When I was a young attending at the Allen Pavilion of Columbia Presbyterian Hospital, I was called into an operating room for a stat consult on a patient about to undergo a cholecystectomy. During the case, the IV had infiltrated and a bag of saline had filled the patient’s hand and forearm with saline, causing the hand to look like an inflated glove. The fingers were cool and white and the edema was firm but yielded to touch.
I elevated the hand and firmly squeezed the edema out of each digit, then gently massaged the edema from the hand onto the forearm. From there, I pushed the edema onto the arm. I then wrapped the hand up in an Ace wrap, and suspended it from an IV pole and returned to my case. Later, I returned and the hand was restored, warm, and perfused.
The lymphatics serve to move extracellular fluid (link). They can be overwhelmed much as drainage from a house can be overwhelmed resulting in puddles and ponds (link). This extracellular space has been “discovered” to be a new organ, but vascular surgeons have known about it for some time. Ultrastructurally, it is very close to a sea sponge with lattices of structural protein connecting cells to form tissues. And like a sea sponge, the salty water can be squeezed out or drained using gravity.
In olden times in central Europe, if you had chronic leg ulcers, you went to abbeys that specialized in their care. There, nuns would milk the edema out of your leg swollen typically from parasites and dress the leg and ulcer in linen cloth soaked in special oils. This is how Dr. Paul Gerson Unna came up with his eponymous Unna’s Boot, substituting Zinc Oxide paste which created a bacteriostatic environment.
Professor Paul Gerson Unna
Every year or so, I will be consulted for what I term a lymphatic emergency. A subset of this is phlegmasia. Whatever color you find -alba (white) or cerulea (blue) is really no matter -who really knows which comes first? It is an emergency in that the time clock for arterial ischemia -minutes to an hour for nerves, an hour to 6 for skeletal muscles, 6-12 for skin and bone, are all in play. The instinct is to go right to fasciotomy, but what you are usually doing is releasing the extracellular space, and the muscles are typically fine, even though their compartment pressures were very high.
Take this patient who developed severe upper extremity edema in the recovery phase after a cardiac arrest.
The ICU staff noted the had discoloration about four hours after the arrest. There were no arterial pulses and the forearm and hand were rock hard, the finger tips ice cold. Compartment pressures measured using the arterial line and needle method didn’t drop after the initial flush of saline below 70mmHg. While I could have been justified in performing upper extremity fasciotomy and even trying thrombectomy in a critically ill, coagulopathic patient on multiple pressors, I could just as easily have been on solid ground for saying the life was more valuable than the dominant hand. Both would have been the wrong move.
I performed the nun’s milking maneuver mentioned at the beginning and lacking an Unna’s boot, I compressed and elevated the best I could with double gloving using a small sized glove and ACE wrap.
Notice the edema has segregated into the arm.
In the morning, taking down the dressing, and re-compressing, there was now a radial artery signal and the fingers were a much improved color. The pulse-oximeter waveform was near normal. As an aside -the pulse oximeter uses the same technology as the digital photoplethysmography for generating toe waveforms in the vascular lab -ie. a vascular lab at every bedside! We have collected and are analyzing the data on this for publication.
The pulse oximetry waveform is the same tech as digital photoplethysmography. Cotton cast padding (Webril) and Coban wrap is a good method of compression that avoids the problems with ACE wrapping.
It’s a hard thing to not run off to the operating room in most cases because that is how we are trained, but understanding how a patient got to that point is crucial in deciding if compression alone will work. If they call you from the ER about a patient with a swollen cold foot with diminished signals, you have to figure out the mechanism. Was it arterial occlusion, rest pain, and chronic dependency of the foot that resulted in this? Typically the swelling appears late. Was it heart failure and inability to walk, resulting in the patient sitting all day in a chair that is the cause? Was it pregnancy with a DVT? Was it the deadly sin of sloth? Only in arterial occlusion in a chronic presentation would compression be contraindicate. In this ICU case, the lack of arterial signal is secondary to the swelling, not the cause of it.
Elevation alone does not manage edema well. Only hanging upside down or being in water up to your neck…
Compression is a necessary component of treating lymphedema emergencies because elevation alone may be insufficient, particularly in the leg.
Wrapping a leg is a critically, undertaught skill. Also, never cover the knee cap.
Elastic compression is ubiquitously available as the ACE wrap, but they can shift and move and roll, causing zones of excess and not enough compression. TED hose and compression stockings are definitely helpful in long term management, but with legs, compression needs to go up to the knee joint, or up to the groin, never halfway or the edema will create a line of ischemia at the end of the stocking that blisters when the stocking is removed, and can progress to full thickness necrosis. Cotton cast padding and Coban, or an Unna’s Boot may be the safest in terms of avoiding skin injury.
ACE wrapping is never taught adequately, and for it to work well and avoid injury to the skin, the wrapping has to be reapplied several times a day. It should be a prerequisite for nursing and medical student certification, as edema is the most common vascular disease.
Moving into our new home after four years out of country, I welcome an old friend from storage, but also unfortunately a health hazard, only mitigated by being fully reclinable.
A long time ago, there was the IVC clip which survives today as a vestigial CPT code. Then in the 1980’s, the Greenfield filter was introduced and changed the management of thromboembolism (reference). The explosive adoption of endovascular technology in the late nineties and early 2000’s drove the growth in implantation of newer generations of IVC filters that were designed to be retrievable. The people requesting the filters -the physicians, surgeons, and even patients looking to stop taking anticoagulation, were basing their decision on common sense –“sometimes, people are vulnerable to pulmonary embolism and are at risk of hemorrhage with anticoagulation, so an IVC filter makes sense.” There was frankly a data gap -a breach into which multiple companies jumped in with their own flavor of filter. Many interventionists saw no need to be selective -these were easy to place, and easy to remove, and if they stayed in there was the excellent long term results of the Greenfield filter to cite, and their referring docs asked for it. There was also the high revenue density (revenue/time) that gave filters a gravitational pull. There were several problems with this endo-enthusiasm (like in so many other cases). In the absence of data and with the aggressive marketing, too many filters went in for weak indications. We now know that most of these filters do not behave like the Greenfield, which itself is not completely innocent. Unless followup is part of a process, many patients neglected to have their filters removed. And finally, the data caught up and failed several filters which are no longer on the market and the indication for these filters is now quite narrow.
In 2009, I was asked to consult on a young man who was hospitalized for upper GI bleeding. The EGD revealed the tines of an IVC filter poking through (the jpg is somewhere I swear). The prior year, he had been in a bad car accident and had a filter placed but never had it removed. The filter had migrated out of the IVC into the duodenum and into the spine and aorta. I removed it operatively, and that was the beginning of a series of cases, about 1-2 annually in my general vascular practice, of filters that had eroded through the IVC and was causing symptoms of bleeding or pain. The pain typically was associated with a tine touching on or eroding into the spine. Biomechanically, the IVC is a collapsible tube and all the viscera on top of it weighs about as much as an equivalent sack of uncooked chitterlings when recumbent and grinds on the filter and any sharp parts. Imagine unbending a paperclip (figure) and putting it in the belly. Over time, that clip will poke a hole in something. Why would we not expect an IVC filter to behave otherwise?
An Iliocaval Thrombosis Below a TrapEase Filter
The patient is a younger man who over a decade ago had a TrapEase permanent IVC filter placed when he had a pulmonary embolism while having multiorgan failure. He was on coumadin briefly, but in the 17 years since filter placement, never had another venous thromboembolic event, but did develop venous insufficiency and varicose veins that were successfully treated. Several days prior to admission, he had been working out and developed back pain. After trying to sleep it off, he woke with severely swollen and painful legs. On admission, he was found to have no lower extremity DVTs, but had slow flow suggesting central occlusion. An abdominal x-ray showed the TrapEase filter (image below).
CT scanning and MRV showed the occlusion of the patient’s iliac veins and erosion of the struts of the filter outside the IVC (axial images below).
On heparin infusion and bedrest, his swelling improved and we had a chance to go over our treatment options. They included
Catheter directed thrombolysis
Angiojet thrombectomy
Large sheath thrombectomy (link)
–with one of the following–
Surgical resection of filter
Endovascular retrieval of filter
Balloon venoplasty and stent exclusion of the filter (link)
Catheter directed thrombolysis of such a large volume of clot in the absence of a good flow channel usually necessitates multiple days of thrombolysis with return for venography and adjustment, with a small but not zero chance of fatal or disabling hemorrhage. It is expensive -multiple ICU days, return trips to the OR angiosuite. Angiojet thrombectomy is useful for clearing smaller vessels and grafts but due to the pulsing of the jet, it has a good chance at creating pulmonary emboli if the filter’s occlusion is not complete. Plus it is expensive and limited by the volume of fluid necessary to create the suction. Large sheath thrombectomy has worked for me in the past (link), but I worry about leaving behind thrombus that would embolize when the filter is removed or pushed aside.
Endovascular removal of the filter is always an option -I have removed a Greenfield filter over two decades in. I have never been able to remove an OptEase or TrapEase filter -there is nothing easy about these. I have a picture somewhere sent to me by a trainee who was consulted on a patient whose IVC was transected during the attempt to remove one of these endovascularly. That said, both my partners Houssam Younes here in Cleveland Clinic Abu Dhabi and Christopher Smolock at Cleveland Clinic Main Campus suggested trying with a two-team approach with a 16F sheath and wire from above and a 12F sheath and wire from below. That would be contingent on being able to clear the thrombus adequately.
Surgery to remove the filter is something I am comfortable with. It sometimes is the only option (link). Several times a year, I scrub in with urologists and oncologic surgeons to remove tumor from the retroperitoneum or IVC and the exposure is straightforward. When I only need control of the IVC, I make a transverse incision slightly above the umbilicus and mobilize the retroperitoneum leaving the kidney down to expose the IVC. For the IVC and iliacs, a midline laparotomy with a Cattell maneuver allows for broad control. Surgical thrombectomy would be great if the thrombus was all fresh, but challenging if there were differing amounts of fresh and chronic occlusion. The CT scan, showing the iliac veins and IVC to be swole with clot, suggesting most of it was fresh. Neither CT nor MRV could tell me if the IVC below the renal confluence was occluded. I had to be certain.
I went over these issues in detail with the patient and we agreed to proceed with diagnostic venography to check out the clot. The verbiage of clot, tofu, and cheese (link) worked well in communicating the information needed to achieve our goal of getting the filter out and the IVC and iliac veins cleared of thrombus. I sent a hypercoagulability study (even on heparin, the genetic component is useful information) which returned negative.
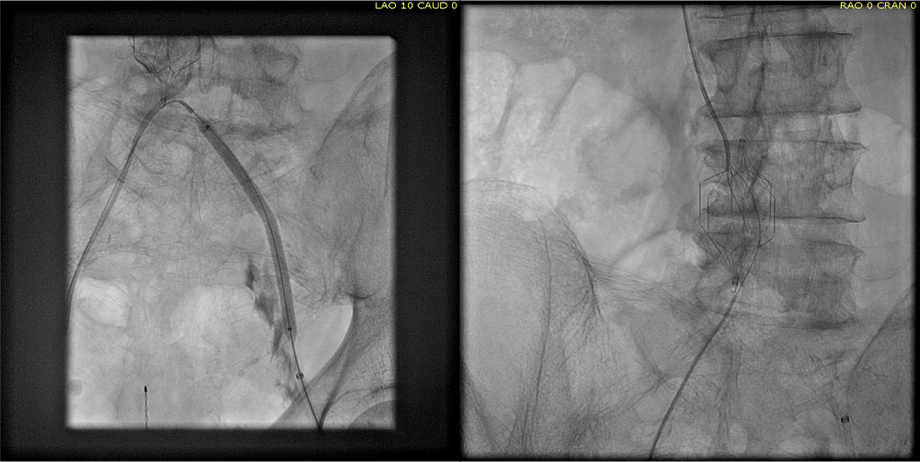
The diagnostic venogram is much more than just the pictures. For me, so much information is transmitted from the tip of a Glidewire as it passes through an obstruction or clot. Venography (image below) showed the thrombus but more importantly, the wire passed effortlessly in either side, got caught up in the bottom of the filter, but I was able to get through and the 5cm of IVC below the renal confluence turned out to be patent. The wire looped easily on both sides to the full extant of the dilated vein suggesting no chronic component.
I recommended surgery in our hybrid angiography suite. It would avoid multiple days of thrombolysis and its attendant risks. It would avoid subtotal clearance of thrombus. It would avoid failed filter retrieval and bailing out by stenting the filter (link), something acceptable in an older higher risk patient but not in an active young man. It would avoid surgery after several days of failed thrombolysis. The ability to perform venography and sonography with a clamp on the IVC ensured the ability to fully clear clot. And we had cell saver. After laying out my thoughts and concerns, the patient agreed.
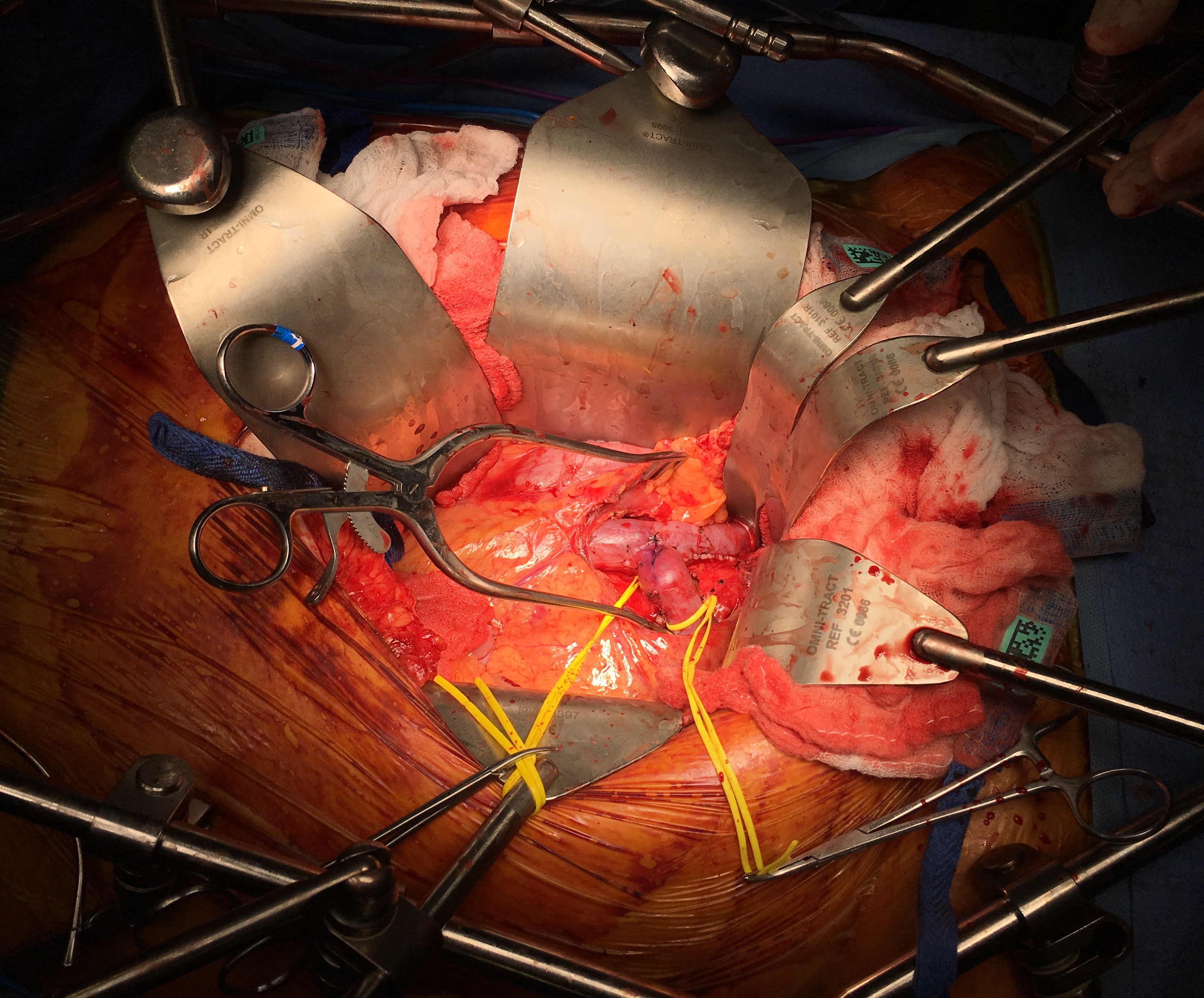
The patient was opened via a generous midline laparotomy. I recruited the assistance of my friend Waleed Hassen, master urologic surgeon here at CCAD, in exposing the IVC. The vessel loop in the picture (below) is around the ureter. Green arrows on the right image show the anterior struts (there are three posterior struts). I had just assisted Waleed recently in removing a metastatic testicular tumor off the IVC, aorta, and mesenteric arteries through the same exposure.
The surprising finding was the anterior hooks of the TrapEase filter had penetrated the serosa of the overlying duodenum. While not perforating, it eventually would have, as the struts had eroded through the wall of the IVC and were outside the adventitial. After heparinizing the patient, the cava was clamped above the filter and I opened the cava lontitudinally along the anterior most strut. I got the sternal wirecutters and removed the anterior three struts along with their hooks. There were large draining lumbar veins which were acting as collaterals that were ligated. The filter was removed internally in pieces leaving the posterior three struts behind as they were outside the IVC lumen. The lower cone can be seen with tissue ingrowth and chronic thrombus. It was dangerous and bloody behind the IVC and I chose to leave these struts behind as they would no longer be pressing into the spine with the filter mostly out. (image below).
The initial thrombectomy was done manually by massaging the vein from either side and up the cava -the thrombus (image below) in the basin on the left expelled as a unit with a spout of blood. Thrombectomy with a #5 Fogarty proved ineffective in the large vessel, and I resorted to using a Foley catheter, directing it left and right, with removal of some more thrombus.
Duplex demonstrated clearance of thrombus from the right iliac vein but adherent thrombus on the left. I placed an 18F sheath into the left femoral vein over a wire I had directed up and over into the right iliac system and advanced the sheath while suctioning -this collapsed the vein and allowed the sheath to scrape the walls of the vein, retrieving the final clot material in the right basin. Duplex confirmed the absence of clot in the left iliac vein. The venotomy was then closed primarily and a completion venogram was performed (below).
The patient recovered and was sent home after a duplex confirmed patency of his leg and iliac veins and IVC. He will be on 3 months of a NOAC for provoked DVT.
Discussion:
Most of these filters can be retrieved with endovascular techniques. The principle is of gaining control of the top of the cone and collapsing it like an umbrella. For the Cordis TrapEase and OptEase filters, both cones have to be collapsed, and the struts which will have grown into the walls of the IVC have to be be stripped away from the IVC. I had attempted removal of an OptEase with control from above when I was in Ohio, but like in this case, the filter had tissue ingrowth on the lower cone making looping and control of the filter difficult as the hook was encased. While I was able to collapse the filter into a 16F sheath supported through an 18F sheath, it was clear the IVC was invaginating into the sheath and with enough force, I would tear the IVC. It is not the worst thing, perforating the IVC, as it is a low pressure system, and a small perforation is tolerated, but a large one needs operative repair. This can be avoided with surgical removal of the filter.
Performing this in the hybrid suite allowed for complete clearance of thrombus. That said, the thrombus in the internal iliac veins likely did not come out, nor did I seek to clear them. Rather, I will rely on systemic anticoagulation to do this for me.
I use duplex sonography intraoperatively liberally during my procedures. During EVAR, transabdominal ultrasound is sufficient in ruling out or specifying endoleaks. During complex kidney transplantation which I sometimes participate in, duplex is a critical tool for evaluating flow. In this case, images showing a cleared vein (will post, currently stuck in portable ultrasound memory) assured me that I could open the clamps with confidence that pulmonary embolism could be avoided. Gratifyingly, the patient had immediate reduction of leg swelling and can be expected to avoid problems as nothing (such as stents) was left behind in the vena cava lumen.
Absolute Neutral Position is suprisingly universal
A body floating in space, a fetus in the womb, a dad lounging in his favorite chair, share the feature of weightlessness and represent the absolute neutral position (figure above) of the human which is the position of a relaxed supine quadruped -a dead mouse. Anything else is a stress position, including standing. Repeating motions outside of this relaxed pose or holding those positions away from this absolute neutral for long periods of time is a nidus for injury and pain. That is why most land animals sleep flat on the ground.
The Pain Operations
Operations to relieve pain are often the most gratifying to both patient and surgeon to perform successfully. This circumstance applies to the commonly performed procedures such as spine surgery, endometrial ablations, and varicose vein resections. When the pain is due to a rare set of circumstances, things are not so easy. Typically for rarer pain syndromes, two things need to coincide for the successful operation to happen. First is the patient must suffer while more common and potentially life threatening diseases are ruled out and even treated if these are found. This may take months or years. The second necessary condition is finding a physician who has seen the particular pain syndrome before and understand how to test for it and treat it. That meant the majority of people never get treated, or are shunted into the circle of shame as malingering, drug seeking, and mentally unstable. The opioid epidemic creates double jeopardy for these patients -they can become addicts as their pain is never successfully diagnosed and treated and they get labeled as drug seeking.
A random list of conditions that cause pain that should be on the mind after the usual things are ruled out. Also, vasculitis, autoimmune disorders, and foreign body reactions
All pain syndromes that can be successfully treated share common features that give you a degree of surety about the diagnosis, but at the end, there is a leap of faith on the part of both patient and practitioner because many of these operations have a failure rate ranging from 5-20 percent. First, the symptoms must be associated with sensory nerves, somatic or visceral. Second, there is a physical mechanism for that nerve to be inflamed from compression, swelling, or irritation that can be accounted for through history, physical examination, and imaging studies. Third, though not a constant, a major nerve trunk will be associated with a blood vessel, typically and artery, that is also affected by compression. Fourth, when swollen veins are the cause of pain, it has to be recognized that at an end stage the organ that the veins drain can also be affected.
The Pain Must Have a Testable Anatomic Basis
The somatic sensory nerves in the periphery are well mapped out and known since even classical times. The described pain should be consistent with a nerve. The best and easiest example is a neuroma that forms in an amputation stump. It triggers pain in its former distribution. It is palpable as a nodular mass. It is visible under ultrasound or cross sectional imaging. And it is easy to turn off temporarily with an injection of lidocaine, either under palpation or image guidance. If you can turn off the nerve and relieve the pain, it is likely that ablating or relieving the nerve of irritation will also relieve the pain. Such is the case in median arcuate ligament syndrome (figure below). The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
Tight Spaces Impinging Nerves, Arteries, and Veins
Many of the tight spaces involving the nerves have accompanying arteries that are compressed. This results in injury to the artery in the form of intimal hyperplasia, post stenotic dilatation, aneurysm formation, and thromboembolism. Shared tight spaces that cause problems for nerves and arteries have the common features of fixed ligaments, adjacent bones and muscles, inflammation, and motion. These include the thoracic outlet, antecubital fossa, cubital canal, diaphragmatic hiatus at median arcuate ligament, inguinal ligament, popliteal fossa, carpal tunnel, obturator canal, mediastinum, retroperitoneum -basically anywhere nerve, compression, and motion occur. In some instances of median arcuate ligament syndrome, postures and breathing trigger the pain. Holding a child in an arm may trigger pain in neurogenic thoracic outlet. Or sitting while wearing tight jeans may trigger a burning pain in meralgia paresthetica. It is not uncommon to find damaged arteries in median arcuate ligament syndrome, thoracic outlet syndrome, and popliteal entrapment or thrombosed veins in nutcracker syndrome, May-Thurner Syndrome, and Paget-von Schroetter Syndrome. Because nerves are typically difficult to visualize, their compression may only be inferred by testing for compression in their adjacent arteries.
Dilated Veins and Swollen Organs and Visceral Pain
Venous hypertension is most commonly conceived of as varicose and spider veins of the legs and offer a model of pain when applied to other pain caused by venous dissension. The visceral sensory fibers veins and arteries trigger a very intense pain that localizes to the trigger. I have often witnessed this when I manipulate a blood vessel during local anesthesia cases. Visceral pain from swelling has a dull achiness that is localizable to my spider veins after a long day standing like a bruise (below). The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
Actual Slide From Midwest Vascular Surgery Traveling Fellowship talk 2017, Chicago, IL, USA
When a limb is swollen from a thrombosis, the veins hurt and is similar to a bone pain from a fracture or a pulled muscle -that is how the brain processes the pain, but when the muscles and skin get tight from edema, the pain is sharp and dire. This is the same kind for pain from a distended left kidney from nutcracker syndrome or a spleen from a splenic vein thrombosis. These conditions can be modeled and predicted based on history and correct differential and confirmed with proper imaging -always.
Build a theory of the pain based on a testable proposition and set of nerves
That is the final message. These pain syndrome require some imagination and empathy to map and model. Predictive tests then can be performed on physical examination, functional testing, or imaging. Often, the adjacent artery is the only thing that can be reliably visualized and tested, knowing that it is the nerve that is compressed. Turning off the offending nerve with a block and relieving the pain is the most powerful argument for operating. It is building the argument for an operation that requires these objective data, but at the end, it does require some experience and faith. You have to believe in your patient and the science and when they coincide, you have to act.
Patient is a 43 year old woman who had been having bouts of severe left sided abdominal pain for several years with worsening episodes of nausea and vomiting resulting in several visits to the emergency room. She has also had microscopic hematuria. Gastrointestinal workup including gastric emptying study, esophagogastroduodenoscopy and colonoscopy were negative, as was a workup for kidney stones. Eventually she was referred to my clinic for management of nutcracker syndrome. She denied lower abdominal pain nor excessive menstrual bleeding.
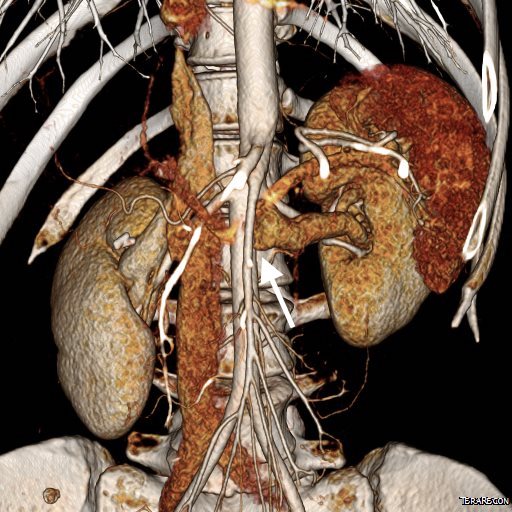
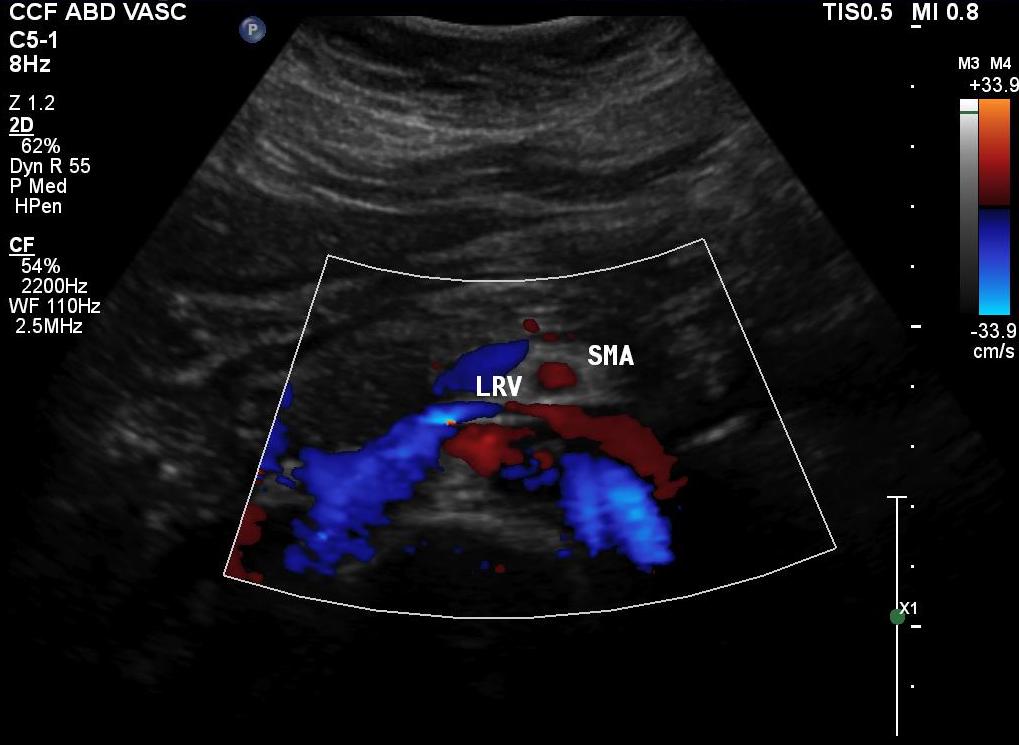
On examination, she was tender over the left kidney and flank. Laboratory examination was positive for microscopic hematuria. CT venography (below) showed an obstruction of her left renal vein by the superior mesenteric artery. Drainage via gonadal vein was not demonstrated, and no pelvic varices or complex of retroperitoneal veins was apparent.
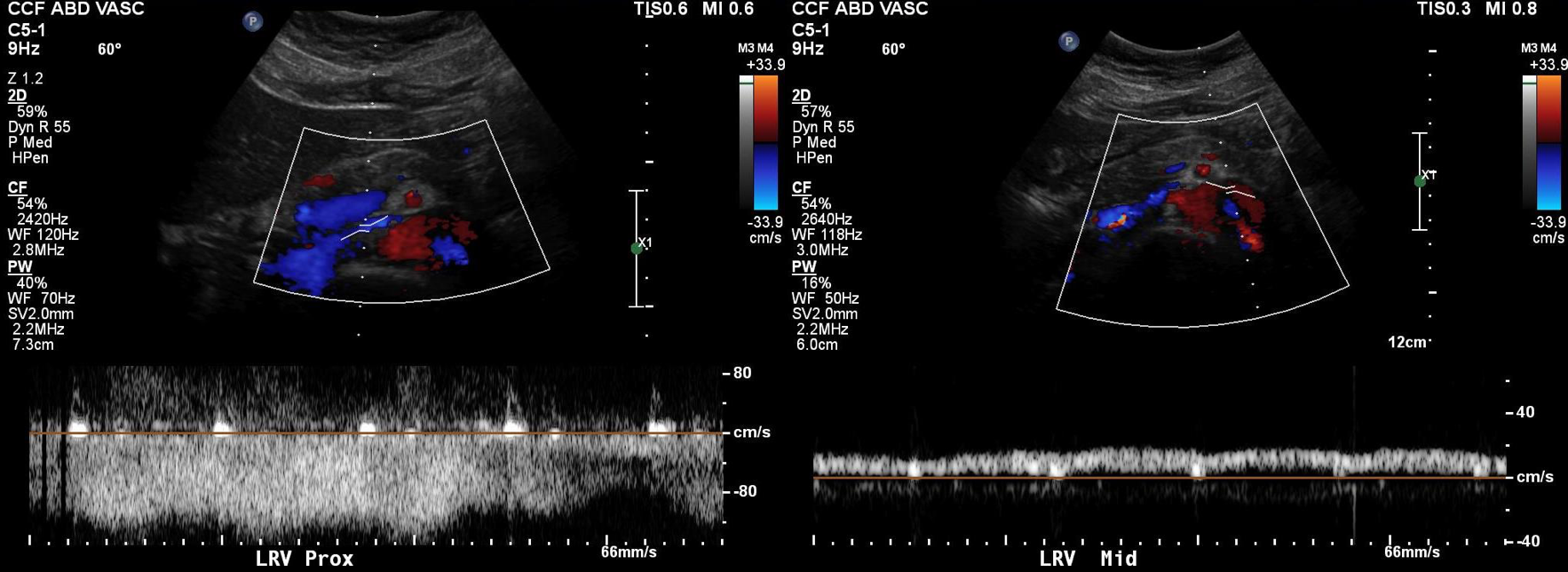
Duplex showed the narrowing in the left renal vein and spectral Doppler showed elevated velocities across the compression caused by the superior mesenteric artery (below). The collecting system was not obstructed.
Treatment options included endovascularization with a large stent in the left renal vein, left renal vein transposition to a lower position on the inferior vena cava, left renal autotransplantation, and left nephrectomy. Stent placement comes with a degree of risk for cardiopulmonary embolism which may require a sternotomy to fish out an errant stent. The risk for this in the US is because the largest nitinol stents available are 14mm in diameter which might result in undersizing in a vein that could easily dilate to well over 20mm. Larger nitinol stents for venous applications are available in Europe but currently are not approved in the US (yet). Wall stents, while certainly wide enough, have the problem of being long and stiff when not fully deployed. A 22×35 Wall stent may be 50mm long if deployed inadvertently into a tributary vein or contrained at the narrowing. Because it slides easily, passing balloons in or out can cause it to slip out of position. Because this stent elongates when compressed and packed, deployment is challenging and it is prone to “watermelon seeding,” a set up for embolism. It does have the virtue of easy reconstraining.
My friend and recent host for Midwest Vascular Surgery Society Travelling Fellowship, Dr. John V. White, in Chicago, seems to have solved this problem by a multistep process of predeploying a temporary suprarenal IVC filter, deploying a stent (whatever fits), leaving the filter as a protection against stent migration for 4 weeks until the stent permanently seats itself through scarring/intimal ingrowth, then removing the filter.
I chose to perform venography and renal vein transposition. The patient was placed in a supine position on a hybrid angiographic operating room table and her right femoral vein was accessed. She was placed in 15 degrees reverse Trendelenberg which is about the upper limit possible. Venography below.
Arrow points to left ascending lumbar vein which is taking most of the reflux. It drains the left kidney across the midline via retroartic channels to the IVCThe films showed left renal vein compression by the superior mesenteric artery with outflow via the ascending lumbar vein, both supra and infrarenal tributaries. A midline exposure was performed and the retroperitoneum opened as in an transabdominal aortic exposure. The vena cava was exposed, and the left renal vein was mobilized by ligating and dividing its tributaries. A point 5cm below the tributary point was marked on the IVC, and this was the target for transposition.
After heparinizing and clamping, the renal tributary was taken with a 5mm cuff –this would ensure proper length without narrowing the IVC.
The vein was anastomosed and flow was excellent by pulse Doppler.
She recovered well but had a longer stay because of an ileus, being discharged on day 5. Because she lived at a distance, and came back for followup the following week prior to boarding a plane for home. She no longer had the left sided abdominal pain and there was no hematuria. CT showed excellent drainage through the transposed vein.
Followup will be periodic (6 monthly) renal venous duplex from home. Given that there was minimal tension on the repair, I expect this to do well.
Discussion:
Nutcracker syndrome is one of the many unfortunate consequences of our bipedal lifestyle. The small intestines hang like baggy sausages off the branched stems of the superior mesenteric artery (SMA), and in some individuals, the SMA compresses the left renal vein against the aorta. The left renal vein receives up to 12-15% of cardiac output via the left kidney, and with outflow obstruction, drains the blood through small collaterals. The renal venous hypertension results in swelling of the left kidney with subsequent left renal colic -with flank and abdominal pain, nausea, and vomiting. There is hematuria which can be gross or microscopic. With drainage via an incompetent gonadal vein, varicoceles can occur with discomfort in men and pelvic varices with pelvic congestion syndrome can occur in women.
Diagnosis is challenging because it is one of the relatively rare non-gastrointestinal causes of abdominal pain (table).
Mesenteric ischemia
Median arcuate ligament syndrome
Nutcracker syndrome
Neuromuscular
Urolithiasis
Inflammatory aortitis/arteritis
Hypersplenism
Portal hypertension
Arterial aneurysm
Infections
Pelvic Congestion Syndrome
Endometriosis
Hernias
A history of left sided abdominal pain, flank pain, nausea, vomiting, associated pelvic pain, and episodes of hematuria are diagnostic. Examination is typically positive for left renal tenderness and flank tenderness. Laboratory examination include urinalysis for hematuria. Duplex, while technically challenging, will show renal venous compression with velocity elevation or loss of respirophasicity, CTA will typically show obstruction of the left renal vein with filling of collaterals, as will MRV.
Venography should be done in a stepwise manner (White protocol) to fully demonstrate the maldistribution of blood. That is the key word, maldistribution. I learned from my fellowship with Dr. White that performing venography in as upright a position as possible recreated the pathophysiology, the physics, particularly for pelvic congestion and nutcracker. Remember, this is a disease of bipedalism, of upright posture. Many negative studies done supine become positive, as the contrast will fall to where it prefers to go. As I have stated in the past, on the venous side, demonstrating drainage has different imaging needs than demonstrating flow. Pathologic venous drainage has three characteristics:
Varicose veins develop as an end stage process
Reversal of flow or reflux is demonstrated, particularly into small tributary veins
The midline is crossed in these usually small, now larger, collateral veins
While pressure gradients are nice if they are large, they are difficult to assess when they narrow to 1-2mmHg, particularly if they vary with cardiac cycle and respiration. Because we are assessing drainage, the distribution of contrast and the direction it goes is particularly important, and far more sensitive than pressure measurements.
Venography was done per a modification of Dr. White’s protocol for pelvic congestion:
Steep reverse Trendelenberg
Hand injection 10mL half diluted contrast, gently as to not create false reflux
Runs with catheter in left EIV, right EIV, left renal vein, right renal vein
With pelvic congestion workup, add selective bilateral gonadal and internal iliac veins.
I have started transposing gonadal veins when they have enlarged from chronic reflux (link, ref 2). Renal vein transposition was chosen because her ovarian vein was competent and too small to transpose (ref 1-3). While the patency rate of stents in veins seems to be acceptable, long term data is unavailable. Also, venographic appearances are deceiving -see the in-vivo measurement of the left renal vein after dissection:
Left renal vein at widest is 22mm, with expansion, possibly up to 28mm, but is relatively short. Do you see the SMA?The variability in diameter and length of the Wallstent in the 22-24mm diameter range makes this a challenging deployment. Given that I would not be able to closely follow this young patient, I felt compelled to recommend a durable solution (ref 4).
References:
White, J. et al, Left ovarian to left external iliac vein transposition for the treatment of nutcracker syndrome. J Vasc Surg Venous Lymphat Disord. 2016;4:114–118.
Miler R, Shang E, Park W. Gonadal Vein Transposition for the Treatment of Nutcracker Syndrome. Annals of Vascular Surgery 2017, July 6. in press. http://dx.doi.org/10.1016/j.avsg.2017.06.153
Markovic J, Shortell C. Right gonadal vein transposition for the treatment of anterior nutcracker syndrome in a patient with left-sided inferior vena cava. J Vasc Surg Venous Lymphat Disord.2016 Jul;4(3):340-2. doi: 10.1016/j.jvsv.2015.09.002.
The patient is a gentleman from out of state who had called about problems he was having with walking and with leg ulcers that wouldn’t heal. He is in his seventies and has a pacemaker for an arrhythmia for which he was on Xarelto. He also had type II diabetes. He had bilateral lower extremity deep venous thromboses 6 years prior requiring IVC filter placement. The filter occluded, and it resulted in sudden sharp and debilitating pain in both legs with walking short distances -some days only 50 paces.He described it as an unbearable pain in calves and thighs that felt like his legs were going to burst. He also had ulcers on his legs that would heal with ministration but soon recur. This was all despite being quite active, with regular workouts, and being fit. He was compliant with compression. He sent a CT scan done last year (below).
Right iliocaval centerline projection
It showed an Optease retrievable vena cava filter that was occluded and the iliac systems bilaterally (right above and left below) were chronically occluded with patent vena cava above and femoral confluences bilaterally below.
Left iliocaval system showing chronic occlusion on centerline projection
He had no hypercoagulability nor ongoing recent DVT’s. I thought there was a good chance that we would be able to recanalize the occluded iliocaval segment and he flew in for a consultation, and he was pencilled into the schedule ahead of his visit.
Examination revealed a fit and trim man in his 70’s in no apparent distress. He had bilateral leg edema that was moderate with small superficial and tender ulcers of the right posterior distal calf. Pulses were normal. He was taken to our hybrid suite and venography from femoral vein access in the proximal thigh in the supine position revealed his right and left iliac venous systems to be occluded (below figures).
Right injection from femoral sheath showing occluded iliac vein with collaterals
Left injection
Wire access into the iliac systems was performed with Glidewire and Glidecatheter periodic venography to confirm that I had not exited the vein. Unlike the arterial system, extravasation from being extravenous does not have the consequence of bleeding, hematoma development, and pseudoaneurysm formation because of the low pressure, but it can be a long procedure and uncomfortable as well so these are done under general anesthesia.
Advancing wire and sheath into iliac vein, crossing filter resulted in extravasation of contrast
Once position confirmed to be in the iliac vein, the vein was dilated to allow for greater ease of movement. In the case of the uncrossable filter, I switched to access from above via a right internal jugular vein access.
Dilating vein (left) for greater mobility, and crossing from above (R. IJV access)
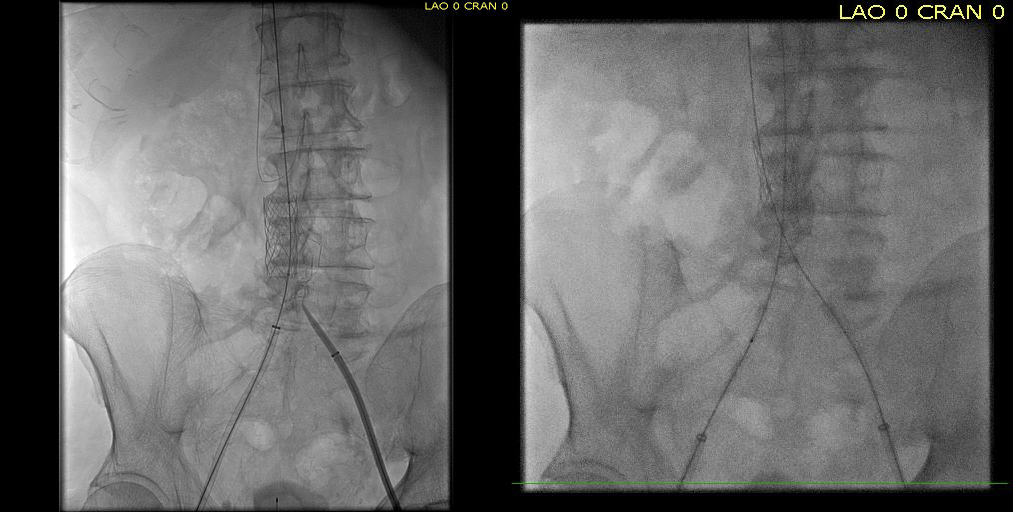
Once the wire crossed into the iliac vein from above, it was captured and brought out. While ballooning by itself is inadequate for revascularization, it greatly eases wire capture and on the right, it was done simply by driving the wire from above into the sheath. Wire capture wins access across the iliocaval and IVC filter occlusion from below.
Wire passage across IVC filter into right and left systems
Once wire access is done, ballooning across the filter is done from both sides. A large sheath is them delivered across the IVC filter. Finally, a Palmaz stent mounted on a large balloon is delivered and deployed. I chose to do this from the right access, and retracted the wire on the left -something done with some trepidation because of the great difficulty gaining this access, but with with prior balloon dilatation, reaccess is made easier. Also, plan B would be reaccess from above.
After balloon dilatation of occlusion typically to 8mm from both sides, a sheath placed and Palmaz stent deployed across filter on a large 24mm balloon
When this is accomplished, the left sided wire is reaccessed across this stent. This is the venous side analogue to gate access in EVAR (below).
Reaccess of the left iliac venous wire across Palmaz stent
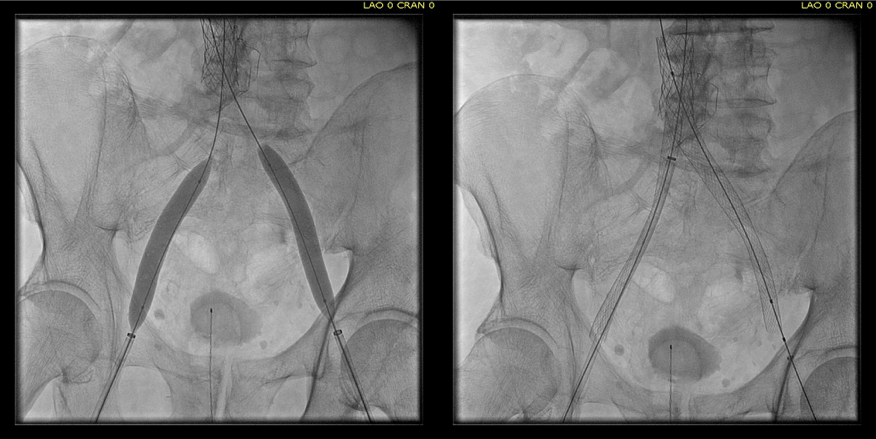
Once this is done, the iliac veins are dilated to 14mm from the IVC to the common femoral arteries. large 18mm Wall stents are deployed in a kissing fashion from the caval stent into both iliac systems and dilated to 18mm.
Predilatation of iliac venous systems with ever larger balloons, deployement of bilateral 18mm Wall Stents
After deployment, the Wall Stents are ballooned to 18mm. These stents were extended into the common femoral artery with 14mm nitinol stents.
Ballooning 18 mm Wall Stents with 18mm Atlas balloons, then extending to CFA with nitinol stents of 14mm
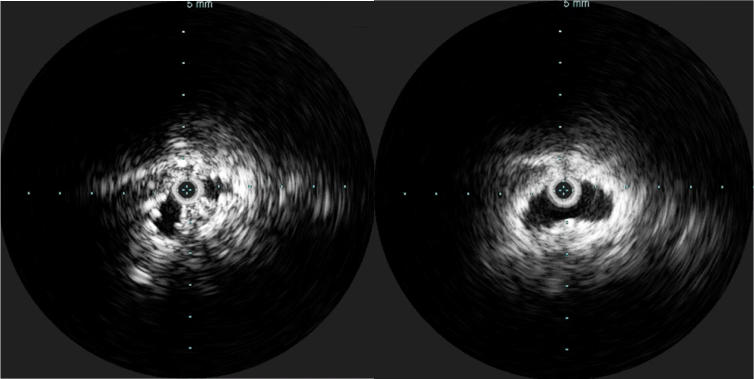
Completion venography suggested successful iliocaval recanalization and revascularization but these procedures are not done without a final intravascular ultrasound (IVUS).
Looks done, but needed final intervention after IVUS.
Intravascular ultrasound revealed incomplete expansion of the right common femoral stent. This was treated with another stent and ballooning with the result on the right.
Stent compression on IVUS treated with second stent
Venography alone is insufficient in determining patency. As illustrated, IVUS ensures a durable outcome.
The leg ulcer was treated with an Unna’s boot. A word about the venerable Unna’s boot –it works. The dressing dries and compresses while the Zinc Oxide prevents bacterial growth. It is interesting that the dressing is so infrequently used nowadays but not so when you consider that it isn’t reimbursed. And patients generally hate it.
This revascularization has an excellent chance at working as the patient has no hypercoagulability and had a patent common femoral confluence bilaterally. As I had mentioned in a prior post, the idea in venous revascularization is connecting confluences that serve as inflow and outflow.
This will require followup, consisting of duplex, and it is advantageous that he is anticoagulated for his arrhythmia. It is becoming more apparent that those languishing with chronic venous insufficiency and its complications need the IVC and iliac veins interrogated with a duplex. When an obstruction is found, they should be treated with these techniques as a first line therapy.
The patient is a younger man in his twenties who began having dizzy spells associated with near syncope and tunnel vision. He was previously an athlete and was fit and never had such episodes -he had a resting heart rate typically in the 60’s or lower. Workup for arrhythmias was ultimately positive for POTS -postural orthostatic tachycardia syndrome and he was referred to Dr. Fredrick Jaeger of our Syncope Clinic. Tilt table testing the demonstrated the reported tachycardia over 140bpm while upright rising from 60bpm while supine. A radionuclide hemodynamic study (Syncope Radionuclide Hemodynamic Test) showed 54% of his blood volume pooled in his left lower extremity and lower abdomen with upright posture. Air plethysmography (PHLEBOTEST) showed abnormal refill and fill times in both legs and a duplex of the legs showed deep venous reflux in both legs. MRV revealed narrowing of left common iliac vein by the overlying right common iliac artery (May-Thurner’s Syndrome, MTS), and this was where the patient came to my clinic.
The MRV, shown above and below showed the typical pathoanatomy for MTS, but the patient had no symptoms related to left leg swelling, DVT, or varicosities. He did have a reducible left inguinal hernia which was quite tender.
After some deliberation, while not promising anything regarding his POTS, I agreed to proceed with treating his pathoanatomy. Discussion with Dr. Jaeger revealed this: normally about 20% of blood volume parks in the legs with standing which is rapidly dissipated with normal calf muscle pump action. In a subset of patients with POTS, there is a 30-40% maldistribution of blood volume into the legs which may or may not drive the autonomic responses leading to POTS. He has never seen a study result showing a 54% distribution.
It made physiologic and anatomic sense to me to proceed with a venogram and intervention, but I confess I was dubious about any affects I might have on the patient’s POTS and I informed him of it. Also, I recommended seeing a general surgeon for his hernia.
Venography showed obstruction of his left common iliac vein as evidenced by the filling of pelvic and lumbar collateral veins.
Intravascular ultrasound showed the narrowing better and more directly (panel below). The right common iliac artery narrowed the left common iliac vein severely.
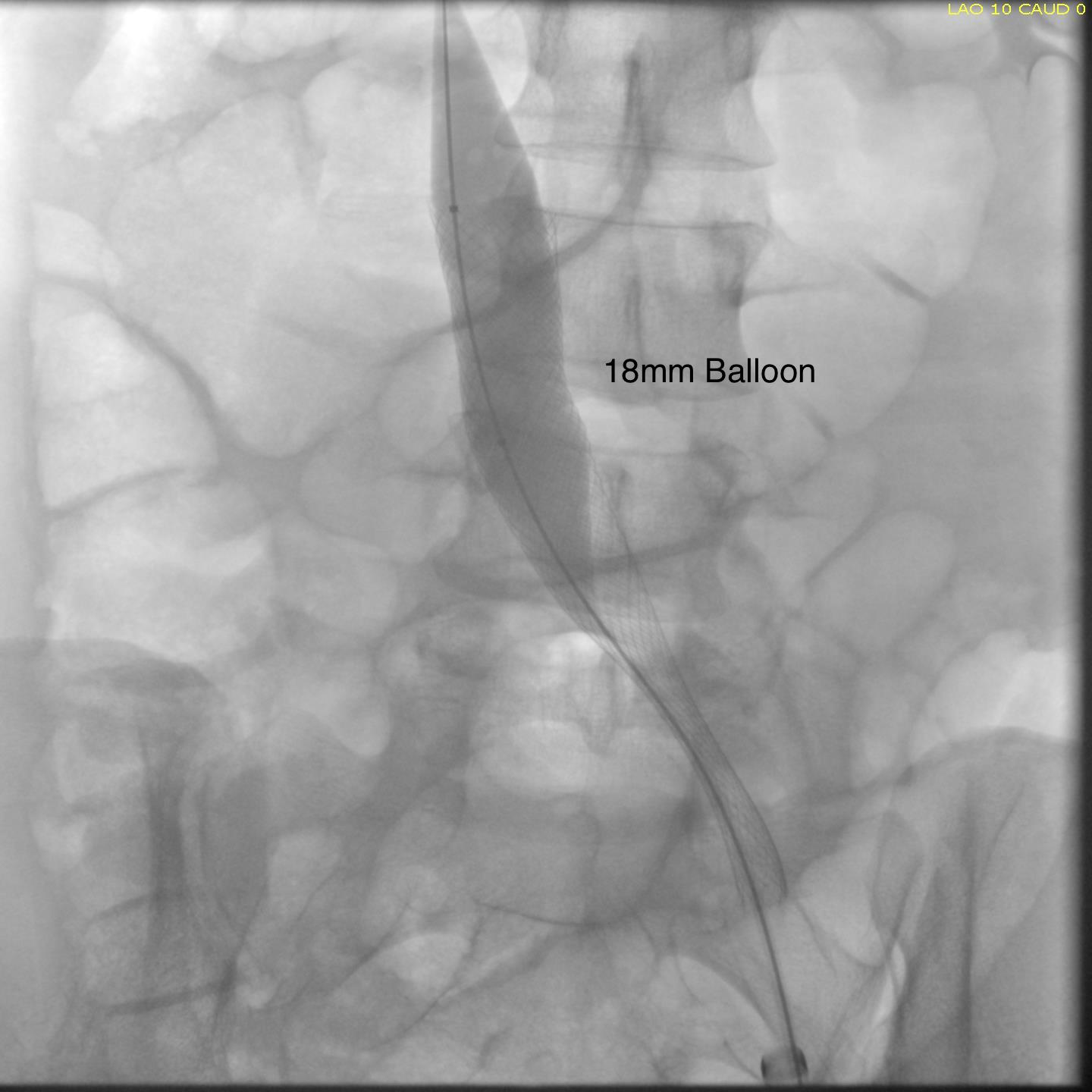
A 22mm Wall Stent was positioned across this and dilated with a 22mm balloon in the IVC and an 18mm balloon in the iliac vein. The resulting venogram showed resolution of the obstruction with collateral veins no longer visualized (below).
But again, IVUS demonstrated more directly the result (and illustrates the importance of having IVUS available for venous interventions).
The patient was discharged after procedure on a baby aspirin only. He subsequently underwent laparoscopic inguinal herniorrhaphy and returned to my clinic about a month later. His followup duplex showed a widely patent stent and normal flows in the left iliac venous system.
Surprisingly -the patient declared that he was cured of his POTS. He said since the stents went in, he has not had any more episodes of near syncope, dizziness, tunnel vision, nor weakness requiring lying down to rest. His wife confirmed that he was a flurry of activity over the holidays that was surprising considering how debilitated he was before. This is astonishing to me.
But it should not be a surprise given this: if the POTS symptoms were the result of autonomic dysregulation, a breakdown of the feedback control loop, there were only several places this could be a problem.
The pathology, the MTS, explains the POTS in this instance very nicely. Because the problem was in the cardiovascular system part of the diagram which I can fix and not the autonomic nervous system control element, which I can’t fix yet, a solution could be tried. This was not an asymptomatic compression of the iliac vein which we do encounter as an incidental finding. It seems to be POTS caused by MTS, and cured for now by treatment of the MTS.
The patient is a young woman who three weeks prior to presentation developed sudden low back pain and left leg pain while exercising on an elliptical. This pain worsened through the subsequent weeks and she developed fevers, chills, and night sweats, and she came to the emergency department. There, she was found to have left thigh and leg swelling. Duplex revealed a left iliofemoral DVT starting from the iliocaval tributary and extending to her left femoral vein (figure above). A CT scan revealed a pulmonary embolism to the left lung (below). No precipitating factors were present. Vascular surgery was consulted.
Plan was for catheter directed thrombolysis. Venography from the patient’s popliteal vein via a short saphenous access revealed thrombotic occlusion from the left common femoral confluence to the iliocaval confluence. The thrombus was crossed, and ballooning showed there was chronicity to the occlusion in the pelvis evidenced by waisting of the balloon on inflation. A multihole infusion catheter was placed across the thrombus from the thigh to the inferior vena cava and recombinant tissue plasminogen activator was infused overnight.
The venogram from the popliteal vein showed a patent popliteal and femoral vein and the goal of this procedure became opening the common femoral vein and its confluence of multiple veins from the thigh, to connect it via stents to the vena cava (second image below).
Clinically, there was no change overnight and when the patient was restudied next morning, there was still an occlusion starting at the common femoral vein.
At this point, I had a choice as to what to do next. First, I could stop, and have the patient start anticoagulation and return several months later -often, the common femoral vein returns to drain into pelvic collaterals. As I had discussed in an earlier post, venous interventions are no different from arterial ones in that inflow, draining vein, and outflow have to be considered. In the case of the veins, I like to think of it as connecting major confluences, and for a leg, the common femoral venous confluence is paramount.
Intervening from the popliteal vein to the vena cava is inferior to being able to connect draining veins at the common femoral confluence to the vena cava. So getting the common femoral vein to patency is critical, and can sometimes be achieved with anticoagulation and time. The second option is to break out a thrombectomy catheter and try to remove the thrombus by various machinations, ie. gadgets and novel catheter systems of which there are many. I felt that given the three week time course of the thrombus, the best we could get was some clearance of thrombus, leaving behind a complex network of chronic thrombus and fibrinous scar with the overnight lysis. I didn’t even try this second option and the thrombectomy machine stayed unplugged, the fancy (and expensive) catheters left hanging. The third option, surgery, was not indicated as the patient did not have signs of phlegmasia, and for the same reasons that the lysis didn’t work, opening the common femoral vein for an endovenectomy has uneven outcomes.
The fourth option, mechanical aspiration sheath thrombectomy (MAST), is a technique developed by Dan Clair, our former chair. As a concept, it is very simple. A large sheath (>12F) is introduced and the thrombus is aspirated while the bare sheath is advanced over a wire. The sheath is then removed and the contents emptied. For this case, an 18 F sheath was introduced into the femoral vein in mid thigh.
The blood is ejected into a basin and a cell saver (in non-malignant cases) is used to salvage the whole blood.
This reopened the common femoral vein. This was for me a very important step as without achieving this, I would have had to stent into the femoral vein, excluding many smaller veins draining into the common femoral vein, and effectively basing my revascularization off the popliteal vein confluence, an inferior inflow source for venous revascularization.
CFV post MAST
With the common femoral vein open, placing stents from the vena cava to the common femoral vein was straightforward and described elsewhere (reference). The iliac vein remained closed due to the chronic thrombosis, which was clinically May Thurner’s Syndrome, and was stented.
Three things deserve comment: the vena cava and iliac veins need to be dilated up to 18mm, and larger for the cava. This is disconcerting, but size does matter. Second, IVUS is critical in confirming that everything is open. Third, the 14mm nitinol stent placed into the common femoral vein will stay open, unlike a stent placed into the artery across the inguinal ligament. It likely has to do with the deeper position of the vein in relation to the artery which protects the vein from the ligament. We don’t have the large diameter nitinol stents designed for iliocaval venous revascularization yet, but the available stents do a good job.
The patient was discharged on anticoagulation with resolving edema in the left leg and thigh. At one month followup, duplex confirmed wide patency of the stents and IVC and no new DVT.
Discussion: MAST illustrates a critical issue for all innovation in the current setting of resource limitation. Innovations must be made with not just a consideration to efficacy and potential market, but also cost. The large sheaths used in MAST are commonly available and cheaper by multiples of tens compared to the thrombectomy systems and catheters. Unpublished data reviewing 13 patients undergoing MAST with a mean followup showed 69% with complete thrombus removal, 31% with subsegmental removal, no operative mortality, and 92% primary patency at an average of 79 days of followup, all with symptom improvement (Clair, correspondence). Other groups have reported similiar results using “large catheters” (reference 2), but nothing can compare to an 18F sheath in clearing the iliocaval system.
The patient can expect to have excellent patency in the short to mid term (reference 1).
References
Titus JM et al. J Vasc Surg. 2011 Mar;53(3):706-12.
Being a homeowner, you are sometimes stuck negotiating a repair with various workmen whose knowledge of building esoterica is only exceeded by their subliminal contempt of a man who can’t rip out flooring and drywall to renovate a kitchen or bathroom. I can only hope that I don’t come off that way when discussing human plumbing. It was a year into my ownership of my current home that I noticed that many of the drains in the window wells were clogged. A very unpleasant afternoon was spent digging out soil and leaves while trying to snake a coat hanger (access wire), and when I gave up, I tried to call a plumber. Only it was the wrong specialist. “You want a sewer guy.”
The sewer gentleman was a meticulously groomed Italian immigrant who walked about the house after inspecting the drain in question. After some harumphing, he declared he needed to do some tests which included running dye through the various downspouts around the house and drains in the house. Contrast drainography! To top it off, he wanted to run a camera on a flexible tube through to check out the drains. Endoscopy! Plumbing, he sniffed, was easy, but drains were an art.
For the record, our basement was dry, but I could see the money meter whirring away. It was only a few weeks removed from a spring storm where several homes a few blocks away had catastrophic flooding when rains overwhelmed the capacity of their drainage –Drainage Insufficiency!
The testing was fine, but he ended up recommending resealing the entire East side of the house and rebuilding the window wells, because while the house was dry, it was compensating by rerouting a lot of drainage down gutters and the downsloping lawn to the street –Collaterals! and he couldn’t promise the house wouldn’t flood with a torrential month of rain which Shaker Heights is prone to being downwind of the Lake.
And it is with this wisdom that I see the increasing numbers of chronic venous occlusions. For example, the patient whose venogram is pictured above initially complained to her obstetrician of persistent heaviness in the pelvis and swelling of the legs after delivering a healthy baby. MRV showed abundant pelvic collateral veins and she was referred to me.
Our first test in our clinic is a venous duplex of both legs and the abdominal veins. There was an occlusion of the inferior vena cava below the renal veins extending the the iliac veins bilaterally. I am about to give a talk on this and I composited the ultrasound.
She had iliocaval occlusion, chronic. Her symptoms were over two years, and were ever worsening. She hadn’t developed permanent skin changes of chronic venous insufficiency, but probably would in a decade or sooner. I recommended venography and an attempt at recanalization.
The procedure went well, and her symptoms abated. For my trainees, the absence of collaterals in the after image is the sign that hemodynamically, the revascularization is the preferred route of egress. Surprisingly, this has stayed open over two years, but again, my exceedingly well paid sewer gentleman consultant, had something to say about it.
Drainage, he declared, was different from plumbing, because things move slower and there is usually solid matter -poop, leaves, dead birds, etc., to contend with. Larger, high volume drains do best with a direct in-line connection with the city sewer, while downspouts and window wells with their twists and turns and only occasional flushings clog up too well. Wise words.
It gave me a reason why iliocaval venous interventions did so much better than femoropopliteal ones.
Venous interventions connect confluences to the main drain, in most cases the suprarenal inferior vena cava. The iliocaval segment drains the common femoral confluence, which even in the worst of chronic lower extremity DVT’s, seems to reopen with several months of anticoagulation. Not the same for the popliteal confluence which, getting much less blood flow to drain, and having a smaller diameter, stents in the femoropopliteal veins just don’t do as well. Plus, it has to drain against a greater hydrostatic pressure. The drain guy’s wisdom seems to apply. It also has implications for the kind of stents we place, and the kinds that are being developed specifically for the venous side.


















 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).

























 The patient is a young woman who three weeks prior to presentation developed sudden low back pain and left leg pain while exercising on an elliptical. This pain worsened through the subsequent weeks and she developed fevers, chills, and night sweats, and she came to the emergency department. There, she was found to have left thigh and leg swelling. Duplex revealed a left iliofemoral DVT starting from the iliocaval tributary and extending to her left femoral vein (figure above). A CT scan revealed a pulmonary embolism to the left lung (below). No precipitating factors were present. Vascular surgery was consulted.
The patient is a young woman who three weeks prior to presentation developed sudden low back pain and left leg pain while exercising on an elliptical. This pain worsened through the subsequent weeks and she developed fevers, chills, and night sweats, and she came to the emergency department. There, she was found to have left thigh and leg swelling. Duplex revealed a left iliofemoral DVT starting from the iliocaval tributary and extending to her left femoral vein (figure above). A CT scan revealed a pulmonary embolism to the left lung (below). No precipitating factors were present. Vascular surgery was consulted.