Adding a vascular surgeon to a hospital is like eating one of these. It turns Mario into Mega Mario. Vascular surgeons turn community hospitals into tertiary care centers.
Recalling the medical school adage, “when you hear hoofbeats, it’s probably horses, not zebras,” it is critical to think about rarities down on the differential list whenever you come across a patient. Vascular diseases suffer from inadvertent obscurantism arising from its absence from medical school curricula such that common disorders like mesenteric ischemia and critical limb threatening ischemia are frequently missed by even experienced medical practitioners. Vascular zebras are even harder to pin down because many experienced vascular specialists practice for years before they encounter, for example, adventitial cystic disease or dysphagia lusoria with a Kommerell’s diverticulum. Even so, real patients have these disorders, and we are all subject to inexperience bias -the feeling that something does not exist until you see it. You may completely miss something staring at you in the face or worse, deny its existence.
The patient is a middle aged man in his 50’s who aside from mild hypertension had no real risk factors. One day, at work, his right leg stopped working. He developed a severe calf cramp and the forefoot was numb and cool. He went to his local hospital and the doctors there appreciated the lack of pulses in the right leg and got a CTA, of which I only had the report which found a right popliteal artery occlusion.
The next morning, as he had signals and was not having rest pain, his doctors discharged the patient on clopidogrel and scheduled for angiography and stenting, per patient. As his debilitating claudication did not go away over the weekend, he came to our emergency room. While he had no rest pain, he did have minimal walking distance before his calf muscles seized up. On exam, his right foot was cool and cyanotic, with intact motor function and sensation. There was a weak monophasic posterior tibial artery signal. Bedside point of care photoplethysmography showed dampened waveforms (below).
Look at the blue line. The waveforms are dampened in the ischemic foot.
Because he did not bring his CT, I repeated the study. I have written extensively on the need to be able to share CTA studies without barriers. After his study, I brought it up on 3D reconstruction software.
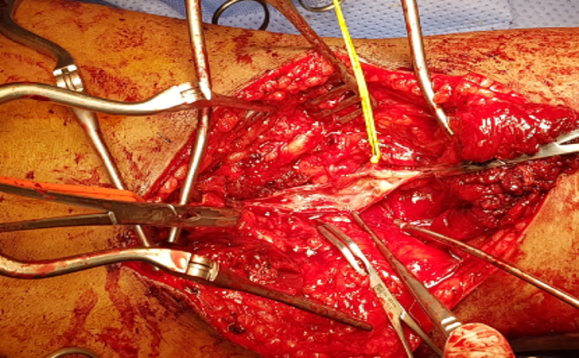
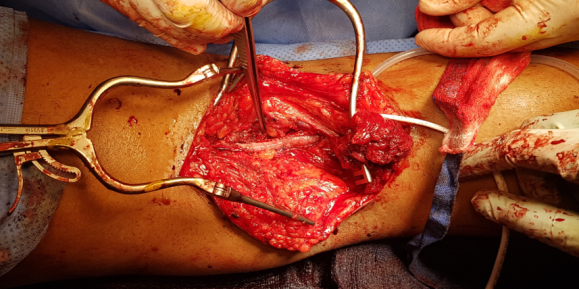
It clearly showed a Type II Popliteal Artery Entrapment affecting both legs (CTA images in series above). Stenting it would have failed. I spoke with the patient about operating the next day. The plan was popliteal artery exploration and thromboendartectomy with myotomy of the congenitally errant medial head of the gastrocnemius muscle. The patient was agreeable and I took him to the operating room for a myotomy and popliteal thrombendarterectomy in the prone position. The medial head of the gastrocnemius muscle went over the popliteal artery and inserted laterally onto the femur.
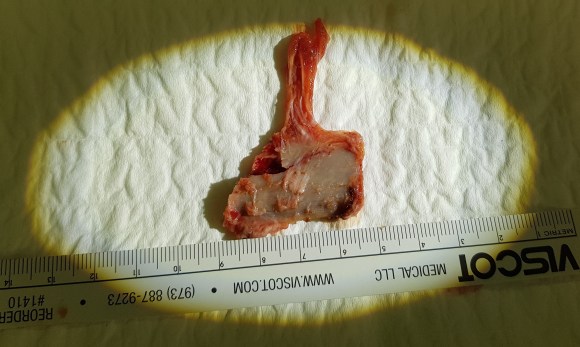
Endofibrosis, cut medial head of gastrocnemius muscle to right of distal clsmp
The artery was opened and while there was fresh clot, the artery showed signs of chronic injury as evidence by endofibrosis which pealed off. Pathology showed to be fibrotic in nature.
Trichrome stain showing chronic endofibrosis
The artery was repaired with a pericardial patch and flow restored to the tibials, not all of which were completely patent.
The patient was discharged after about a week and will be scheduling repair of his contralateral popliteal artery entrapment.
The vascular surgeon has a vital role in a hospital’s medical ecosystem. One time, I heard hospital administrator say that with the advance of endovascular technologies, the vascular surgeon would become an expensive, redundant luxury easily replaced by the overlapping skillset of radiologists, cardiologists, general surgeons, trauma surgeons, cardiac surgeons, nephrologists, neurosurgeons, neurologists, podiatrists, infectious disease, and wound care specialists. When I identify these zebras, these rare diagnoses, I am neither replacing all those aforementioned specialties, nor having special insight unavailable to the uninitiated. I am keeping my eyes open. In a non-smoking, active, otherwise healthy and employed middle aged man with no cardiac history, it is very strange to have isolated popliteal occlusion with otherwise pristine arteries throughout the rest of the CT scan. That is a statistical outlier. People who occlude blood vessels in this fashion usually have more comorbidities, usually are older, and usually have more atherosclerotic disease burden. While not quite like the teenager who presented last year with the same diagnosis (after a month of misdiagnosis and delayed treatment), the cleanliness of the arteries elsewhere in the body was disturbing to me. This puts me on a zebra hunt and not the usual horse roundup.
A hospital needs vascular surgeons in the way that America need the US Marine Corps. Every decade, there is some congressional movement to see how the USMC, which has fighter jets, tanks, planes, aircraft carriers, helicopters, and riflemen, can be phased out because it seems to duplicate the services of the Navy, Air Force, and Army, and every generation a conflict proves these arguments wrong. Individuals who know things broadly and deeply, who can do many things across specialty lines, work from head to toe, and whose specialty is to customize solutions to complex problems is the special quality that is the difference between tertiary hospitals and quaternary hospitals. While these qualities are goals within Vascular Surgery, it is a generalizable goal for anyone working in healthcare. My favorite professor in medical school was Dr. Harold Neu, chair of infectious diseases at P&S. He knew everything and was interested in everything and took every moment in the hospital to increase his knowledge a little more. That’s how and why I diagnosed a case of schistosomiasis earlier this year -the upper abdominal pain was not from a coincidental aortic aneurysm, but the fellow did swim in the Nile.
I texted Dr. Sean Lyden, my former boss and partner at the Cleveland Clinic main campus, if there was any situation where an asymptomatic popliteal entrapment who had gone over 50 years of life without complications could just be watched -it was a question from the patient actually. Dr. Lyden treats popliteal entrapment weekly and maintains a clinic specializing in popliteal artery entrapment (link). One of advantages of working in vascular is that the community is small and highly accessible, and I have a group of living textbooks on speed dial (that term pegs me as antique). There is an active social network of vascular specialists and the SVS maintains SVS Connect (link) for posting and discussing difficult questions. Despite the horrible hour that he received the text (“What’s the matter? Are you in trouble?” he asked) because of the time differences between Abu Dhabi and Cleveland, he answered, “no.” Sorry, Sean, for texting you at 4 in the morning.
When you look for four leaf clovers, and you have never seen one in your life, the moment you find one must be transformative. I have never found one, but I keep my eyes open, lest I trod on one.
Mid Century Modern is a design philosophy from the mid twentieth century that seemed terribly dated and out of style while I was growing up but now seems to have come back as people dig around their parents and grandparents’ stuff. Television shows like Mad Men and Marvelous Mrs. Maisel are rotten with mid-century design. Yet it is an apt term for vascular surgeons of a certain generation like me who at about fifty years of age remember a time when vascular surgery was about big incisions and bypass grafts. We were trained in open vascular surgery and rode along with (or were drowned by) the tsunami of endovascular techniques that have come to dominate. Most of us learned to do them as well. Mid-century vascular surgeons straddle the divide between our mentors who, like me, specialized in vascular after completing general surgery training and the current trainees who have trained solely in vascular surgery. At one time it was fashionable to believe that we were fossils. But, like the coelacanth discovered after an eon’s absence, guidelines and recommendations are being made for open surgery which is supposed to be making a comeback. But it turns out, open surgery-capable vascular surgeons are, like the coelacanth, rare, and endangered. Unless we completely change the way we train people today, open vascular surgery will become extinct. At first glance, it does not look good.
The Dinosaur
My first ever encounter with a vascular surgeon was in 1989, as a lab tech in Boston the year after I graduated from college. It was at the West Roxbury VA Hospital, and like the vets, this one chain smoked in his office. Friendly enough, but a bit aloof, he rasped out well elocuted English in the same way soldiers did in old war movies like The Longest Day. Laconic and Robert Mitchum-like. He would have been among the first generations of vascular surgeons, contemporary to Jack Wylie, Michael DeBakey, and other luminaries. He couldn’t have cared less, I believe, as he performed fem-pop and aortobi-iliac and femoral bypasses and carotid endarterectomies with a furious incandescence that didn’t jibe with his reserved demeanor outside the OR. He was equally fierce to the residents when he had to scrub in to get them out of jam. But he was kind to the medical students and pre-meds like me. His type of surgeon is most definitely extinct, remembered only in old war stories like this.
What is it about my generation of surgeons? We remember things and balance the new against the old ways. We remember a time before work hours restrictions but are young enough to understand why it is not too healthy to work 120 hours a week. Yet we are also conflicted about the benefits we retained from that kind of training, now viewed with about as much approval as Sparta’s agoge system of child abuse and military training. I trained at the outset of laparoscopic surgery, so I did about 50 open cholecystectomies before learning how to do laparoscopic cholecystectomies. Most of my appendectomies were done open. As were my colectomies, gastrectomies, thyroidectomies, mastectomies, and yes, aortic surgeries, carotid endarterectomies, arteriovenous fistulae, and leg bypasses. And I did them.
We All Agreed…
This was the deal. You worked at 110%, fell exhausted and gave a little more, and you were rewarded. That meant being up all night on call, but after morning rounds, you could turn your pager off and operate all day. If you were learning, you had to be prepared by knowing the patient, the disease, the anatomy, and the operation. If you were teaching, you had to have the approval of the attending who would be somewhere nearby, and never happy if you grabbed them. If you were chief resident, you were basically junior staff and expected to run your service like a practice. The leash was longer for those who could, and short for those who could not. In the grade before mine, it was pyramidal, meaning there was attrition of those who could not progress. Like ringing the bell at Navy SEAL school in Coronado, people quit. Or were, rarely, fired. Being categorical was seen as a kind of entitlement by the disbelieving chiefs welcoming the new categorical interns. Dishonesty was the worst sin, but weakness, like showing fatigue or expressing a desire to have a life outside of work, was equally bad. And training was long. Four years of medical school, followed by five years of general surgery residency with mine extended by a year of research between third and fourth year, and then followed by a two-year vascular fellowship. By the time I was a full-fledged vascular surgeon, I had college friends who had actual homes and summer homes, children, divorces, and travels around the world. They had lived real adult lives. I started out on life at 35 where everyone else had done it at 21. But I had 1600 cases in my residency, of which over 300 were major vascular including 50 open aortic cases, and nearly 500 cases during my fellowship, adding another 100 aortic cases, most of them open, as it was the first years that EVAR was introduced. Nothing better in the world than to start a case with Ken Cherry quipping over your shoulder -“make me proud.” I finished my endovascular training apprenticed to Dan Clair during my first staff job at Columbia P&S -cue Dan intoning “you’re killing me” over the Cath Lab’s PA from the control desk on the weekends we had time in there.
There is no going back…
That represented one way of training a vascular surgeon. Even after graduating, I never stopped learning and perfecting my craft. The two years at Columbia gave me insight on how to run a practice completely alone -I was the lone vascular surgeon up at the Allen Pavilion on the northern tip of Manhattan next to Baker’s Field. It taught me the critical importance of availability and extracting useful information over my tiny flip phone. During my private practice years in Iowa, I learned the amazing productivity that can be attained when you work in collaboration and partnership with cardiologists and cardiac surgeons -something I do today here in the Heart and Vascular Institute. I also learned how to use vascular technologists and the lab as a force multiplier. And it was during the Iowa years that I underwent a period of endo-enthusiasm followed by a realism and I performed over a hundred aorto-bifemoral bypasses on middle aged patients with an average length of stay of 3 days, no deaths. When I plunged back into academia, taking a position at Cleveland Clinic, I was apprenticed again to Dan, but this time in understanding how to use the whole clinic as a tool for taking impossibly challenging patients through to an acceptable resolution. All of that started with those frantic days on call as an intern at St. Luke’s Hospital, drawing blood cultures, placing IV’s, babysitting traumas in the CT scanner, and putting chest tubes into the perforated. But there is no going back. It is most definitely probably illegal today to subject people to the intensity and duration of experience that I went through. And I wouldn’t trade that experience for all the treasure in the world (although I do regret not buying Apple, Dell, and Microsoft in 1994).
What a completely trained vascular surgeon can do
The hardest case that I have taken care of ever was at the Clinic a couple of years ago. The patient was a middle aged man who had ruptured an aortic aneurysm in another state some months prior and had undergone a repair complicated by a pancreatic injury along with some enterotomies resulting in a graft infection along with high output pancreatic and enteric fistulae from an open abdomen. He arrived cachectic, in septic shock and had a pseudoaneurysm from the distal anastomosis of a short tube graft. I immediately took him to the OR to place a stent graft across the pseudoaneurysm neck to prevent rupture and placed him on TPN to correct his cachexia. The abscesses and hematomata were drained percutaneously, and an effort was made to control the fistula with a heroic effort on the part of the ostomy team. He turned around and was able go to an LTAC on TPN and antibiotics. There he gained twenty pounds and returned flush and active. Stage two was three months later and done to replace the still infected grafts with cryopreserved homograft. I did this via a right retroperitoneal approach as the left side and abdomen were a mess from the inflammation. After I removed the grafts and sewed in the homograft, general surgery reorganized his bowel and discovered that he only had about 30cm of useable small bowel and would be on TPN for life. But he was alive and learning to walk again, and eventually came back 6 months later for follow-up and gave me a hug.
That case took all of my skill to solve, and I could not have done it without the whole hospital working in sync with me. When it comes my time, I wonder who would be able to do that for me?Who would manage my ruptured AAA properly and not have bowel and pancreatic injuries?
How to do a CABG according to Dr. Swistel
When I was an intern, I wanted to be a cardiac surgeon more than anything else, and got myself slotted for 6 months of cardiac during my second year. It was an unwanted rotation because of the 5am to 11pm hours, all nighters in the unit on call, and because the CT surgeons were notorious for not letting you do anything, except for Dan Swistel. Years before he had been one of us, a resident at St. Luke’s/Roosevelt and was Dr. George Green’s protege. He had a deal with us where he had you learn and master all the following steps in this order:
1. take vein
2. put in pacing wires and chest tubes
3. close chest
4. open chest
5. open the pericardium and set up the way he wanted
6. put the venous cannulas in
7. put the arterial cannulas and secondary lines in and go on bypass
8. decannulate and repair
9. dissect the aorta, set up and place the cross clamp
10. do the proximal anastomosis on the vein grafts
11. do the distal anastomosis on the vein grafts under the microscope which was the way he and Dr. Green did it.
12. dry up…really dry up and learn to come off pump
13. take mammary
14. book a ward service CABG and do it skin to skin
Through the history of St. Luke’s up to that point, most residents never got past taking vein. That was the great barrier, and most people really didn’t stick around after taking vein and closing the leg. They did not see the point of standing around and second or third assist. Those residents who were going to Cardiac did make it to taking the mammary, but only a handful by chief year. No one made it to 14. Dr. Swistel was always true to his word, even though some residents suspected this was all some bet that he had between himself and his brother who was not a cardiac surgeon -something about I can train a monkey to do this. To me, that last step, doing a CABG skin to skin, seemed like the final level of a very difficult computer game, like casting the One Ring into the volcano, like blowing up Agent Smith.
Every step on the ladder was something I immediately applied to my general surgery experience. On call and at home, I practiced. I practiced holding the instruments correctly and performing anastomoses on discarded grafts. I learned that every hard operation is made up of small technically feasible components, so I worked to make those moves natural and smooth. I progressed rapidly up the ladder and was by the end of my last cardiac rotation firmly at 13 on more than one occasion. Every other part of my skill set expanded during this time -central lines went smoothly, appendices and gall bladders were fished out efficiently, and fear shifted its focus to different things from what made me anxious as an intern. I learned the skill of keeping people alive through the night and making the call to take people back.
With some social engineering (ordering the cardiology fellows takeout Chinese) and vacation days traded, I got to that last step during my third year. If not a monkey, then at least Park. The act of learning and mastering each component skill lets you start and finish an operation. I don’t think Dr. Swistel was ever out to lunch while I was operating, but all those moments of letting me take the knife was crucial to my education and I am grateful to him and all my teachers, including my current partners and colleagues, as I approach PGY-25. As surgical educators, we must recognize that surgery at the sharp end of the knife is a precision craft that has to be taught much as tennis is taught starting with grip, stance, swing. That golf is learned on a driving range with a bucket of balls.
The Mid-Century Vascular Surgeon
Like Mid-Century Modern Design furniture, surgeons in my cohort are sought after by hospitals and practices for being able to let a hospital do more. What do I mean? A urologist resecting a kidney with a renal vein tumor thrombus extending into the inferior vena cava needs to have someone expose, extract, and repair the vena cava. A gynecologist debulking retroperitoneal metastases needs to be able to call for help when part of the aorta needs to go with the tumor. Cardiac surgeons need to be able to place ECMO cannulas in imaginative locations and not lose extremities in the process. A thoracic surgeon resecting a Pancoast tumor needs a vascular surgeon to repair the subclavian artery and vein. An orthopedic surgeon resecting a spindle cell tumor from the thigh needs help reconstructing the femoral artery and vein. And so on. We are safety net, the fire brigade, the SEAL team, and unfortunately many hospitals understand only when their last fully trained, full service vascular surgeon retires.
Vascular surgeons are a keystone species in a hospital’s ecosystem. When wolves were reintroduced to Yellowstone, it was noticed that decades later the forests returned to their ancient glory, that wetlands flourished breeding fish and insects and small mammal species, and the secondary predators that feed on them, and many missing bird species returned. Vascular surgeons capable of operating on the whole body as well as intervening on the whole body are increasingly a missing element in a hospital. And many of us chose to go missing -into our private endovascular suites and vein centers because it often does not pay to go do a 5-hour bypass when you can do three femoral angioplasties for claudication in the same time. Reading 10 carotid ultrasounds is easier on the back and more renumerative than a carotid endarterectomy. And I am not judging -it is a rational choice that is framed by the way healthcare is reimbursed.
The solution starts in the US with a shift in reimbursement to recognize the time and effort required to perform open vascular surgery well and to reward the programs and surgeons who are consistently good. Training in open vascular surgery will be sought after much as everyone wanted to be a cardiac surgeon back in the 1970’s. Government and society mandates set the menu, but the economics determine what is served.
And finally, every year thousands of surgeon-years of experience is retiring with the very skills that are now sought after. Rather than lose this human capital to golf courses and beaches, we should be grabbing them at the door. Like those mid-century chairs and tables, we have always been there somewhere, and its time to make some more.
It was only last month when I came across a post of an aortic aneurysm in a difficult spot (link) and I couldn’t help chiming in some comments. Reading it now, I sound insufferable, because I wrote,
“Depends on etiology and patient risk stratification. Also assuming aneurysm goes to level of SMA and right renal artery origins and involves side opposite celiac. Options depending on resources of your institute: 1.Open repair with cannulation for left heart bypass and/or circulatory arrest 2.Open debranching of common hepatic, SMA, R. Renal from infrarenal inflow and then TEVAR 3.FEVAR from custom graft from manufacturer on protocol 4.Parallel grafting to CA, SMA, R. RA with TEVAR 5.Surgeon modified FEVAR 6.Open Repair We would have a multidisciplinary huddle around this patient -Vascular, Cardiac Surgery, Cardiology, Anesthesia, and ID (if needed) to help choose. Be ready to refer to a center with more resources -including prepping patient for transfer and imaging -including uploading images to the cloud for transfer with patient’s permission. More info please”
More Info Please, Indeed
The post I commented on was of a saccular aneurysm in the transdiagphragmatic segment of aorta. Ironically, only a few weeks later, I got called from hospital transfer center about a patient with a leaking aortic aneurysm, a type V thoracoabdominal aortic aneurysm as it turned out, from an outside hospital, needing urgent attention, and we accepted in transfer based on the conversation I had with the tranferring physician. And that was the problem -usually in taking these inter-hospital transfers, you have to pray that the precious CT scans come along with the patient burned correctly onto a CD-ROM. You can buy and watch a movie in 4K resolution over the internet -about 4 gigabytes, but a patient’s CT scan which is about 200 megabytes -because of various self imposed limits, overly restrictive interpretations of laws, and lack of computer skills, these life saving images get transferred on CD in 2019. That last time I purchased a CD for anything was over 15 years ago.
An Interested Party
The technical solution –to use the internet to transfer critical life saving information between hospitals – came about when our IT folks took an interest in my quarterly complaint email about using the newfangled internet for sharing files. After mulling various solutions ranging from setting up a server to using commercial cloud solutoins, we came upon the compromise of using our internal cloud with an invitation sent to the outside hospital. I would send this invitation to upload the DICOM folder of the CD-ROM to an outisde email address. It was simple and as yet untried until this night. “Would the patient agree to have his CT scan information transmitted to us electronically?” I asked the other physician. He assured me that the patient was in agreement.
It Takes Two to Tango
Of course, being able to transfer these pictures requires a willing partner on the other side, and the referring physician made it clear he did not have the technical expertise to do so. It took a bit of social engineering to think about who would have that ability. Basically, aside from myself, who spend all their time in dark rooms in the hospital in front of giant computer monitors? The radiologists! I got through to the radiologist who had interpreted the report and explained the simple thing I needed. Gratefully, he agreed, and I sent him a link to our cloud server. I explained to him, “When you receive this, clicking the link opens a browser window and then you open the CD-ROM and find the DICOM folder and drag and drop it on the browser window.” The 200-500 megabytes of data then get sent in electronic form, as it was meant to in 2019.
The Internet Saves a Life
The brutal truth is that in locking down a computer system, many hospitals make it impossible to even load an outside CD-ROM, creating many self imposed barriers to care. Thankfully, at CCAD, we were able to work together to find a secure solution. With the CTA on our servers, I was able to review the study within 15 minutes of accepting the patient, and arrange for the right team to be assembled, and confirm that we had the right material (stent grafts) for treating the patient. When the patient arrived, OR was ready to go, saving hours of time that normally would have been required if the CT scan had to be reviewed from the CD-ROM that came with the patient. Sometimes, the CD-ROM does not come, and in a critical situation, the CTA has to be repeated with some risk to the patient for complications of the contrast and radiation.
What to Do
The patient had a 8cm sphere shaped aneurysm arising in the transdiagphragmatic aorta, leaking into the right pleural cavity.
The patient was otherwise a healthy middle aged man with risk factors of smoking and hypertension. The centerline reconstructions showed the thoracic aorta above the aneurysm to be around 20mm in diameter and same below, with the celiac axis and superior mesenteric artery in the potential seal zone of a stent graft. The only plaque seen was around the level of the renal arteries and was focal and calcified. Looking at the list I had made as a comment to the Linked-In post, I realized that I really only had one viable option.
Open repair, usually the most expeditious option, was made challenging by the right hemothorax, making a left thoracotomy hazardous if the lung had to be deflated. Cardiopulmonary bypass would have to be arranged for, and that adds a metabolic hit that greatly raises the stakes. Of the endovascular solutions, the only viable option was TEVAR to exclude the rupture and debranching of the celiac axis and superior mesenteric artery. To those who would advocate for parallel grafts, there was no room in the normal 20mm diameter aorta. And branch systems for rupture are some time in the future. Also, the patient was becoming hypotensive. So the planned operation was first TEVAR to stop the bleeding, and then open surgical debranching. A hybrid repair.
The smallest stent graft we have is a 21mm graft, but it would not be suitable for this aorta. In practice, the normal aorta is quite elastic and will dilate much more than what is captured on a CTA. The next size we have is 28mm graft and I chose this to exclude the rupture, which was done percutaneously.
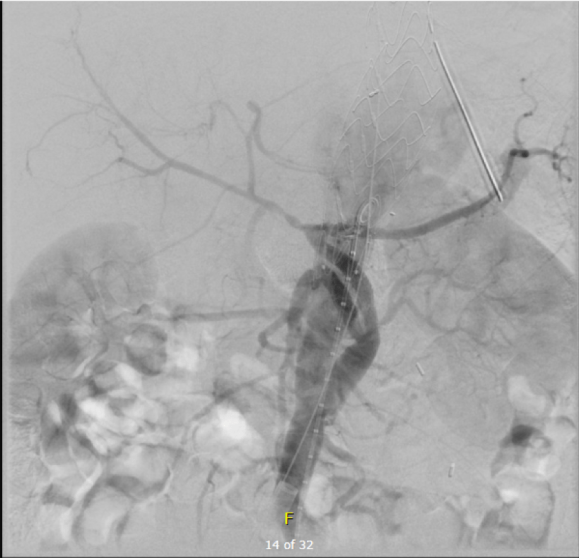
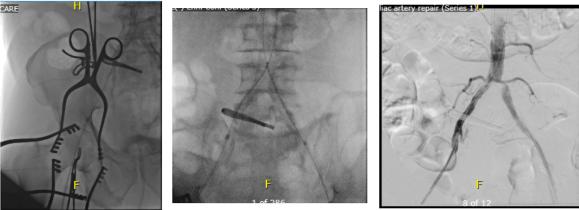
As seen below, the graft excluded the celiac and SMA. Late in the phase of the final aortogram (second panel) there was an endoleak that persisteed despite multiple ballooning. The timing suggested the intercostals and phrenic vessels contributed to a type II endoleak, but it was concerning.
Find the Endoleak
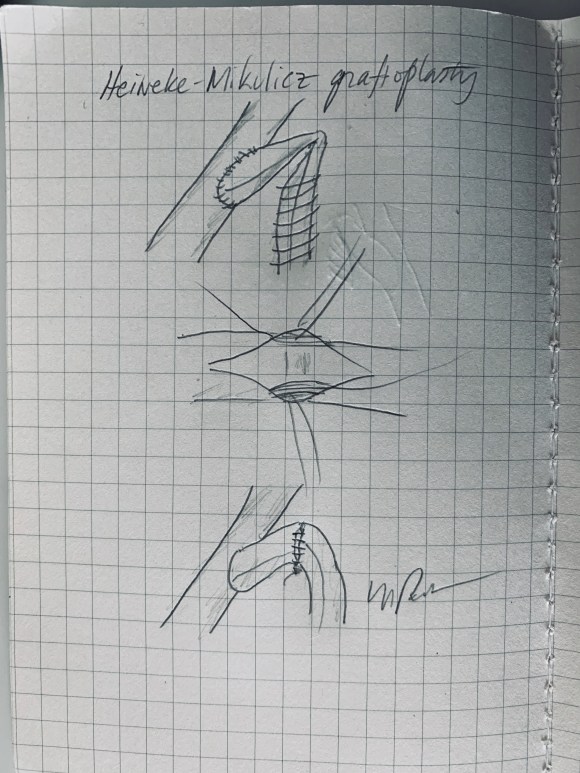
The bypasses were sent from the infrarenal aorta to the common hepatic artery and the SMA close to its origin, and the origins of the celiac axis and SMA were clipped. The bypasses were then done with a 10x8mm bifurcate Dacron graft originally for axillofemoral bypassing. It had spiral rings which I removed at the anastomosis and this resulted in a kink at the closer bypass. Usually, I loop this for iliomesenteric bypass but there was not enough distance from the infrarenal aorta. I have to add a little trick I modified from my pediatric surgery experience as a resident -a Heinecke-Mikulwicz graftoplasty:
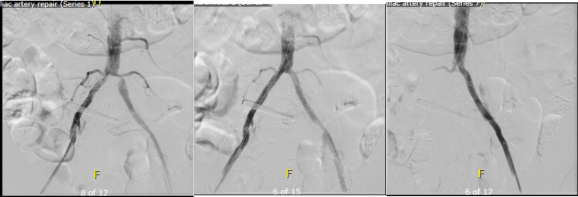
This worked to relieve the kink as evidenced on the aortogram above. After closing the laparotomy, I placed a chest tube in the right chest. The patient had a course prolonged by a classic systemic inflammatory response syndrome, with fevers, chills, and leukocytosis. He bled for a while but stopped with correction of his coagulopathy. All blood cultures were negative, but a CT scan was performed out of concern for the endoleak, and the possibility of continued bleeding.
No endoleak was detected as the sac was fully thrombosed. There was a consolidation of the blood in the right chest, but it resolved with fibrinolytic therapy.
Discussion
This case illustrates several points I have been making on this blog.
Hybrid repairs are not some kind of compromise but the full realization of a complete skill set. When students ask me how to judge a training program, one of the best metrics is how frequently are hybrid operations performed. It means either the endovascularist and open surgical operator are in complete synchrony or there are individual surgeons competent in both open and endovascular surgery. Hybrid operations, rather than being a compromise, are an optimization.
Time -Laying the stent graft across the celiac and SMA origins starts a warm ischemia clock. The liver and intestines, in my reckoning, should be able to tolerate the 2 hours of work to get the bypasses working. Cardiopulmonary bypass may give you less ichemia but at the metabolic cost of the pump time. These negative factors add up, but were surmounted by the fact that early control of hemorrhage was achieved. Stopping the bleeding and restoring flow are the core functions of vascular surgery.
Planning and preparation. The ability to see the CT images and prepare the teams and materiel before the patient transferred was lifesaving. This is where our IT gets credit for responding to a critical need and formulating a solution that meets internal policies, external regulations, and saves a life. It illustrates so many opportunities particularly with electronic medical records and their processes which focus more on documentation for billing. A discharge summary should be multimedia like this blog post and it should be normal and easy to generate. And finally, as clinicians, we should mind technology with as much attention as we give to the latest medical devices and techniques.
The patient is a man over 70 years of age who came to the hospital with severe pain of his right foot and leg with walking short distances and at night while recumbent. He had a history of hypertension, diabetes, and coronary artery disease, and several years ago had his left common iliac artery stented. On examination, he had no lesions of his foot, and his pulses were only palpable (barely) in the femoral arteries only. He did have strong monophasic signals in the anterior tibial arteries bilaterally.
Initial vascular lab testing showed only mildly depressed ankle brachial (above), with dampened waveforms consistent with inflow and femoropopliteal disease on the right. He underwent arteriography by our vascular medicine specialist and cardiologist Dr. Faisal Hasan, and it showed bilateral common iliac stenoses, a severely calcified and nearly occlusive plaque in the right common femoral artery, and a long segment occlusion in the superficial femoral artery with diffuse calcified plaque extending into the popliteal artery. There was diseased but patent 3 vessel tibial runoff.
To Act As A Unit are the Cleveland Clinic’s words and it shows the Clinic’s roots as an US Army field hospital on the vasty fields of World War I France a little over a century ago, and we take it seriously. It may come as a surprise to some that a cardiologist referred me this patient after mutually deciding that the common femoral disease and the TASC D SFA occlusive disease, but we both decided that a surgical approach was the best one. The question then is how much more flow?
I ordered a CTA (CT angiogram) particularly for endarterectomies as I find it imperative to know the actual end point of plaque. Arteriography only hints at it, and while a 5mm lumen may look large and patent, it may be a channel in a 10mm wide plaque that when a stent terminates within it, breaks and becomes biologically active as intimal hyperplasia at best or embolizes at worst. CTA shown below revealed the plaque where contrast angio showed only the lumena of the vessels.
The 3D reconstruction function also allowed me to see and plan the operative approach and predict the lack of saphenous vein confirmed on duplex ultrasound.
For the students reading this, ischemic rest pain is often simpler to treat because it requires only a little more blood flow. There is a neurologic ischemia component that is not well studied, particularly in diabetics, as ischemia may result in anesthesia in someone who has underlying diabetic neuropathy, but that is not an indication for revascularization while rest pain is, and someone should investigate this. This little more blood flow in the form of treating inflow disease only may be sufficient in relieving rest pain while avoiding interventions on the superficial femoral, popliteal and tibial arteries which have limited longevity.
The common femoral artery on the other hand is the throttle of inflow and as a principle, inflow can be considered as the infrarenal aorta to profunda femoral artery, and repairing the common femoral necessitates an operation. There is no durable or laudable endovascular procedure for occlusive disease of the common femoral artery, a feature shared with the subclavian artery at the thoracic outlet and the celiac axis at the median arcuate ligament. All three are externally compressed by hard structures and revascularization must be ever mindful of the inguinal ligament, the thoracic outlet, and median arcuate ligament. The only exception to the “you must operate” rule of the CFA is calcified atherosclerotic disease in high risk individuals, and I make careful exception here with rotational atherectomy devices.
Claudication is another thing entirely. Claudication limits lifestyle and can be corrected by changing lifestyle -either with more exercise or limiting exercise. The thing is, when a patient has reached a certain age, that lifestyle may be walking slowly from chair to commode, and if that activity is limited, no amount of haranguing may be able to induce that person to embark on an ambitious exercise program. Sometimes, you have to be realistic about telling a frail old man to go for a 60 minute walk. But if that person has difficulty getting to the bathroom because of leg cramps, then either they have to get assistance or more bloodflow, and ironically, a little more blood flow represented by improving inflow, may not be enough.
That was what I was thinking when I was planning this operation. Improve the inflow with stents to the common iliacs and a right CFA endarterectomy, but use the opportunity of surgical exposure to extend the endarterectomy to the distal external iliac and through the entire SFA.
My fondness of remote endarterectomy is well known from my many blog posts on it (link). It is a modern update on a very old procedure -the ring endarterectomy, done since the middle of the last century when bypass grafts were unavailable. The occlusive plaque is removed, and an end-point reached and cut with a scissor like device (available from LeMaitre). It is the ultimate hybrid operation (below) requiring open and endovascular skills. I tell prospective trainees to judge training programs by how facile are the surgeons and how many are the procedures with and involving a hybrid approach, because any program can have few (getting fewer) old surgeons doing only open surgery and a lot of young surgeons doing only endovascular procedures, but a rare few will do a lot of hybrid procedures.
I chose to add femoral EndoRE. This would bring the extra blood flow needed to kickstart any walking program, barring cardiopulmonary limitations.
The patient was brought to our hybrid operating theatre and prepped from nipples to toes. The right common femoral artery was exposed for endarterectomy, and accessed then with a sheath along with a left femoral sheath for kissing balloon angioplasty and stenting of the common iliac artery stenoses (below).
Afterword, the CFA was opened and endarterectomized, and the SFA was remote endarterectomized (below).
The endpoint was chosen in the above knee popliteal artery to avoid having to stent the dissected end point plaque well into the popliteal artery. If I wanted to go all the way to the below knee popliteal artery, I would have to open it to manage the plaque and artery at the so-called trifurcation, typically with a patch angioplasty. The plaque came out in one piece (below):
The terminus of the plaque in the POP where it was cut has to be managed with a stent, unless you open and complete the endarterectomy and patch the artery. I was able to cross the dissection (no small feat) and plaque a stent. The artery was widely patent and even the small branches off the previously occluded SFA were now reopened.
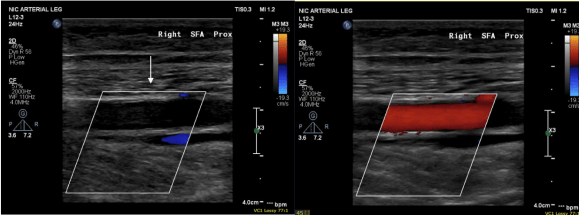
His pulse volume recording done after intervention reflects the improved flows (below).
His rest pain resolved, but more gratifyingly, he has regained the confidence to walk and exercise, which he now does without limitation up to 45 minutes a day. In two month followup, we performed a duplex which showed his right SFA to be basically normal (below), including an intimal stripe and media. This is not an anomaly. When I took a punch out of restored artery to perform an anastomosis (from this case link), I sent it. Previously it had been an artery that was obstructed for nearly a decade, but after EndoRE, had become an elastic, compliant vessel. The pathology returned as “normal artery.”
When these fail, they typically do so a random points on the endarterectomized vessel and on the stent. While stent grafting may have better outcomes with regard to restenosis, doing so covers collateral vessels and PTFE grafts behave poorly by embolizing while clotting off, and PTFE stent grafts are no different. Data from over a decade ago suggests that EndoRE of the SFA while inferior in patency to vein grafts, are equivalent to PTFE [reference 1] and superior to endovascular revascularization [reference 2] in terms of primary patency. When they occlude, they achieve a “soft landing” without the furious acute ischemia and embolization seen with PTFE bypasses.
I think these handful of cases I performed here in the UAE represent the first in the region. The main difference here is that the arteries tend to be smaller by about 20%, and in one instance, the smallest Vollmer ring was too large for the vessel in a case where I abandoned the SFA revascularization -the profunda and inflow revascularization proved sufficient in reversing rest pain. The intriguing property of endarterectomy is something that we all try to do with surgery but rarely achieve -a restoration to an earlier time. I believe this patient’s right femoral artery is now back to a youthful state.
Recently, I saw a case presentation uploaded to LinkedIn of a subclavian venous stenosis treated with balloon venoplasty and a stent for venous congestion of the arm. The images were beautifully clear. The stenosis was at the thoracic outlet. The comments were generally favorable, including congratulations for a nice case, but I had to put in my two cents: The thoracic outlet is a terrible place for a stent due to external compression, and once occluded, a stent in the venous position is a permanent obstruction. The justification was that the patient did not want surgery and there were no surgeons who did first rib resections where the post author worked. I refrained from commenting something about primum non nocere.
This patient from the images above is a middle aged man who competes in triathalons and who noted sudden onset of discomfort and heaviness and pain in his left arm. Ultrasound revealed DVT in his axillosubclavian veins extending into his brachial veins and he was started on anticoagulation. He had been on anticoagulation for about a month by the time he came to my clinic. On examination, he had a prominent superficial veins on his shoulder, but otherwise had a normal examination. He did not have arterial obstruction on TOS (thoracic outlet syndrome) maneuvers and had no neurologic symptoms. I recommended first rib resection.
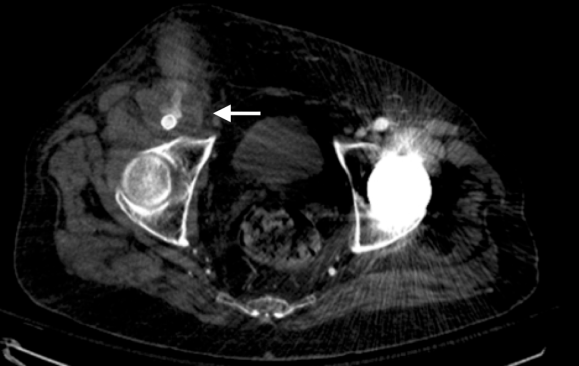
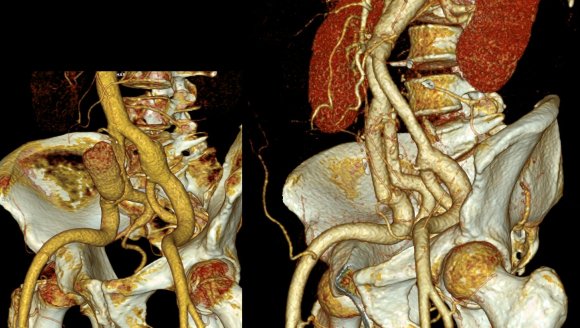
The patient’s first reaction was a dubious expression. After all, in this day and age, isn’t it barbaric to offer to cut out a rib? Why not put a stent there? A CT venogram was obtained showing the subclavian vein occlusion, but we knew that. I use the 3D surface reconstructions extensively as a visual map to determine surgical approach. I remove first ribs through both supraclavicular and transaxillary approaches, choosing one or the other.
The 3D reconstruction of the bones showed that to get to the first rib section underlying the vein, it was best approached via a transaxillary approach. The arrow in the image shows the flare in the first rib where the anterior scalene muscle attaches. Adding muscle shows that in this well muscled patient, getting to the first rib would be a challenge -for the people holding the retractors.
The operation is done with the patient in right lateral decubitus position and requires deep retraction and good lighting -I have played with using the laparoscope (more to come). Laparoscopic instruments such as the Maryland tipped ligasure and hook cautery get much use in this operation. The special sauce to getting this done quickly here in Abu Dhabi where I don’t have the army of residents and fellows is getting my colleagues in Orthopedic spine (Dr. Nader Hebela) and Thoracic Surgery (Dr. Redha Souilamas) interested in TOS.
Where I would laboriously chew through the ribs with a Kerrison, Dr. Hebela has shown me the high art of the hammer and chisel (notice the clean lines on the cut rib below). Dr. Souilamas has seeded the idea of doing this entirely thoracoscopically from the thoracic cavity, and yes, it is right there to see when I recently visited one of his operations -where is that cadaver lab when you need one? Enough rib was resected to ensure the vein, artery, and plexus were completely free.
A bit of anterior scalene came out with the specimen, splayed upwards in this image
The patient did well, recovering much of his range of motion quickly with the help of physical therapy. He was taken to the angio suite and underwent venography shown below. There is an occlusion of the subclavian with outflow via collateral veins. Not seeing collaterals is as important as seeing a good angiographic result.
Venoplasty was done to 8mm -I try not be overly aggressive here, just to break the strictures that caused the balloon to have a waist in two sections. The final result is below, with the absence of the venous collaterals. If they were still present despite an angiographically satisfactory result, I would perform IVUS to see what the problem was. In no circumstances would I place a stent at this juncture -my plan is to keep the patient on anticoagulation for 3 more months.
First rib resection should be in the armamentarium of every vascular surgeon. I sense a rise in the diagnosis of this and this has been commented on the SVSConnect boards (link), possibly from a greater awareness of the signs and symptoms of the diseases associated with the thoracic outlet. Since coming to CCAD, there have been enough cases for it to become a routine which I did not expect.
The thoracic outlet, like the median arcuate ligament and the inguinal ligament, cause trouble for stents.
Looking at the thoracic outlet (above), the vein has a particularly narrow outlet under the hinge of clavicle and rib. I generally find it tragic to see a stent here because it limits the possibility of improvement with rib resection. Like the median arcuate ligament for the celiac axis and the inguinal ligament for the common femoral artery, stents get crushed in this position. If you think about it, it is probably our insistence on bipedalism that engendered these design flaws. Stents get compressed by the weight of the shoulder and arm (thoracic outlet), the mediastinum (median arcuate ligament), and the abdominal cavity organs (inguinal ligament) under these choke points, something the quadruped does not suffer.
Quadrupeds that come to mind, RIP GOT.
So is it barbaric, this open surgery? No. The barbarism is in offering patients an easy solution that will get that patient out the door happy, but not knowing (at best) or not caring (at worst) that the biomechanics do not favor any kind of durability.
From Dr. Dmitirios Virvilis, formerly my trainee, now my colleague, who had this interesting case of end-stage iatrogenic pseudoaneurysm.
History
85-year-old gentleman with history of atrial fibrillation on anticoagulation, mechanical valve on Coumadin presented to our emergency department with significant hemorrhaging from the right groin (figure above). The patient had a coronary angiogram 2 months earlier done elsewhere complicated by a pseudoaneurysm which was managed with ultrasound guided thrombin injection that was not successful. Patient was sent to a vascular surgeon at another facility and the decision was made to intervene with the placement of a covered stent on the common femoral artery (possibly due to high patient risk?) compromising the junction of the SFA and profunda artery. The patient developed a large hematoma following placement of the covered stent and was managed solely with antibiotics for over a month prior to presentation.
On physical examination, the patient was septic, lethargic with grossly infected groin (image above). A CT scan with contrast was performed which showed active extravasation with stranding around the femoral vessels (below).
The patient was taken emergently into the operating room. Due to the extent of the infection under the inguinal ligament I obtained proximal control by performing a retroperitoneal flank incision. The iliac vessels were controlled and then I proceed with exploration of the hematoma. The junction of the superficial femoral artery and the profunda artery was separated and the common femoral artery was liquefied. There was only a very thin posterior layer of the common femoral artery and the cover stent was floating in the hematoma. The wound was thoroughly debrided. The distal external iliac artery was transected and the stent was removed. The junction of the superficial femoral artery and profunda artery were separated. A Rifampin soaked graft was used (picture below), which was an 8mm gelatin impregnated Dacron graft soaked in Rifampin (600mg in 200mL of saline) for 20 minutes.
The graft was anastomosed to the common iliac artery to fully exclude the external iliac artery which was debrided and ligated. The profunda artery was reimplanted on the side of the graft in an end-to-side fashion. After the wound was thoroughly irrigated and the graft was covered . The muscle flap was created in the usual fashion with lateral mobilization preserving the medial vascular pedicle. The wound was partially approximated and the top of the wound was left open for an application of wound VAC (below). The fact that I am practicing in a remote area has made me to be more efficient and incorporate in my practice many procedures picked up through training that fall under general surgery, plastic surgery, and advanced vascular surgery.
Patient remained hemodynamically stable and recovered in the ICU for 48 hours. After hospital course of approximately 5 days was finally discharged to rehabilitation center. Patient was seen 1 month and 2 months after the first operation and has had completely healed incision (below). There is a strong femoral pulse on the right groin with multiphasic pedal signals. Patient has completed 8 weeks of IV antibiotics. I am planning to perform a CT angio with runoff in the next few months in order to evaluate my distal anastomosis because I am concerned about the Pseudomonas that grew from the OR cultures.
From technical standpoint there is 2 things that I would like to address:
#1: The textbook answer would be to perform a bypass with a native conduit with deep femoral vein or great saphenous vein, but this is difficult to perform efficiently solo. I do not have CryoVein on the shelf and the cost of such a conduit is prohibitive in my institution. And extra-anatomic bypass also on the lateral approach, an obturator bypass, adds time and complexity especially with the separation of profunda and superficialis.
#2 Next time I will have to perform a bypass like that I will probably perform the bypass first to the profunda artery and then reimplant the SFA which is more mobile.
Discussion by W. Michael Park, MD
I have to congratulate Dr. Virvilis on this nice outcome. I agree on remaining vigilant for late re-emergence of infection, but it is very unlikely to occur as time passes without signs and symptoms. I have three things to add. First is that Rifampin soaked graft is effective in revascularizing within a decontaminated field while sewing to uninfected artery. Taking the graft to the common iliac bifurcation which was exposed to gain proximal control was wise as anastomoses to the external iliac under the inguinal ligament are challenging and there was an unknown degree of infection here. Second is the sartorius muscle flap must be in the armamentarium of every vascular surgeon and is an easy jumpoff point to learning gracilis and rectus femoris flaps as well. The lateral mobilization and medial rotation is done preserving the medial arteries that feed the graft -dividing too many of these to mobilize the flap kills the flap. The flap delivers the immune cells and vascularity to clear the remnants of infection and forms a better granulation source bed than debrided, infected wound.
Finally, Dr. Virvilis did reach out to me from around the planet (I work in Abu Dhabi, he in Mississippi) for a run through of his plan. I cannot tell you how valuable this is to be able to bounce ideas off of someone you trust. When I graduated from my fellowship, Tom Bower put his hand on my shoulder and said, “Do not hesitate to call me if you have a difficult situation.” I have since grown a long short-list of mentors, friends, and partners on speed dial. It taps me into cumulative millennia of surgeon-years of experience. With social media and increasing acceptance of its use to share ideas, there is absolutely no reason to work in isolation.
The patient is an active man in his 60’s with a history of hypertension who had known about a right common iliac artery aneurysm for several years and had come for an opinion. He was asymptomatic of pain. He had a prior splenic artery aneurysm embolization about a decade prior to presentation.. CT scan showed a large eccentric aneurysm arising from a retrograde chronic dissection dilating the right common iliac artery to over 4cm. This is typically iatrogenic, but impossible to know for sure. The left common iliac artery was ectatic to 2cm as was the aorta to 3 cm and all were “wavy.” This sort of tortuosity is the result of remodeling in the axis of flow resulting in lengthening of the artery and is found in those with the substrate for aneurysmal degeneration (footnote). He did not smoke and he could climb stairs without dyspnea or chest pain.
On examination, he was a fit middle aged man with a slight paunch. His abdomen was soft and his peripheral pulses were present and normal. Laboratory results were normal, including creatinine. EKG and echocardiogram were also normal.Treatment options were discussed in detail. The patient was paying for the operation himself and wanted to understand in detail the possible options. These included
1. Open aortobi-iliac bypass with a jump bypass to the right internal iliac artery
2. Open aortobi-iliac bypass with ligation of right internal iliac artery
3. EVAR with right external iliac extension after embolization of right internal iliac artery
4. EVAR with parallel grafts to right external and internal iliac artery (off label)
5. EVAR with iliac branched graft to right internal and external iliac artery (off label)
People are known to react with emotions and to decide typically for near term gain over far term benefits. The offer of an operation involving laparotomy and a possible weeklong hospitalization with all the attendant risks of death, heart attack, stroke, ileus, wound infection, pneumonia, organ failure and so on provides a stark contrast to the appeal of endovascular repair which can be done percutaneously, with local anesthesia, and with a short hospital stay. The lifelong CT scans are in the murky future compared to the present which is sharply in focus. This is why few people save for retirement, why profligate grasshoppers far outnumber industrious ants. In the same vein, the offer of an “advanced minimally invasive” solution plays to several cognitive biases that exists in the mind of not only the patient but the health-care provider. These include this preference for short term gain over long term gain, but also viewing all innovation as being necessarily better than what was available.
After going over the operation in great detail, the patient cut me off when I mentioned the need for lifelong followup CT scanning. Because he lives in several countries, typically, he has to pay for his healthcare out of pocket and he balked at the notion of paying for an annual CT scan. He was also disdainful of the possibility of reintervention (quoted at 10%) and having to pay for it. Also, the stent grafts, which he would have to pay for, end up being as costly as a new luxury sedan based on local pricing.
We chose open surgical repair via a midline laparotomy. An aortobi-iliac bypass was performed from proximal aorta to right internal iliac artery and left common iliac artery bifurcation with a jump bypass from the right graft branch to the right external iliac artery. Technically, this sequence was chosen for ease of access to the internal iliac artery with the external clear of graft. Operative time was 3 hours. He was in the ICU for one night. He went home after 10 days after contracting a UTI. In followup three weeks after discharge, because he had fevers, a CT scan was performed (figure). He was treated for an upper respiratory infection which cleared, and he has been doing well since. We are both happy that he will never need a followup CT scan.
Before and After
The literature supports this stance. The long term followup of the EVAR-1 Trial (Reference 1) is an example. This was the late followup of the prospective randomized study looking at open surgery versus EVAR in 1252 patients. The initial EVAR 1 findings are well known and put into question the long term benefits of EVAR as the initial mortality benefit of EVAR is lost within a few years of treatment. At a mean of 12.7 years of followup, there were more deaths from aortic aneurysm rupture and aneurysm related death in the EVAR group compared OPEN surgery (adjusted HR 5.82, p=.0064), with 13 AAA ruptures. I have mentioned before that the failure of a handful of pacemakers drove the Guidant company to recall over 20,000 of their devices. Plus, the cost of annual CT scans in the treatment group and cost of devices and cost of reintervention have driven the UK’s NICE Guidelines recommending against EVAR in elective AAA repair. The meta-analysis of EVAR-1, DREAM, OVER, and ACE trials comprising 2783 patients is confirmatory, that aneurysm related mortality was significantly higher after the initial mortality benefit of EVAR fades away, and that patients of marginal fitness gain no advantage from EVAR, particularly those with heart or renal disease, and those with PAD had lower mortality in the period of 6 months to 4 years (reference 2).
I post this case, because despite a complications, in this case UTI and URI, the patient did fine. So why is open aortic surgery considered a dying art? Why is there such pushback against the UK NICE Guidelines?During my residency in the 1990’s, in the heyday of open surgery, I observed a lot of mediocre vascular surgeons and a very few great ones. The average vascular surgeon would take 6-8 hours to perform open aortic surgery, and the patient would come out with a typical picture of oliguria, third spacing, SIRS, that would generate a 1-2 week stay that would even be described as the normal and expected course for AAA repair in surgical and critical care textbooks. The best surgeons back in the day did these operations under 3 hours with 100mL blood loss and the patients would spend a day in the ICU (often not needing it), and 3-7 days in the hospital, but they were the exception.A higher percentage of surgeons today can do EVAR well than surgeons 25 years ago could perform competent open aortic surgery. Most surgeons graduating from training rarely see or do open aortic surgery compared to the multitude of interventions. Capable open surgery basically is not available outside of a few centers, and most surgeons admit to not having equipoise to start a new trial with modern devices. Open aortic surgery is a lost art, like growing your own vegetables, dressing your own game, reading cursive script, and dialing a rotary telephone.
It is not for a lack of desire. I have several younger colleagues I have met or interacted with via social media who have an intense interest in gaining open vascular skills. They have organized open skills courses at major European vascular meetings, but I believe that is not enough.The need for exovascular fellowship, the running topic of conversation of older surgeons through the 2000’s, is never as critical as it is now as we see milennia of surgeon-years of experience retiring to golf courses and cottages. The recommendation for preferring open surgery in the younger and fitter patients is sadly out of reach for most patients and surgeons. The same passion in disseminating endovascular knowledge needs to be applied to repair the damage to vascular education by over-relying on and over-prescribing endovascular approaches.
Finally, and sadly, this patient is the exception. When given clear options and outcomes and costs, this patient made a rational decision, choosing value over convenience.
Pearls for finding AAA:
1. Tortuosity of the internal carotid arteries including loops and hairpin turns found in patients particularly smokers implies the present of a AAA until proved otherwise
2. Palpating bounding popliteal or pedal pulses in an older smoker implies the presence of a AAA until proved otherwise. Especially if the medical student can feel these pulses.
3. African-American Females with Diabetes almost never get AAA.
4. Palpate their abdomen
Absolute Neutral Position is suprisingly universal
A body floating in space, a fetus in the womb, a dad lounging in his favorite chair, share the feature of weightlessness and represent the absolute neutral position (figure above) of the human which is the position of a relaxed supine quadruped -a dead mouse. Anything else is a stress position, including standing. Repeating motions outside of this relaxed pose or holding those positions away from this absolute neutral for long periods of time is a nidus for injury and pain. That is why most land animals sleep flat on the ground.
The Pain Operations
Operations to relieve pain are often the most gratifying to both patient and surgeon to perform successfully. This circumstance applies to the commonly performed procedures such as spine surgery, endometrial ablations, and varicose vein resections. When the pain is due to a rare set of circumstances, things are not so easy. Typically for rarer pain syndromes, two things need to coincide for the successful operation to happen. First is the patient must suffer while more common and potentially life threatening diseases are ruled out and even treated if these are found. This may take months or years. The second necessary condition is finding a physician who has seen the particular pain syndrome before and understand how to test for it and treat it. That meant the majority of people never get treated, or are shunted into the circle of shame as malingering, drug seeking, and mentally unstable. The opioid epidemic creates double jeopardy for these patients -they can become addicts as their pain is never successfully diagnosed and treated and they get labeled as drug seeking.
A random list of conditions that cause pain that should be on the mind after the usual things are ruled out. Also, vasculitis, autoimmune disorders, and foreign body reactions
All pain syndromes that can be successfully treated share common features that give you a degree of surety about the diagnosis, but at the end, there is a leap of faith on the part of both patient and practitioner because many of these operations have a failure rate ranging from 5-20 percent. First, the symptoms must be associated with sensory nerves, somatic or visceral. Second, there is a physical mechanism for that nerve to be inflamed from compression, swelling, or irritation that can be accounted for through history, physical examination, and imaging studies. Third, though not a constant, a major nerve trunk will be associated with a blood vessel, typically and artery, that is also affected by compression. Fourth, when swollen veins are the cause of pain, it has to be recognized that at an end stage the organ that the veins drain can also be affected.
The Pain Must Have a Testable Anatomic Basis
The somatic sensory nerves in the periphery are well mapped out and known since even classical times. The described pain should be consistent with a nerve. The best and easiest example is a neuroma that forms in an amputation stump. It triggers pain in its former distribution. It is palpable as a nodular mass. It is visible under ultrasound or cross sectional imaging. And it is easy to turn off temporarily with an injection of lidocaine, either under palpation or image guidance. If you can turn off the nerve and relieve the pain, it is likely that ablating or relieving the nerve of irritation will also relieve the pain. Such is the case in median arcuate ligament syndrome (figure below). The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
Tight Spaces Impinging Nerves, Arteries, and Veins
Many of the tight spaces involving the nerves have accompanying arteries that are compressed. This results in injury to the artery in the form of intimal hyperplasia, post stenotic dilatation, aneurysm formation, and thromboembolism. Shared tight spaces that cause problems for nerves and arteries have the common features of fixed ligaments, adjacent bones and muscles, inflammation, and motion. These include the thoracic outlet, antecubital fossa, cubital canal, diaphragmatic hiatus at median arcuate ligament, inguinal ligament, popliteal fossa, carpal tunnel, obturator canal, mediastinum, retroperitoneum -basically anywhere nerve, compression, and motion occur. In some instances of median arcuate ligament syndrome, postures and breathing trigger the pain. Holding a child in an arm may trigger pain in neurogenic thoracic outlet. Or sitting while wearing tight jeans may trigger a burning pain in meralgia paresthetica. It is not uncommon to find damaged arteries in median arcuate ligament syndrome, thoracic outlet syndrome, and popliteal entrapment or thrombosed veins in nutcracker syndrome, May-Thurner Syndrome, and Paget-von Schroetter Syndrome. Because nerves are typically difficult to visualize, their compression may only be inferred by testing for compression in their adjacent arteries.
Dilated Veins and Swollen Organs and Visceral Pain
Venous hypertension is most commonly conceived of as varicose and spider veins of the legs and offer a model of pain when applied to other pain caused by venous dissension. The visceral sensory fibers veins and arteries trigger a very intense pain that localizes to the trigger. I have often witnessed this when I manipulate a blood vessel during local anesthesia cases. Visceral pain from swelling has a dull achiness that is localizable to my spider veins after a long day standing like a bruise (below). The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
Actual Slide From Midwest Vascular Surgery Traveling Fellowship talk 2017, Chicago, IL, USA
When a limb is swollen from a thrombosis, the veins hurt and is similar to a bone pain from a fracture or a pulled muscle -that is how the brain processes the pain, but when the muscles and skin get tight from edema, the pain is sharp and dire. This is the same kind for pain from a distended left kidney from nutcracker syndrome or a spleen from a splenic vein thrombosis. These conditions can be modeled and predicted based on history and correct differential and confirmed with proper imaging -always.
Build a theory of the pain based on a testable proposition and set of nerves
That is the final message. These pain syndrome require some imagination and empathy to map and model. Predictive tests then can be performed on physical examination, functional testing, or imaging. Often, the adjacent artery is the only thing that can be reliably visualized and tested, knowing that it is the nerve that is compressed. Turning off the offending nerve with a block and relieving the pain is the most powerful argument for operating. It is building the argument for an operation that requires these objective data, but at the end, it does require some experience and faith. You have to believe in your patient and the science and when they coincide, you have to act.











































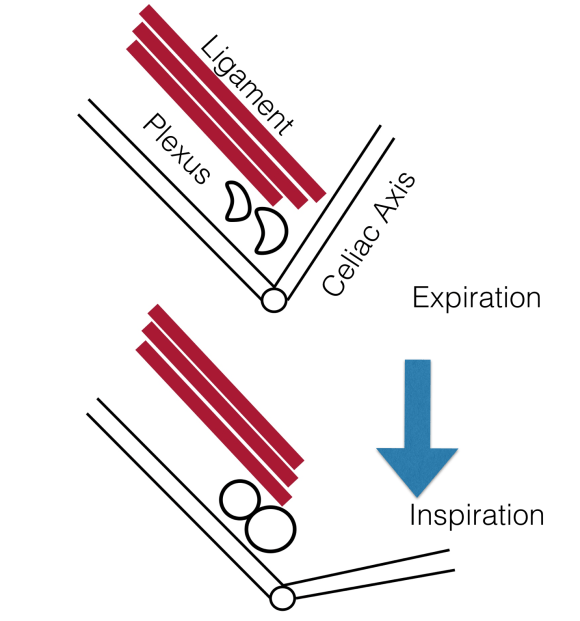 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
