that a well planned bypass is usually both effective and durable even in high risk patients, but clearly it is not the only option.
Ongoing developments in endovascular technology bring greater possibilities for revasularizing patients. As someone who does both interventions and operations, I have seen spectacular success (and occasional failure) with both approaches, and I admit to having biases. It is human nature to be biased, but it is because of my biases, I support further ongoing study, as the mistake would be to establish monumental truths without supporting evidence. There is an ongoing randomized prospective trial (BEST-CLI) that aims to answer important questions about what approach brings about the best results in critical limb ischemia. It will bring evidence and hopefully, clarity, to this important disease.*
Finally, I am very proud to have participated in Dr. Wohlauer’s training, and look forward to seeing his evidence, experience, and even biases, presented at future meetings.
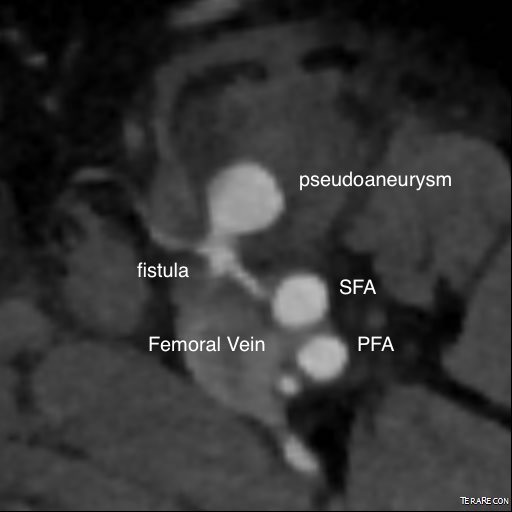
The patient is a middle aged man who after an interventional procedure was referred to my clinic with an expanding hematoma due to a pseudoaneurysm complicated by an arteriovenous fistula. He was a week out from his procedure and had grown a hematoma roughly the size of a hard boiled egg in his left groin which caused him pain. A duplex scan showed a pseudoaneurysm (below) with fistula flow.
On examination, he had this well circumscribed indurated hematoma of hard boiled egg size with tenderness. There was a bruit on auscultation. Duplex showed a small chamber of flow adjacent to the proximal superficial femoral artery emptying into the femoral vein. Doppler in the common femoral vein showed relatively high fistula flow, and this is reported to be associated with failure of thrombin injection. CTA (top) demonstrated flow of contrast from femoral artery to vein through a pseudoaneurysm chamber that laid between. Angulation to an axial orientation showed this better (below).
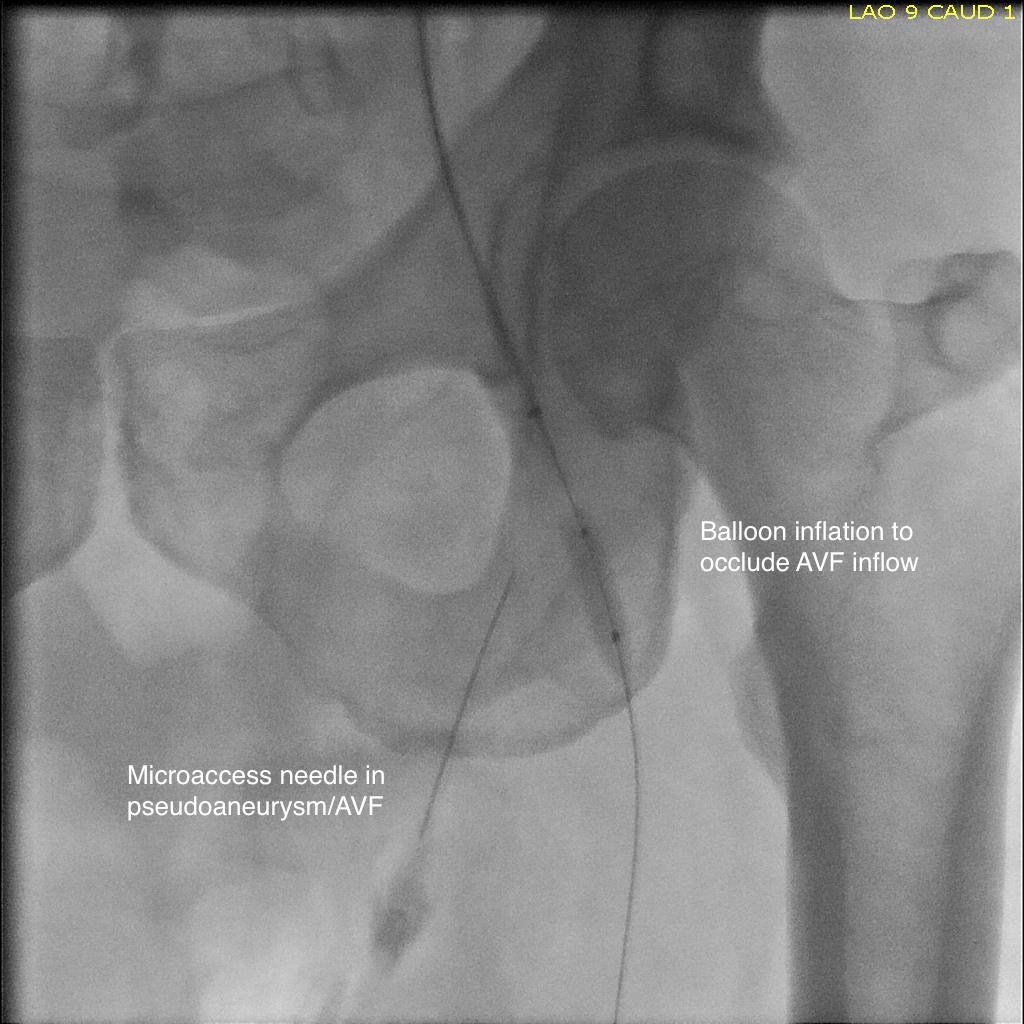
Contrast flows from femoral artery (right) to the fistula chamber, then into the femoral vein. Axial MPROperation was planned, but in the days leading up to the operation, I had a thought -the primary reason why ultrasound guided thrombin injection would fail is the AVF. It would be simple to fluoroscopically guide an angioplasty balloon on the arterial side to occlude the fistula inflow. The next step would be to get access to the pseudoaneurysm with a needle under ultrasound guidance, confirm location with a contrast injection. Once confirmed, the balloon is inflated and a small volume of thrombin would be injected. I discussed this with the patient in detail and he was enthusiastic about trying this before proceeding with an open repair.
Schematic of procedureThe procedure went as planned. Ultrasound guided access is aided with dual live display of B-mode and color flow (below)
Arteriography showed much of the contrast from injection of the pseudoaneurysm to preferentially go to the artery which made me worry less about creating a DVT/PE. With balloon inflated (below), thrombin was injected and balloon inflation held for about 30 seconds.
There was resolution of flow in the pseudoaneurysm and in the fistula. Before and after duplexes are composited below.
Repeat duplex on the following day showed resolution of the pseudoaneurysm and arteriovenous fistula.
In the days before ultrasound guided thrombin injection of pseudoaneurysms, open surgical repair of these was fraught with complications. First, these patients typically had cardiac disease. Second, they were usually anticoagulated often with multiple agents. And finally, they were many times obese, making not only the operation fraught with complexity, but the ultimate wound healing a delicate and rare phenomena. Even now, we get emergency repairs when access hemostasis fails, and these patients are typically high risk. With hematoma evacuation, inflammation, lymph leaks, and infections may follow; the patient was correct in his enthusiasm for agreeing to proceed with a minimally invasive effort.
As to the techniques, they are all well established in the vascular surgeon’s toolbox. Ultrasound guided access of the pseudoaneursm should be obtained before arterial occlusion. This was facilitated by general anesthesia which kept the patient from moving. Having access to excellent ultrasound and angiographic imaging made this possible. The patient felt much better and was discharged home the next day after his confirmatory duplex.