In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.
Reading this article on Vascular Specialist, the vascular surgeons’s Daily Prophet, “Likes, dislikes and reposts: The new age of the vascular surgery influencer” by Drs. Jean Bismuth (@jeanbismuth) and Jonathan Cardella (@yalevascular), they rightly point the spotlight on the trend of some vascular surgeons posting cases on social media for the purposes of self-promotion, virtue signaling, and influencing.
I can agree with their point that many of these posts are made by mediocre practitioners who display only the best and curated images, but I felt uncomfortable with the feeling that I may be one of those people being castigated for over-exposure on social media. They warn the readers of the dangers of misinformation fed to an uninformed public, but overlook the potential of social media for education and community. Being a vascular surgeon who has been on social media for over a 15 years, there are reasons why I am here which are not explained by this article, and I am compelled to elaborate on them.
Be the Lede
My journey started with hacking Google searches. My first job out of fellowship was a faculty position at my medical alma mater, Columbia P&S. The PR department asked everyone to compose a blurb for a web page and after searching on Google on how to rise in a Google search, I wrote out a paragraph full of the right verbiage to maximize my relevance on search. It wasn’t very difficult in 2002 to do this. Searching “vascular surgeon in New York” on Google after posting that info page consistently brought me up to the top five links, ahead of whole departments and many big names. I did over 400 cases my first year out, and I really felt if I could make it there, I could make it anywhere.
Bury the Lede
Unfortunately, like many vascular surgeons in New York, I got named in a lawsuit, and like many young surgeons with limited means and large loans to pay off, I couldn’t fight it and took the advice of hospital lawyers and settled. After that lawsuit, a Google search would return an article by the law industry PR around 2007, and I was at that point very busy in private practice in Iowa. It was so discouraging seeing that as the only thing speaking for me. I decided that I had to take an active part in shaping the message around me, to not let my Google search profile be defined by that article.
I decided to write and figured a few articles every week over a year would bury that article behind many better articles. I began to blog about something I am both horrible at but aspire to greatness in –golf (www.golfism.org). Writing about myself and my struggles in golf and being a young father and husband was how I found my voice. It was during this period that I found my best pieces were when I gave something of myself.
After finding my author legs, I began writing about vascular surgery, something I’m pretty good at but aspire to greatness in, on a personal blog (docparkblog, on Apple’s defunct cloud service). After a year, the blog got only 30-50 hits a day, at most 100. By internet standards, that’s low, and I kept my day job. After giving a talk at Midwest Vascular to an audience of about 50 mildly interested surgeons, that 30-50 engaged readers on my blog a day felt pretty good. A hundred was amazing. Medscape eventually tapped me for blogging on their site. My blog there, “The Pipes Are Calling,” was rated among the top 5 most read medical blogs in the world when I shut it down in 2011.
The Influencer
This social media presence generated influence -I was asked to participate in prominent research trials like PIVOTAL, CVRx, and CREST and others despite being in private practice. This is common now, but rare 15 years ago. The blogging did bury the lede. It eventually generated misunderstanding in the hospital administration at that time in 2011 and I was asked to stop blogging, at least until they could figure out what this internet thing was about. In 2012, I joined the Cleveland Clinic, I huddled with their social media department and came up with ironclad rules:
All accounts were to have the header that posts and articles were my own opinion and not of my employer
All patients sign a media release for posting of case histories and images
After launching www.vascsurg.me in 2013, I chose to focus on technique and opinion. I used my Linked-In and Twitter accounts to promote my articles. I always communicate in my authentic voice, although over the years, I’ve toned down the irony which is frequently misunderstood. In moving to my current hospital, University Hospitals, the first thing I did was arrange for a social media release and confirm what I was doing was okay. In reading the article by Drs. Bismuth and Cardella, in 2023, misunderstanding is still at the core of arguments against the use of social media.
The Worst
I have seen egregious examples of bad behavior on social media by physicians, as mentioned in the article. On my Twitter stream, I’ve seen people put stents in subclavian veins for thoracic outlet compression and wait for praise, which they get from similarly ill informed people who don’t realize I see patients like this several times a year with swollen arms and faces. While I was in Abu Dhabi, someone put stents in a patient from the common femoral to popliteal artery, and receive accolades for “minimally invasive skills” from all corners of the globe, only for me to remove the stents a month later and perform fasciotomies on the same patient -a middle-aged claudicator! There, I couldn’t post a rebuttal to the original case presentation because of local social media laws. Despite the word getting out, the surgeon only doubled down on his minimally-invasive fantasies. About the same time, I witnessed a relatively famous person self-implode on Twitter while accusing vascular surgeons of butchery (his words) by supporting open surgery over head to toe interventions. He got crushed by the general disapproval of his misrepresentation and personal bullying of a vascular surgeon, and then disappeared from social media. Evaporated. Good. We all have to do better.
The Best
I have also seen patients with rare diseases such as median arcuate ligament syndrome reach out and connect with each other and with physicians about diseases that aren’t taught in medical school or residency training on social media. There are Facebook groups, Twitter hashtags, and sub-Reddits, a rich communities of people who have to make serious decisions about their lives, many with limited access to specialists in their far-flung burgs and precincts. I think the fear is that bad decisions will be made based on bad information, but even in the highest, most rarified medical institutions, patients may get misguidance, have a complication, a poor outcome, in-person which can be worse than a social media interaction. If we value patient autonomy, access to the best information needs to be available. Social media lowers the barriers to access, for bad or good. Yes, it can do a whole lot of bad, but also an immense amount of good.
Keeping it Real
The authors are correct in that people will prefer to promote themselves rather than air complications and bad outcomes. The American surgical M&M process is an amazing and cherished tradition and protected process. It has no place in social media. Most surgeons also take the view that social media presence doesn’t lengthen your CV, it doesn’t bill. The many cheap suits of medical social media, the hawkers, the hucksters, the fragile egos will always be there on Twitter and Linked-In.
But other functions such as access and broad dissemination of information, experience, and opinion, are legitimate and critical. Comparatively few people get the message from a closed academic conferences and traditional modes of dissemination are slow. Most of the best social media posts are, as the authors mention, case reports. They fail to mention case reports under “open access” cost about 500USD to publish.
The peer review process, which I participate in, results in sometimes glacial turnaround times with papers landing often a year or more after presentation at a conference. I also learned from my time in private practice that these barriers block the voices of many legitimately great surgeons whose remarkable talents are only shared locally. I also learn from my time in academic practice that too many departments are not multiplicities of talents (Avengers Assemble!), but shops built around single personalities, who may declare that having never seen something, it cannot exist -to the detriment of those with unseen problems. Social media is the great leveler. Young surgeons can raise their profile, and non-academic surgeons can have a broader platform to share their expertise. If legitimately good people are dissuaded from participating, only the cheap suits will remain. As always, caveat emptor, et primum non nocere.
There was an OpMed article on Doximity (https://www.doximity.com/newsfeed/1946e8dd-eddc-4eb4-aad6-46fe59c86da5/public) which reports that 69% of 58,000 physicians surveyed said they would provide emergency care. That number is depressingly low at first view but can be answered by asking how many of us are ATLS, ACLS, or BLS certified? A quick search fails to give a result, although various pro CPR groups have on their websites that all caregivers should be trained in BLS. The darker question is how often do fully trained and certified physicians choose to withhold care and hide their identities?
I can give you a quick answer. Most doctors will sit on their hands when the PA announces “is there a doctor on the plane?” hoping that someone else will raise their hand. Back when I was a second year surgical resident, I took a vacation with my wife to London and Paris. On the flight, over the Atlantic, the cabin crew asked for any medical assistance. Before I had a chance to contemplate the question my wife jumped up and pointed at me and shouted “He’s a Doctor!”
I was in shorts and hoodie, with a baseball cap. Back then in my late twenties, I looked about 15 years old. The British Airways stewardess looked at me dubiously, then looked around behind me to see if any other hands were raised. <sound of crickets>
She escorted me up the stairs to first class and in one of the giant chair-and-a-half recliners was a pale fellow in a nice suit, diaphoretic, dyspneic, and maybe a little drunk. He couldn’t speak well but was awake and maintaining his airway. His radial pulse was thready and weak. I pressed the button that fully reclined him into a bed, not a little jealous.
“Are you having chest pain?” <head shake>
“Do you have pain anywhere?” <head shake>
“Are you diabetic?” <¯\_(ツ)_/¯>
Cold, clammy, dehydrated, drunk -hypoglycemia was my diagnosis. I asked the stewardess if they had any tubing, a funnel, and orange juice -because that is how you deliver sugar to someone who can’t protect their airway. I was an enthusiastic PGY2 and the orange juice enema was one I was eager to roll out. She looked at me funny and handed me a large black leather suitcase -the kind you see sniper rifles disassembled and packed. In it was a pretty thorough crash cart with defibrillator, airways, Mac blades and handles, bag mask, IV’s, bags of saline, and boxed syringes of code meds including D50. Oxygen was available. It was British Airways first class after all.
I looked around and saw no great place to hang an IV, so I grabbed the D50, horse needle and all, and found his cephalic vein and injected the whole vial. The change was instantaneous -the eyes which were spinning beachballs, stopped wobbling and focused. All that was missing was that Apple Macintosh “bongggg” sound. I gave the fellow a gauze and instructed the stewardess to give him orange juice spiked with sugar.
“Shall we land?” asked the stewardess. The neighboring passengers, all dressed as if for a fancy cocktail party, looked at me with eyes that said, “We really need to get to London.”
“Where are we?” I asked.
“Over Reykjavik. The captain needs to know now.”
I look at my patient, and he had unreclined himself in his fancy leather loveseat, and shook his head. “Thanks. I’ve got to get to London for a meeting.” He was going to be fine. I recommended he see someone for his diabetes (which he confessed to neglecting), and I walked downstairs and back to my seat in steerage.
A older couple (I’m sure they were middle-aged like I am now) was next to us and the lady smiled, and the man leaned over and asked, “how did it go?”
“Hypoglycemia. Are you a doctor?” I says.
“Why yes, a cardiologist. We’re going to London for a conference!” he chirped. I think he caught that I was giving him an accusing look, and added, “you’re wife volunteered you so well, so enthusiastically, I figured you had it well in hand. Good job.”
I sat down and my wife immediately asked, “did you ask them to upgrade us?”
“No.” That is the advantage of a wife when she isn’t volunteering you for missions, she’s looking out for your interests. I was going to make some grand statement of my purpose in life, but was interrupted. The stewardess came up with a brown bag full of tiny bottles of liquors, spirits, and whiskeys, which made me very happy, but my wife just rolled her eyes.
“You would have been happy with a cookie,” she hissed. “Why didn’t you ask for an upgrade? What’s wrong with these people?” And I thought the same, for a different reason. Seated all around me were likely cardiologists headed to London for that conference. Just counting bald heads, there were at least twenty.
Now, nearly thirty years on, I don’t blame those fine folk for not being quick on the draw. I am sure one of them would have stood up eventually, but the last thing you want to do on vacation is work, and what I did upstairs in first class was not much different from the work I was doing every other night on call (this was 1995).
Now, in the middle of my career, there isn’t much that gets my blood running, so I empathize with the festive, sanguine attitudes of the many physicians probably on the plane with me, headed for a nice holiday and conference in London. Some happy fellow jumps up and takes care of the problem, so no need.
Also, I’m not shy in crowds or stressful situations. Everyone in first class was watching me get venipuncture with the D50 syringe and the horse needle which was easy because the fellow was so thin. At that point in my life, screaming HIV positive crack addicts fighting you while getting central lines and spinal taps were the norm. I suppose I couldn’t fault someone more bookish and scholarly for not standing up right away. I assume 69% would have.
I’ve been called about a half dozen other times on planes. It used to be my wife volunteering me, but over the years, even she has taken on a bit of a glazed attitude. The last one a few years ago was a poor fellow whose wedding ring was causing an ischemic finger, made worse by traumatic attempts at removing the ring. Soap and rubber bands fixed him. It barely elicited an eye roll from the spouse who did not volunteer me that time. It was one of those cheap airlines in the American Southwest and I got nary a thanks.
I have never contemplated the medical malpractice ramifications of rescuing someone, saving a life. I assume something like sea-law prevails up in the air, where the captain can marry folks and push them off gang planks, where decency, need, and common sense prevails over tort law. Unfortunately, I have never seen another black suitcase since that first time on British Airways, and the pre-9/11 days of carrying a pocket knife are long gone, making emergency surgeries and fashioning of MacGyvered medical devices impossible. The idea of embarking on supporting the life of someone when the last time you ran a code was in medical school may be too much to ask someone, and doing the wrong thing may be worse than doing the right thing badly.
Did you know you can fix a tension pneumothorax with a pen, a rubber band, and a condom, with the appropriate knife and fortitude, and maybe a tiny bottle of vodka.
But isn’t that why we went into medicine? To save a life is to save the world, the Talmud tells us, and we can be heroes, if just for one day.
At the VEITH Symposium, which I attended briefly last week, while I foraged for lunch and sought out friends, I wandered into a crab trap (diagram above). Or more specifically, the WL Gore exhibit hall (below).
The coffee and bevarages featured all day, and the steak buffet at lunch, draws people in, like the smell of chicken to a crab, and once you have a plate of food, you then are kind of committed to moving forward into the conference room where they have a video feed of aortic symposium and tables to gobble your lunch.
Like a hand reaching into a crab trap to retrieve the catch, the reps wander in and chat you up, but thankfully only if they know you, which is fine because any hard sales tactic would trigger a fight or flight reflex that would ruin the generally chill atmosphere. There are exits to the left because, you know, fire codes, but they are small, and going out the way you came in risked bumping people juggling plates of their lunch, cups of their coffee. So you go in, sit down, and nibble, watch someone you vaguely know up on the big screen who just decided to go full head shave bald (why is that a thing?), check your phone and find out your friends are in another trap on the other side of the center. And their doors are closed, invitation only. Silly crabs.
In no particular order, I list these problematic situations that are outsized in their ability to take a case sideways.
Ischemia syndromes in the unconscious. The unconscious tell you nothing about their pain and follow no commands. Therefore, vigilance and a low threshold for operating are what will save the patient if they are salvageable. Objective evidence of flow -examination, handheld pulse Doppler, duplex ultrasound, CT angiogram, exploration and visual inspection, must be obtained. The typical scenarios are dissections of the ascending thoracic aorta, polytrauma patients, and patients on ECMO. By the time the dissection is repaired and the patient is off pump, they may be long past the 6 hour threshold for irreversible ischemia for gut or muscles. The patient involved in a rollover MVA who had their femur fracture reduced after ten hours waiting on the add on schedule should have their compartments assessed visually through fasciotomies. Patients on ECMO via femoral access must by practice have distal perfusion cannulation. Assessment for ischemia need to start at admission for the unconscious patient with assessments of flow and function. Waiting until markers of cell death are apparent on blood tests is not the right approach unless the patient is DNR.
Operations in redo or irradiated fields. Preparation and coordination is key. Most vascular surgeons have a plan for controlling arteries and veins in these settings, but a common scenario is in trauma or oncologic surgery. I don’t know if anyone has done this, but the idea comes to me that if there is concern for oncologic invasion of a major artery -an aorta or iliac, it would be reasonable to place a wire, balloon, or stent graft across that area with solid seal zones to allow for free dissection and resection of any involved artery.
Central venous rupture during venoplasty for hemodialysis access with an open fistula. Instead of venous pressures, with a fistula attached, arterial pressure is driving the leak. A leak of an SVC can lead to a fatal cardiac tamponade. Because the heart fails to fill, CPR is futile. The only thing can be done once this has occurred is to be prepared to a. ligate the fistula, b. Drain the pericardium either with needle pericardiocentesis or left anterior thoracotomy. Better still is preparing for SVC venoplasty by balloon occluding the fistula prior to inflating the balloon in the SVC.
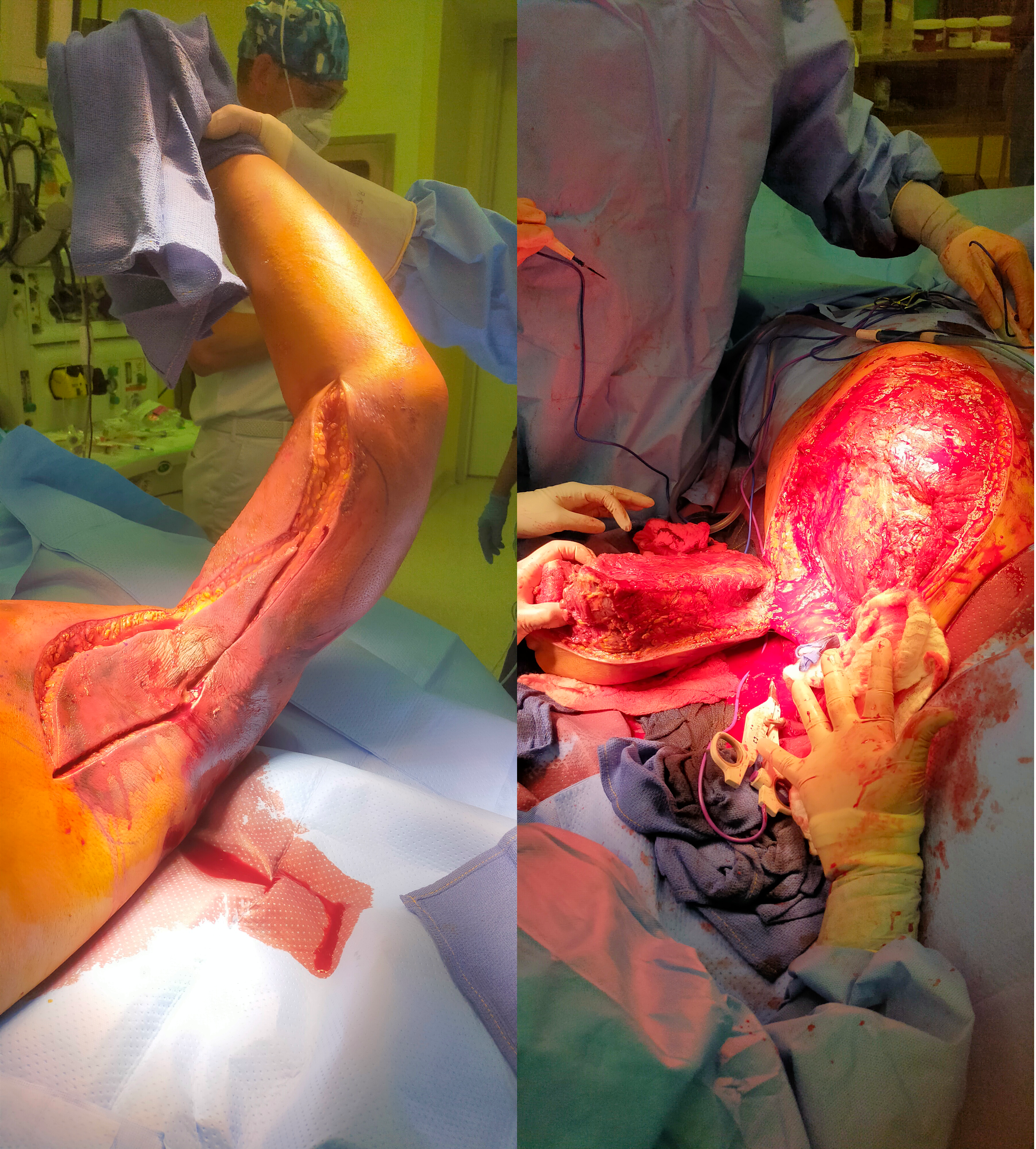
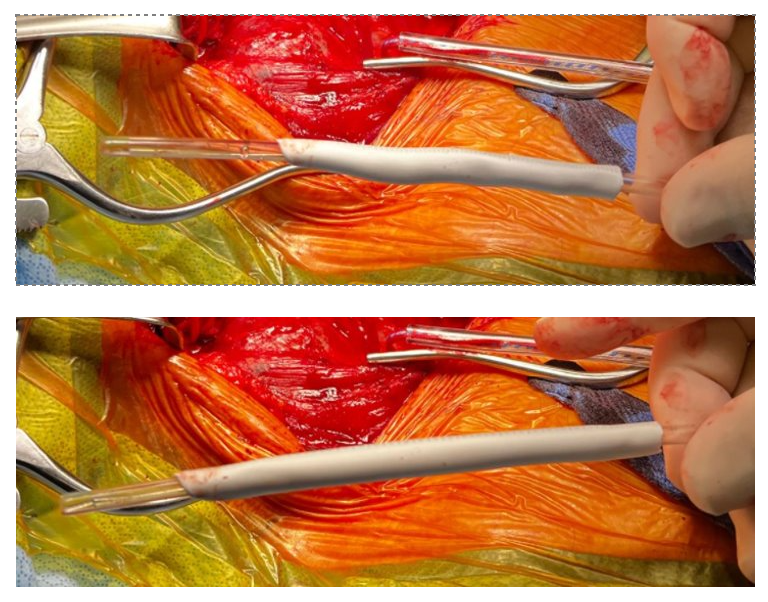
Rapidly progressing skin infections. It is amazing how fast necrotizing infections can progress. I’ve seen simple infections of a finger spread to the whole arm over the course of an hour or two in the waiting room of an emergency room. There are forgotten anecdotes of medical students dying after nicking their hands in gross anatomy. I saw a concert pianist lose her arm after getting a thorn from her rose garden. The image below is of a forequarter amputation I had to perform on a young man with a fulminant infection of the muscles of the left upper extremity undergoing a forequarter amputation after an overnight of misdiagnosis as a cellulitis at an outside facility. It grew among other things Candida auris, a terribly frightening organism and spread to his chest wall and ribs, resulting in death.
5. Iliocaval venous injury, particularly small tributaries going under aorta or around its branches. While not pressurized, they have tremendous flow like a hole in a plastic bag holding a goldfish, and without precise control, you are as likely to widen the hole or make more holes as you try to suture the holes. I’ve had some success using the Park clamp (link). You can’t buy one but you are free to have one made by your local smith. Otherwise, you need to keep your finger on the hole while you call in help, usually in the form of more vascular surgeons to get exposure and the vein properly clamped for repair.
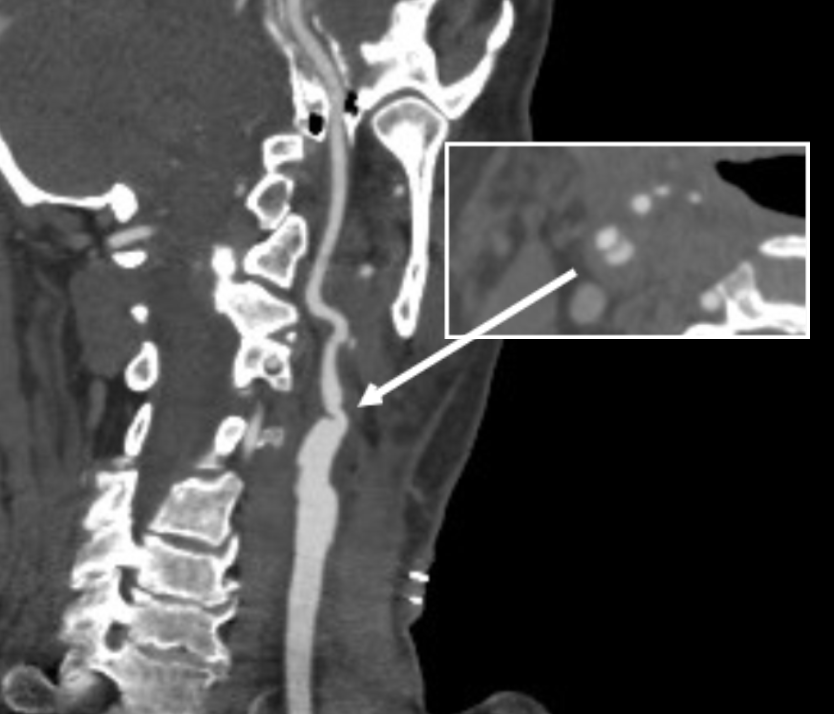
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
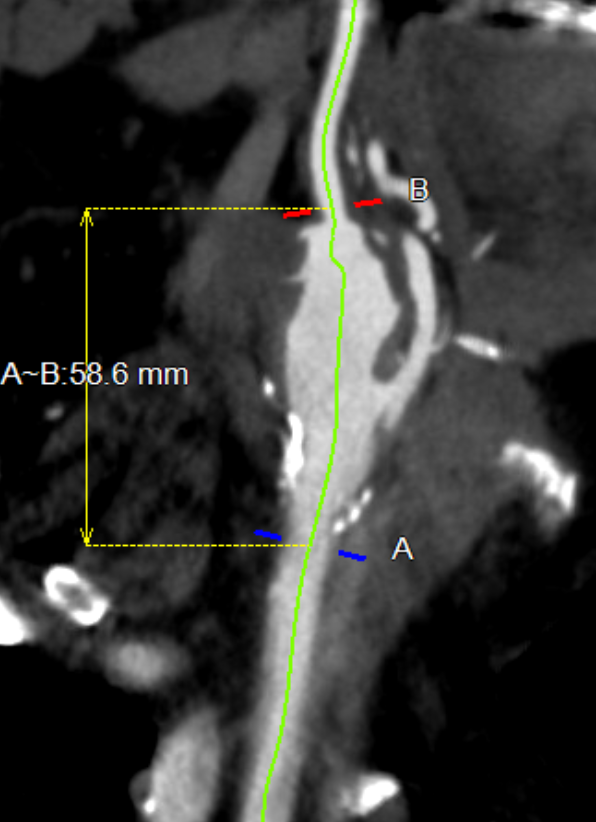
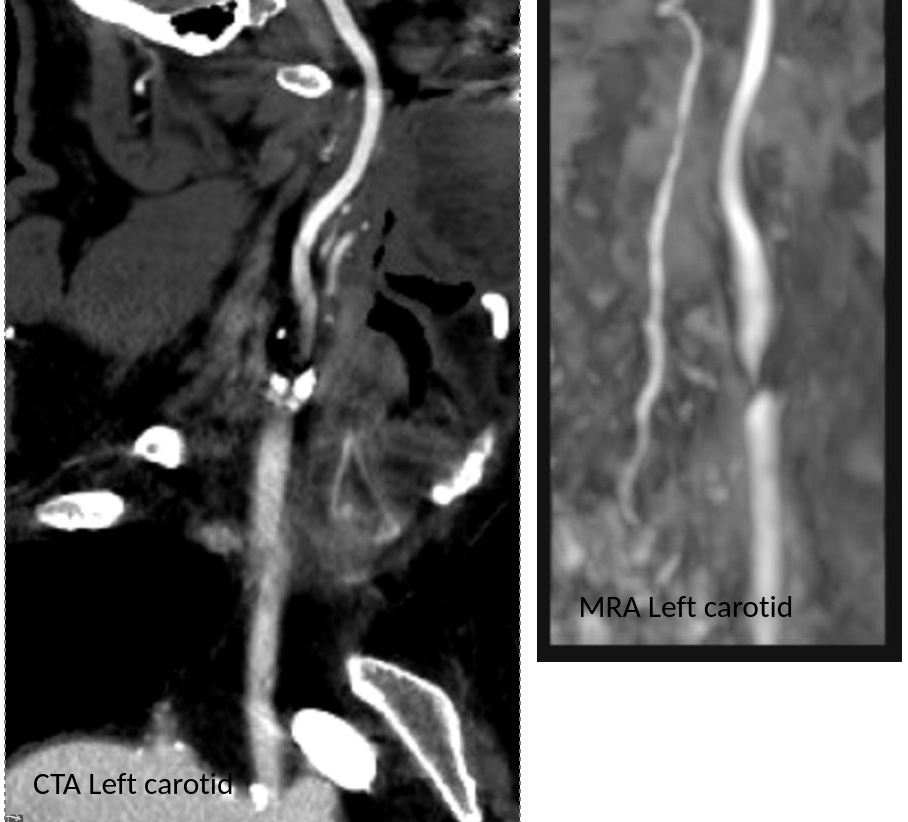
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
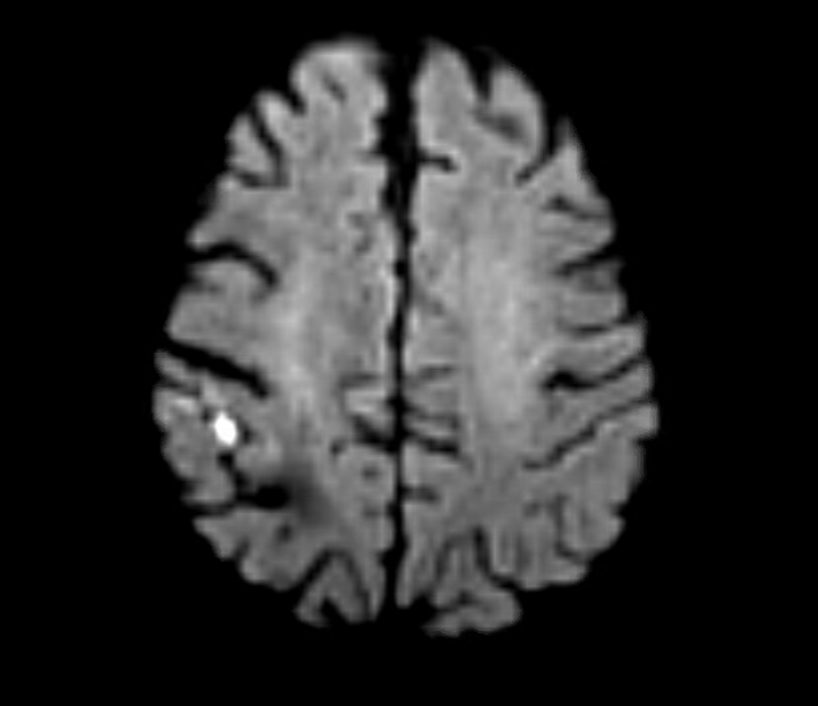
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
During a thoracoscopic lung resection, bleeding along staple lines, even of the main pulmonary artery, can be managed with a Park Clamp
The Park Clamp isn’t a true clamp, but rather a compressor. It was designed initialy for the troublesome venous bleeding. It is a ring with ridged edges to provide grip securely welded to a handle. It allows for circumferential compression of tissues, allowing for hemostasis while creating a open space for suturing. The picture above are my colleagues from CCAD -Drs. Andres Obeso and Redha Souilamas perfoming a partial pneumonectomy. The staple line on the artery was bleeding and this can be troublesome, and may require conversion to thoracotomy. The Park Clamp was inserted and provided excellent hemostasis (below).
Hemostasis achieved, a suture can be placed without ongoing hemorrhage without having to convert to a thoracotomy
During one of my cases as a fellow at the Mayo Clinic, I ran into venous bleeding behind the aortic bifurcation. Dr. Thomas Bower, recently retired, came in and lengthened the incision to create more space for more hands, and got all of us -me, the resident, the intern, the RNFA’s, to retract and compress with sponge-on-a-stick to repair the linear tear on the vena cava under the aortic bifurcation.
I’ve always hated this approach because outside of Mayo in 2002, it is very hard to get five people to become your voice activated retractor system, and the sponge on a stick only works well when you are on the hole and less effectively next to the hole. There had to be a better way.
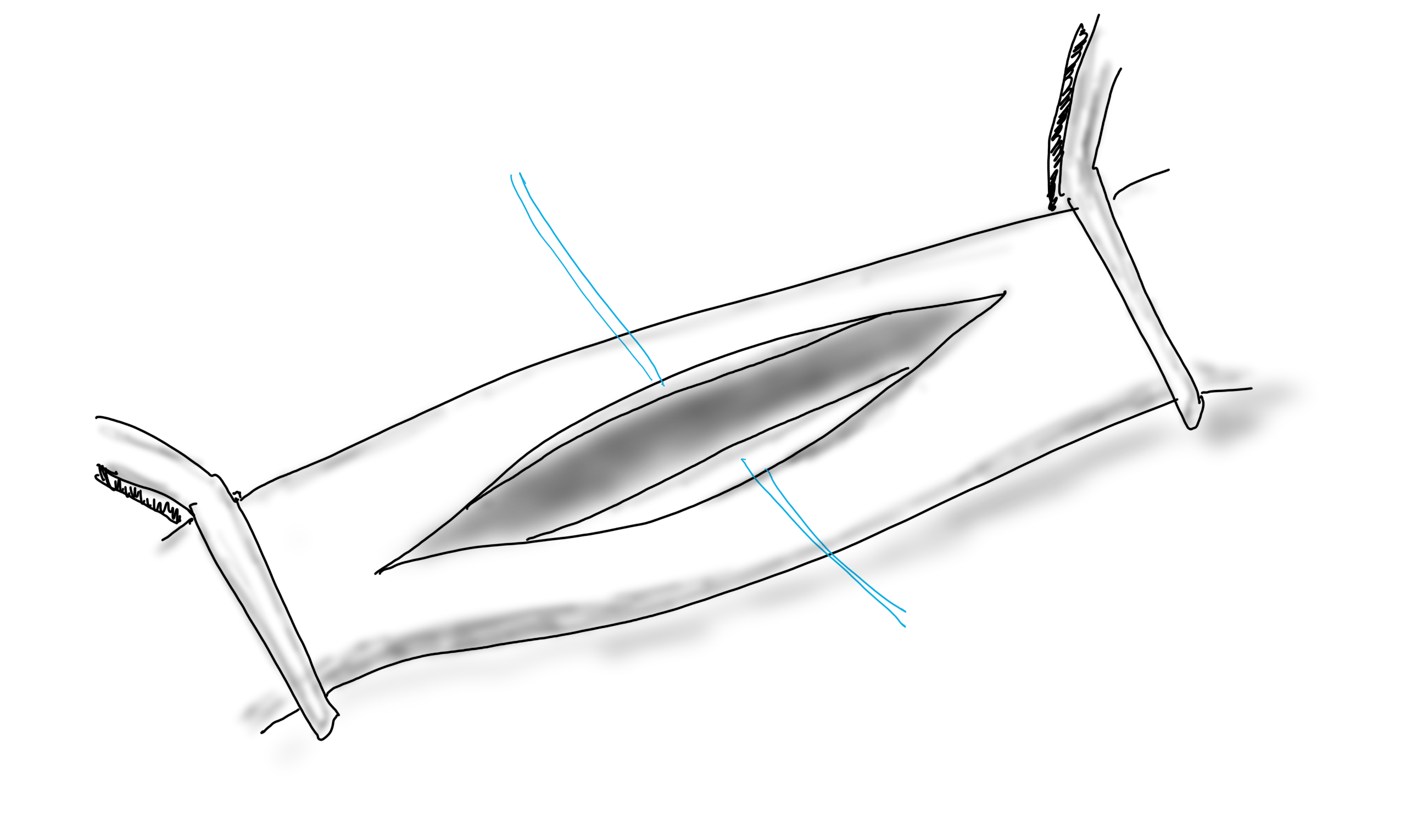
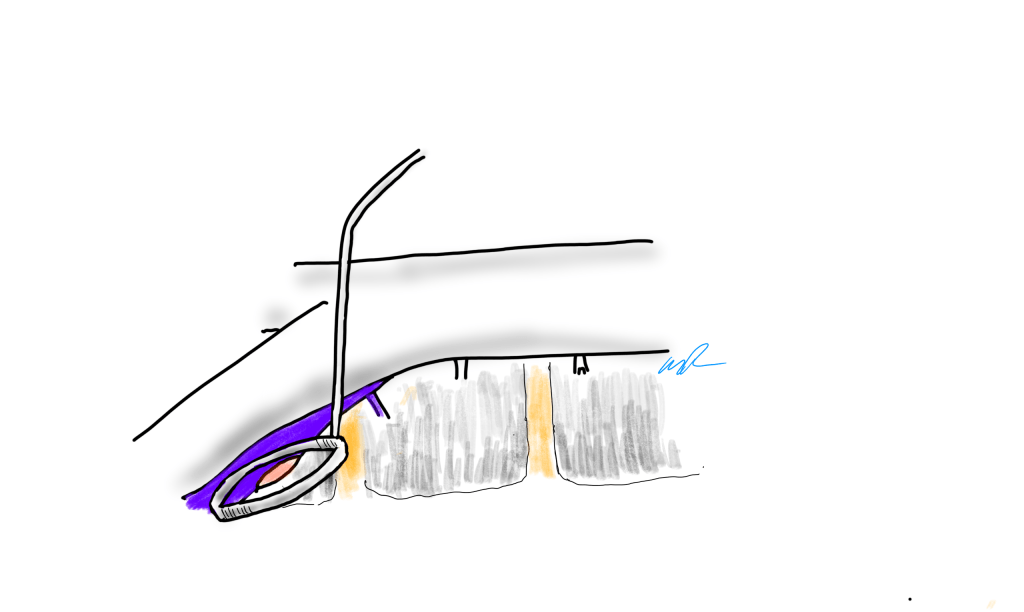
Spinal exposure at the L5-S1 level is treacherous because of the veins
When I returned to academic practice at the Cleveland Clinic, combined cases with other specialties got me operating on tight spaces, frequently heavily scarred, with many blood vessels to control, such as a retroperitoneal spinal exposure illustrated above.
The veins are fragile here and as they are in communication with the central veins, bleed copiously and rapidly.
Look above at the dreaded linear tear on the left iliac vein that can result from simple manipulation of this fragile structure -typically a tributary vein will anchor the iliac and simple retraction can cause a tear.
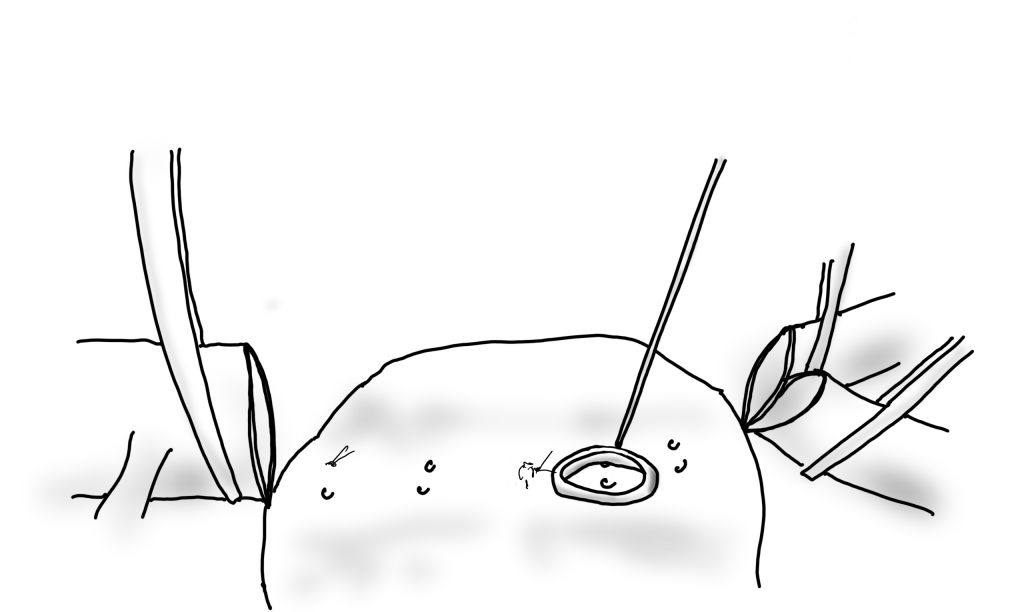
Sponge on a stick limits view of the injury
Using a sponge on a stick greatly hampers your ability to repair the injury. First, the people applying the sponge on a stick have to have some skill. Second, because they are long and straight, they are constrained by the incision you have created. When applied, the “airspace” above the injury is greatly reduced. Third, hemostasis is never complete unless the whole vein is compressed, which is challenging in the above scenario.
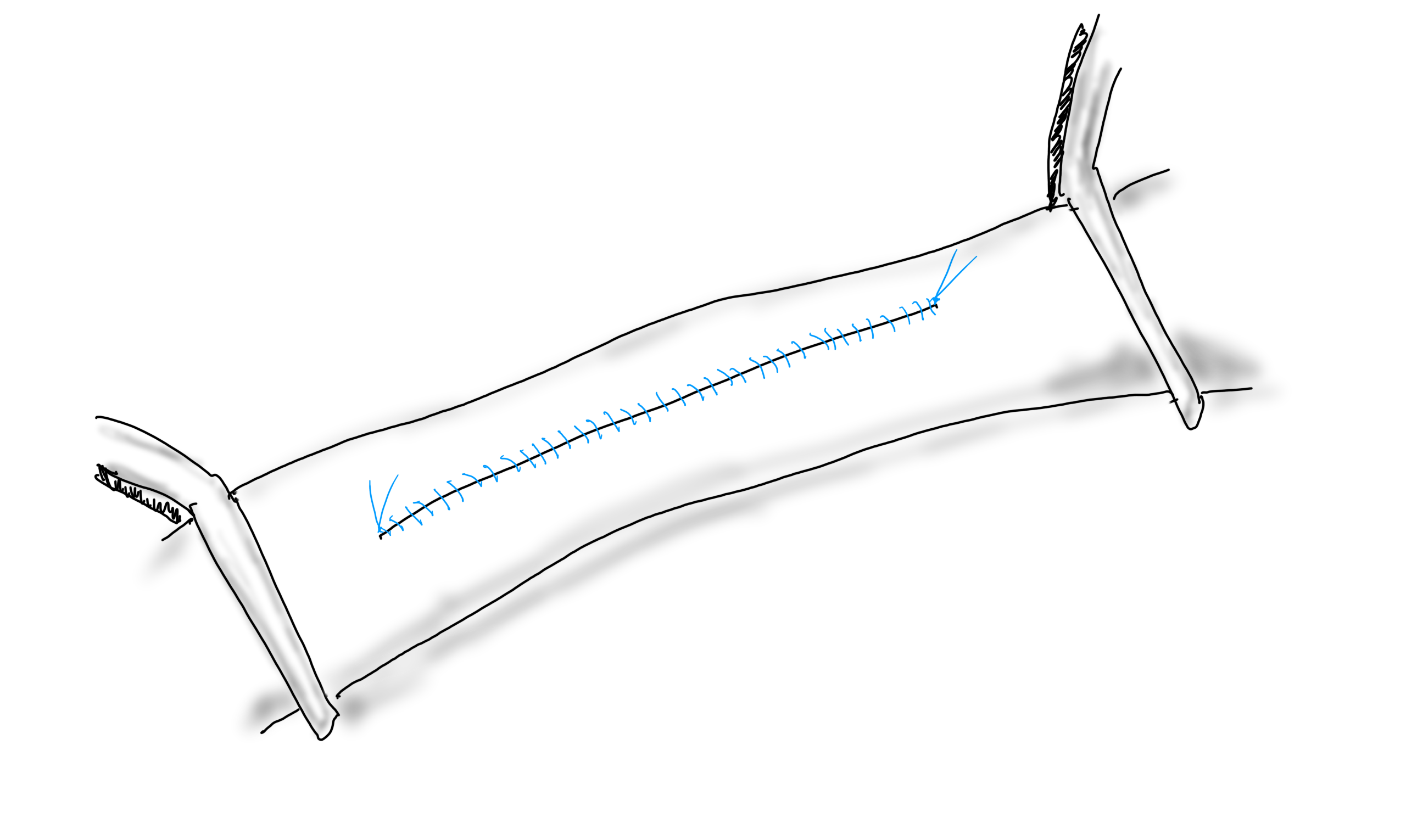
The handle can be bent to create more “airspace” for operating
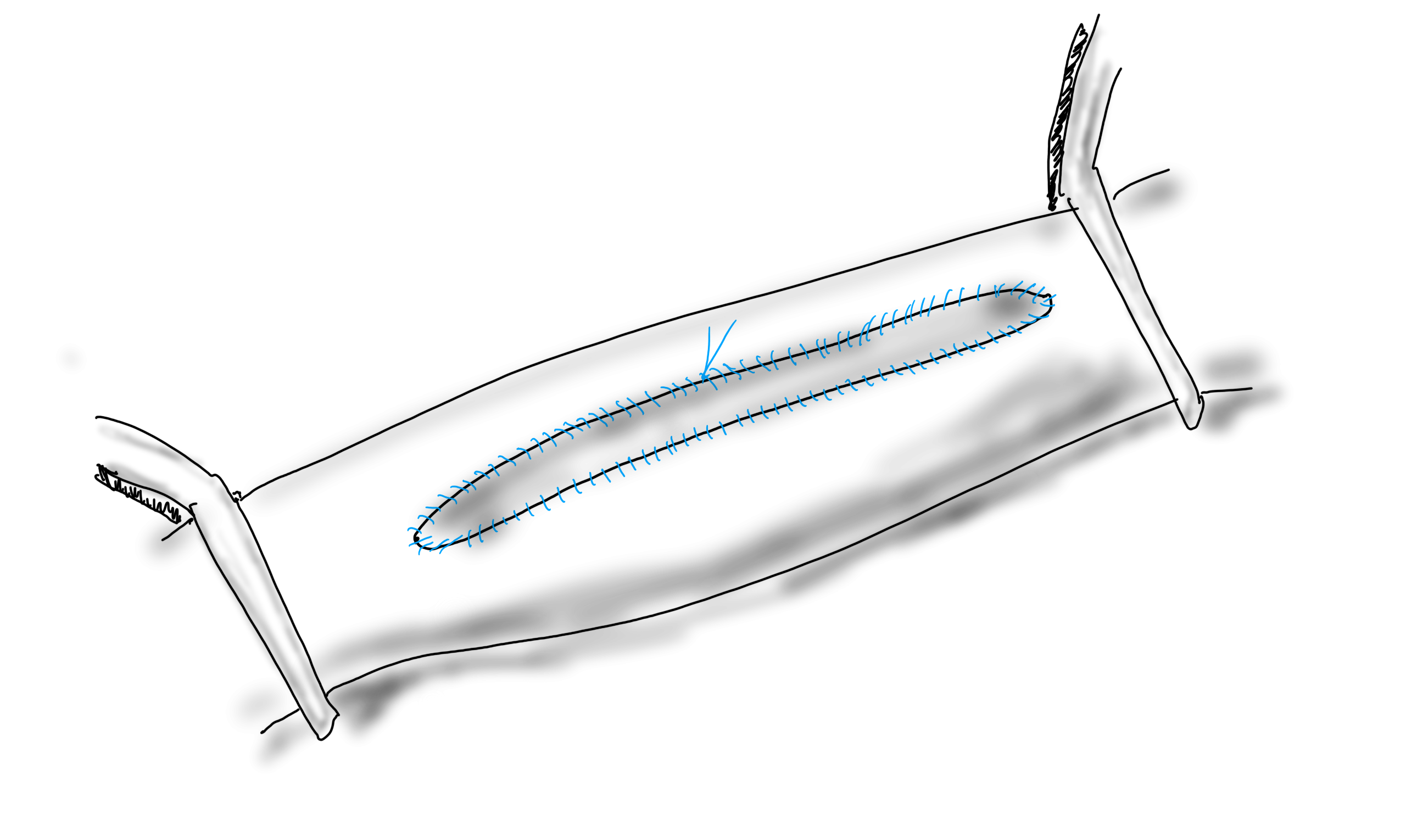
When the ring is applied, two things happen. Hemostasis is in general complete and there is room to operate, in this case suture. Even in the instance where an artery is bleeding from a flat surface as in a bleeding duodenal ulcer or a lumbar artery in an open aorta, hemostasis is achievable.
Bleeding lumbar arterise can cause a significant blood loss in the time it takes to apply a suture. Fingers will occlude, but no one likes getting stuck with a needle.
The bleeding lumbar artery illustrated above responds well to ring compression. This is also the case where you have bleeding from scarred or irradiated tissue surfaces, or from varicose veins or AV fistulae from the skin. If you don’t have a Park Clamp, you can use the finger rings of the handle on a tonsil or Kelly clamp.
If you don’t have a Park Clamp, you can have one made or you can use the ring handle of a standard clamp.
There seems to be interest among surgeons who have seen this device used, and I will look into manufacturing these. I would not object to surgeons making their own for their personal use -taking apart a long tonsil clamp and bending the ring at a right angle should be simple enough. The clamps I use were manufactured at our prototypic facilities, but 3D printed ones should work fine.
And I will leave you with this final thought. I am in the profession of surgery, and at its core, it’s about helping the patient. If you adapt this idea and help someone, I will have fulfilled my duties.
Recently, in clinic, my nurse handed me the patient sheet with the comment, “this is for iliac stents.” This caught my attention as “iliac stents” does not make sense as a chief complaint. The patient had been sent with a vascular lab report. It was a duplex scan documenting peak systolic velocities over 300cm/s in the common iliac arteries, appropriately diagnosing 50-99% stenoses. The patient had hip and thigh pain with walking short distances. I could have been excused for just cancelling the visit and booking an angiogram, except that would make me just a technician responding to a request. So I talked to the patient.
The patient was a nice lady over 70 years of age with recent onset of hip and thigh pain with walking 50-100 feet. This was incapacitating her as she was used to living an active and independent lifestyle. Her pulse examination was normal, not an uncommon finding with aortoiliac occlusive disease which manifests as a hemodynamic phenomena best explained as “small pipes.” Except she had never smoked, and had only hypertension and mild hypercholesterolemia. The review of systems was notable for fatigue and arm and shoulder pain. While she had not lost weight, strangely, her jaws hurt when chewing food.
I do not claim any kind of magic skills when it comes to diagnostics, but these other complaints did not fit. And it is not uncommon for someone to have several common conditions. Maybe she had TMJ, shoulder arthritis, early heart failure, and aortoiliac occlusive disease, to fit all of her complaints. Why was I wasting my time diving into nonvascular ephemera when I could be sending her to be scheduled for an aortogram and iliac angioplasty and stent?
I’ve carried with me this notion that all physicians can be mapped on x-y axes with one axis representing degrees of intelligence peaking at perfectly smart. Perfectly smart doctors have seemingly magical skills. While they are not rolling back their eyes while waving their hands over the patient, the handful of perfectly smart physicians I have worked with can quietly listen and digest a case and come up with the diagnosis, no matter how obscure and rare. On the other axis is compulsion, with the perfectly compulsive marching their patients through every test and algorithm to rule out every diagnosis on a exhaustively long differential list.
Intelligence and Compulsion, Written with a Doctor’s Penmanship
Those striving to be perfectly smart hope to bring efficiency to the clinical process -such as for this patient, it would have made sense for efficiency’s sake to move forward with an exercise treadmill ABI test and booking for an aortogram. Those stuck in perfect compulsion never quite reach a diagnosis, even after ordering batteries of tests, but rarely make mistakes, which is the point of perfect compulsion, because if you carpet bomb the diagnostic possibilities, something will hit. They are especially bulletproof to malpractice, particularly when patients choose not to have any more tests out of exhaustion. Their patients are rarely happy having to go through a myriad of tests to paint away the rule-outs while never quite identifying the disease. Those who play around with being perfectly smart get burned by that which are unknown and unfamiliar. They get blindsided. You want to revert to compulsion when you are tired and overloaded. You want to be smart, all the time.
The point of training, which never ends, is you have strive to be both perfectly smart and selectively compulsive, but it’s better to be lucky than good. It was my luck that I recently reviewed temporal arteritis. Every few weeks, I get asked to remove temporal arteries, and choosing not to be just a technician (although admittedly in the workup of TA, we kind of are), I plowed into UpToDate and Pubmed, seeing if there was a way out of doing these procedures -there really is not, except in the requests for temporal artery biopsy in younger patients -go read it yourself. It was here that I refreshed myself on polymyalgia rheumatica, which has as its symptom complex, muscle pain, lethargy, and jaw claudication. Out of duty, and compulsion, I ordered a CTA, because I knew that the patient had risk for atherosclerosis and arteries stiffened by calcium can have elevated velocities without critical stenoses. Out of curiosity, and after a quick call to one of the Clinic’s rheumatologists who order these temporal artery biopsies, I ordered an ESR and CRP.
The CTA came back with calcium at the aortic bifurcation and origins of the common iliac arteries where the outside duplex showed elevated velocities, but only revealed mild disease on the CTA. Both ESR and CRP came back very elevated. I referred the patient to our rheumatologist, and with steroid therapy, all of her symptoms resolved. Without an aortogram or stents.
I sat and thought about this for a while before posting. The patient was quite happy to give her permission. I cannot fault the outside vascular lab for their diagnosis of iliac stenosis because the diagnostic criteria are basically the same as our labs. It has made me think that approaching this case as a revenue opportunity as increasingly happens would not necessarily have been in error if I had performed an aortogram as long as I did not place stents. I can’t imagine the pressures put upon physicians who have put themselves into situations where they are paying for costly angio suites or their own 90th percentile salaries and lifestyles from not over-calling a stenosis and deploying stents, particularly when there is no oversight.
41 percent of my patients with median arcuate ligament syndrome present missing their gallbladders because biliary colic was the diagnosis that was both familiar and vaguely fit the complaints (reference 1). Not much harm can come from taking out a gallbladder, no? We know that a minority of operators harvest a significant share of the Medicare pie when it comes to peripheral interventions (link to terrific OPED, reference 2). Oh, I am sure each of these cases can be “justified.” Pleading justification from limits of knowledge means I proceed to treat what I am familiar and comfortable with -vascular disease, rather than an unfamiliar disease (at least to vascular surgeons) like polymyalgia rheumatica. If I can fail to recognize my ignorance, who can fault the perfectly compulsive? Like a broken clock that can be correct twice a day, someone of poor intelligence but perfect compulsion can be more effective than a greedy hack seeking to be perfectly smart and efficient.
Dunning and Kruger found that those with lower competence overestimate their ability, and those with higher competence underestimate their ability. Medicine is a perfect laboratory of Dunning Kruger. To be effective, you have to be correct and assertive. The problem is you are trained to project that confidence in the early stages of training and career when you are not ready. What patient would seek an unconfident physician? What person truly knows what they don’t know? The hardest step in medicine is both admitting what we don’t know but also applying hard-gained knowledge and experience with audacity. True humility comes from self knowledge and awareness. False modesty is externally directed, but true humility is internally focused. I don’t have a pat answer, but to become perfectly smart, you have to be perfectly compulsive about filling your knowledge and experience base. You have to submit your complications for peer review, you have seek and collaborate with sound partners, and you have to avoid financial traps that bias you to bad behavior. Above all, you have to stay curious.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
Sheaffer WW, Davila VJ, Money SR, Soh IY, Breite MD, Stone WM, Meltzer AJ. Practice Patterns of Vascular Surgery’s “1%”. Ann Vasc Surg. 2021 Jan;70:20-26. doi: 10.1016/j.avsg.2020.07.010. Epub 2020 Jul 29. PMID: 32736025.
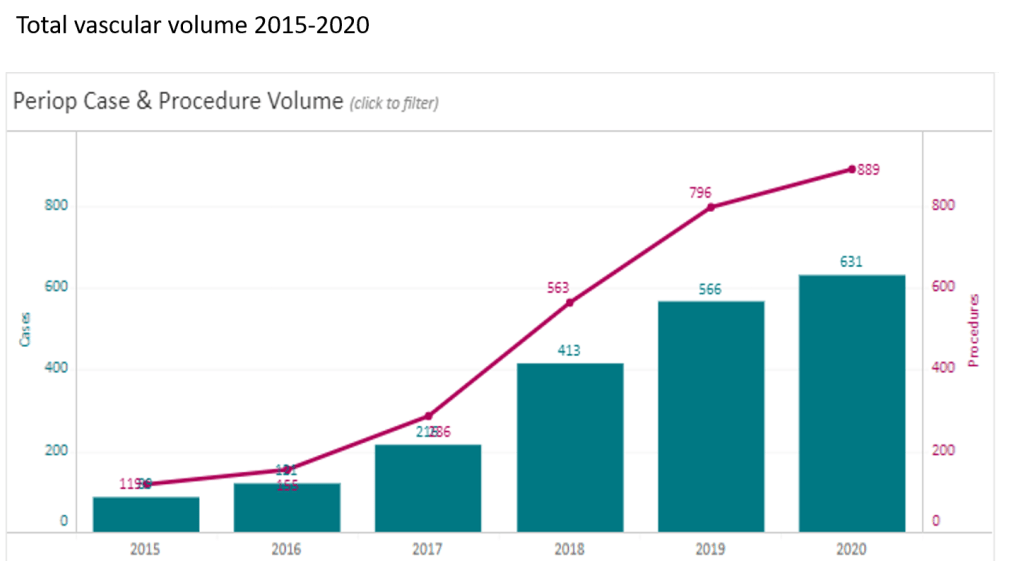
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
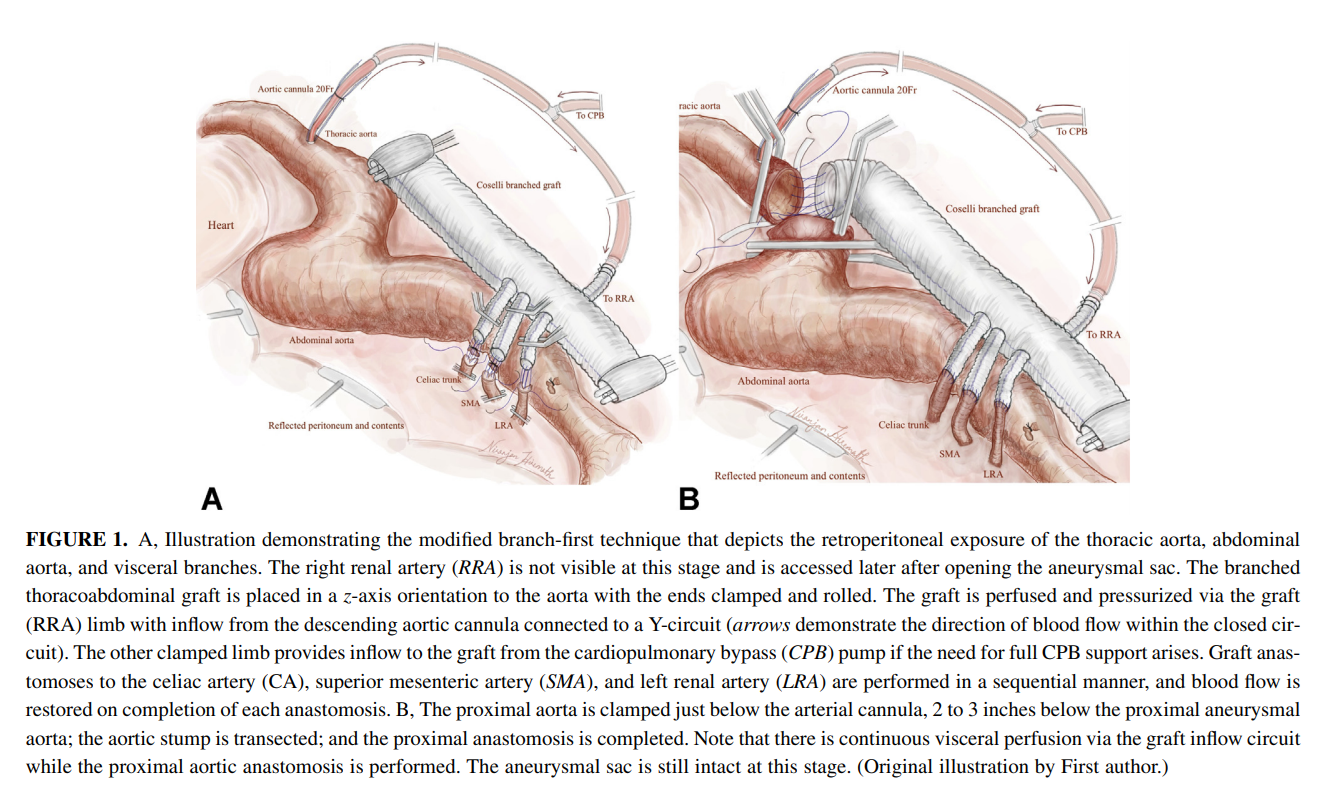
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
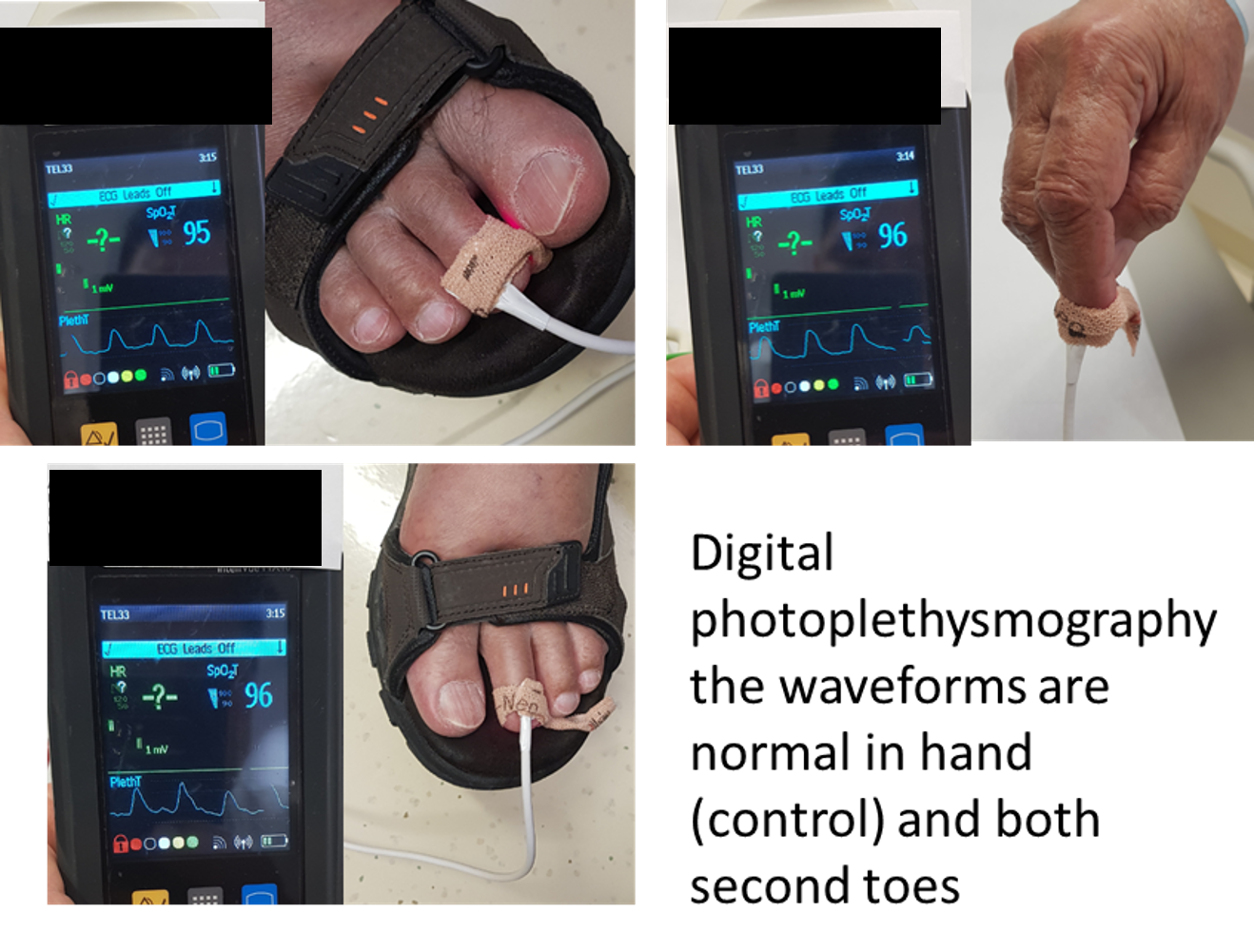
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.
This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).
an abnormal DPPG captured with a hospital ICU pulse oximeter
We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).
At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).
The distal perfusion cannula is in the dorsalis pedis artery
This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery
The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).
Pulmonary artery staple line bleeding controlled, ready for suturing.
In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.
My list of favorite things this year is simpler than in the past, in respect for the difficulties of the past year. Everything is under $300, and I use these every day. Treat your surgeon well and she will give you a nice scar.
1. Lenovo Ideapad Duet. Cloud computing has diminished the need to carry processing power unless you are editing Pixar films or playing super high resolution video games. For composing words on the go, and sketching diagrams for patients, and putting together powerpoints, this Chromebook hits the sweetspot of price, battery life, and quality. It comes with easel stand and attached keyboard with trackpad. An Apple Magic Keyboard for the iPad costs more than the Duet! Battery life is easily all day, and in tablet mode, streaming movies is great. It fits on the stunted traytables on airplanes well because of its petite size. I drew this sketch for planning an arch repair on it. Can’t beat the price at $249 and cheaper with discounts. I got mine as a open box at Best Buy for $200.
Sketch made on a Lenovo Duet
2. Theragun Mini. It is a stereotype that middle aged Asians buy giant massage chairs, which are AMAZING, but if you want something more manageable, the Theragun Mini is the ticket. It is a personal massager designed for deep tissue massage, with a lithium ion battery built in. After a long day of operating, all the aches are pulverized by this machine.
Theragun Mini
3. Masterclass Subscription -During pandemic, diversions like enrolling in an MBA program and Youtube yoga, are the hot ticket, but for someone with a short attention span in need of non-work diversion, these classes are great! Penn and Teller teach magic. Steve Martin teaches comedy. And FBI hostage negotiator Chris Voss teaches high stakes negotiation. All of these highly relevant to a vascular surgeon. Trust me.
4. Moleskine Backpack -I have struggled with overly heavy work bags, but need to carry my computer and some papers and maybe a water bottle, pens, a powerbank, some cables. I find black vinyl laptop bags generally horrible to look at, and too easy to overpack. Expensive leather designer bags carry a similar price as a handbag from Gucci or Louis Vuitton, and would not survive a day without getting scuffed. This backpack from Moleskine, yes the notebook company, is both beautiful to look at but practical as well. It is water resistant and holds everything I need for the day. Has a measured number of compartments and inner panels for pens, cables, and cards, and is well padded for carrying your electronics. Looks great, and would survive medical school.
Moleskine Backpack -not just for notebooks
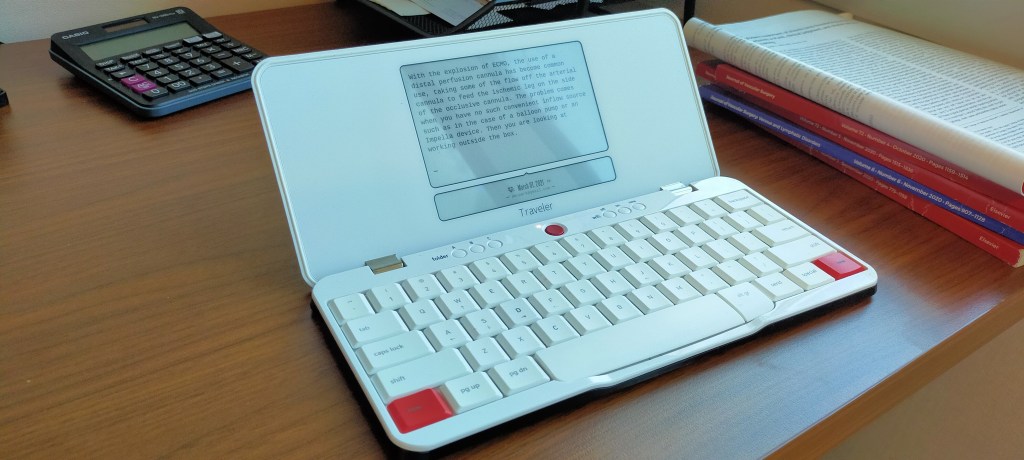
5. Freewrite Traveler -a writing appliance, a typewriter. The original Freewrite was designed to look like a typewriter, and the spirit of the machine is it takes away all the distractions of the internet for the focus of plain paper. The Traveler is the second machine by the Freewrite people, and offers the same focused writing in a portable package. Not for everyone, this one, but if you like writing, if you must write, this is amazing. It features a Kindle-like e-ink screen, and you type without the ability to edit. Everything you write goes to the cloud of your choice, including Dropbox and Drive, and so you won’t lose it. It has internal space for thousands of pages, and a 4 week battery life. If you hope to write the Great American Novel, this is the gadget for you.
Freewrite Traveler for the Hemigway in you
6. LED UV Blacklight -If you’re of a certain age, Spencer’s Gifts was one of the stops you made at the mall, and you always checked out the blacklight section, with its fluorescent posters and purple lamps that made your white shirt glow. As a surgeon, you want a Wood’s Lamp, but most hospitals do not have one, and most nursing staff have no idea what you are talking about. Good thing is that there are many cheap but powerful LED Blacklight options that emit UV light. This is great to have in the OR for a fluorescein test of gut perfusion (link). Take it camping in the deserts around here and you can see the scorpions at night! Or you can torture yourself by breaking it out at the next hotel you stay at and visualize all the glowing “protein stains.” Under $10, but slightly more for the higher power ones.
portable LED blacklight!
7. Old School iPod -This is as close as you can get to getting a Walkman without dealing with the inconvenience or poor sound quality of cassette tapes. In 2004, these were cutting edge, and Apple to its credit still supports file transfers of purchased (but not streaming) music files. The cool thing about these is that if you can do a carotid endarterectomy, replacing the battery and upgrading the memory are nothing, and there are many videos on line to show you how. These units are cheap to find on eBay, and there is nothing cooler than carrying around 10,000 songs in your pocket, without the need for a network, meaning uninterrupted music in the OR without relying on the network.
An iPod I purchased in 2006, upgraded to 32gB from original 8gB, just replaced battery for third time, still works.
8. Golf Ball Stamps -These stamps are meant to mark golf balls, but they are incredibly useful for graphically marking up a printed list. Each of these symbols represents a status or an action, which lets me look at a list at a glance and remember exactly what needs to happen. At pro shops everywhere.
Meant for golf, repurposed to act as semiotic markers on lists
9. Swiss Army Knife -the first one I got was as a graduation gift from my dad, thought technically not a gift as superstition dictated I purchase it from him for a dollar, it was the same as this one which is currently my fourth, bought at a Boy Scout camp for about $10. I keep one in my checked luggage for use at my destination for opening bottles, uncorking wine, cutting salume and cheeses, tightening screws, and when the occasion arises, performing an appendectomy (need a hotel sewing kit). This one also has tiny forceps and a toothpick.
With this, I can do several life saving operations.
10. Skirt steak -rarely seen any more shrink wrapped at chain groceries, you generally have to ask the fellow behind the counter or know a butcher. This diaphragmatic muscle used to be cheap. Considered offal in many places, this formerly cheap meat ended up being the go to meet for tacos and street cart barbecues in Asia, but don’t sniff at it. As it is not a structural muscle, it is not tough, has great flavor, and while leaner than traditional steak cuts, not devoid of fat like a filet (which is not my favorite) giving it enough buttery fat tones to remind you it is meat. Because it’s harder to find, that means the people who supply it know beef. Here in Abu Dhabi, I ordered this from the CarniStore in Dubai. Dinner is served.