

Recalling the medical school adage, “when you hear hoofbeats, it’s probably horses, not zebras,” it is critical to think about rarities down on the differential list whenever you come across a patient. Vascular diseases suffer from inadvertent obscurantism arising from its absence from medical school curricula such that common disorders like mesenteric ischemia and critical limb threatening ischemia are frequently missed by even experienced medical practitioners. Vascular zebras are even harder to pin down because many experienced vascular specialists practice for years before they encounter, for example, adventitial cystic disease or dysphagia lusoria with a Kommerell’s diverticulum. Even so, real patients have these disorders, and we are all subject to inexperience bias -the feeling that something does not exist until you see it. You may completely miss something staring at you in the face or worse, deny its existence.
The patient is a middle aged man in his 50’s who aside from mild hypertension had no real risk factors. One day, at work, his right leg stopped working. He developed a severe calf cramp and the forefoot was numb and cool. He went to his local hospital and the doctors there appreciated the lack of pulses in the right leg and got a CTA, of which I only had the report which found a right popliteal artery occlusion.
The next morning, as he had signals and was not having rest pain, his doctors discharged the patient on clopidogrel and scheduled for angiography and stenting, per patient. As his debilitating claudication did not go away over the weekend, he came to our emergency room. While he had no rest pain, he did have minimal walking distance before his calf muscles seized up. On exam, his right foot was cool and cyanotic, with intact motor function and sensation. There was a weak monophasic posterior tibial artery signal. Bedside point of care photoplethysmography showed dampened waveforms (below).

Because he did not bring his CT, I repeated the study. I have written extensively on the need to be able to share CTA studies without barriers. After his study, I brought it up on 3D reconstruction software.

It clearly showed a Type II Popliteal Artery Entrapment affecting both legs (CTA images in series above). Stenting it would have failed. I spoke with the patient about operating the next day. The plan was popliteal artery exploration and thromboendartectomy with myotomy of the congenitally errant medial head of the gastrocnemius muscle. The patient was agreeable and I took him to the operating room for a myotomy and popliteal thrombendarterectomy in the prone position. The medial head of the gastrocnemius muscle went over the popliteal artery and inserted laterally onto the femur.
The artery was opened and while there was fresh clot, the artery showed signs of chronic injury as evidence by endofibrosis which pealed off. Pathology showed to be fibrotic in nature.

The artery was repaired with a pericardial patch and flow restored to the tibials, not all of which were completely patent.
The patient was discharged after about a week and will be scheduling repair of his contralateral popliteal artery entrapment.
The vascular surgeon has a vital role in a hospital’s medical ecosystem. One time, I heard hospital administrator say that with the advance of endovascular technologies, the vascular surgeon would become an expensive, redundant luxury easily replaced by the overlapping skillset of radiologists, cardiologists, general surgeons, trauma surgeons, cardiac surgeons, nephrologists, neurosurgeons, neurologists, podiatrists, infectious disease, and wound care specialists. When I identify these zebras, these rare diagnoses, I am neither replacing all those aforementioned specialties, nor having special insight unavailable to the uninitiated. I am keeping my eyes open. In a non-smoking, active, otherwise healthy and employed middle aged man with no cardiac history, it is very strange to have isolated popliteal occlusion with otherwise pristine arteries throughout the rest of the CT scan. That is a statistical outlier. People who occlude blood vessels in this fashion usually have more comorbidities, usually are older, and usually have more atherosclerotic disease burden. While not quite like the teenager who presented last year with the same diagnosis (after a month of misdiagnosis and delayed treatment), the cleanliness of the arteries elsewhere in the body was disturbing to me. This puts me on a zebra hunt and not the usual horse roundup.
A hospital needs vascular surgeons in the way that America need the US Marine Corps. Every decade, there is some congressional movement to see how the USMC, which has fighter jets, tanks, planes, aircraft carriers, helicopters, and riflemen, can be phased out because it seems to duplicate the services of the Navy, Air Force, and Army, and every generation a conflict proves these arguments wrong. Individuals who know things broadly and deeply, who can do many things across specialty lines, work from head to toe, and whose specialty is to customize solutions to complex problems is the special quality that is the difference between tertiary hospitals and quaternary hospitals. While these qualities are goals within Vascular Surgery, it is a generalizable goal for anyone working in healthcare. My favorite professor in medical school was Dr. Harold Neu, chair of infectious diseases at P&S. He knew everything and was interested in everything and took every moment in the hospital to increase his knowledge a little more. That’s how and why I diagnosed a case of schistosomiasis earlier this year -the upper abdominal pain was not from a coincidental aortic aneurysm, but the fellow did swim in the Nile.
I texted Dr. Sean Lyden, my former boss and partner at the Cleveland Clinic main campus, if there was any situation where an asymptomatic popliteal entrapment who had gone over 50 years of life without complications could just be watched -it was a question from the patient actually. Dr. Lyden treats popliteal entrapment weekly and maintains a clinic specializing in popliteal artery entrapment (link). One of advantages of working in vascular is that the community is small and highly accessible, and I have a group of living textbooks on speed dial (that term pegs me as antique). There is an active social network of vascular specialists and the SVS maintains SVS Connect (link) for posting and discussing difficult questions. Despite the horrible hour that he received the text (“What’s the matter? Are you in trouble?” he asked) because of the time differences between Abu Dhabi and Cleveland, he answered, “no.” Sorry, Sean, for texting you at 4 in the morning.
When you look for four leaf clovers, and you have never seen one in your life, the moment you find one must be transformative. I have never found one, but I keep my eyes open, lest I trod on one.


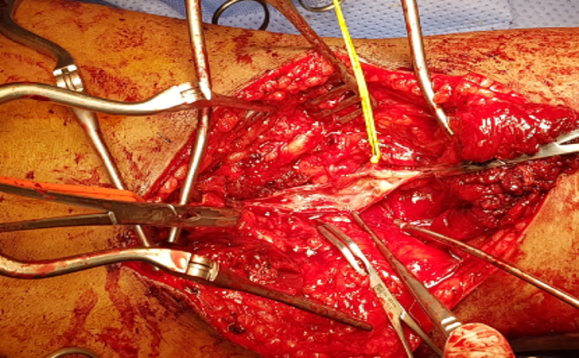
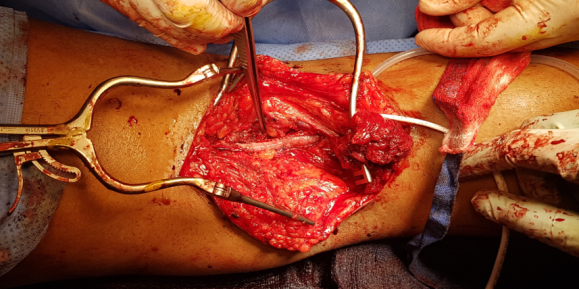
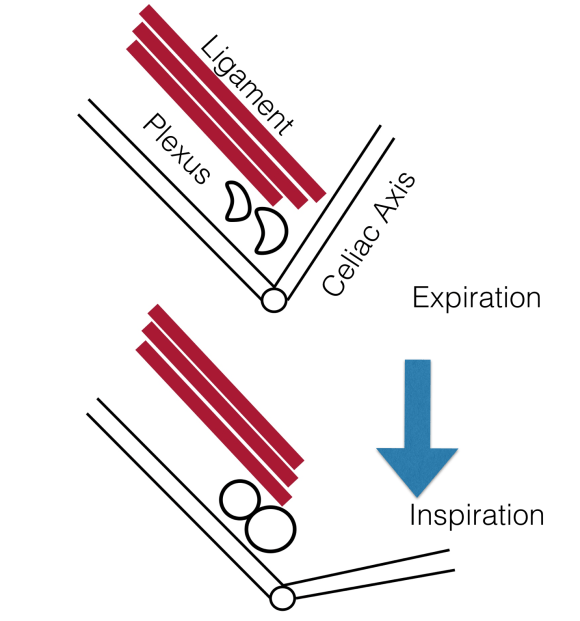 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
