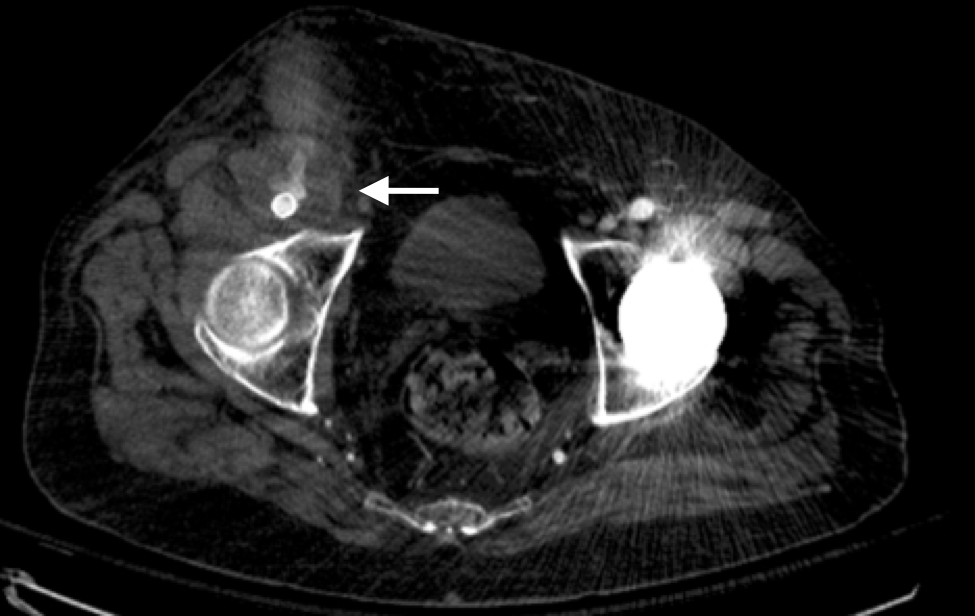
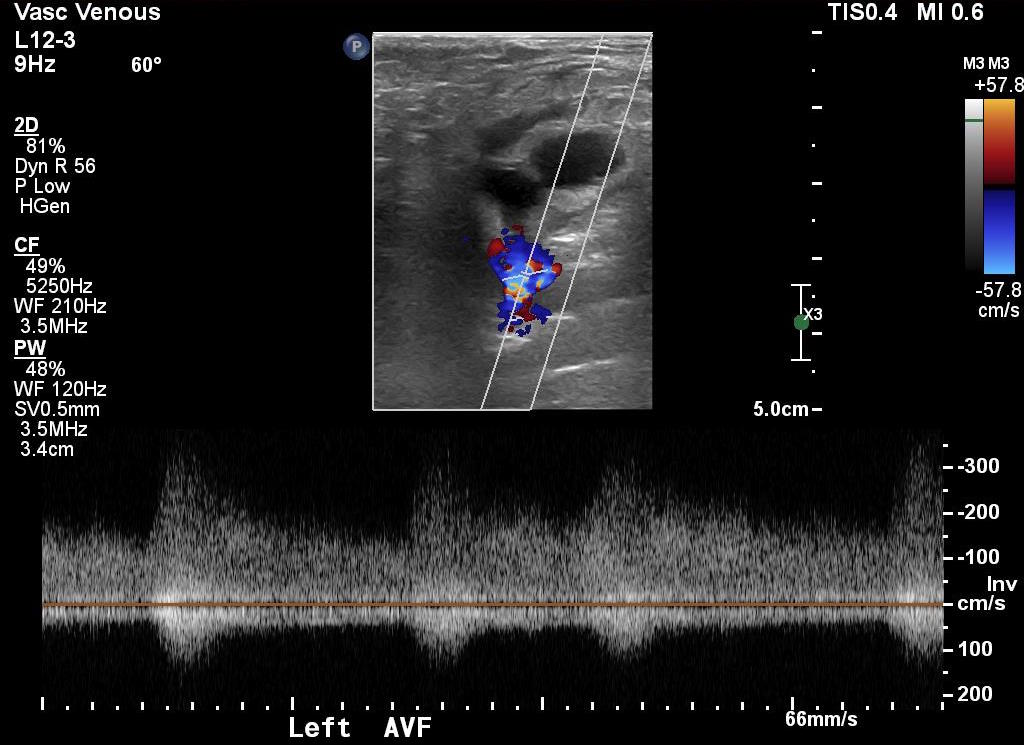
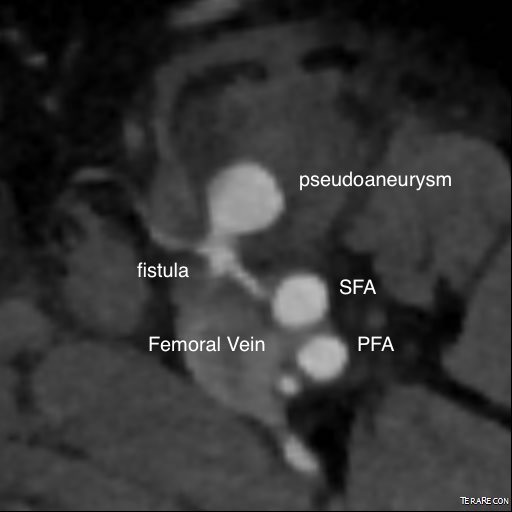
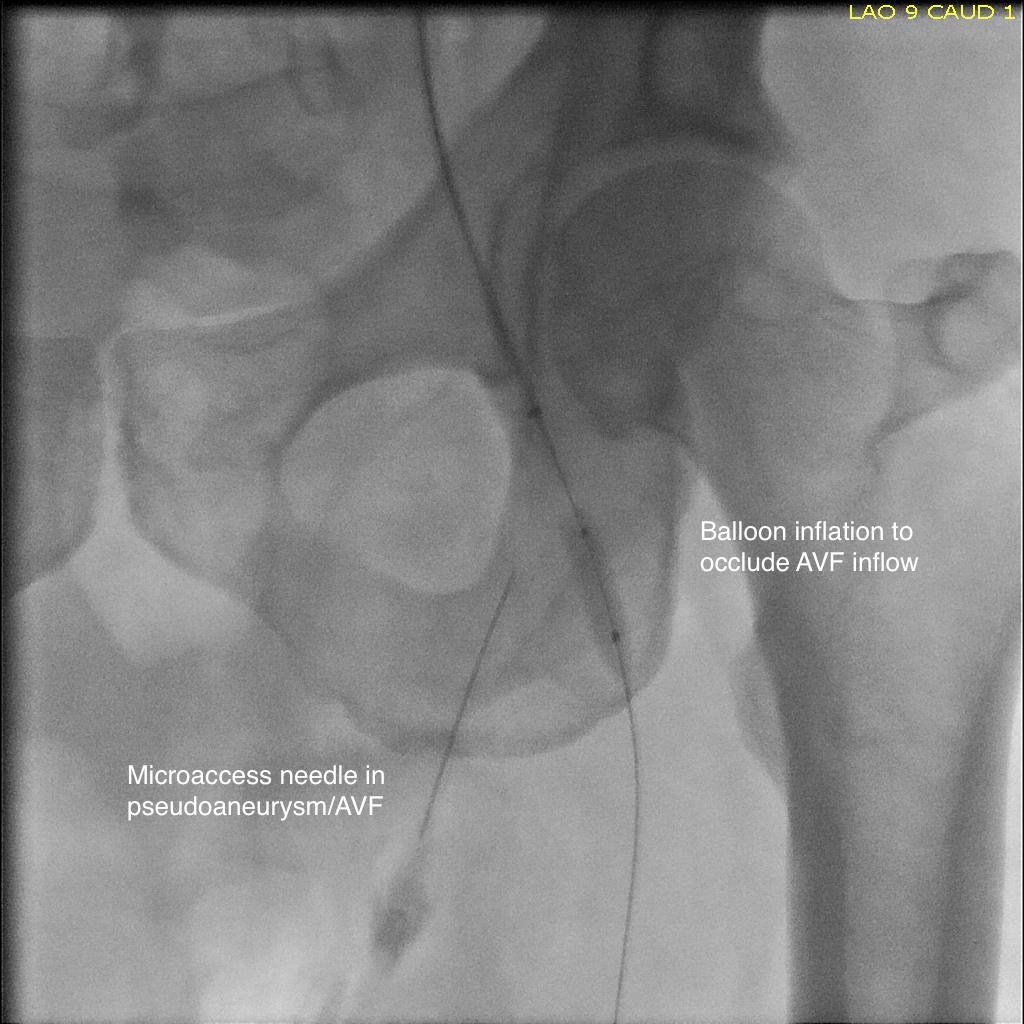
A surgeon from Nepal posted a case of a ruptured common femoral pseudoaneurysm infected from IV drug abuse on LinkedIn. The comments centered around typical textbook responses which were:
- Ligate, debride, obturator bypass
- In situ bypass with femoral vein +/- sartorius flap
- Rifampin soaked graft or crypreserved allograft
- Ligate only
My preferred treatment is #2, in-situ bypass with harvest of adjacent deep femoral vein. I never liked that procedure because in general in these patients, everything bleeds. Then I had a thought -how about if you mobilize the external iliac artery in the pelvis over its entire length and pull it out from under the inguinal ligament to sew to the femoral bifurcation or SFA? That is, when you enter the pelvic retroperitoneum to gain proximal control:

You mobilize the external iliac artery from the iliac bifurcation to the inguinal ligament, detaching the inferior epigastrics as a last step. And then you pull it out from under the inguinal ligament, and anastomose it to the femoral bifurcation or the SFA.

This makes sense because in young people and those with AAA and minimal atherosclerosis, the external iliac artery is both redundant and elastic, making it suitable for a pull down transposition. But then, how do you know as you mobilize the artery in the pelvis that you have enough to pull down?
Pythagoras figured that out two an a half millenia ago. If you measure the straight line distance from iliac bifurcation to the takeoff of the inferior epigastric arteries, you get the straight line external iliac artery distance. The length of the common femoral artery which is the excess EIA length needed, is assigned the value x. Then the height of the stretched artery off the line between the iliac bifurcation and the inguinal ligament will determine how much extra artery you have.

Taking these values, I did some maths.
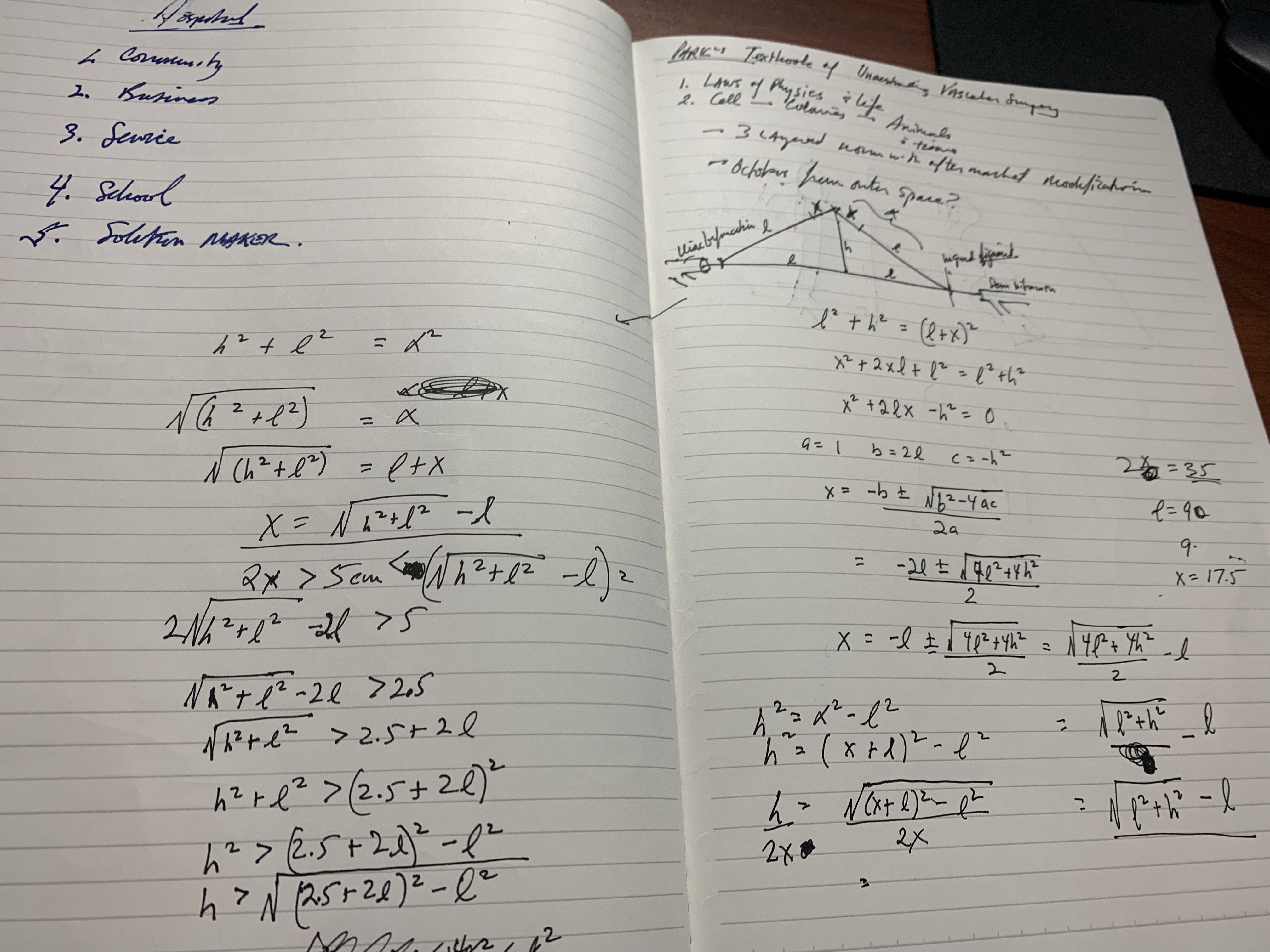
The solution for h, the height, is highlighted in yellow below. (note, the variable x in my notes is half the length of CFA, l is half the length of EIA, ie. 2x is CFA length).

Creating a spreadsheet for CFA lengths from 2 to 6cm and EIA straight distances of 5-10cm, the ratio of height H to CFA length varies from a minimum of 0.7 to maximum of 1.7 with an average of 1.1. That means the majority of the time, if you get 1.5x the length of CFA height off the pelvis, you should reach.

If you are short, you can detach the profunda and mobilize the SFA, pulling upwards, then reattach the PFA. Though this is entirely a thought experiment, there is no reason why it should not work. As with most things, I predict that it already has been done!
The advantages are using autologous tissues and leveraging the natural anatomy. There is a cost benefit in that OR time is shorter with less time for venous harvest and avoiding grafts, patches, and devices. The patient would avoid ischemia as would happen in the staged repair. The disadvantage is when you are short, but if you mobilize the appropriate amount (height off pelvis at least 1.5x the CFA length) you should be okay. The more curvature and tortuosity seen on 3DVR recontstruction and absence of significant atherosclerosis would predict feasibility.