A basic recipe for treating complicated aortic dissection
#aorticsurgery #tevar
 A Surgeon's Notes
A Surgeon's NotesA basic recipe for treating complicated aortic dissection
#aorticsurgery #tevar
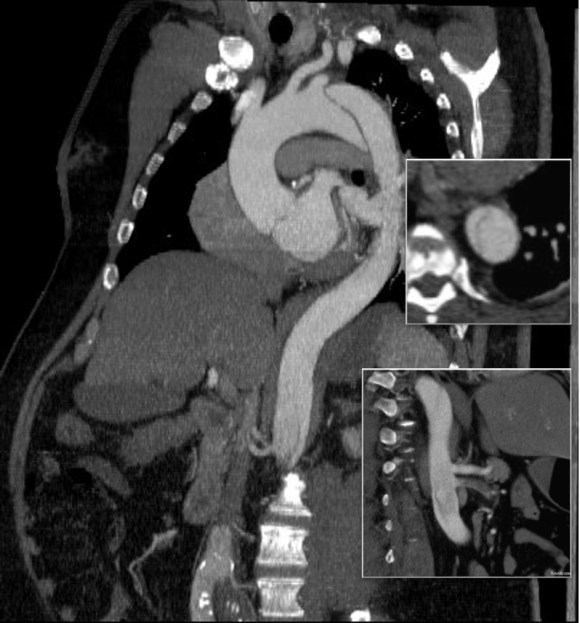
The patient is middle aged and had a type B thoracic aortic dissection (TBAD) as a consequence of recreational substances that acutely raised his blood pressure. At the outside hospital, he had a CTA showing the dissection extending from his left subclavian artery and causing occlusion of his superior mesenteric artery (SMA). He developed abdominal pain and was swiftly transported to our acute aortic syndrome unit. He was taken to the operating room and underwent a TEVAR of the dissection and stenting of his SMA -this is similar to other cases I have discussed in prior posts so I am omitting the technical details. The stent covered the left subclavian artery origin to exclude the origin of the dissection. The stent was extended to the distal thoracic aorta but did not go to the celiac origin.

Post procedure, his lactate never rose and he was maintained on the usual post procedure protocol of keeping MAP’s (mean arterial pressure) above 80mmHg. His left subclavian artery was covered but I do not routinely bypass, especially when the left vertebral artery is at least equal in size to the contralateral one. I don’t often place spinal drains for urgent/emergent cases particularly in patients who have never had infrarenal aortic surgery and patent hypogastric arteries. He was kept sedated overnight and awoke in the morning unable to move his legs to command. He had no pain sensation up to his umbilicus.
A spinal drain was emergently placed and his blood pressure was raised to MAPs of 90+, but these failed to reverse his paralysis. After discussion among my world class partners, I chose to take the patient back for a carotid subclavian bypass which was done through a single incision with a dacron bypass graft.
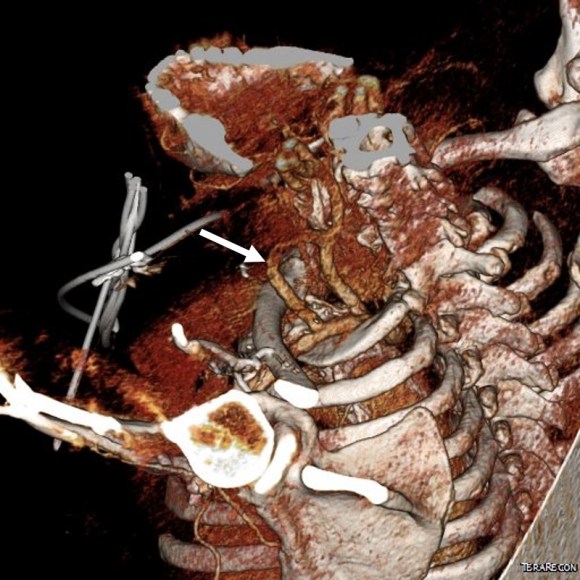
His paralysis resolved. He was discharged home, ambulating without assistance. Spinal cord complications are reported to occur between 1-5 percent of patients undergoing TEVAR for complicated TBAD. They were seen in 2 of 72 patients in the TEVAR arm of the INSTEAD trial (Circulation, 2009 vol. 120(25) pp. 2519-28), and was permanent in 1. While there are some who routinely place prophylactic drains, it is unclear to me that they have a significant effect if placed unselectively. I will place a Preop drain in the instance of infra renal graft, hypogastric arterial occlusive disease. In the instance of a dominant left vertebral, I will perform concomitant bypass, but just as often not. This is a gratifying and rare outcome of paralysis reversed with a carotid subclavian bypass when spinal drain and permissive hypertension did not.
