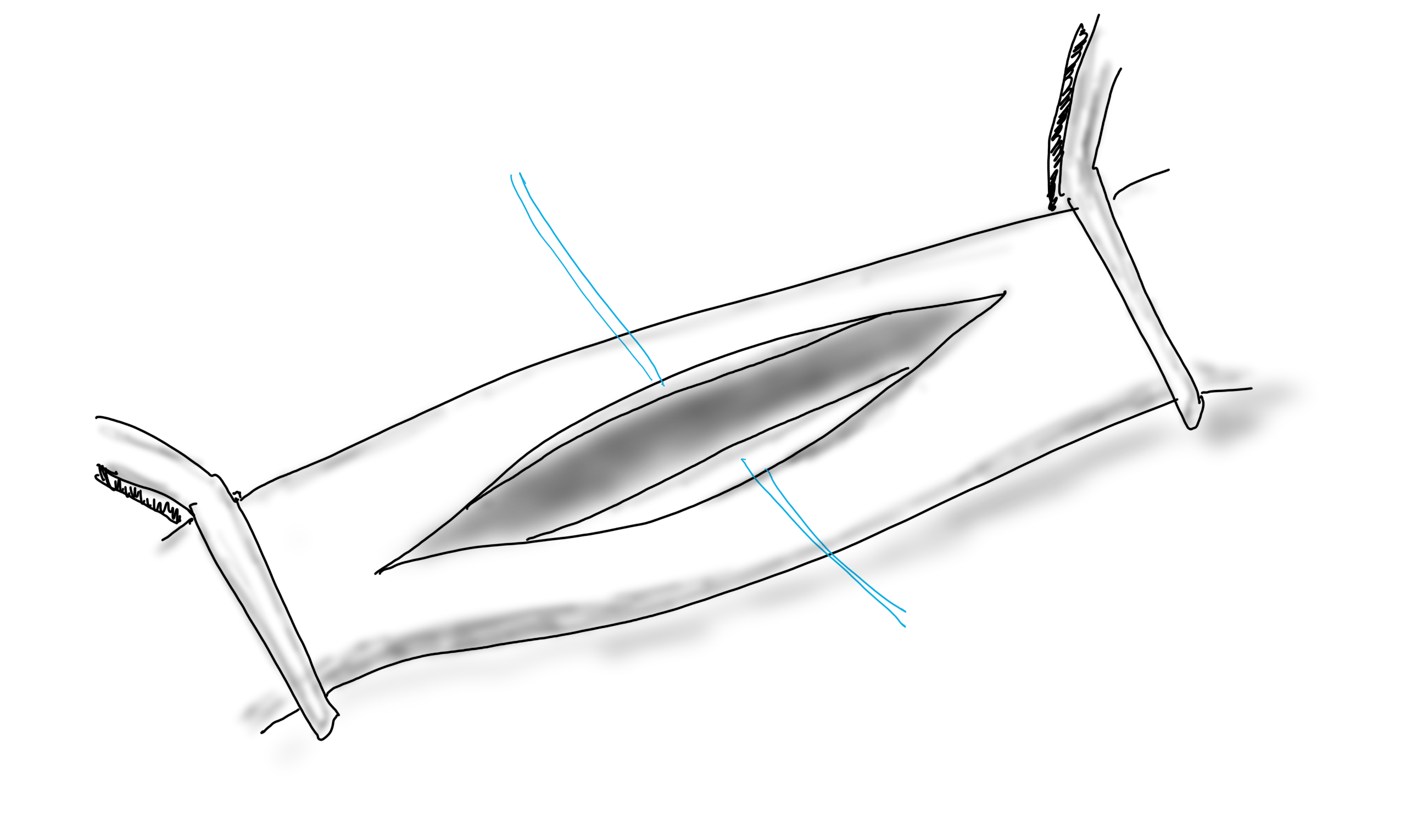
PTFE bypass to a smaller tibial artery with Taylor vein patch
One of the conclusions of the BEST-CLI trial (ref 1) was that of equivalency between alternate bypass conduits and interventions when a single saphenous vein is not available. I recently contacted Dr. Matt Menard to see if there had been subgroup analysis of these bypasses which represents a heterogeneous group of conduits including PTFE, PTFE with vein patch, spliced vein, composite vein, and even possibly allograft. The results from the abstract were intriguing -“83 of 194 patients (42.8%) in the surgical group and in 95 of 199 patients (47.7%) in the endovascular group (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; P = 0.12) after a median follow-up of 1.6 years” with the primary MALE endpoint. If this was a football game, there would be a video review of the call. And they are looking at this, I was assured by Matt, but we would all have to wait for this year’s SVS VAM. Dr. Matt Menard is coming to speak at our 12th Annual Vascular Disease Update (link) which I highly encourage you to register and attend (addendum).
The Cohort 1 from BEST-CLI is an illustration of the vascular surgeons’ LIMA to LAD. It’s something we already knew from years of experience, but laid out in level 1 data (below).
The BEST-CLI paper is short on detail about cohort 2. This is where a lot of clinical decisions get made, and I suspect the vast majority of patients are getting interventions because fewer surgeons are facile with leg bypasses and vein patches.
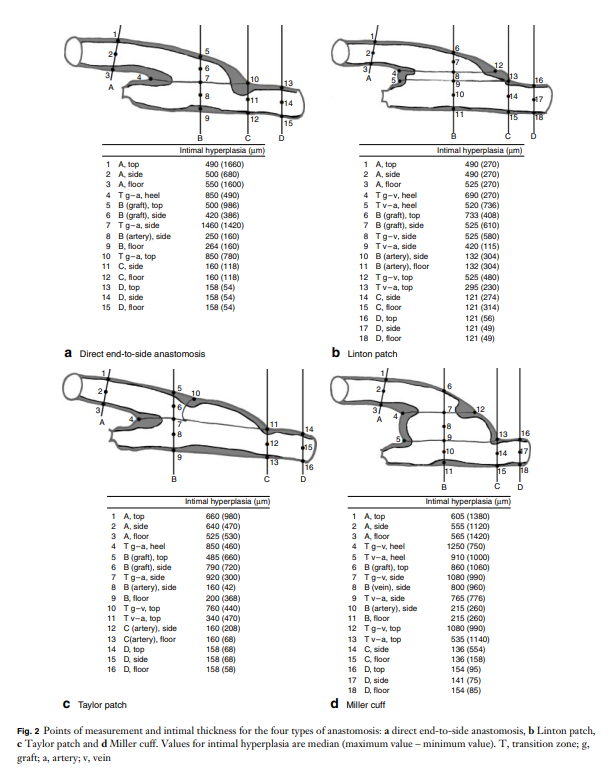
Why the vein patch? While not a panacea for the lack of vein, from its inception, it has proved a worthy adjunct in limb salvage. Decades before endovascular therapies showed good limb salvage with modest to poor patency rates, Dr. Frank Veith showed that infrageniculate PTFE bypasses showed good limb salvage with poor patency (reference 2). Vein patches, such as the Taylor patch illustrated at the top, showed good patencies (reference 3) in an era where DOACS, DAPT, and statins were not available.
Results of the Taylor Patch from Mr. RS Taylor.
Why a patch works is debated. Some feel it is the modification of the end to side anastomosis that creates an optimal shape for containing turbulence which leads to intimal hyperplasia. This was the concept behind the Distaflo graft which I tried but have abandoned for not improving patency in my personal experience.
The Distaflow Mini-Cuff which applies the concept of flow optimization by the shape of the anastomosis achieved by vein cuffs.
The best explanation of why vein cuffs work is from an animal study from Vienna. Intimal hyperplasia is best explained as a foreign body reaction and the reaction is worse with a true foreign body than with autologous materials. A simple anastomosis with PTFE to tibial artery creates a ring of hyperplasia. Vein patching moves this severe foreign body reaction off of the artery, leaving a gentler vein to artery reaction to occur on the outflow (reference 4).
My final point is that these surgical papers used to be the mainstay of podium presentation in the 90’s and ’00’s, but are now infrequent as the bulk of the time at these meetings is devoted to gadgets which almost always involves purchasing a box and contracting for disposables (the printer and ink business model). I am going to review our institutional results of these PTFE bypasses, and hope to see more from other groups. I look forward to the BEST-CLI papers to come, and other trials.
References
Farber A, Menard MT, et al. BEST-CLI Investigators. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N Engl J Med. 2022 Dec 22;387(25):2305-2316. doi: 10.1056/NEJMoa2207899. Epub 2022 Nov 7. PMID: 36342173.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
Taylor RS, Loh A, McFarland RJ, Cox M, Chester JF. Improved technique for polytetrafluoroethylene bypass grafting: long-term results using anastomotic vein patches. Br J Surg. 1992 Apr;79(4):348-54. doi: 10.1002/bjs.1800790424. PMID: 1576506.
Trubel W, Schima H, Czerny M, Perktold K, Schimek MG, Polterauer P. Experimental comparison of four methods of end-to-side anastomosis with expanded polytetrafluoroethylene. Br J Surg. 2004 Feb;91(2):159-67. doi: 10.1002/bjs.4388. PMID: 14760662.
Addendum
The Annual Vascular Update at University Hospital has something for everyone, including a presentation on IRAD by Dr. Santi Trimarchi, and BEST-CLI by Dr. Matthew Menard. Local faculty from Cleveland are also featured in a broad review of vascular medicine and surgery chaired by Drs. Mehdi Shishehbor, Heather Gornik, and our chair in vascular surgery, Dr. Jae Sung Cho. Link. I will be presenting on neurovascular compression syndromes and renal failure/heart failure.
The patient is a woman in her forties who works hard and smokes cigarettes to find stress relief. The year prior to presentation, she began to get cramps in her calves while she walked the halls of the building she cleaned, and this became unbearable. A consultation at our hospital revealed moderate to severe diffuse atherosclerosis without a dominant lesion but notable small distal aorta and iliac arteries with a 50% stenosis of the left iliac origin. Recommendations were to quit smoking and exercise. She found this difficult to achieve and went to another hospital nearby.
There, 6 months prior to presentation, she began complaining of painful cyanosis of her toes which was described as blue toe syndrome. These outside studies were not available. She was taken to the OR and her common iliac arteries were stented. This gave her relief, but the soon pain returned three months later -her stents had occluded. This was treated with more stents, extending them proximally into the aorta and distally in the case of the right across the iliac bifurcation. This afforded her relief for three more months until one weekend she found herself unable to walk again for more than minimal distances, and she took herself to my hospital, University Hospital, Cleveland Medical Center.
On examination, she was a large woman with no femoral pulses, but signals could be obtained in her popliteal and tibial arteries. Her PVR’s showed inflow disease and poor flow at the feet.
Her baseline CTA in workup of her claudication the year prior to getting stented shows the aorta and iliacs, while open, are small, with aortic lumen diameter reaching 10mm and common iliac lumen diameter at 6mm with diffuse atherosclerosis (below).
Aorta scanned winter prior to index intervention showing small aorta diameter of 10mm and diffuse narrowing of common iliac artery, 50% stenosis left CIA orgiin. Intervention was not scheduled. Patient went elsewhere and underwent intervention .
The CTA on presentation shows bilateral stent occlusion. A closer look shows the second set of stents extending the original stents both proximally into the aorta (raising the bifurcation) and distally into the external iliac and across the internal iliac origins (white arrows). The internal iliac arteries, despite the stents and on the right thrombus in the stent, supply flow to the external iliac arteries which have not thrombosed.
The treatment options were
Exercise and risk factor modification
Reintervention
Axillo-bifemoral bypass
Aortobifemoral bypass
Aortoiliac endarterectomy and patch angioplasty, stent removal
Although exercise and risk factor modification should be part of the treatment regimen, the best time to institute this was before her first intervention. With the long segment occlusion of her stents, coverage of the right internal iliac artery and occlusion, and acuity of her symptoms, this is no longer feasible.
It reveals a certain kind of bias when we prescribe walking exercise to those who can’t afford gyms or equipment, and whose neighborhoods are unwalkable.
Reintervention, having failed once, will not be durable. Even with anticoagulation, any recanalization -thrombolysis, thrombectomy, balloon angioplasty, atherectomy, lasering, and restenting, would not be durable.
It is likely the patient is frequently vasoconstricted and this is exacerbated by smoking. While never diagnosed with Raynaud’s, she did give a history of easily have numb, cold fingers and toes in the chilly winters in Cleveland. Even normal spectral Doppler signals will show pauses in flow in the peripheral arteries. Combined with any hypercoagulability and injured lumenal surfaces from interventions, and stents will go down.
An Aside on Small Aorta Syndrome in Women
One of the advantages of being a village elder is you remember forgotten concepts that guided treatment “back in the day.” The small aorta syndrome defined as having an aorta smaller than 12mm in diameter is one of those. Best described as not having enough pipe -imagine a small caliber fuel line throttling an engine. For all the muscles involved in standing and walking, there is a minimal diameter necessary for function.
Small aorta syndrome stands up to objective testing. A patient with a small aorta but otherwise patent lower extremity arteries, can present with claudication and demonstrate drops in ABI with exercise. These are typically female smokers with elevated BMI. Along with their small aortas, their external iliac arteries will be small, and I used to wonder if some critical period of inactivity in their early years failed to grow these arteries, or if this process of normal growth and remodeling is retarded by smoking.
Small aorta was a common indication for aortobifemoral bypass (ref). Unlike some abandoned indications for operation like “4.5cm AAA” and “asymptomatic 60% internal carotid artery stenois,” it had a testable finding of drop in ABI with exercise, but its acceptance has waned in the advent of the endovascular era. In a purely open era, I think there was greater emphasis and awareness on engineering the hemodynamics. While endovascular interventions simplify treatment, just stenting a small arteries usually doesn’t fix the problem as illustrated in this case. That is because there is a maximum size that the arteries receiving the stents will allow.
The iliac artery and aortic bifurcation will only tolerate so much upsizing with stents before rupturing. The interventions are constrained by the size of the adventitia. What is also ignored is the concept of elasticity -the 7mm lumen through a reopened and restented artery provides more resistance to flow than a 7mm artery restored via endarterectomy. All stents decrease elasticity of the circuit and decreases flow in a pulsatile circuit because of the increased impedance. Bovine pericardial patches on the other hand add elasticity. Endarterectomy restores elasticity. .
Enough Pipe
In the early 2000’s, I used to live in an pre-war apartment in Riverdale down the hill from Drs. Takao Ohki and Frank Veith. The apartments above and below me all shared this same feature -poor water pressure, because during a restoration twenty years before, the owner used the wrong, smaller size of pipe for this line of apartments. The taps would run, but if more than one apartment ran the shower or dishwasher, the taps would drip. The apartments would claudicate. The pipes were all patent, but inadequate. Not enough pipe. This patient endowed with small vessels, grew a large body, and smoked, and her muscles needed more pipe to support the added load. Not enough pipe.
So is the solution an aortobifemoral bypass? It is the board answer and a durable one, but it shares with axillobifemoral bypasses the risk of groin infections, particularly with a large body habits (below). The outflow arteries, all patent, are small and likely subject to vasoconstriction. My choice of ABF graft in this patient is a 14x7mm bifurcate which is on the small side, but I would be afraid that a 16x8mm graft would be too large on both the aortic and iliac side, resulting in mural thrombus formation.
A vertical groin incision will create a 3 inch deep canyon in the fat to get to the CFA
Axillo femoral bypasses, aside from the groin issues, suffer from poor long term durability and is not a great choice for a 40 year old. Her axillary artery was 6mm and sourcing flow to the lower torso from that is never great. Also, supplying a long 8 or 10mm graft would recapitulate the original problem of a small aorta. Not enough pipe.
For me, the best option would be to remove the stents and restore the distal aorta and iliac arteries to their original elasticity and slightly larger than original diameter. I would then be able to reopen flow to the occluded right internal iliac artery. Not just enough lumen, but enough and correct pipe.
Technique: Exposure
Exposure is predicated on the planned extent of the endarterectomy, place for clamping, and plans for aortobifemoral bypass if the endarterectomy results in poor adventitia. In a woman, the iliac bifurcations are easier to reach. A midline laparotomy is the incision of choice here. Let me digress here about the laparotomy. Over the three decades since the launch of laparoscopic surgery and subsequently endovascular surgery, the midline laparotomy has gotten an undeserved bad rap. Laparotomies are well tolerated and should not be viewed as a rare bailout or outright failure of laparoscopic therapy. Rather, it is still the gold standard exposure.
The infrarenal aorta to the right external iliac artery is exposed as well as the common iliac. In this patient the sigmoid mesentery was fatty and did not readily expose the iliac bifurcation so a separate exposure of the distal left common iliac artery was performed by mobilizing the left colon.
The aorta above the bifurcation was prepared for clamping. This involves circumferential exposure as I prefer a transverse aortic cross clamp. The lumbar arteries are clamped with bulldogs or aneurysm clips. The right external iliac well beyond the stent is controlled and the internal iliac is exposed and controlled. On the left the internal and external iliac arteries are expose and controlled.
The patient is heparinized clamps applied, and I make the arteriotomy with a 15 blade cutting down to the stent. The aorta is cut to a point about a centimeter below the clamp. The external iliac is cut to where there is patency of the artery and the plaque is mild. The endarterectomy is performed in the same way one does a carotid or femoral, with care to find the correct endarterectomy plane outside the plaque and good end points where the plaque adheres well. The internal iliac plaque on the right was chronically occluded but was successfully removed via eversion resulting in back bleeding. I sound the artery with a dilator to make sure a dissected plaque isn’t occluding it then reclamp.
The left common iliac artery is opened via a separate arteriotomy as I find tailoring a Y-shaped patch laborious. The arteriotomy is extended under the sigmoid mesentery and then moving the left colon medially the arteriotomy is finished slightly beyond the external iliac origin. The endarterectomy is finished short of the iliac bifurcation and any narrowing at the bifurcation is treated with the patch.
The specimen shows that the adventitia remains separated from the stents by the plaque. I rarely use tacking sutures as I feel a properly performed endarterectomy results in no plaque or well adherent mild plaque.
The patch needs to be thoughtfully applied. An overly large one will billow, and at worse case, create an artificial aneurysm. For example, for a 7mm iliac artery, the circumference is 22mm. Adding an 8mm patch with 1mm suture bites results in a 26mm circumference and an 8.3mm end diameter. Narrower is okay, but much larger will result in size mismatch that the body compensates for by laying mural thrombus. A long 8mm wide patch can be cut from a large swatch of bovine pericardium, remembering to add a slight angulation onto the iliac artery.
This operation avoids the groins with exposure or access into a small artery with a large sheath. A 4mm artery with 12.6mm circumference receiving an 8F sheath receives a 2.6mm hole, a 40% defect across the anterior hemicircumference of 6.3mm. This is not trivial, particularly because the arteries are often atretic after prolonged occlusion, may tear with a closure device, most of which are off IFU for such a small vessel. Avoiding the groins altogether is a great benefit to this type of procedure.
A postoperative CTA showed wide patency of the restored aorta and iliac arteries.
At followup several months after the procedure, the patient was walking well without claudicating and was ready to return to work. PVRs showed excellent flows down to the toes.
Hemodynamic Engineering
A surgical trainee has to develop a sense for flow. Looking at a circuit, she has to ask “how does blood get from point A to point B?” Merely providing a pipe does not mean a cure. For example, replacing a blocked artery with a steel pipe would provide flow but it has a hemodynamic impact that is different from the native vessel. Flow stoppages during the cardiac cycle that is modulated in a normal artery by the elasticity of its wall. While we don’t deliver steel pipes, we do something similar in ballooning heavily calcified arteries, or stenting them. ABF with prosthetic bypass offers a safe, broadly available method of treating this, but is fraught with problems for patient who develop groin infections or occlude a bypass for the reasons previously mentioned. Endarterectomy and patching with bovine pericardium allows for more precise restoration which would be a laudable goal in a young patient.
And my final point is this. This patient can yet undergo aortobifemoral bypass. Ironically, even larger stents may be safely placed than was previously possible. One of the principles laid out by Dr. Jack Wylie in his peerless surgical atlases was of leaving a patient in a condition to allow for future necessary operations. For a forty year old patient with many decades left, this is a critical concept.
This case represents the second aortoiliac endarterectomy I performed to remove failed stents. The third just happened today with resection of failed CERAB stents which I did with my chair and fellow Mayo Alum, Dr. Jae Cho. I think that there is a room for this operation which should not remain in the history books.
Median arcuate ligament syndrom (MALS), also known as celiac axis compression syndrome (CACS) and its eponym Dunbar Syndrome, is manifest as epigastric abdominal pain and a compendium of symptoms, arising from chronic compression and inflammation resulting from compression of the celiac plexus between the median arcuate ligament and the celiac axis.
Graphic showing the pathoanatomy of neurogenic MALS (from ref 1). The repeated trauma to the celiac plexus results in inflammation and nerve injury with transmission of pain and neuropathic sensations.
The diaphragm muscle descends from the neck during development (the phrenic nerve originates from C3-C5 nerve roots), and in perhaps up to 25 percent of individuals, drapes across the origin of the celiac axis, and sometimes anchors further down impinging on the SMA or renal artery origins.
While a significant number of patients have this coverage of the celiac axis origin, not everyone has pain. Some whose celiac axis is compressed develop post-stenotic dilatation. For some of these, there is damage to the celiac axis resulting in intimal injury, dissections, thromboses, webs. Turbulent flow causing post-stenotic dilatation in the celiac axis can proceed to aneurysm formation. Downstream in the splenic and hepatic artery and its branches, turbulent flow can engender tortuosity (lengthening) and aneurysms (widening). This disease subset of celiac axis compression should be termed aMALS (arterial median arcuate ligament syndrome).
A question was asked at this year’s VEITH Symposium as to whether post-stenotic dilatation due to median arcuate ligament compression could be considered an aneurysm. The answer given was no, but I think it would be yes in the above example.
Both arterial and neurogenic manifestations of celiac axis compression are under the same ICD code of I77.4, referring to both celiac axis compression syndrome and median arcuate ligament syndrome. While I would never suggest more ICD codes, there should be a differentiation similar to the other compression syndrome, thoracic outlet syndrome (TOS). The pain-based syndrome, which is more common, should be termed neurogenic MALS, or nMALS, and the arterial disease secondary to celiac axis compression should be termed arterial MALS or aMALS. The treatment of nMALS is surgical ablation of the celiac plexus along with median arcuate ligament release, done via open, laparoscopic, and robotic techniques. The treatment of aMALS is the treatment of the arterial complications of celiac axis compression and should involve median arcuate release and treatment of the arterial pathology with either open or endovascular techniques.
Case Presentation
The patient is a middle-aged man with several months of right sided abdominal pain, mostly in the right midaxillary line at the costal margin, right upper quadrant abdominal pain, and right sub-scapular pain. He did not have gallstones, and had no gastrointestinal complaints. He is hypertensive and was on a single agent which he took in the mornings. His pain began during the day and crescendoed in the evening. His prior visits to the emergency room had revealed a hepatic artery aneurysm and celiac axis aneurysm. In the ED, his examination was significant for pain and mild tenderness in the right upper quadrant of his abdomen. He underwent a CT scan.
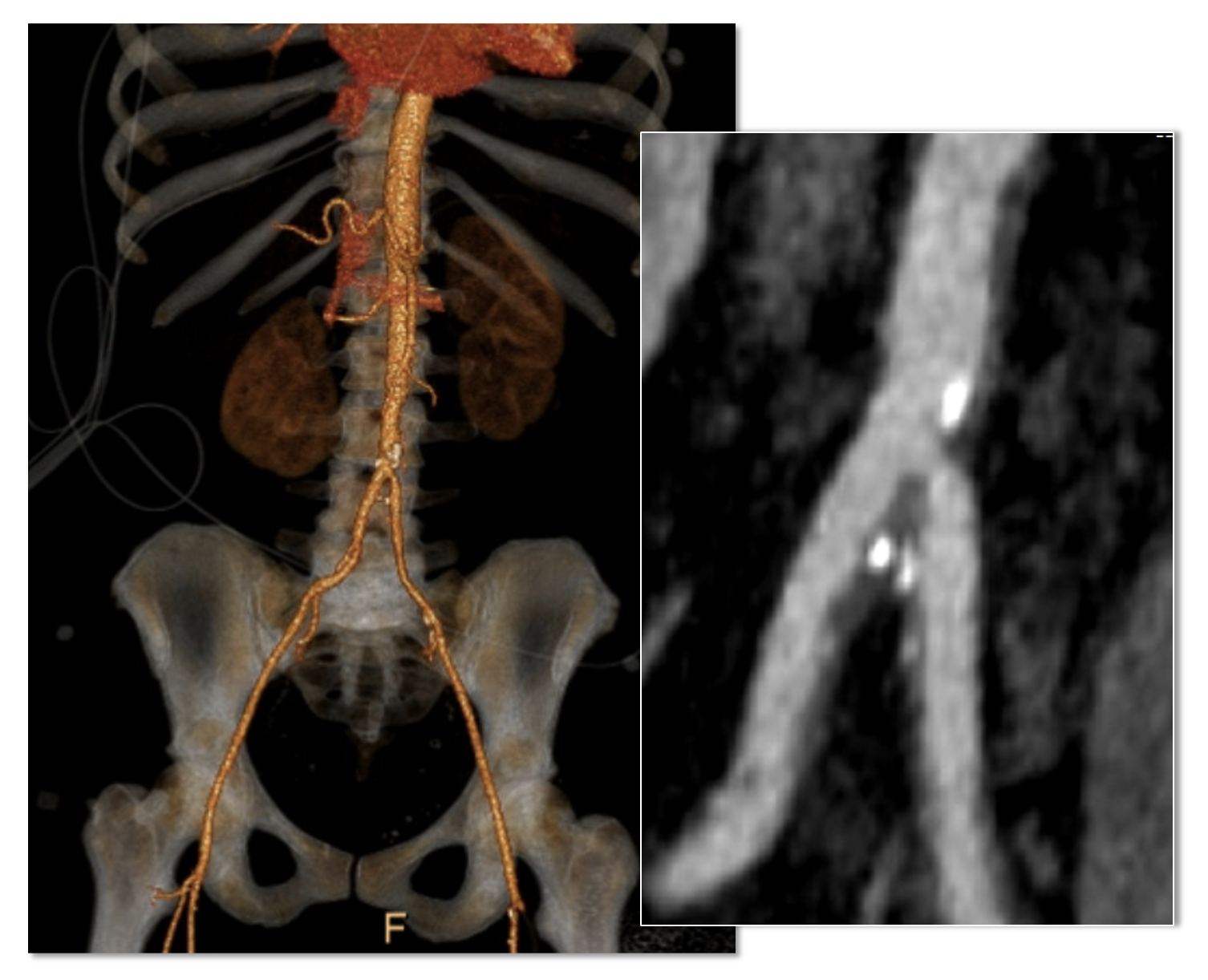
Common Hepatic Artery Aneurysm, 2.4cm with celiac axis ectasia to 14mm, median arcuate ligament compression of celiac axis
The CTA showed compression of the first centimeter of the celiac axis by the median arcuate ligament of the diaphragm and mild post-stenotic dilatation to 14mm. At the terminus of the common hepatic artery, where the hepatic bifurcated was a 2.4cm aneurysm with mural thrombus. With blood pressure control, his pain remitted.
The trainees and I had a lively discussion as to indications for repair and whether this constituted a symptomatic aneurysm. As I have stated in past posts, all pain has a nerve and a mechanism for pain. Abdominal pain and its points of referral are well known going back to the 19th century and encapsulated in Cope’s Early Diagnosis of the Acute Abdomen, whose most recent steward, Dr. William Silen just passed this September. Processes involving the gallbladder and nearby hepatic artery refer to the right upper quadrant abdomen, right chest, right shoulder and scapula which was where the patient’s pain was. And it improved with controlling his hypertension. There was no question to me the aneurysm was symptomatic, likely from strain on the aneurysm.
The question then devolves to whether this is to be done endovascularly or open. While it seems straightforward for me, I have realized at large meetings there will always be some endovascularist proposing something. For me, to exclude pressure from the aneurysm and avoid rupture, the aneurysm had to be isolated from the blood flow and pressure. Ideally, this would be done with tiny covered stents. There are no 7mm x 4mm stents bifurcation stents.
Hypothetical bifurcated small stent system -does not exist, would not work.
Embolization of the hepatic aneurysm, which is done for the splenic, offers hazard of hepatic ischemia. Despite what is written in the textbooks about the portal venous system providing most of the perfusion of the liver, you have to remember there is only portal flow when there is food. Acutely losing one of the hepatics, even clamping it for a time, reverberates as a spike in the LFTs, along with attendant systemic inflammatory response. While the liver, like spleen, can recover and regrow, you mess with it at your great peril. Based on the CTA, closing the hepatic artery with coils and plugs will likely be tolerated as hepatic flow would continue via the gastroduodenal artery which is not small, but there is no guarantee that the aneurysm wouldn’t be pressurized yet by the prominent GDA (if you disagree please feel free to comment).
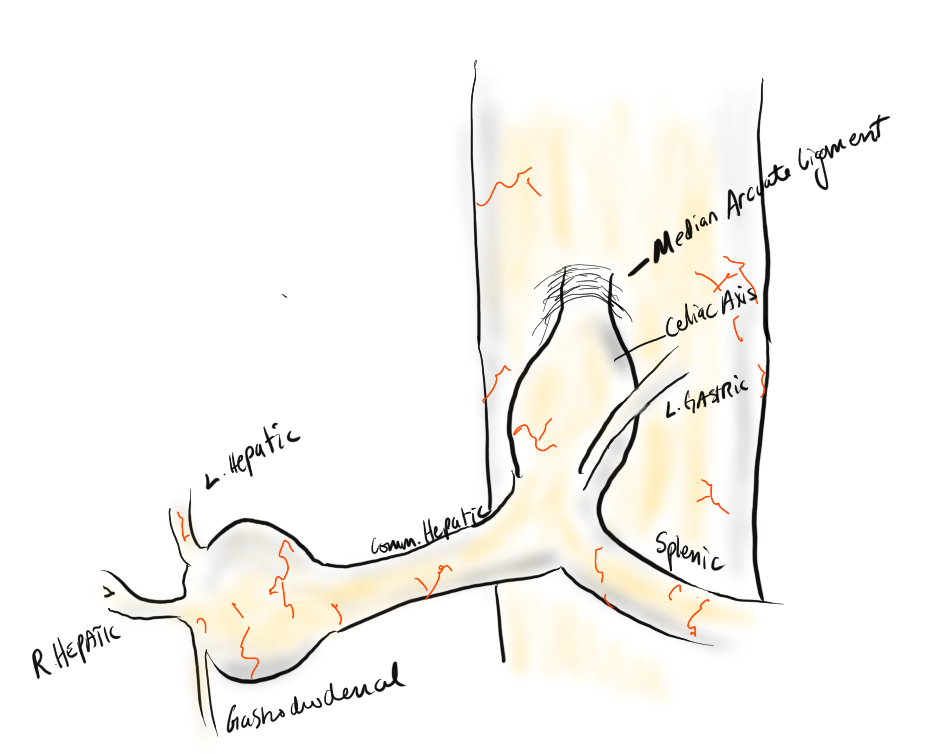
He was prepared for surgery with echocardiography (normal) and lab testing (normal LFT’s, CBC, BMP, INR), and taken to the OR. A chevron incision was made to broadly expose the area. The median arcuate ligament was exposed and released -there was dense tissues proximal to the dilated celiac axis. The aneurysm was dissected out and the small branches were carefully dissected out and controlled. It is easy to injure the branch hepatic arteries which can constrict on dissection.
A suitable length of saphenous vein was harvested and prepared. The three vessels diagrammed above did not present themselves suitable for a single Carrel patch so I sewed end to end to a patch incorporating the right hepatic and gastroduodenal arteries, and performed a sequential side to end anastomosis to the left gastric artery.
The patient recovered well and was discharged home on POD#5, and in followup had no further symptoms.
Discussion:
The differentiation of arterial and neurogenic manifestations of MALS is an important refinement of our understanding of this disease, which I believe to be a byproduct of our bipedal lifestyle. The lordotic curvature of the spine, necessary to balance our upper torso on a vertical spine, pushes the spine forward and applies tension to the median arcuate ligament, along with other structures such as the duodenum and left renal vein in superior mesenteric artery syndrome and nutcracker syndrome, and the left iliac vein in May-Thurner Syndrome.
This compression is not only enough to narrow the celiac, but injure the artery by crushing. Stenting here does not do well because of the external compression and even after release, the artery may be damaged and require repair.
The chevron exposure heals well and is well tolerated and offers perfect exposure. While I was doing it, it occurred to me that a laparoscopic bypass is technically possible, and may be preferred to the long incision. Recent multi-institution study of MALS treatment would suggest laparoscopic approach offers a lower complication rate compared to open surgery (ref 2.)
The critical thing is having more surgeons recognize the compression that occurs in the abdomen and manifests in disparate and unconventional ways. The key is tying pain to a lesion, a mechanism, a nerve, just the way Cope’s does.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
DeCarlo C, Woo K, van Petersen AS, Geelkerken R, Chen AJ, Yeh SL, Kim GY, Henke PK, Tracci MC, Schneck MB, Grotemeyer D, Meyer B, DeMartino RR, Wilkins PB, Iranmanesh S, Rastogi V, Aulivola B, Korepta LM, Shutze WP, Jett KG, Sorber R, Abularrage CJ, Long GW, Bove PG, Davies MG, Miserlis D, Shih M, Yi J, Gupta R, Loa J, Robinson DA, Gombert A, Doukas P, de Caridi G, Benedetto F, Wittgen CM, Smeds MR, Sumpio BE, Harris S, Szeberin Z, Pomozi E, Stilo F, Montelione N, Mouawad NJ, Lawrence P, Dua A. Factors Associated With Successful Median Arcuate Ligament Release in an International, Multi-Institutional Cohort. J Vasc Surg. 2022 Oct 25:S0741-5214(22)02443-0. doi: 10.1016/j.jvs.2022.10.022. Epub ahead of print. PMID: 36306935.
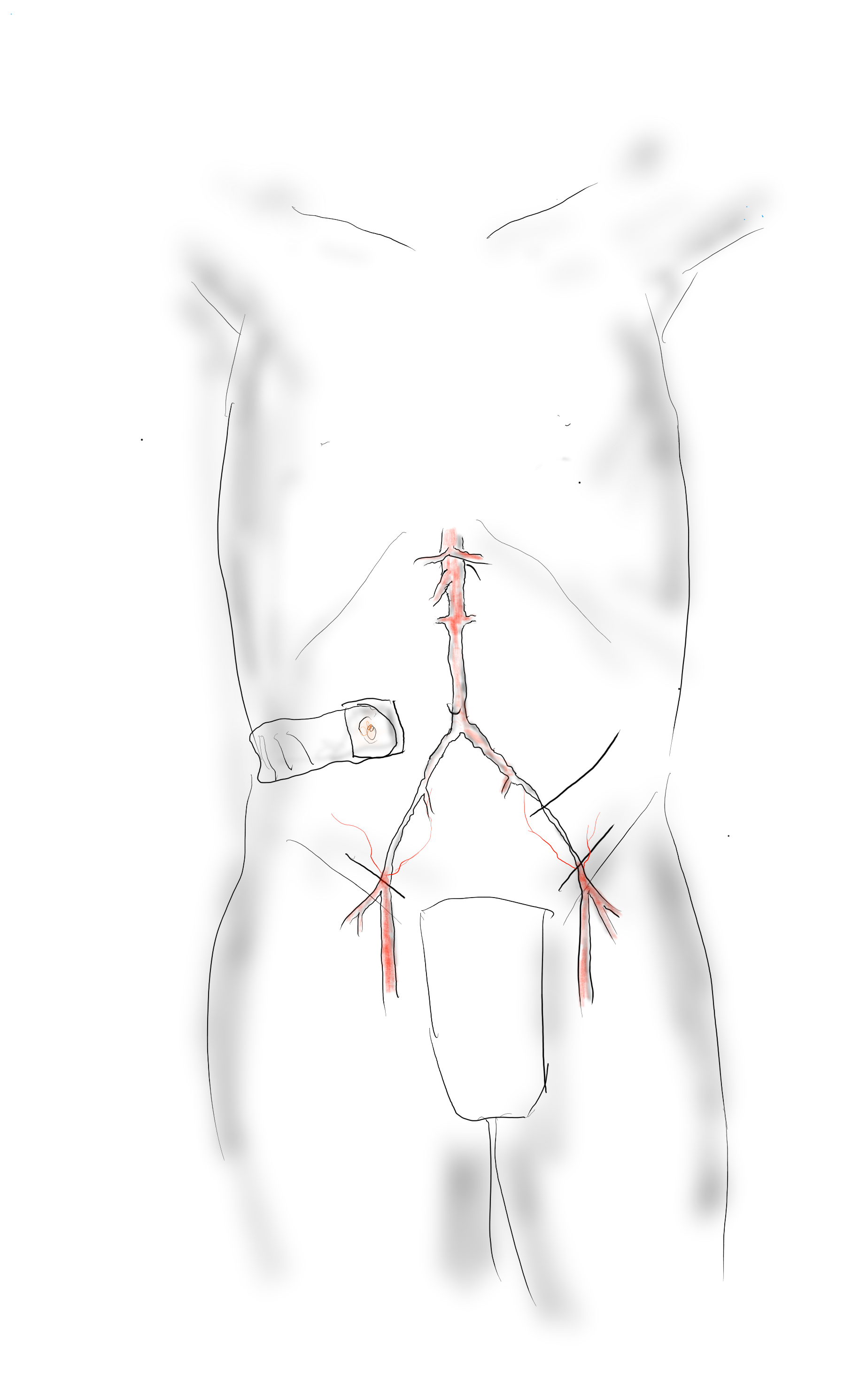
I had posted the above picture from over 15 years ago during my time in Iowa of my hybrid AUI-Fem-Fem (under unclampable 2, link). This technique came back to me as I was strategizing the upcoming aortic revascularization of a patient with iliac occlusions with the added complexity of an ileal conduit in the right abdomen. He had multiple failed prior iliac stents and failed femorofemoral bypasses -his right CIA and EIA were occluded while the left EIA had become occluded resulting in ischemic rest pain. While the picture alone is sufficient for me, it was brought to my attention by Dr. Joedd Biggs, fellow alum of the Mayo Clinic, on faculty at University of Kansas Hospital, that more detail was needed. So while resting my tired dogs, I got on my tablet and drew it out. Joedd, I present you my technique for a hybrid AUI-Fem-Fem bypass of the aorta.
This technique is made easier if one of the iliac arteries are patent. It is not a necessary condition.
The image above shows the necessary incisions for the femorofemoral bypass and the retroperitoneal pelvic (transplant) exposure of the left iliac bifurcation. I nearly always make oblique rather than vertical skin incisions in the groin to avoid wound complications from incising the inguinal crease orthagonally.
The transplant exposure facilitates a retropubic tunneling of the femorofemoral bypass which is performed first.
A left lower quadrant retroperitoneal exposure of the pelvis is performed -this is a standard renal “transplant exposure.” The two groin incisions are made and the common femoral arteries are exposed. Endarterectomy may be performed, although if the orifices of the SFA and PFA are patent, I don’t. The bypass graft is tunneled retropublicly and this is facilitated by the transplant incision. I generally use a 7mm ringed PTFE graft. Once done, the common iliac artery is divided above its bifurcation and the bifurcation is oversewn or stapled. A 12mm bypass graft is then sewn end to end to the common iliac artery (below).
The secret sauce in this technique is the end-to-end anastomosis of a 12mm bypass graft to the common iliac artery.
Through the conduit, a suitably chosen iliac limb of an EVAR system is brought through to the aorta and deployed with its end across the anastomosis into the conduit. A Gore Excluder 12mm ending iliac limb is ideal as its proximal end is appropriately sized for the diseased abdominal aorta. The limb is then aggressively ballooned to profile, particularly in the 12mm graft (below).
The Excluder 12mm limb works nicely and will seal against the 12mm bypass graft with sufficient overlap. It is then aggressively ballooned to profile from inflow to end.
The 12mm conduit graft is then sewn end to side to the femorofemoral bypass (below), completing the AUI-Fem-Fem.
I believe there are hemodynamic advantages to this over reintervening on native aortoiliac segment. First, size does matter, and until a suitable aortoiliac occlusive disease stent graft system is engineered, this represents an optimum. The Gore excluder graft limb is 16mm proximally and this is usually more than enough to diameter for the diseased abdominal aorta. The end diameter of 12 or 14.5mm will seal nicely in a 12mm conduit. I have not used a 16mm conduit only because I prefer not rupturing the aortic bifurcation with the “aggressive ballooning” mentioned above. The 12mm diameter is the boundary above the “small aorta syndrome” diameter of 10mm.
If the iliac is occluded, a wire can be driven through it from above and the conduit sewn over it. The iliac limb can be delivered after some pre-dilatation then followed by the “aggressive ballooning” of the iliac limb. The deployment into the conduit creates a stable “endo-anastomosis.”
Patients like my upcoming patient usually fail intervention due to the lumen size issues. An 8mm fem-fem bypass fed by a diseased series of iliac stents with at most 7mm lumen diameter is a recipe for the development of mural thrombosis and occlusion. The lower half of the body are fed by the diseased conduit of the donor EIA. This way, true aortic inflow is created.
I recently had lunch with Dr. PJ O’Hara, emeritus professor, and former partner of mine from the Cleveland Clinic. We hadn’t met since 2018 at the VAM in Boston, while I was still in Abu Dhabi. It was a recent case I did that caused me to reach out. I won’t be posting that recent case in detail today -it was a patient who had had multiple aortoiliac interventions for aortic bifurcation disease, but who closed up their stents within a few months of intervention. Rather than subject that patient to another round of interventions, I chose aortoiliac endarterectomy because the prior interventions failed to address the basic problem of the undersized aorta and iliac arteries.
The last case that Dr. O’Hara did before retiring was an aortoiliac endarterectomy which I assisted with, nearly a decade ago. During that case, Dr. O’Hara mentioned a video he had put together for an SVS meeting. He was kind enough to give me a copy share.
Aortoiliac endarterectomy -forget thee not!
The modern application of this technique is in the removal of occluded aortoiliac stents. The aorta and iliac arteries are restored, and yes, stents can go back in if needed.
A quick survey of some of my contacts at major centers reveals that this technique is rapidly becoming forgotten as its practitioner retire or revert to teaching the technically easier aortobifemoral bypass (ABF) graft. I hope to revive this because I know there are many patients who have challenging anatomy for ABF but potentially could undergo plaque and stent removal and restoration of their aorta and iliac arteries.
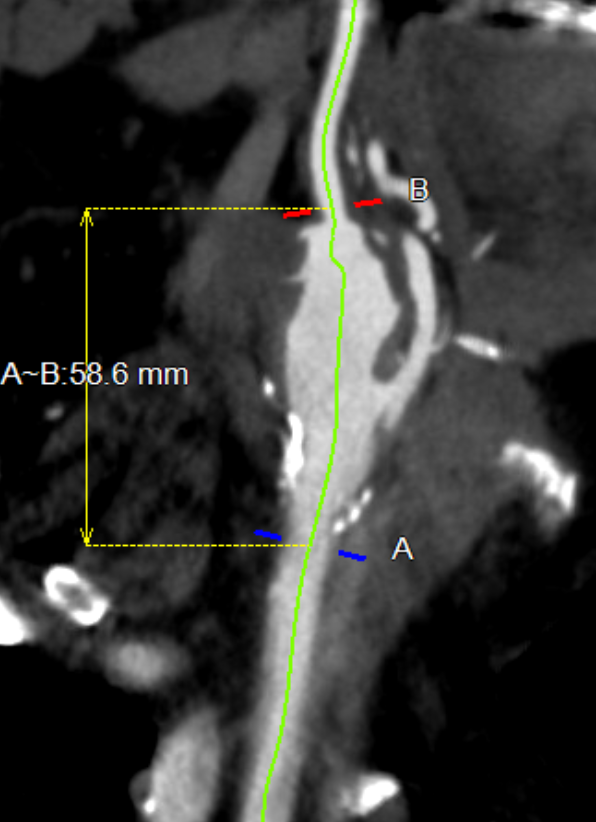
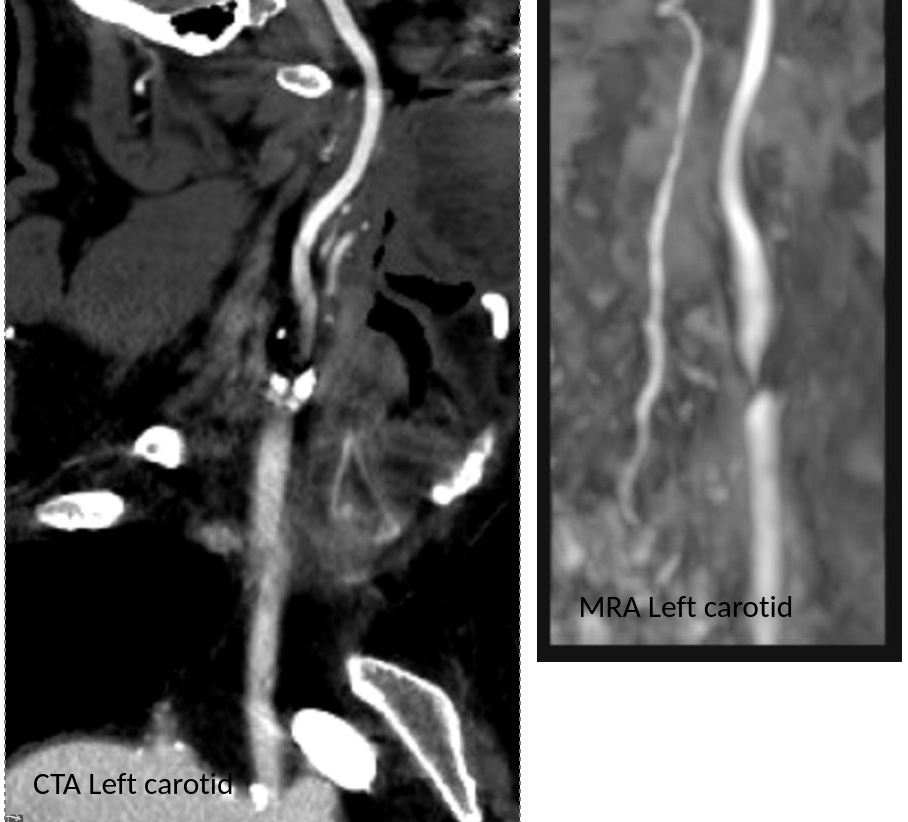
CTA tends to overread stenoses which was in the 60-79% range on duplex
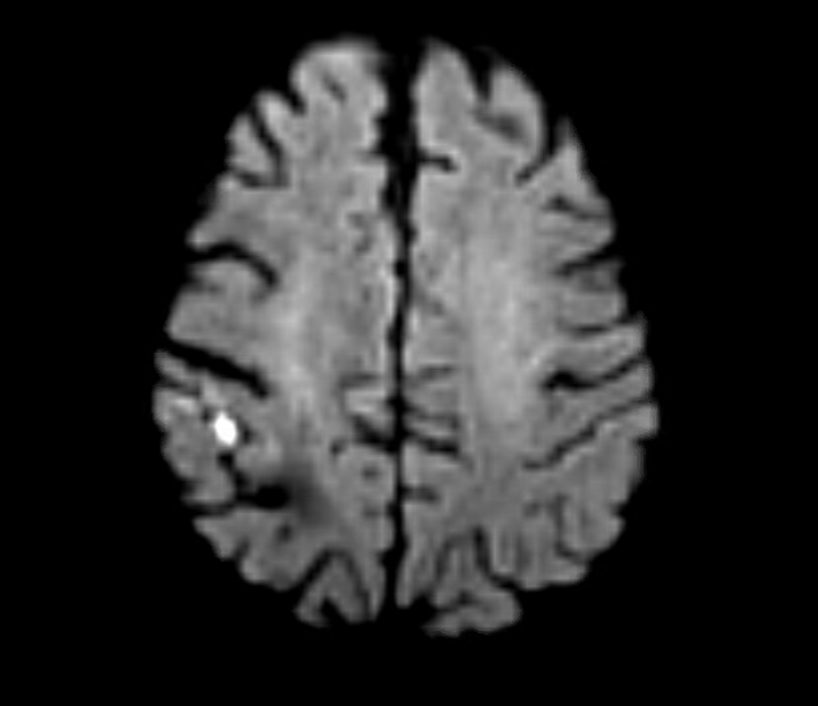
The patient is a middle aged executive who complains of bouts of aphasia triggered by intense conversations and business meetings. It first occurred while driving to Dubai on a conference call. Since then, they occurred several times a week, typically triggered during meetings where he needs to think and speak. Casual conversation and cognition does not seem to trigger this. Workup revealed a heterogeneous plaque affecting the left ICA with velocities in the 60-79% range. CTA confirmed this plaque. MRI failed to show any stroke or other lesions. Neurology evaluation showed normal exam. The patient underwent endarterectomy, and had a normal recovery. In followup, he denied any further episodes of aphasia.
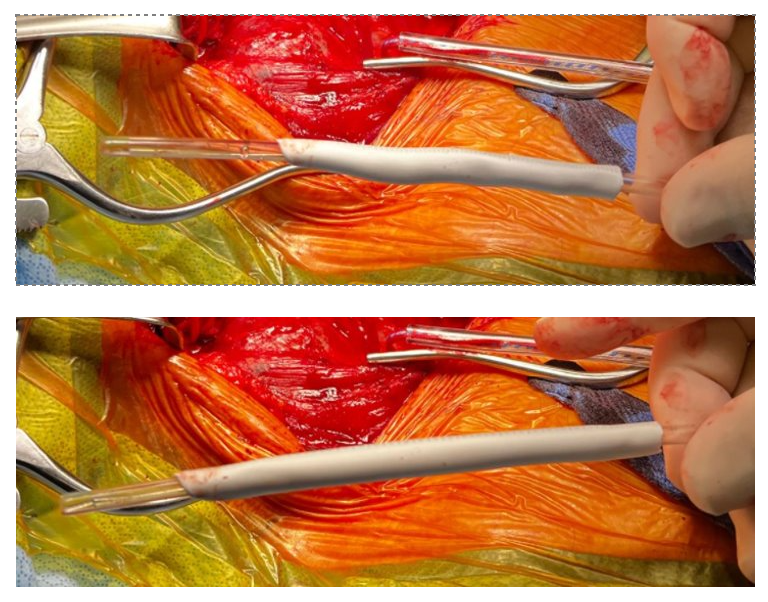
Standard endarterectomy with patch
Aphasia, the loss of function in the language centers, typically of the left brain, although in a minority, it may live in the right hemisphere, is terrifying manifestation of stroke. This case, if examined superficially, is nothing special in that TIA’s associated with a reasonable culprit lesion went away after elimination of that culprit lesion. To me, it was fascinating because it represents a possible case of brain claudication.
The human brain is believed to have evolved to its large size in conjunction with bipedalism, social hunting and gathering, and climate change in the Great Rift Valley favoring a savannah over forests, that created heat stresses on the brain, favoring the development of sweating and redundancies in brain tissue. The advent of fire and cooking enhanced available calories to feed this enlarged brain’s metabolic needs. When the metabolism isn’t supported through adequate blood supply, the brain tissue dies. Rarely, it blinkers on and off, and even more rarely, this occurs in the motor strip triggering today a neurologic evaluation including a carotid duplex that brings these patients to our attention. The fascinating question for me is, does increased metabolic demand in the form of complex thinking result in a supply-demand mismatch much as seen in exercise induced angina or claudication? If it can, can we test for it?
The tests we have available are hemodynamically based. At its simplest, after carotid angiography, an occluding balloon can be inflated to test for symptoms. This is an archaic test and I do not do it. There are nuclear medicine, PET CT, and MRI tests that use pharmacologic agents to induce hypotension, but again, for this patient, it wouldn’t apply. This patient needed the equivalent of a treadmill in the MRI machine. Maybe having him read a dry, technical treatise on neurobiology taped to the MRI tube?
I went to the OR with the indication of TIAs associated with a >50% lesion, but I did tell the patient that it was possible his thinking-induced aphasia would not remit. Thankfully it did.
Steve Jobs is credited with popularizing the saying credited to Pablo Picasso, “good artists copy, great artists steal.” While its provenance may be apocryphal, it makes an excellent point about how we learn. Even in the lack of understanding, it is still possible to learn by copying. Toddlers do this. We, as land mammals, are hard wired to copy.
Take for example this patient below with Leriche syndrome with a triad of smoking, claudication, and impotence.
Aortoiliac occlusive disease with history of smoking, claudication, and impotence in a middle aged man = Leriche Syndrome
Because of his relative youth, being his 50’s, I felt the most appropriate procedure was an aortobifemoral bypass.
I frequently use these diagrams to illustrate for the patient.
The only real complexity to manage was the severe stenosis he had in his left renal artery.
A severe stenosis of left renal artery
The options included
renal endarterectomy as part of aortic thromboendarterectomy
renal artery bypass from the aortic graft
reimplantation of renal artery
something else
Something Else: The complexity of renal revascularization creates risk. An antegrade endarterectomy of the renal artery would be done below a suprarenal clamp, adding to clamp time. A bypass would require the kidney to bide its time during the proximal aortic anastomosis, and the anastomosis for a jump graft, then the anastomosis to the left renal artery. This renal ischemia time can be extended by cooling the kidneys with cold (5 degree) LR, but why risk it? A renal endarterectomy can devolve into a visceral segment endarterectomy. After an hour, a nephrectomy.
That’s where this whole copying concept comes into play. Back in 2012, I worked with Dr. Jeanwan Kang, who had just come out of training with Dr. Richard Cambria. We were doing a type IV thoracoabdominal aortic aneurysm, and the right renal artery had a ostial stenosis. While I was figuring out the best way to manage this, Dr. Kang asked for a 6x18mm renal stent and an insufflator. She stuck the stent into the renal orifice and deployed the stent, opening the orifice. I had to find my jaw which had dropped to the floor.
Now, ten years on, that’s how I managed this patient’s ostial renal artery stenosis.
The patient’s thrombotic plaque went up to the renal origins and needed to be endarterectomized, but embarking on a renal endarterectomy adds potentially harmful renal ischemia time. Therefore, through the vertical aortotomy, I was able to get a clean end point to the aortic thromboendarterectomy and position a stent in the renal orifice and deploy it.
After thromboendarterectomy of the aortic plaque, the left renal ostium is treated with a balloon expandable stent. The aorta then is partially closed primarily to move the clamp below the renal arteries
Once the stent was deployed, the aorta was partially closed primarily to allow the clamp to be moved below the renal arteries. This all took less than ten minutes of ischemia time. The aortic graft was then sewn end to side to the remaining aortotomy.
The patient recovered and was discharged on POD#6 with normal renal function. In followup, his CTA showed excellent graft and stent patency.
A followup CTA shows a patent 14x7mm aortobifemoral bypass. I choose the bypass based on avoiding excess size mismatching distally as I find that patients who get 20x10mm grafts run into problem with mural thrombus because of limited flows into smaller femoral vessels. The renal stent is patent.
The centerline view of the renal stent shows it to be widely patent.
Patent stent with avoidance of the pitfalls of a renal endarterectomy
The patient is walking well without limitations and has improved blood pressure control, achieving normotensions at times.
If you are curious about the results from MGH, I refer you to their paper on 67 patients treated with open hybrid revascularization of the renal artery during complex aortic reconstructions (reference). At a mean followup of a year, they reported a 98% stent patency.
There is a comfort in sticking to what you know. The extreme example of this is the practitioner who graduates with a skill set from training and never expands on it. Yet there is an opportunity cost to blind devotion to sticking what you know and that is never growing. I recall this in the panel discussions during the VEITH Symposia I used to sneak into as a resident in the 90’s where great authorities pooh-poohed or condemned anything endovascular.
It’s a sign of a nimble mind that Dr. Cambria, after learning endovascular techniques mid-career, adapted these skills to his open surgical toolkit. His trainee, Dr. Kang, soon after, taught me.
Or was I just looking over her shoulders taking notes?
Reference:
Patel R, Conrad MF, Paruchuri V, Kwolek CJ, Cambria RP. Balloon expandable stents facilitate right renal artery reconstruction during complex open aortic aneurysm repair. J Vasc Surg. 2010 Feb;51(2):310-5. doi: 10.1016/j.jvs.2009.04.079. Epub 2009 Oct 22. PMID: 19853403.
The patient was a 50 something year old man who I took care of in 2016 before I left for Abu Dhabi. He had a background of hypertension, hypercholesterolemia, and IDDM with chronic immunosuppression for rheumatoid arthritis. For several weeks he had rest pain in his feet and impending gangrene of his left great toe. More worrisome was the development of punched out ulcers on his groin crease resulting in weeping wounds after a bout of cellulitis. He had no palpable femoral pulses. Pulse volume recordings showed flat lines from the thigh to the feet.
CTA of the abdomen and pelvis with runoff showed aortic occlusion due to heavily calcified plaque with reconstitution of the external iliac arteries via the internal iliac arteries. The common femoral arteries were only mildly diseased and there was patent runoff.
Centerline up right femoral into aorta shows occluded aorto-iliac segment and diseased external iliac artery. Centerline up left femoral into aorta shows mirror image of disease on left side
He was one of the rare instances of chronic limb threatening ischemia due to aortoiliac occlusive disease, AKA Leriche syndrome. The added background of autoimmunity made him vulnerable to the ulcers in the groin crease, and the infections there made access challenging.
Leriche Syndrome
The choices were endovascular versus open surgical repair. The groins were a problem with recent cellulitis, immunosuppression and open wounds, but with careful prep, and coverage with Ioban, access was possible, even for stent grafting. The problem was the aortic bifurcation was heavily calcified, and manipulating this likely thrombotic material with an end stump of aorta can cause renal embolism. There was a small risk of rupture at the bifurcation and of renal failure.
Standard aortobifemoral bypass graft was out of the question because of the lack of a safely clampable aorta -there was circumferential aortic plaque below and above the renal arteries and the infections in the groins would jeopardize any prosthetic graft. You have to respect unclampable aortas but like anything else, there are ways around it (link).
Regarding the groins, during fellowship, Dr. Thomas Bower used to take the distal anastomoses to the external iliac arteries which could be exposed via short lower abdominal incisions if not through the midline incision itself, avoiding groin incisions in hazardous groins.
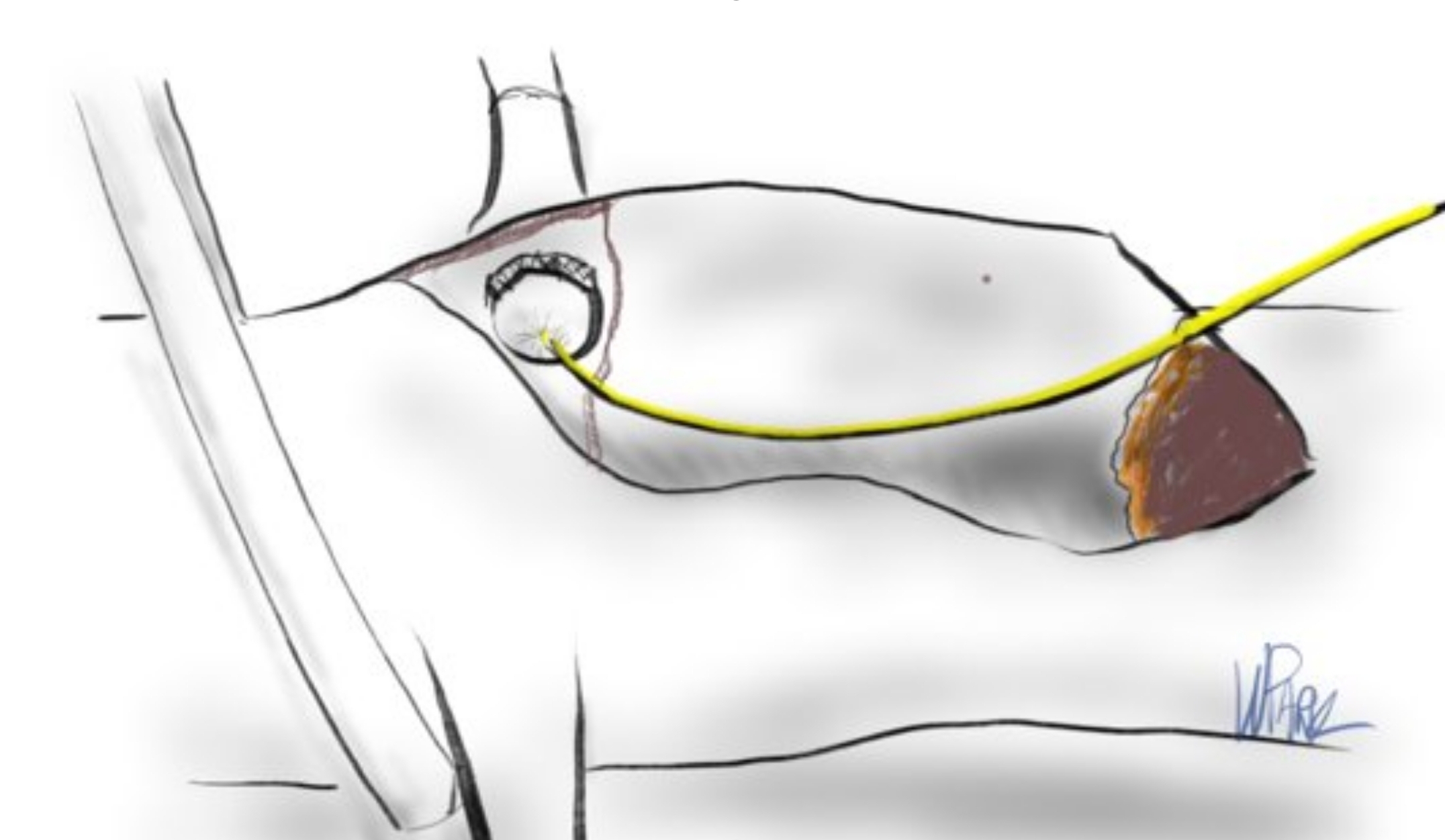
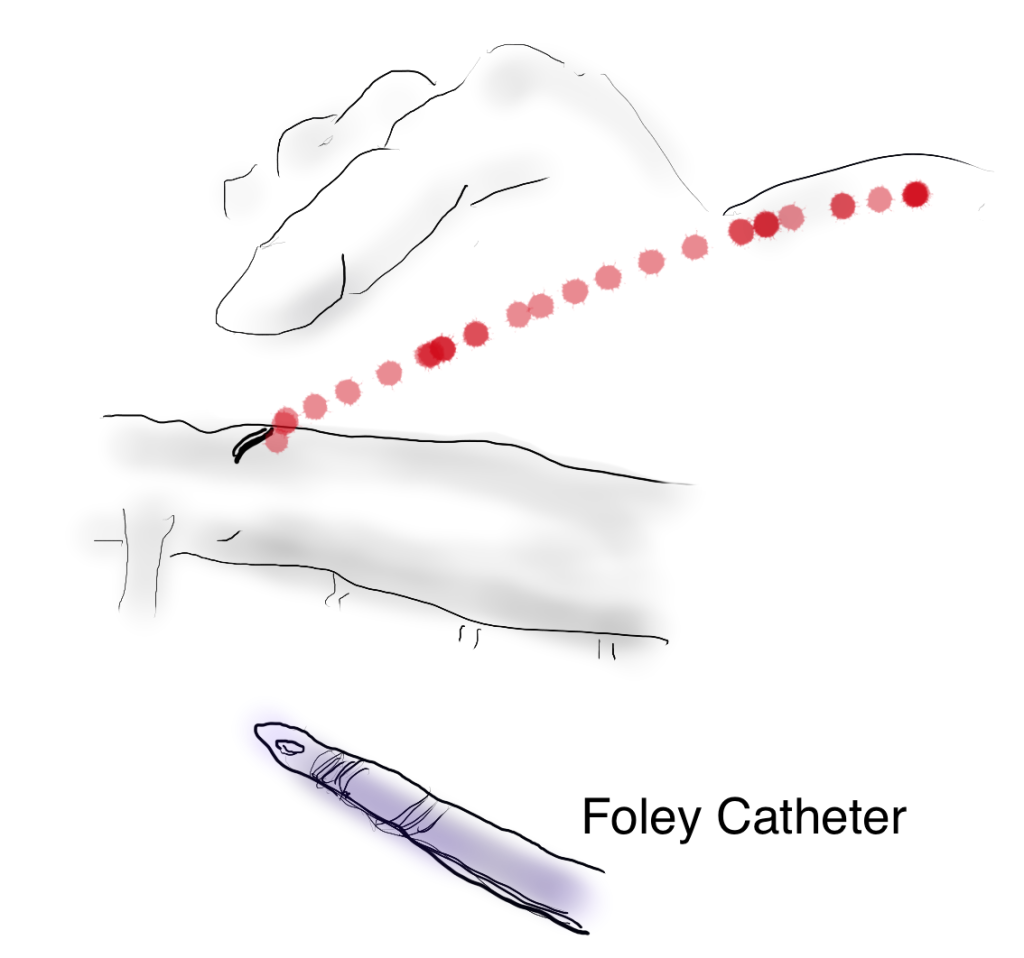
I performed an aorto-bi-iliac bypass using the balloon in the infrarenal technique after obtaining supraceliac control described in my technical post (link).
A small aortotomy can be controlled with a finger and a foley easily slipped in -just remember to clamp itThis typically provides adequate hemostasis and space to perform a proximal anastomosis
I was able to endarterectomize a nice segment of aorta and anastomose end to side -always end to side as it preserves endovascular options. The distal anastomoses was to the external iliac arteries. He did well in the immediate postoperative period but I soon left for Abu Dhabi.
In the five years since the operation, he has needed an SMA stent and has devloped worsening CKD and autoimmune diseases. But one of the gratifying things is he healed his wounds on this groins and thighs and the left hallux, and pain has never recurred. He had a contrast CT at the 5 year point (figure) showing a widely patent graft, and he sought me out when he heard that I was back in Cleveland.
His PVRs remain normal (figure).
The PVRs and ABI’s remain robustly normal even after 5 years
I’m not saying that iliac stents from the iliac bifurcation to the renal arteries was a bad option, but there is a particular sadness and weariness when I have to take care of occluded stents. As an engineer, what is worse than ballooning an occluded stent and placing another stent inside? Knowing what I know about cell biology, what is worse than lasering, drilling, cutting, that cicatricial scar tissue that is neointimal hyperplasia in terms of what you leave behind. This man still has decades left to live and he will have his bypass graft far longer than any stent. This durability, a byproduct of the technique, is a worthy virtue.
When I operated, he was in his mid fifties and despite his comorbidities, was able to undergo a big operation. Now he is in his sixties and his autoimmune issues have progressed to where he is suffering from stiff person syndrome with difficulty walking. His renal function is poor and overall he is a terrible open surgical candidate. If I had done interventions at that time, which I was tempted to, he could today be facing amputations in the setting of cytotoxic immunosuppression having run out of endovascular options.
We have lost too much to innovation. The fact is, aortic surgery for critical limb ischemia was once and it still is a thing, because it works.
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
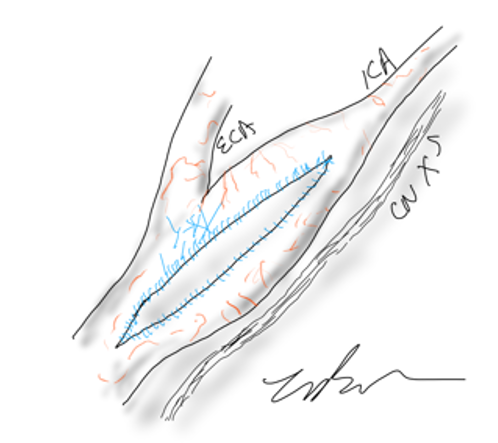
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
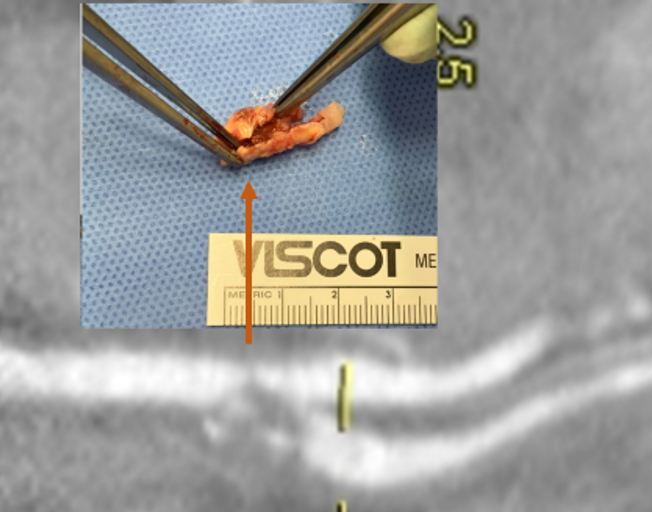
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
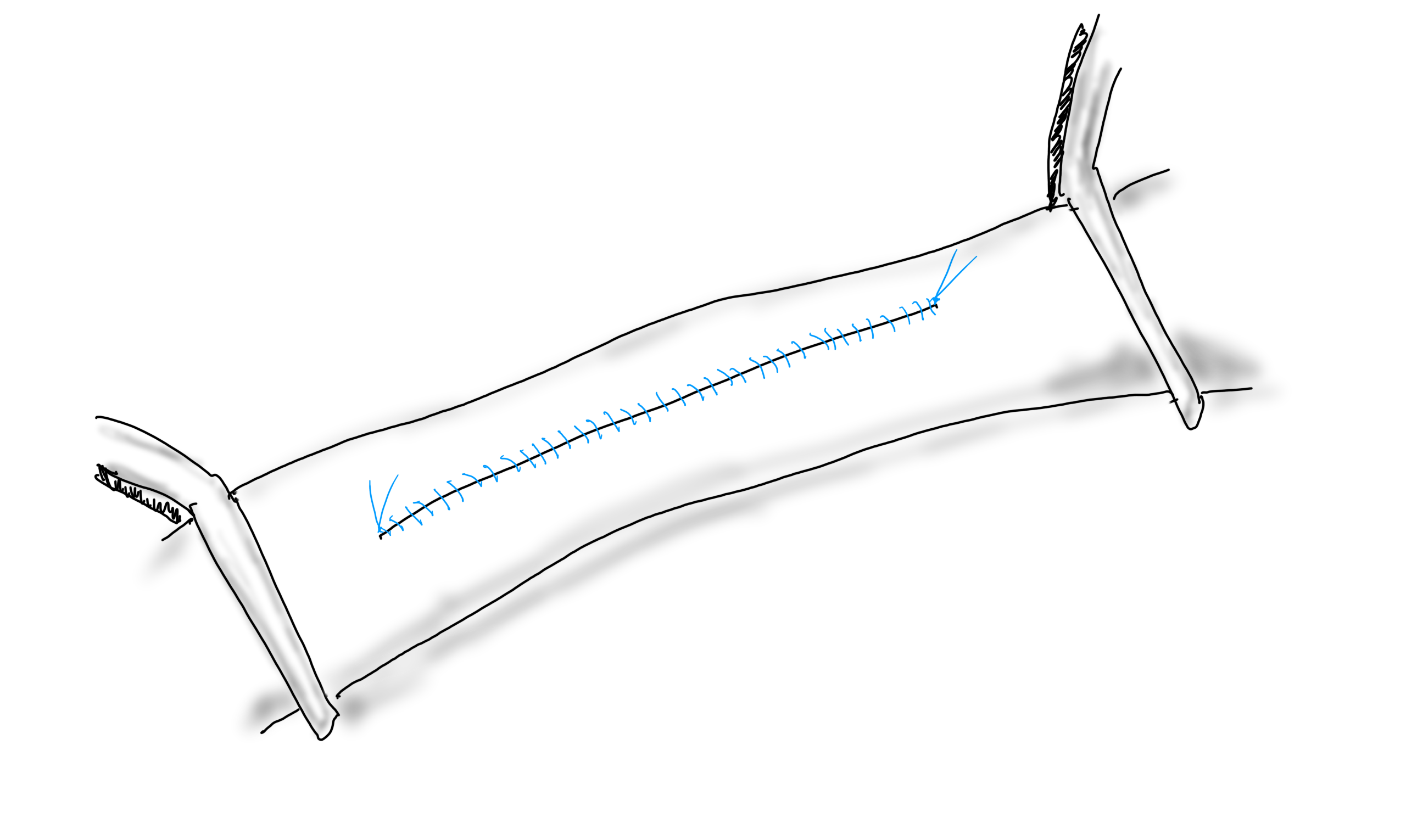
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
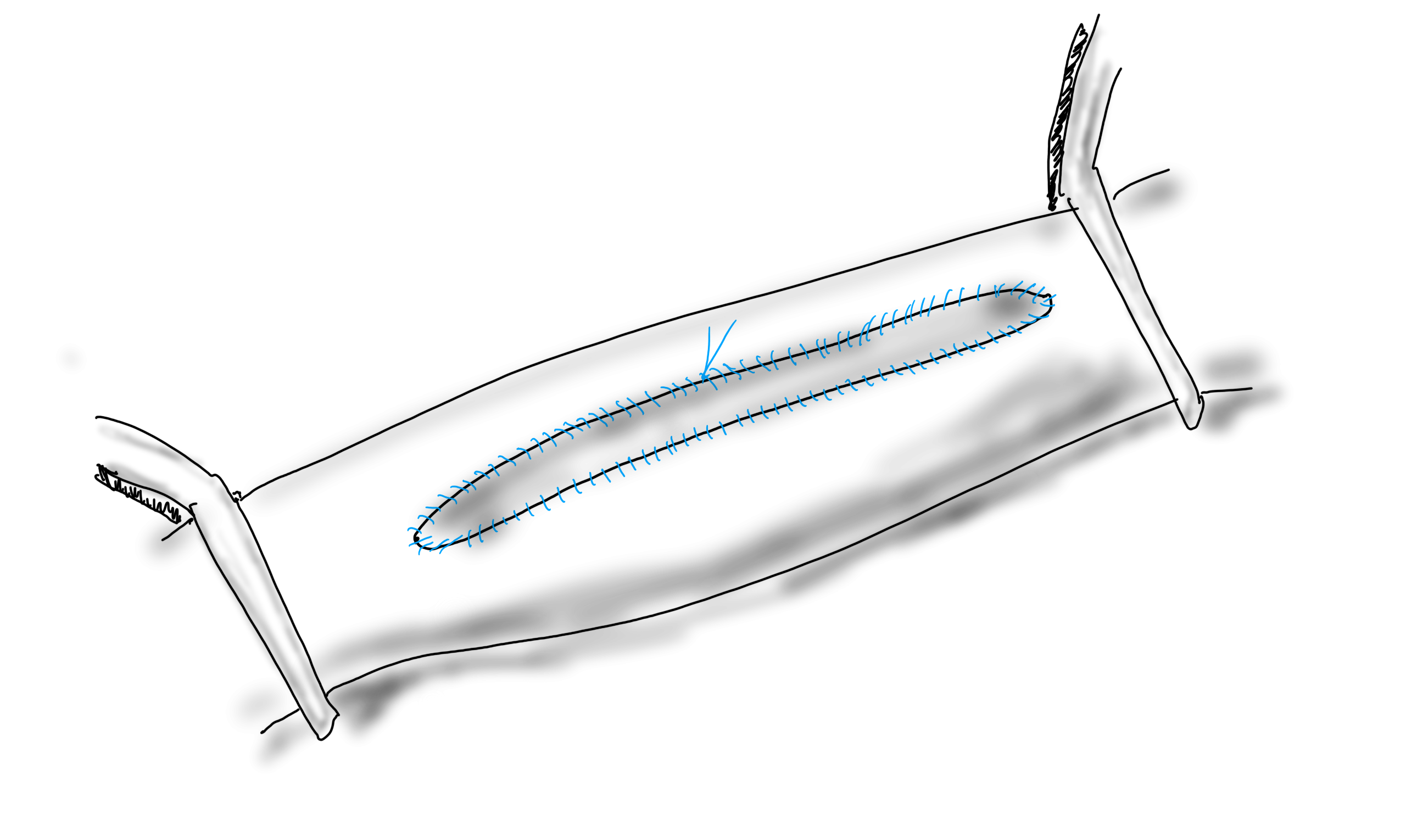
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
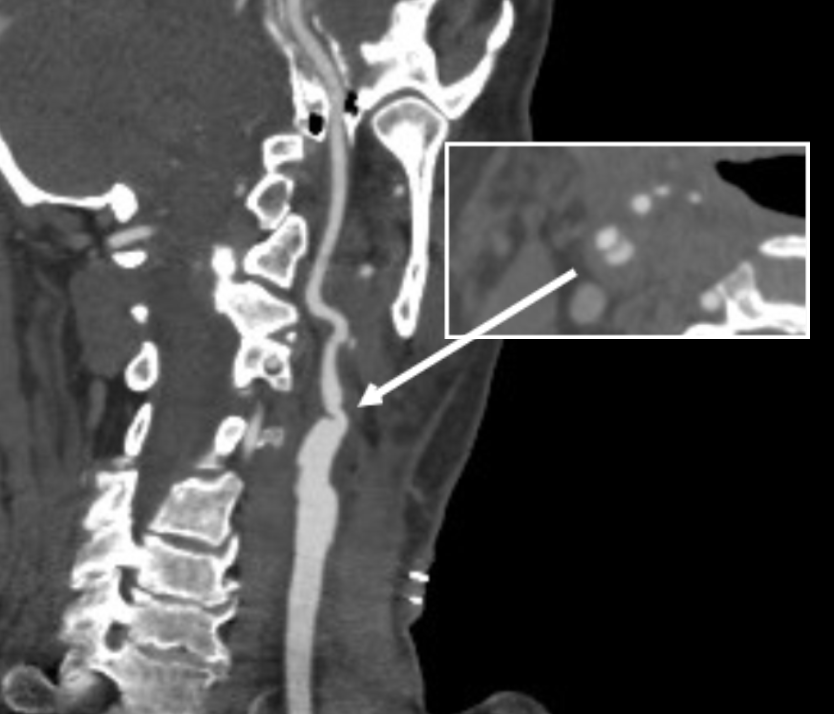
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
When I was a young attending at the Allen Pavilion of Columbia Presbyterian Hospital, I was called into an operating room for a stat consult on a patient about to undergo a cholecystectomy. During the case, the IV had infiltrated and a bag of saline had filled the patient’s hand and forearm with saline, causing the hand to look like an inflated glove. The fingers were cool and white and the edema was firm but yielded to touch.
I elevated the hand and firmly squeezed the edema out of each digit, then gently massaged the edema from the hand onto the forearm. From there, I pushed the edema onto the arm. I then wrapped the hand up in an Ace wrap, and suspended it from an IV pole and returned to my case. Later, I returned and the hand was restored, warm, and perfused.
The lymphatics serve to move extracellular fluid (link). They can be overwhelmed much as drainage from a house can be overwhelmed resulting in puddles and ponds (link). This extracellular space has been “discovered” to be a new organ, but vascular surgeons have known about it for some time. Ultrastructurally, it is very close to a sea sponge with lattices of structural protein connecting cells to form tissues. And like a sea sponge, the salty water can be squeezed out or drained using gravity.
In olden times in central Europe, if you had chronic leg ulcers, you went to abbeys that specialized in their care. There, nuns would milk the edema out of your leg swollen typically from parasites and dress the leg and ulcer in linen cloth soaked in special oils. This is how Dr. Paul Gerson Unna came up with his eponymous Unna’s Boot, substituting Zinc Oxide paste which created a bacteriostatic environment.
Professor Paul Gerson Unna
Every year or so, I will be consulted for what I term a lymphatic emergency. A subset of this is phlegmasia. Whatever color you find -alba (white) or cerulea (blue) is really no matter -who really knows which comes first? It is an emergency in that the time clock for arterial ischemia -minutes to an hour for nerves, an hour to 6 for skeletal muscles, 6-12 for skin and bone, are all in play. The instinct is to go right to fasciotomy, but what you are usually doing is releasing the extracellular space, and the muscles are typically fine, even though their compartment pressures were very high.
Take this patient who developed severe upper extremity edema in the recovery phase after a cardiac arrest.
The ICU staff noted the had discoloration about four hours after the arrest. There were no arterial pulses and the forearm and hand were rock hard, the finger tips ice cold. Compartment pressures measured using the arterial line and needle method didn’t drop after the initial flush of saline below 70mmHg. While I could have been justified in performing upper extremity fasciotomy and even trying thrombectomy in a critically ill, coagulopathic patient on multiple pressors, I could just as easily have been on solid ground for saying the life was more valuable than the dominant hand. Both would have been the wrong move.
I performed the nun’s milking maneuver mentioned at the beginning and lacking an Unna’s boot, I compressed and elevated the best I could with double gloving using a small sized glove and ACE wrap.
Notice the edema has segregated into the arm.
In the morning, taking down the dressing, and re-compressing, there was now a radial artery signal and the fingers were a much improved color. The pulse-oximeter waveform was near normal. As an aside -the pulse oximeter uses the same technology as the digital photoplethysmography for generating toe waveforms in the vascular lab -ie. a vascular lab at every bedside! We have collected and are analyzing the data on this for publication.
The pulse oximetry waveform is the same tech as digital photoplethysmography. Cotton cast padding (Webril) and Coban wrap is a good method of compression that avoids the problems with ACE wrapping.
It’s a hard thing to not run off to the operating room in most cases because that is how we are trained, but understanding how a patient got to that point is crucial in deciding if compression alone will work. If they call you from the ER about a patient with a swollen cold foot with diminished signals, you have to figure out the mechanism. Was it arterial occlusion, rest pain, and chronic dependency of the foot that resulted in this? Typically the swelling appears late. Was it heart failure and inability to walk, resulting in the patient sitting all day in a chair that is the cause? Was it pregnancy with a DVT? Was it the deadly sin of sloth? Only in arterial occlusion in a chronic presentation would compression be contraindicate. In this ICU case, the lack of arterial signal is secondary to the swelling, not the cause of it.
Elevation alone does not manage edema well. Only hanging upside down or being in water up to your neck…
Compression is a necessary component of treating lymphedema emergencies because elevation alone may be insufficient, particularly in the leg.
Wrapping a leg is a critically, undertaught skill. Also, never cover the knee cap.
Elastic compression is ubiquitously available as the ACE wrap, but they can shift and move and roll, causing zones of excess and not enough compression. TED hose and compression stockings are definitely helpful in long term management, but with legs, compression needs to go up to the knee joint, or up to the groin, never halfway or the edema will create a line of ischemia at the end of the stocking that blisters when the stocking is removed, and can progress to full thickness necrosis. Cotton cast padding and Coban, or an Unna’s Boot may be the safest in terms of avoiding skin injury.
ACE wrapping is never taught adequately, and for it to work well and avoid injury to the skin, the wrapping has to be reapplied several times a day. It should be a prerequisite for nursing and medical student certification, as edema is the most common vascular disease.
Moving into our new home after four years out of country, I welcome an old friend from storage, but also unfortunately a health hazard, only mitigated by being fully reclinable.