Last December, I received an email from a LOCUMS company begging for Christmas coverage at a nearby hospital. It offered an eye watering $330/hr for coverage during Christmas week and weekend. A friend posted about this on X, and it was edifying because no vascular surgeon gets this as regular pay, but it reveals the current market price of an on-call vascular surgeon, at least as much as travel nursing, and the willingness of hospitals to pay for it, reveals the true value of an experienced nurse. If you wonder why it takes so long to see a specialist in 2026, the answer is in the fact that very few people were biting for this offer to be cast so far and wide.
The fact is that no hospital can do things with sharp objects without running into the need for a vascular surgeon.
References
Ojeda LM, Arcila SM, Nunes VA, Duarte CM, Papi M, Jacobs DL, Malgor EA, Malgor RD. The value of vascular surgeons in modern health care systems: A systematic review and meta-analysis. J Vasc Surg. 2025 Oct 28:S0741-5214(25)01865-8. doi: 10.1016/j.jvs.2025.07.062. Epub ahead of print. PMID: 41167378.
Kim Y, Weissler EH, Williams ZF, Mohan S, Coleman DM. Defining the Value of Vascular Surgery Service at a Tertiary Academic Medical Center. Ann Vasc Surg. 2024 Dec;109:198-205. doi: 10.1016/j.avsg.2024.06.040. Epub 2024 Jul 24. PMID: 39059626.
Powell R, Brown K, Davies M, Hart J, Hsu J, Johnson B, Makaroun M, Schanzer A, Shutze W, Weaver F, White J; SVS Valuation Work Group. The value of the modern vascular surgeon to the health care system: A report from the Society for Vascular Surgery Valuation Work Group. J Vasc Surg. 2021 Feb;73(2):359-371.e3. doi: 10.1016/j.jvs.2020.05.056. Epub 2020 Jun 23. PMID: 32585182.
Johnson CE, Manzur MF, Wilson TA, Brown Wadé N, Weaver FA. The financial value of vascular surgeons as operative consultants to other surgical specialties. J Vasc Surg. 2019 Apr;69(4):1314-1321. doi: 10.1016/j.jvs.2018.07.035. Epub 2018 Oct 24. PMID: 30528406; PMCID: PMC8386947.
PTFE bypass to a smaller tibial artery with Taylor vein patch
One of the conclusions of the BEST-CLI trial (ref 1) was that of equivalency between alternate bypass conduits and interventions when a single saphenous vein is not available. I recently contacted Dr. Matt Menard to see if there had been subgroup analysis of these bypasses which represents a heterogeneous group of conduits including PTFE, PTFE with vein patch, spliced vein, composite vein, and even possibly allograft. The results from the abstract were intriguing -“83 of 194 patients (42.8%) in the surgical group and in 95 of 199 patients (47.7%) in the endovascular group (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; P = 0.12) after a median follow-up of 1.6 years” with the primary MALE endpoint. If this was a football game, there would be a video review of the call. And they are looking at this, I was assured by Matt, but we would all have to wait for this year’s SVS VAM. Dr. Matt Menard is coming to speak at our 12th Annual Vascular Disease Update (link) which I highly encourage you to register and attend (addendum).
The Cohort 1 from BEST-CLI is an illustration of the vascular surgeons’ LIMA to LAD. It’s something we already knew from years of experience, but laid out in level 1 data (below).
The BEST-CLI paper is short on detail about cohort 2. This is where a lot of clinical decisions get made, and I suspect the vast majority of patients are getting interventions because fewer surgeons are facile with leg bypasses and vein patches.
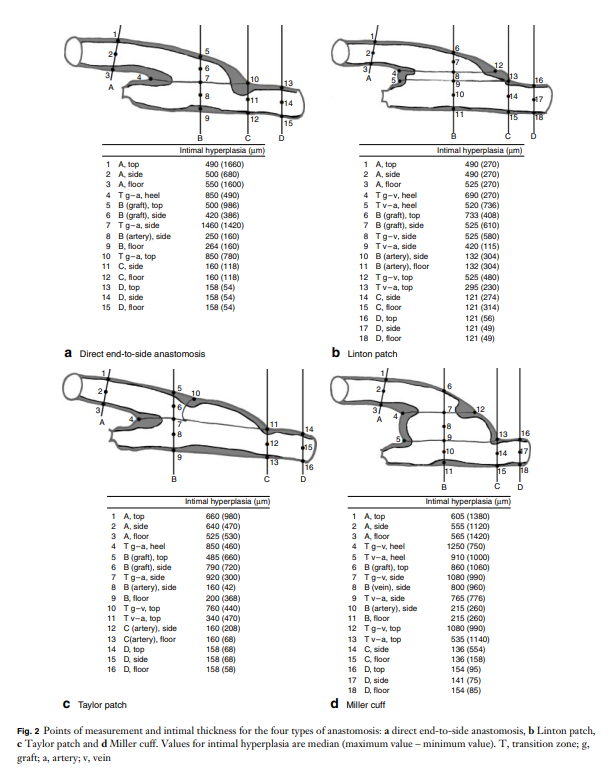
Why the vein patch? While not a panacea for the lack of vein, from its inception, it has proved a worthy adjunct in limb salvage. Decades before endovascular therapies showed good limb salvage with modest to poor patency rates, Dr. Frank Veith showed that infrageniculate PTFE bypasses showed good limb salvage with poor patency (reference 2). Vein patches, such as the Taylor patch illustrated at the top, showed good patencies (reference 3) in an era where DOACS, DAPT, and statins were not available.
Results of the Taylor Patch from Mr. RS Taylor.
Why a patch works is debated. Some feel it is the modification of the end to side anastomosis that creates an optimal shape for containing turbulence which leads to intimal hyperplasia. This was the concept behind the Distaflo graft which I tried but have abandoned for not improving patency in my personal experience.
The Distaflow Mini-Cuff which applies the concept of flow optimization by the shape of the anastomosis achieved by vein cuffs.
The best explanation of why vein cuffs work is from an animal study from Vienna. Intimal hyperplasia is best explained as a foreign body reaction and the reaction is worse with a true foreign body than with autologous materials. A simple anastomosis with PTFE to tibial artery creates a ring of hyperplasia. Vein patching moves this severe foreign body reaction off of the artery, leaving a gentler vein to artery reaction to occur on the outflow (reference 4).
My final point is that these surgical papers used to be the mainstay of podium presentation in the 90’s and ’00’s, but are now infrequent as the bulk of the time at these meetings is devoted to gadgets which almost always involves purchasing a box and contracting for disposables (the printer and ink business model). I am going to review our institutional results of these PTFE bypasses, and hope to see more from other groups. I look forward to the BEST-CLI papers to come, and other trials.
References
Farber A, Menard MT, et al. BEST-CLI Investigators. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N Engl J Med. 2022 Dec 22;387(25):2305-2316. doi: 10.1056/NEJMoa2207899. Epub 2022 Nov 7. PMID: 36342173.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
Taylor RS, Loh A, McFarland RJ, Cox M, Chester JF. Improved technique for polytetrafluoroethylene bypass grafting: long-term results using anastomotic vein patches. Br J Surg. 1992 Apr;79(4):348-54. doi: 10.1002/bjs.1800790424. PMID: 1576506.
Trubel W, Schima H, Czerny M, Perktold K, Schimek MG, Polterauer P. Experimental comparison of four methods of end-to-side anastomosis with expanded polytetrafluoroethylene. Br J Surg. 2004 Feb;91(2):159-67. doi: 10.1002/bjs.4388. PMID: 14760662.
Addendum
The Annual Vascular Update at University Hospital has something for everyone, including a presentation on IRAD by Dr. Santi Trimarchi, and BEST-CLI by Dr. Matthew Menard. Local faculty from Cleveland are also featured in a broad review of vascular medicine and surgery chaired by Drs. Mehdi Shishehbor, Heather Gornik, and our chair in vascular surgery, Dr. Jae Sung Cho. Link. I will be presenting on neurovascular compression syndromes and renal failure/heart failure.
Reading this article on Vascular Specialist, the vascular surgeons’s Daily Prophet, “Likes, dislikes and reposts: The new age of the vascular surgery influencer” by Drs. Jean Bismuth (@jeanbismuth) and Jonathan Cardella (@yalevascular), they rightly point the spotlight on the trend of some vascular surgeons posting cases on social media for the purposes of self-promotion, virtue signaling, and influencing.
I can agree with their point that many of these posts are made by mediocre practitioners who display only the best and curated images, but I felt uncomfortable with the feeling that I may be one of those people being castigated for over-exposure on social media. They warn the readers of the dangers of misinformation fed to an uninformed public, but overlook the potential of social media for education and community. Being a vascular surgeon who has been on social media for over a 15 years, there are reasons why I am here which are not explained by this article, and I am compelled to elaborate on them.
Be the Lede
My journey started with hacking Google searches. My first job out of fellowship was a faculty position at my medical alma mater, Columbia P&S. The PR department asked everyone to compose a blurb for a web page and after searching on Google on how to rise in a Google search, I wrote out a paragraph full of the right verbiage to maximize my relevance on search. It wasn’t very difficult in 2002 to do this. Searching “vascular surgeon in New York” on Google after posting that info page consistently brought me up to the top five links, ahead of whole departments and many big names. I did over 400 cases my first year out, and I really felt if I could make it there, I could make it anywhere.
Bury the Lede
Unfortunately, like many vascular surgeons in New York, I got named in a lawsuit, and like many young surgeons with limited means and large loans to pay off, I couldn’t fight it and took the advice of hospital lawyers and settled. After that lawsuit, a Google search would return an article by the law industry PR around 2007, and I was at that point very busy in private practice in Iowa. It was so discouraging seeing that as the only thing speaking for me. I decided that I had to take an active part in shaping the message around me, to not let my Google search profile be defined by that article.
I decided to write and figured a few articles every week over a year would bury that article behind many better articles. I began to blog about something I am both horrible at but aspire to greatness in –golf (www.golfism.org). Writing about myself and my struggles in golf and being a young father and husband was how I found my voice. It was during this period that I found my best pieces were when I gave something of myself.
After finding my author legs, I began writing about vascular surgery, something I’m pretty good at but aspire to greatness in, on a personal blog (docparkblog, on Apple’s defunct cloud service). After a year, the blog got only 30-50 hits a day, at most 100. By internet standards, that’s low, and I kept my day job. After giving a talk at Midwest Vascular to an audience of about 50 mildly interested surgeons, that 30-50 engaged readers on my blog a day felt pretty good. A hundred was amazing. Medscape eventually tapped me for blogging on their site. My blog there, “The Pipes Are Calling,” was rated among the top 5 most read medical blogs in the world when I shut it down in 2011.
The Influencer
This social media presence generated influence -I was asked to participate in prominent research trials like PIVOTAL, CVRx, and CREST and others despite being in private practice. This is common now, but rare 15 years ago. The blogging did bury the lede. It eventually generated misunderstanding in the hospital administration at that time in 2011 and I was asked to stop blogging, at least until they could figure out what this internet thing was about. In 2012, I joined the Cleveland Clinic, I huddled with their social media department and came up with ironclad rules:
All accounts were to have the header that posts and articles were my own opinion and not of my employer
All patients sign a media release for posting of case histories and images
After launching www.vascsurg.me in 2013, I chose to focus on technique and opinion. I used my Linked-In and Twitter accounts to promote my articles. I always communicate in my authentic voice, although over the years, I’ve toned down the irony which is frequently misunderstood. In moving to my current hospital, University Hospitals, the first thing I did was arrange for a social media release and confirm what I was doing was okay. In reading the article by Drs. Bismuth and Cardella, in 2023, misunderstanding is still at the core of arguments against the use of social media.
The Worst
I have seen egregious examples of bad behavior on social media by physicians, as mentioned in the article. On my Twitter stream, I’ve seen people put stents in subclavian veins for thoracic outlet compression and wait for praise, which they get from similarly ill informed people who don’t realize I see patients like this several times a year with swollen arms and faces. While I was in Abu Dhabi, someone put stents in a patient from the common femoral to popliteal artery, and receive accolades for “minimally invasive skills” from all corners of the globe, only for me to remove the stents a month later and perform fasciotomies on the same patient -a middle-aged claudicator! There, I couldn’t post a rebuttal to the original case presentation because of local social media laws. Despite the word getting out, the surgeon only doubled down on his minimally-invasive fantasies. About the same time, I witnessed a relatively famous person self-implode on Twitter while accusing vascular surgeons of butchery (his words) by supporting open surgery over head to toe interventions. He got crushed by the general disapproval of his misrepresentation and personal bullying of a vascular surgeon, and then disappeared from social media. Evaporated. Good. We all have to do better.
The Best
I have also seen patients with rare diseases such as median arcuate ligament syndrome reach out and connect with each other and with physicians about diseases that aren’t taught in medical school or residency training on social media. There are Facebook groups, Twitter hashtags, and sub-Reddits, a rich communities of people who have to make serious decisions about their lives, many with limited access to specialists in their far-flung burgs and precincts. I think the fear is that bad decisions will be made based on bad information, but even in the highest, most rarified medical institutions, patients may get misguidance, have a complication, a poor outcome, in-person which can be worse than a social media interaction. If we value patient autonomy, access to the best information needs to be available. Social media lowers the barriers to access, for bad or good. Yes, it can do a whole lot of bad, but also an immense amount of good.
Keeping it Real
The authors are correct in that people will prefer to promote themselves rather than air complications and bad outcomes. The American surgical M&M process is an amazing and cherished tradition and protected process. It has no place in social media. Most surgeons also take the view that social media presence doesn’t lengthen your CV, it doesn’t bill. The many cheap suits of medical social media, the hawkers, the hucksters, the fragile egos will always be there on Twitter and Linked-In.
But other functions such as access and broad dissemination of information, experience, and opinion, are legitimate and critical. Comparatively few people get the message from a closed academic conferences and traditional modes of dissemination are slow. Most of the best social media posts are, as the authors mention, case reports. They fail to mention case reports under “open access” cost about 500USD to publish.
The peer review process, which I participate in, results in sometimes glacial turnaround times with papers landing often a year or more after presentation at a conference. I also learned from my time in private practice that these barriers block the voices of many legitimately great surgeons whose remarkable talents are only shared locally. I also learn from my time in academic practice that too many departments are not multiplicities of talents (Avengers Assemble!), but shops built around single personalities, who may declare that having never seen something, it cannot exist -to the detriment of those with unseen problems. Social media is the great leveler. Young surgeons can raise their profile, and non-academic surgeons can have a broader platform to share their expertise. If legitimately good people are dissuaded from participating, only the cheap suits will remain. As always, caveat emptor, et primum non nocere.
Every time someone on Seinfeld went to the hospital, a stock scene (above) would play. It’s the old ER of Roosevelt Hospital on 9th Ave before the renovations moved it to current 59th street entrance. I was a surgery resident there in the 90’s and watched each Seinfeld episode for the upper West Side stuff that would pop up. The soup Na2i was a few blocks over. Not seen on this pic is the Sym’s operating theater designed by Dr. Charles McBurney which is a designated landmark and currently a private school for “gifted but difficult” children (link). I used to round on patients in the red building -they would be ten in a room separated, if lucky, by rolling privacy screens. My sister was born here. John Lennon died here. All that gone, because hospital buildings are like dressings on a city’s wounds and need to be changed every generation. In fact, it’s not even called Roosevelt Hospital any more.
Roosevelt Hospital’s name was changed to Mount Sinai West, and its sister hospital, St. Luke’s, was changed to Mount Sinai Morningside. I would like to imagine that it was vengeance a century in the making, for pearl clutching slights originating from the gilded age, of blue bloods v. upstart Jews. Because no matter how far you are from the shtetl, there is always another golden door closed to you in New York City. So it seemed for me, an immigrant who had worked hard to get to Harvard College, and Columbia P&S, to look with squinted eyes at my letter on match day and see St. Luke’s/Roosevelt Hospital Center, my last choice that I listed out of a general interest to avoid not matching.
When I landed on St. Luke’s-Roosevelt for my general surgery training, the house officers were quartered in the older parts of the hospital, some rooms dating back to the 19th century, unchanged like unearthed chambers from Pompeii. Both hospitals still had the open wards for the “ward” patients with segregation of the private patients up in the towers. For a time, they still had seamstresses to mend your white coat and cafeterias that still cooked their foods fresh. The resident’s lounge at St. Luke’s was like a frat house common room from the thirties, with a scratched-up pool table, a broken piano, pedastaled hotel ashtrays, and card tables. An old handprinted sign (which I regret not taking) listed the house officer’s rules and entitlements which included two beers or a shot of whiskey per night on call.
After my intern year, both hospitals started sorely needed renovations. The surgery office had to be cleaned out, and behind an antique cabinet, wooden boxes of chromic cat-gut suture were found, still in their glass tubes and preserving fluids, little brown skeins of suture floating like preserved fetuses, a strange message from a faraway time. I ran into Walter Wichern, chairman emeritus, who showed up randomly to the hospital in blue blazer and bow tie. I had just stained my dress shirt pocket with my soon-to-be-lost Mont Blanc fountain pen, and he launched into a story about how he repaired a ruptured aortic aneurysm back in 60’s by cutting his new polyester dress shirt into a tube and sewing a graft out of it down in the laundry, after hearing a talk from Arthur Vorhees at P&S. And he was smiling an enigmatic little smile, recalling how that patient on being discharged gifted him annually with ten new dress shirts every year. I later found out that Dr. Wichern was famously taciturn, and I had somehow unlocked an achievement -getting a story out of an old surgeon. It was around then that I had started to feel that it wasn’t all a big mistake.
When I recently changed hospitals from the Cleveland Clinic to University Hospitals, I had to submit documents for privileging, and I get a testy email. “Where did you do your residency?” The administrator couldn’t find St. Luke’s/Roosevelt anywhere on the ACGME website, or even on Google. When I offered the new names, the reply came back, “They only have records going back to when they took over in 2008.” I briefly contemplated retiring, then asked if sending pictures of my framed degrees would be sufficient. Only partly, was the reply. She wanted witnesses.
My first night on call was terrifying. I was on call with Bobby Borromeo -my fellow intern, Anil Hingorani -our PGY4, and Jesse Jean-Claude -our Chief Resident. All of us are now practicing vascular surgeons -Bobby (fellowship Yale), Anil (fellowship Montefiore), Jesse (fellowship UCSF), and myself (fellowship Mayo), embarked on a night of call that involved no sleep and little food. The single moment I recall was taking Bobby through a blood draw and filling the forms for processing the labs and performing EKGs with an antique strip recorder, cutting and pasting the strips onto a formatted sheet for the chart. Bobby didn’t know how because there were many people to do these things in his home hospital in the Phillipines. For myself, I knew the two hospitals from my rotations during medical school. I could draw blood and cut, sew and tie above my level from my time as a senior student at P&S. I got a bit too comfortable with my privilege, and I was still thinking I should have been somewhere else. Over breakfast, I absentmindedly voiced this out loud and was corrected in a way that is no longer possible in 2022. It was the tone that I remember, of being chewed out.
One of chiefs snapped at me,”You have no idea how big and important these hospitals are. They are older than all the other hospitals here in NY. McBurney did the first appy here. Halsted was chief at Roosevelt and invented cancer surgery and the surgical residency. Green invented the LIMA bypass at St. Luke’s. Our chiefs go to better fellowships year over year than any other hospital in Manhattan. You should be grateful to be allowed to round with us.”
Tie given out at graduation, designed by Howard Nay, MD (link), RIP. One of the few keepsakes of my time there. Dr. Skip Nay, was old school, and gave everyone nicknames. Learning surgery from him was like taking blues guitar lessons from Mr. Robert Leroy Johnson.
It was by my third year I got used to the 120 hours a week. It is only now a quarter century later, that I value it. I was expending my. youth living and breathing surgery in the latter days of St. Luke’s and Roosevelt Hospitals. I was missing my friend’s weddings, missing time with my wife, seeing New York during the glory of the 90’s through the dank recesses of a trauma bay. I was six figures in debt, but I could take out your appendix in twenty minutes. I had just signed on for a year of research with the peerless Dr. David Tilson and was not looking forward to telling my wife who found the original five year deal of residency interminable. Add to that, two years of fellowship. Walking out on the deck of the call room overlooking the Cathedral of St. John the Divine and Columbia’s campus, listening for the sirens, I really felt the spirit of the hospital.
It’s not the name of the place, neither its splendor nor its comforts, but the commitment of the people in the teams that you build, which allows you to do great things. And yet…
Summer 2022, in front of Mt. Sinai West, formerly and forever Roosevelt Hospital.
When I was a young attending at the Allen Pavilion of Columbia Presbyterian Hospital, I was called into an operating room for a stat consult on a patient about to undergo a cholecystectomy. During the case, the IV had infiltrated and a bag of saline had filled the patient’s hand and forearm with saline, causing the hand to look like an inflated glove. The fingers were cool and white and the edema was firm but yielded to touch.
I elevated the hand and firmly squeezed the edema out of each digit, then gently massaged the edema from the hand onto the forearm. From there, I pushed the edema onto the arm. I then wrapped the hand up in an Ace wrap, and suspended it from an IV pole and returned to my case. Later, I returned and the hand was restored, warm, and perfused.
The lymphatics serve to move extracellular fluid (link). They can be overwhelmed much as drainage from a house can be overwhelmed resulting in puddles and ponds (link). This extracellular space has been “discovered” to be a new organ, but vascular surgeons have known about it for some time. Ultrastructurally, it is very close to a sea sponge with lattices of structural protein connecting cells to form tissues. And like a sea sponge, the salty water can be squeezed out or drained using gravity.
In olden times in central Europe, if you had chronic leg ulcers, you went to abbeys that specialized in their care. There, nuns would milk the edema out of your leg swollen typically from parasites and dress the leg and ulcer in linen cloth soaked in special oils. This is how Dr. Paul Gerson Unna came up with his eponymous Unna’s Boot, substituting Zinc Oxide paste which created a bacteriostatic environment.
Professor Paul Gerson Unna
Every year or so, I will be consulted for what I term a lymphatic emergency. A subset of this is phlegmasia. Whatever color you find -alba (white) or cerulea (blue) is really no matter -who really knows which comes first? It is an emergency in that the time clock for arterial ischemia -minutes to an hour for nerves, an hour to 6 for skeletal muscles, 6-12 for skin and bone, are all in play. The instinct is to go right to fasciotomy, but what you are usually doing is releasing the extracellular space, and the muscles are typically fine, even though their compartment pressures were very high.
Take this patient who developed severe upper extremity edema in the recovery phase after a cardiac arrest.
The ICU staff noted the had discoloration about four hours after the arrest. There were no arterial pulses and the forearm and hand were rock hard, the finger tips ice cold. Compartment pressures measured using the arterial line and needle method didn’t drop after the initial flush of saline below 70mmHg. While I could have been justified in performing upper extremity fasciotomy and even trying thrombectomy in a critically ill, coagulopathic patient on multiple pressors, I could just as easily have been on solid ground for saying the life was more valuable than the dominant hand. Both would have been the wrong move.
I performed the nun’s milking maneuver mentioned at the beginning and lacking an Unna’s boot, I compressed and elevated the best I could with double gloving using a small sized glove and ACE wrap.
Notice the edema has segregated into the arm.
In the morning, taking down the dressing, and re-compressing, there was now a radial artery signal and the fingers were a much improved color. The pulse-oximeter waveform was near normal. As an aside -the pulse oximeter uses the same technology as the digital photoplethysmography for generating toe waveforms in the vascular lab -ie. a vascular lab at every bedside! We have collected and are analyzing the data on this for publication.
The pulse oximetry waveform is the same tech as digital photoplethysmography. Cotton cast padding (Webril) and Coban wrap is a good method of compression that avoids the problems with ACE wrapping.
It’s a hard thing to not run off to the operating room in most cases because that is how we are trained, but understanding how a patient got to that point is crucial in deciding if compression alone will work. If they call you from the ER about a patient with a swollen cold foot with diminished signals, you have to figure out the mechanism. Was it arterial occlusion, rest pain, and chronic dependency of the foot that resulted in this? Typically the swelling appears late. Was it heart failure and inability to walk, resulting in the patient sitting all day in a chair that is the cause? Was it pregnancy with a DVT? Was it the deadly sin of sloth? Only in arterial occlusion in a chronic presentation would compression be contraindicate. In this ICU case, the lack of arterial signal is secondary to the swelling, not the cause of it.
Elevation alone does not manage edema well. Only hanging upside down or being in water up to your neck…
Compression is a necessary component of treating lymphedema emergencies because elevation alone may be insufficient, particularly in the leg.
Wrapping a leg is a critically, undertaught skill. Also, never cover the knee cap.
Elastic compression is ubiquitously available as the ACE wrap, but they can shift and move and roll, causing zones of excess and not enough compression. TED hose and compression stockings are definitely helpful in long term management, but with legs, compression needs to go up to the knee joint, or up to the groin, never halfway or the edema will create a line of ischemia at the end of the stocking that blisters when the stocking is removed, and can progress to full thickness necrosis. Cotton cast padding and Coban, or an Unna’s Boot may be the safest in terms of avoiding skin injury.
ACE wrapping is never taught adequately, and for it to work well and avoid injury to the skin, the wrapping has to be reapplied several times a day. It should be a prerequisite for nursing and medical student certification, as edema is the most common vascular disease.
Moving into our new home after four years out of country, I welcome an old friend from storage, but also unfortunately a health hazard, only mitigated by being fully reclinable.
Okay, so I have made this intermittent list of top ten gadgets and gewgaws which I used to to call “Top Ten Things to Get Your Favorite Vascular Surgeon” but even in jest, over the years that I have been publishing this blog, the world has changed. As a watcher of technology, I have always had my eye out for the next great thing, and here is my list. I hope you all have a great Christmas and a wonderful New Year.
Giant Laptops with Complications -old automatic watches with complications are still coveted, and the tech space is no different. Whereas, Apple has always veered to minimalism, there is an exuberance to adding “stuff” in among the Chinese manufacturers and ASUS is no different.
This laptop, the ASUS ZenBook Pro UX581 is a perfect example of innovation by jamming as much possible onto your ADHD-addled field of view. What would I use it for? Who knows, but I want!
2. Timex watches retroversions. Like automakers making updated versions of classic muscle cars, the old standby Timex, has launched watches that that make you want to party like it’s 1979.
The Navi XL Automatic 41mm by Timex is beautiful to look at and of all the knockoff Omega Seamasters out there, it is nice to see a classic American branded offering. Cheaper watches are a smart thing for surgeons in that it’s easy to lose them when you take them off to scrub for a case. While Apple watches are popular, the only square watches I like are Cartier Tanks, and for health data, I wear a Fitbit on my right wrist.
3. Entertainment tablets have made the large family TV obsolete. Add in good audio, and you have that weird future that they promised back in the 1980’s when they swindled your parents to buy a $3000 computer that really couldn’t do anything.
The Lenovo Yoga Tab is an incredible value for what you get which is a bright screen, fast enough processor, long battery life and great sound (JBL speakers with Dolby Atmos processing). It comes in 8, 10, and 13 inch sizes. Coupled with a keyboard and mouse, and an Office or Drive account, and you have a very portable workstation. The only thing missing is the ability to draw as it does not pair with a stylus.
4. E-ink based tablets. If you have ever had a Kindle, you know what an E-Ink based tablet is like. Viewable in direct light, these displays have the advantage of minimizing fatigue in the same way paper does compared to staring at a monitor. These 3rd generation tablets run full Android and can run the Kindle app, as well as advanced note taking and PDF markup software, and have that warm backlighting that comes with the modern Kindles.
The Boox Max Lumi does all of that. Paired with a keyboard, it recreates a basic typewriter well. It also functions as a second screen, allowing you to stare at and markup documents driven by a laptop computer. I want.
5. The modern update to the Psion Series 5mx. The Psion Series 5mx was a pocketable computer that ran a very efficient operating system, powered by two AA cells which lasted up to 40 hours, and had a tiny keyboard that with practice was fine for authoring chart notes that I would then print out to HP printers that that infrared ports (IrDA). This allowed me over a three year period of residency, to collect my personal EMR that I kept on a huge for that time 32mB flash drive. I sold my 5mx, along with a considerable box of hard to find accessories, to a journalist in Mexico who needed to author articles and fax them to his paper in 2007.
The Gemini PDA was made by a group of engineers and programmers who remember that time and updated the Psion Series 5mx form factor, down to the legendary keyboard. Available in Android and a Linux, it is a pocketable microlaptop.
6. Asian stationary, notebooks and pens, are next level. In certain malls in coastal cities in the US, you can find the odd Japanese store that has a section for stationary. The bindings are fantastic and the pens work forever. My favorites are mechanical pencils and fountain pens, which despite the incredible builds, are really affordable.
7. Instant Coffee is anathema to serious coffee snobs. I have a friend who keeps a water heater, lab style glassware, digital food scale, and grinder to make a perfect cup of drip brewed coffee for himself -a fifteen minute process. The disposable pod coffees -blurgh. In Abu Dhabi, I got introduced to high end instant coffees at the grocery -the packaging and brands oozed luxury, and the coffee was much better than the instant coffee I grew up with.
Mount Hagen Fairtrade Organic Freeze Dried Coffee is what I found as an alternative to the old instant brands that represented bad instant coffee. This stuff mixes well with cold water as well, and delivers a bright kick of caffeine. It lets me make a to-go cup of coffee, well, instantly.
8. Headlights are always fun, but running in them is challenging because they sit off the center axis and tend to drop down. I have tried many times to incorporate them as cheap operating room headlamps, but failed largely as they are not bright enough. These light band headlamps which popped up in my Facebook were intriguing.
These lights (link) have both the light band which is amazingly bright and a regular flash light on the side, both of which can be turned on by waving your hand by a sensor next to your head. I thought this was the answer to my search for a cheap OR headlamp (the regular ones cost way over 1500USD), but the problem is that anyone looking at you is immediately blinded and their retinas seared. But for running, these forehead based high beams are amazing.
9. If you are surprised at the lack of Apple products, it’s because I typically aren’t in the market for them. They last forever. My 2007 Macbook Pro still runs, survived a major upgrade which included maxing out RAM and swapping the spinning platter hard drive for an SSD, resulting in lightning speed. Unfortunately, they are exhorbitantly expensive and so I find myself hesitating at purchasing a 2500USD laptop, especially one that I can no longer upgrade and maintain as I could the older Apple laptops. The problem is the battery and the SSD. They have finite lives. You can still buy batteries for the 2007 Macbook Pro, and get all day work from several batteries. Apple solves the problem of owners keeping their Apple gear for decades by imposing obsolescence, and recently even slowing down the performance of older machines to get owners to buy new iPhones.
So this makes the purchase of iPad, Macbook Pro, and even the iMac problematic in that they are all closed box systems with limited lifespans. Of the recent Apple products, the best bang for the buck comes from the Mac Mini. The older ones from 2012 can be found in droves, refurbished, and can still be upgraded, but the new ones with the blisteringly fast M1 chip that can run iOS apps is worthy of my consideration. It may be the last Mac that I ever purchase. My 2007 MacBook no longer runs the latest OS version, and I will be turning it into a Chromebook.
10. Typewriters are a fantastic way to write. They don’t let you check social media or email, and encourage that focused state where words just flow. That is the concept behind the Freewrite and its special edition Hemigwrite.
Whatever you type gets stored in you choice of cloud account, including Google, Dropbox, and Evernote. You can work on 3 different files, and as you type, the Wifi connection updates your file in the cloud. The keys are that clickety clack mechanism reminiscent of original keyboards from the 80’s, and the E-Ink screen, now backlit on this beautiful aluminum clad Hemingway edition of the Freewrite, makes it easy on the eyes. The great American novel awaits to come erupting out of your head.
Recently, in clinic, my nurse handed me the patient sheet with the comment, “this is for iliac stents.” This caught my attention as “iliac stents” does not make sense as a chief complaint. The patient had been sent with a vascular lab report. It was a duplex scan documenting peak systolic velocities over 300cm/s in the common iliac arteries, appropriately diagnosing 50-99% stenoses. The patient had hip and thigh pain with walking short distances. I could have been excused for just cancelling the visit and booking an angiogram, except that would make me just a technician responding to a request. So I talked to the patient.
The patient was a nice lady over 70 years of age with recent onset of hip and thigh pain with walking 50-100 feet. This was incapacitating her as she was used to living an active and independent lifestyle. Her pulse examination was normal, not an uncommon finding with aortoiliac occlusive disease which manifests as a hemodynamic phenomena best explained as “small pipes.” Except she had never smoked, and had only hypertension and mild hypercholesterolemia. The review of systems was notable for fatigue and arm and shoulder pain. While she had not lost weight, strangely, her jaws hurt when chewing food.
I do not claim any kind of magic skills when it comes to diagnostics, but these other complaints did not fit. And it is not uncommon for someone to have several common conditions. Maybe she had TMJ, shoulder arthritis, early heart failure, and aortoiliac occlusive disease, to fit all of her complaints. Why was I wasting my time diving into nonvascular ephemera when I could be sending her to be scheduled for an aortogram and iliac angioplasty and stent?
I’ve carried with me this notion that all physicians can be mapped on x-y axes with one axis representing degrees of intelligence peaking at perfectly smart. Perfectly smart doctors have seemingly magical skills. While they are not rolling back their eyes while waving their hands over the patient, the handful of perfectly smart physicians I have worked with can quietly listen and digest a case and come up with the diagnosis, no matter how obscure and rare. On the other axis is compulsion, with the perfectly compulsive marching their patients through every test and algorithm to rule out every diagnosis on a exhaustively long differential list.
Intelligence and Compulsion, Written with a Doctor’s Penmanship
Those striving to be perfectly smart hope to bring efficiency to the clinical process -such as for this patient, it would have made sense for efficiency’s sake to move forward with an exercise treadmill ABI test and booking for an aortogram. Those stuck in perfect compulsion never quite reach a diagnosis, even after ordering batteries of tests, but rarely make mistakes, which is the point of perfect compulsion, because if you carpet bomb the diagnostic possibilities, something will hit. They are especially bulletproof to malpractice, particularly when patients choose not to have any more tests out of exhaustion. Their patients are rarely happy having to go through a myriad of tests to paint away the rule-outs while never quite identifying the disease. Those who play around with being perfectly smart get burned by that which are unknown and unfamiliar. They get blindsided. You want to revert to compulsion when you are tired and overloaded. You want to be smart, all the time.
The point of training, which never ends, is you have strive to be both perfectly smart and selectively compulsive, but it’s better to be lucky than good. It was my luck that I recently reviewed temporal arteritis. Every few weeks, I get asked to remove temporal arteries, and choosing not to be just a technician (although admittedly in the workup of TA, we kind of are), I plowed into UpToDate and Pubmed, seeing if there was a way out of doing these procedures -there really is not, except in the requests for temporal artery biopsy in younger patients -go read it yourself. It was here that I refreshed myself on polymyalgia rheumatica, which has as its symptom complex, muscle pain, lethargy, and jaw claudication. Out of duty, and compulsion, I ordered a CTA, because I knew that the patient had risk for atherosclerosis and arteries stiffened by calcium can have elevated velocities without critical stenoses. Out of curiosity, and after a quick call to one of the Clinic’s rheumatologists who order these temporal artery biopsies, I ordered an ESR and CRP.
The CTA came back with calcium at the aortic bifurcation and origins of the common iliac arteries where the outside duplex showed elevated velocities, but only revealed mild disease on the CTA. Both ESR and CRP came back very elevated. I referred the patient to our rheumatologist, and with steroid therapy, all of her symptoms resolved. Without an aortogram or stents.
I sat and thought about this for a while before posting. The patient was quite happy to give her permission. I cannot fault the outside vascular lab for their diagnosis of iliac stenosis because the diagnostic criteria are basically the same as our labs. It has made me think that approaching this case as a revenue opportunity as increasingly happens would not necessarily have been in error if I had performed an aortogram as long as I did not place stents. I can’t imagine the pressures put upon physicians who have put themselves into situations where they are paying for costly angio suites or their own 90th percentile salaries and lifestyles from not over-calling a stenosis and deploying stents, particularly when there is no oversight.
41 percent of my patients with median arcuate ligament syndrome present missing their gallbladders because biliary colic was the diagnosis that was both familiar and vaguely fit the complaints (reference 1). Not much harm can come from taking out a gallbladder, no? We know that a minority of operators harvest a significant share of the Medicare pie when it comes to peripheral interventions (link to terrific OPED, reference 2). Oh, I am sure each of these cases can be “justified.” Pleading justification from limits of knowledge means I proceed to treat what I am familiar and comfortable with -vascular disease, rather than an unfamiliar disease (at least to vascular surgeons) like polymyalgia rheumatica. If I can fail to recognize my ignorance, who can fault the perfectly compulsive? Like a broken clock that can be correct twice a day, someone of poor intelligence but perfect compulsion can be more effective than a greedy hack seeking to be perfectly smart and efficient.
Dunning and Kruger found that those with lower competence overestimate their ability, and those with higher competence underestimate their ability. Medicine is a perfect laboratory of Dunning Kruger. To be effective, you have to be correct and assertive. The problem is you are trained to project that confidence in the early stages of training and career when you are not ready. What patient would seek an unconfident physician? What person truly knows what they don’t know? The hardest step in medicine is both admitting what we don’t know but also applying hard-gained knowledge and experience with audacity. True humility comes from self knowledge and awareness. False modesty is externally directed, but true humility is internally focused. I don’t have a pat answer, but to become perfectly smart, you have to be perfectly compulsive about filling your knowledge and experience base. You have to submit your complications for peer review, you have seek and collaborate with sound partners, and you have to avoid financial traps that bias you to bad behavior. Above all, you have to stay curious.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
Sheaffer WW, Davila VJ, Money SR, Soh IY, Breite MD, Stone WM, Meltzer AJ. Practice Patterns of Vascular Surgery’s “1%”. Ann Vasc Surg. 2021 Jan;70:20-26. doi: 10.1016/j.avsg.2020.07.010. Epub 2020 Jul 29. PMID: 32736025.
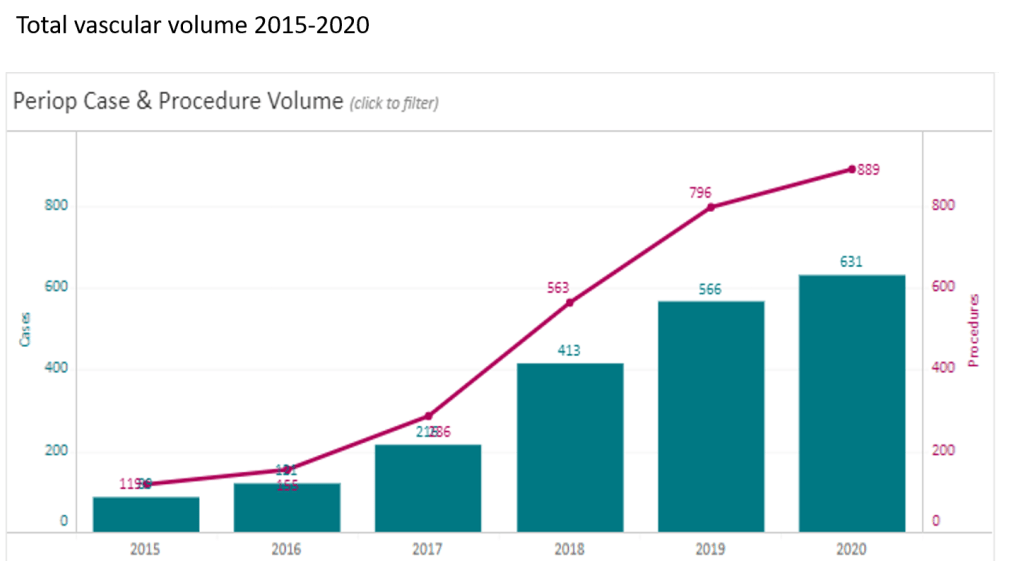
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
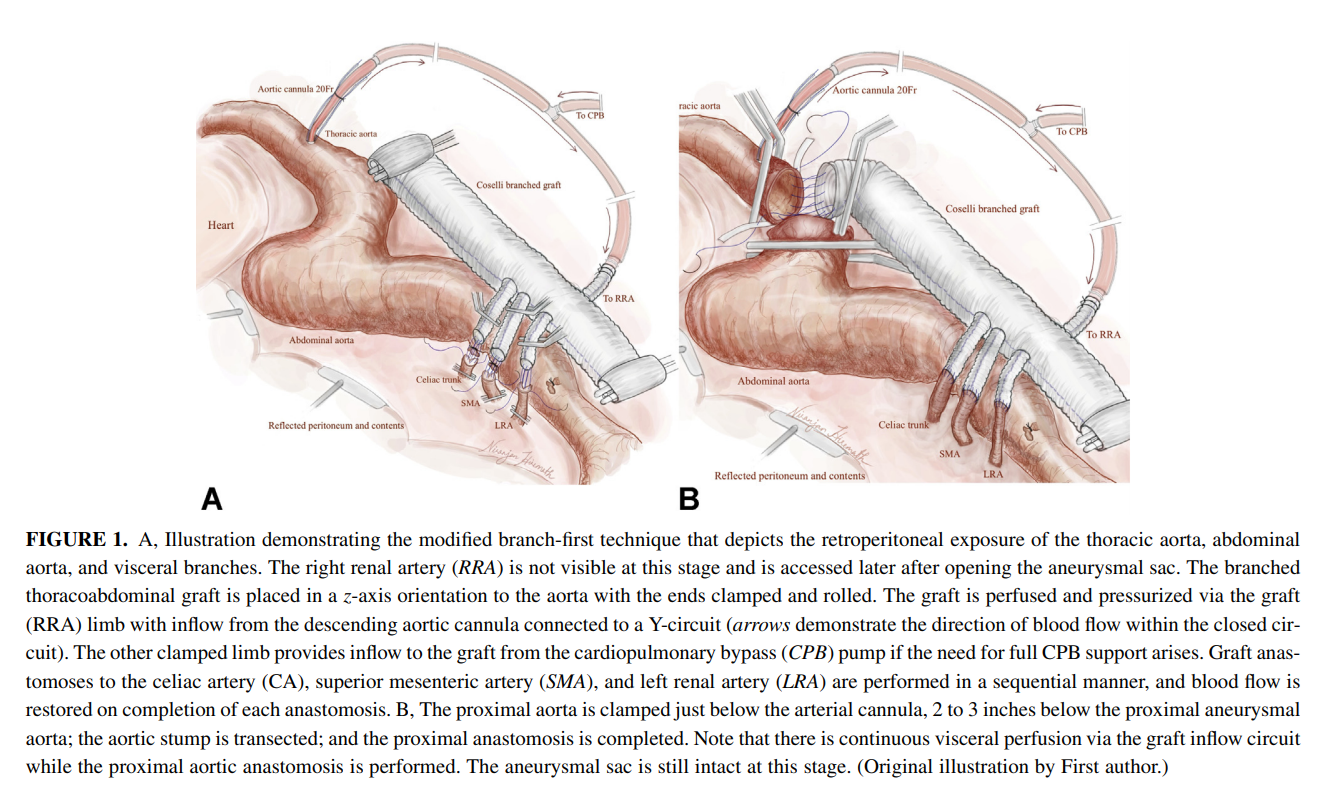
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
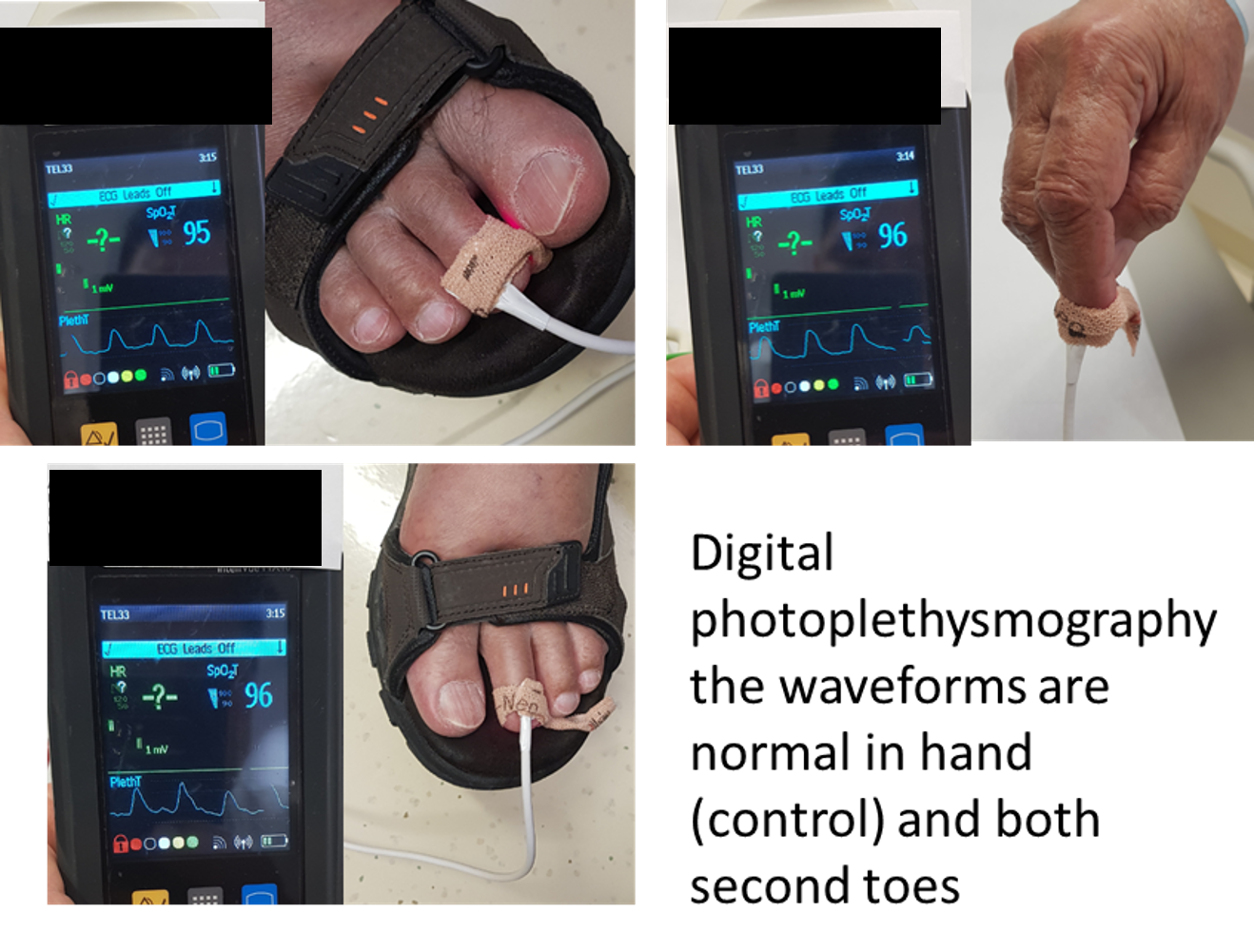
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.
This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).
an abnormal DPPG captured with a hospital ICU pulse oximeter
We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).
At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).
The distal perfusion cannula is in the dorsalis pedis artery
This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery
The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).
Pulmonary artery staple line bleeding controlled, ready for suturing.
In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.
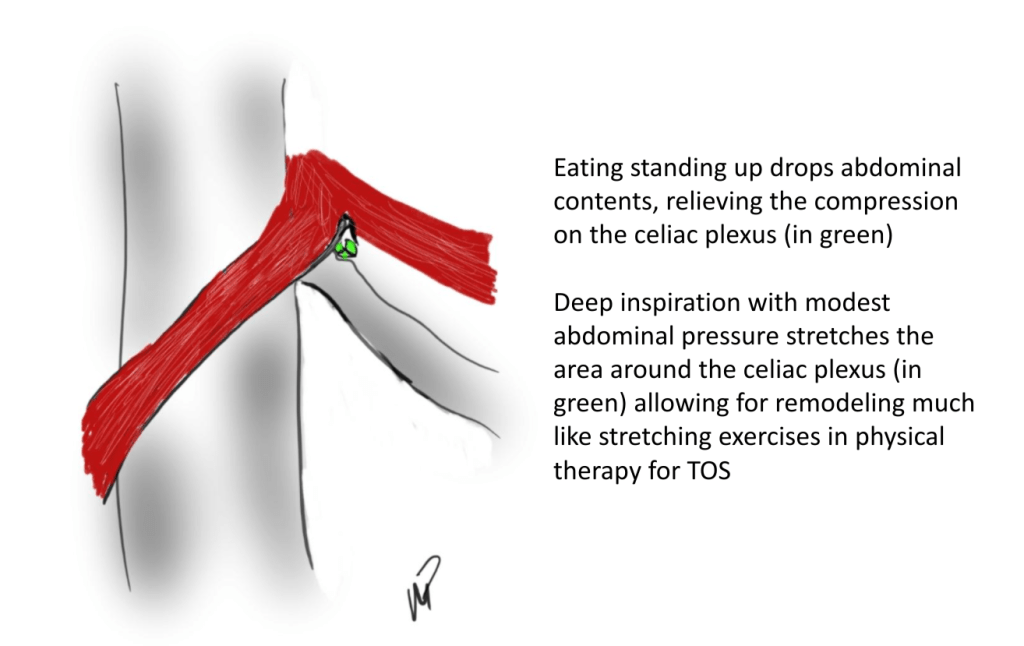
The patient is a young woman who presented with classic symptoms and findings of median arcuate ligament syndrome (MALS). She avoided food because eating triggered severe pain in her upper abdomen. Over a year, this resulted in 15 pounds of weight loss. As a result, she no longer had the energy to work or exercise. She had an extensive gastrointestinal workup including blood work (LFT’s, amylase, cholesterol panel), abdominal CT scan, and upper endoscopy which were normal except for the finding of narrowing of the celiac axis due to compression by the median arcuate ligament. Examination was notable for upper abdominal pain exacerbated by pressure and seated, hunched-over posture. Unfortunately, due to her health insurance, surgery was not covered and she did not want any. So I recommended she try the following.
Eat standing up with good posture, shoulder back, back arched, taking deep breaths and holding once food passes
Practice upward facing dog yoga pose (figure) 5 reps daily with deep inhalation breath holds. If this is difficult, do this standing up.
Improve the posture during seated work, never hunch over and pressed forward with “shrimp back,” periodically take a deep breath and hold with excellent posture.
Upward facing dog yoga pose -shoulders square, outward collar bone tension, with deep inhalation breath holds
Over the past several years, I’ve noted that most patients respond to this, even in acute MALS pain situations (yes, there is acute MALS like slipped discs, for another post). That patient came back a few weeks later reporting that she was able to eat more food, more frequently. She also acknowledged compliance with the exercise and postural adjustments at work. A month later she reported regaining her lost weight and only mild pain with sitting in a car for a long time. She was still eating standing up, and she was grateful for having been treated without surgery.
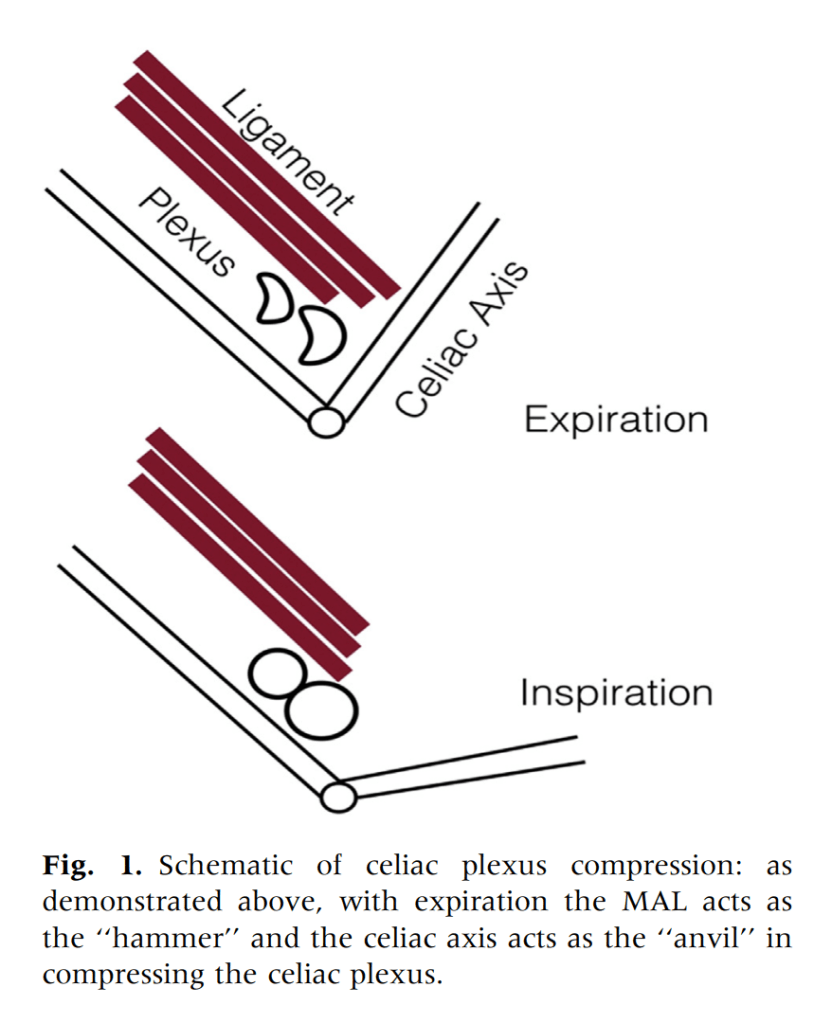
From reference below, a mechanism for celiac plexus compression, injury, fibrosis, and development of neuropathy
We have postulated that MALS is a nerve compression syndrome of the celiac plexus by the median arcuate ligament (reference). There are two consequences to MALS, neither of which is mesenteric ischemia. The first is this compression of the celiac plexus with injury resulting in inflammation and fibrosis, resulting in further compression and a neuropathy of the celiac plexus. This neuropathy triggers aberrant pain sensations in response to eating. The other consequence is remodeling and injury due to arterial compression. The celiac axis can develop post-stenotic dilatation, growing large enough to be considered aneurysmal. The compression can damage the intima resulting in dissection. The artery can be injured and a pseudoaneurysm can develop. Finally, the aneurysmal segments may develop thrombosis and be the source of thromboembolism, usually to the spleen. Even when the celiac axis clots off, unless there has been resectional surgery such as a Whipple or splenectomy, the stomach gets enough collateral flow that ischemia is rare when celiac axis occlusion occurs. So similarly to thoracic outlet syndrome (TOS), there is a neurogenic MALS and an arterial MALS.
The first line of therapy in neurogenic TOS is physical therapy. With symptomatic MALS, I wondered if there could be physical therapy as well. This young woman and others I have managed nonoperatively suggests good response in some, and partial response in most to exercises and maneuvers designed to address the compression.
Currently, in lieu of celiac plexus block, I have patients treat their MALS nonoperatively using the above protocol for 2-4 weeks, typically while they undergo further workup to rule out more common gastrointestinal etiologies of their abdominal pain, and many have been able to improve their circumstances with these measures alone. This patient chose not to have operation as she was able to live symptom free and regain lost weight with these recommendations alone.
Addendum
I received a comment from Ms. Suzanne Peek, president of the National MALS Foundation, who correctly pointed out not everyone presents in this way. I agree each patient undergoes a unique journey that is often marked by diagnostic delays because this is a rare condition. As I stated, not every patient responds to this regimen and after work up typically will undergo surgery to which in our published results 85% have a positive response to when diagnosed with MALS. Is certainly an area of further study to see if more people can respond to this non-operative approach. Our previous protocol which we instituted after the publication of our report was to use celiac plexus blockade as a diagnostic study and occasionally permanent blockade as therapy for those with prohibitive operative risk. A positive response to this regimen may signal a positive response to surgical celiac plexus ablation.
Reference
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
Every once in a while, I will make an exception to the SVS guidelines on AAA repair with regard to size at time of repair (link). I have a bunch of excuses. When I trained in 2000-2002 with several giants of vascular surgery, there was some controversy when the first guidelines came out in 2003 (link). The board answer became 5.5cm that year, but where I trained, it was a minority opinion held by Dr. Jeb Hallett. The majority was in the belief that as long as operative mortality was low, even high risk AAA repair could be undertaken (link). The published risk for Mayo was low, and that came from both technical excellence and high volume (more on that later). The criteria during my fellowship was 4.5cm in good risk patients for open repair based on data generated in the 1980’s and 90’s during Dr. Hollier’s tenure.
Then as now, the debate centered around the balance of risk. At specialty centers that achieved less than 1% mortality rate for elective open AAA repair, 4.5cm in good risk patients would seem perfectly reasonable. But given the 5-10% mortality seen in the Medicare database at that time for community practice, the 5.5 cm criteria was not only good science, it was prudent. The first set of guidelines held off the contentious volume recommendations that was the nidus of conflict within other surgical societies.
The advent of endovascular was a game changer -the mortality rate in the Medicare databases was 1-2% for EVAR in the community setting, meaning more surgeons in most hospitals could achieve tertiary center levels of mortality with this new technology. The issue was never really settled in my mind through the 2000’s, even with the PIVOTAL Study. I enrolled patients into the PIVOTAL Study (link) at that 4.5cm threshold during my time in Iowa. Eventually I lost equipoise and I stopped enrolling after a handful of patients. It had to do with graft durability.
Around that time, I took two patients in a row to the operating room for sac expansion without identifiable endoleak. They were Dacron and stent-based endografts placed about 5-7 years before by another surgeon and aortography failed to show type I or III endoleak. Sac growth was over a centimeter in 6 months and the aneurysm size was over 6cm in both. I chose to marsupialize the sac and oversew any leaks, with the plan to replace the graft if there was a significant leak. On opening the sac, no significant lumbar or IMA leaks were encountered but in these patients a stream of blood could be seen coming from the sutures securing the stents. It was the same graft that was in the trial, the AneuRx, and that was when I realized that these grafts have the potential to fail in the same way that patio umbrellas leak after years of use -cloth sewn to rigid metal with movement wears open the cloth wherever there is stitching. This did not happen with open repair. I lost enthusiasm for the trial as I lost faith in this graft which was retired from the market. I placed pledgetted sutures to close the leaks on both patients, and closed the aneurysm sac tightly around the graft in one patient who was higher risk, and replaced the stent graft in the other.
There are some exceptions to justify repair of 4.5-5.5cm AAA. During my time in practice, there were patients who lived far away from major medical centers who would not survive a ruptured AAA even if the rupture rate was low and who confessed they only came into town every five years or so. There were patients who suffered from clinical anxiety whose AAA was documented by a psychiatrist to amplify their anxiety. There were patients with vague abdominal pain for whom thorough workup have ruled out gastrointestinal causes and every visit to the ER triggered a CT scan to rule out AAA rupture. And there seemed to be some patients who seemed to have such perfect anatomy for EVAR, whose risks were low, and whose growth rates were so consistent that their repairs could be timed on the calendar. Some combination of these factors and lobbying on the part of the patient got them their repair in the 5cm range. And they still do.
The patient is a man in his sixties with hypertension who presented with a 4.7cm AAA which in various reports he came with described 5.2×4.7cm. After review of his images, it was clear it was 4.7cm. If measured on a typical axial cut CT scan or a horizontally oriented ultrasound probe, a cylindrical aortic aneurysm will be seen as an ellipse in cross section. A radiology report will typically report an aneurysms length and the anteroposterior and lateral dimensions. If you cut a sausage at an angle, the ovals you cut can be quite wide but the smaller length of the oval reflects the diameter of the sausage.
Looking back at his records, for three years he had multiple CT scans for abdominal pain showing the AAA and a well documented record of growth of about 2-3mm annually -the normal growth rate. He asked me to prognosticate and so I relayed that 4.7cm in 2017 with a 3mm growth rate, we would be operating in 2020. The anatomy was favorable with a long infrarenal neck and good iliac arteries for distal seal and access. He was quite anxious as whenever he had abdominal pain, his local doctors would discuss the AAA and its risks or order a CT. After a long discussion and considerable lobbying by the patient and family, I agreed to repair his 4.7cm AAA.
The EVAR was performed percutaneously. No endoleak was detected by completion arteriography (figure). He was soon discharged and was grateful. In followup, CT scan showed excellent coverage of the proximal and distal zones and absence of type III endoleaks. There was increased density to suggest a type II leak, but his inferior mesenteric artery was not the source of it. over a three year period, his aneurysm sac continued its 2-3mm of annual growth despite the presence of the the stent graft.
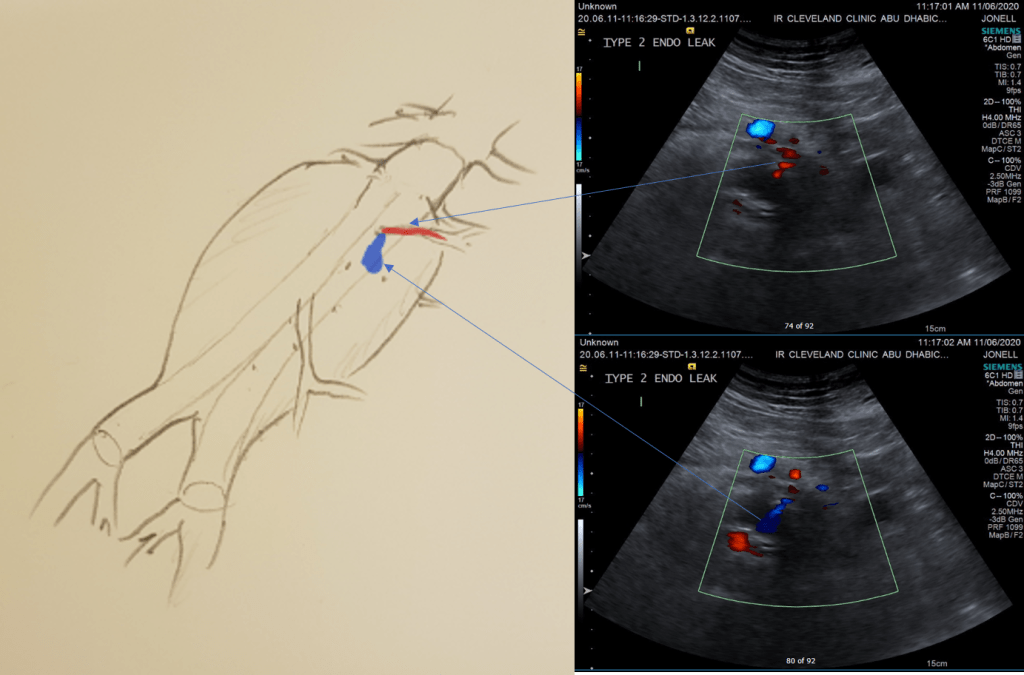
While CT failed to locate this endoleak, abdominal duplex ultrasound did showing flow from a small surface vessel (duplex below, figure at beginning of post). It was not the inferior mesenteric artery which can be treated endovascularly (link) or laparoscopically (link). CT scan suggested that it was one of those anterior branch vessels that one would encounter in exposing the aorta. Usually these were higher up as accessory phrenic arteries, but these fragile vessels, larger than vasovasorum, but smaller than named aortic branches, are seen feeding the tissues of the retroperitoneum.
Ultrasound revealed the type II endoleak from an anterior retroperitoneal branch artery.
Type II endoleaks are not benign. The flow of blood into the aneurysm sac after stent graft repair is almost never benign. It is a contained hemorrhage. There are three components to the pressure signal seen by the aortic aneurysmal wall that could trigger breakdown, remodeling, and aneurysm growth. They include pressure, heart rate, and the rate of change of pressure. The presence of fresh thrombus may play an inflammatory role. Some endoleaks clearly have a circuit and others are sacs at the terminus of their feeding vessels, never shutting down because the AAA sac can both accept and eject the blood flow. Changes in AAA sac morphology due to sac growth can cause problems with marginal seals, component separation, and component wear. Sac growth can cause pain. Ruptures, while rare, can cause death. Mostly, type II endoleaks generate more procedures because it is hard to ignore continued growth.
Review of aortogram from device implantation showed a small anterior artery arising from the proximal aortic sac (arrow)
Three years of followup showed growth of the AAA sac to 5.5cm, which ironically threshold for repair. Again, no type I or III endoleak could be seen. He reached his calculated repair date, and I discussed our options in detail.
1. Do nothing, keep following
2. Endovascular attempt
3. Open surgery, marsupialization
4. Laparoscopic ligation of target vessel
Doing nothing hasn’t worked for 3 years. What would more time buy? Endovascular -to where. The IMA is the usual target for an endovascular attempt, although iliolumbar access is possible (link), we really needed to fix this with one attempt. Open surgery is a great option -a short supraumbilical incision is all that would be needed to open the AAA sac and oversew the collaterals. The patient did not want a laparotomy. There are reports of laparoscopic guided endovascular access with endovascular coiling of the remnant sac with fluoroscopy. This adheres to the letter of the claim of minimal access, but really?
I compromised with the patient and offered laparoscopy. I have ligated the IMA a handful of times laparoscopically -these are relatively fast and straightforward cases. As I had the location of the endoleak, I felt it should be straighforward to dissect out the anterior sac much as in open repair and clip this vessel.
Use of ultrasound allowed localization of the leak and identification of the artery for clipping.
Of course, what should have been a 30 minute procedure through a minilaparotomy became a two hour enterprise getting through scar tissue (not the first time encountering this after EVAR) while pushing away retroperitoneum. I recruited the help of general surgery to get extra hands, but the patient was well aware that there was a good chance of conversion. Patience won out as the artery was ultimately clipped and endoleak no longer seen on ultrasound.
I waited a year before putting this together as I wanted CT followup. The sac stopped growing and has shrunk a bit back to 5cm or so. There will be those who argue that nothing needed to have been done about this leak as it would have stopped growing eventually, but I would counter that an aneurysm sac that kept growing like the stent graft never went in is one demanding attention. The key role of duplex ultrasound cannot be minimized. We have an excellent team of vascular scientists (their title in Europe), and postop duplex confirmed closure of the leak.
Not seeing the leak anymore is a positive, but the stent graft remains.
The patient is quite satisfied having avoided laparotomy. His hospital stay was but a few days. During my conversations with our general surgeons who are amazing laparoscopists, that this would have been a nice case with the robot. That’s a post for another day.
The definition of success in this case and many EVAR’s plagued by type II leaks leaves me wondering. Excellent marketing of the word “minimally invasive” has subtly defined laparotomy as failure, and not just in vascular surgery. When costs and efficacy are reviewed as we come out of this pandemic, I suspect that open surgery will selectively have its day in the sun. A ten blade, a retractor, a 3-0 silk is so much more cost effective than five ports and disposable instruments. And a stent graft system?