Generated from my prior posts on the biomechanical problems generated by a bipedal lifestyle, this podcast discusses those issues. This was discussed by Dr. Elen Feurriegel on her lecture series “Big Mysteries of Human Evolution” available on Audible where she describes the human spine as a stack of teacups and saucers supporting a bowling ball.
Narrow shoulders means the arm hangs off the first rib tethered by the brachial plexus
When Australopithecus began to walk upright, there were many consequences. It freed the hands from weight bearing, but it also burdened the shoulder girdle with the weight of the extremity. Boticelli’s Venus shows the Renaissance ideal of the narrow shouldered maiden, but that bulk of shoulder and arm meat and bone, roughly equal to the weight of a jamón ibérico (vacation pic below), hangs off the neck with pathologic consequences. Also, the australopithecine usually died by disease or trauma by the second decade if chimpanzees are to be believed, but we live for nearly a century wearing down tissues designed for 10-20 years.
jamón ibérico
Mechanically speaking, there is a weight and a rope. The brachial plexus is the rope and it is draped over the first rib. The muscles of the shoulder girdle should support the weight of the arm but with bad posture, another consequence of bipedalism, the muscles may not be up to the task.
When there is a cervical rib, the situation is worse. The thoracic outlet is narrowed, and the weight of the arm, the jamón, is borne on the cervical rib. The brachial plexus becomes stretched over this anomalous bone and the trauma results in symptoms of pain, weakness, and strange sensations. I am of the opinion that cervical ribs in general should just go when found as nerve (and arterial) injury when found late may be irreversible.
CASE
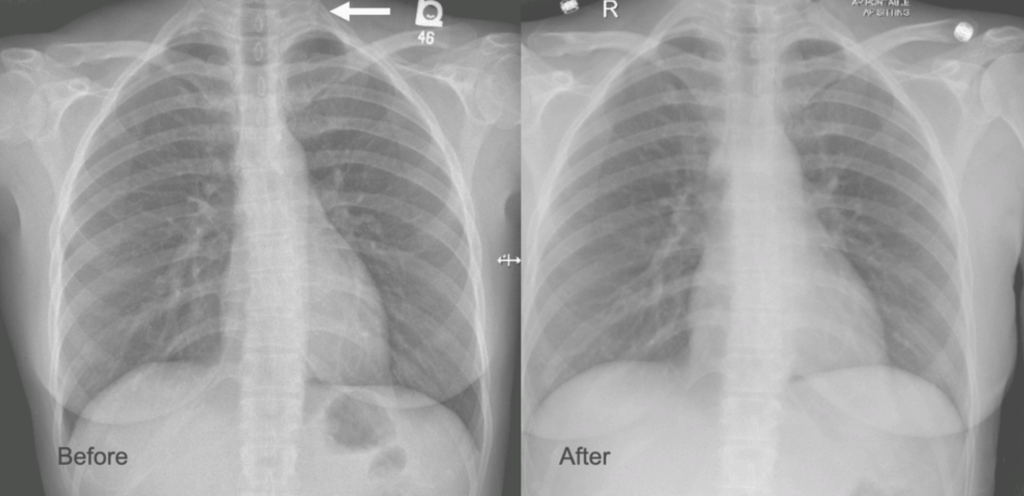
The patient is a younger woman who was referred from cardiology after workup of chest pain and left arm pain was negative for cardiac disease. She also had occasional right arm pain. The only finding of note during an extensive cardiac workup were cervical ribs found bilaterally on chest x-ray (below).
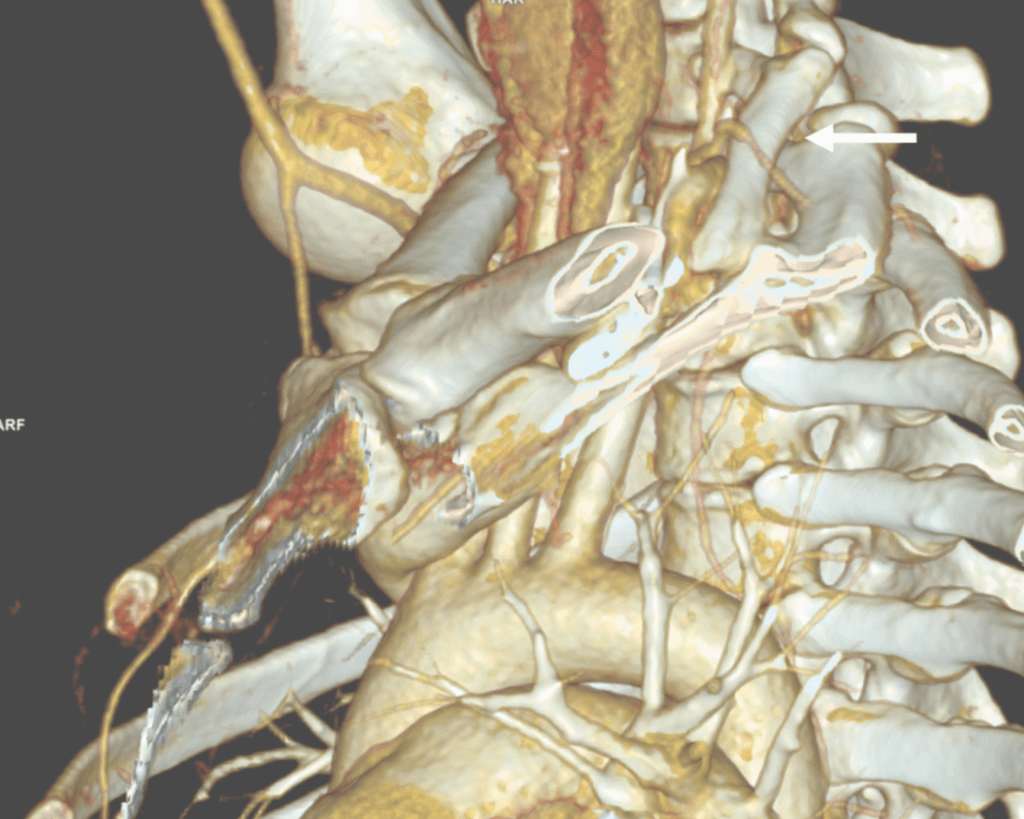
On examination, she was petite and had narrow shoulders. Stress maneuvers extinguished the arterial pulse in both extremities. EAST test was vaguely positive -weakness and numbness in the fingertips. Tapping on the cervical ribs which were prominent bumps in the supraclavicular fossae triggered shooting discomfort in both arms. I ordered a CT scan with contrast -this helps with operative planning as the 3D reconstructions allow you to view the operation before you perform it.
White arrow points to left cervical rib. The artery and plexus which is not seen are draped over it.
I recommended cervical rib resection, bilateral, staged. The left side was chosen first as it was the more symptomatic side. I recruited the assistance of Dr. Nader Habela, our spine surgeon.
Cleveland Clinic Abu Dhabi, has its roots in Cleveland Clinic,and was founded over a century ago in the vasty fields of wartime France by the four founders in an US Army tent. The observation at that time formed the root of the culture, the meme being that without barriers, the distinctions of competitive, siloed specialities made less sense than collective knowledge. It is encapsulated in our words, “To Act As a Unit.” CCAD is close to those roots. Lacking trainees in vascular (working on that), we totally depend on each other for extra pairs of hands in the OR. While it drives my nurses crazy, working with experts in other specialties exposes me to different techniques, instruments, and gadgets, which I load my trays with. Working with Dr. Habela, I saw that for cutting bone in tight spaces, an osteotome and mallet (hammer and chisel) worked with diamond cutter precision is faster and more precise than chewing your way through with a Kerrison. I do wish I had a surgical light saber.
Exposure was via supraclavicular approach. The cervical rib had a joint on the first rib and it was removed. The picture below shows its dimensions.
The artery and brachial plexus were tented up and there was inflammation around these structures. The anterior scalene was released for added measure, but first rib resection, I felt, was unnecessary.
The patient underwent contralateral cervical rib resection a few months later and had significant relief of symptoms but not total relief which I believe has to do with the slower relief time course with neuropathy. The chest pain never recurred. While I do know that diaphragmatic issues refer to the shoulder because of the emryologic origins of the diaphragm and shared roots of the phrenic nerve with brachial plexus, I do not know of a brachial plexus issue referring symptoms to the chest outside of autoimmune neuropathies which the patient did not have. The chest x-ray, which I always get after these procedures to check on diaphragm innervation and for pneumothorax showed the removal of the left cervical rib only, but no insight in why she had chest pain along with the extremity symptoms.
Cervical Ribs Must Go
I have never comes across a benign cervical rib. Because they are easy to remove, they should come out. While no arterial injury had occurred in this patient, we see many instances where compression and aneurysmal degeneration beyond the compression with embolization results in tissue loss, frequently misdiagnosed as rheumatologic arteriopathies. The cervical rib is a special case of neurologic thoracic outlet syndrome (nTOS) where the pathoanatomic mechanism is magnified by the extra bone. While physical therapy has a role in standard nTOS, no amount of PT will address the cervical rib. The inclusion of the Boticelli Venus has to do with the fact that stature and posture plays a significant role in nTOS. Even after first rib resection, there are some people who need a second rib resection to clear the space.
The critical need to treat this is that nerve injury is sometimes irreversible if left untreated. The worst outcome is a causalgia -the feeling that the upper extremity is being electrocuted, put on fire, eaten by flesh eating ants, that is perfectly and completely disabling because our function is defined by our ability to use out upper extremities. Once this sets in, surgical neurolysis or any reoperation has very little chance of working.
So many problems from a bipedal lifestyle
There are so many chronic problems arising from bipedalism, that I will have to work on a whole monograph about it. Humans are the only vertebrates (aside from a few burrowing fish and sea horses) in the history of vertebrates with a vertical spine in orientation to gravity. Yes, there are bipedal dinosaurs like pigeons and velociraptors, but look at their spines -they are horizontal to gravity with the mass centered around the hip. Aside from the obvious ones of spinal compression and arthritis, hernias, and prolapses, are vascular diseases like venous insufficiency, median arcuate ligament syndrome (MALS), and popliteal entrapment. While the first one, venous insufficiency makes sense, MALS does not until you understand how much the heart full of blood weighs. Suspend this bag of meat and blood on your celiac axis, grind the celiac plexus between the diaphragmatic ligaments and the artery, and voila -MALS. Popliteal entrapment -easy – being upright means straightening our knees, something no animal does, which exacerbates the entrapment.
Bonus for my readers -POTS -postural orthostatic tachycardia syndrome -does not exist for quadrupeds -cannot. Our swift (a million years?) transition to bipedalism did not happen with the proper adjustment of our pressure gauges for some, and those with POTS struggle with this change in posture from the natural horizontal state practiced by all other vertebrates.
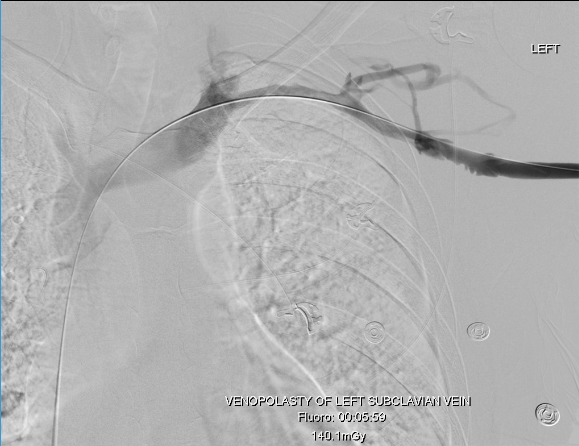
Recently, I saw a case presentation uploaded to LinkedIn of a subclavian venous stenosis treated with balloon venoplasty and a stent for venous congestion of the arm. The images were beautifully clear. The stenosis was at the thoracic outlet. The comments were generally favorable, including congratulations for a nice case, but I had to put in my two cents: The thoracic outlet is a terrible place for a stent due to external compression, and once occluded, a stent in the venous position is a permanent obstruction. The justification was that the patient did not want surgery and there were no surgeons who did first rib resections where the post author worked. I refrained from commenting something about primum non nocere.
This patient from the images above is a middle aged man who competes in triathalons and who noted sudden onset of discomfort and heaviness and pain in his left arm. Ultrasound revealed DVT in his axillosubclavian veins extending into his brachial veins and he was started on anticoagulation. He had been on anticoagulation for about a month by the time he came to my clinic. On examination, he had a prominent superficial veins on his shoulder, but otherwise had a normal examination. He did not have arterial obstruction on TOS (thoracic outlet syndrome) maneuvers and had no neurologic symptoms. I recommended first rib resection.
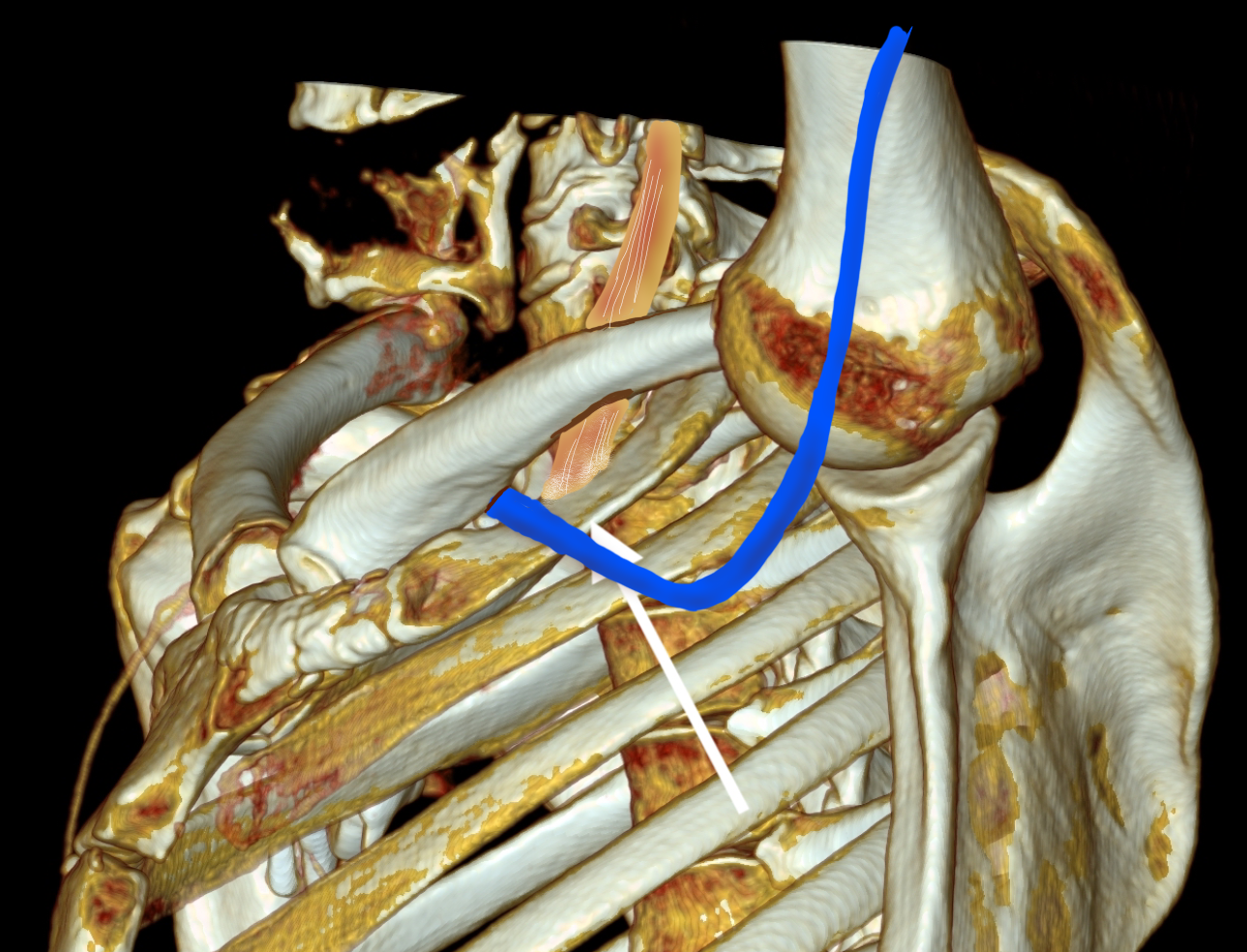
The patient’s first reaction was a dubious expression. After all, in this day and age, isn’t it barbaric to offer to cut out a rib? Why not put a stent there? A CT venogram was obtained showing the subclavian vein occlusion, but we knew that. I use the 3D surface reconstructions extensively as a visual map to determine surgical approach. I remove first ribs through both supraclavicular and transaxillary approaches, choosing one or the other.
The 3D reconstruction of the bones showed that to get to the first rib section underlying the vein, it was best approached via a transaxillary approach. The arrow in the image shows the flare in the first rib where the anterior scalene muscle attaches. Adding muscle shows that in this well muscled patient, getting to the first rib would be a challenge -for the people holding the retractors.
The operation is done with the patient in right lateral decubitus position and requires deep retraction and good lighting -I have played with using the laparoscope (more to come). Laparoscopic instruments such as the Maryland tipped ligasure and hook cautery get much use in this operation. The special sauce to getting this done quickly here in Abu Dhabi where I don’t have the army of residents and fellows is getting my colleagues in Orthopedic spine (Dr. Nader Hebela) and Thoracic Surgery (Dr. Redha Souilamas) interested in TOS.
Where I would laboriously chew through the ribs with a Kerrison, Dr. Hebela has shown me the high art of the hammer and chisel (notice the clean lines on the cut rib below). Dr. Souilamas has seeded the idea of doing this entirely thoracoscopically from the thoracic cavity, and yes, it is right there to see when I recently visited one of his operations -where is that cadaver lab when you need one? Enough rib was resected to ensure the vein, artery, and plexus were completely free.
A bit of anterior scalene came out with the specimen, splayed upwards in this image
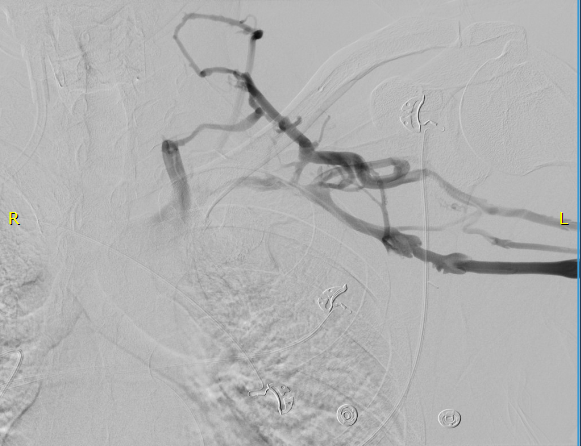
The patient did well, recovering much of his range of motion quickly with the help of physical therapy. He was taken to the angio suite and underwent venography shown below. There is an occlusion of the subclavian with outflow via collateral veins. Not seeing collaterals is as important as seeing a good angiographic result.
Venoplasty was done to 8mm -I try not be overly aggressive here, just to break the strictures that caused the balloon to have a waist in two sections. The final result is below, with the absence of the venous collaterals. If they were still present despite an angiographically satisfactory result, I would perform IVUS to see what the problem was. In no circumstances would I place a stent at this juncture -my plan is to keep the patient on anticoagulation for 3 more months.
First rib resection should be in the armamentarium of every vascular surgeon. I sense a rise in the diagnosis of this and this has been commented on the SVSConnect boards (link), possibly from a greater awareness of the signs and symptoms of the diseases associated with the thoracic outlet. Since coming to CCAD, there have been enough cases for it to become a routine which I did not expect.
The thoracic outlet, like the median arcuate ligament and the inguinal ligament, cause trouble for stents.
Looking at the thoracic outlet (above), the vein has a particularly narrow outlet under the hinge of clavicle and rib. I generally find it tragic to see a stent here because it limits the possibility of improvement with rib resection. Like the median arcuate ligament for the celiac axis and the inguinal ligament for the common femoral artery, stents get crushed in this position. If you think about it, it is probably our insistence on bipedalism that engendered these design flaws. Stents get compressed by the weight of the shoulder and arm (thoracic outlet), the mediastinum (median arcuate ligament), and the abdominal cavity organs (inguinal ligament) under these choke points, something the quadruped does not suffer.
Quadrupeds that come to mind, RIP GOT.
So is it barbaric, this open surgery? No. The barbarism is in offering patients an easy solution that will get that patient out the door happy, but not knowing (at best) or not caring (at worst) that the biomechanics do not favor any kind of durability.