Every time someone on Seinfeld went to the hospital, a stock scene (above) would play. It’s the old ER of Roosevelt Hospital on 9th Ave before the renovations moved it to current 59th street entrance. I was a surgery resident there in the 90’s and watched each Seinfeld episode for the upper West Side stuff that would pop up. The soup Na2i was a few blocks over. Not seen on this pic is the Sym’s operating theater designed by Dr. Charles McBurney which is a designated landmark and currently a private school for “gifted but difficult” children (link). I used to round on patients in the red building -they would be ten in a room separated, if lucky, by rolling privacy screens. My sister was born here. John Lennon died here. All that gone, because hospital buildings are like dressings on a city’s wounds and need to be changed every generation. In fact, it’s not even called Roosevelt Hospital any more.
Roosevelt Hospital’s name was changed to Mount Sinai West, and its sister hospital, St. Luke’s, was changed to Mount Sinai Morningside. I would like to imagine that it was vengeance a century in the making, for pearl clutching slights originating from the gilded age, of blue bloods v. upstart Jews. Because no matter how far you are from the shtetl, there is always another golden door closed to you in New York City. So it seemed for me, an immigrant who had worked hard to get to Harvard College, and Columbia P&S, to look with squinted eyes at my letter on match day and see St. Luke’s/Roosevelt Hospital Center, my last choice that I listed out of a general interest to avoid not matching.
When I landed on St. Luke’s-Roosevelt for my general surgery training, the house officers were quartered in the older parts of the hospital, some rooms dating back to the 19th century, unchanged like unearthed chambers from Pompeii. Both hospitals still had the open wards for the “ward” patients with segregation of the private patients up in the towers. For a time, they still had seamstresses to mend your white coat and cafeterias that still cooked their foods fresh. The resident’s lounge at St. Luke’s was like a frat house common room from the thirties, with a scratched-up pool table, a broken piano, pedastaled hotel ashtrays, and card tables. An old handprinted sign (which I regret not taking) listed the house officer’s rules and entitlements which included two beers or a shot of whiskey per night on call.
After my intern year, both hospitals started sorely needed renovations. The surgery office had to be cleaned out, and behind an antique cabinet, wooden boxes of chromic cat-gut suture were found, still in their glass tubes and preserving fluids, little brown skeins of suture floating like preserved fetuses, a strange message from a faraway time. I ran into Walter Wichern, chairman emeritus, who showed up randomly to the hospital in blue blazer and bow tie. I had just stained my dress shirt pocket with my soon-to-be-lost Mont Blanc fountain pen, and he launched into a story about how he repaired a ruptured aortic aneurysm back in 60’s by cutting his new polyester dress shirt into a tube and sewing a graft out of it down in the laundry, after hearing a talk from Arthur Vorhees at P&S. And he was smiling an enigmatic little smile, recalling how that patient on being discharged gifted him annually with ten new dress shirts every year. I later found out that Dr. Wichern was famously taciturn, and I had somehow unlocked an achievement -getting a story out of an old surgeon. It was around then that I had started to feel that it wasn’t all a big mistake.
When I recently changed hospitals from the Cleveland Clinic to University Hospitals, I had to submit documents for privileging, and I get a testy email. “Where did you do your residency?” The administrator couldn’t find St. Luke’s/Roosevelt anywhere on the ACGME website, or even on Google. When I offered the new names, the reply came back, “They only have records going back to when they took over in 2008.” I briefly contemplated retiring, then asked if sending pictures of my framed degrees would be sufficient. Only partly, was the reply. She wanted witnesses.
My first night on call was terrifying. I was on call with Bobby Borromeo -my fellow intern, Anil Hingorani -our PGY4, and Jesse Jean-Claude -our Chief Resident. All of us are now practicing vascular surgeons -Bobby (fellowship Yale), Anil (fellowship Montefiore), Jesse (fellowship UCSF), and myself (fellowship Mayo), embarked on a night of call that involved no sleep and little food. The single moment I recall was taking Bobby through a blood draw and filling the forms for processing the labs and performing EKGs with an antique strip recorder, cutting and pasting the strips onto a formatted sheet for the chart. Bobby didn’t know how because there were many people to do these things in his home hospital in the Phillipines. For myself, I knew the two hospitals from my rotations during medical school. I could draw blood and cut, sew and tie above my level from my time as a senior student at P&S. I got a bit too comfortable with my privilege, and I was still thinking I should have been somewhere else. Over breakfast, I absentmindedly voiced this out loud and was corrected in a way that is no longer possible in 2022. It was the tone that I remember, of being chewed out.
One of chiefs snapped at me,”You have no idea how big and important these hospitals are. They are older than all the other hospitals here in NY. McBurney did the first appy here. Halsted was chief at Roosevelt and invented cancer surgery and the surgical residency. Green invented the LIMA bypass at St. Luke’s. Our chiefs go to better fellowships year over year than any other hospital in Manhattan. You should be grateful to be allowed to round with us.”
Tie given out at graduation, designed by Howard Nay, MD (link), RIP. One of the few keepsakes of my time there. Dr. Skip Nay, was old school, and gave everyone nicknames. Learning surgery from him was like taking blues guitar lessons from Mr. Robert Leroy Johnson.
It was by my third year I got used to the 120 hours a week. It is only now a quarter century later, that I value it. I was expending my. youth living and breathing surgery in the latter days of St. Luke’s and Roosevelt Hospitals. I was missing my friend’s weddings, missing time with my wife, seeing New York during the glory of the 90’s through the dank recesses of a trauma bay. I was six figures in debt, but I could take out your appendix in twenty minutes. I had just signed on for a year of research with the peerless Dr. David Tilson and was not looking forward to telling my wife who found the original five year deal of residency interminable. Add to that, two years of fellowship. Walking out on the deck of the call room overlooking the Cathedral of St. John the Divine and Columbia’s campus, listening for the sirens, I really felt the spirit of the hospital.
It’s not the name of the place, neither its splendor nor its comforts, but the commitment of the people in the teams that you build, which allows you to do great things. And yet…
Summer 2022, in front of Mt. Sinai West, formerly and forever Roosevelt Hospital.
A New Day -created by @nightcafestudios AI upon my suggestion.
Ten years ago, I joined the Cleveland Clinic. I worked five years at the main campus as teaching faculty. I learned as much as I taught, as I got to apply the accumulated volume of experience and knowledge from the previous decades in New York, Rochester (MN), and Des Moines. Five years ago, I took myself and my family to Abu Dhabi, and started a vascular surgery program at CCAD (Cleveland Clinic Abu Dhabi). Last year, still in the middle of the second year of the pandemic, we returned, and I had the privilege of working at Cleveland Clinic Fairview and Cleveland Clinic Avon on Cleveland’s west side. This spring, I made the decision to join University Hospitals, where I will be starting this August. I crave these new days and am so grateful to have them. Thank you, Cleveland Clinic, for ten amazing years. Hello University Hospitals! I can be reached at docpark(at)golfism.org during this transition.
Steve Jobs is credited with popularizing the saying credited to Pablo Picasso, “good artists copy, great artists steal.” While its provenance may be apocryphal, it makes an excellent point about how we learn. Even in the lack of understanding, it is still possible to learn by copying. Toddlers do this. We, as land mammals, are hard wired to copy.
Take for example this patient below with Leriche syndrome with a triad of smoking, claudication, and impotence.
Aortoiliac occlusive disease with history of smoking, claudication, and impotence in a middle aged man = Leriche Syndrome
Because of his relative youth, being his 50’s, I felt the most appropriate procedure was an aortobifemoral bypass.
I frequently use these diagrams to illustrate for the patient.
The only real complexity to manage was the severe stenosis he had in his left renal artery.
A severe stenosis of left renal artery
The options included
renal endarterectomy as part of aortic thromboendarterectomy
renal artery bypass from the aortic graft
reimplantation of renal artery
something else
Something Else: The complexity of renal revascularization creates risk. An antegrade endarterectomy of the renal artery would be done below a suprarenal clamp, adding to clamp time. A bypass would require the kidney to bide its time during the proximal aortic anastomosis, and the anastomosis for a jump graft, then the anastomosis to the left renal artery. This renal ischemia time can be extended by cooling the kidneys with cold (5 degree) LR, but why risk it? A renal endarterectomy can devolve into a visceral segment endarterectomy. After an hour, a nephrectomy.
That’s where this whole copying concept comes into play. Back in 2012, I worked with Dr. Jeanwan Kang, who had just come out of training with Dr. Richard Cambria. We were doing a type IV thoracoabdominal aortic aneurysm, and the right renal artery had a ostial stenosis. While I was figuring out the best way to manage this, Dr. Kang asked for a 6x18mm renal stent and an insufflator. She stuck the stent into the renal orifice and deployed the stent, opening the orifice. I had to find my jaw which had dropped to the floor.
Now, ten years on, that’s how I managed this patient’s ostial renal artery stenosis.
The patient’s thrombotic plaque went up to the renal origins and needed to be endarterectomized, but embarking on a renal endarterectomy adds potentially harmful renal ischemia time. Therefore, through the vertical aortotomy, I was able to get a clean end point to the aortic thromboendarterectomy and position a stent in the renal orifice and deploy it.
After thromboendarterectomy of the aortic plaque, the left renal ostium is treated with a balloon expandable stent. The aorta then is partially closed primarily to move the clamp below the renal arteries
Once the stent was deployed, the aorta was partially closed primarily to allow the clamp to be moved below the renal arteries. This all took less than ten minutes of ischemia time. The aortic graft was then sewn end to side to the remaining aortotomy.
The patient recovered and was discharged on POD#6 with normal renal function. In followup, his CTA showed excellent graft and stent patency.
A followup CTA shows a patent 14x7mm aortobifemoral bypass. I choose the bypass based on avoiding excess size mismatching distally as I find that patients who get 20x10mm grafts run into problem with mural thrombus because of limited flows into smaller femoral vessels. The renal stent is patent.
The centerline view of the renal stent shows it to be widely patent.
Patent stent with avoidance of the pitfalls of a renal endarterectomy
The patient is walking well without limitations and has improved blood pressure control, achieving normotensions at times.
If you are curious about the results from MGH, I refer you to their paper on 67 patients treated with open hybrid revascularization of the renal artery during complex aortic reconstructions (reference). At a mean followup of a year, they reported a 98% stent patency.
There is a comfort in sticking to what you know. The extreme example of this is the practitioner who graduates with a skill set from training and never expands on it. Yet there is an opportunity cost to blind devotion to sticking what you know and that is never growing. I recall this in the panel discussions during the VEITH Symposia I used to sneak into as a resident in the 90’s where great authorities pooh-poohed or condemned anything endovascular.
It’s a sign of a nimble mind that Dr. Cambria, after learning endovascular techniques mid-career, adapted these skills to his open surgical toolkit. His trainee, Dr. Kang, soon after, taught me.
Or was I just looking over her shoulders taking notes?
Reference:
Patel R, Conrad MF, Paruchuri V, Kwolek CJ, Cambria RP. Balloon expandable stents facilitate right renal artery reconstruction during complex open aortic aneurysm repair. J Vasc Surg. 2010 Feb;51(2):310-5. doi: 10.1016/j.jvs.2009.04.079. Epub 2009 Oct 22. PMID: 19853403.
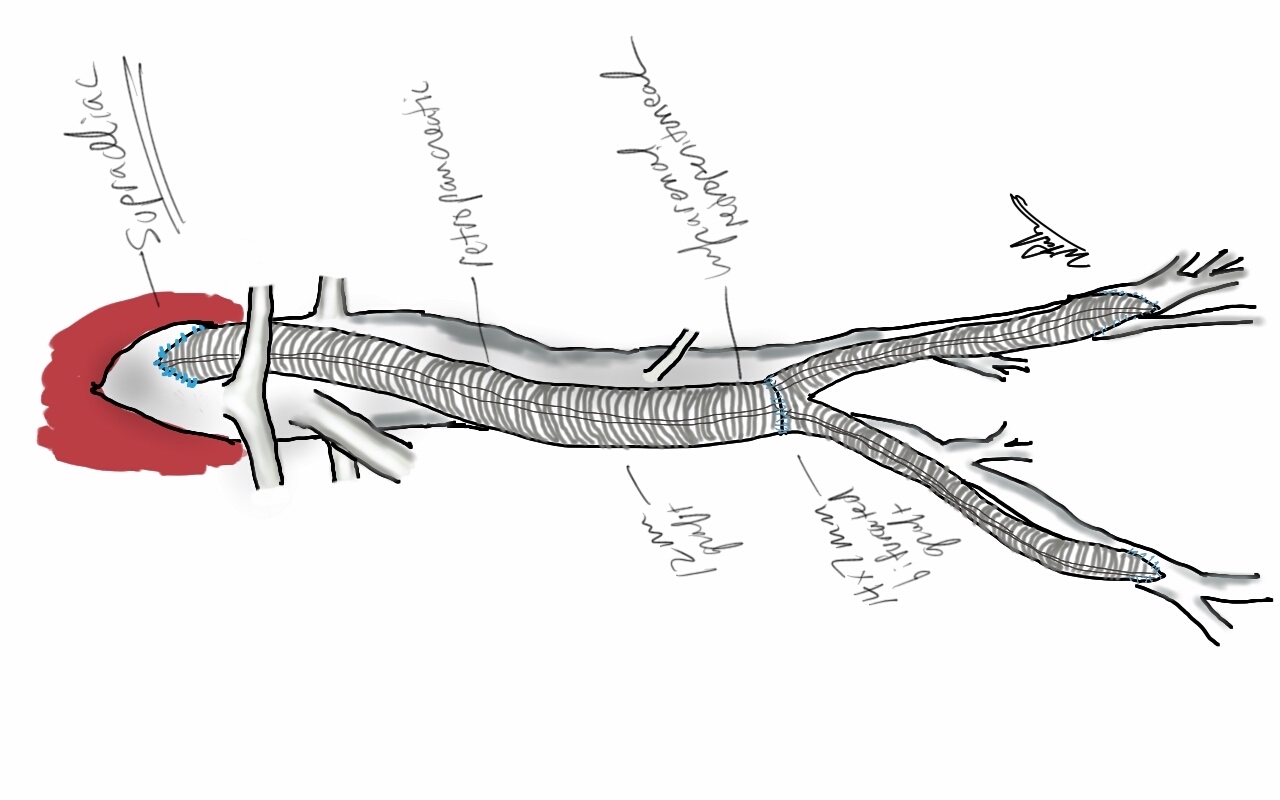
The patient was a 50 something year old man who I took care of in 2016 before I left for Abu Dhabi. He had a background of hypertension, hypercholesterolemia, and IDDM with chronic immunosuppression for rheumatoid arthritis. For several weeks he had rest pain in his feet and impending gangrene of his left great toe. More worrisome was the development of punched out ulcers on his groin crease resulting in weeping wounds after a bout of cellulitis. He had no palpable femoral pulses. Pulse volume recordings showed flat lines from the thigh to the feet.
CTA of the abdomen and pelvis with runoff showed aortic occlusion due to heavily calcified plaque with reconstitution of the external iliac arteries via the internal iliac arteries. The common femoral arteries were only mildly diseased and there was patent runoff.
Centerline up right femoral into aorta shows occluded aorto-iliac segment and diseased external iliac artery. Centerline up left femoral into aorta shows mirror image of disease on left side
He was one of the rare instances of chronic limb threatening ischemia due to aortoiliac occlusive disease, AKA Leriche syndrome. The added background of autoimmunity made him vulnerable to the ulcers in the groin crease, and the infections there made access challenging.
Leriche Syndrome
The choices were endovascular versus open surgical repair. The groins were a problem with recent cellulitis, immunosuppression and open wounds, but with careful prep, and coverage with Ioban, access was possible, even for stent grafting. The problem was the aortic bifurcation was heavily calcified, and manipulating this likely thrombotic material with an end stump of aorta can cause renal embolism. There was a small risk of rupture at the bifurcation and of renal failure.
Standard aortobifemoral bypass graft was out of the question because of the lack of a safely clampable aorta -there was circumferential aortic plaque below and above the renal arteries and the infections in the groins would jeopardize any prosthetic graft. You have to respect unclampable aortas but like anything else, there are ways around it (link).
Regarding the groins, during fellowship, Dr. Thomas Bower used to take the distal anastomoses to the external iliac arteries which could be exposed via short lower abdominal incisions if not through the midline incision itself, avoiding groin incisions in hazardous groins.
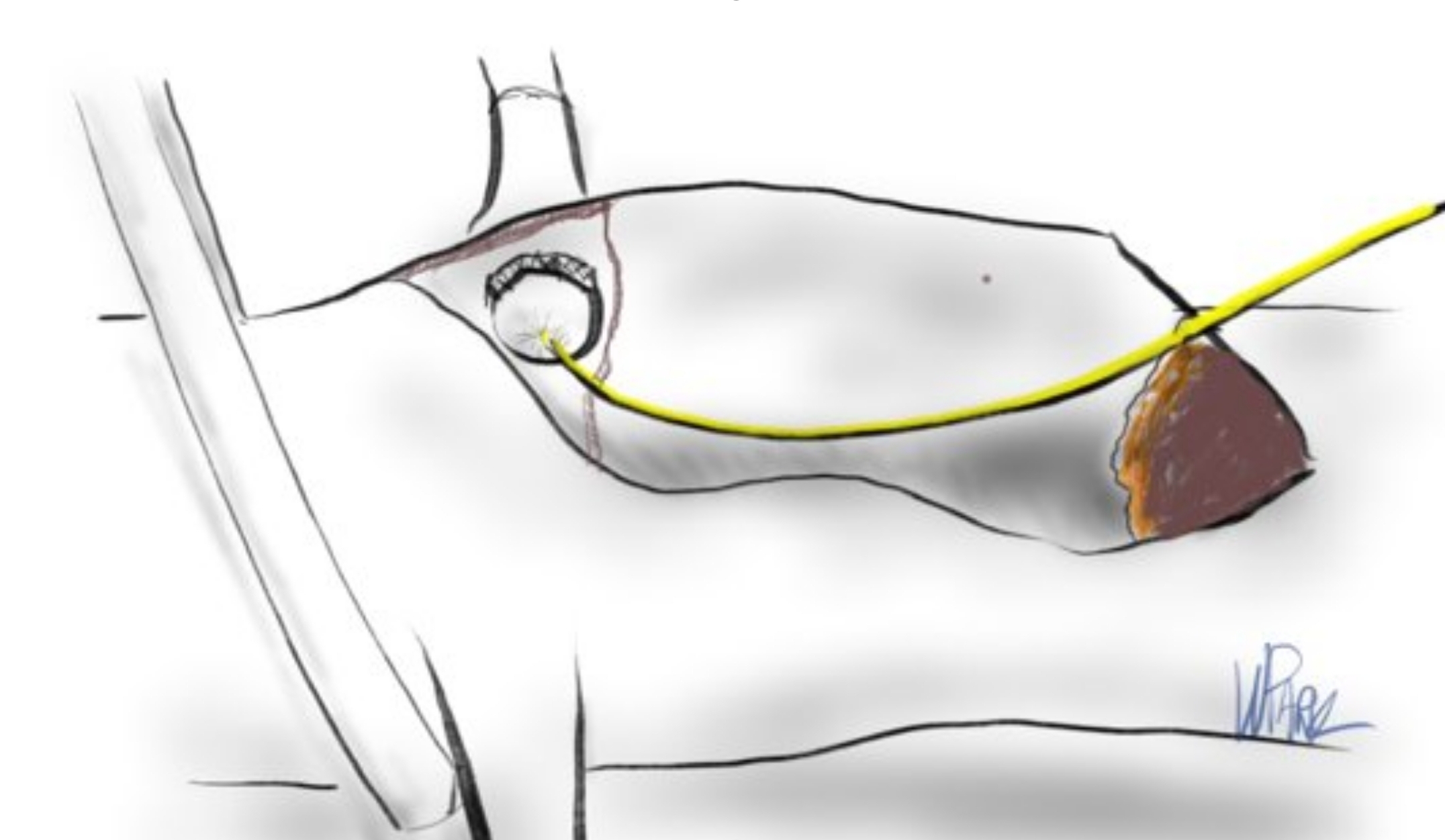
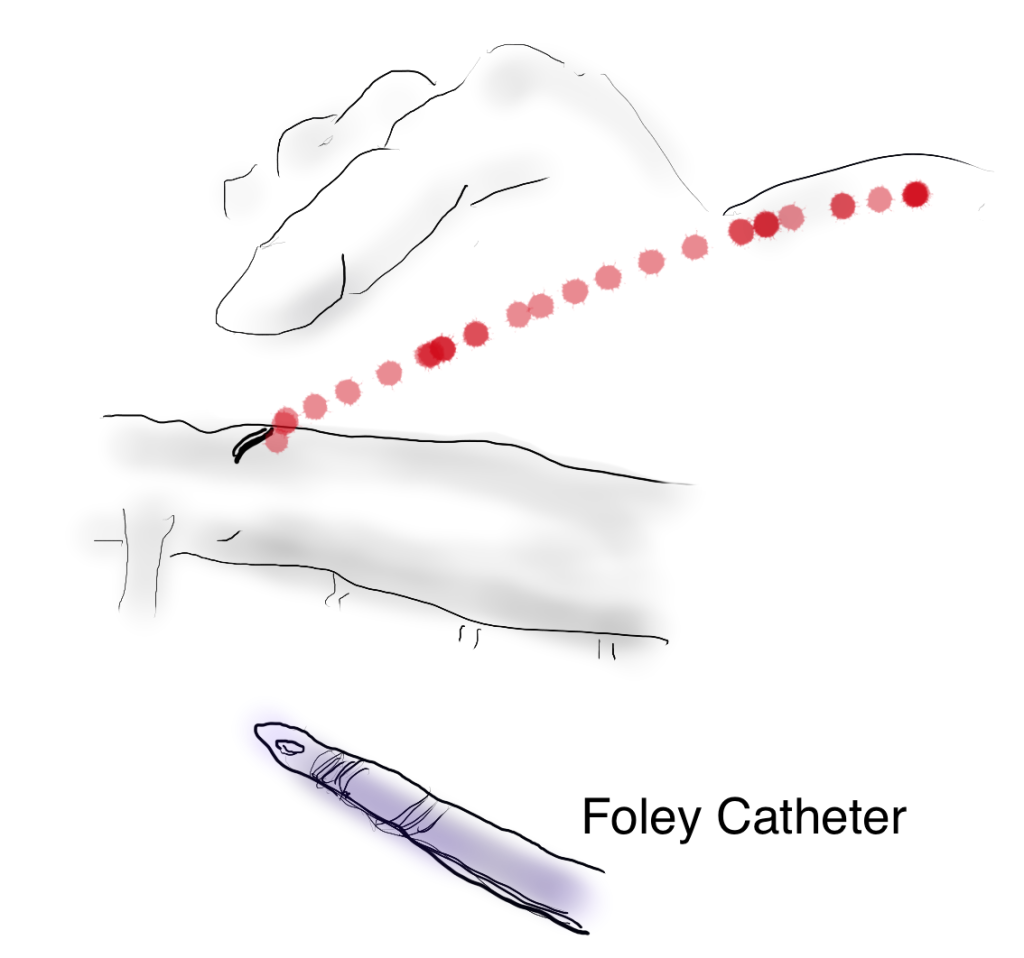
I performed an aorto-bi-iliac bypass using the balloon in the infrarenal technique after obtaining supraceliac control described in my technical post (link).
A small aortotomy can be controlled with a finger and a foley easily slipped in -just remember to clamp itThis typically provides adequate hemostasis and space to perform a proximal anastomosis
I was able to endarterectomize a nice segment of aorta and anastomose end to side -always end to side as it preserves endovascular options. The distal anastomoses was to the external iliac arteries. He did well in the immediate postoperative period but I soon left for Abu Dhabi.
In the five years since the operation, he has needed an SMA stent and has devloped worsening CKD and autoimmune diseases. But one of the gratifying things is he healed his wounds on this groins and thighs and the left hallux, and pain has never recurred. He had a contrast CT at the 5 year point (figure) showing a widely patent graft, and he sought me out when he heard that I was back in Cleveland.
His PVRs remain normal (figure).
The PVRs and ABI’s remain robustly normal even after 5 years
I’m not saying that iliac stents from the iliac bifurcation to the renal arteries was a bad option, but there is a particular sadness and weariness when I have to take care of occluded stents. As an engineer, what is worse than ballooning an occluded stent and placing another stent inside? Knowing what I know about cell biology, what is worse than lasering, drilling, cutting, that cicatricial scar tissue that is neointimal hyperplasia in terms of what you leave behind. This man still has decades left to live and he will have his bypass graft far longer than any stent. This durability, a byproduct of the technique, is a worthy virtue.
When I operated, he was in his mid fifties and despite his comorbidities, was able to undergo a big operation. Now he is in his sixties and his autoimmune issues have progressed to where he is suffering from stiff person syndrome with difficulty walking. His renal function is poor and overall he is a terrible open surgical candidate. If I had done interventions at that time, which I was tempted to, he could today be facing amputations in the setting of cytotoxic immunosuppression having run out of endovascular options.
We have lost too much to innovation. The fact is, aortic surgery for critical limb ischemia was once and it still is a thing, because it works.
When I was a young attending at the Allen Pavilion of Columbia Presbyterian Hospital, I was called into an operating room for a stat consult on a patient about to undergo a cholecystectomy. During the case, the IV had infiltrated and a bag of saline had filled the patient’s hand and forearm with saline, causing the hand to look like an inflated glove. The fingers were cool and white and the edema was firm but yielded to touch.
I elevated the hand and firmly squeezed the edema out of each digit, then gently massaged the edema from the hand onto the forearm. From there, I pushed the edema onto the arm. I then wrapped the hand up in an Ace wrap, and suspended it from an IV pole and returned to my case. Later, I returned and the hand was restored, warm, and perfused.
The lymphatics serve to move extracellular fluid (link). They can be overwhelmed much as drainage from a house can be overwhelmed resulting in puddles and ponds (link). This extracellular space has been “discovered” to be a new organ, but vascular surgeons have known about it for some time. Ultrastructurally, it is very close to a sea sponge with lattices of structural protein connecting cells to form tissues. And like a sea sponge, the salty water can be squeezed out or drained using gravity.
In olden times in central Europe, if you had chronic leg ulcers, you went to abbeys that specialized in their care. There, nuns would milk the edema out of your leg swollen typically from parasites and dress the leg and ulcer in linen cloth soaked in special oils. This is how Dr. Paul Gerson Unna came up with his eponymous Unna’s Boot, substituting Zinc Oxide paste which created a bacteriostatic environment.
Professor Paul Gerson Unna
Every year or so, I will be consulted for what I term a lymphatic emergency. A subset of this is phlegmasia. Whatever color you find -alba (white) or cerulea (blue) is really no matter -who really knows which comes first? It is an emergency in that the time clock for arterial ischemia -minutes to an hour for nerves, an hour to 6 for skeletal muscles, 6-12 for skin and bone, are all in play. The instinct is to go right to fasciotomy, but what you are usually doing is releasing the extracellular space, and the muscles are typically fine, even though their compartment pressures were very high.
Take this patient who developed severe upper extremity edema in the recovery phase after a cardiac arrest.
The ICU staff noted the had discoloration about four hours after the arrest. There were no arterial pulses and the forearm and hand were rock hard, the finger tips ice cold. Compartment pressures measured using the arterial line and needle method didn’t drop after the initial flush of saline below 70mmHg. While I could have been justified in performing upper extremity fasciotomy and even trying thrombectomy in a critically ill, coagulopathic patient on multiple pressors, I could just as easily have been on solid ground for saying the life was more valuable than the dominant hand. Both would have been the wrong move.
I performed the nun’s milking maneuver mentioned at the beginning and lacking an Unna’s boot, I compressed and elevated the best I could with double gloving using a small sized glove and ACE wrap.
Notice the edema has segregated into the arm.
In the morning, taking down the dressing, and re-compressing, there was now a radial artery signal and the fingers were a much improved color. The pulse-oximeter waveform was near normal. As an aside -the pulse oximeter uses the same technology as the digital photoplethysmography for generating toe waveforms in the vascular lab -ie. a vascular lab at every bedside! We have collected and are analyzing the data on this for publication.
The pulse oximetry waveform is the same tech as digital photoplethysmography. Cotton cast padding (Webril) and Coban wrap is a good method of compression that avoids the problems with ACE wrapping.
It’s a hard thing to not run off to the operating room in most cases because that is how we are trained, but understanding how a patient got to that point is crucial in deciding if compression alone will work. If they call you from the ER about a patient with a swollen cold foot with diminished signals, you have to figure out the mechanism. Was it arterial occlusion, rest pain, and chronic dependency of the foot that resulted in this? Typically the swelling appears late. Was it heart failure and inability to walk, resulting in the patient sitting all day in a chair that is the cause? Was it pregnancy with a DVT? Was it the deadly sin of sloth? Only in arterial occlusion in a chronic presentation would compression be contraindicate. In this ICU case, the lack of arterial signal is secondary to the swelling, not the cause of it.
Elevation alone does not manage edema well. Only hanging upside down or being in water up to your neck…
Compression is a necessary component of treating lymphedema emergencies because elevation alone may be insufficient, particularly in the leg.
Wrapping a leg is a critically, undertaught skill. Also, never cover the knee cap.
Elastic compression is ubiquitously available as the ACE wrap, but they can shift and move and roll, causing zones of excess and not enough compression. TED hose and compression stockings are definitely helpful in long term management, but with legs, compression needs to go up to the knee joint, or up to the groin, never halfway or the edema will create a line of ischemia at the end of the stocking that blisters when the stocking is removed, and can progress to full thickness necrosis. Cotton cast padding and Coban, or an Unna’s Boot may be the safest in terms of avoiding skin injury.
ACE wrapping is never taught adequately, and for it to work well and avoid injury to the skin, the wrapping has to be reapplied several times a day. It should be a prerequisite for nursing and medical student certification, as edema is the most common vascular disease.
Moving into our new home after four years out of country, I welcome an old friend from storage, but also unfortunately a health hazard, only mitigated by being fully reclinable.
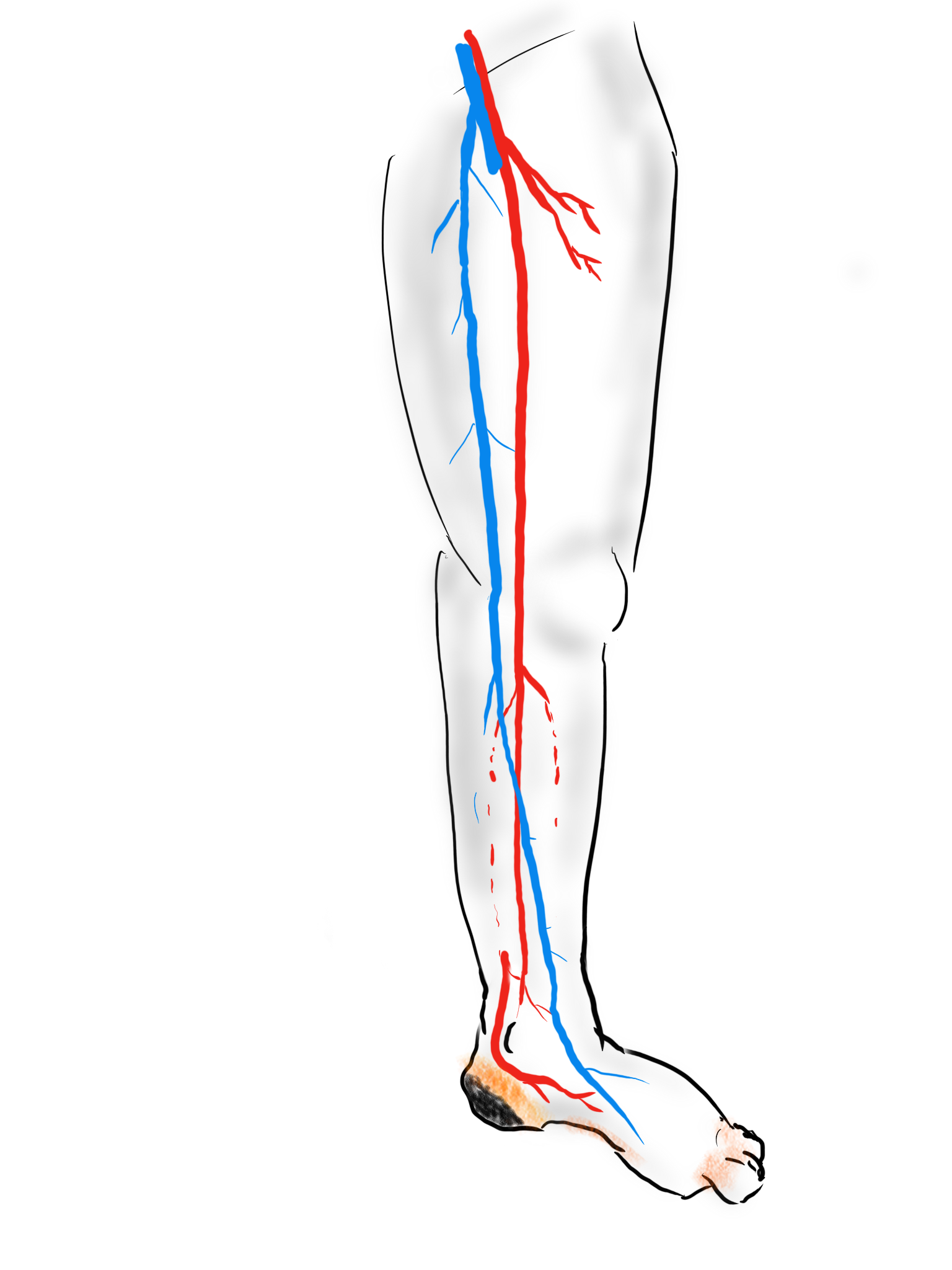
The patient is a 70 year old man with risk factors of cigarette smoking, type II diabetes mellitus, hypertension, and hypercholesterolemia who presents with rest pain and gangrene of the tip of his left great toe. Several weeks prior to this, he went to his pharmacy and received a flu vaccination and picked up over the counter topical medication for an ingrown toenail. who developed pain from an ingrown toenail. Several weeks later, the tip of his toe blackened and the pain became unbearable and he came to the hospital.
No pulses, dry gangrene of tip of toe
Physical examination was notable for the dry gangrene affecting the distal phalanx of the left hallux. There was a left femoral pulse, but nothing was palpable below. His forefoot was cool and painful and this pain was relieved with dependency.
Pulse volume recording showed a drop in flow across the left knee and flate waveforms at the ankle, foot, and digits. The ABI was zero. WIfI 2 3 2, Stage 4, potential benefit of revascularization high (reference 1). CTA was performed and revealed patent aortoiliac segment, patent common femoral and profunda femoral arteries, with occlusion of the mid to distal SFA, reconstitution of the above knee popliteal artery with 2 vessel runoff via a patent posterior tibial and peroneal arteries.
CTA VR Reconstruction Shows Reconstitution of AK POP and 2V Runoff via PT and Peroneal Arteries
The centerline reconstructions, adapted from aortic planning, lets me determine the character of the arteries for size, calcification, stiffness, collateralization, and length of occlusion. This was had low density and given the timecourse of the events -from claudication to gangrene, and the lack of collaterization implying an acute process possibly on a chronic lesion, I felt there was likely to be some thrombus burden over a chronic plaque across Hunter’s Canal with occlusion of the geniculate arteries. Usually, when the occlusion is chronic, femoropopliteal occlusions of this type come with an ABI of 0.5-0.7, not 0.
Global Limb Anatomical Staging System (GLASS) Classification of CLTI (reference 2) through the easy to use SVS calculator came out Stage II: Intermediate Complexity. I had the good fortune of being in the audience when GLASS was presented to a rapt audience in Lyons, France, by Dr. John White in 2017, at the ESVS meeting. I include it because Dr. Devin Zarkowsky on a tweet that generated this post wanted WIfI and GLASS. WIfI I find helpful. GLASS I am still figuring out, because it tends to tell me what I already know: this is a lesion of intermediate complexity that could go either way to open or endovascular.
Treatment options include:
Endovascular -starting with POBA and escalating to various additional therapies such as stents, covered stents, DCB, drug coated stents, atherectomy, thrombectomy, thrombolysis (then any of the previously mentioned).
Bypass with PTFE
Bypass with vein
White Arrows Show the Excellent GSV
The data tells us so far that open or endovascular is broadly equivalent, but experience guides me. For rest pain, any incremental increase of flow will do, and it does not necessarily have to be in-line. For healing major tissue loss, there really can’t be enough flow. Bypasses with good runoff deliver a lot of flow. Bypasses with vein have great longevity and the shorter they are, the longer they last.
So is long patency important? Numerous studies have shown that patency does not impact limb salvage or amputation free survival, going to BASIL Trial (reference 3), but even stretching back to Dr. Frank Veith’s advocacy of PTFE bypass to infrageniculate targets (reference 4), patency does not add to limb salvage beyond the initial wound healing. The patency of a PTFE bypass to a tibial target is less than 20% at 5 years, but the limb salvage rate is a laudable 80% plus, and this is repeated in numerous evaluations of POBA, stents, and every new technology that has accrued in the nearly 4 decades since that paper.
What does patency buy you? Less reinterventions. There is nothing worse to me than having to reintervene within a year or two of an intervention. When a bypass works well, the patients just come for a hello-how-do-you-do for years. The BASIL trial concluded that bypass operations were more expensive, and I dispute this. In 2021, operations were far less expensive than the latest energy weapon, their box you have to purchase, and the catheters you use once and throw away. The argument given by interventionalists is that bypass operations are disfiguring and ridden with complications and that argument holds water as there are many points where vascular surgeons fail or have largely stopped work on investigating and optimizing open surgery. What if bypass surgery could be brought to the level of dialysis access surgery in terms of invasiveness? What if groin complications could be minimized? What if long filleting-type incisions of the thigh and leg could be eliminated entirely? What if edema could be prevented or minimized postoperatively to prevent serous drainage and infections? If you focus on the art of bypass surgery and choose patients well, you can get a quick, minimally invasive bypass with the overall physiologic impact of a Brescia-Cimino AV fistula. After considering endovascular, I chose bypass.
This patient had on mapping excellent saphenous vein between 3-5mm in diameter. He had excellent skin and was not obese. A vertical groin incision could be avoided by making a skin line incision over the saphenofemoral junction and transposing it to the adjacent SFA which was patent. Skin line oblique incisions in the groin heal much better than the standard vertical incisions, and it is possible to mobilize and expose the saphenous vein using an appendiceal retractor and clipping the generous proximal thigh tributary. In this patient, the most proximal incision was well away from the inguinal crease, the generator of wound infections in the groin. Essentially, if there is no groin incision there can be no groin complication.
The distal vein is mobilized first before dropping on the above knee popliteal artery which is exposed through a separate incision. This is because the AK POP space is best exposed over the sartorius, and the vein in this patient was well below (posterior) to the sartorius. The vein was tunneled under the sartorius to the AK POP. With the in-situ technique, the proximal anastomosis is completed, then the valves lysed with a retrograde LeMaitre valvulotome. Doing, after two or three passes, the pulse was strong, and the flow strong enough to fling the blood beyond the foot -a key step. If there is no such flow, if there is a weak pulse, or poor blood flight, I do one more pass of the valvulotome then duplex for any large diverting tributaries and tie them off one by one until good flow is achieved.
I do not mobilize the entire vein (and tie off every collateral) unless I cannot do an in-situ technique. It defeats the purpose of this beautiful minimally invasive procedure.
Femoral artery to above knee popliteal bypass with in-situ vein
He recovered rapidly and was discharged home after a partial hallux amputation by podiatry. In followup, he was feeling better. All of his surgical wounds had healed. Duplex and ABI did find this:
Retained valve, very hard to see but present on B-mode, causing a hemodynamically significant stenosis, with ABI of 0.57
I took him to the angiosuite for repair of this retained valve. Rarely, retained valves occur after in-situ bypasses, but require generally unsatisfactory solutions involving either open valvulectomy and patch venoplasty or stenting of a virgin vein. Valvulotomy is possible, but generally described as an open procedure as well, but I had other plans.
Downstream of this retained valve were tributaries which could be seen on duplex, and therefore accessible with a micropuncture needle. This would then allow for placement of a 4F sheath, through which the LeMaitre valvulotome would pass unhindered, allowing for valvulotomy. I would use this session in the angiosuite to deliver embolization coils to the diverting tributaries as well.
Arteriography reveals a retained valve and diverting AVF’sRetained valve catches the catheter sent up and over from the other side
LeMaitre is a unique company in that it focuses on vascular surgical operations and arises from the original product and reason for the company the eponymous valvulotome. Because it comes sheathed in a low profile catheter, it is immediately familiar to modern surgeons even though it was made in another century.
Cutting of retained valve with LeMaitre valvulotome using ultrasound guidance
Cutting the valves involved passing the valvulotome several under fluoroscopy through a 4F sheath placed through the tributary seen above. After the valvulotomy, the diverting tributaries, only one of which drained quickly into a deep vein, were coiled. At the end of the procedure, a manual cuff was found and an ABI checked. It was now 1.05.
Diverting tributaries coiled
In 2015, the Oxford English Dictionary added McGyver as a verb -“Make or repair (an object) in an improvised or inventive way, making use of whatever items are at hand.” A television show from the 80’s and early 90’s, the main character, McGyver, was able to make useful tools out of what was available, allowing him to come out victorious, but usually just survive. It is a useful concept that is a must have in managing complex and dynamic situations. Just because it hasn’t been done before to your knowledge doesn’t mean that it isn’t a simple solution. I have only one ask that LeMaitre flip their blades around and design an ante grade valvulotome. Those who know what I’m getting at know what I am getting at.
The LeMaitre valvulotome allows for in-situ saphenous vein bypass, a prototypical hybrid vascular procedure from the 80’s that portended the endovascular revolution that followed. It is meant to be used intraoperatively, but because of its low profile, it can be applied.
I will allow that this second procedure likely makes any argument to cost moot, but numerous incisions and extra time in the OR is avoided. The patient now has a vein bypass that could last many years which diminishes the need for follow up procedures to maintain assisted patency.
We will be arguing this point for years even after BEST-CLI is presented. BASIL-2 just closed enrollment. Hopefully we will get some clarity.
Reference
Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014 Jan;59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12. PMID: 24126108.
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28. Erratum in: J Vasc Surg. 2019 Aug;70(2):662. PMID: 31159978; PMCID: PMC8365864.
Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005 Dec 3;366(9501):1925-34. doi: 10.1016/S0140-6736(05)67704-5. PMID: 16325694.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
The Long of It and the Short, or What You Are Trying to Do With That Level 82 Note on Your EMR?
I struggle to keep my sanity reading through electronic medical records. Medical billing pays by the amount of note written. Back in the 90’s, the insurance companies demanded that paper records be sent by mail or fax to confirm billing. Clerks in medical records departments would spend the whole day copying and faxing stacks of charts to payers and billers. EMRs were suppose to solve this, but the paradigm of the paper record lives on. Each note in the EMR is printable as a paper record for billing. It is a static text document. And like in the 90’s, billing is based on the amount of note written into the EMR. The simplest way to achieve this is to copy and paste what already exists elsewhere in the EMR -a past note, a systems review, a medical history, a spreadsheet of lab results, imaging reports. This gets you more note, more billing. The electronic medical record succeeds in its primary function as a cardboard box of copied records and as a cash register, but fails miserably in being an active part of patient care.
Any sane system would allow you to pick links to prior notes or tests -a referencing system to include even published articles, to show your logic and data, while allowing you to focus on the information that is important at the moment. The modern note needs to be turned into a searchable, linkable, living element in a dynamic database reflecting the patient’s status, a powerful tool in the patient’s care. There needs to be an App Store where third party vendors can craft solutions not imagined by the EMR. There needs to be a common file format to allow for interoperability and easy transfer of records between institutions -like JPGs and MPGs. There needs to be a complete re-engineering of the user interface. The various caregivers interacting with the EMR need to be allowed to input data in non-linear ways using mobile devices. The EMR needs to evolve to being a platform.
The Blue Ink
When I was a fellow in 2000, one of my staff, Ken Cherry, had this distinct light blue ink in his fountain pen that he wrote notes with in pithy, grammatically correct sentences conveying the diagnosis and plan. It was up to me, his fellow, to write the more detailed note, but there at the bottom, in a sky blue cursive fit for the Declaration of Independence, was the word. You just had to look for that ink in the chart to understand where the patient was and where he was going. He’d write something like, “This patient, who was seen in clinic with classic Leriche Syndrome, is now admitted with rest pain in his right foot. I intend to revascularize him after appropriate workup. My fellow will make these arrangements.” Stylistically, it was wonderful, but assumed a lot of contextual knowledge about Leriche Syndrome, and if you didn’t know, you could read Park’s two page note. He’s making the arrangements.
Compare that to an imaginary level 19 note (won’t burden you with it), rotten with copy pasted operative note and prior discharge summary, spreadsheet of laboratory values, and 12 system review of systems, 12 organ system examination, and multiparty listing of every organ in impression, bullet pointed plan, never mind that many of these have no relationship to the problem at hand. The first note is a financial disaster as it cannot be maximally billed, but it is full of meaning and action. The second note is unreadable and therefore likely unread. Like those strange tropical fruits that take power tools to get to a small bit of sweet at the center, the level 23 notes littering electronic medical records take time to pore over the chaff to get to the point which is often hidden -day to day only a few things may actually change on a note. There is just too much husk. Most of the action, the orders, have to be typed back into the note rather than automatically populating it. Supposedly, that function exists but the software has been written with the user interface of Windows from the early 1990’s and the functions are buried, only to be fished out by superusers and support staff that take time away from clinical duties to read about and learn.
Context Implied and Explicit
The fashioning of a good note recognizes that too much implied context results in confusion. Rather than say, “Leriche Syndrome,” one should say, “aortoiliac occlusive disease from advanced atherosclerosis resulting in a symptom complex of severe claudication known by the moniker, Leriche Syndrome.” The note needs to educate as much as it does document. The exposition of expertise needs to be explicit for the note to show value. Value and bill-ability do not live on the same axis. The reader should come away from the note with maximal meaning in the shortest amount of time. That means most consult notes and H&P’s need to be ideally case studies and earn their length and perform a teaching function.
Copy/Paste -Note as EMR Fractal
The position of the average physician is a poor one. The need to bill means writing long notes, but physically typing and formatting long notes is a drudgery that occupies a significant time away from seeing patients, performing procedures on patients, and thinking. The easy solution to this dilemma, the lack of time, is the Copy/Paste. There are notes where the entirety of past notes is copy pasted, creating a self-repeating element like a fractal where the entire EMR is reflected in the note. Like error mutations of the genes that persist and damage organisms, copying and pasting of documentation errors perpetuates itself and can cause disease. I remember years ago as a young staff being stuck by a needle during a procedure and dying a little inside when I checked the chart and found the patient was HIV positive. When I talked to the patient, I found out that was a persistent error, manually copied and pasted by residents and consultants, billed as a diagnosis, resulting in years of problems for the patient who had to threaten lawsuits to expunge that HIV status. Each note should be unique and uniquely authored by the caregiver, and if there is not much to report, necessarily brief. A daily summary should be generatable like those news apps that can scrape headlines and context out of the day’s production from the internet and present it to you in a easy to consume quadrilateral of data.
The Shield -Speaking to the Jury
A proper note will protect you. It is the only shield that protects you along with your education and reputation. Civil proceedings involve going over these notes in great detail and the notes should be either unimpeachably explicit or vague like a fortune cookie. Even the limited tech of current EMRs allows you to achieve granular levels of detail. I recommend referencing (but not copy/pasting) important societal guidelines and journal articles that reflect your thinking, but it the EMR does not make this easy. The hack is keeping these references as a macro to spew out relevant text. For example, if you chose not to operate on a 5.4cm AAA, after referencing the CT scan report, an image showing your measuring line, and the growth velocity from prior scans if available, a line reference to the SVS guidelines spat out by a macro gives you some shielding. But more important, in the ideal EMR, that reference would be that characteristic blue color of a hypertext link to the pubmed reference or PDF download. Hyperlinks within EMRs should be a thing. Your EMR note should be a hypertext document, not a text document, and allow referencing other notes and reports without copy/pasting them. Images, audio, and video should live within your EMR note as naturally as they do in every other document you create in 2020 that does not have to be excreted through a printer. The fact that these functions are extraneous to the primary function of the EMR -to be cheap to produce and maintain, and good for billing, means no innovation will occur for EMRs.
The Platform
EMRs vendors cling to their market share by making sharing of data impossible through proprietary data formats and security regimes. Health care systems have no incentive to make their patient information transferable beyond a minimum of paper or their PDF equivalent. Patient safety and information security is invoked for preventing needed innovation. For the patient, this can be a life or death issue -the ability to transfer health care data. Imagine if you are the patient with a ruptured aortic aneurysm who is transferred without the CT scan burned to a CD. In 2020, NO.ONE.USES.CD’s. I can download a 4K file of the last Avenger’s movie in 30 seconds on the right network, but a lifesaving CT scan -NO WAY!
A more everyday example is a patient seeking a second opinion or moving cities to a different health care system. The only way to move the data is an expensive printout of the chart. How can we keep this important information linked with the patient? Social media has cracked this. Your Facebook is a good model of what a potential EMR 2.0 could be. A patient-centric EMR would be controlled by the patient in terms of access control. Federal laws would prevent misbehavior by the EMR vendor. The patient’s data generated by practices or hospitals would be owned by these practices or hospitals but posted on the patient’s EMR, in specific specialty adapted formats. Temporal ordering would be natural, not based on shuffling reams of paper or virtually with PDFs with overlapping timelines. More importantly, imaging data and lab results would be immediately available to all healthcare providers through access to the patient’s EMR. Practices and hospitals would pay a nominal fee to the EMR provider much as advertisers are on Facebook. Patients would be in control of who gets access to the data, and importantly if they want to participate in research. App developers would proliferate and innovate in the space, providing functionality via apps in a marketplace, allowing different specialists look at the data in their own particular way, and patients to understand their data on their own terms. Gaming companies, for example, could take the virtual coordinates of a CT scan and match it up with ultrasound and MRI to do a lot of cool stuff. EMR 2.0 is not more ways to personalize your window with colorful graphics. EMR 2.0 is a complete upending of the way patient data is stored and moved, and it will take an act of Congress to make this happen. EMR 2.0 recognizes that it needs to become a platform and it needs to be a part of a collective national effort. EMR 2.0 needs to be a platform, not an app.
A Multimedia EMR
The EMR needs to incorporate multimedia. Current EMRs live in the tech levels of the early 1990’s. Imaging studies must live as actual windows in chart notes. Video or voice comments must be documentable in the chart. Hypertext to the resources of the internet must live in the chart. Data must flow just like blood.
This should suffice as an op note
Shape of the Future
As a vascular surgeon, the most important function is to provide an accurate documentation of the condition of the blood vessels to date, the current condition of the blood vessels, and the future fate of the blood vessels and the patient. Technology needs to help the vascular surgeon in this role, and most importantly, the patient. Tech is not a third party vendor in this battle space. Tech is a caregiver, and must be held to the same standards placed on physicians, nurses, and technicians. Until that day comes, we as vascular surgeons must write amazing, publishable case reports for the consult notes, and short pithy updates for the subsequent notes.
Mid Century Modern is a design philosophy from the mid twentieth century that seemed terribly dated and out of style while I was growing up but now seems to have come back as people dig around their parents and grandparents’ stuff. Television shows like Mad Men and Marvelous Mrs. Maisel are rotten with mid-century design. Yet it is an apt term for vascular surgeons of a certain generation like me who at about fifty years of age remember a time when vascular surgery was about big incisions and bypass grafts. We were trained in open vascular surgery and rode along with (or were drowned by) the tsunami of endovascular techniques that have come to dominate. Most of us learned to do them as well. Mid-century vascular surgeons straddle the divide between our mentors who, like me, specialized in vascular after completing general surgery training and the current trainees who have trained solely in vascular surgery. At one time it was fashionable to believe that we were fossils. But, like the coelacanth discovered after an eon’s absence, guidelines and recommendations are being made for open surgery which is supposed to be making a comeback. But it turns out, open surgery-capable vascular surgeons are, like the coelacanth, rare, and endangered. Unless we completely change the way we train people today, open vascular surgery will become extinct. At first glance, it does not look good.
The Dinosaur
My first ever encounter with a vascular surgeon was in 1989, as a lab tech in Boston the year after I graduated from college. It was at the West Roxbury VA Hospital, and like the vets, this one chain smoked in his office. Friendly enough, but a bit aloof, he rasped out well elocuted English in the same way soldiers did in old war movies like The Longest Day. Laconic and Robert Mitchum-like. He would have been among the first generations of vascular surgeons, contemporary to Jack Wylie, Michael DeBakey, and other luminaries. He couldn’t have cared less, I believe, as he performed fem-pop and aortobi-iliac and femoral bypasses and carotid endarterectomies with a furious incandescence that didn’t jibe with his reserved demeanor outside the OR. He was equally fierce to the residents when he had to scrub in to get them out of jam. But he was kind to the medical students and pre-meds like me. His type of surgeon is most definitely extinct, remembered only in old war stories like this.
What is it about my generation of surgeons? We remember things and balance the new against the old ways. We remember a time before work hours restrictions but are young enough to understand why it is not too healthy to work 120 hours a week. Yet we are also conflicted about the benefits we retained from that kind of training, now viewed with about as much approval as Sparta’s agoge system of child abuse and military training. I trained at the outset of laparoscopic surgery, so I did about 50 open cholecystectomies before learning how to do laparoscopic cholecystectomies. Most of my appendectomies were done open. As were my colectomies, gastrectomies, thyroidectomies, mastectomies, and yes, aortic surgeries, carotid endarterectomies, arteriovenous fistulae, and leg bypasses. And I did them.
We All Agreed…
This was the deal. You worked at 110%, fell exhausted and gave a little more, and you were rewarded. That meant being up all night on call, but after morning rounds, you could turn your pager off and operate all day. If you were learning, you had to be prepared by knowing the patient, the disease, the anatomy, and the operation. If you were teaching, you had to have the approval of the attending who would be somewhere nearby, and never happy if you grabbed them. If you were chief resident, you were basically junior staff and expected to run your service like a practice. The leash was longer for those who could, and short for those who could not. In the grade before mine, it was pyramidal, meaning there was attrition of those who could not progress. Like ringing the bell at Navy SEAL school in Coronado, people quit. Or were, rarely, fired. Being categorical was seen as a kind of entitlement by the disbelieving chiefs welcoming the new categorical interns. Dishonesty was the worst sin, but weakness, like showing fatigue or expressing a desire to have a life outside of work, was equally bad. And training was long. Four years of medical school, followed by five years of general surgery residency with mine extended by a year of research between third and fourth year, and then followed by a two-year vascular fellowship. By the time I was a full-fledged vascular surgeon, I had college friends who had actual homes and summer homes, children, divorces, and travels around the world. They had lived real adult lives. I started out on life at 35 where everyone else had done it at 21. But I had 1600 cases in my residency, of which over 300 were major vascular including 50 open aortic cases, and nearly 500 cases during my fellowship, adding another 100 aortic cases, most of them open, as it was the first years that EVAR was introduced. Nothing better in the world than to start a case with Ken Cherry quipping over your shoulder -“make me proud.” I finished my endovascular training apprenticed to Dan Clair during my first staff job at Columbia P&S -cue Dan intoning “you’re killing me” over the Cath Lab’s PA from the control desk on the weekends we had time in there.
There is no going back…
That represented one way of training a vascular surgeon. Even after graduating, I never stopped learning and perfecting my craft. The two years at Columbia gave me insight on how to run a practice completely alone -I was the lone vascular surgeon up at the Allen Pavilion on the northern tip of Manhattan next to Baker’s Field. It taught me the critical importance of availability and extracting useful information over my tiny flip phone. During my private practice years in Iowa, I learned the amazing productivity that can be attained when you work in collaboration and partnership with cardiologists and cardiac surgeons -something I do today here in the Heart and Vascular Institute. I also learned how to use vascular technologists and the lab as a force multiplier. And it was during the Iowa years that I underwent a period of endo-enthusiasm followed by a realism and I performed over a hundred aorto-bifemoral bypasses on middle aged patients with an average length of stay of 3 days, no deaths. When I plunged back into academia, taking a position at Cleveland Clinic, I was apprenticed again to Dan, but this time in understanding how to use the whole clinic as a tool for taking impossibly challenging patients through to an acceptable resolution. All of that started with those frantic days on call as an intern at St. Luke’s Hospital, drawing blood cultures, placing IV’s, babysitting traumas in the CT scanner, and putting chest tubes into the perforated. But there is no going back. It is most definitely probably illegal today to subject people to the intensity and duration of experience that I went through. And I wouldn’t trade that experience for all the treasure in the world (although I do regret not buying Apple, Dell, and Microsoft in 1994).
What a completely trained vascular surgeon can do
The hardest case that I have taken care of ever was at the Clinic a couple of years ago. The patient was a middle aged man who had ruptured an aortic aneurysm in another state some months prior and had undergone a repair complicated by a pancreatic injury along with some enterotomies resulting in a graft infection along with high output pancreatic and enteric fistulae from an open abdomen. He arrived cachectic, in septic shock and had a pseudoaneurysm from the distal anastomosis of a short tube graft. I immediately took him to the OR to place a stent graft across the pseudoaneurysm neck to prevent rupture and placed him on TPN to correct his cachexia. The abscesses and hematomata were drained percutaneously, and an effort was made to control the fistula with a heroic effort on the part of the ostomy team. He turned around and was able go to an LTAC on TPN and antibiotics. There he gained twenty pounds and returned flush and active. Stage two was three months later and done to replace the still infected grafts with cryopreserved homograft. I did this via a right retroperitoneal approach as the left side and abdomen were a mess from the inflammation. After I removed the grafts and sewed in the homograft, general surgery reorganized his bowel and discovered that he only had about 30cm of useable small bowel and would be on TPN for life. But he was alive and learning to walk again, and eventually came back 6 months later for follow-up and gave me a hug.
That case took all of my skill to solve, and I could not have done it without the whole hospital working in sync with me. When it comes my time, I wonder who would be able to do that for me?Who would manage my ruptured AAA properly and not have bowel and pancreatic injuries?
How to do a CABG according to Dr. Swistel
When I was an intern, I wanted to be a cardiac surgeon more than anything else, and got myself slotted for 6 months of cardiac during my second year. It was an unwanted rotation because of the 5am to 11pm hours, all nighters in the unit on call, and because the CT surgeons were notorious for not letting you do anything, except for Dan Swistel. Years before he had been one of us, a resident at St. Luke’s/Roosevelt and was Dr. George Green’s protege. He had a deal with us where he had you learn and master all the following steps in this order:
1. take vein
2. put in pacing wires and chest tubes
3. close chest
4. open chest
5. open the pericardium and set up the way he wanted
6. put the venous cannulas in
7. put the arterial cannulas and secondary lines in and go on bypass
8. decannulate and repair
9. dissect the aorta, set up and place the cross clamp
10. do the proximal anastomosis on the vein grafts
11. do the distal anastomosis on the vein grafts under the microscope which was the way he and Dr. Green did it.
12. dry up…really dry up and learn to come off pump
13. take mammary
14. book a ward service CABG and do it skin to skin
Through the history of St. Luke’s up to that point, most residents never got past taking vein. That was the great barrier, and most people really didn’t stick around after taking vein and closing the leg. They did not see the point of standing around and second or third assist. Those residents who were going to Cardiac did make it to taking the mammary, but only a handful by chief year. No one made it to 14. Dr. Swistel was always true to his word, even though some residents suspected this was all some bet that he had between himself and his brother who was not a cardiac surgeon -something about I can train a monkey to do this. To me, that last step, doing a CABG skin to skin, seemed like the final level of a very difficult computer game, like casting the One Ring into the volcano, like blowing up Agent Smith.
Every step on the ladder was something I immediately applied to my general surgery experience. On call and at home, I practiced. I practiced holding the instruments correctly and performing anastomoses on discarded grafts. I learned that every hard operation is made up of small technically feasible components, so I worked to make those moves natural and smooth. I progressed rapidly up the ladder and was by the end of my last cardiac rotation firmly at 13 on more than one occasion. Every other part of my skill set expanded during this time -central lines went smoothly, appendices and gall bladders were fished out efficiently, and fear shifted its focus to different things from what made me anxious as an intern. I learned the skill of keeping people alive through the night and making the call to take people back.
With some social engineering (ordering the cardiology fellows takeout Chinese) and vacation days traded, I got to that last step during my third year. If not a monkey, then at least Park. The act of learning and mastering each component skill lets you start and finish an operation. I don’t think Dr. Swistel was ever out to lunch while I was operating, but all those moments of letting me take the knife was crucial to my education and I am grateful to him and all my teachers, including my current partners and colleagues, as I approach PGY-25. As surgical educators, we must recognize that surgery at the sharp end of the knife is a precision craft that has to be taught much as tennis is taught starting with grip, stance, swing. That golf is learned on a driving range with a bucket of balls.
The Mid-Century Vascular Surgeon
Like Mid-Century Modern Design furniture, surgeons in my cohort are sought after by hospitals and practices for being able to let a hospital do more. What do I mean? A urologist resecting a kidney with a renal vein tumor thrombus extending into the inferior vena cava needs to have someone expose, extract, and repair the vena cava. A gynecologist debulking retroperitoneal metastases needs to be able to call for help when part of the aorta needs to go with the tumor. Cardiac surgeons need to be able to place ECMO cannulas in imaginative locations and not lose extremities in the process. A thoracic surgeon resecting a Pancoast tumor needs a vascular surgeon to repair the subclavian artery and vein. An orthopedic surgeon resecting a spindle cell tumor from the thigh needs help reconstructing the femoral artery and vein. And so on. We are safety net, the fire brigade, the SEAL team, and unfortunately many hospitals understand only when their last fully trained, full service vascular surgeon retires.
Vascular surgeons are a keystone species in a hospital’s ecosystem. When wolves were reintroduced to Yellowstone, it was noticed that decades later the forests returned to their ancient glory, that wetlands flourished breeding fish and insects and small mammal species, and the secondary predators that feed on them, and many missing bird species returned. Vascular surgeons capable of operating on the whole body as well as intervening on the whole body are increasingly a missing element in a hospital. And many of us chose to go missing -into our private endovascular suites and vein centers because it often does not pay to go do a 5-hour bypass when you can do three femoral angioplasties for claudication in the same time. Reading 10 carotid ultrasounds is easier on the back and more renumerative than a carotid endarterectomy. And I am not judging -it is a rational choice that is framed by the way healthcare is reimbursed.
The solution starts in the US with a shift in reimbursement to recognize the time and effort required to perform open vascular surgery well and to reward the programs and surgeons who are consistently good. Training in open vascular surgery will be sought after much as everyone wanted to be a cardiac surgeon back in the 1970’s. Government and society mandates set the menu, but the economics determine what is served.
And finally, every year thousands of surgeon-years of experience is retiring with the very skills that are now sought after. Rather than lose this human capital to golf courses and beaches, we should be grabbing them at the door. Like those mid-century chairs and tables, we have always been there somewhere, and its time to make some more.
I taught myself to draw during medical school when I couldn’t figure out the three dimensional relations of structures. I discovered that if you just draw the shading of an object, it pops out in three dimensions. Over the years, I took to carrying little notebooks to sketch out anatomy and proposed operations for patients through this medium. While I found this to be a handy tool that I used only occasionally, since moving to Abu Dhabi, where much of my communicating is done through an interpreter, my drawings carry a much greater weight as direct communication of my thoughts and intentions.
Drawing helps the patient and family understand the unseeable. It gives form to words that are often confused like blood vessel, graft, stent, artery, and vein.
What is informed consent when patient’s cannot describe their problems to their friends and relatives what the problem is and what is going to be done about it?
I usually draw with the pen in my shirt pocket and some copier paper, but sitting down and doing a proper sketch is soothing and very helpful for me as the surgeon to previsualize the goals that I have to reach during an operation to take the patient across the finish line. During meetings and conferences, I sketch into one of those fancy bound notebooks that I collect.
Funny thing is I was doodling during class as a kid, but it was spaceships, not aneurysms.
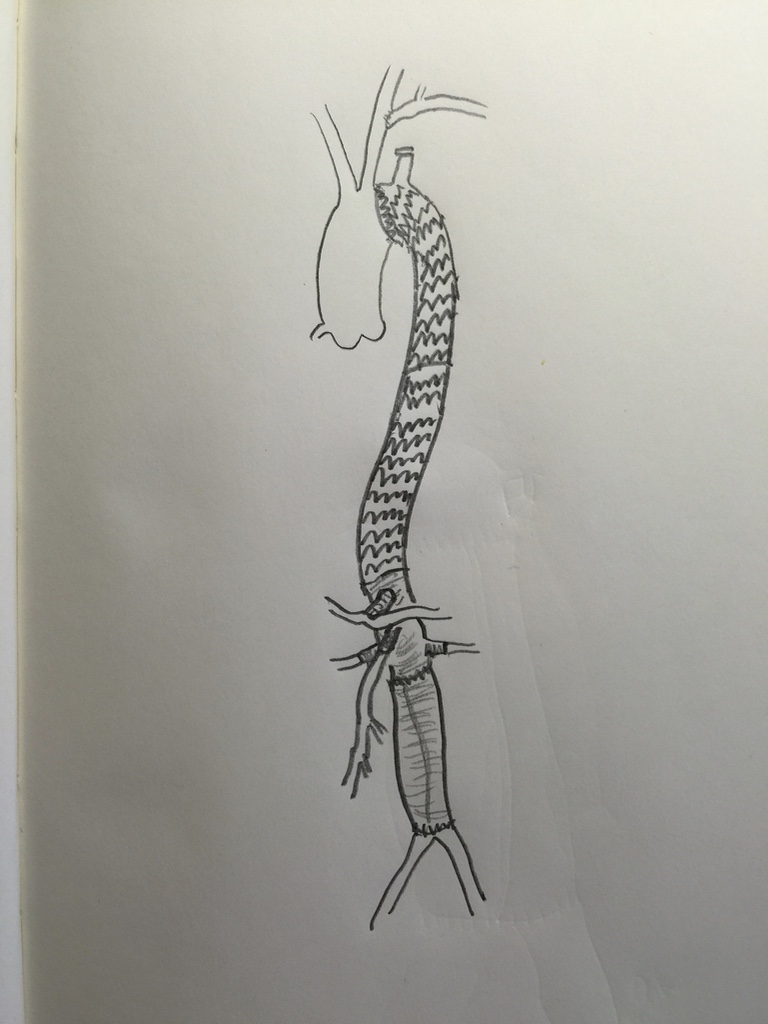
While pencil and markers do a fine job, the real magic is in using tablet based sketching software, using layers, to build serial images of the steps of an operation.
I am increasingly tempted to use these images as my operative note, but understanding that words are needeed for billing, I comply. Even so, I find it helpful to put these illustrations on my EMR notes, because it allows everyone to see and understand what I saw and what I did. I leave you with some of my illustrations with attached comments.
Long segment disease stents in their natural occluded state
Our best shot
The nutcracker
The fractal
Hybridized aorto-bi-iliac revascularization
Retrieving the unretrievable embedded filter
3 step treatment of a type II thoracoabdominal aortic aneurysm
View out of my balcony, sometimes you need many pieces to assemble a beautiful whole
Innovating Our Way Out of Not Having Enough Vascular Surgeons
This year’s SVS meeting featured a sobering assessment about the vascular manpower deficit affecting North America at the E. Stanley Crawford Critical Issues Forum, moderated by Dr. Michel Makaroun, MD, president-elect of the SVS. 35-45% of practicing vascular surgeons plan on retiring in the next decade by conservative estimates. We are not attracting enough candidates for the training programs. The solutions, including decreasing the length of training, public relations campaigns, and incentivizing retention have had mixed results, but we have yet to see a sustainable rise in vascular surgeon numbers.
Burnout driven by lack of work-life balance, the advent of electronic medical records optimized for billing, the passing of the private practice era, and the constant need to adapt to new techniques, create a persistent downdraft on staffing. So as some hospital face the reality of having to contract services, little attention is given to delivering best care with the staffing that we have. Changing how we practice is the only viable solution.
There are an estimated 3000 active vascular surgeons in the US. Imagine if all the cheese needs of this country could only be met by 3000 artisanal cheesemakers who make cheeses one at a time and want to live in places with international airports, BMW dealerships, and major league sports teams, and must have 3-4 partners to share cheese call. If you are a rural hospital in dire need of vascular surgery services and your one vascular surgeon is retiring, you are probably SOL.
When I was training, vascular surgery was oft touted as a primary care specialty. And that is how many of us still practice, managing risk factors, monitoring mild disease, as well as planning and performing interventions and operations. As much as I enjoy that kind of interaction, the half hour to an hour visit for a head to toe cardiovascular survey and discussion, educating patients and families about pipes and pumps, is incredibly inefficient. A healthcare system, a hospital, facing a staffing shortfall, has to do everything possible keep that vascular surgeon in the OR during work hours.
What is the core function of a vascular surgeon? Making good decisions and executing plans well. Decisions require data. What is this data? We laud the history and physical examination, but this is a throwback to another era. If you look at the diagnosis of myocardial infarction, it is not standard practice for a cardiologist to come and get a history, examine the patient, and declare that the patient is having a heart attack based solely on history and physical examination. It is a triage nurse in the ED who draws labs and orders an EKG which is read by a machine. These data points will tell you if heart muscle is being damaged. A process is started which triggers a team to come and take care of this patient. The hospitals focused on this actually drill their cath lab teams like pit crews. A stopwatch starts with the goal of revascularization under an hour.
Not so with peripheral vascular disease. The ischemic foot might have only a few hours depending on its presentation before it is irretrievably lost, but no matter -they sit in the ED until a vascular surgeon comes to speak to the patient and family, examine them, and then order tests, admission, consults, and operating room -typically all by themselves. Getting these patients into the operating room is in many places hampered by the lack of dedicated OR staffing, radiology techs, anesthesiologists, space, equipment, and critical care capacity. During work hours, there are scheduled cases that have to be delayed or canceled for another time, which takes time to do. After hours, the patient may have too many comorbidities to handle safely with the available staff. The vascular surgeon may have to bargain and cajole, to align several factions whose attention is demanded by many equally important concerns. If you decide to hold a lavish dinner party of twenty important guests -reserving space, calling caterers, inviting guests, arranging transportation – on short notice, you might pull it off once, but if you do this regularly, you are a masochist of the first order.
In the heart attack model, the history and physical examination is relegated to a series of yes/no or how long questions, and positive responses trigger a series of coordinated actions of a system -a reflex. In the leg attack model, there is no such system. I have to blame the vascular surgeons for preserving the current model. Vascular surgeons are organized as a guild. Guilds are protective of their monopolies on skills and markets and fiercely resist change. Most vascular surgeons are terrified by loss of control, and cling to the notion of being misunderstood and unappreciated saviors. We can do better.
The area that needs streamlining is at the point of referral. The majority of time of a vascular surgeon is spent working up normal blood vessels, varicose and spider veins, leg edema and pain, and mild and moderate arterial atherosclerosis. This work initially does not require a vascular surgeon but rather a focused set of policies and initial diagnostic studies that can be administered or ordered by any caregiver. Reducing the need for vascular surgeons at this point in vascular care will go a long way in extending the vascular work force at hand.
Point of Care Blood Flow Evaluation
Finding and declaring blood vessels to be normal is challenging and too often time consuming. Streamlining this will go a long way in freeing vascular surgeons to take care of disease.
The average caregiver is an inconsistent pulse taker. The palpable pulses are not always easy to find. Asking over the phone or as policy for someone to examine pedal pulses -the posterior tibial artery and dorsalis pedis artery pulses, is challenging. A positive is just as likely to be true or false as a negative. No cardiologist would ask a similarly detailed and technical question about an MI. In fact, they can’t ask, “Is there a pulse in the LAD?” Cardiologists make do with tests easy to obtain and interpret with certainty -the plasma troponin level and the EKG. The EKG is read by an algorithm so established and so tested, that it should stand as an example of early machine intelligence taking over a human job -but I digress.
What is our EKG? It is not the ABI -the ankle brachial index, because it is terrible at identifying disease, and is difficult to obtain reliably without practice. The closest thing to an EKG we have in terms of simplicity and accuracy is the pulse volume recording, the PVR (figure below). A FloLab machine, the machine used to obtain PVRs, will basically run itself once the cuffs are correctly applied on the leg, and the tracings are very easy to interpret. Unlike an EKG, there are no electrodes whose locations you must memorize. If the closest vascular surgeon is an hour away by ambulance, the transfer of a patient with flat waveforms and ischemic foot does not require a consultation on site. The patient would go to the vascular surgeon with no time wasted and no kidneys injured by CTA’s that too often fail to travel with the patient. Unlike an EKG which can be performed by many caregivers, a PVR requires both the equipment and a vascular technologist. A vascular technologist is not available 24-7 in most hospitals, and FloLab machines purchased for vascular labs are not meant to be dragged around the hospital.
So let’s think out of the box about another box in every triage nurse’s cell, every ER and ICU bed, and on every hospital nursing floor. These are pulse oximeters with a digital tracing, and bonus points, some come with strip printers! Placing a pulse oximeter probe on the second toe and comparing to an erstwhile normal wave signal such as on an index finger can provide qualitative information about normality and disease. Normal waveforms and abnormal ones can be easily discerned. A flat line is another obvious finding when in comparison, a finger or an ear on the same patient has normal signals.
How much better would a vascular surgeon feel about a transfer call that has this information, “digital waveforms are flat in this patient with rest pain and a bruised toe.” How much better would a vascular surgeon feel about a call about a patient with “digital wave forms are normal in this patient with toe pain and a bruised toe. We got an x-ray and there was a fracture.” The communication can be quite detailed and refined. For example: “The patient had no pulses, we think. Digital wave forms were dampened but pulsatile in a patient with a bruised toe, we’ll send to vascular clinic in the morning.”
A study comparing pulse oximetry signals and ABI in type 2 Diabetes Mellitus found the following results (link).[i]
Method
Sensitivity
Specificity
PPV
NPV
Pulse oximetry
74.1%
95.7%
83.3%
92.7%
ABI
70.3%
87.1%
61.3%
91.0%
These data suggests pulse oximetry signal is equal to and somewhat better than ABI. Why is this important? Cost. This information is better than asking unsure people, “Is there a pulse?” A vascular technologist need not be on call 24/7. Extra FloLabs for ED, ICU, and floors need not be purchased. The pulse oximeter with waveform tracing is nearly ubiquitous wherever patient’s oxygenation needs to be assessed in most hospitals. While not perfect, it has great potential for serving as vascular surgery’s EKG machine for critical limb ischemia. Policies and algorithms can be built out in collaboration with Emergency Departments and nursing departments that can effectively determine if blood flow is normal or abnormal at point of care. Effective emergency responses to critical limb ischemia can be authored triggered by abnormal findings. Acute limb ischemia protocols based on time sensitive responses can be initiated. All of these can flow from referring entities being able to determine objectively normal or abnormal blood flow.
Clinic
The vascular clinic is a sorting process where patients are determined to be normal or have mild, moderate, or severe disease. The vast majority of the time spent in clinic can be spent in triage by trained nurses and testing by technologists. Clear pathways and guidelines can dictate the ordering of vascular laboratory tests obviating the need for vascular consultation at this stage. Patients with normal blood vessels and vascular function are sent back to their physicians with the normal report. Patients with mild disease and moderate disease are sent to a physician with specialization in cardiovascular medicine for management of risk factors and periodic surveillance. At any point in the process, a vascular surgeon can be called to provide guidance and direct patients to different tests and consultations. The patients needing operations, based on correct indications and imaging are sent to a focused clinic where the surgeon and interventional team can review films, determine the urgency of indications balanced against risk, and plan and schedule procedures. Currently, vascular surgeons do all of this by themselves, as well as make hospital rounds, perform procedures, and interpret vascular laboratory studies, seeing one patient at a time.
In introductory computer sciences courses, search algorithms are taught to be brute force if you look at one item at a time for the thing you want, and to be efficient if you have presorted those items because every time you look, you can exclude part of the data set, ever shrinking the pool in which you search, making the search shorter and faster
The shortfalls in vascular surgeon numbers have as much to do with this dependence on the star chef cooking up one meal at a time, rather than a team working off recipes, with the chef directing the flow and occasionally jumping by the fire to make the most difficult of dishes. The first restaurant can seat three parties. The latter, easily ten times the number. Everyone gets fed.
Only asking how many vascular surgeons you need misses the big picture because there are many equally important questions. How many vascular technologists do you need? An accredited laboratory provides the critical diagnostics upon which decisions are made, and the surgeon should oversee but not be directly involved in the initial screening. Nurses trained to triage and order vascular laboratory tests and even perform the simpler ones is the second need. Third, is the cardiovascular medicine physician who manages those patients discovered to have mild to moderate disease, and depending on symptoms, refers severely symptomatic moderate disease and severe disease to a scheduling clinic. The scheduling clinic is composed of both interventionalists and vascular surgeons who plan interventions and operations.
Surgeons must be in the operating room to be effective. A well thought out and organized system, with interlocking teams, and well disseminated basic knowledge and awareness of vascular diseases reduces the need for a vascular surgeon to be present all the time in many places and ultimately increases the effectiveness of the vascular surgeons that are available by keeping them in the operating room. The system needs to be set up by the surgeon to allow clinic to be a setting mostly for consenting the patient for an operation or a discussion of treatment options.
Finally, vascular surgeons must be aligned with all the resources of the hospital including the considerable numbers of interventional cardiologists and radiologists, neurologists, and nephrologists. There is no reason someone should wait a month to get on the OR list for an iliac angioplasty and stent if an equally skilled and privileged cardiologist or radiologist has an opening the next day. The surgeon’s special talent should be open surgery and hybrid surgery -that which mixes open surgery and intervention in optimal measures which is not possible from a purely percutaneous approach. The key is frequent and easy communication between specialities and trust built by being in one shared cardiovascular institute.
Execution
There is a critical need of good operators. The acuity of disease and their solutions demand the continued presence and availability of open surgery. The fact is, many solutions are optimal in a hybrid fashion and for peripheral vascular disease, these options can only be offered via a vascular surgeon trained in both open surgery and peripheral interventions, or in a combined effort of open surgeon and interventionalist. And many disease categories can only be managed by open surgery.
The reality is that silos, economics, and practice patterns prevent this kind of combined effort. Market forces have pushed the training of vascular surgeons forcefully into the interventional realm at the cost of open surgical training. Some of the geographic maldisdribution of vascular surgeons has to do with younger vascular surgeons flocking to established practices where there are senior surgeons more comfortable in opening a belly or chest (or both). The trap they and hospital systems fall into is then allowing these new recruits to become the interventional specialist of that group, relegating the aging open surgeon to a narrow role, and then finding that the hospital has a problem when that surgeon announces retirement at 60. Every year, millennia of surgical experience retires to beaches and golf courses. The hospital systems should recognize this brain drain as a crisis and create work arounds that keep these skills going. The other opportunity lost is close coordination with interventional cardiologists, radiologists, and nephrologists who in many cases compete with vascular surgeons for the same patients but treat the patients based on their training and skill sets to the exclusion of potentially better operations offered by surgeons. This disjointed care creates both suboptimal outcomes for patients and high costs for hospital systems.
Commerce should never dictate the fate of a patient. A particular point is where competencies and privileging overlap, and guidelines recommend intervention over surgery as in the case of a TASC A or B iliac artery lesion. A patient should not be kept waiting weeks for a spot on a busy surgeon’s OR schedule when an open interventional cardiologist or radiologist slot is available for a iliac stent the next day. It should be a matter of practice that these cases are discussed and distributed, optimally in a shared indication clinic or rounds. Patients bumped off of a surgeon’s elective schedules for emergencies who could be cared for by an interventional partner without an added delay should be given that option. This kind of change requires a commitment to continual reorganization and optimization into a vascular institute.
Conclusion
The perfect vascular surgeon is a unicorn -well skilled, and experienced in open vascular surgery, but also versatile, innovative, and skillful in wielding a wire. I can name just a handful of unicorns. An apt analogy from the book Moneyball is the signing of superstars in baseball on the free agent market. The upshot of that book is that you can arbitrage for the valued metrics through signing several utility players with an aptitude for one thing or another which in sum equals or exceeds that superstar and get the final result -wins, in the same proportions as overspending on a superstar. Rather than searching for that unicorn, it is more important to set up the right system. Screening, testing, and management of mild vascular disease by a nurses and cardiovascular medicine physicians, while directing operations and interventions to vascular surgeons, cardiologists, and interventional radiologists should be the next step in the evolution of vascular care systems. There will never be enough vascular surgeons in the current system. The critical and rare competency is open vascular surgical skill. A surgeon who performs only interventions is not an “advanced minimally invasive practitioner” but rather someone equally privileged as an interventional cardiologist or radiologist, and therefore easily replaceable by an interventional cardiologist or radiologist specializing in peripheral vascular disease. A surgeon skilled in open vascular surgery is becoming rarer every year, but they are still out there, looking at brochures of real estate in sunny places. A team consisting of a cardiovascular medicine physician, many vascular technologists, nurses specializing in vascular diseases, several interventionalists, and a vascular surgeon skilled in open vascular surgery working as a single unit, is far more easy to assemble than finding and recruiting a herd of unicorns.