The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
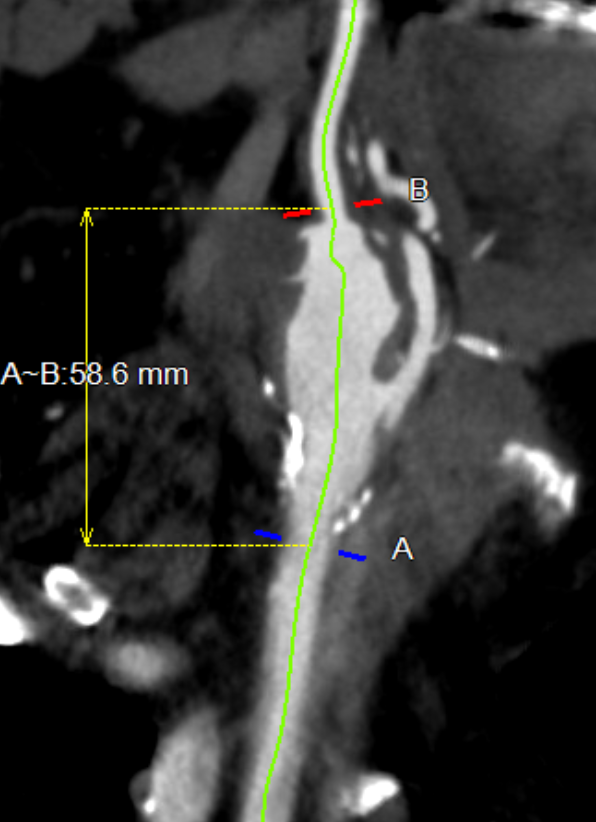
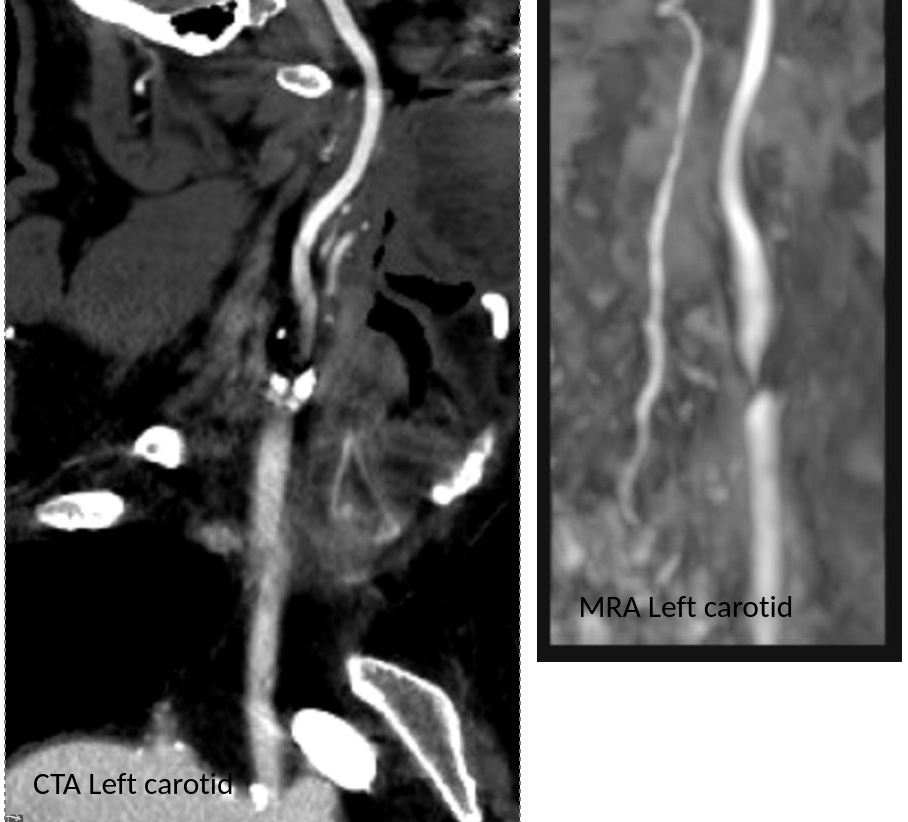
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
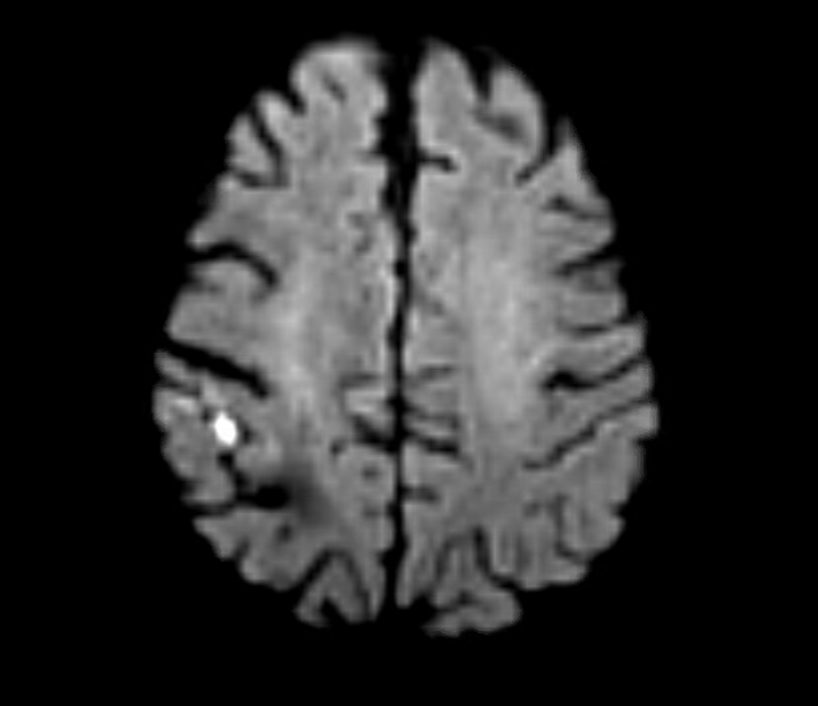
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
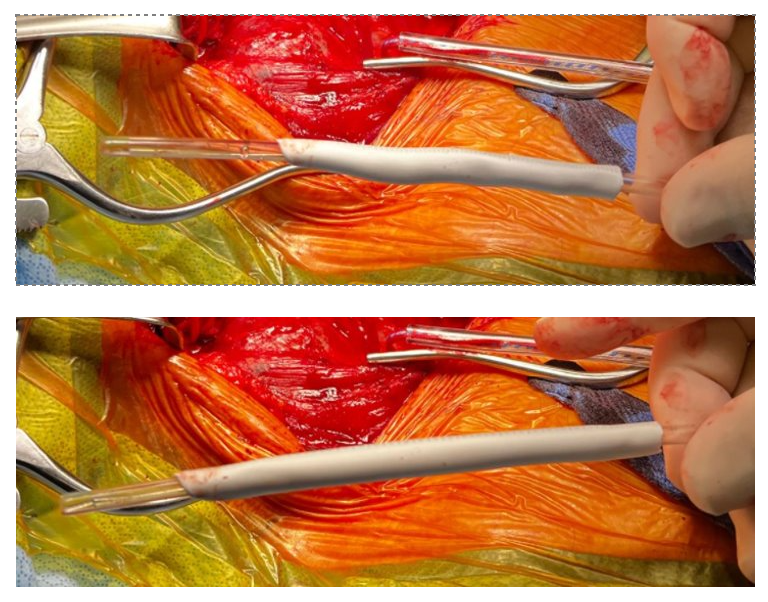
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
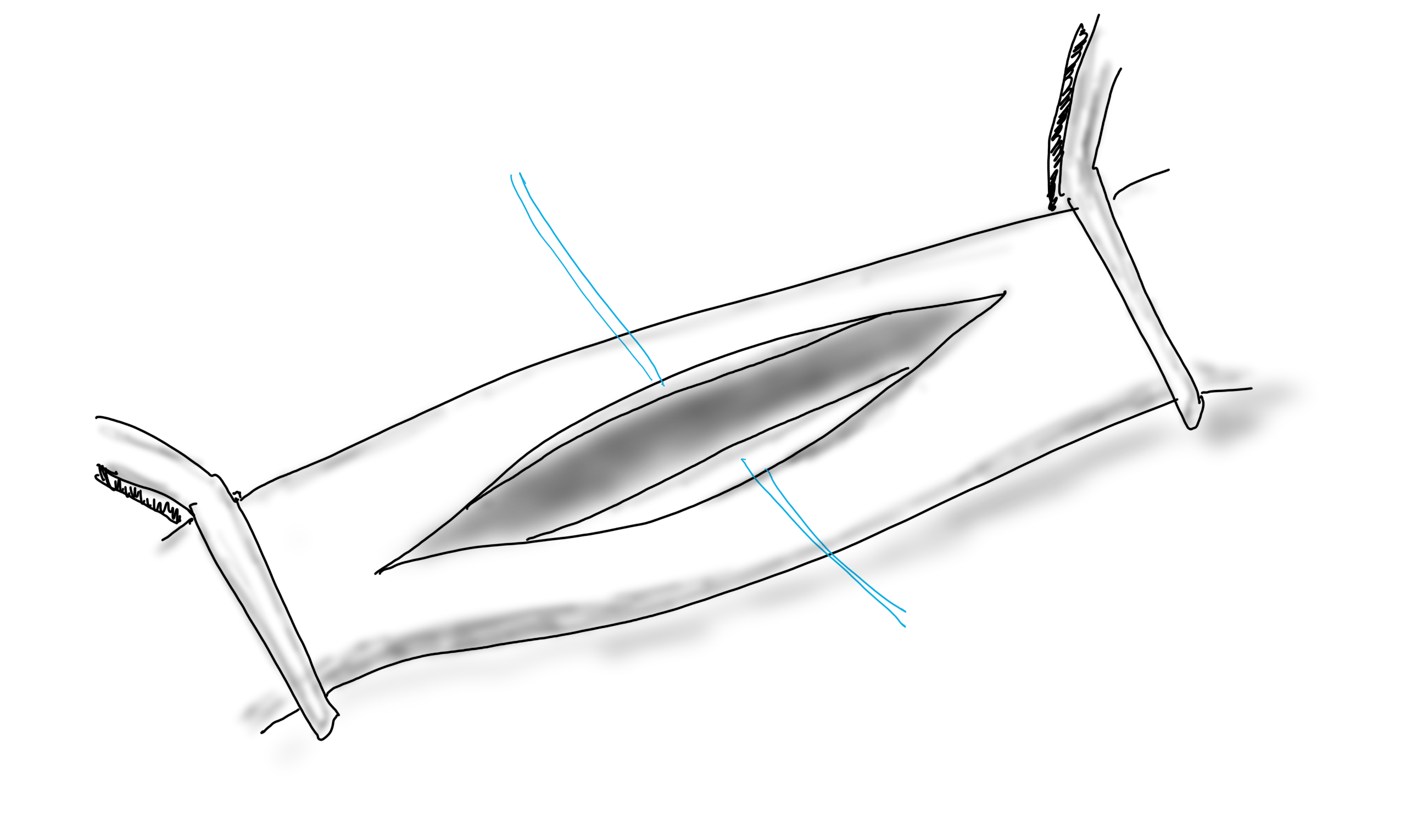
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
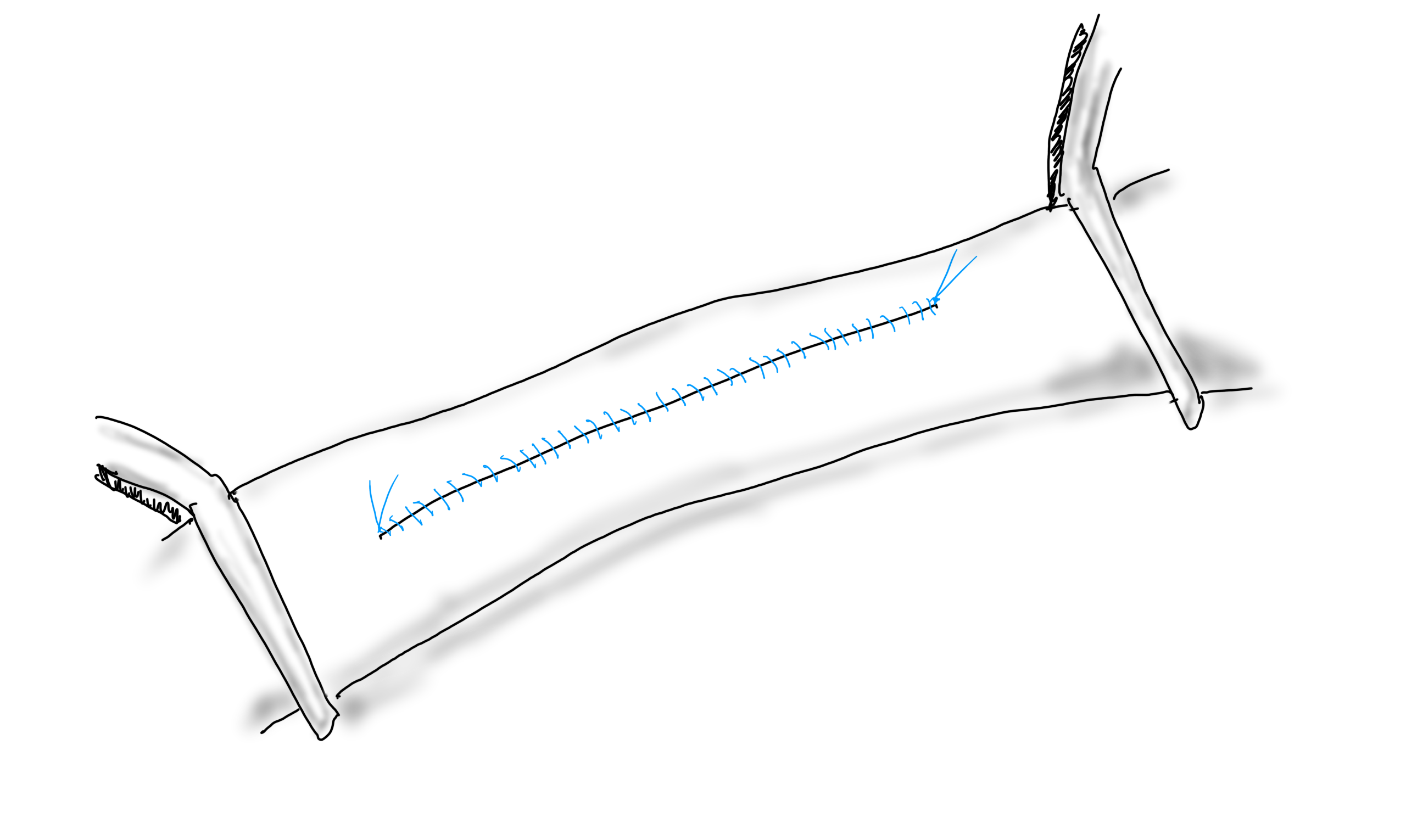
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
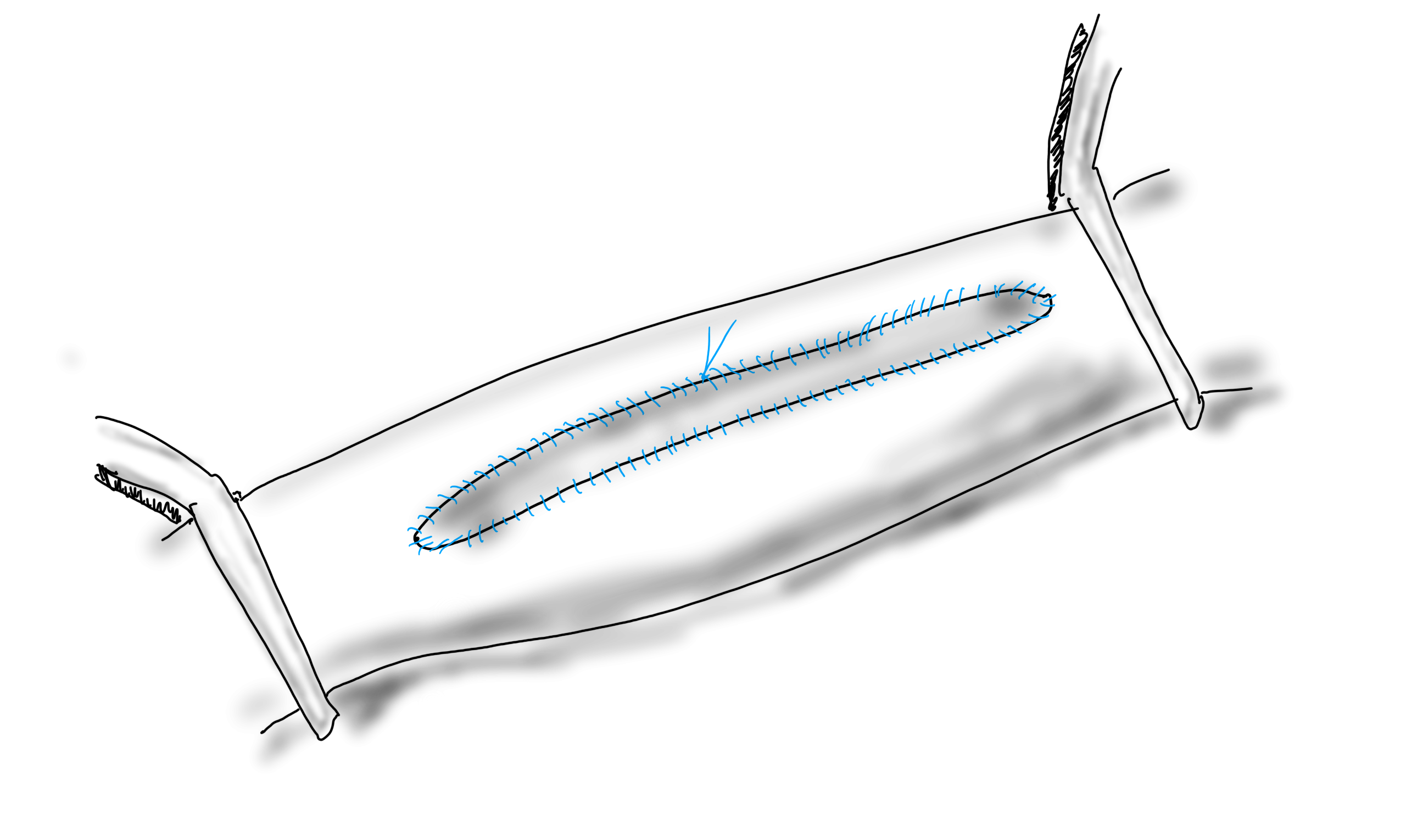
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
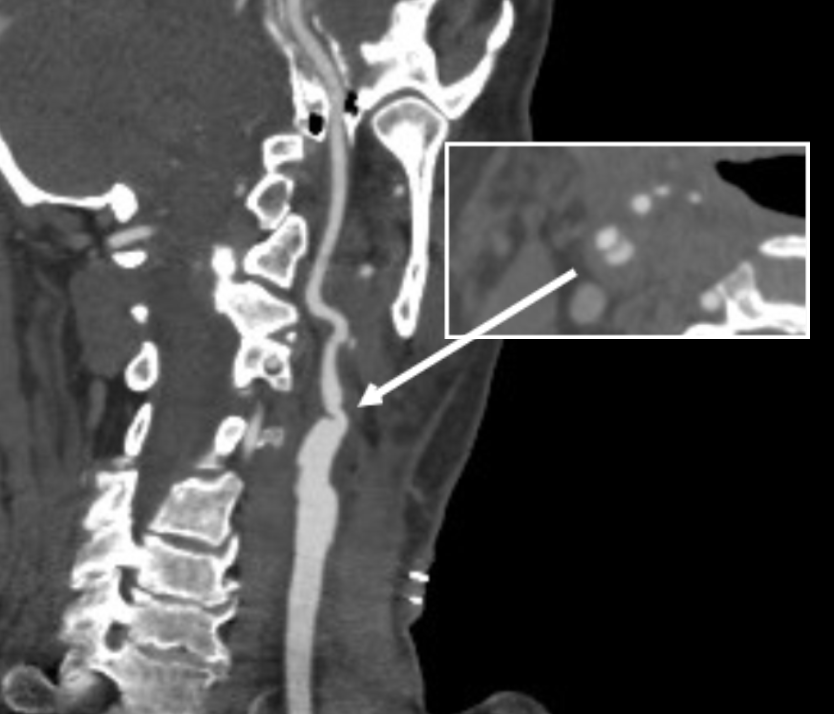
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
Patient with infected femoral pseudoaneurysm, skin necrosis, about to blow
A surgeon from Nepal posted a case of a ruptured common femoral pseudoaneurysm infected from IV drug abuse on LinkedIn. The comments centered around typical textbook responses which were:
Ligate, debride, obturator bypass
In situ bypass with femoral vein +/- sartorius flap
Rifampin soaked graft or crypreserved allograft
Ligate only
My preferred treatment is #2, in-situ bypass with harvest of adjacent deep femoral vein. I never liked that procedure because in general in these patients, everything bleeds. Then I had a thought -how about if you mobilize the external iliac artery in the pelvis over its entire length and pull it out from under the inguinal ligament to sew to the femoral bifurcation or SFA? That is, when you enter the pelvic retroperitoneum to gain proximal control:
The external iliac artery is usually redundant and elastic in young people
You mobilize the external iliac artery from the iliac bifurcation to the inguinal ligament, detaching the inferior epigastrics as a last step. And then you pull it out from under the inguinal ligament, and anastomose it to the femoral bifurcation or the SFA.
The mobilized external iliac artery is pulled down to reach normal femoral artery. The distance x is the length of CFA that needs replacing
This makes sense because in young people and those with AAA and minimal atherosclerosis, the external iliac artery is both redundant and elastic, making it suitable for a pull down transposition. But then, how do you know as you mobilize the artery in the pelvis that you have enough to pull down?
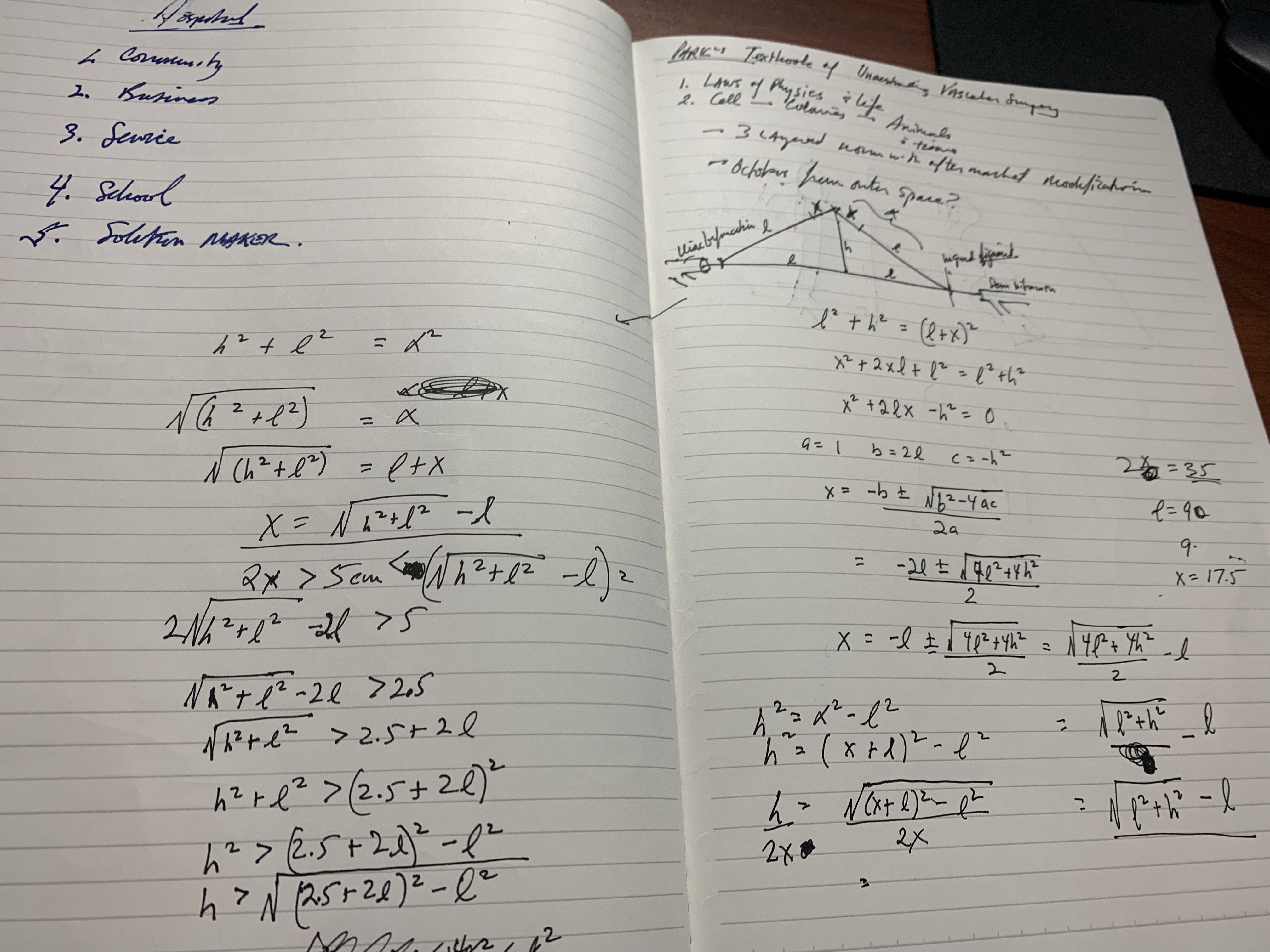
Pythagoras figured that out two an a half millenia ago. If you measure the straight line distance from iliac bifurcation to the takeoff of the inferior epigastric arteries, you get the straight line external iliac artery distance. The length of the common femoral artery which is the excess EIA length needed, is assigned the value x. Then the height of the stretched artery off the line between the iliac bifurcation and the inguinal ligament will determine how much extra artery you have.
Taking these values, I did some maths.
The solution for h, the height, is highlighted in yellow below. (note, the variable x in my notes is half the length of CFA, l is half the length of EIA, ie. 2x is CFA length).
Creating a spreadsheet for CFA lengths from 2 to 6cm and EIA straight distances of 5-10cm, the ratio of height H to CFA length varies from a minimum of 0.7 to maximum of 1.7 with an average of 1.1. That means the majority of the time, if you get 1.5x the length of CFA height off the pelvis, you should reach.
If you are short, you can detach the profunda and mobilize the SFA, pulling upwards, then reattach the PFA. Though this is entirely a thought experiment, there is no reason why it should not work. As with most things, I predict that it already has been done!
The advantages are using autologous tissues and leveraging the natural anatomy. There is a cost benefit in that OR time is shorter with less time for venous harvest and avoiding grafts, patches, and devices. The patient would avoid ischemia as would happen in the staged repair. The disadvantage is when you are short, but if you mobilize the appropriate amount (height off pelvis at least 1.5x the CFA length) you should be okay. The more curvature and tortuosity seen on 3DVR recontstruction and absence of significant atherosclerosis would predict feasibility.
One of the greatest surgical texts, Cope’s Early Diagnosis of the Acute Abdomen, is something every surgical resident, vascular or general, should read. The mid-century edition which I owned during my residency, has since been updated, but the central message of the book is this: every complaint or pain the patient has comes from a nerve, either peripheral or visceral, and understanding the nature of the pain, you narrow the diagnosis to only a few possibilities. Irritation of the psoas muscle results in a characteristic pain that years of diagnosing appendicitis the old fashioned way -by exam, then operation, makes it easy to recognize, like Marilyn Manson showing up as your substitute teacher (I would have said Alice Cooper, but that completely dates me). When the psoas muscle is irritated, by a hematoma, injury, inflammation, or abscess, the muscle relays intense pain localized to the retroperitoneum. Stretching the muscle worsens the pain, and the patient is often seen with the ipsilateral hip flexed. The genitofemoral nerve which rides on top of the psoas, is triggered and there is pain referred to the groin and proximal anterior thigh. Seeing this, and fitting the story allows for a diagnosis, before imaging. Without this insight, there is no swift vector to treatment and resolution.
Patient with inability to straighten left hip after iliac stent placement
The patient, a middle aged man, had undergone a redo-iliac angioplasty and stent for left iliac in-stent restenosis. He relayed that on the table, he felt immediate left lower quadrant abdominal pain and the desire to flex his left hip. He was restrained, sedated, and the procedure finished -a covered stent had been placed. When he came to my office a month after his initial procedure done elsewhere, he was in wheel chair, unable to straighten his leg. He claimed before coming to see me, he had gone to another hospital, where he had a CT scan and was told nothing was wrong (will have to confirm). He was having subjective fevers at home.
On examination, he sat on the exam table with left hip flexed. His pedal pulses were easily palpable. He had furuncles in his groins which he relayed he had had all of his life. I sent him for CTA and subsequently admitted him for surgery.
left iliopsoas abscess
The CT showed a large collection around the left iliac artery and stents and on the psoas muscle, an abscess. The blood cultures on admission were positive for Staphylococcus lugadensis sensitive to penicillin.
Putting the story together after the fact is much easier than when you are in the moment, but being aware of the location and type of pain should give you a clue. Very likely, he had a brief rupture on the angiosuite table resulting in his sudden pain, drowned out by the sedatives typically given in response to a patient moving when a stent is deployed. Inflating a balloon in an artery typically causes some discomfort -as the vessels are lined with visceral nerve fibers which are quite sensitive but less localizable than say a pin poking on the index finger. If you ever had bloating with gas, that general discomfort localizable to the mid abdomen, that nausea and discomfort is from stretched visceral pain fibers. If you have ever had dull aching pain of distended spider veins, that is visceral pain. It’s there, but you would not be able to pinpoint it exactly. That is not what this patient had when he flexed his hip on the angio suite table. While the covered stent was deploying, he likely briefly ruptured causing both somatic and visceral pain around his left common iliac artery and iliopsoas muscle. Additionally, if the sheath had been entered through an area of a skin abscess, likely the sheath, wires, and gloves were contaminated. Any handling of the balloon expandable stent graft, which I highly discourage, would have contaminated it, resulting in a device infection, which was made more likely due to his diabetes. As the hematoma got infected, it resulted in the worsening symptoms he was having of left lower quadrant abdominal pain, groin pain, thigh pain, and inability to straighten his hip without pain.
I took him to the operating room and drained his abscess, assisted by Dr. Andrew Tang, chief resident headed to CT Surgery fellowship here at the Clinic, and Dr. Jenny Chang, PGY 2 Surgery. I gave Dr. Chang a copy of Cope’s with the admonition to read it soon and pass it on, as most of the current generation claim no knowledge of this important text. While I am not against interventional drainage, it takes time to drain the collection through a tube whereas sticking your hand in, sampling the collection, observing the injury, and breaking up collections and washing out with brown-bubbly -a mix of betadine/peroxide diluted in saline, I believe speeds the recovery from the infection. His drainage was done through a retroperitoneal approach from the left side and notably, his psoas muscle while viable, did not retract to cautery energy, suggesting some degree of rhabdomyolysis. The iliac artery was an indurated, thickened, and hard from the calcium and plaque that was the original problem affecting his distal aorta and iliac arteries (see left arteriogram centerline). I placed a pair of JP drains, removed one that wasn’t draining much on POD #3, and the other about a week after discharge on POD#5. His WBC elevation which was never high promptly resolved. I kept him on oxacillin with consultation from ID, and waited. After 3 weeks, I repeated his CTA.
His right iliac centerline showed patent stent with diffuse plaque and calcium starting in mid infrarenal aorta.
His abscess had significantly resolved and his pain was gone. He was ambulating again.
Before and after abscess drainage
The choices at this point were the following
Continue treatment of patient with supressing antibiotics for life
Resection of left iliac stent graft which is presumed to be infected
If resection chosen, the options for repair that I considered included:
NAIS (ref 1). Neoaortoiliac System graft using femoral vein
Aortoiliac homograft
Rifampin soaked gelatin coated graft (ref 2)
Extra-anatomic bypass with axillofemoral bypass or femorofemoral bypass.
Aortoiliac endarterectomy and repair with bovine pericardial patch and graft
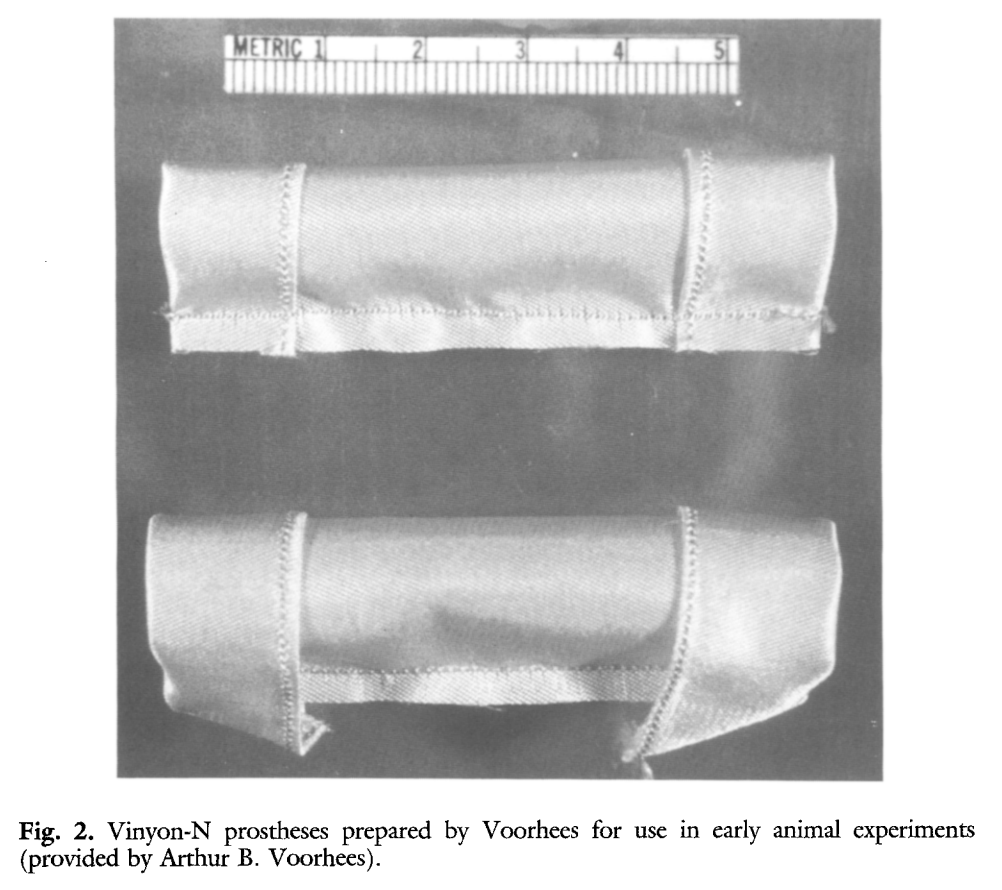
The choice of replacement is becoming clearer in that while rifampin soaked grafts offer immediacy and expedience, all grafts seem to be prone to reinfection at a higher rate than autologous material (ref 3). The NAIS bypass is a great option, but is hampered by the addition of several hours invested in harvest of the femoral veins. While it can be staged with mobilization done one day and harvest another, those added hours add complications. We often forget that the simple metric of procedure time is the most important determinant of complication rate. Any operation going over 2 hours risks wound infection for example simply from ambient colonization of the open wounds from the rain of dead skin from the surgeon’s face, aerosolized fecal flora from flatii (prohibited in my ORs). The microenvironment of the open wound is also room temperature and not 37, having an impact on organ function and hemostasis. The homograft is the original aortic graft -before Arthur Voorhees invented the cloth vascular graft as a resident at Columbia P&S (my medical school alma mater, ref 4), major hospitals had tissue banks of aortic homografts harvested from the recently deceased. Having homografts is now an outsourced function, but does require having proper refrigeration for the cyropreserved grafts and generally can’t be ordered with short notice.
Rifampin soaked grafts work well, especially wrapped in omental flap, in the short and medium term but suffer a reinfection rate that is higher than seen with autologous tissues, and prosthetic grafts without rifampin, such as PTFE for extraanatomic bypass, have the highest rates of reinfection (3), despite being the board answer decades ago.
Endarterectomy allows for use of native tissues for repair. The adventitia around plaque and stents, while thin, can support physiologic pressures, even when they have been occluded for years. And while practice of aortoiliac endarterectomy is a bit of a lost art, it has both a long history stretching back nearly a century and a modern track record with carotid and femoral endarterectomy. It is merely a matter of scale. Pinch and zoom in on a femoral endarterectomy at the bifurcation and you have the same case as with an aortic one.
The question is, is bovine pericardium more autologous than prosthetic? It is a decellularized sheet of collagen from a cow’s pericardium, used in heart valves and vascular patches, but only recently applied as a graft (ref 5-7). I have long used bovine pericardium as a patch with some caution, but the rule of thumb is are there well vascularized tissues around it? A layer of Scarpa’s fascia and fat in a groin wound are not sufficient to protect a bovine patch, but a sartorius flap is. For me, once the infected stent graft is out, knowing if the surrounding tissues bleeds well is an important one.
I chose to do aortoiliac endarterectomy. The patch and graft would be made with bovine pericardium, unless I found the left iliac segment to be devitalized and foul with anaerobic vapors, then, I would close and go NAIS or extra-anatomic. The key point is that choices have to be on the table and constantly rearranged during the conduct of the operation.
The patient was preoperatively vein mapped and had suitable deep femoral vein for bypass conduit, having robust duplicated systems that would impact the patient minimally. The patient was placed in a supine position and via a midline laparotomy, the infrarenal aorta and the common iliac arteries beyond the short iliac stents exposed. I chose this limited exposure as any further into the phlegmon on the left risk injury to ureter and vein. The aorta had a palpable demarcation between plaque and mildly diseased proximal segment, predicted by the CTA to be at the IMA. A longitudinal arteriotomy was created on the right side from mid aorta to mid right iliac, and the left side had a separate arteriotomy to release the stent. The plaque came out in a single specimen (image).
The exposed stent is the left iliac stent holding within a stent graft.
The left iliac artery was destroyed by the infection but the tissues around it bled avidly and were not foul or infected. I avoided excess debridement here as the iliac vein was intimate with the phlegmon. There was a 3cm gap. Again, I thought briefly about taking femoral vein, but proceeded to make a graft from the bovine pericardium. This was sewn around the rod portion of a renal vein retractor from the OMNI set. The finished product resembled Voorhees’ graft. It was sewn into the orifice of the iliac from inside the aorta and end to end to the freshened iliac stump. Unfortunately, the omentum was atropic across the transverse colon, but the tissues around the resected artery and stent graft bled well, indicating good penetration of antibiotic. The retroperitoneum was closed after hemostasis obtained. Dr. Shashank Sharma, our chief resident headed to a vascular surgery fellowship at the renown Houston Methodist next year got to see what is unfortunately a rare occurrence -an aortoiliac endarterectomy, which through me puts him three degrees of separation from Cid Dos Santos (ref 8). Dr. D’Andre Williams, PGY-2 Vascular Surgery Resident, got important lessons on sewing the aorta. She’s part of a fortunate cohort that get exposed to open aortic surgery at our main campus which is unfortunately rare throughout the world.
The pericardium was soaked in rifampin, but probably did not bond to the collagen.
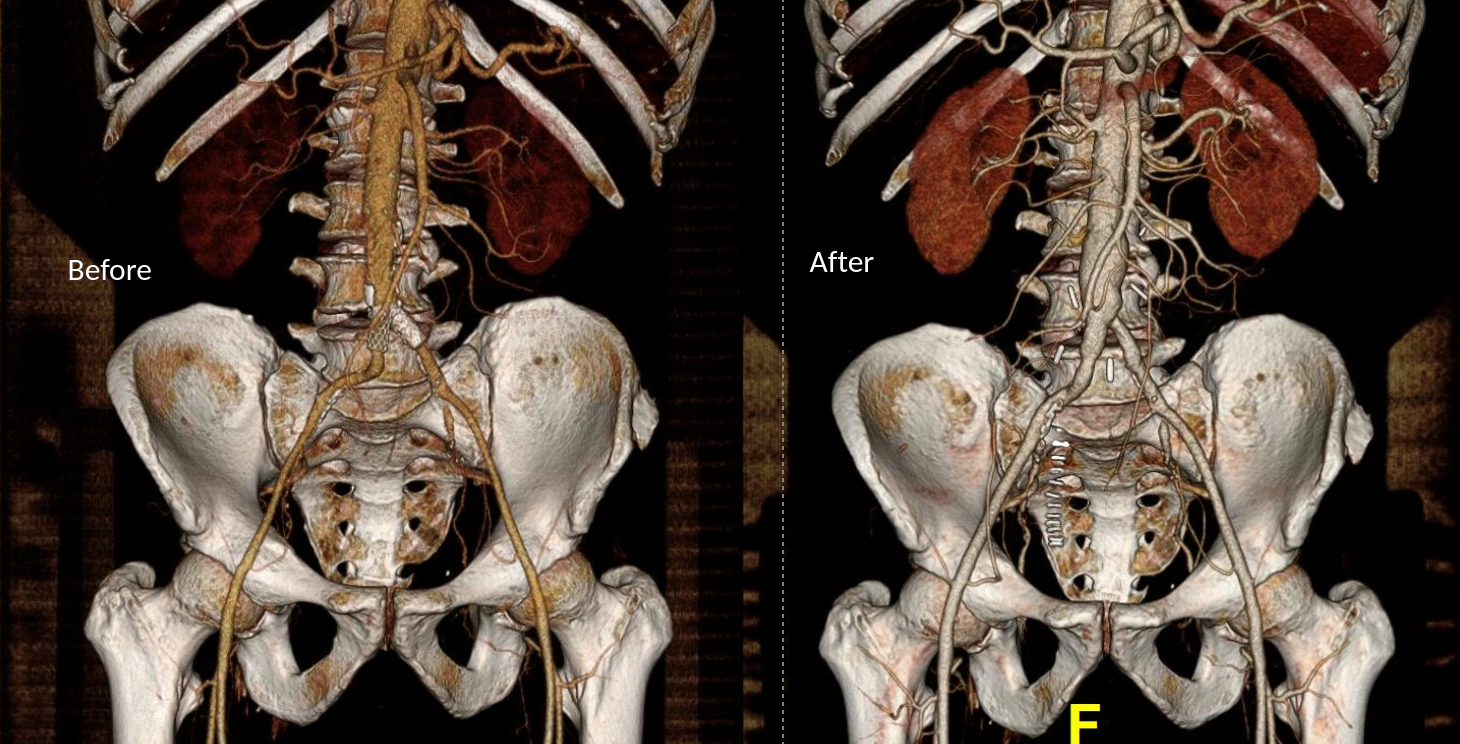
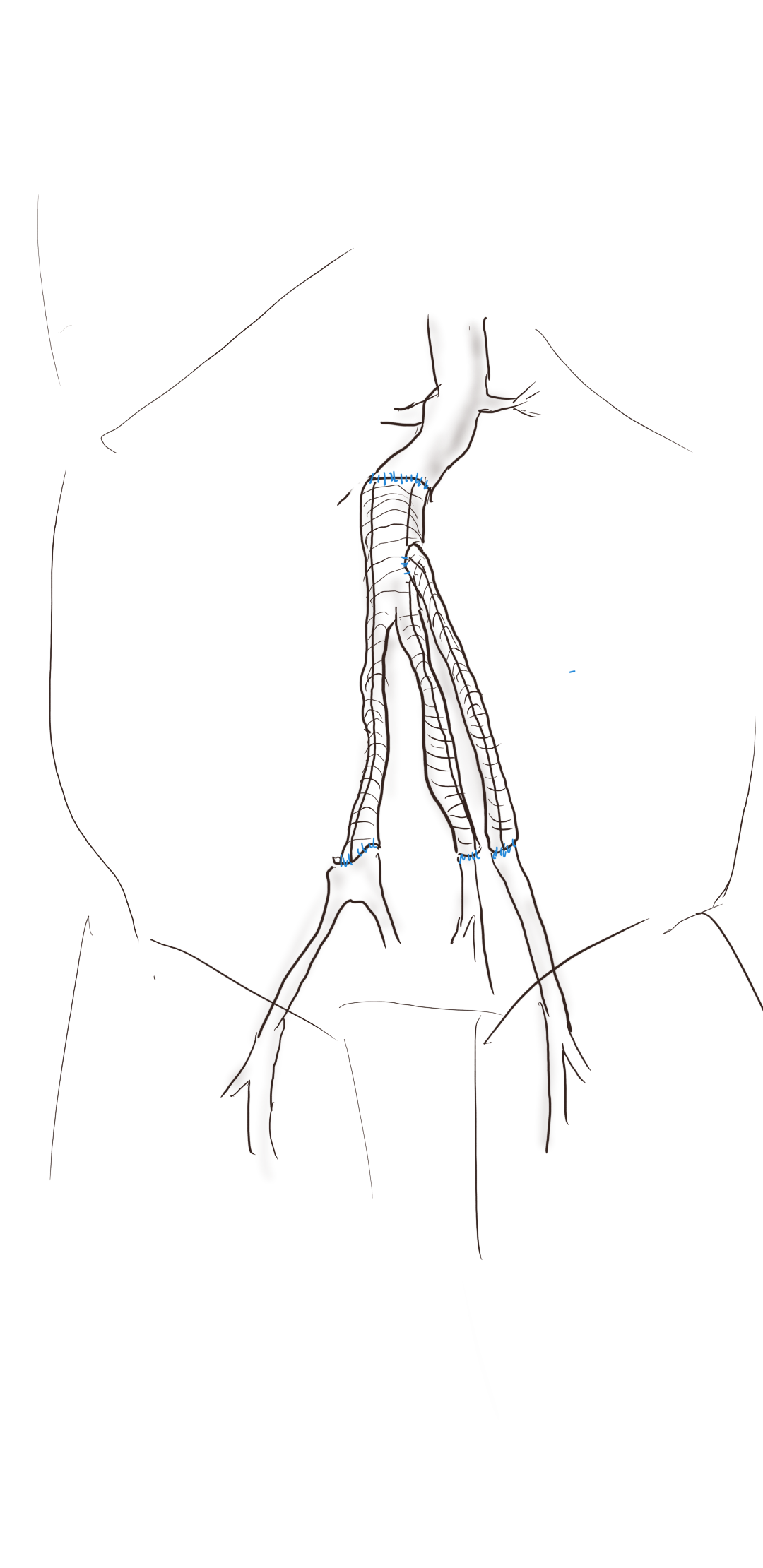
The final graphic shows the operative end result.
The patient recovered well and was discharged within the week with another month of IV antibiotics planned.
Before and After
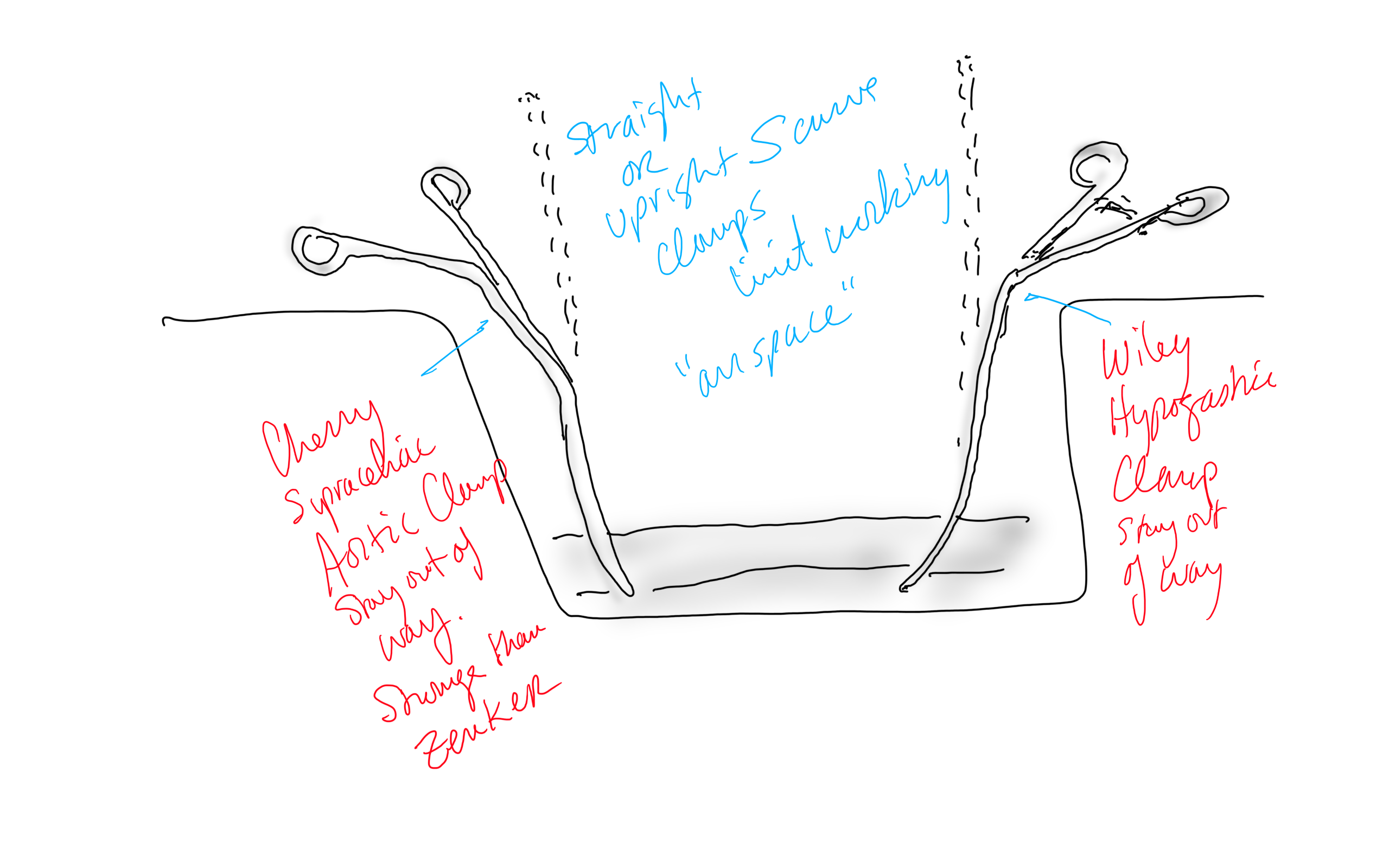
Conclusion: The operation was started at 8 in the morning and was done by lunch time. For aortic cases, this is a crucial metric, as when the clock winds past the surgeon’s comfort, the patient suffers even more. Adding the femoral vein for a NAIS may have been the textbook thing to do, but we don’t do extra-anatomic bypasses that much either. I don’t believe that adding two more hours for retrieving the femoral vein would have enhanced the procedure, and would have served to add potential areas for complication. Technically, the aorta closes much as with a carotid or femoral endarterectomy, but the adventia is thin and really should be sewn with 5-0 or 6-0 Prolene. The larger needles such as the SH size creates unnecessary bleeding unless sewn with a line of felt which could become infected. Despite the thinness, it will hold pressure if it is not infected. Clamps that bend out of the “airspace” above the laparotomy, such as the Cherry Supraceliac Clamp and Wiley Hypogastric Clamp, prevent limiting the operative space with long clamps such as aortic Fogarty or DeBakey clamps, while being stronger than the Zenker.
A final comment for Staphyloccocus lugudensis. This is the second major vascular graft infection with this organism I encountered this year. The other was an infected aortic stent graft. Lugudensis means from Lyons. I do not know why that is, but it is so far not the nasty player that is S. aureus. I am sure it will share some plasmids, and become resistant one day, but in the earlier case in Abu Dhabi and now this, it is sensitive to penicillin, and came from the skin at the femoral puncture site, and for this we are fortunate. Major vascular infections are one of the few areas that still demand open surgical skills, and we foresake them at great peril. It’s critical to remember all the collective memory of surgery from the past, or we will become mere technicians fixing whatever comes out of the radiologist’s report with whatever knowledge obtained from a Zoom meeting for the latest, greatest device.
Acknowledgement
Gratefully, the patient gave his permission, as with all patient, for use of his case for educational purposes.
References
Chung J, Clagett GP. Neoaortoiliac System (NAIS) procedure for the treatment of the infected aortic graft. Semin Vasc Surg. 2011 Dec;24(4):220-6. doi: 10.1053/j.semvascsurg.2011.10.012. PMID: 22230677.
Oderich GS, Bower TC, Hofer J, Kalra M, Duncan AA, Wilson JW, Cha S, Gloviczki P. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011 Jan;53(1):99-106, 107.e1-7; discussion 106-7. doi: 10.1016/j.jvs.2010.08.018. PMID: 21184932.
Smith RB 3rd. Arthur B. Voorhees, Jr.: pioneer vascular surgeon. J Vasc Surg. 1993 Sep;18(3):341-8. PMID: 8377227.
Almási-Sperling V, Heger D, Meyer A, Lang W, Rother U. Treatment of aortic and peripheral prosthetic graft infections with bovine pericardium. J Vasc Surg. 2020 Feb;71(2):592-598. doi: 10.1016/j.jvs.2019.04.485. Epub 2019 Jul 18. PMID: 31327614.
Lutz B, Reeps C, Biro G, Knappich C, Zimmermann A, Eckstein HH. Bovine Pericardium as New Technical Option for In Situ Reconstruction of Aortic Graft Infection. Ann Vasc Surg. 2017 May;41:118-126. doi: 10.1016/j.avsg.2016.07.098. Epub 2016 Nov 27. PMID: 27903471.
Belkorissat RA, Sadoul C, Bouziane Z, Saba C, Salomon C, Malikov S, Settembre N. Tubular Reconstruction with Bovine Pericardium Xenografts to Treat Native Aortic Infections. Ann Vasc Surg. 2020 Apr;64:27-32. doi: 10.1016/j.avsg.2019.10.104. Epub 2020 Jan 10. PMID: 31931127.
Barker WF. A history of endarterectomy. Perspectives in Vascular and Endovascular Therapy. 1991;4(1)1-12. doi:10.1177/153100359100400102
Every once in a while, I will make an exception to the SVS guidelines on AAA repair with regard to size at time of repair (link). I have a bunch of excuses. When I trained in 2000-2002 with several giants of vascular surgery, there was some controversy when the first guidelines came out in 2003 (link). The board answer became 5.5cm that year, but where I trained, it was a minority opinion held by Dr. Jeb Hallett. The majority was in the belief that as long as operative mortality was low, even high risk AAA repair could be undertaken (link). The published risk for Mayo was low, and that came from both technical excellence and high volume (more on that later). The criteria during my fellowship was 4.5cm in good risk patients for open repair based on data generated in the 1980’s and 90’s during Dr. Hollier’s tenure.
Then as now, the debate centered around the balance of risk. At specialty centers that achieved less than 1% mortality rate for elective open AAA repair, 4.5cm in good risk patients would seem perfectly reasonable. But given the 5-10% mortality seen in the Medicare database at that time for community practice, the 5.5 cm criteria was not only good science, it was prudent. The first set of guidelines held off the contentious volume recommendations that was the nidus of conflict within other surgical societies.
The advent of endovascular was a game changer -the mortality rate in the Medicare databases was 1-2% for EVAR in the community setting, meaning more surgeons in most hospitals could achieve tertiary center levels of mortality with this new technology. The issue was never really settled in my mind through the 2000’s, even with the PIVOTAL Study. I enrolled patients into the PIVOTAL Study (link) at that 4.5cm threshold during my time in Iowa. Eventually I lost equipoise and I stopped enrolling after a handful of patients. It had to do with graft durability.
Around that time, I took two patients in a row to the operating room for sac expansion without identifiable endoleak. They were Dacron and stent-based endografts placed about 5-7 years before by another surgeon and aortography failed to show type I or III endoleak. Sac growth was over a centimeter in 6 months and the aneurysm size was over 6cm in both. I chose to marsupialize the sac and oversew any leaks, with the plan to replace the graft if there was a significant leak. On opening the sac, no significant lumbar or IMA leaks were encountered but in these patients a stream of blood could be seen coming from the sutures securing the stents. It was the same graft that was in the trial, the AneuRx, and that was when I realized that these grafts have the potential to fail in the same way that patio umbrellas leak after years of use -cloth sewn to rigid metal with movement wears open the cloth wherever there is stitching. This did not happen with open repair. I lost enthusiasm for the trial as I lost faith in this graft which was retired from the market. I placed pledgetted sutures to close the leaks on both patients, and closed the aneurysm sac tightly around the graft in one patient who was higher risk, and replaced the stent graft in the other.
There are some exceptions to justify repair of 4.5-5.5cm AAA. During my time in practice, there were patients who lived far away from major medical centers who would not survive a ruptured AAA even if the rupture rate was low and who confessed they only came into town every five years or so. There were patients who suffered from clinical anxiety whose AAA was documented by a psychiatrist to amplify their anxiety. There were patients with vague abdominal pain for whom thorough workup have ruled out gastrointestinal causes and every visit to the ER triggered a CT scan to rule out AAA rupture. And there seemed to be some patients who seemed to have such perfect anatomy for EVAR, whose risks were low, and whose growth rates were so consistent that their repairs could be timed on the calendar. Some combination of these factors and lobbying on the part of the patient got them their repair in the 5cm range. And they still do.
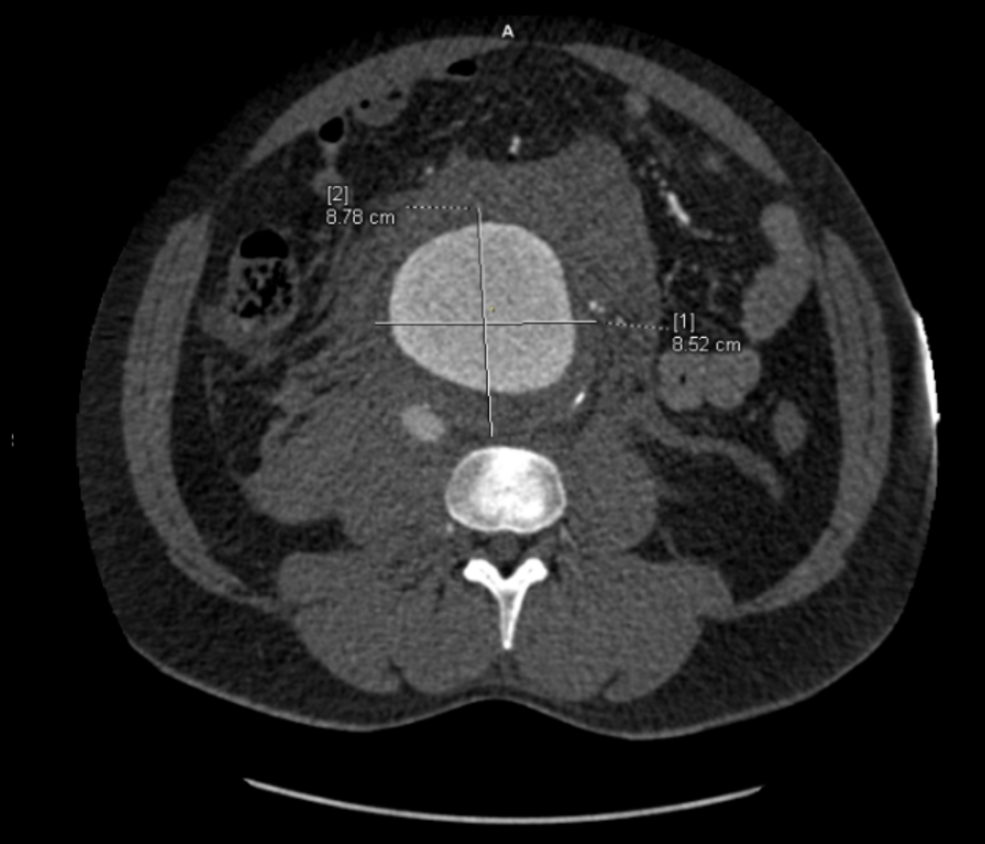
The patient is a man in his sixties with hypertension who presented with a 4.7cm AAA which in various reports he came with described 5.2×4.7cm. After review of his images, it was clear it was 4.7cm. If measured on a typical axial cut CT scan or a horizontally oriented ultrasound probe, a cylindrical aortic aneurysm will be seen as an ellipse in cross section. A radiology report will typically report an aneurysms length and the anteroposterior and lateral dimensions. If you cut a sausage at an angle, the ovals you cut can be quite wide but the smaller length of the oval reflects the diameter of the sausage.
Looking back at his records, for three years he had multiple CT scans for abdominal pain showing the AAA and a well documented record of growth of about 2-3mm annually -the normal growth rate. He asked me to prognosticate and so I relayed that 4.7cm in 2017 with a 3mm growth rate, we would be operating in 2020. The anatomy was favorable with a long infrarenal neck and good iliac arteries for distal seal and access. He was quite anxious as whenever he had abdominal pain, his local doctors would discuss the AAA and its risks or order a CT. After a long discussion and considerable lobbying by the patient and family, I agreed to repair his 4.7cm AAA.
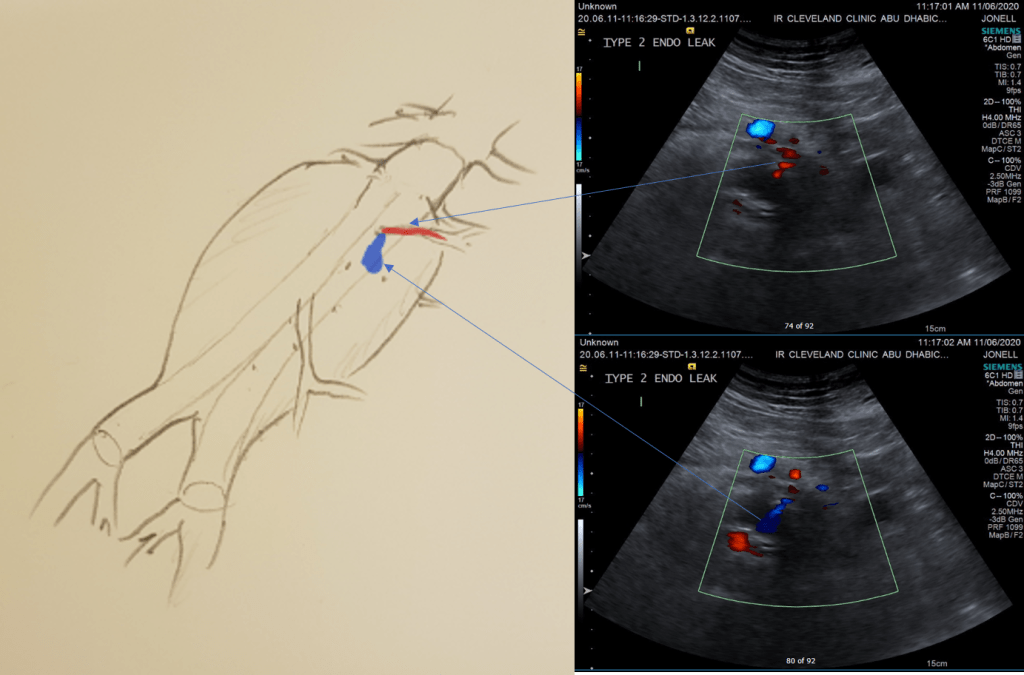
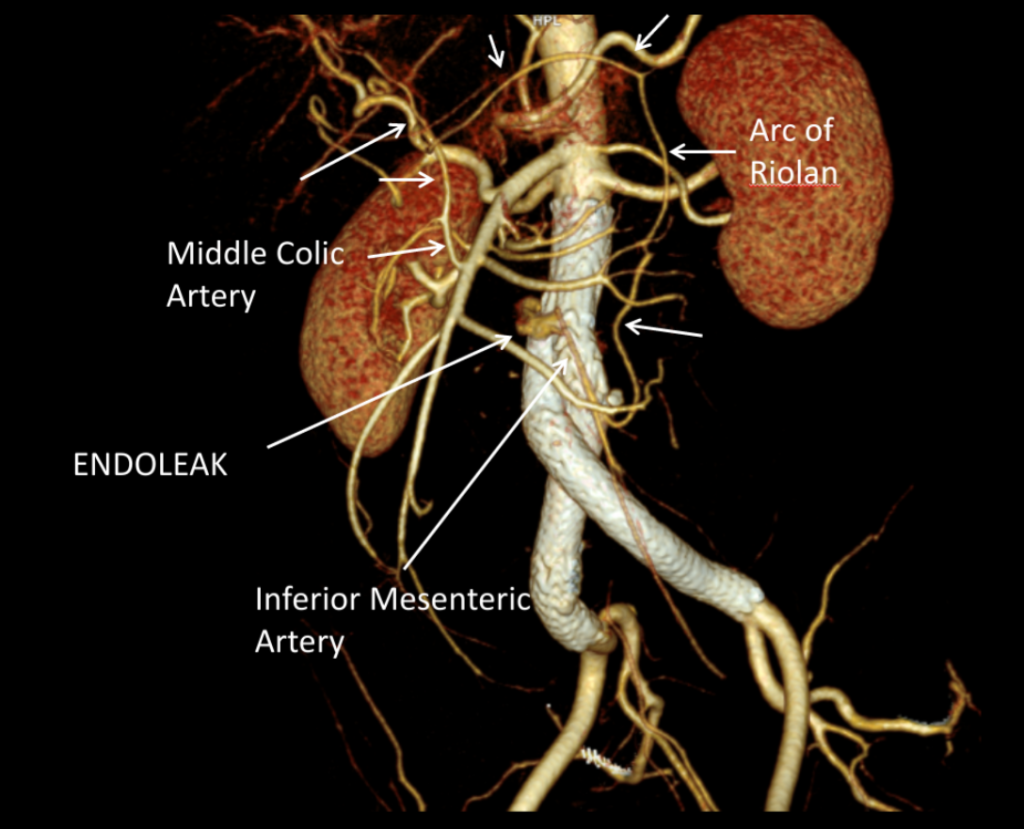
The EVAR was performed percutaneously. No endoleak was detected by completion arteriography (figure). He was soon discharged and was grateful. In followup, CT scan showed excellent coverage of the proximal and distal zones and absence of type III endoleaks. There was increased density to suggest a type II leak, but his inferior mesenteric artery was not the source of it. over a three year period, his aneurysm sac continued its 2-3mm of annual growth despite the presence of the the stent graft.
While CT failed to locate this endoleak, abdominal duplex ultrasound did showing flow from a small surface vessel (duplex below, figure at beginning of post). It was not the inferior mesenteric artery which can be treated endovascularly (link) or laparoscopically (link). CT scan suggested that it was one of those anterior branch vessels that one would encounter in exposing the aorta. Usually these were higher up as accessory phrenic arteries, but these fragile vessels, larger than vasovasorum, but smaller than named aortic branches, are seen feeding the tissues of the retroperitoneum.
Ultrasound revealed the type II endoleak from an anterior retroperitoneal branch artery.
Type II endoleaks are not benign. The flow of blood into the aneurysm sac after stent graft repair is almost never benign. It is a contained hemorrhage. There are three components to the pressure signal seen by the aortic aneurysmal wall that could trigger breakdown, remodeling, and aneurysm growth. They include pressure, heart rate, and the rate of change of pressure. The presence of fresh thrombus may play an inflammatory role. Some endoleaks clearly have a circuit and others are sacs at the terminus of their feeding vessels, never shutting down because the AAA sac can both accept and eject the blood flow. Changes in AAA sac morphology due to sac growth can cause problems with marginal seals, component separation, and component wear. Sac growth can cause pain. Ruptures, while rare, can cause death. Mostly, type II endoleaks generate more procedures because it is hard to ignore continued growth.
Review of aortogram from device implantation showed a small anterior artery arising from the proximal aortic sac (arrow)
Three years of followup showed growth of the AAA sac to 5.5cm, which ironically threshold for repair. Again, no type I or III endoleak could be seen. He reached his calculated repair date, and I discussed our options in detail.
1. Do nothing, keep following
2. Endovascular attempt
3. Open surgery, marsupialization
4. Laparoscopic ligation of target vessel
Doing nothing hasn’t worked for 3 years. What would more time buy? Endovascular -to where. The IMA is the usual target for an endovascular attempt, although iliolumbar access is possible (link), we really needed to fix this with one attempt. Open surgery is a great option -a short supraumbilical incision is all that would be needed to open the AAA sac and oversew the collaterals. The patient did not want a laparotomy. There are reports of laparoscopic guided endovascular access with endovascular coiling of the remnant sac with fluoroscopy. This adheres to the letter of the claim of minimal access, but really?
I compromised with the patient and offered laparoscopy. I have ligated the IMA a handful of times laparoscopically -these are relatively fast and straightforward cases. As I had the location of the endoleak, I felt it should be straighforward to dissect out the anterior sac much as in open repair and clip this vessel.
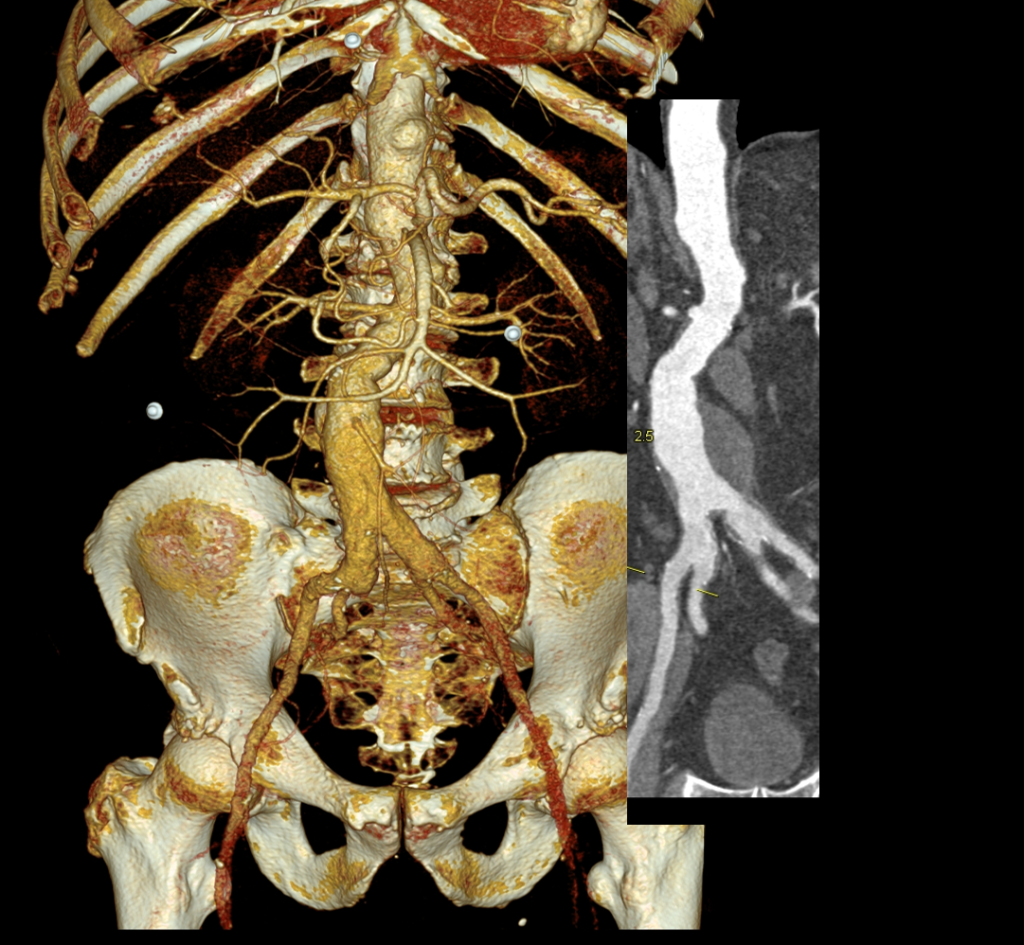
Use of ultrasound allowed localization of the leak and identification of the artery for clipping.
Of course, what should have been a 30 minute procedure through a minilaparotomy became a two hour enterprise getting through scar tissue (not the first time encountering this after EVAR) while pushing away retroperitoneum. I recruited the help of general surgery to get extra hands, but the patient was well aware that there was a good chance of conversion. Patience won out as the artery was ultimately clipped and endoleak no longer seen on ultrasound.
I waited a year before putting this together as I wanted CT followup. The sac stopped growing and has shrunk a bit back to 5cm or so. There will be those who argue that nothing needed to have been done about this leak as it would have stopped growing eventually, but I would counter that an aneurysm sac that kept growing like the stent graft never went in is one demanding attention. The key role of duplex ultrasound cannot be minimized. We have an excellent team of vascular scientists (their title in Europe), and postop duplex confirmed closure of the leak.
Not seeing the leak anymore is a positive, but the stent graft remains.
The patient is quite satisfied having avoided laparotomy. His hospital stay was but a few days. During my conversations with our general surgeons who are amazing laparoscopists, that this would have been a nice case with the robot. That’s a post for another day.
The definition of success in this case and many EVAR’s plagued by type II leaks leaves me wondering. Excellent marketing of the word “minimally invasive” has subtly defined laparotomy as failure, and not just in vascular surgery. When costs and efficacy are reviewed as we come out of this pandemic, I suspect that open surgery will selectively have its day in the sun. A ten blade, a retractor, a 3-0 silk is so much more cost effective than five ports and disposable instruments. And a stent graft system?
About ten years ago, I had a patient who came to see me for moderate carotid disease. While his carotid disease was asymptomatic, he also had metastatic colon cancer. With colectomy, cryoablation of liver mets, and chemotherapy, he was in remission. Every 6 to twelve months he had some kind of CT scan with contrast. His renal function was poor and this was blamed on his chemotherapy. While it had nothing to do with this patient, I thought to myself, “Having an aortic stent graft was a lot like having metastatic cancer in remission.” After a stent graft, the patient is forever tied to the health care system. Without surveillance, there may be an endoleak, sac expansion, rupture, and even death. Patients and vascular surgeons can make choices that lengthen life, improve its quality, and avoid the complications of disease. But what if a treatment becomes a condition and a burden on healthcare resources and the patient’s finances?
Fool me once…
Type Ib Endoleak Causing re-Rupture of a previous r-AAA after no surveillance
Take this patient who had previously ruptured his AAA and undergone EVAR. Several years out from his rupture, he ruptured again from a type Ib endoleak due to aneurysmal degeneration of his right common iliac artery. Per his family, he never followed up. Perhaps he assumed he was cured of his disease? Repairing this was tricky, primarily because I hopped up and down, thinking, “I could cure this!” An open revision with a bifurcated graft would eliminate the need for EVAR surveillance, avoid abdominal compartment syndrome, and the physiologic consequences of a large retroperitoneal hematoma. But who wants a laparotomy? Not this patient, who was hypovolemic shock, and whose family chose the minimally invasive option that everyone assumes is better.
Not a clamp
I took him to the hybrid operating room, balloon occluding to stabilize his blood pressure, embolizing the normal internal iliac artery and extending the stent graft into the external iliac artery.
Completion -there is an Amplatzer plug in the right internal iliac artery
This patient stabilized and had abdominal tightness due to his large hematoma which did not need evacuation. After a stay lengthened by concern for abdominal compartment syndrome, moderate pain, fevers, and bilirubinemia (due to the hematoma), he was discharged and never showed up for followup. None of the phone numbers work. Without followup, EVAR is a menace. We will keep trying.
Regrets, I’ve Had a Few…
The great feature of EVAR is that the complications up-front at the time of surgery are wonderfully low. This patient pictured above here presented in middle age with a rupture into the retroperitoneum. He was unconscious and had hemorrhagic shock.
The decision to perform EVAR was made late in the transfer because I did not have the images from the transferring hospital (another subject for another blog post) so I set up for both open repair and EVAR. En route to the OR, I scanned, slowly, through the CT images sent via CD-ROM, and my internal discussion went something like this.
“He’s a 50-something smoker in shock with a contained rupture of a 8cm infrarenal AAA with a good neck. Let’s take care of this in 30 minutes with a percutaneous endovascular aneurysm repair (p-EVAR).”
“He’s a 50-something smoker in shock with a contained rupture with a good neck -let’s take care of this in 90 minutes with a tube graft, open aortic repair (OAR).”
“With p-EVAR, he’s going to have just two groin punctures and much lower complication rate, shorter length of stay, similar to lower mortality. Look -his blood pressure is 75mmHg systolic!“
“That hypotension is permissive to minimize bleeding. With OAR, he’ll avoid abdominal hypertension and complications of a giant hematoma. Because he’s young, he’ll avoid lifelong surveillance. If anyone can clamp this AAA, it’s me...”
“Pride cometh before the fall. Get this man off the table and figure out the logistics later. p-EVAR. You open him up, he’ll exsanguinate and expire before you get the clamp on.“
I sighed, looked up at the gathered team, and announced, “p-EVAR.” The percutaneous EVAR is something I’ve been doing since 2004, long before it was a big deal, and we were done under an hour. His blood pressure stabilized, but general surgery was consulted for his abdominal compartment syndrome. With sedation, fluids and time, his urine out put recovered but his belly remained distended and his bladder pressures which were never seriously elevated, trended down.
It was made known to me that the patient had very limited insurance making followup surveillance challenging. Due to his coverage, he had to have his imaging done at designated hospitals, so I wrote a detailed note -basically the timings of his followup CT scan, and asked that the reports should be sent to me. I ordered a CTA prior to discharge which showed a type II endoleak adjacent to the graft and connected to both lumbar and inferior mesenteric arteries (first image above). After some thinking, I took the patient for an aortogram, accessed the IMA via the SMA and coiled into his AAA sac and the IMA.
It was only a few weeks ago one of my colleagues across town contacted me that the patient had been admitted with abdominal pain, a CT showing a type II endoleak from his lumbars, but a smaller AAA sac than his pre-repair size of 8.5cm. The patient is seeking to repatriate, and I doubt he would be able to get adequate followup in his home country without paying in cash. Happy that the patient survived his rupture, I still have persistent regrets at not getting him through an open repair, which I am sure he would have done fine with… Or maybe not.
Je Ne Regret Rien…
Recently I admitted a patient, in his 70’s, with a symptomatic 6.5cm infrarenal AAA with bilateral common iliac artery aneurysms, the right being 25mm, the left over 30mm. Because of the pandemic, he was stuck here, seeking to repatriate. Over ten years before, he had a segment of descending thoracic aorta repaired for a traumatic tear -probably one of the last before the wide adoption of thoracic stent grafts which work great by the way.
Cardiac risk evaluation revealed an ejection fraction of 35% with reversible ischemia on nuclear stress test. CTA of the coronaries revealed triple vessel coronary artery disease corroborated by catheterization. Off-pump CABG was planned which would eliminate the effects of cardiopulmonary bypass.
Preparations were made for EVAR with IBE of the left iliac aneurysm as a contingency, but there was no question that if the patient recovered well from his CABG, he would undergo open repair. This was because bell-bottoming or IBE must have regular coordinated surveillance which was not going to be easy with the patient leaving for another country in the middle of a pandemic. It is difficult to get followup to happen in normal circumstances (see above cases). I expressed my opinion to the patient and family and we agreed to see how the patient responded to off-pump CABG.
He underwent off-pump CABG with three vessels revascularized. He was extubated POD#1 and mobilized. By POD #4, he was on a regular patient floor, being co-managed by hospital medicine who takes care of all of our patients. The patient expressed readiness for the next operation. His kidney function remained normal. He was transfused 2 units of PRBC to bring his hematocrit to 30%. He was taken off Plavix, but kept on aspirin. On POD#6, he was taken back to the operating room for open aortic bypass. This would not have been possible without close coordination of cardiology, cardiac surgery, and vascular surgery. Choosing off-pump CABG was a critical element in being able to proceed with open aortic surgery.
Right branch taken to iliac bifurcation, separate bypasses sent to left internal and external iliac bypasses.
I do several things to decrease the physiologic impact of the operation. First is keeping all the viscera retracted under the skin. This simple move has the effect of decreasing the rate of intestinal paralysis and amount of fluid shifts that occur postop, akin to going retroperitoneal. This decreases the space you potentially have if you use standard clamps, but I use the Cherry Supraceliac clamp (image), DeBakey Sidewinder (transverse), or just a Satinsky clamp oriented transversely. This minimizes the occupation of volume over the anastomosis which always happens with standard aortic cross clamps. The anastomosis is easier without the clamp taking up valuable space.
Cherry Supraceliac Aortic Clamp
The iliacs are always clamped with Wylie Hypogastric clamps, again, with the principle of eliminating clamp overhang. Suturing is done with 4-0 Prolene on SH needles -this is plenty (link). The proximal anastomosis wants to bleed, and sewing to a fully cut ring of aorta ensures good posterior bites but also allows for sliding a band of graft down over the anastomosis (Dan Clair calls this a gusset) which works well at creating a hemostatic proximal anastomosis rapidly-trust me, getting this done well is the key step of the operation. Before closing, I infiltrate the rectus sheath and preperitoneum bilaterally with local anesthesia -lidocaine 1% with epinephrine 1:1 with bupivicaine 0.5%. The skin is closed with absorbable dermal sutures because staples create as many problems as they solve. The patient had cell salvage through the case and no extra units of transfused blood.
The patient was extubated that night and started on clear liquid diet. The next day his lines were removed and he was moved to the floor and started on regular diet when he expressed hunger. On POD#2, he was pacing floor, asking when he could be discharged.
Sternotomy and Laparotomy POD#2, walking the floor
As he was eating, walking, talking, breathing, evacuating bowel and urine, and pain free (well controlled), I saw no reason to keep him beyond POD #3 AAA/#9 CABG. I have kept in touch with him and his family and he is doing well and has given permission for this posting.
Satisfaction
This final case has confirmed several of my beliefs. First, calling something high risk can drive one to make bad choices and in fact endanger patients. This last patient would qualify as high risk on any international criteria, and you would not be wrong in quoting upwards of 30% major morbidity and mortality for cardiac revascularization and AAA repair, but you would also be tying your hands from offering the best solution for this man who fortunately was able to undergo two prodigious operations. He will not require much in the way of followup. Coronary revascularization with arterial conduit and open aortic grafting frees him from the need for close followup and reassures us that his repair is durable.
Second, calling something advanced and minimally invasive gives one cachet in the marketplace but forgoes careful discussion and consideration of what is being abandoned. The first two patients survived their ruptures but now face the consequences of having stent grafts. It is a shame when podium speakers at international symposia declare surgery to represent failure because this affects training by encouraging abandonment of hard to acquire skills. It seeps into patient perceptions and expectations. I hope that a balanced approach prevails. You have to be capable of both open and endovascular approaches to be able to offer the best treatment for a particular patient.
Finally, these old operations are cost efficient and there is a lot of room to improve these procedures with new perspectives, techniques, and data. I don’t operate the same way I trained, and it is only through continued application of operations that improvements can come about. As budgets tighten and economies are stressed, cost efficacy will rein in much of the interest and demand in new stuff unless it adds value. That said, I am grateful to our stent graft representatives who have worked to get us bell bottoms and IBE’s for when they will be needed. These grafts will be used when the time is right.
It is a rare day that passes without the announcement of a stroke alert at CCAD. A reflex arc of activity is initiated, as time becomes the critical metric of success. Patients with strokes have a limited window of time to reverse the effects of the arterial occlusion, and the whole hospital is organized around getting the patient into the angiographic suite to open up blood vessels. If you watch it happen, it is the pinnacle of modern medicine, to achieve what only a decade ago was deemed unachievable. It was built around a foundation laid by cardiologists for heart attacks -the STEMI alert. The teams practice like racing pit crews with a stopwatch to get a patient from the emergency room, to CT scan, to angio suite. A long time ago, as a young surgeon, I had to work hard to get institutional support of ruptured AAA and cold legs. Vascular surgery has traditionally struggled to get recognition for its patients, their diseases, and its work, which is nothing less than the most important safety net for any large general multi-specialty hospital, critical infrastructure like oxygen plumbing and backup generators. As I transition to that weird designation of mid-career surgeon (please don’t call me a senior surgeon), I have also appreciated that Steve Jobs aphorism about good artists copying, great artists stealing. It’s only stealing if you don’t give credit. Here is what I borrowed from the neurologists.
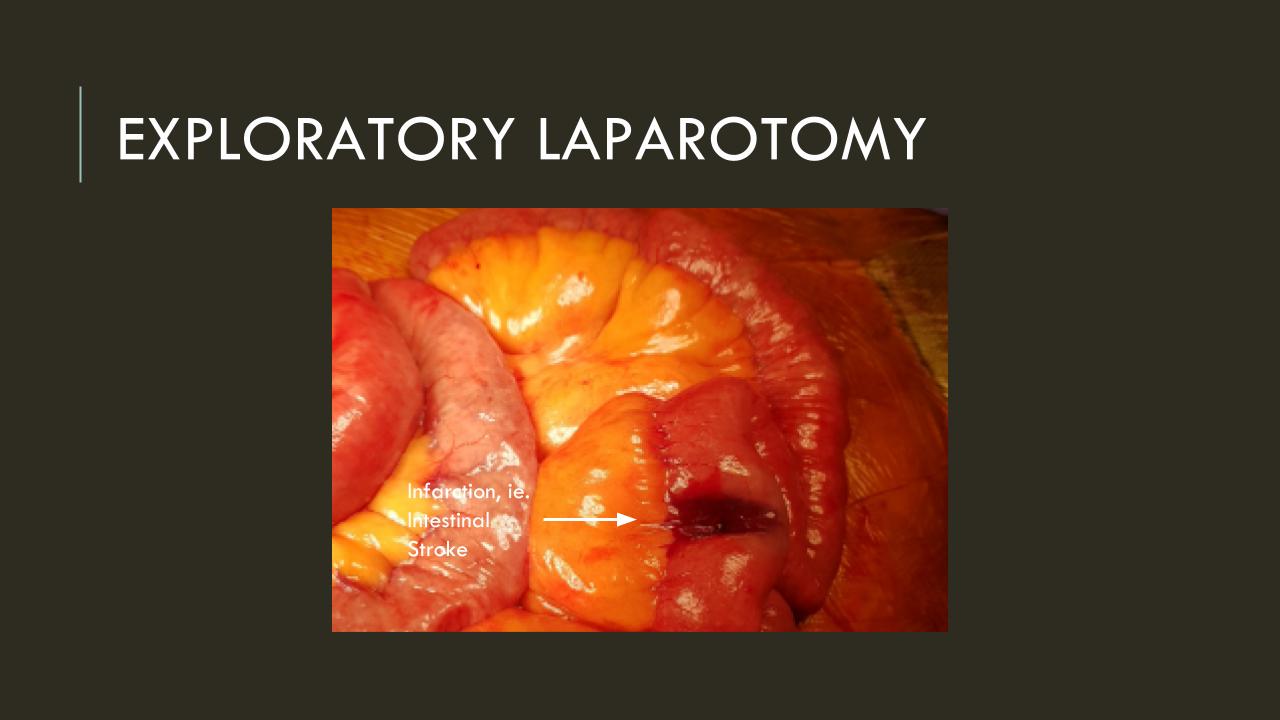
Acute mesenteric ischemia is an abdominal stroke. Use it in your conversations with other people as you speed your patients way into the angio suite. The reflex arc is in there. For the emergency department, the operating room, and all the physicians, acute mesenteric ischemia sounds like tummy trouble, but abdominal stroke brings sudden clarity to conversations like:
“Well, you’re in line behind a gallbladder and a cystoscopy. Is the patient NPO?”
Me: “It’s an abdominal stroke. We literally only have a few hours before the patient dies…”
“I’ll bring the backup team in!”
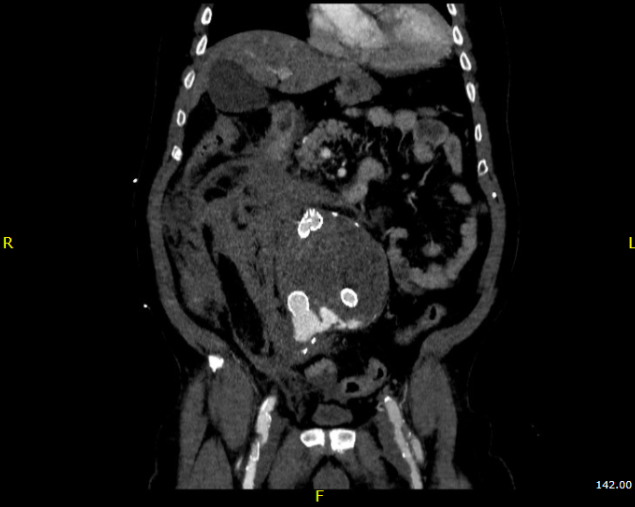
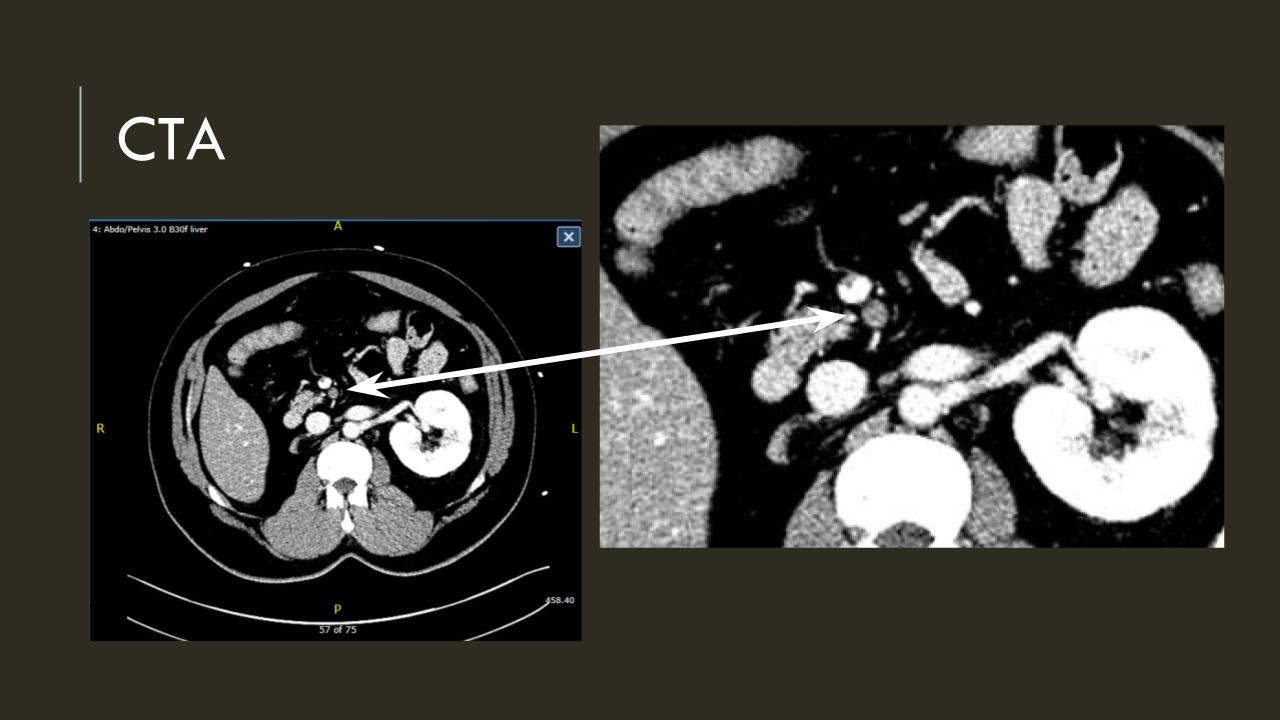
The patient is a middle aged man with risk factors of NIDDM and prior history of DVT who developed severe mid-abdominal pain at 5pm. He came to the ED at around 11pm and had a general surgery consultation who ordered a CT Angiogram showing SMA occlusion (pictured below).
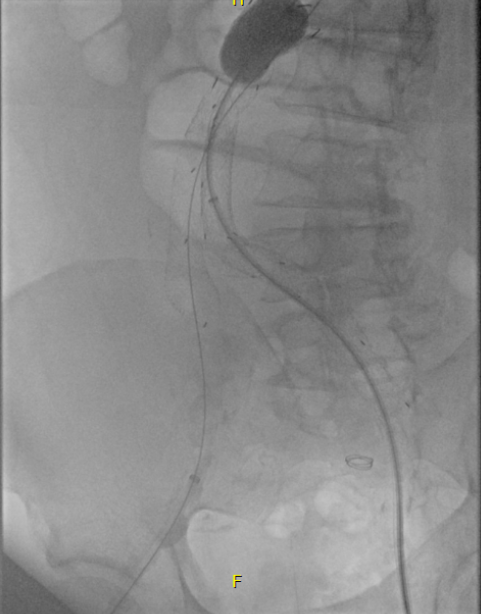
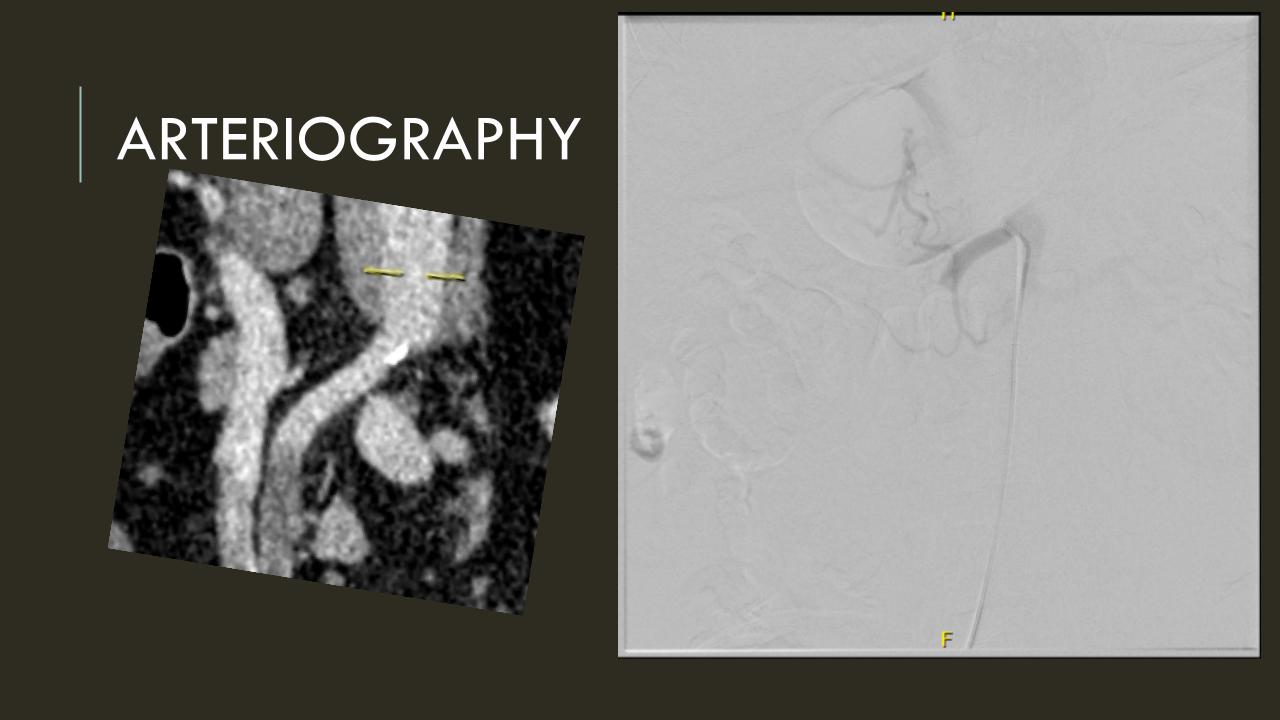
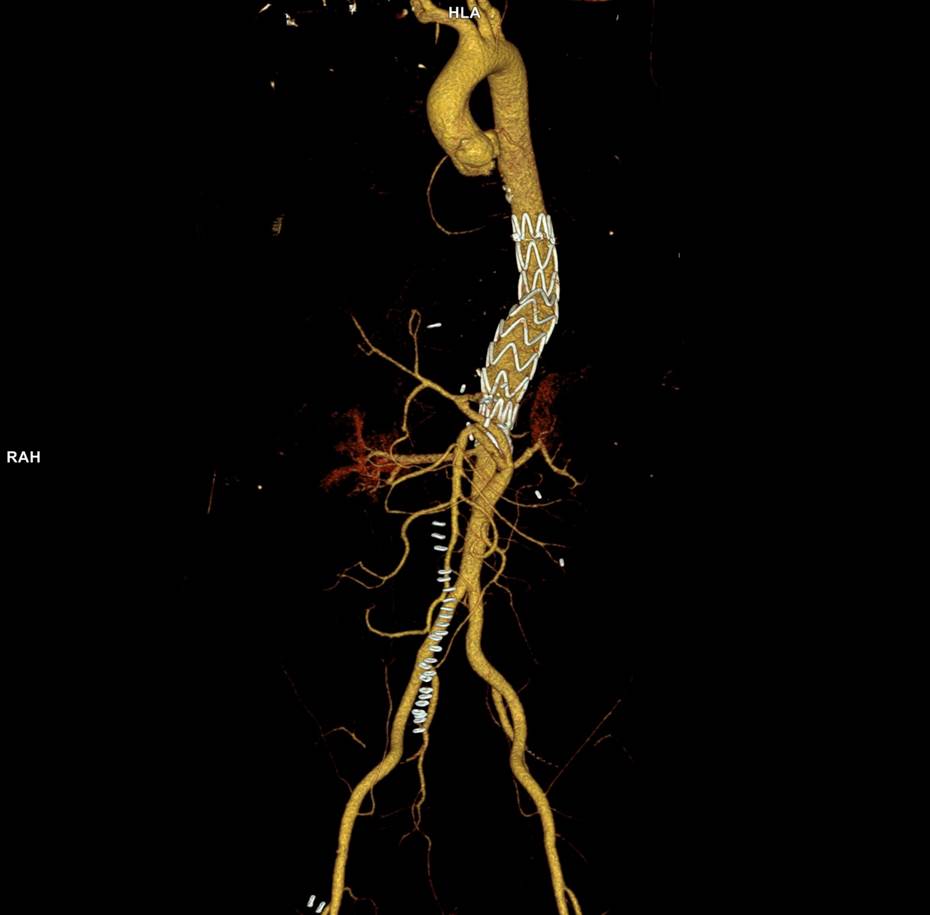
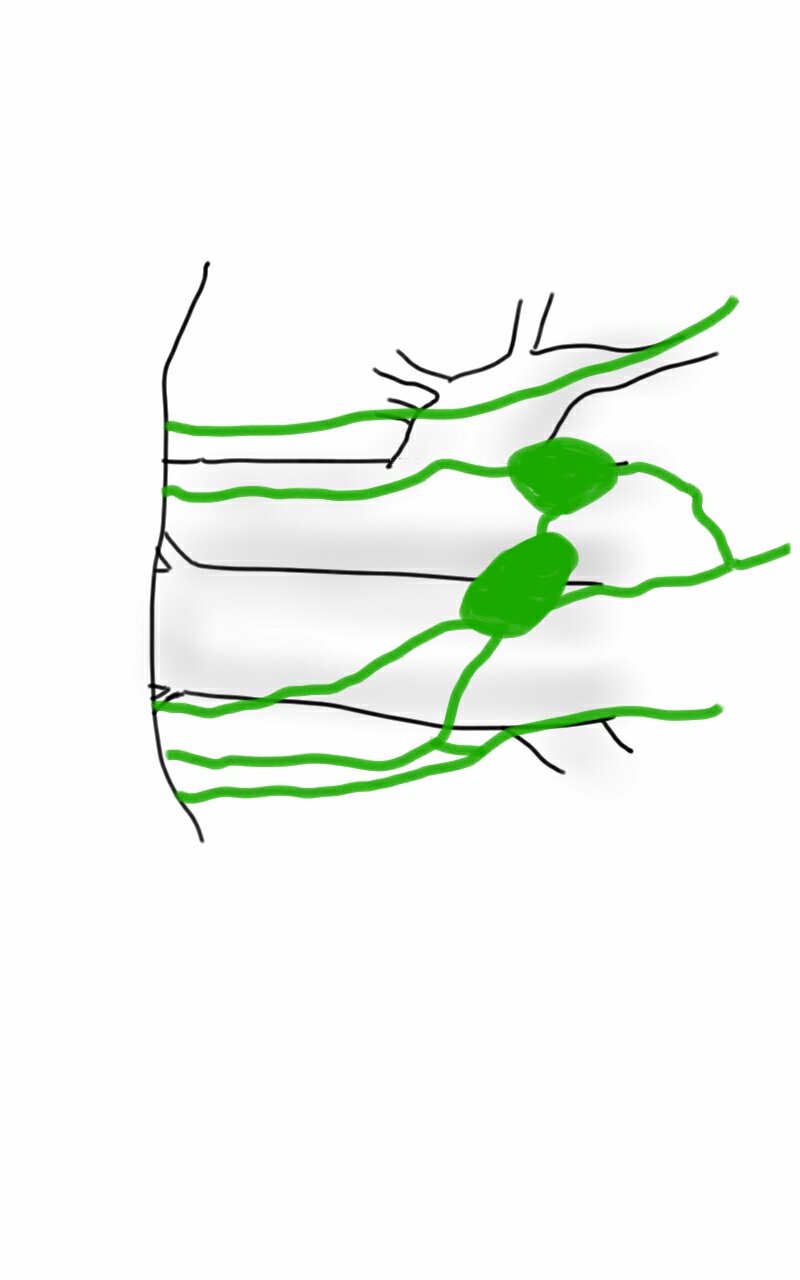
Heparin was started, and at 11:30, vascular surgery was consulted. The patient had a soft, doughy texture to his abdomen, but great pain with palpation -classic pain out of proportion to the exam. Determining the patient to have acute mesenteric ischemia from a thromboembolism, I took the patient to our hybrid angiographic OR suite with the plan for arteriography, possible open thrombectomy, and exploratory laparotomy. Arteriography from femoral access showed an occlusion of the SMA beyond the middle colic artery, a typical pattern for an embolism that occurs when embolism lodges distally and propogates proximally (image below).
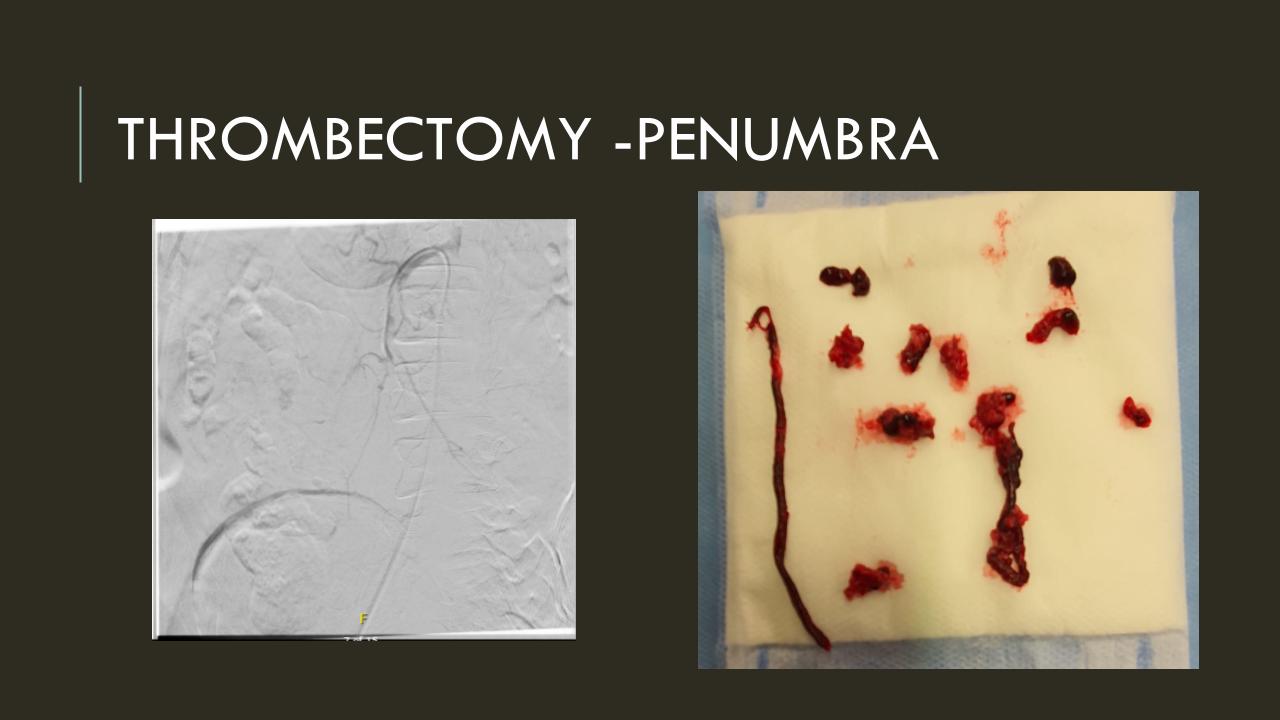
I got Glidewire access into the ileocolic terminus of the SMA, exchanged for a Rosen wire, over which I placed an 8F sheath into the proximal SMA. This was a rather large sheath meant to catch thrombus as I suctioned it out with a 6F Penumbra catheter. This is another technique I borrowed from the neurointerventionalists. Whenever a stroke alert is going on, curiosity drives me to peak in and see what marvelous gadget or gewgaw they are using, and I was impressed by how efficiently the neurointerventionalists were able to get to the smallest thrombus in the furthest branch vessels. I was prepped for open thrombectomy, consented for bypass if necessary, but having experience in suctioning clot through single catheters and sheaths, I thought the simple design of the Penumbra and its efficacy in the cerebral system could easily translate into the mesenteric.The problem with open thrombectomy is the inability to see if you have cleared thrombus from all the branches unless you do an arteriogram after you’ve completed your procedure. This may be a significant contributor to the 20-30% bowel resection rate that occurs on second look laparotomy in my old paper and in the literature since its publication.
The Penumbra was effective in removing much of the fresh thrombus, but I was also cognizant of the fact that pulling out the catheter will draw clot into the 8F sheath that did not make it into the catheter. I placed a wire, and removed the sheath to expel much of the bulky thrombus (picture below).
The completion angiogram (below) doesn’t show the intermediate angiograms showing thrombus that embolized to other arteries as I manipulated the catheters and thrombectomized -I was able to successfully retrieve these with selective catheterization, another neurointerventional series of maneuvers that I have successfully borrowed.
After being satisfied with the completion, I removed the sheaths and explored the abdomen finding this segment of infarcted small bowel (next image).
There was no question in my mind that there would be some dead bowel based on the time course described by the patient. Despite my excitement about calling for GIA staplers -I am general surgery boarded- I called in the general surgeons for their help in resecting and anastomosing this segment of bowel. They would be the ones taking the patient back for any second look laparotomy, although in this patient, I determined that there would likely be no need. After the anastomosis was completed, I did a Wood’s Lamp examination (pictured), which is accomplished with a black light after giving the patient an ampule or two of Fluorescein.
The bowel had a splotchy fluorescence pattern which is typical of ischemia-reperfusion. This is where you have to ask the anesthesiologist and any critical care specialist who follows -no pressors please! Edema won’t kill an anastomosis as badly as ischemia will, and the gut is as sensitive to norepinephrine as are the toes. Workup in the hospital including echocardiography and CTA of the entire aorta failed to reveal a proximal source or cardiac shunts or thrombus. The patient recovered and has recently followed up, eating well, and tolerating his anticoagulation which he will be on for life. I sent out the pictures to my neurointerventional friends with some glee, but also with the purpose of informing them that in the case that the vascular surgeons become incapacitated or quarantined due to the COVID-19 pandemic, their skills would be recruited in the care of an abdominal stroke -a blood vessel is a blood vessel. Acute mesenteric ischemia should be the first thing on everyone’s differential of sudden onset abdominal pain because of its time dependence, yet it does not have the same resonance to the unfamiliar as abdominal stroke. Survival is dismal when too much time and intestinal death has occurred. When associated with the stroke alert concept, it translates into processes already in place throughout the hospital and it becomes natural for everyone to appreciate the urgency of treating abdominal stroke. This is the system adopted by Roussel et al. in France, where they have regionalized care of intestinal stroke. They report mortality rate of 6.9%, which is in a selected population, but significantly lower than the traditionally reported 30-60% mortality.
I am still an advocate of an open approach, especially when angiographic resources are unavailable, and every trainee needs to be able to describe the exposure of the SMA, and management of acute mesenteric ischemia. Hopefully, everyone will appreciate the urgency of all the various ischemic conditions manifest in the peripheral circulation, but rebranding them as a stroke (leg stroke, hand stroke, intestinal stroke…) is helpful. Finally, there is no survival with dead bowel -it must be found through exploration and resected.
Reference:
Roussel A, Castel Y, et al. Revascularization of acute mesenteric ischemia after creation of a dedicated multidisciplinary center. J Vasc Surg. 2015 Nov;62(5):1251-6. doi: 10.1016/j.jvs.2015.06.204.
Adding a vascular surgeon to a hospital is like eating one of these. It turns Mario into Mega Mario. Vascular surgeons turn community hospitals into tertiary care centers.
Recalling the medical school adage, “when you hear hoofbeats, it’s probably horses, not zebras,” it is critical to think about rarities down on the differential list whenever you come across a patient. Vascular diseases suffer from inadvertent obscurantism arising from its absence from medical school curricula such that common disorders like mesenteric ischemia and critical limb threatening ischemia are frequently missed by even experienced medical practitioners. Vascular zebras are even harder to pin down because many experienced vascular specialists practice for years before they encounter, for example, adventitial cystic disease or dysphagia lusoria with a Kommerell’s diverticulum. Even so, real patients have these disorders, and we are all subject to inexperience bias -the feeling that something does not exist until you see it. You may completely miss something staring at you in the face or worse, deny its existence.
The patient is a middle aged man in his 50’s who aside from mild hypertension had no real risk factors. One day, at work, his right leg stopped working. He developed a severe calf cramp and the forefoot was numb and cool. He went to his local hospital and the doctors there appreciated the lack of pulses in the right leg and got a CTA, of which I only had the report which found a right popliteal artery occlusion.
The next morning, as he had signals and was not having rest pain, his doctors discharged the patient on clopidogrel and scheduled for angiography and stenting, per patient. As his debilitating claudication did not go away over the weekend, he came to our emergency room. While he had no rest pain, he did have minimal walking distance before his calf muscles seized up. On exam, his right foot was cool and cyanotic, with intact motor function and sensation. There was a weak monophasic posterior tibial artery signal. Bedside point of care photoplethysmography showed dampened waveforms (below).
Look at the blue line. The waveforms are dampened in the ischemic foot.
Because he did not bring his CT, I repeated the study. I have written extensively on the need to be able to share CTA studies without barriers. After his study, I brought it up on 3D reconstruction software.
It clearly showed a Type II Popliteal Artery Entrapment affecting both legs (CTA images in series above). Stenting it would have failed. I spoke with the patient about operating the next day. The plan was popliteal artery exploration and thromboendartectomy with myotomy of the congenitally errant medial head of the gastrocnemius muscle. The patient was agreeable and I took him to the operating room for a myotomy and popliteal thrombendarterectomy in the prone position. The medial head of the gastrocnemius muscle went over the popliteal artery and inserted laterally onto the femur.
Endofibrosis, cut medial head of gastrocnemius muscle to right of distal clsmp
The artery was opened and while there was fresh clot, the artery showed signs of chronic injury as evidence by endofibrosis which pealed off. Pathology showed to be fibrotic in nature.
Trichrome stain showing chronic endofibrosis
The artery was repaired with a pericardial patch and flow restored to the tibials, not all of which were completely patent.
The patient was discharged after about a week and will be scheduling repair of his contralateral popliteal artery entrapment.
The vascular surgeon has a vital role in a hospital’s medical ecosystem. One time, I heard hospital administrator say that with the advance of endovascular technologies, the vascular surgeon would become an expensive, redundant luxury easily replaced by the overlapping skillset of radiologists, cardiologists, general surgeons, trauma surgeons, cardiac surgeons, nephrologists, neurosurgeons, neurologists, podiatrists, infectious disease, and wound care specialists. When I identify these zebras, these rare diagnoses, I am neither replacing all those aforementioned specialties, nor having special insight unavailable to the uninitiated. I am keeping my eyes open. In a non-smoking, active, otherwise healthy and employed middle aged man with no cardiac history, it is very strange to have isolated popliteal occlusion with otherwise pristine arteries throughout the rest of the CT scan. That is a statistical outlier. People who occlude blood vessels in this fashion usually have more comorbidities, usually are older, and usually have more atherosclerotic disease burden. While not quite like the teenager who presented last year with the same diagnosis (after a month of misdiagnosis and delayed treatment), the cleanliness of the arteries elsewhere in the body was disturbing to me. This puts me on a zebra hunt and not the usual horse roundup.
A hospital needs vascular surgeons in the way that America need the US Marine Corps. Every decade, there is some congressional movement to see how the USMC, which has fighter jets, tanks, planes, aircraft carriers, helicopters, and riflemen, can be phased out because it seems to duplicate the services of the Navy, Air Force, and Army, and every generation a conflict proves these arguments wrong. Individuals who know things broadly and deeply, who can do many things across specialty lines, work from head to toe, and whose specialty is to customize solutions to complex problems is the special quality that is the difference between tertiary hospitals and quaternary hospitals. While these qualities are goals within Vascular Surgery, it is a generalizable goal for anyone working in healthcare. My favorite professor in medical school was Dr. Harold Neu, chair of infectious diseases at P&S. He knew everything and was interested in everything and took every moment in the hospital to increase his knowledge a little more. That’s how and why I diagnosed a case of schistosomiasis earlier this year -the upper abdominal pain was not from a coincidental aortic aneurysm, but the fellow did swim in the Nile.
I texted Dr. Sean Lyden, my former boss and partner at the Cleveland Clinic main campus, if there was any situation where an asymptomatic popliteal entrapment who had gone over 50 years of life without complications could just be watched -it was a question from the patient actually. Dr. Lyden treats popliteal entrapment weekly and maintains a clinic specializing in popliteal artery entrapment (link). One of advantages of working in vascular is that the community is small and highly accessible, and I have a group of living textbooks on speed dial (that term pegs me as antique). There is an active social network of vascular specialists and the SVS maintains SVS Connect (link) for posting and discussing difficult questions. Despite the horrible hour that he received the text (“What’s the matter? Are you in trouble?” he asked) because of the time differences between Abu Dhabi and Cleveland, he answered, “no.” Sorry, Sean, for texting you at 4 in the morning.
When you look for four leaf clovers, and you have never seen one in your life, the moment you find one must be transformative. I have never found one, but I keep my eyes open, lest I trod on one.
It was only last month when I came across a post of an aortic aneurysm in a difficult spot (link) and I couldn’t help chiming in some comments. Reading it now, I sound insufferable, because I wrote,
“Depends on etiology and patient risk stratification. Also assuming aneurysm goes to level of SMA and right renal artery origins and involves side opposite celiac. Options depending on resources of your institute: 1.Open repair with cannulation for left heart bypass and/or circulatory arrest 2.Open debranching of common hepatic, SMA, R. Renal from infrarenal inflow and then TEVAR 3.FEVAR from custom graft from manufacturer on protocol 4.Parallel grafting to CA, SMA, R. RA with TEVAR 5.Surgeon modified FEVAR 6.Open Repair We would have a multidisciplinary huddle around this patient -Vascular, Cardiac Surgery, Cardiology, Anesthesia, and ID (if needed) to help choose. Be ready to refer to a center with more resources -including prepping patient for transfer and imaging -including uploading images to the cloud for transfer with patient’s permission. More info please”
More Info Please, Indeed
The post I commented on was of a saccular aneurysm in the transdiagphragmatic segment of aorta. Ironically, only a few weeks later, I got called from hospital transfer center about a patient with a leaking aortic aneurysm, a type V thoracoabdominal aortic aneurysm as it turned out, from an outside hospital, needing urgent attention, and we accepted in transfer based on the conversation I had with the tranferring physician. And that was the problem -usually in taking these inter-hospital transfers, you have to pray that the precious CT scans come along with the patient burned correctly onto a CD-ROM. You can buy and watch a movie in 4K resolution over the internet -about 4 gigabytes, but a patient’s CT scan which is about 200 megabytes -because of various self imposed limits, overly restrictive interpretations of laws, and lack of computer skills, these life saving images get transferred on CD in 2019. That last time I purchased a CD for anything was over 15 years ago.
An Interested Party
The technical solution –to use the internet to transfer critical life saving information between hospitals – came about when our IT folks took an interest in my quarterly complaint email about using the newfangled internet for sharing files. After mulling various solutions ranging from setting up a server to using commercial cloud solutoins, we came upon the compromise of using our internal cloud with an invitation sent to the outside hospital. I would send this invitation to upload the DICOM folder of the CD-ROM to an outisde email address. It was simple and as yet untried until this night. “Would the patient agree to have his CT scan information transmitted to us electronically?” I asked the other physician. He assured me that the patient was in agreement.
It Takes Two to Tango
Of course, being able to transfer these pictures requires a willing partner on the other side, and the referring physician made it clear he did not have the technical expertise to do so. It took a bit of social engineering to think about who would have that ability. Basically, aside from myself, who spend all their time in dark rooms in the hospital in front of giant computer monitors? The radiologists! I got through to the radiologist who had interpreted the report and explained the simple thing I needed. Gratefully, he agreed, and I sent him a link to our cloud server. I explained to him, “When you receive this, clicking the link opens a browser window and then you open the CD-ROM and find the DICOM folder and drag and drop it on the browser window.” The 200-500 megabytes of data then get sent in electronic form, as it was meant to in 2019.
The Internet Saves a Life
The brutal truth is that in locking down a computer system, many hospitals make it impossible to even load an outside CD-ROM, creating many self imposed barriers to care. Thankfully, at CCAD, we were able to work together to find a secure solution. With the CTA on our servers, I was able to review the study within 15 minutes of accepting the patient, and arrange for the right team to be assembled, and confirm that we had the right material (stent grafts) for treating the patient. When the patient arrived, OR was ready to go, saving hours of time that normally would have been required if the CT scan had to be reviewed from the CD-ROM that came with the patient. Sometimes, the CD-ROM does not come, and in a critical situation, the CTA has to be repeated with some risk to the patient for complications of the contrast and radiation.
What to Do
The patient had a 8cm sphere shaped aneurysm arising in the transdiagphragmatic aorta, leaking into the right pleural cavity.
The patient was otherwise a healthy middle aged man with risk factors of smoking and hypertension. The centerline reconstructions showed the thoracic aorta above the aneurysm to be around 20mm in diameter and same below, with the celiac axis and superior mesenteric artery in the potential seal zone of a stent graft. The only plaque seen was around the level of the renal arteries and was focal and calcified. Looking at the list I had made as a comment to the Linked-In post, I realized that I really only had one viable option.
Open repair, usually the most expeditious option, was made challenging by the right hemothorax, making a left thoracotomy hazardous if the lung had to be deflated. Cardiopulmonary bypass would have to be arranged for, and that adds a metabolic hit that greatly raises the stakes. Of the endovascular solutions, the only viable option was TEVAR to exclude the rupture and debranching of the celiac axis and superior mesenteric artery. To those who would advocate for parallel grafts, there was no room in the normal 20mm diameter aorta. And branch systems for rupture are some time in the future. Also, the patient was becoming hypotensive. So the planned operation was first TEVAR to stop the bleeding, and then open surgical debranching. A hybrid repair.
The smallest stent graft we have is a 21mm graft, but it would not be suitable for this aorta. In practice, the normal aorta is quite elastic and will dilate much more than what is captured on a CTA. The next size we have is 28mm graft and I chose this to exclude the rupture, which was done percutaneously.
As seen below, the graft excluded the celiac and SMA. Late in the phase of the final aortogram (second panel) there was an endoleak that persisteed despite multiple ballooning. The timing suggested the intercostals and phrenic vessels contributed to a type II endoleak, but it was concerning.
Find the Endoleak
The bypasses were sent from the infrarenal aorta to the common hepatic artery and the SMA close to its origin, and the origins of the celiac axis and SMA were clipped. The bypasses were then done with a 10x8mm bifurcate Dacron graft originally for axillofemoral bypassing. It had spiral rings which I removed at the anastomosis and this resulted in a kink at the closer bypass. Usually, I loop this for iliomesenteric bypass but there was not enough distance from the infrarenal aorta. I have to add a little trick I modified from my pediatric surgery experience as a resident -a Heinecke-Mikulwicz graftoplasty:
This worked to relieve the kink as evidenced on the aortogram above. After closing the laparotomy, I placed a chest tube in the right chest. The patient had a course prolonged by a classic systemic inflammatory response syndrome, with fevers, chills, and leukocytosis. He bled for a while but stopped with correction of his coagulopathy. All blood cultures were negative, but a CT scan was performed out of concern for the endoleak, and the possibility of continued bleeding.
No endoleak was detected as the sac was fully thrombosed. There was a consolidation of the blood in the right chest, but it resolved with fibrinolytic therapy.
Discussion
This case illustrates several points I have been making on this blog.
Hybrid repairs are not some kind of compromise but the full realization of a complete skill set. When students ask me how to judge a training program, one of the best metrics is how frequently are hybrid operations performed. It means either the endovascularist and open surgical operator are in complete synchrony or there are individual surgeons competent in both open and endovascular surgery. Hybrid operations, rather than being a compromise, are an optimization.
Time -Laying the stent graft across the celiac and SMA origins starts a warm ischemia clock. The liver and intestines, in my reckoning, should be able to tolerate the 2 hours of work to get the bypasses working. Cardiopulmonary bypass may give you less ichemia but at the metabolic cost of the pump time. These negative factors add up, but were surmounted by the fact that early control of hemorrhage was achieved. Stopping the bleeding and restoring flow are the core functions of vascular surgery.
Planning and preparation. The ability to see the CT images and prepare the teams and materiel before the patient transferred was lifesaving. This is where our IT gets credit for responding to a critical need and formulating a solution that meets internal policies, external regulations, and saves a life. It illustrates so many opportunities particularly with electronic medical records and their processes which focus more on documentation for billing. A discharge summary should be multimedia like this blog post and it should be normal and easy to generate. And finally, as clinicians, we should mind technology with as much attention as we give to the latest medical devices and techniques.
Drs. Roy Miler and Xiao Yi Teng performing anastomosis on open coversion of an aortic stent graft, now graduated and in practice. A significant part of their open aortic experience is in addressing failing stent grafts.
I recently had to remove a stent graft for infection and got to thinking about how the number of people who could comfortably and confidently manage that has thinned out in the world through the unintended consequence of the medical device market place. In every surgical specialty over the past twenty years, many open procedures were replaced with a minimally invasive option which generally involved adoption of new technology and large costs to the hospital. These newer procedures were touted as easier on the patient while being easier to perform for the average physician than the open procedure that they were replacing. That was the other selling point -that one could do several of these operations in the time it took one open procedure. In most cases, they were at best almost as good as the open procedure but at higher cost.
In the marketplace, minimally invasive always wins. In many specialties it became untenable to practice without marketing these “advanced minimally invasive” skills. Hence, the wide adoption of robotics in urology outside major academic centers -during those years of rapid adoption the surgeons would get flown to a course, work on an animal model, then for their first case a proctor would be flown out and voila -a minimally invasive specialist is born. The problem comes when learning these skills displaces the learning of traditional open surgical skills. In general surgery, it is not uncommon to hear of residents graduating without having ever having done an open cholecystectomy. It is also the case that many vascular trainees graduate with but a few if any open aortic cases. What happens when minimally invasive options run out? Who will do my carotid endarterectomy or open AAA repair?
The first case is an elderly man with an enlarging AAA sac despite having had EVAR about seven years prior. No endoleak was demonstrated but the proximal seal was short on CT. Also, it was a first generation graft which is prone to “peek a boo” endoleaks from graft junctions and stent anchoring sutures. On that last point, I use the analogy of a patio umbrella -after seven seasons, they can leak where cloth is sewn to the metal struts. It is very hard to demonstrate leak of this kind on CTA or duplex ultrasound because they are small. The patient had his EVAR because he was considered high risk for open repair at the time of his operation -moderate COPD, mild cardiac dysfunction. His sac had enlarged to over 6cm in a short time, and therefore open conversion was undertaken. No clinical signs of infection were present. A retroperitoneal approach was undertaken. After clamps were positioned, the sac was opened.
The picture does not show it, but a leak from the posterior proximal seal zone was seen with clamp off. The clamp was reapplied and the graft transected flush to the aortic neck. A bifurcated graft was sewn to this neck incorporating the main body stent graft and aortic neck in a generous running suture. The left iliac limb came out well and the new graft limb sewn to the iliac orifice, the right iliac limb was harder to clamp and therefore I clamped the stent graft and sewed the open graft to the stent graft.
The patient recovered well and went home within the week. He was relieved at no longer needing annual CT scans.
Who needs annual CT scans? Patients with metastatic cancer in remission.
The second patient was an older man referred for enlarging AAA sac without visible endoleak. The aneurysm had grown over 7cm and was causing discomfort with bending forward. He too had been deemed high risk for open repair prior to his EVAR. If he had had an early generation Excluder graft, the possibility of ultrafiltration would be more likely and relining the graft would be reasonable (link). This was again a cloth and metal stent graft which can develop intermittent bleeding from graft to stent sutures, and I don’t think relining will help.
The patient was taken for open repair (above), and on opening the AAA sac, bleeding could be seen coming from the flow divider. It stopped with pressure, but I replaced the graft in a limited fashion from the neck to the iliac limbs as in the first case. This patient did very well and was discharged home under a week.
The third patient was another fellow referred from outside who had an EVAR for a very short and angulated neck, and a secondary procedure with an aortic extension in an attempt to seal the leak had been done. This failed to seal the type Ia leak. This patient too was deemed too high risk for open surgery of what was basically a juxtarenal AAA with very tortuous anatomy.
The patient was taken for open repair, and the stent grafts slid out easily (below).
A tube graft was sewn to the short aortic neck and distally anastomosed to the main body of the stent graft -with pledgets because of the thin PTFE graft material in this particular graft. This patient did well and went home within a week.
All three cases are patients who were deemed originally too high risk for open repair, who underwent EVAR, then underwent explantation of their failing stent graft. Only one involved a patient whose graft was placed off the IFU (short angled neck), but the rationale was that he was too high risk.
What is high risk? In non-ruptured, non-infected explantation of failing stent graft, the mortality is 3% (ref 2) from an earlier series from Cleveland Clinic. With stent graft infection, the 30-day mortality of surgical management from a multi-institutional series was 11% (ref 3) when there was no rupture. From a Mayo Clinic series, stent graft resection for infection came with a 4% 30-day mortality (ref 4). These were nominally all high risk patients at the time of the original EVAR.
Real world risk is a range at the intersection of patient risk and the expertise of the operating room, critical care, and hospital floor teams. The constant factor is the surgeon.
Endografts for AAA disease (EVAR, endovascular aortic aneurysm repair), makes simple work of a traditionally complex operation, the open aortic aneurysm repair. The issue has been the cost and risks of long term followup as well as endograft failure and aneurysm rupture. The Instructions For Use on these devices recommend a preop, a followup 1 month, 6 month, and 12 month CTA (with contrast) and annual followup with CTA for life. These devices were meant to treat high risk patients but high risk patients with limited life spans do not benefit from EVAR (ref 1, EVAR-2 Trial). These have lead the NHS in the UK to propose that EVAR has no role in the elective repair of abdominal aortic aneurysms in their draft proposal for the NICE guidelines for management of AAA (link). While this is a critical discussion, it is a discussion that is coming at least ten years too late. A generation of surgeons have been brought up with endovascular repair, and to suddenly announce that they must become DeBakey’s, Wiley’s, Imperato’s, and Rutherford’s is wishful thinking at best or wilful rationing of services at worst.
In 2006, Guidant pacemakers were recalled because of a 1000 cases of possible capacitor failure out of 28,000 implants for a failure rate of 3.7% -there were 2 deaths for a fatality rate of 0.00007%. EVAR-1 Trial’s 8 year result (ref 5) reported 16 aneurysm related deaths out of 339 patients (1.3%) in the EVAR group compared to 3 aneurysm related deaths out of 333 patients (0.2%) in the OPEN group.
Academic medical centers, behemoths though they are, serve a critical function in that they are critical repositories of human capital. The elders of vascular surgery, that first and second generation of surgeons who trained and received board certification, are still there and serving a vital role in preserving open aortic surgery. My generation -the ones who trained in both open and endovascular, are still here, but market forces have pushed many of my colleagues into becoming pure endovascularists. The younger generation recognizes this and last year, I sat in on an open surgical technique course at the ESVS meeting in Lyons organized by Dr. Fernando Gallardo and colleagues. It was fully attended and wonderfully proctored by master surgeons. This is of critical importance and not a trivial matter. As in the 2000’s when endovascular training was offered as a postgraduate fellowship in centers of excellence, there is no doubt in my mind that today, exovascular fellowships need to be considered and planned and that current training must reinvigorate and reincorporate their open surgical components.
During our daily morning huddles, peopled by cardiologists and cardiac surgeons, one thing impresses me more than anything else. The assembled interventional cardiologists, world class and renown, they who can place a stent in any part of the body, will defer to the unassailable superiority of the LIMA to LAD bypass over any existing intervention. I am always a little sad that the analog for this, the vein bypass in the leg does not get the same love. The open surgical bypass of the leg is the great straw man at international symposia. It is fast becoming a diminishing and curious habit of a fading generation.
The acknowledged superior hemodynamics and patency of the bypass is diminished in the literature by pooling patency loss with other factors such as amputation, heart attacks, and death. Some vascular surgeons dogmatically cling to habits learned in training that favor complications, making themselves their own worst enemies both in the literature and in the marketplace. These bad habits involve long incision length, closure techniques that do not anticipate edema, and wound orientation that makes failure more likely.
Operations require far more support and resources to succeed than do interventions that soon go home. Brilliant operations alone will not heal the patient. It is pathways and postoperative care infrastructure and staff that prevent these secondary complications -the very complications that keep the leg vein bypass from being as respected, if not loved, as the LIMA to LAD.
The postoperative care of these patients devolves to management of leg edema. No medical or nursing school adequately teaches the basic science nor management of edema, which is the most common vascular condition
The incisions are too long in the classic vein bypass. When you create and then close an incision, the inflammation drives the accumulation of fluid in the extracellular space – creating edema. This postoperative edema, poorly managed, results in complications that leave the patient hobbled with time lost to healing wound complications, pain, and excess limb weight. Additionally, vein bypasses usually involve groin exposure and the delicate lymphatics that coalesce there are perturbed or destroyed during exposure. Postop, this damage and the inflammation rapidly overcomes the capacity of a lymphatic system. The traditional vein harvest also involves cutting through deep layers of fat. The fat is typically closed by broad sutures that create areas of fat necrosis -potential fodder for bacteria. The best ways the complications of long and deep incisions is to avoid them altogether. The calculus of the operative moment – “I must see the vein,” must include the vision of a patient losing months to wound therapies to heal a gaping, necrotic, infected wound. I recommend skip incisions or adopting in-situ bypass technique with endovascular management of fistulae. Or corral your cardiac PA to harvest the vein segment in the thigh after mobilizing the vein in the leg with the endoscope.
The incisions are often closed with Nylon sutures and skin clips which can become potential foci of infection. With edema, they create zones of ischemia around them, killing skin and creating entry points for skin flora as the skin expands under an unyielding clip or suture. Placed under a pannus, these sutures or clips fester in an anaerobic environment. Closure should adhere to anatomy. The body relies on connective tissue planes to keep itself together. In the groin, these are Scarpa’s layer and the dermis. They should be closed with absorbable monofilament in a buried interrupted fashion at the dermis with a final running subcuticular layer of 4-0 absorbable monofilament. Steristrips or glue at the skin finishes the job. If you use sutures, particularly at the distal anastomotic site, take care to realize that you have about 12 hours before the skin dies in the best of circumstances, and less with microangiopathy of diabetes and ESRD. Squeezing out the edema before closure with a sterile Esmarch or short counterincisions or even a large one to allow for tension free closure over an anastomosis will prevent wound complications over your graft.
The classic longitudinal groin incisions that cut across the inguinal crease divides a tension point -that crease is like a cord that supports the pannus that is slung over it and when divided and then closed with a stitch, that stitch then bears the weight of that pannus every time the patient sits up or stands. If you are observant, wound necrosis typically starts at the groin crease under a surgical clip or suture. Incisions in the groin should be obqlique and parallel to this crease, or if you can, even inside this crease. When these wounds are closed, the natural lines of tension are in line with the incision rather than orthogonal to it. The natural forces keep the wound shut.
This is only the first step. The next is keeping the wound clean and dry for at least 5 days. At the Mayo Clinic, where I trained, the nurses up on 5 Mary Brigh were trained to blow dry the groin wounds every few hours on cool setting and redressing the wound with dry gauze. You can get something close to it by ensuring the wounds painted with betadine, allowed to air dry, and dressed with dry gauze. If there is a constant leak of fluid, you have a serious problem as there is too much edema in the leg, or the wound isn’t closed, or there is a lymph leak. It needs to be actively dried out or you get a wet, macerated, infected wound like a grenade went off in the groin.
They don’t teach compression wrap techniques in medical or nursing school
The simplest thing to avoid lymph leaks is to not make them. Cutting near lymph nodes is hazardous, and once below Scarpa’s you have to orient your dissection directly over the femoral artery. Stray horizontally and you will undoubtedly cut one of the 4 to 10 invisible lymph channels.
They are invisible but detectable -after you break them, you will see a constant wetness in the wound. Think about injecting a cc or two of Lymphazurin (Isosulfan Blue, for those not allergic to Sulfa) into the intertriginous space on the same foot and you will see the lymph channel in bright blue, or stare carefully at the likely spots for a lymph leak and clip it, burn it, Ligasure or Harmonic scalpel it.
Lymph leak identified from saphenectomy incision (for CABG)
So how did we get to a rather dry discussion about edema? Wound complications are tremendously debilitating and offset any benefit from vein bypass operations. These long incisions become terrible big wounds if not prevented. It takes the concerted effort of a team and particularly nursing in actively managing edema. And at the end, the patient too must be included in this discussion. For the vein bypass of the leg to get the same respect and love as the LIMA to LAD bypass, surgical wound complications must become never events.