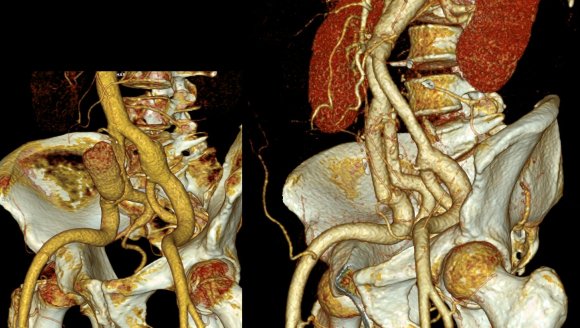
The patient is an active man in his 60’s with a history of hypertension who had known about a right common iliac artery aneurysm for several years and had come for an opinion. He was asymptomatic of pain. He had a prior splenic artery aneurysm embolization about a decade prior to presentation.. CT scan showed a large eccentric aneurysm arising from a retrograde chronic dissection dilating the right common iliac artery to over 4cm. This is typically iatrogenic, but impossible to know for sure. The left common iliac artery was ectatic to 2cm as was the aorta to 3 cm and all were “wavy.” This sort of tortuosity is the result of remodeling in the axis of flow resulting in lengthening of the artery and is found in those with the substrate for aneurysmal degeneration (footnote). He did not smoke and he could climb stairs without dyspnea or chest pain.

On examination, he was a fit middle aged man with a slight paunch. His abdomen was soft and his peripheral pulses were present and normal. Laboratory results were normal, including creatinine. EKG and echocardiogram were also normal.Treatment options were discussed in detail. The patient was paying for the operation himself and wanted to understand in detail the possible options. These included
1. Open aortobi-iliac bypass with a jump bypass to the right internal iliac artery
2. Open aortobi-iliac bypass with ligation of right internal iliac artery
3. EVAR with right external iliac extension after embolization of right internal iliac artery
4. EVAR with parallel grafts to right external and internal iliac artery (off label)
5. EVAR with iliac branched graft to right internal and external iliac artery (off label)
People are known to react with emotions and to decide typically for near term gain over far term benefits. The offer of an operation involving laparotomy and a possible weeklong hospitalization with all the attendant risks of death, heart attack, stroke, ileus, wound infection, pneumonia, organ failure and so on provides a stark contrast to the appeal of endovascular repair which can be done percutaneously, with local anesthesia, and with a short hospital stay. The lifelong CT scans are in the murky future compared to the present which is sharply in focus. This is why few people save for retirement, why profligate grasshoppers far outnumber industrious ants. In the same vein, the offer of an “advanced minimally invasive” solution plays to several cognitive biases that exists in the mind of not only the patient but the health-care provider. These include this preference for short term gain over long term gain, but also viewing all innovation as being necessarily better than what was available.
After going over the operation in great detail, the patient cut me off when I mentioned the need for lifelong followup CT scanning. Because he lives in several countries, typically, he has to pay for his healthcare out of pocket and he balked at the notion of paying for an annual CT scan. He was also disdainful of the possibility of reintervention (quoted at 10%) and having to pay for it. Also, the stent grafts, which he would have to pay for, end up being as costly as a new luxury sedan based on local pricing.
We chose open surgical repair via a midline laparotomy. An aortobi-iliac bypass was performed from proximal aorta to right internal iliac artery and left common iliac artery bifurcation with a jump bypass from the right graft branch to the right external iliac artery. Technically, this sequence was chosen for ease of access to the internal iliac artery with the external clear of graft. Operative time was 3 hours. He was in the ICU for one night. He went home after 10 days after contracting a UTI. In followup three weeks after discharge, because he had fevers, a CT scan was performed (figure). He was treated for an upper respiratory infection which cleared, and he has been doing well since. We are both happy that he will never need a followup CT scan.
The literature supports this stance. The long term followup of the EVAR-1 Trial (Reference 1) is an example. This was the late followup of the prospective randomized study looking at open surgery versus EVAR in 1252 patients. The initial EVAR 1 findings are well known and put into question the long term benefits of EVAR as the initial mortality benefit of EVAR is lost within a few years of treatment. At a mean of 12.7 years of followup, there were more deaths from aortic aneurysm rupture and aneurysm related death in the EVAR group compared OPEN surgery (adjusted HR 5.82, p=.0064), with 13 AAA ruptures. I have mentioned before that the failure of a handful of pacemakers drove the Guidant company to recall over 20,000 of their devices. Plus, the cost of annual CT scans in the treatment group and cost of devices and cost of reintervention have driven the UK’s NICE Guidelines recommending against EVAR in elective AAA repair. The meta-analysis of EVAR-1, DREAM, OVER, and ACE trials comprising 2783 patients is confirmatory, that aneurysm related mortality was significantly higher after the initial mortality benefit of EVAR fades away, and that patients of marginal fitness gain no advantage from EVAR, particularly those with heart or renal disease, and those with PAD had lower mortality in the period of 6 months to 4 years (reference 2).
I post this case, because despite a complications, in this case UTI and URI, the patient did fine. So why is open aortic surgery considered a dying art? Why is there such pushback against the UK NICE Guidelines?During my residency in the 1990’s, in the heyday of open surgery, I observed a lot of mediocre vascular surgeons and a very few great ones. The average vascular surgeon would take 6-8 hours to perform open aortic surgery, and the patient would come out with a typical picture of oliguria, third spacing, SIRS, that would generate a 1-2 week stay that would even be described as the normal and expected course for AAA repair in surgical and critical care textbooks. The best surgeons back in the day did these operations under 3 hours with 100mL blood loss and the patients would spend a day in the ICU (often not needing it), and 3-7 days in the hospital, but they were the exception.A higher percentage of surgeons today can do EVAR well than surgeons 25 years ago could perform competent open aortic surgery. Most surgeons graduating from training rarely see or do open aortic surgery compared to the multitude of interventions. Capable open surgery basically is not available outside of a few centers, and most surgeons admit to not having equipoise to start a new trial with modern devices. Open aortic surgery is a lost art, like growing your own vegetables, dressing your own game, reading cursive script, and dialing a rotary telephone.
It is not for a lack of desire. I have several younger colleagues I have met or interacted with via social media who have an intense interest in gaining open vascular skills. They have organized open skills courses at major European vascular meetings, but I believe that is not enough.The need for exovascular fellowship, the running topic of conversation of older surgeons through the 2000’s, is never as critical as it is now as we see milennia of surgeon-years of experience retiring to golf courses and cottages. The recommendation for preferring open surgery in the younger and fitter patients is sadly out of reach for most patients and surgeons. The same passion in disseminating endovascular knowledge needs to be applied to repair the damage to vascular education by over-relying on and over-prescribing endovascular approaches.
Finally, and sadly, this patient is the exception. When given clear options and outcomes and costs, this patient made a rational decision, choosing value over convenience.
Reference
1. Lancet 2016;388: 2366-2374.
2. BJS 2017;104:166-178
Footnote:
Pearls for finding AAA:
1. Tortuosity of the internal carotid arteries including loops and hairpin turns found in patients particularly smokers implies the present of a AAA until proved otherwise
2. Palpating bounding popliteal or pedal pulses in an older smoker implies the presence of a AAA until proved otherwise. Especially if the medical student can feel these pulses.
3. African-American Females with Diabetes almost never get AAA.
4. Palpate their abdomen
 The inflow graft area is taken from its measured diameter. Then usually one or the other artery has an obligate size -a size the graft has to be while the other has more “wiggle room.” The other thing that comes from experience is that the AFX graft’s iliac limb extension don’t get the B-infolding that can affect an oversized stent graft placed in a small artery and it accomodates a neighbor well.
The inflow graft area is taken from its measured diameter. Then usually one or the other artery has an obligate size -a size the graft has to be while the other has more “wiggle room.” The other thing that comes from experience is that the AFX graft’s iliac limb extension don’t get the B-infolding that can affect an oversized stent graft placed in a small artery and it accomodates a neighbor well.