

The patient is an elderly man who had bilateral above knee amputations after failure of aortobifemoral bypass grafts at an outside institution. Unfortunately, he had no femoral pulses and his amputation on the right broke down (image above). His left stump had erosion of his femur to the skin with rest pain as well, but was at least covered by skin for now. He was declared too sick for hip disarticulations and was sent to a hospice where he failed to pass away. After a year there, he was sent to us for an evaluation.
He was suffering from rest pain and had complete breakdown of the skin over his amputation stump. More worrisome was the development of gangrenous scrotal and decubitus ulcers which were small but persistent and also foci of pain. CTA showed the following:

The aorta was occluded below his renal arteries. An AV fistula near his common femoral vein lit up his right iliac vein on the CT above. He had had a prior aortobifemoral bypass but this was occluded. Gratifyingly, it was anastomosed proximally end to side, giving us options. As with any revascularization, we had an inflow source -his aorta, and several potential outflow sources (CTA below, contrast filling iliac vein from AVF’s).

In particular, his distal profunda femoral artery showed promise. Vein mapping revealed a short segment of basilic vein in his arm to use as bypass, but we needed inflow from the aorta.
I have come to appreciate two things about aortoiliac recanalization. First is that passing the wire antegrade is far likelier to stay in the true lumen at least in the aortic inflow segment -retrograde wire passage inevitably dissects the occlusive aortic plaque and reentry into the true lumen of the diseased aorta is just as challenging as in the leg. The second is vein bypasses have excellent patency in challenging conditions -you just need excellent inflow and an arterial bed to perfuse.
My plan was to cross the aortoiliac occlusion with a wire from the left arm. Once the right iliac system was entered, it didn’t matter if I was in a subintimal plane. The wire could be seated in the common femoral artery to access with a surgical exposure. Once this was done, my intention was to perform remote endarterectomy of the external iliac artery and stent from the aorta to the common iliac artery. The endarterectomized external iliac artery would be the inflow source of a later staged ilio-cross femoral bypass to revascularize his left AKA stump. The common femoral artery at its origin would provide inflow to a short vein bypass to his profound femoral artery.
The wire passed readily into the right iliofemoral system and a groin exposure and common femoral arteriotomy allowed me to retrieve the wire which had been passed from the left arm. A remote endarterectomy was performed over the wire which I do to ensure access in case the artery ruptures (specimen below).

This allowed me to place a sheath into the right iliac system in the now reopened external iliac artery. Balloon angioplasty of the aortoiliac segment created working space for placement of balloon expandable stents from the infrarenal aorta to the common iliac artery, restoring an excellent pulse in the right groin.
The profunda femoral artery was encased in scar tissue, but following the occluded PFA from the CFA, I was able to expose an open segment and cut it open in the scar tissue. There was back bleeding, and I controlled the artery by placing a small Argyll shunt into the artery and reperfusing it from the recanalized right iliac system.

The Doppler flow in the shunt was excellent, suggesting great outflow potential. The bypass was performed over the shunt with reversed basilic vein. Completion arteriography showed excellent flow.

The amputation stump was debrided of dead bone and muscle and the graft was covered with a sartorius muscle flap.
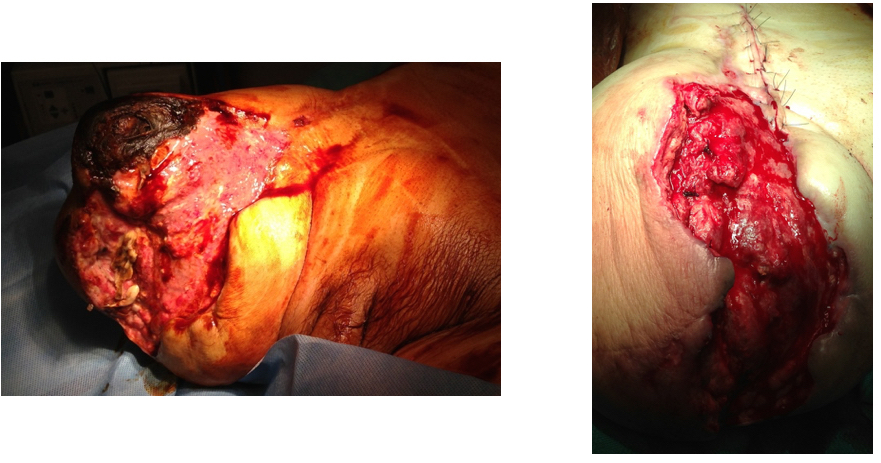
Before and after images are shown. The remaining open wound granulated well, and ultimately accepted a split thickness skin graft. His scrotal and decubitus ulcers healed as well (below at 6 months post op).

His left AK stump subsequently degraded while he recovered so three months after this operation, he underwent a right external iliac to left profunda femoral artery bypass with cadaveric vein.


I don’t like using cadaveric vein, but we really had no options. The right external iliac artery was approached through a right lower quadrant (transplant) incision and a punch biopsy of the artery revealed only normal adventitia on pathology. The EIA was soft and sewed well -essentially a normal artery brought back from the dead. The left profunda femoral artery was large after endarterctomizing its origin and accepted the bypass flow well.
The mortality from hip disarticulation in the setting of gangrene and infection is very high, and I feel that standard approaches to this problem -prosthetic axillo femoral bypasses, thoracobi-femoral bypasses, in the setting of advanced infection and gangrene were unlikely to succeed. In over 1.5 years of followup, everything has remained patent, and the patient lives independently.
