One of the nice things about practicing at the Clinic is being able to offer unique solutions. A severely diseased or occluded external iliac artery (EIA) can be a vexing problem, particularly if bilateral, in this endovascular era. Many cardiovascular devices require femoral access that has to traverse compromised iliac arteries -those with large (>16F) delivery systems require a sufficiently wide path to get the devices to the heart and aorta. Also, living related donor kidney transplantation is predicated on minimizing risk to maximize results and having significant iliac plaque negates one as a recipient for this high stakes elective procedure. In situations where the EIA is too small to accommodate devices because of atherosclerotic plaque, the typical solution is placement of a conduit to the common iliac artery or the aorta. The practice of “endopaving” with a covered stent graft and ballooning is also described, but its long term outcomes are not reported and the internal iliac artery is usually sacrificed in this maneuver.
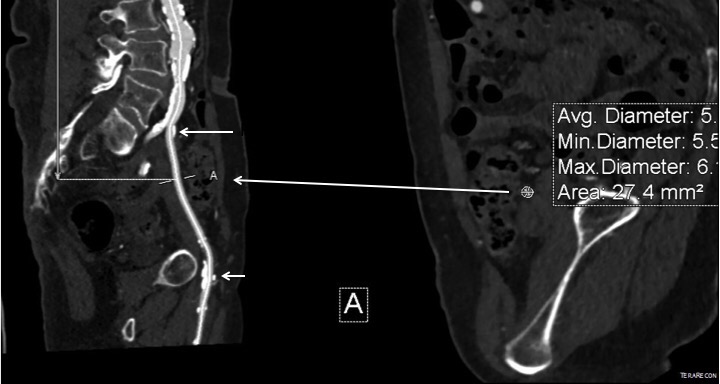
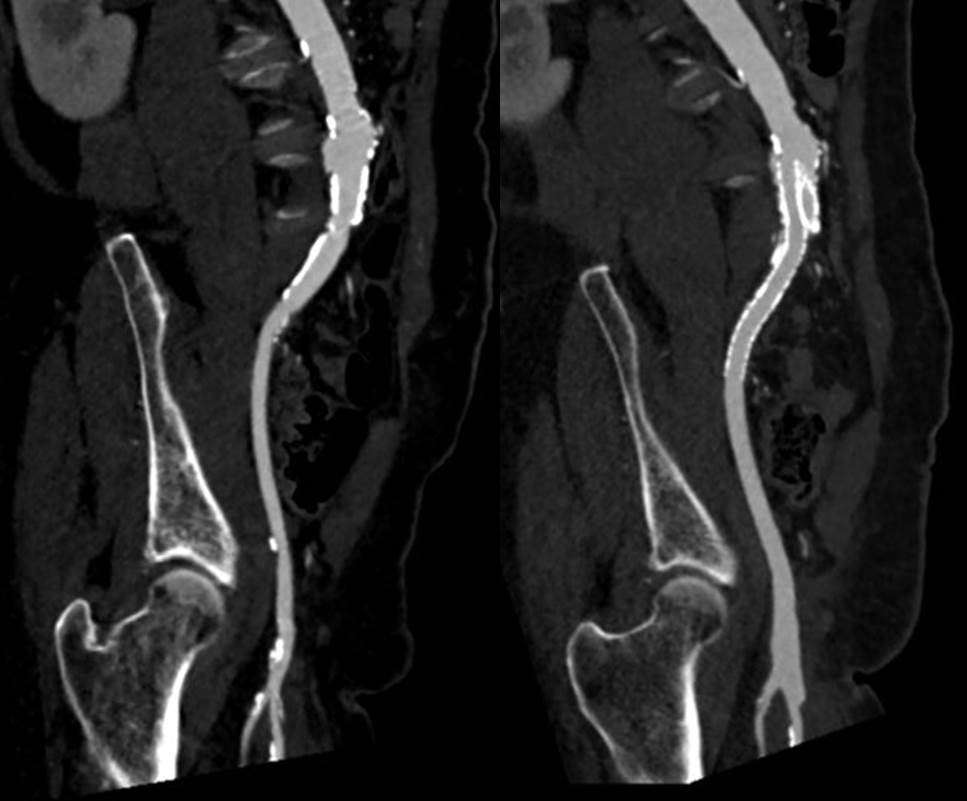
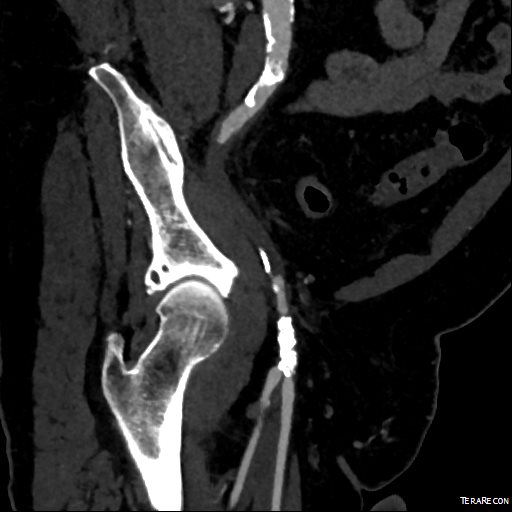
This patient presents with lifestyle limiting claudication and an absent right femoral pulse. ABI is moderately reduced on the right to 0.57, and he had no rest pain. CTA at our clinic revealed an occluded EIA bracketed by severely calcified and nearly occlusive plaque of the common iliac artery (CIA) and common femoral artery (CFA).
The patient was amenable to operation. Traditionally, this would have been treated with some form of bypass -aortofemoral or femorofemoral with a common femoral endarterectomy. While endovascular therapy of the occluded segment is available, one should not expect the patencies to be any better than that of occlusive lesions (CTO’s) in other arteries. Hybrid open/endovascular therapy is an option as well with CFA endarterecotmy and crossing CIA to EIA stents, but I have a better solution.
The common femoral endarterectomy rarely ends at the inguinal ligament, and is uniquely suitable for remote endarterectomy, a procedure from the early to mid twentieth century.
The addition of modern fluoroscopic imaging and combining with endovascular techniques makes this a safe and durable operation.

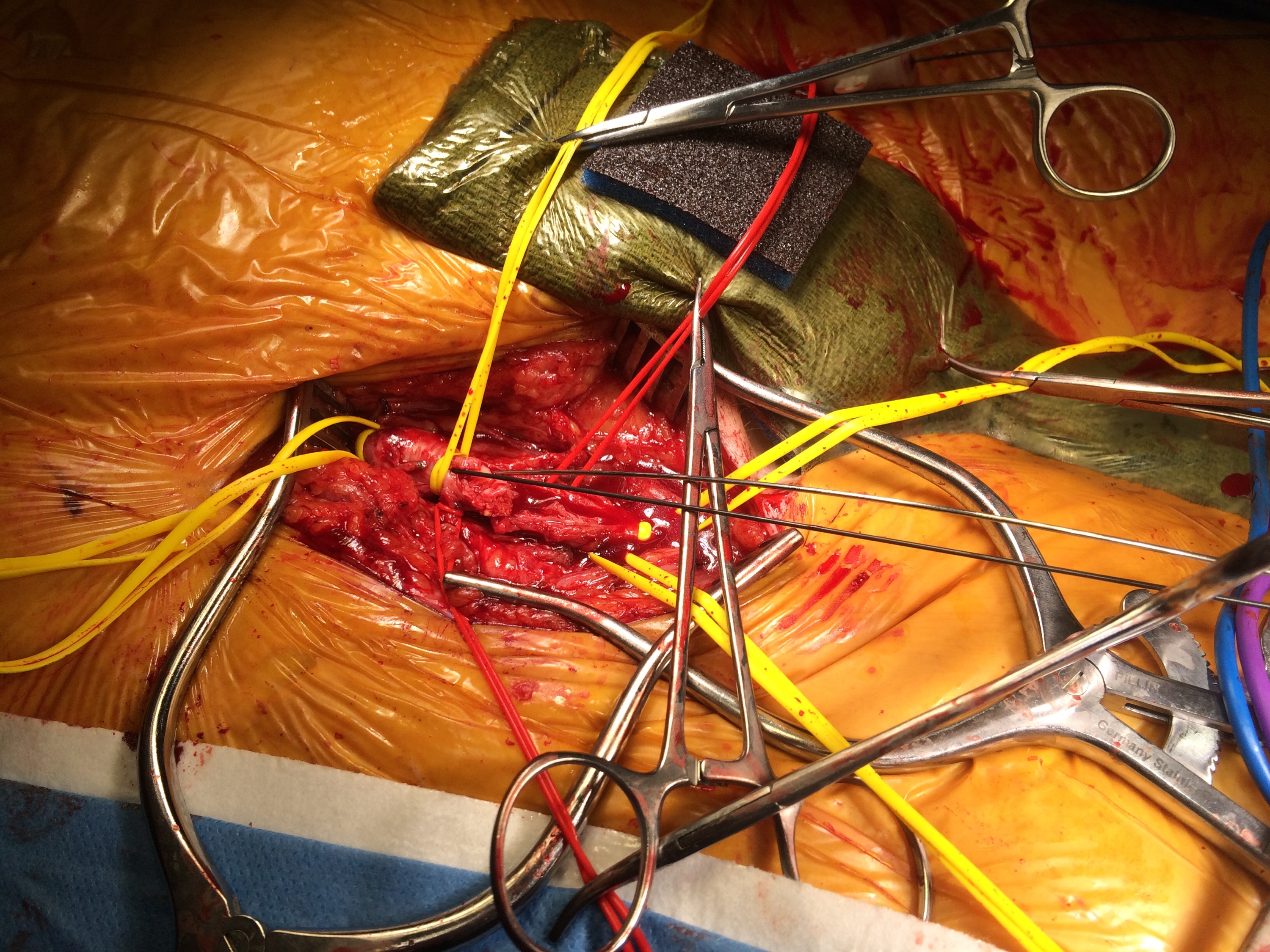
The patient was operated on in a hybrid endovascular OR suite. A right groin incision was made to expose the common femoral artery for endarterectomy and left common femoral access was achieved for angiographic access, but also to place a wire across the occlusion into the common femoral artery.
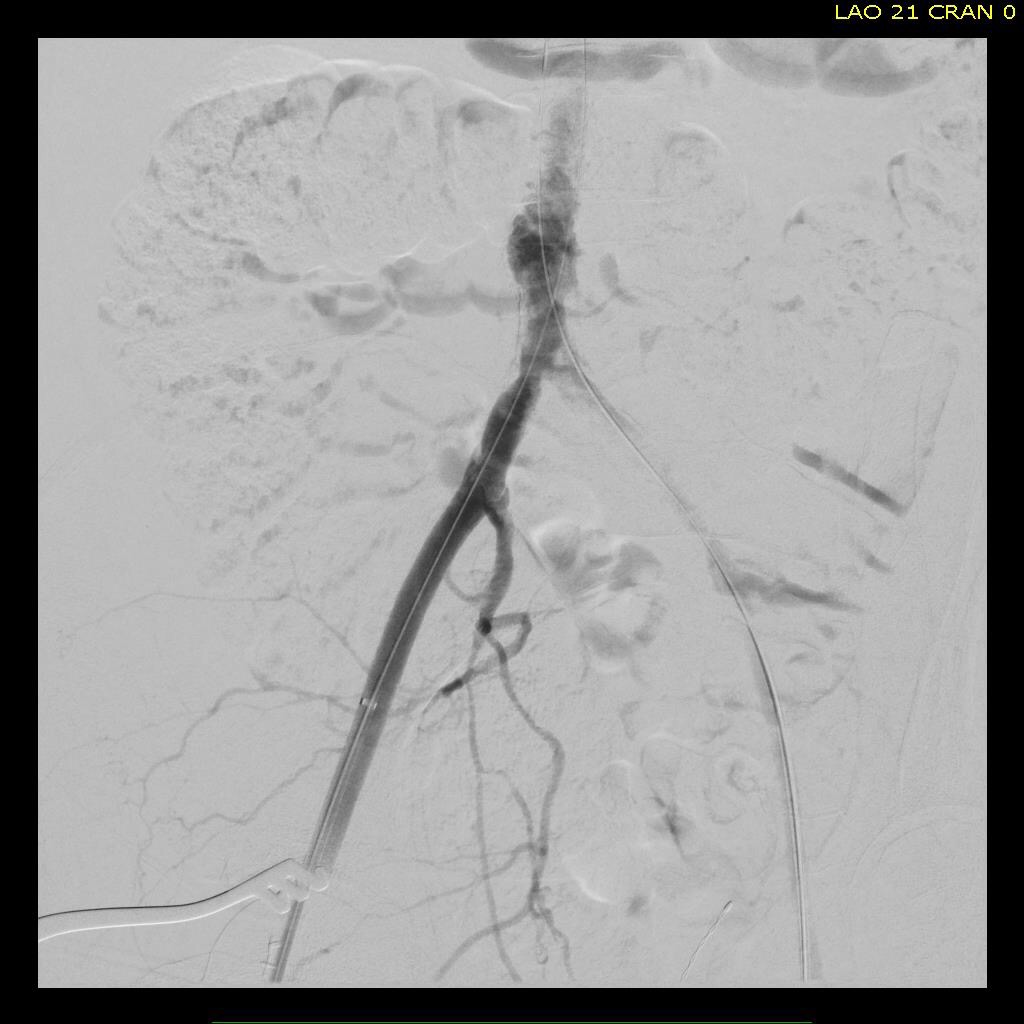
All actions on the external iliac artery plaque are done with an up-and-over wire, allowing for swift action in the instance that arterial perforation or rupture occur. This event is exceedingly rare when the operation is well planned. With this kind of access, an occlusive balloon or repairing stent graft can be rapidly delivered.
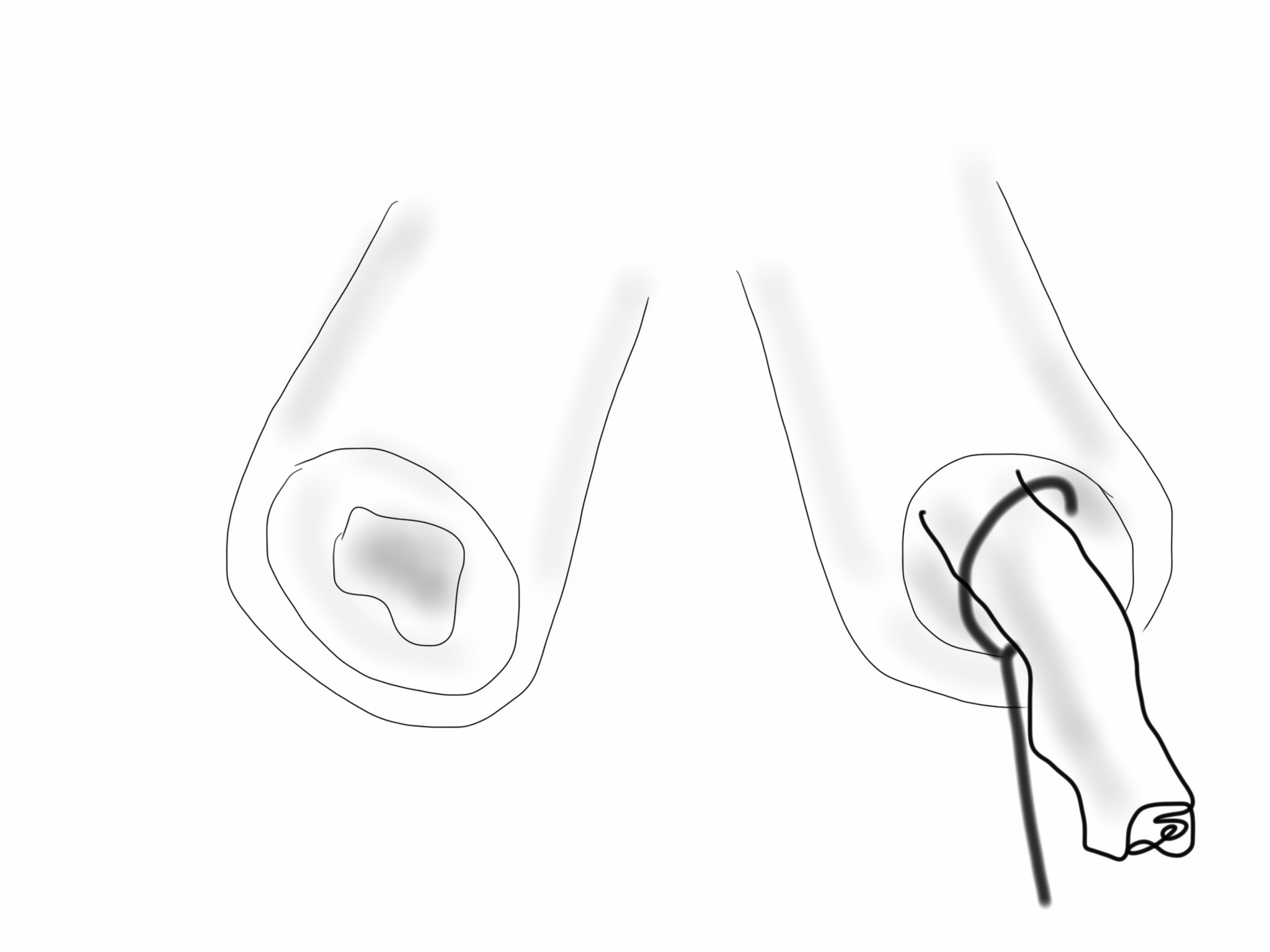
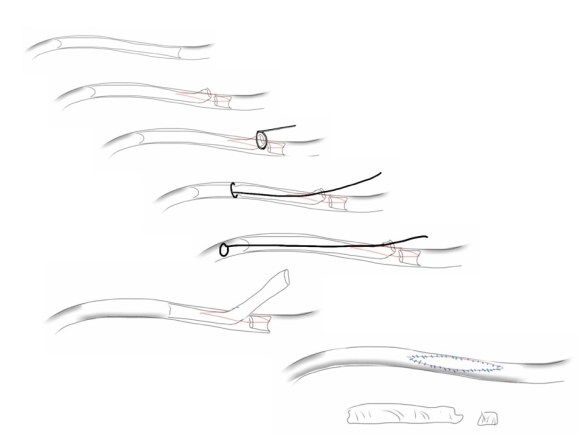
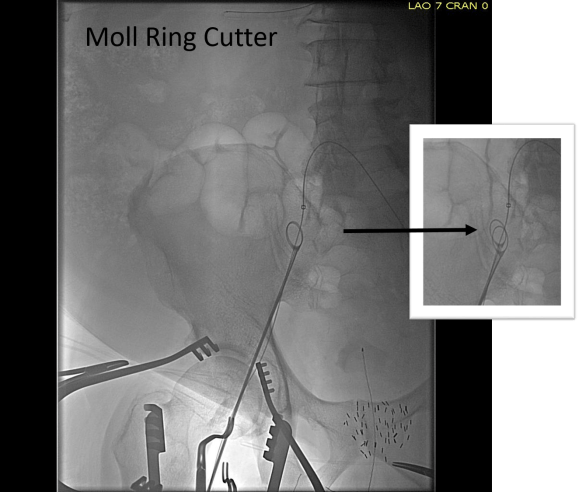
The common femoral endarterectomy is done from its distal most point and the Vollmer ring is used to mobilize the plaque. A Moll Ring Cutter (LeMaitre Vascular) is then used to cut the plaque.

The plaque is extracted and re-establishes patency of the EIA.

The plaque end point is typically treated with a stent -in this case, the common iliac plaque was also treated.

What is nice about this approach is that this artery has been restored to nearly its original condition. I have taken biopsies of the artery several months after the procedure in the process of using the artery as inflow for a cross femoral bypass, and the artery clamped and sewed like a normal artery and the pathology returned normal artery.
This has several advantages over conduit creation which can be a morbid and high risk procedure in patients who require minimally invasive approach. A graft is avoided. The artery is over 8mm in diameter where with stenting up to 8mm with an occlusive plaque, the danger of rupture is present, and often ballooning is restricted to 6mm-7mm. This is insufficient for many TEVAR grafts and TAVR valves.
For patients being worked up for living related donor transplants who are turned down because of the presence of aortoiliac plaque, those with the right anatomy can undergo this procedure and potentially become candidates after a period of healing.