The patient is a 70 year old man with risk factors of cigarette smoking, type II diabetes mellitus, hypertension, and hypercholesterolemia who presents with rest pain and gangrene of the tip of his left great toe. Several weeks prior to this, he went to his pharmacy and received a flu vaccination and picked up over the counter topical medication for an ingrown toenail. who developed pain from an ingrown toenail. Several weeks later, the tip of his toe blackened and the pain became unbearable and he came to the hospital.

Physical examination was notable for the dry gangrene affecting the distal phalanx of the left hallux. There was a left femoral pulse, but nothing was palpable below. His forefoot was cool and painful and this pain was relieved with dependency.

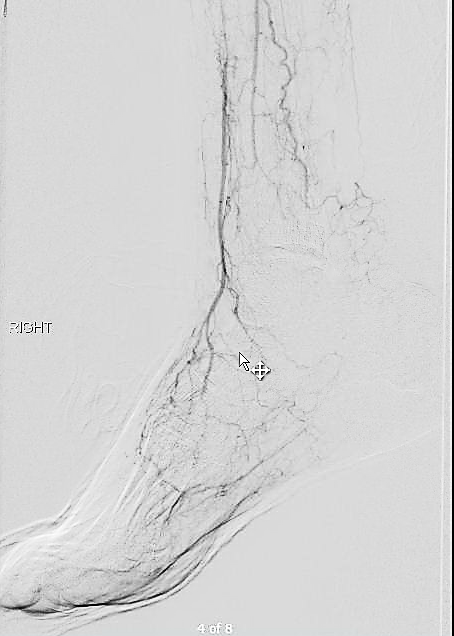
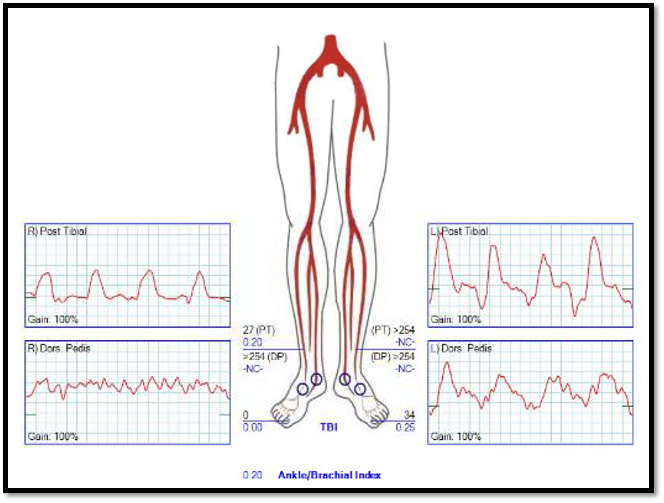
Pulse volume recording showed a drop in flow across the left knee and flate waveforms at the ankle, foot, and digits. The ABI was zero. WIfI 2 3 2, Stage 4, potential benefit of revascularization high (reference 1). CTA was performed and revealed patent aortoiliac segment, patent common femoral and profunda femoral arteries, with occlusion of the mid to distal SFA, reconstitution of the above knee popliteal artery with 2 vessel runoff via a patent posterior tibial and peroneal arteries.

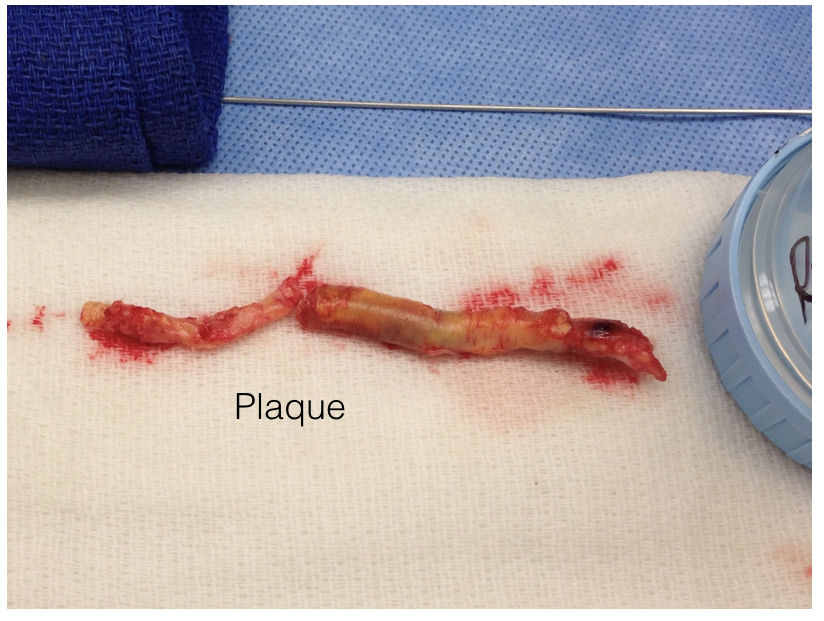
The centerline reconstructions, adapted from aortic planning, lets me determine the character of the arteries for size, calcification, stiffness, collateralization, and length of occlusion. This was had low density and given the timecourse of the events -from claudication to gangrene, and the lack of collaterization implying an acute process possibly on a chronic lesion, I felt there was likely to be some thrombus burden over a chronic plaque across Hunter’s Canal with occlusion of the geniculate arteries. Usually, when the occlusion is chronic, femoropopliteal occlusions of this type come with an ABI of 0.5-0.7, not 0.

Global Limb Anatomical Staging System (GLASS) Classification of CLTI (reference 2) through the easy to use SVS calculator came out Stage II: Intermediate Complexity. I had the good fortune of being in the audience when GLASS was presented to a rapt audience in Lyons, France, by Dr. John White in 2017, at the ESVS meeting. I include it because Dr. Devin Zarkowsky on a tweet that generated this post wanted WIfI and GLASS. WIfI I find helpful. GLASS I am still figuring out, because it tends to tell me what I already know: this is a lesion of intermediate complexity that could go either way to open or endovascular.
Treatment options include:
- Endovascular -starting with POBA and escalating to various additional therapies such as stents, covered stents, DCB, drug coated stents, atherectomy, thrombectomy, thrombolysis (then any of the previously mentioned).
- Bypass with PTFE
- Bypass with vein

The data tells us so far that open or endovascular is broadly equivalent, but experience guides me. For rest pain, any incremental increase of flow will do, and it does not necessarily have to be in-line. For healing major tissue loss, there really can’t be enough flow. Bypasses with good runoff deliver a lot of flow. Bypasses with vein have great longevity and the shorter they are, the longer they last.
So is long patency important? Numerous studies have shown that patency does not impact limb salvage or amputation free survival, going to BASIL Trial (reference 3), but even stretching back to Dr. Frank Veith’s advocacy of PTFE bypass to infrageniculate targets (reference 4), patency does not add to limb salvage beyond the initial wound healing. The patency of a PTFE bypass to a tibial target is less than 20% at 5 years, but the limb salvage rate is a laudable 80% plus, and this is repeated in numerous evaluations of POBA, stents, and every new technology that has accrued in the nearly 4 decades since that paper.
What does patency buy you? Less reinterventions. There is nothing worse to me than having to reintervene within a year or two of an intervention. When a bypass works well, the patients just come for a hello-how-do-you-do for years. The BASIL trial concluded that bypass operations were more expensive, and I dispute this. In 2021, operations were far less expensive than the latest energy weapon, their box you have to purchase, and the catheters you use once and throw away. The argument given by interventionalists is that bypass operations are disfiguring and ridden with complications and that argument holds water as there are many points where vascular surgeons fail or have largely stopped work on investigating and optimizing open surgery. What if bypass surgery could be brought to the level of dialysis access surgery in terms of invasiveness? What if groin complications could be minimized? What if long filleting-type incisions of the thigh and leg could be eliminated entirely? What if edema could be prevented or minimized postoperatively to prevent serous drainage and infections? If you focus on the art of bypass surgery and choose patients well, you can get a quick, minimally invasive bypass with the overall physiologic impact of a Brescia-Cimino AV fistula. After considering endovascular, I chose bypass.
This patient had on mapping excellent saphenous vein between 3-5mm in diameter. He had excellent skin and was not obese. A vertical groin incision could be avoided by making a skin line incision over the saphenofemoral junction and transposing it to the adjacent SFA which was patent. Skin line oblique incisions in the groin heal much better than the standard vertical incisions, and it is possible to mobilize and expose the saphenous vein using an appendiceal retractor and clipping the generous proximal thigh tributary. In this patient, the most proximal incision was well away from the inguinal crease, the generator of wound infections in the groin. Essentially, if there is no groin incision there can be no groin complication.
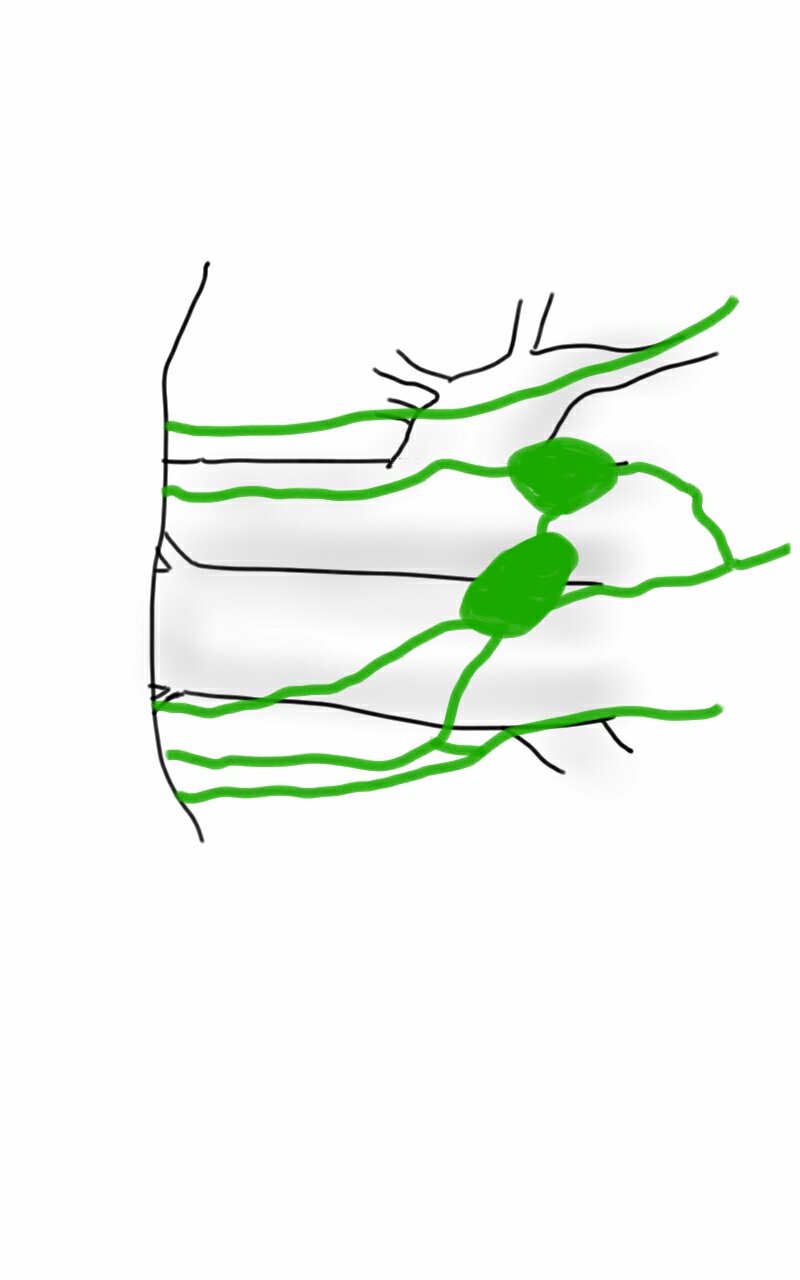
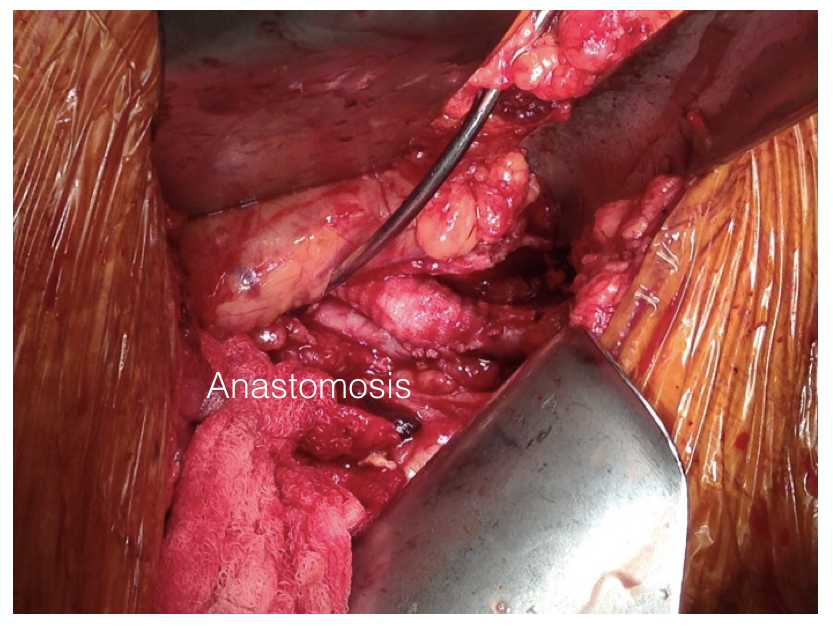
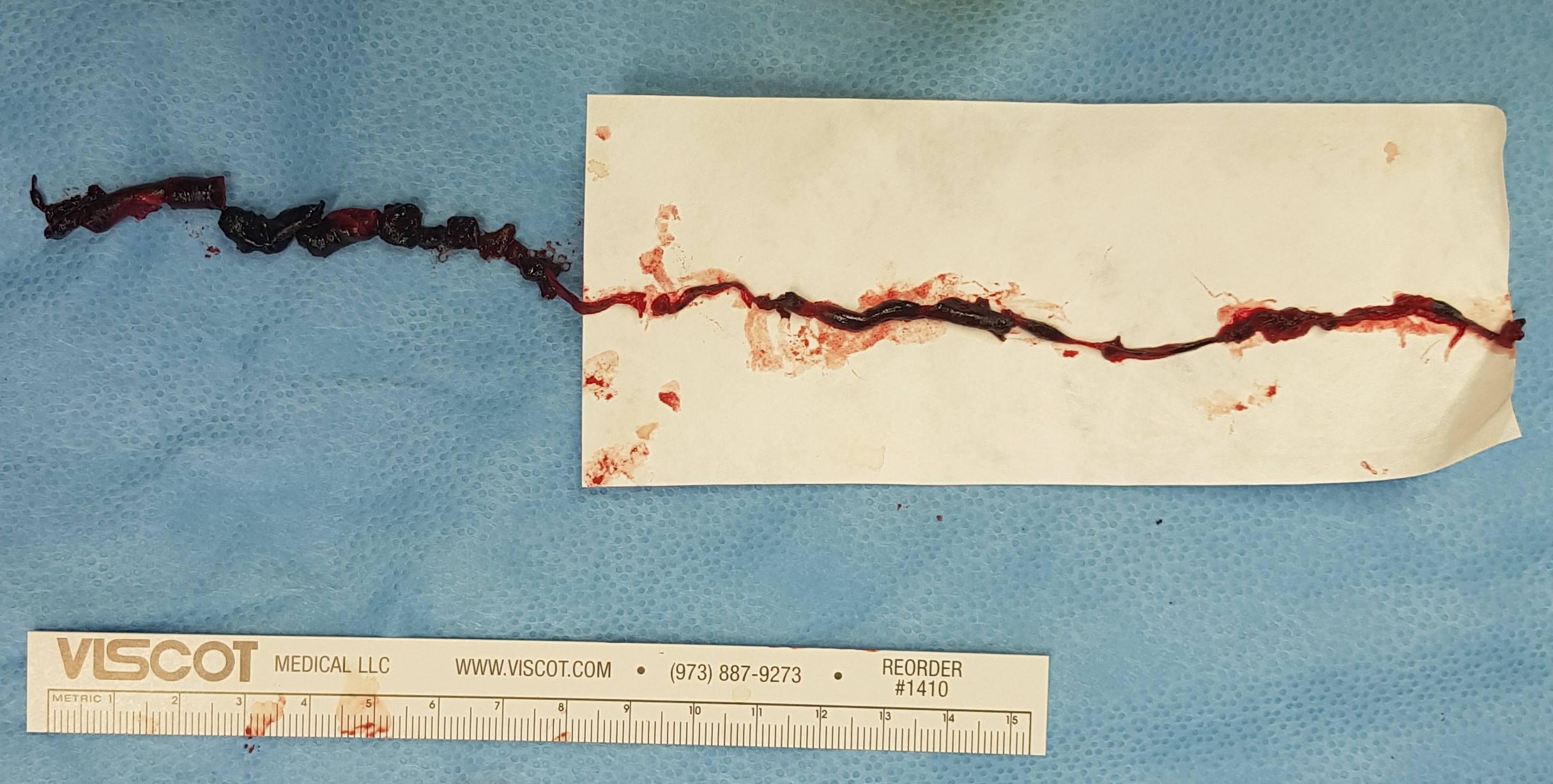
The distal vein is mobilized first before dropping on the above knee popliteal artery which is exposed through a separate incision. This is because the AK POP space is best exposed over the sartorius, and the vein in this patient was well below (posterior) to the sartorius. The vein was tunneled under the sartorius to the AK POP. With the in-situ technique, the proximal anastomosis is completed, then the valves lysed with a retrograde LeMaitre valvulotome. Doing, after two or three passes, the pulse was strong, and the flow strong enough to fling the blood beyond the foot -a key step. If there is no such flow, if there is a weak pulse, or poor blood flight, I do one more pass of the valvulotome then duplex for any large diverting tributaries and tie them off one by one until good flow is achieved.
I do not mobilize the entire vein (and tie off every collateral) unless I cannot do an in-situ technique. It defeats the purpose of this beautiful minimally invasive procedure.

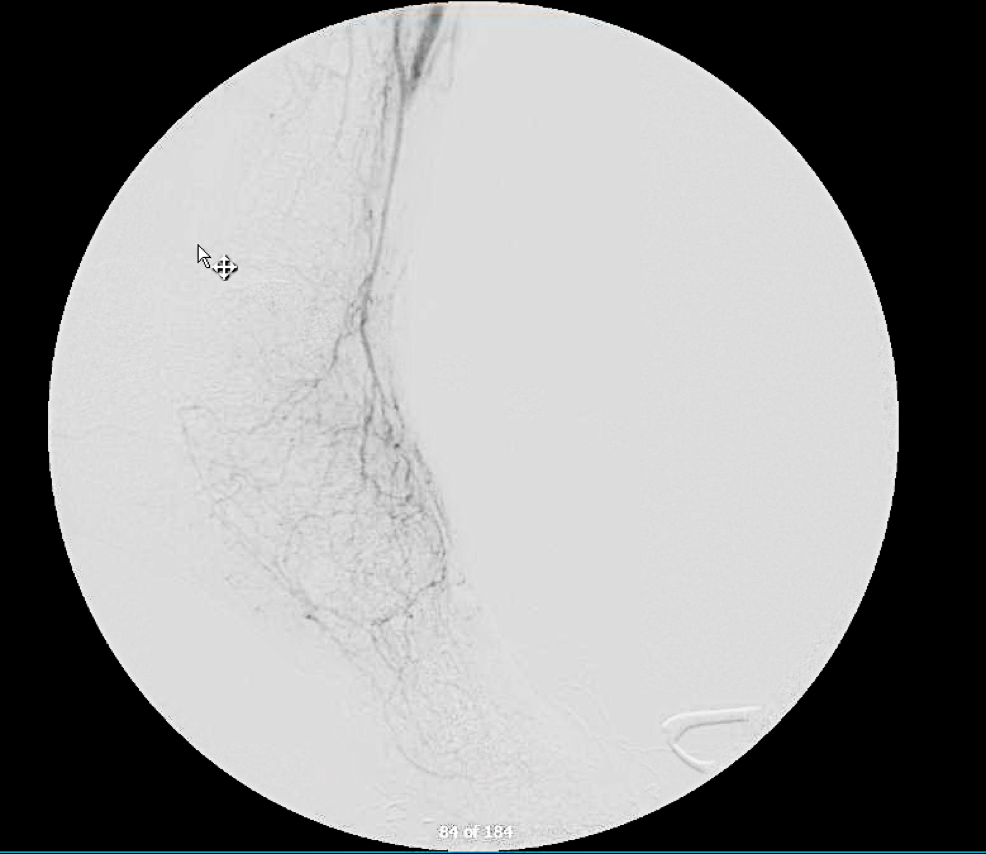
He recovered rapidly and was discharged home after a partial hallux amputation by podiatry. In followup, he was feeling better. All of his surgical wounds had healed. Duplex and ABI did find this:

I took him to the angiosuite for repair of this retained valve. Rarely, retained valves occur after in-situ bypasses, but require generally unsatisfactory solutions involving either open valvulectomy and patch venoplasty or stenting of a virgin vein. Valvulotomy is possible, but generally described as an open procedure as well, but I had other plans.
Downstream of this retained valve were tributaries which could be seen on duplex, and therefore accessible with a micropuncture needle. This would then allow for placement of a 4F sheath, through which the LeMaitre valvulotome would pass unhindered, allowing for valvulotomy. I would use this session in the angiosuite to deliver embolization coils to the diverting tributaries as well.


LeMaitre is a unique company in that it focuses on vascular surgical operations and arises from the original product and reason for the company the eponymous valvulotome. Because it comes sheathed in a low profile catheter, it is immediately familiar to modern surgeons even though it was made in another century.

Cutting the valves involved passing the valvulotome several under fluoroscopy through a 4F sheath placed through the tributary seen above. After the valvulotomy, the diverting tributaries, only one of which drained quickly into a deep vein, were coiled. At the end of the procedure, a manual cuff was found and an ABI checked. It was now 1.05.

In 2015, the Oxford English Dictionary added McGyver as a verb -“Make or repair (an object) in an improvised or inventive way, making use of whatever items are at hand.” A television show from the 80’s and early 90’s, the main character, McGyver, was able to make useful tools out of what was available, allowing him to come out victorious, but usually just survive. It is a useful concept that is a must have in managing complex and dynamic situations. Just because it hasn’t been done before to your knowledge doesn’t mean that it isn’t a simple solution. I have only one ask that LeMaitre flip their blades around and design an ante grade valvulotome. Those who know what I’m getting at know what I am getting at.
The LeMaitre valvulotome allows for in-situ saphenous vein bypass, a prototypical hybrid vascular procedure from the 80’s that portended the endovascular revolution that followed. It is meant to be used intraoperatively, but because of its low profile, it can be applied.
I will allow that this second procedure likely makes any argument to cost moot, but numerous incisions and extra time in the OR is avoided. The patient now has a vein bypass that could last many years which diminishes the need for follow up procedures to maintain assisted patency.
We will be arguing this point for years even after BEST-CLI is presented. BASIL-2 just closed enrollment. Hopefully we will get some clarity.
Reference
- Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014 Jan;59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12. PMID: 24126108.
- Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28. Erratum in: J Vasc Surg. 2019 Aug;70(2):662. PMID: 31159978; PMCID: PMC8365864.
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005 Dec 3;366(9501):1925-34. doi: 10.1016/S0140-6736(05)67704-5. PMID: 16325694.
- Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.






 If you work long enough, you will not only see everything, but you may end up doing something that you say you would never do. You will be confronted with a scenario that would test not just your skills but also your boundaries. The adage, never say never is a warning that all of us may face a choice -to remain rigidly consistent with some earlier proclamation or to excuse a little hypocrisy for the sake of the patient.
If you work long enough, you will not only see everything, but you may end up doing something that you say you would never do. You will be confronted with a scenario that would test not just your skills but also your boundaries. The adage, never say never is a warning that all of us may face a choice -to remain rigidly consistent with some earlier proclamation or to excuse a little hypocrisy for the sake of the patient.