This podcast generated from this blog post “perfectly compulsive, perfectly smart” discusses the critical importance of not falling into the efficiency trap of algorithms and treatment pathways. Algorithmic thinking is the bane of modern medicine -ask patient where it hurts, touch the part that hurts and describe it, order labs and imaging studies, read the report and do what it says. That space between the algorithm and the truth is where AI will step in. The patient with a rare disease usually struggles within this system.
Every time someone on Seinfeld went to the hospital, a stock scene (above) would play. It’s the old ER of Roosevelt Hospital on 9th Ave before the renovations moved it to current 59th street entrance. I was a surgery resident there in the 90’s and watched each Seinfeld episode for the upper West Side stuff that would pop up. The soup Na2i was a few blocks over. Not seen on this pic is the Sym’s operating theater designed by Dr. Charles McBurney which is a designated landmark and currently a private school for “gifted but difficult” children (link). I used to round on patients in the red building -they would be ten in a room separated, if lucky, by rolling privacy screens. My sister was born here. John Lennon died here. All that gone, because hospital buildings are like dressings on a city’s wounds and need to be changed every generation. In fact, it’s not even called Roosevelt Hospital any more.
Roosevelt Hospital’s name was changed to Mount Sinai West, and its sister hospital, St. Luke’s, was changed to Mount Sinai Morningside. I would like to imagine that it was vengeance a century in the making, for pearl clutching slights originating from the gilded age, of blue bloods v. upstart Jews. Because no matter how far you are from the shtetl, there is always another golden door closed to you in New York City. So it seemed for me, an immigrant who had worked hard to get to Harvard College, and Columbia P&S, to look with squinted eyes at my letter on match day and see St. Luke’s/Roosevelt Hospital Center, my last choice that I listed out of a general interest to avoid not matching.
When I landed on St. Luke’s-Roosevelt for my general surgery training, the house officers were quartered in the older parts of the hospital, some rooms dating back to the 19th century, unchanged like unearthed chambers from Pompeii. Both hospitals still had the open wards for the “ward” patients with segregation of the private patients up in the towers. For a time, they still had seamstresses to mend your white coat and cafeterias that still cooked their foods fresh. The resident’s lounge at St. Luke’s was like a frat house common room from the thirties, with a scratched-up pool table, a broken piano, pedastaled hotel ashtrays, and card tables. An old handprinted sign (which I regret not taking) listed the house officer’s rules and entitlements which included two beers or a shot of whiskey per night on call.
After my intern year, both hospitals started sorely needed renovations. The surgery office had to be cleaned out, and behind an antique cabinet, wooden boxes of chromic cat-gut suture were found, still in their glass tubes and preserving fluids, little brown skeins of suture floating like preserved fetuses, a strange message from a faraway time. I ran into Walter Wichern, chairman emeritus, who showed up randomly to the hospital in blue blazer and bow tie. I had just stained my dress shirt pocket with my soon-to-be-lost Mont Blanc fountain pen, and he launched into a story about how he repaired a ruptured aortic aneurysm back in 60’s by cutting his new polyester dress shirt into a tube and sewing a graft out of it down in the laundry, after hearing a talk from Arthur Vorhees at P&S. And he was smiling an enigmatic little smile, recalling how that patient on being discharged gifted him annually with ten new dress shirts every year. I later found out that Dr. Wichern was famously taciturn, and I had somehow unlocked an achievement -getting a story out of an old surgeon. It was around then that I had started to feel that it wasn’t all a big mistake.
When I recently changed hospitals from the Cleveland Clinic to University Hospitals, I had to submit documents for privileging, and I get a testy email. “Where did you do your residency?” The administrator couldn’t find St. Luke’s/Roosevelt anywhere on the ACGME website, or even on Google. When I offered the new names, the reply came back, “They only have records going back to when they took over in 2008.” I briefly contemplated retiring, then asked if sending pictures of my framed degrees would be sufficient. Only partly, was the reply. She wanted witnesses.
My first night on call was terrifying. I was on call with Bobby Borromeo -my fellow intern, Anil Hingorani -our PGY4, and Jesse Jean-Claude -our Chief Resident. All of us are now practicing vascular surgeons -Bobby (fellowship Yale), Anil (fellowship Montefiore), Jesse (fellowship UCSF), and myself (fellowship Mayo), embarked on a night of call that involved no sleep and little food. The single moment I recall was taking Bobby through a blood draw and filling the forms for processing the labs and performing EKGs with an antique strip recorder, cutting and pasting the strips onto a formatted sheet for the chart. Bobby didn’t know how because there were many people to do these things in his home hospital in the Phillipines. For myself, I knew the two hospitals from my rotations during medical school. I could draw blood and cut, sew and tie above my level from my time as a senior student at P&S. I got a bit too comfortable with my privilege, and I was still thinking I should have been somewhere else. Over breakfast, I absentmindedly voiced this out loud and was corrected in a way that is no longer possible in 2022. It was the tone that I remember, of being chewed out.
One of chiefs snapped at me,”You have no idea how big and important these hospitals are. They are older than all the other hospitals here in NY. McBurney did the first appy here. Halsted was chief at Roosevelt and invented cancer surgery and the surgical residency. Green invented the LIMA bypass at St. Luke’s. Our chiefs go to better fellowships year over year than any other hospital in Manhattan. You should be grateful to be allowed to round with us.”
Tie given out at graduation, designed by Howard Nay, MD (link), RIP. One of the few keepsakes of my time there. Dr. Skip Nay, was old school, and gave everyone nicknames. Learning surgery from him was like taking blues guitar lessons from Mr. Robert Leroy Johnson.
It was by my third year I got used to the 120 hours a week. It is only now a quarter century later, that I value it. I was expending my. youth living and breathing surgery in the latter days of St. Luke’s and Roosevelt Hospitals. I was missing my friend’s weddings, missing time with my wife, seeing New York during the glory of the 90’s through the dank recesses of a trauma bay. I was six figures in debt, but I could take out your appendix in twenty minutes. I had just signed on for a year of research with the peerless Dr. David Tilson and was not looking forward to telling my wife who found the original five year deal of residency interminable. Add to that, two years of fellowship. Walking out on the deck of the call room overlooking the Cathedral of St. John the Divine and Columbia’s campus, listening for the sirens, I really felt the spirit of the hospital.
It’s not the name of the place, neither its splendor nor its comforts, but the commitment of the people in the teams that you build, which allows you to do great things. And yet…
Summer 2022, in front of Mt. Sinai West, formerly and forever Roosevelt Hospital.
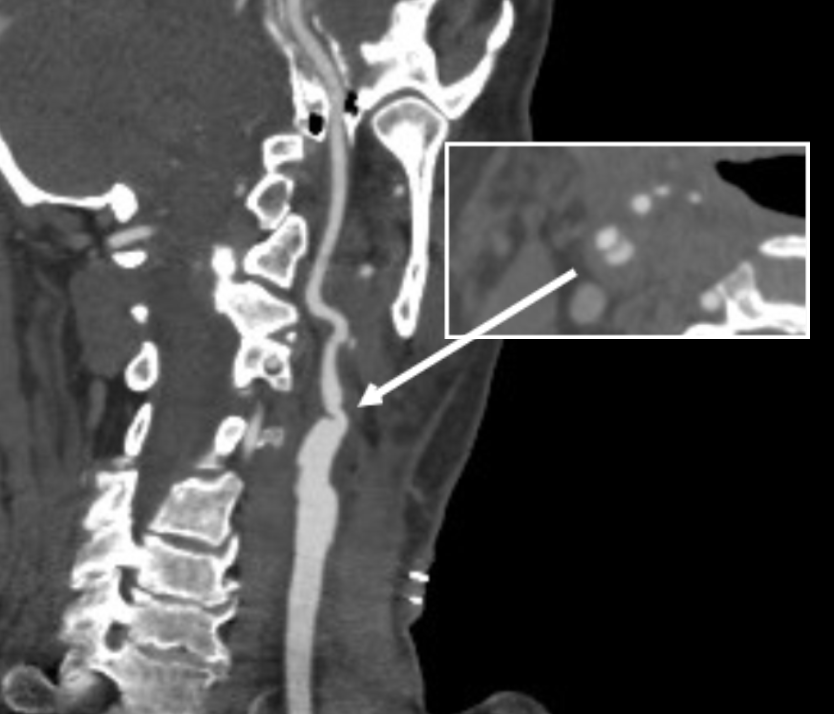
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
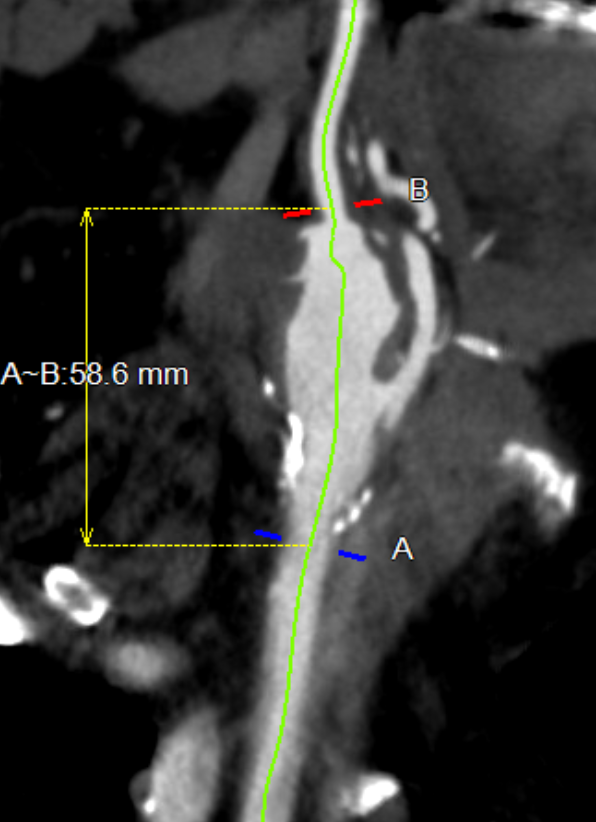
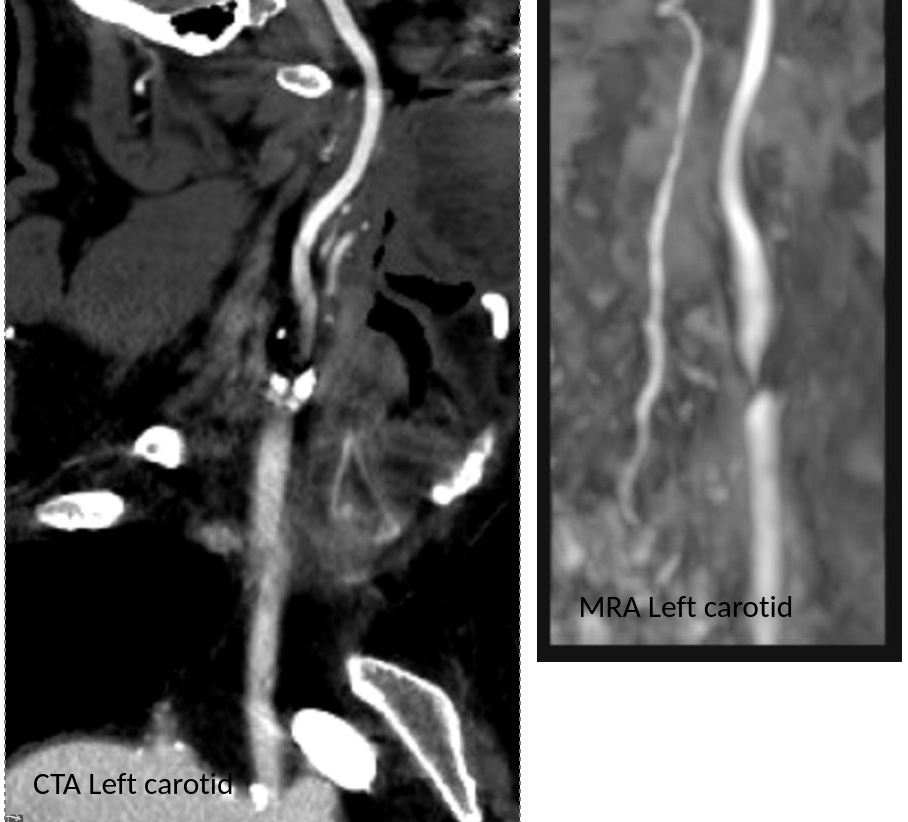
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
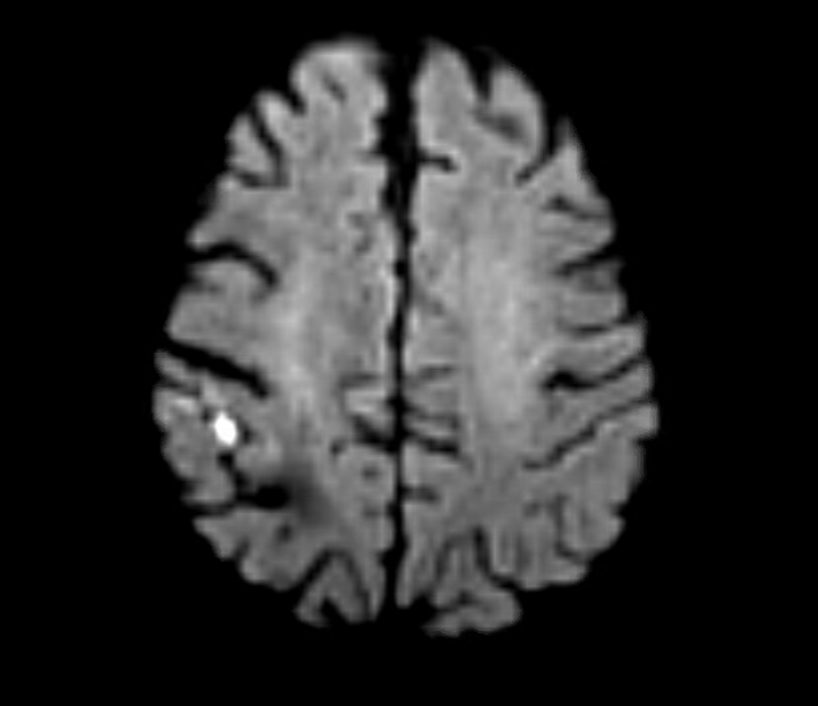
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
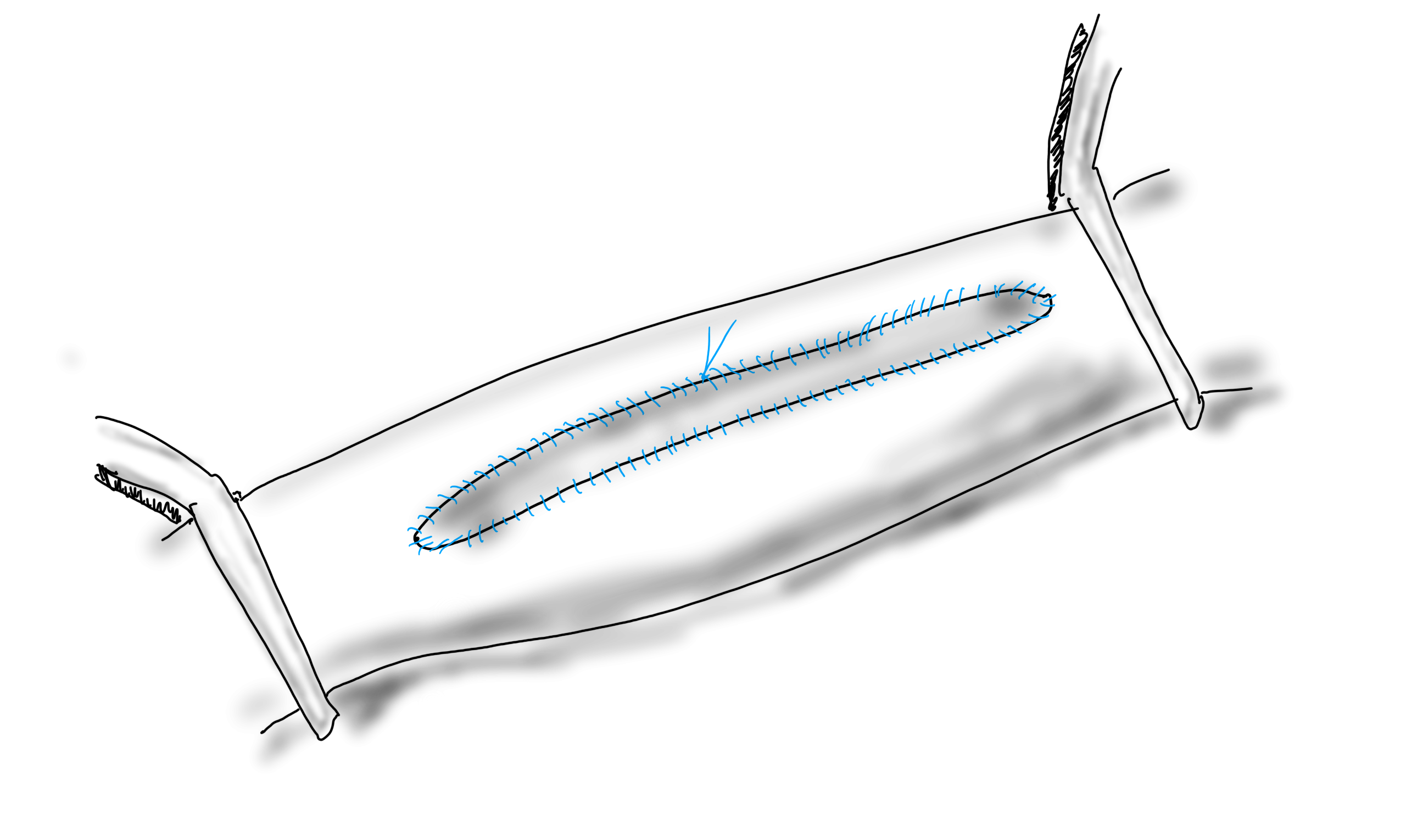
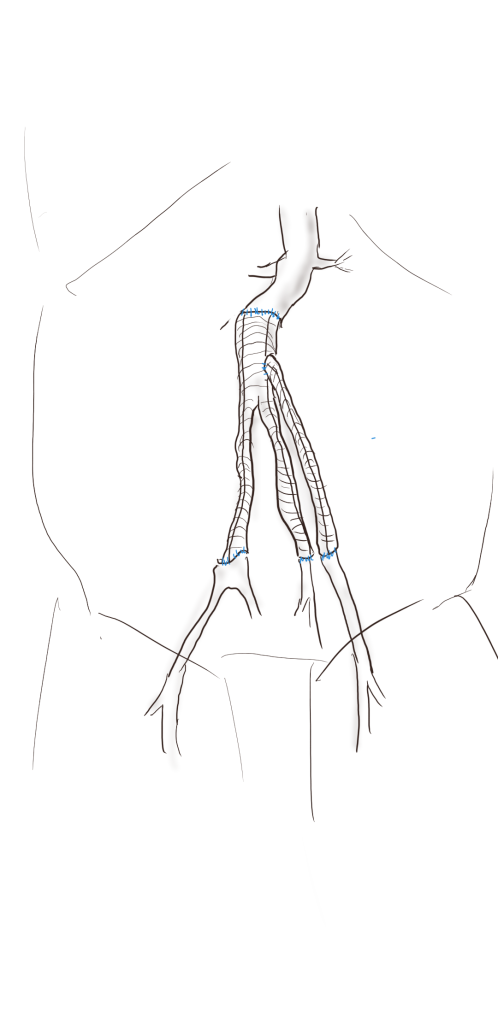
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
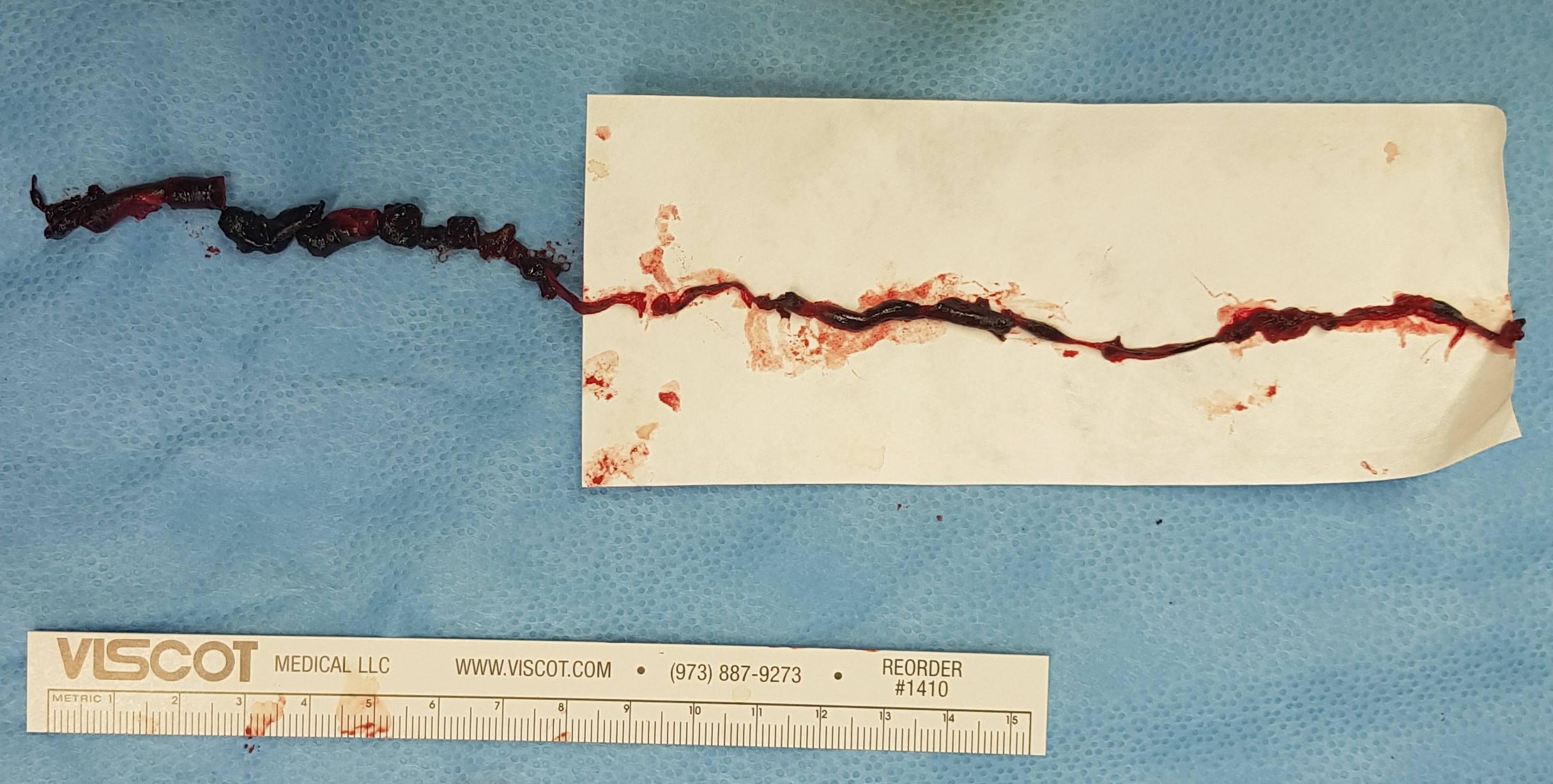
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
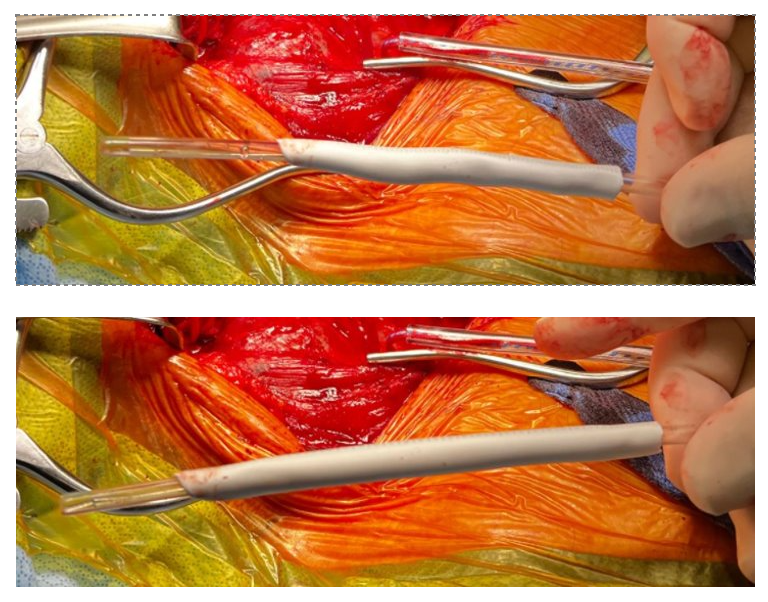
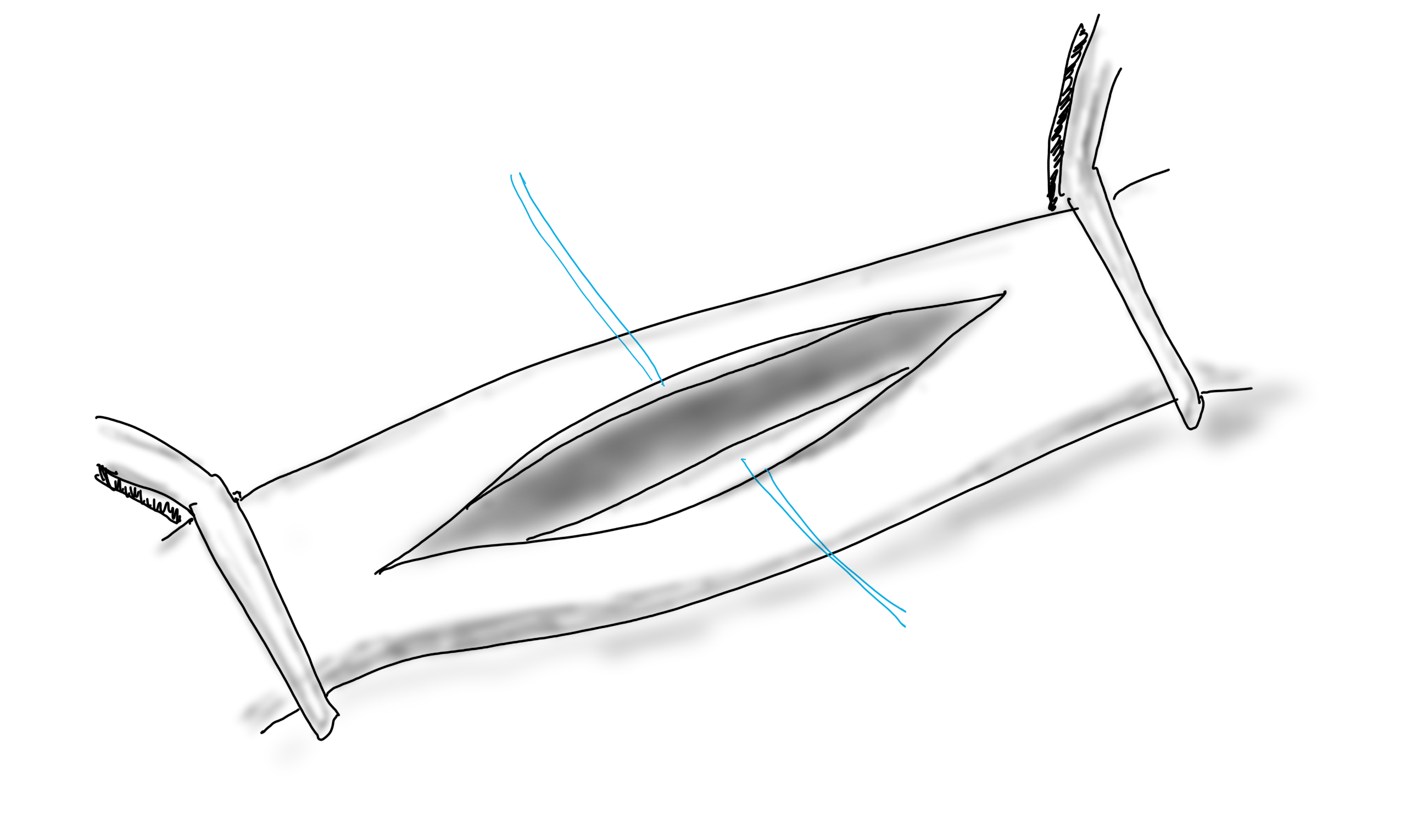
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
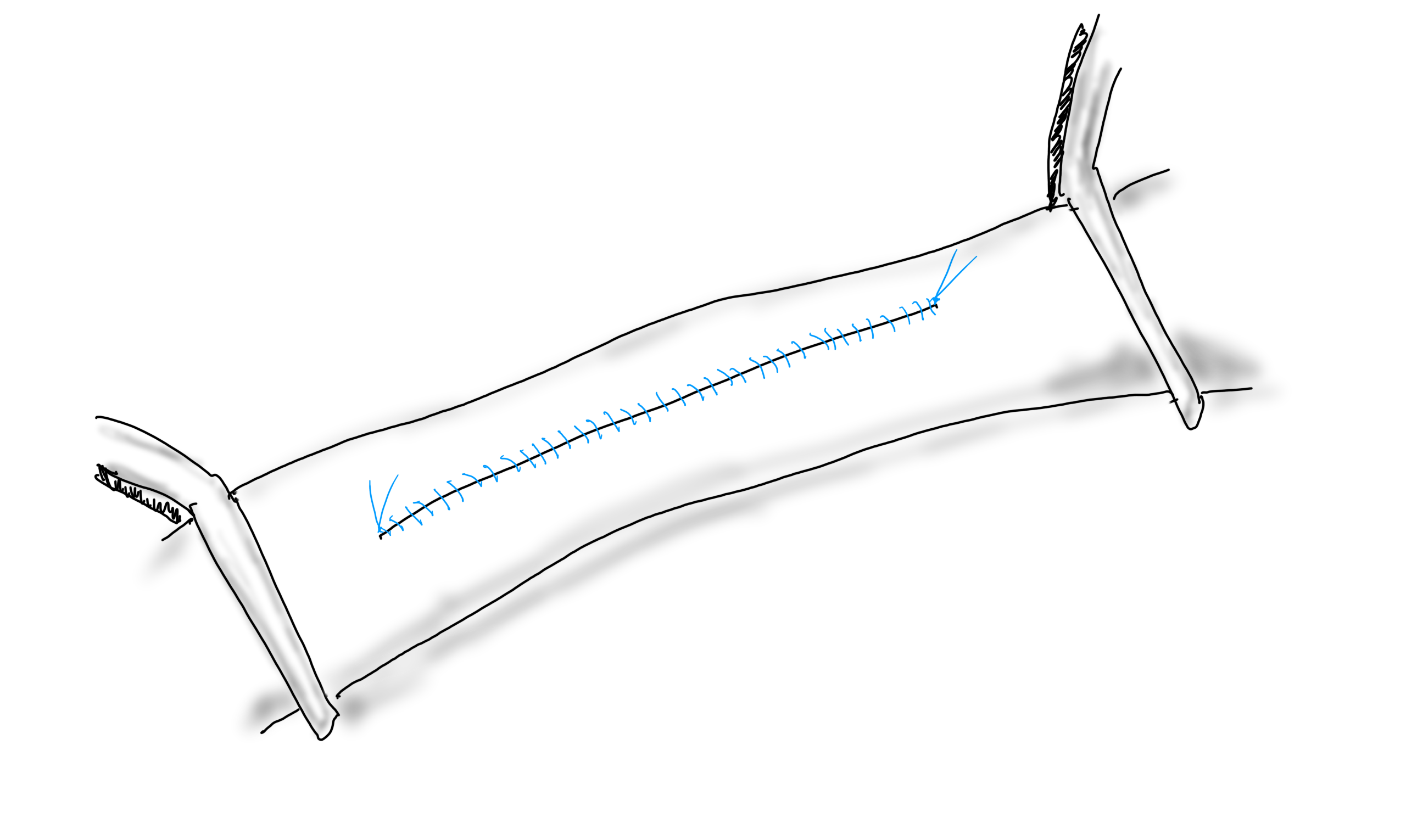
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
About ten years ago, I had a patient who came to see me for moderate carotid disease. While his carotid disease was asymptomatic, he also had metastatic colon cancer. With colectomy, cryoablation of liver mets, and chemotherapy, he was in remission. Every 6 to twelve months he had some kind of CT scan with contrast. His renal function was poor and this was blamed on his chemotherapy. While it had nothing to do with this patient, I thought to myself, “Having an aortic stent graft was a lot like having metastatic cancer in remission.” After a stent graft, the patient is forever tied to the health care system. Without surveillance, there may be an endoleak, sac expansion, rupture, and even death. Patients and vascular surgeons can make choices that lengthen life, improve its quality, and avoid the complications of disease. But what if a treatment becomes a condition and a burden on healthcare resources and the patient’s finances?
Fool me once…
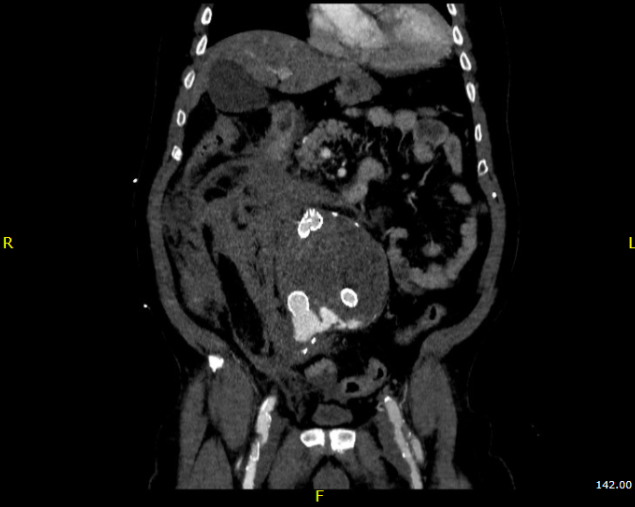
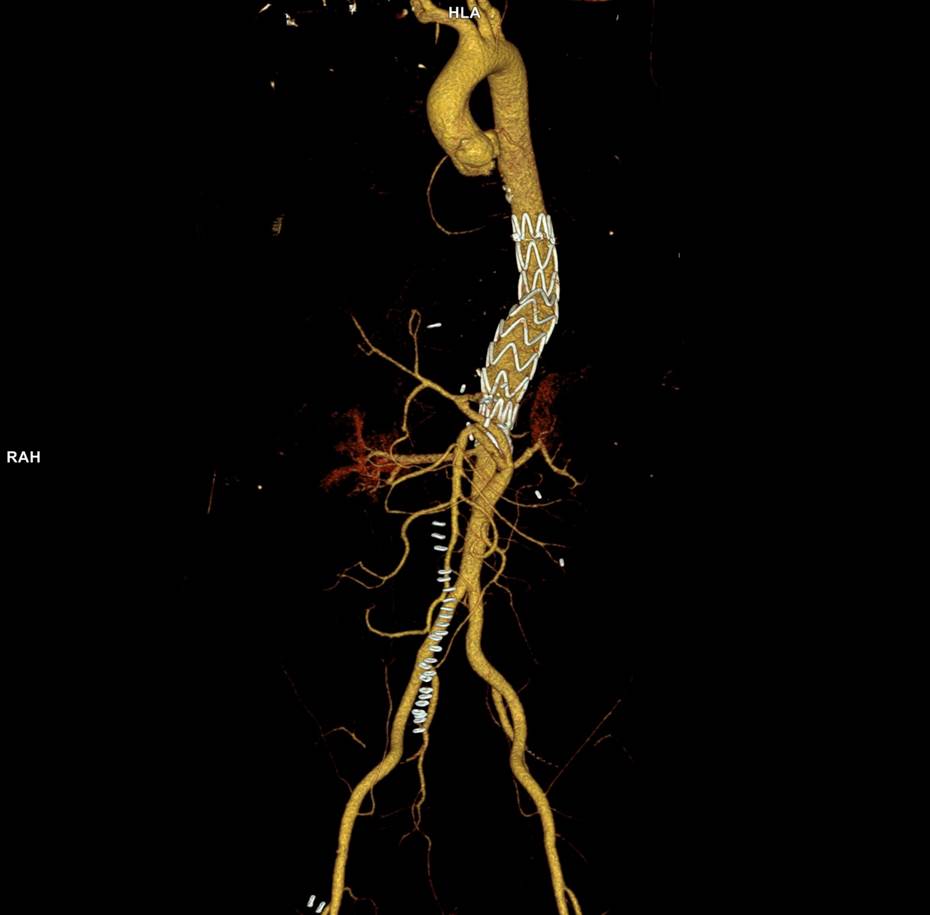
Type Ib Endoleak Causing re-Rupture of a previous r-AAA after no surveillance
Take this patient who had previously ruptured his AAA and undergone EVAR. Several years out from his rupture, he ruptured again from a type Ib endoleak due to aneurysmal degeneration of his right common iliac artery. Per his family, he never followed up. Perhaps he assumed he was cured of his disease? Repairing this was tricky, primarily because I hopped up and down, thinking, “I could cure this!” An open revision with a bifurcated graft would eliminate the need for EVAR surveillance, avoid abdominal compartment syndrome, and the physiologic consequences of a large retroperitoneal hematoma. But who wants a laparotomy? Not this patient, who was hypovolemic shock, and whose family chose the minimally invasive option that everyone assumes is better.
Not a clamp
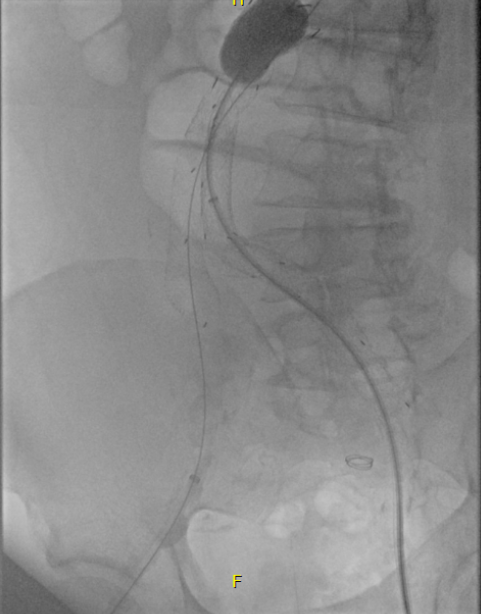
I took him to the hybrid operating room, balloon occluding to stabilize his blood pressure, embolizing the normal internal iliac artery and extending the stent graft into the external iliac artery.
Completion -there is an Amplatzer plug in the right internal iliac artery
This patient stabilized and had abdominal tightness due to his large hematoma which did not need evacuation. After a stay lengthened by concern for abdominal compartment syndrome, moderate pain, fevers, and bilirubinemia (due to the hematoma), he was discharged and never showed up for followup. None of the phone numbers work. Without followup, EVAR is a menace. We will keep trying.
Regrets, I’ve Had a Few…
The great feature of EVAR is that the complications up-front at the time of surgery are wonderfully low. This patient pictured above here presented in middle age with a rupture into the retroperitoneum. He was unconscious and had hemorrhagic shock.
The decision to perform EVAR was made late in the transfer because I did not have the images from the transferring hospital (another subject for another blog post) so I set up for both open repair and EVAR. En route to the OR, I scanned, slowly, through the CT images sent via CD-ROM, and my internal discussion went something like this.
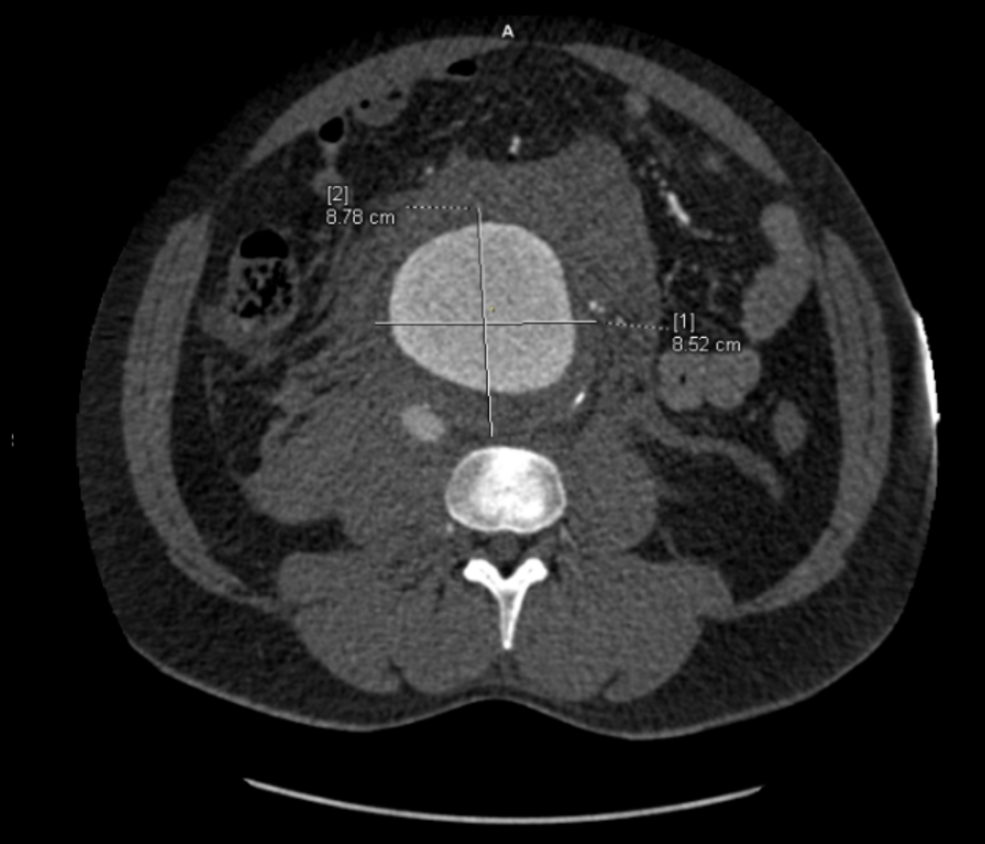
“He’s a 50-something smoker in shock with a contained rupture of a 8cm infrarenal AAA with a good neck. Let’s take care of this in 30 minutes with a percutaneous endovascular aneurysm repair (p-EVAR).”
“He’s a 50-something smoker in shock with a contained rupture with a good neck -let’s take care of this in 90 minutes with a tube graft, open aortic repair (OAR).”
“With p-EVAR, he’s going to have just two groin punctures and much lower complication rate, shorter length of stay, similar to lower mortality. Look -his blood pressure is 75mmHg systolic!“
“That hypotension is permissive to minimize bleeding. With OAR, he’ll avoid abdominal hypertension and complications of a giant hematoma. Because he’s young, he’ll avoid lifelong surveillance. If anyone can clamp this AAA, it’s me...”
“Pride cometh before the fall. Get this man off the table and figure out the logistics later. p-EVAR. You open him up, he’ll exsanguinate and expire before you get the clamp on.“
I sighed, looked up at the gathered team, and announced, “p-EVAR.” The percutaneous EVAR is something I’ve been doing since 2004, long before it was a big deal, and we were done under an hour. His blood pressure stabilized, but general surgery was consulted for his abdominal compartment syndrome. With sedation, fluids and time, his urine out put recovered but his belly remained distended and his bladder pressures which were never seriously elevated, trended down.
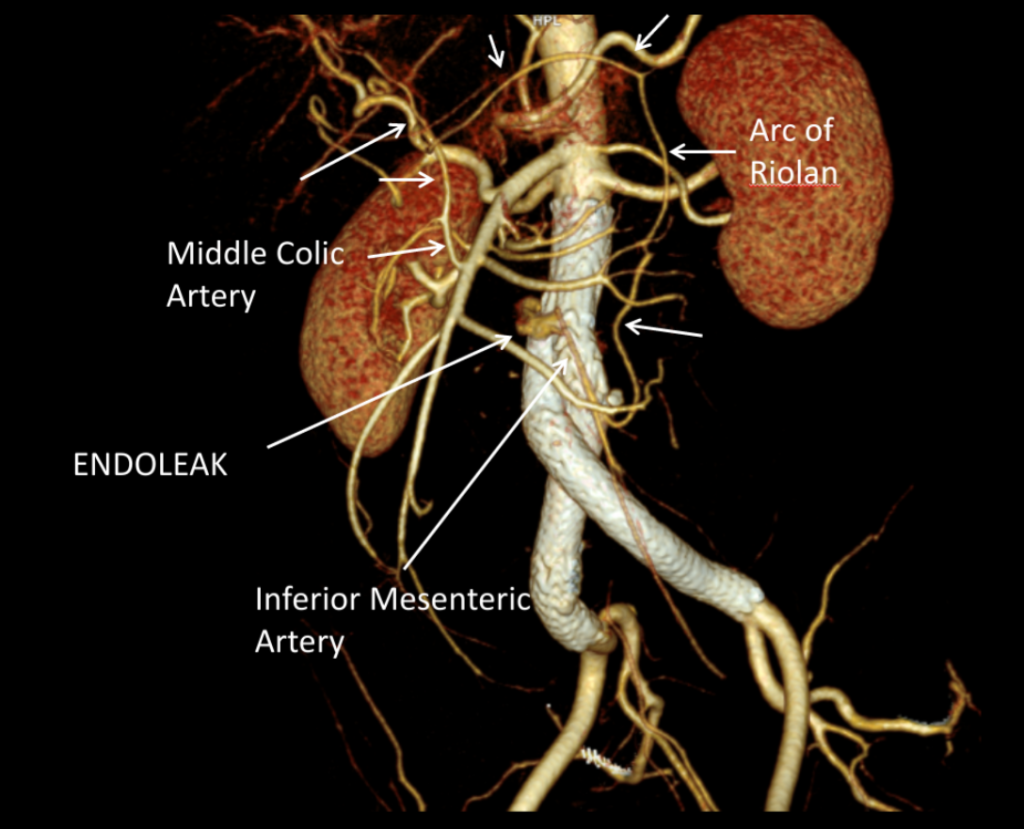
It was made known to me that the patient had very limited insurance making followup surveillance challenging. Due to his coverage, he had to have his imaging done at designated hospitals, so I wrote a detailed note -basically the timings of his followup CT scan, and asked that the reports should be sent to me. I ordered a CTA prior to discharge which showed a type II endoleak adjacent to the graft and connected to both lumbar and inferior mesenteric arteries (first image above). After some thinking, I took the patient for an aortogram, accessed the IMA via the SMA and coiled into his AAA sac and the IMA.
It was only a few weeks ago one of my colleagues across town contacted me that the patient had been admitted with abdominal pain, a CT showing a type II endoleak from his lumbars, but a smaller AAA sac than his pre-repair size of 8.5cm. The patient is seeking to repatriate, and I doubt he would be able to get adequate followup in his home country without paying in cash. Happy that the patient survived his rupture, I still have persistent regrets at not getting him through an open repair, which I am sure he would have done fine with… Or maybe not.
Je Ne Regret Rien…
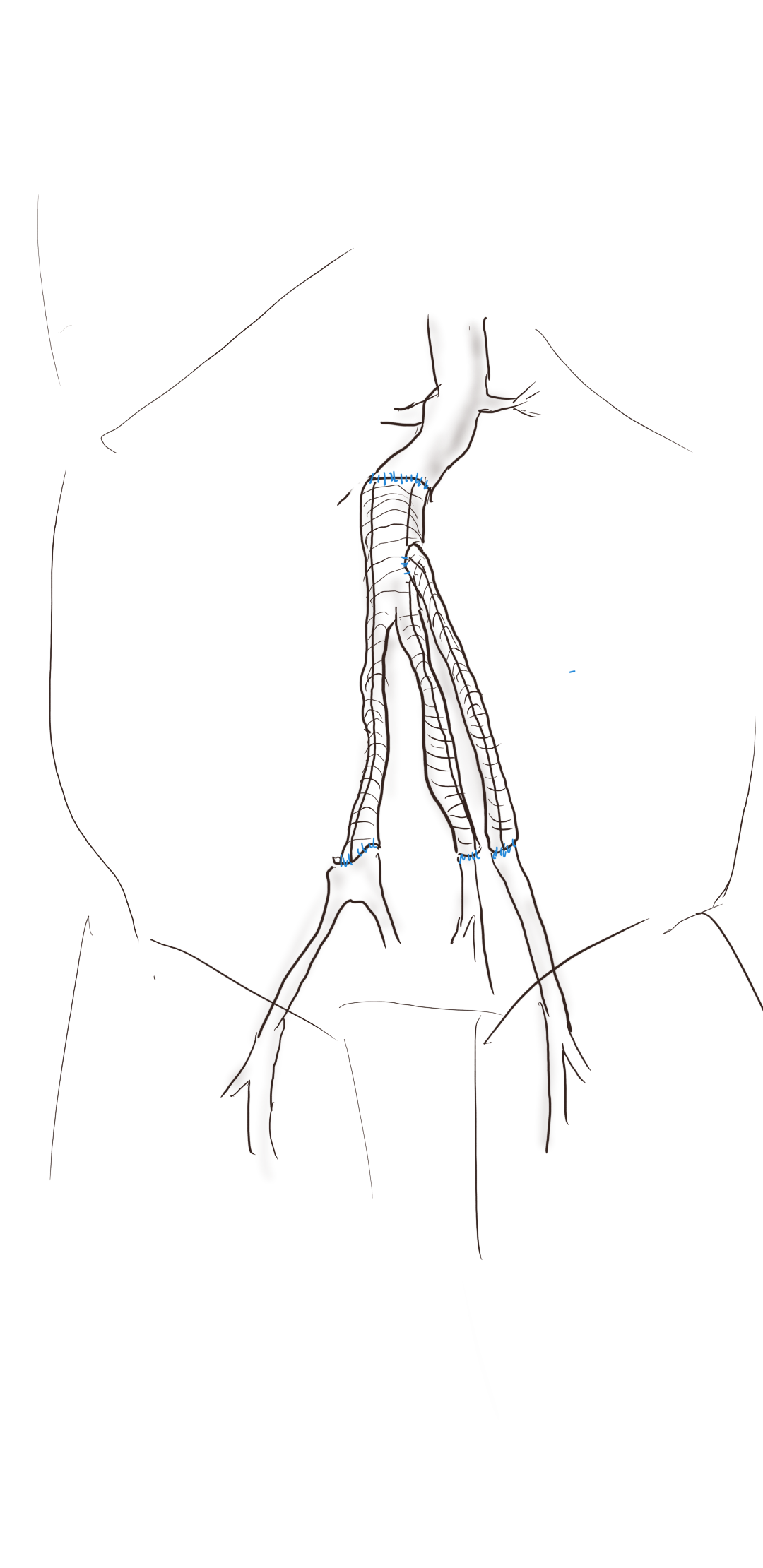
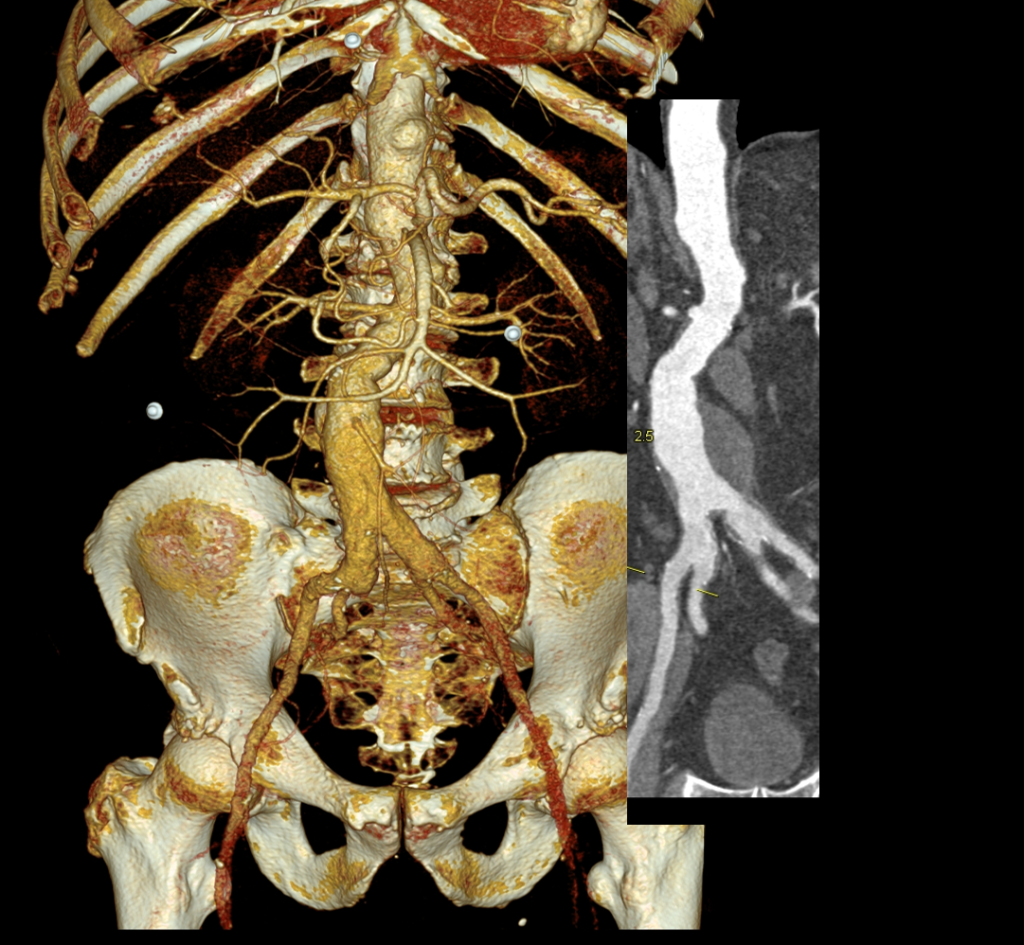
Recently I admitted a patient, in his 70’s, with a symptomatic 6.5cm infrarenal AAA with bilateral common iliac artery aneurysms, the right being 25mm, the left over 30mm. Because of the pandemic, he was stuck here, seeking to repatriate. Over ten years before, he had a segment of descending thoracic aorta repaired for a traumatic tear -probably one of the last before the wide adoption of thoracic stent grafts which work great by the way.
Cardiac risk evaluation revealed an ejection fraction of 35% with reversible ischemia on nuclear stress test. CTA of the coronaries revealed triple vessel coronary artery disease corroborated by catheterization. Off-pump CABG was planned which would eliminate the effects of cardiopulmonary bypass.
Preparations were made for EVAR with IBE of the left iliac aneurysm as a contingency, but there was no question that if the patient recovered well from his CABG, he would undergo open repair. This was because bell-bottoming or IBE must have regular coordinated surveillance which was not going to be easy with the patient leaving for another country in the middle of a pandemic. It is difficult to get followup to happen in normal circumstances (see above cases). I expressed my opinion to the patient and family and we agreed to see how the patient responded to off-pump CABG.
He underwent off-pump CABG with three vessels revascularized. He was extubated POD#1 and mobilized. By POD #4, he was on a regular patient floor, being co-managed by hospital medicine who takes care of all of our patients. The patient expressed readiness for the next operation. His kidney function remained normal. He was transfused 2 units of PRBC to bring his hematocrit to 30%. He was taken off Plavix, but kept on aspirin. On POD#6, he was taken back to the operating room for open aortic bypass. This would not have been possible without close coordination of cardiology, cardiac surgery, and vascular surgery. Choosing off-pump CABG was a critical element in being able to proceed with open aortic surgery.
Right branch taken to iliac bifurcation, separate bypasses sent to left internal and external iliac bypasses.
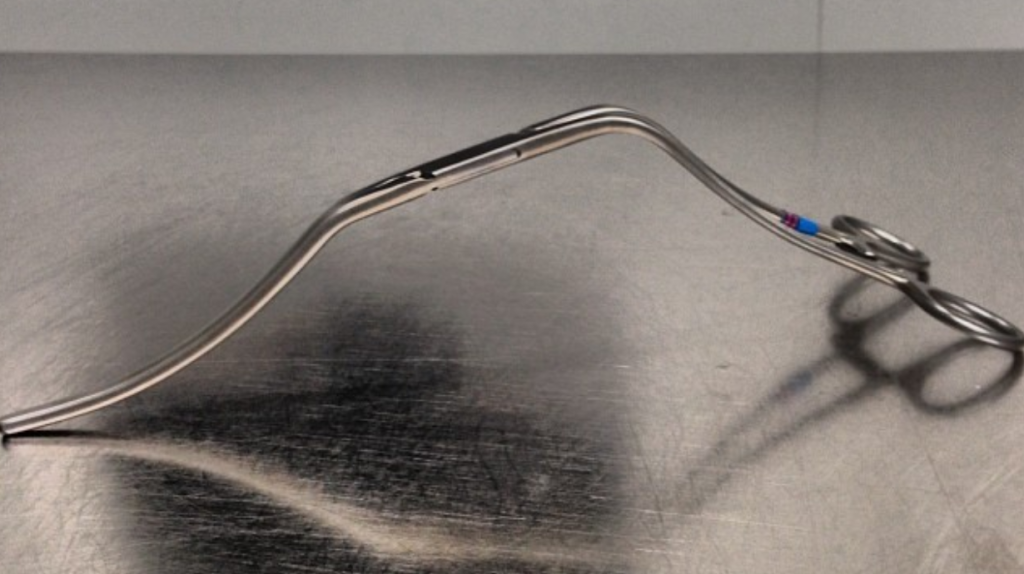
I do several things to decrease the physiologic impact of the operation. First is keeping all the viscera retracted under the skin. This simple move has the effect of decreasing the rate of intestinal paralysis and amount of fluid shifts that occur postop, akin to going retroperitoneal. This decreases the space you potentially have if you use standard clamps, but I use the Cherry Supraceliac clamp (image), DeBakey Sidewinder (transverse), or just a Satinsky clamp oriented transversely. This minimizes the occupation of volume over the anastomosis which always happens with standard aortic cross clamps. The anastomosis is easier without the clamp taking up valuable space.
Cherry Supraceliac Aortic Clamp
The iliacs are always clamped with Wylie Hypogastric clamps, again, with the principle of eliminating clamp overhang. Suturing is done with 4-0 Prolene on SH needles -this is plenty (link). The proximal anastomosis wants to bleed, and sewing to a fully cut ring of aorta ensures good posterior bites but also allows for sliding a band of graft down over the anastomosis (Dan Clair calls this a gusset) which works well at creating a hemostatic proximal anastomosis rapidly-trust me, getting this done well is the key step of the operation. Before closing, I infiltrate the rectus sheath and preperitoneum bilaterally with local anesthesia -lidocaine 1% with epinephrine 1:1 with bupivicaine 0.5%. The skin is closed with absorbable dermal sutures because staples create as many problems as they solve. The patient had cell salvage through the case and no extra units of transfused blood.
The patient was extubated that night and started on clear liquid diet. The next day his lines were removed and he was moved to the floor and started on regular diet when he expressed hunger. On POD#2, he was pacing floor, asking when he could be discharged.
Sternotomy and Laparotomy POD#2, walking the floor
As he was eating, walking, talking, breathing, evacuating bowel and urine, and pain free (well controlled), I saw no reason to keep him beyond POD #3 AAA/#9 CABG. I have kept in touch with him and his family and he is doing well and has given permission for this posting.
Satisfaction
This final case has confirmed several of my beliefs. First, calling something high risk can drive one to make bad choices and in fact endanger patients. This last patient would qualify as high risk on any international criteria, and you would not be wrong in quoting upwards of 30% major morbidity and mortality for cardiac revascularization and AAA repair, but you would also be tying your hands from offering the best solution for this man who fortunately was able to undergo two prodigious operations. He will not require much in the way of followup. Coronary revascularization with arterial conduit and open aortic grafting frees him from the need for close followup and reassures us that his repair is durable.
Second, calling something advanced and minimally invasive gives one cachet in the marketplace but forgoes careful discussion and consideration of what is being abandoned. The first two patients survived their ruptures but now face the consequences of having stent grafts. It is a shame when podium speakers at international symposia declare surgery to represent failure because this affects training by encouraging abandonment of hard to acquire skills. It seeps into patient perceptions and expectations. I hope that a balanced approach prevails. You have to be capable of both open and endovascular approaches to be able to offer the best treatment for a particular patient.
Finally, these old operations are cost efficient and there is a lot of room to improve these procedures with new perspectives, techniques, and data. I don’t operate the same way I trained, and it is only through continued application of operations that improvements can come about. As budgets tighten and economies are stressed, cost efficacy will rein in much of the interest and demand in new stuff unless it adds value. That said, I am grateful to our stent graft representatives who have worked to get us bell bottoms and IBE’s for when they will be needed. These grafts will be used when the time is right.
The process of clotting is something vascular surgeons take for granted, but patients may have a hard time understanding what a clot is because in most people’s experience, it is rare for someone to see enough blood to form clot. How many patients or even health care providers have seen a tube or a basin of blood clot? So how do we describe clot to patients? I think the solution lies in food.
Most people who know me will say that I propose food as the answer for most things but hear me out. In describing clot, food is particularly salient. Clot is protein made insoluble, and there are many foods that have similar properties. Tofu, jello, and cheese and their making can give context where the word “clot” cannot.
All are made by taking a solution of protein and allowing them to form clumps that cause them to fall out of solution. It may require an acid, as in the case of tofu and cheese, but mere time and cooling may be sufficient as in the case of jello. And like these, clot may take on a soft crumbly quality when it is fresh clot, to a tenacious formed clump when given enough time. The difference is like silken or soft tofu and firm tofu. Or fresh ricotta cheese before it has time to set in its mold and the firmer cheese you get after weeks of curing.
With enough time, you get a hard substance that you can slice with a knife, like a dry cheddar or Parmesan. That is how I think of clot. It can be soft and formless like early jello before it is ready to eat. Or it can be hard and formed like mature dry cheese. The softer it is, the easier it is to dissolve or suck out via gadget or catheter, but there is a time factor to this softness -thing of your jello setting and hardening in your fridge. The harder the thrombus is, the less likely it is you can remove it with catheters and more likely you will have success with an operation as in the first picture. The harder stuff in fact crumbles well like a parmesan cheese and is harder to remove.
Burrata, handmade in Calabria is similar to the kind of semi-mature clot that deforms well but is tenacious and difficult to break up and remove except in one piece.
There are several things to draw from this with regard to devices designed to retrieve clot. Clot can occlude catheters as much as they can occlude arteries. Clot retrieval depends on net output of fresh clot that deforms well and flows well but fails in the hardened brittle clot that is well organized and adherent. Retrieving these crusty dried clot matter may be impossible for a device that depends on clot deformability or a maximum particle size, and these clots are the ones that are more partial to crumbling and embolizing. All devices must accept the fact that the unclogging is done in a flowing circulatory system where items swept downstream have the consequence of killing tissues whose arteries are blocked by emboli. There is always embolism with minimally invasive approaches. These devices make sense for hard to access circuits like the brain, but make far less sense in circuits like the extremities where surgical control is relatively low risk and results in reversal of blood flow -like in TCAR. Each of these devices can cost several thousand dollars. The fact is, operations can be faster and safer because embolism can be controlled and a wider range of clots, and larger amounts of it, can be removed at a lower cost. The first picture shows the results of a popliteal cut down and tibial thrombectomy where inflow was first restored in the below knee popliteal artery, and clot retrieved from each of the three tibial vessels (misleadingly, the tibial thrombus is all lined up), and a simultaneous 4 compartment fasciotomy performed, all under 90 minutes with no use of contrast. Unfortunately, open thrombectomy is a bit of a lost art in that many of the maneuvers and steps required to revascularize a limb successfully with no preoperative imaging requires experience. A younger patient with an arrthymia related embolism and normal soft arteries is approached far differently from an older person with atherosclerosis and diabetes, where open thrombectomy is better suited for the first, and catheter based approaches better for the latter.
Diagnostic and Therapeutic
The open surgical exploration of the extremity arteries is fast becoming a lost art along with the physical examination. In the setting of acute limb ischemia, the first decision in my mind is: was this an embolism? The presence of arrrhythmias, cardiac shunts, and aneurysms may suggest this, the next question is did this patient have a prodrome of limb ischemia related symptoms and history of atherosclerosis. The fact is, you have about 4-6 hours to return blood flow before irreversible neuromuscular damage sets in, maybe less if important collaterals are lost. Choice of procedure then devolves to choices about the most expedient methods for returning blood flow to the extremity, and between endovascular procedures and open surgery, it is rarely possible to manage significant clot burden with endovascular methods without adding the burden of procedural time. These considerations are balanced by patient risk. If the patient cannot tolerate general anesthesia, it is still possible to operate under local anesthesia. Otherwise, one is faced with choices like stenting across clot or common femoral artery. The algorithm is simple -ensure inflow, thrombectomize outflow, check for backbleeding, restore flow, check flow, repeat as necessary downstream. Fasciotomy as needed and close the skin if you can.
Endovascular options deal with the basic physics of trying to pull clot of varying consistency through a small lumen over a long length while not pushing emboli. The needs are simple -a low profile, cheap, over the wire solution for evacuating clot without embolizing nor injuring the patient on a 100cm and 150cm length catheter. Cost wise, open surgery always beats any endovascular option if wound complications of open surgical exposure are avoided. Both methods can’t cover themselves if open fasciotomy wounds keep the patient in the hospital for weeks. The fact is, we already have this magic system in the catheters that we already have on the wall, albeit, they don’t work particularly well if you are dealing with Parmesan, but none of the systems do. I recently declotted a graft fistula with just 6F sheaths, a regular #3 Fogarty ballon, 6mg of tissue plasminogen activator, and was able to salvage the blood and return to the patient.
Conclusion
Vascular surgeons should have as many words for clot as Eskimos purportedly do for snow. There is no one solution to a problem, but all the tools must be available to the vascular surgeon. Ironically, only the simplest are needed most of the time.
My partner, Lee Kirksey, Vice-Chair of Vascular Surgery, just got a paper on-line (link) about the curiously increasing volume of open surgical repairs we were experiencing from 2010-2014 at the Cleveland campus of the Cleveland Clinic. When I joined in 2012, my impressions at that time were mostly the paucity of straightforward EVAR cases that I had seen in private practice, and the high prevalence of stent graft explantation, infected aortic grafts, and open aortic aneurysm repairs (OAR) for juxtarenal and thoracoabdominal aortic aneurysms for nominally high risk patients. My TAAA muscles had atrophied during my years out of fellowship and I eagerly took the opportunity to recruit the help of my partners and scrub in on these cases with Pat O’Hara, Jean Kang, Dan Clair, Ezequiel Parodi, and Lee Kirksey. It is without any shame that I sought out not just extra expert hands, but interrogated these experts for different ideas and approaches, and absorbed feedback. At the time, I was ten years removed from graduation, a full-fledged vascular surgeon who thought he could do any operation put before him. I cannot imagine the thoughts churning through the head of a recent graduate faced with the choice of taking on an open aortic operation with only 5 cases under their belt, referring the case on to the regional tertiary center, or trying to McGyver an endovascular solution. I contributed probably about 35-50 cases to this paper, but the outcomes were a collective effort. Even today, I will run cases by Sean Lyden, Christopher Smolock, or Lee, if only for the company and gossip.
“We explain this distribution of cases as a function of several factors: a unique, broad regional quaternary referral practice whereby patients with complex aneurysmal disease are referred to our institution; an institutional practice evolution resulting from a critical analysis and understanding of EVAR failure modes that lead to explantation, thus generating a different perspective in the EVAR vs open decision-making process; a parallel high-risk IDE fenestrated graft study; a historical willingness to accept all physician and self-directed patient referrals (ie, a willingness to manage more complex cases); and a published expertise in the area of EVAR device explantation with an annually growing volume of commercial device removals” -from El-Arousy et al.
Reading through that paper, I have come to the conclusion that the increasing open aortic volumes at the Cleveland campus has as much to do with the ongoing retirement of experienced surgeons regionally as it does with the ability to attract these cases. Loss of these surgeons has a cascade effect like losing a species in an ecosystem. The operating rooms forget where the OMNI retractor is because nobody asks for it anymore. The ICU’s are no longer familiar with the ebb and flow of the postoperative open aortic operation. The floors lose institutional memory of the care of these vascular patients as the stent grafts and interventions go home within 48 hours, sometimes the same day.
If you were a vascular surgeon born before 1970, your approach to the scenario of the ruptured abdominal aortic aneurysm may differ substantially from that of surgeons born after the Carter administration. Most of my cohort, Gen-X and older, feel comfortable applying some betadine, opening the belly and placing a clamp. Those younger than us have told me they feel more comfortable putting up a large balloon and deploying a stent graft. In this generation, it is normal to call a general surgeon to decompress the abdominal compartment syndrome and manage the abdominal vacuum dressing. For our generation, the giant industrial robot arms and 80 inch monitors creates a barrier to the problem at hand, and gathering all the extra staff after hours and on weekends requires the logistical skills of a wedding planner.
We prefer an operating table, a willing anesthesiologist, a cooler full of O-neg blood, Prolene and a graft, strong suction, and an extra set of hands. The data suggests either method is equivalent in outcome, but I would argue that depending on the circumstance, there is an optimal method for that patient and you have to have the ability to do either open or endovascular or some hybrid combination. Unfortunately, it is clear that open vascular surgery is year over year diminishing, and and it might not be so great when we start rupturing our aneurysms.
The open approach is preferred because we got good at it by doing a lot of these cases. Your hands -it becomes natural to change the course of the disease and the fate of the patient with your hands. One of the things you lose with a wire based approach is the tactile feedback from the organ that you are treating. Yes, there is a subtle feedback from the flexible tip of a Glidewire, but that’s missing the point. The thing that is rarely considered with open surgery is the tactile aspects of operating.
Your fingers are your point of care ultrasound. As an intern, one of my earliest tasks was reaching in through a 2cm incision with my index finger, feeling for what I would describe as a rotten shrimp, and delivering it out by hooking my distal phalanx around its base. Adhesions were rubbed like money between finger and thumb to judge if you could bovie through it. If you felt a sliding sensation, it was mucosa to mucosa and you looked for another spot to cut. Into my fellowship which could be called the triple-redo, no-one else wants to do-, difficult vascular operations fellowship, the pulse or the plaque felt under the finger would guide me to carve away scar tissue from blood vessel, visualizing the feedback from the fingers. In a rupture, with the belly under a dark mire of blood, there is no seeing, only feeling. Your hands reach into the lesser sac or transverse mesocolon and strangle the aorta -your fingers while clamping, feel and avoid the caudate lobe, the NG tube in the esophagus, and split the crura of the diaphragm like a pick pocket. Once the pulse returns as anesthesia refills the tank, you scratch free the aorta with your thumb and forefinger, then slide the jaws of the aortic cross clamp over your fingers and against the spine and clamp. This takes about 60 to 90 seconds (link).
When a patient is bleeding out, this is the way to control the bleeding. In practice, no amount of rehearsing for getting a patient into a endovascular suite, getting airway and access, swinging in the industrial robot arm, and getting everyone into lead aprons, sending up wire, placing a 12F sheath and an aortic occlusion balloon, will be satisfactorily smoothly and efficiently as a STEMI or STROKE alert. The rAAA is for most hospitals, unless you are in Seattle, a once in a while occurence. Many more people can find a scalpel and an aortic clamp than they can find a 32 inch aortic balloon, a stiff exchange length wire, and a 12F sheath.
When a patient presents with a slowly bleeding, contained rupture, there is time to assemble the teams required for an endovascular repair, and for opening and decompressing the abdomen, for anesthesia to get IV’s, central lines, arterial lines, and order crossmatched blood. One has the time to get and review CT scans and choose grafts. One can even do things backwards, debranching after securing the leak (link) with a stent graft. The luxury of time should signal to you that the endovascular option is the preferable route, as all the advantages of minimally invasive repair are possible. Rural hospitals sending patients two hours by ambulance or arranging for a helicopter -this is the great filter through which those likely to survive make it into the endovascular suite. These patients do great with EVAR, because everything moves more or less like a routine elective EVAR.
The setting up the operating room for tackling rAAA is quite simple. Keep everything nearby. Nothing should ever be stored out of sight, retrievable only by arcane codes whispered in the ears of people down in the basement or across the street. Amazon gives itself a day to get that gadget to you, but the rupturing patient does not have the time to have a 28mm stent graft ordered by looking up a Lawson number, finding the materials person in the faraway room to find it, running it over a city block. The stuff has to be next to the OR. Every scenario is unique, and the best planning is assuming no one person knows where everything is but everything is close at hand -major vascular sets, retractors, C-arm, cell saver, stent grafts, open grafts, balloons, cardiopulmonary bypass -every gewgaw is few steps away. The inventory is what you see, because if you can’t grab it, it does not help the hemorrhaging patient.
If you are a vascular surgeon born after 1980, it is likely that you may have trained in a 0-5 residency and all the old people harumphing about the old ways seem biased. Rather than being rational about their awful upbringing, the old people seem to suffer from Stockholm Syndrome, turning from victims of a harsh and brutal system inherited from the original, Halsted, a cocaine addict, to willing collaborators now mooning about the good old days of every other day call and 120 hour work weeks.
There might be a growing suspicion about advocating for open surgery when fewer people can perform it. One of the truisms of surgery is if only one surgeon claims to be able to do a rare operation with great results when everyone else abandons it, like venous valve surgery or robot assisted mastectomies, it can mean that surgeon might be uniquely talented or shamelessly selling something. It is a shame that open vascular surgery is devolving into that category of arcana, like the Jedi. I have no doubt that the last open vascular surgeon will be a reclusive, bitter, wild eyed hermit like Luke Skywalker was in episode VIII, if we let it get that far.
Bald eagles were saved from extinction. The methods of species reclamation may be what is needed to save open vascular surgery. Financial metabolism drives behavior, and there must be recognition of the time and dedication required to perform good open vascular surgery in the form of increased RVUs and reimbursement. The surgeons retiring in their mid 60’s with straight backs and steady hands need to be incentivized to stay around and coach the next generation in the ways of the Jedi. Call it the master surgeon designation. Every 0-5 graduate needs to focus on getting 100 leg bypasses, 50 carotid emdarterectomy, and 25 open aortas within the first five years of practice with a master surgeon if they did not get this experience during training. Like dead Jedi, it would help even if they were just virtually present, shimmering on Facetime in their (bath)robes to go over planning and approaches, but being physically present and reimbursed for it would make the most sense.
There is always self service in any human activity. One mildly prominent vascular surgeon that I have come across is famous for saying he did not have a vascular fellowship because he did not want to train his competition. It is easy for the fifty somethings to sit and proffer their open skills and profit from its scarcity but it goes against decency to not pass on this collective body of hard won knowledge and skills. There must be stewardship of this great thing we do, this honorable and treasured endowment.
Of the concrete ways we are trying is creating a network of advanced open surgery capable surgeons regionally organized by Martin Maresch, capitalizing on social media and electronic communications. Here at CCAD we are in the organizing phase of a vascular residency, and I very fortunate to have Houssam Younes join us as he shares my interest in surgical education and open vascular surgery. We are contemplating a non-accredited fellowship. We have general surgery residents coming through our service as well as medical students.
One of my mentors told me, “I can train a monkey to do cardiac surgery,” as he was training me to do cardiac surgery. And he was right. The final comment I have is you have to demystify surgery, take away the Instagram perfection, the romance, and list in practical terms the toolkit of maneuvers that form the component parts of all operations and propagate it. Let us not kid ourselves. The technical skills of surgery can be taught to anyone. The Mayo brothers were performing surgery as teenagers before medical school. The knowledge and experience and judgement -that varies as much as people vary and we have a curriculum for that, but the physical acts of surgery need to be taught starting at the medical school level. Standardized drills and exercises need to be created so that proficiency can be metered.
“The individual per trainee OAR volume did not decrease during this period. In the training program, the use of “component separation” (separation of each
operation into discrete, instructionable steps that facilitates trainee mastery) is integral to instruction of open aortic aneurysm repair techniques and permits the
trainee to master all of the technical exposure and repair skills necessary to address and to manage both straightforward and complex aneurysm anatomy. Component
separation is essential to maximize trainee experience across all levels” –from reference 1
Here is my list of things a trainee must accomplish by the time they graduate from a vascular residency or fellowship.
1. Tying knots with gloves on with 6-0 Prolene inside a pickle jar without lifting or moving a 12 ounce lead fishing weight to which the suture is being tied, fast, one handed, two handed, left and right handed.
2. Holding forceps, needle holders, and clamps
3. Correct operation of the OMNI retractor, Weitlander retractor, Balfour retractor, Thompson retractor
4. Incise skin through dermis through correct depth and length with both #15 and #10 blade
5. Open the abdomen through midline and flank incisions and close these incisions
6. Harvest saphenous vein
7. Vascular anastomosis on a table, inside a pickle jar, inside a short Pringle’s can
8. Dissection of adhesions and scar tissue around blood vessels and organs
9. Dissect and expose the common femoral artery via vertical and oblique incisions and close these incisions
10. Dissect and expose the carotid bifurcation, left and right side, and close these incisions
11. Dissect and expose the tibial vessels in various parts of the leg and foot
12. Dissect out the brachial artery at the elbow
13. Dissect out the axillary artery and vein below the clavicle
14. Dissect out the axillary artery and vein from the axilla
15. Dissect out the subclavian artery, vein, and brachial plexus above the clavicle
16. Dissect out the arm veins
17. Dissect out the iliac artery via a lower quadrant pelvic retroperitoneal exposure
18. Dissect out the abdominal aorta via midline laparotomy
19. Dissect out the abdominal aorta via retroperitoneal approach
20. Dissect out the thoracoabdominal aorta via a thoracoabdominal exposure
21. Dissect out the popliteal artery via suprageniculate, infrageniculate incisions and prone position
22. Dissect out the inferior vena cava
23. Dissect out the iliac veins
24. Harvest deep femoral vein
25. Temporal artery biopsy
26. Endarterectomy of carotid, femoral artery, any artery with patch angioplasty
27. Exposure and control of supraceliac aorta, suprarenal aorta for clamping
28. Exposure and control of thoracic aorta
29. Exposure and control of the great vessels via sternotomy and supraclavicular incisions
30. Exposure and control of the vertebral artery
31. Safe removal of vascularized tumors
32. Amputations of digits, legs and arms up to pelvis and shoulder
33. Exposure and control of radial and ulnar arteries
34. Hand surgical techniques of exposing arteries, tendons, and nerves in forearm and hand
35. Plastic surgical techniques of skin grafting and basic rotational flaps
36. Fasciotomy of arms and legs, hands and feet.
37. Exposure and control of celiac axis
38. Exposure and control of superior mesenteric artery
39. Exposure and control of left renal vein
40. Exposure and control of hepatic veins, portal vein
41. Exposure and control of renal arteries
42. Exposure and control of profunda femoral arteries
43. Safe removal of spleen
44. Transabdominal retroperitoneal exposures of the abdominal aorta and inferior vena cava
45. All of the above in a reoperative field
46. All of the above with limited visualization and by sense of feel only
47. Laparoscopic and thoracoscopic techniques
48. Orthopaedic surgical techniques of myodesis, bone grafting, precision osteotomies, infection control, external fixation, spinal exposure
49. Safe resection and anastomosis of bowel
50. Drainage of infection
51. Intensive care of SIRS, MOFS, CHF, Septic shock, postoperative fluid shifts
52. Nonsurgical and surgical management of lymphedema, seromas, and edema
53. First rib resection
54. Spinal exposure
55. Organ harvest and transplantation
56. Planning of complex open, hybrid, and endovascular procedures
Every year, it is apparent that endovascular options suffer from some flaw when outcomes are studied beyond 2 years, but progress will march on in that sphere. It has to. The loss of open capable surgeons to early retirement is accompanied by overapplication of endovascular techniques at least partly due to the lack of knowledge of these open surgical options and achievable good results and partly due to financial incentives. The solution lies in redistribution of reimbursement to open procedures and creation of open surgical fellowships and identifying and empowering mentors who still walk among us.
Mid Century Modern is a design philosophy from the mid twentieth century that seemed terribly dated and out of style while I was growing up but now seems to have come back as people dig around their parents and grandparents’ stuff. Television shows like Mad Men and Marvelous Mrs. Maisel are rotten with mid-century design. Yet it is an apt term for vascular surgeons of a certain generation like me who at about fifty years of age remember a time when vascular surgery was about big incisions and bypass grafts. We were trained in open vascular surgery and rode along with (or were drowned by) the tsunami of endovascular techniques that have come to dominate. Most of us learned to do them as well. Mid-century vascular surgeons straddle the divide between our mentors who, like me, specialized in vascular after completing general surgery training and the current trainees who have trained solely in vascular surgery. At one time it was fashionable to believe that we were fossils. But, like the coelacanth discovered after an eon’s absence, guidelines and recommendations are being made for open surgery which is supposed to be making a comeback. But it turns out, open surgery-capable vascular surgeons are, like the coelacanth, rare, and endangered. Unless we completely change the way we train people today, open vascular surgery will become extinct. At first glance, it does not look good.
The Dinosaur
My first ever encounter with a vascular surgeon was in 1989, as a lab tech in Boston the year after I graduated from college. It was at the West Roxbury VA Hospital, and like the vets, this one chain smoked in his office. Friendly enough, but a bit aloof, he rasped out well elocuted English in the same way soldiers did in old war movies like The Longest Day. Laconic and Robert Mitchum-like. He would have been among the first generations of vascular surgeons, contemporary to Jack Wylie, Michael DeBakey, and other luminaries. He couldn’t have cared less, I believe, as he performed fem-pop and aortobi-iliac and femoral bypasses and carotid endarterectomies with a furious incandescence that didn’t jibe with his reserved demeanor outside the OR. He was equally fierce to the residents when he had to scrub in to get them out of jam. But he was kind to the medical students and pre-meds like me. His type of surgeon is most definitely extinct, remembered only in old war stories like this.
What is it about my generation of surgeons? We remember things and balance the new against the old ways. We remember a time before work hours restrictions but are young enough to understand why it is not too healthy to work 120 hours a week. Yet we are also conflicted about the benefits we retained from that kind of training, now viewed with about as much approval as Sparta’s agoge system of child abuse and military training. I trained at the outset of laparoscopic surgery, so I did about 50 open cholecystectomies before learning how to do laparoscopic cholecystectomies. Most of my appendectomies were done open. As were my colectomies, gastrectomies, thyroidectomies, mastectomies, and yes, aortic surgeries, carotid endarterectomies, arteriovenous fistulae, and leg bypasses. And I did them.
We All Agreed…
This was the deal. You worked at 110%, fell exhausted and gave a little more, and you were rewarded. That meant being up all night on call, but after morning rounds, you could turn your pager off and operate all day. If you were learning, you had to be prepared by knowing the patient, the disease, the anatomy, and the operation. If you were teaching, you had to have the approval of the attending who would be somewhere nearby, and never happy if you grabbed them. If you were chief resident, you were basically junior staff and expected to run your service like a practice. The leash was longer for those who could, and short for those who could not. In the grade before mine, it was pyramidal, meaning there was attrition of those who could not progress. Like ringing the bell at Navy SEAL school in Coronado, people quit. Or were, rarely, fired. Being categorical was seen as a kind of entitlement by the disbelieving chiefs welcoming the new categorical interns. Dishonesty was the worst sin, but weakness, like showing fatigue or expressing a desire to have a life outside of work, was equally bad. And training was long. Four years of medical school, followed by five years of general surgery residency with mine extended by a year of research between third and fourth year, and then followed by a two-year vascular fellowship. By the time I was a full-fledged vascular surgeon, I had college friends who had actual homes and summer homes, children, divorces, and travels around the world. They had lived real adult lives. I started out on life at 35 where everyone else had done it at 21. But I had 1600 cases in my residency, of which over 300 were major vascular including 50 open aortic cases, and nearly 500 cases during my fellowship, adding another 100 aortic cases, most of them open, as it was the first years that EVAR was introduced. Nothing better in the world than to start a case with Ken Cherry quipping over your shoulder -“make me proud.” I finished my endovascular training apprenticed to Dan Clair during my first staff job at Columbia P&S -cue Dan intoning “you’re killing me” over the Cath Lab’s PA from the control desk on the weekends we had time in there.
There is no going back…
That represented one way of training a vascular surgeon. Even after graduating, I never stopped learning and perfecting my craft. The two years at Columbia gave me insight on how to run a practice completely alone -I was the lone vascular surgeon up at the Allen Pavilion on the northern tip of Manhattan next to Baker’s Field. It taught me the critical importance of availability and extracting useful information over my tiny flip phone. During my private practice years in Iowa, I learned the amazing productivity that can be attained when you work in collaboration and partnership with cardiologists and cardiac surgeons -something I do today here in the Heart and Vascular Institute. I also learned how to use vascular technologists and the lab as a force multiplier. And it was during the Iowa years that I underwent a period of endo-enthusiasm followed by a realism and I performed over a hundred aorto-bifemoral bypasses on middle aged patients with an average length of stay of 3 days, no deaths. When I plunged back into academia, taking a position at Cleveland Clinic, I was apprenticed again to Dan, but this time in understanding how to use the whole clinic as a tool for taking impossibly challenging patients through to an acceptable resolution. All of that started with those frantic days on call as an intern at St. Luke’s Hospital, drawing blood cultures, placing IV’s, babysitting traumas in the CT scanner, and putting chest tubes into the perforated. But there is no going back. It is most definitely probably illegal today to subject people to the intensity and duration of experience that I went through. And I wouldn’t trade that experience for all the treasure in the world (although I do regret not buying Apple, Dell, and Microsoft in 1994).
What a completely trained vascular surgeon can do
The hardest case that I have taken care of ever was at the Clinic a couple of years ago. The patient was a middle aged man who had ruptured an aortic aneurysm in another state some months prior and had undergone a repair complicated by a pancreatic injury along with some enterotomies resulting in a graft infection along with high output pancreatic and enteric fistulae from an open abdomen. He arrived cachectic, in septic shock and had a pseudoaneurysm from the distal anastomosis of a short tube graft. I immediately took him to the OR to place a stent graft across the pseudoaneurysm neck to prevent rupture and placed him on TPN to correct his cachexia. The abscesses and hematomata were drained percutaneously, and an effort was made to control the fistula with a heroic effort on the part of the ostomy team. He turned around and was able go to an LTAC on TPN and antibiotics. There he gained twenty pounds and returned flush and active. Stage two was three months later and done to replace the still infected grafts with cryopreserved homograft. I did this via a right retroperitoneal approach as the left side and abdomen were a mess from the inflammation. After I removed the grafts and sewed in the homograft, general surgery reorganized his bowel and discovered that he only had about 30cm of useable small bowel and would be on TPN for life. But he was alive and learning to walk again, and eventually came back 6 months later for follow-up and gave me a hug.
That case took all of my skill to solve, and I could not have done it without the whole hospital working in sync with me. When it comes my time, I wonder who would be able to do that for me?Who would manage my ruptured AAA properly and not have bowel and pancreatic injuries?
How to do a CABG according to Dr. Swistel
When I was an intern, I wanted to be a cardiac surgeon more than anything else, and got myself slotted for 6 months of cardiac during my second year. It was an unwanted rotation because of the 5am to 11pm hours, all nighters in the unit on call, and because the CT surgeons were notorious for not letting you do anything, except for Dan Swistel. Years before he had been one of us, a resident at St. Luke’s/Roosevelt and was Dr. George Green’s protege. He had a deal with us where he had you learn and master all the following steps in this order:
1. take vein
2. put in pacing wires and chest tubes
3. close chest
4. open chest
5. open the pericardium and set up the way he wanted
6. put the venous cannulas in
7. put the arterial cannulas and secondary lines in and go on bypass
8. decannulate and repair
9. dissect the aorta, set up and place the cross clamp
10. do the proximal anastomosis on the vein grafts
11. do the distal anastomosis on the vein grafts under the microscope which was the way he and Dr. Green did it.
12. dry up…really dry up and learn to come off pump
13. take mammary
14. book a ward service CABG and do it skin to skin
Through the history of St. Luke’s up to that point, most residents never got past taking vein. That was the great barrier, and most people really didn’t stick around after taking vein and closing the leg. They did not see the point of standing around and second or third assist. Those residents who were going to Cardiac did make it to taking the mammary, but only a handful by chief year. No one made it to 14. Dr. Swistel was always true to his word, even though some residents suspected this was all some bet that he had between himself and his brother who was not a cardiac surgeon -something about I can train a monkey to do this. To me, that last step, doing a CABG skin to skin, seemed like the final level of a very difficult computer game, like casting the One Ring into the volcano, like blowing up Agent Smith.
Every step on the ladder was something I immediately applied to my general surgery experience. On call and at home, I practiced. I practiced holding the instruments correctly and performing anastomoses on discarded grafts. I learned that every hard operation is made up of small technically feasible components, so I worked to make those moves natural and smooth. I progressed rapidly up the ladder and was by the end of my last cardiac rotation firmly at 13 on more than one occasion. Every other part of my skill set expanded during this time -central lines went smoothly, appendices and gall bladders were fished out efficiently, and fear shifted its focus to different things from what made me anxious as an intern. I learned the skill of keeping people alive through the night and making the call to take people back.
With some social engineering (ordering the cardiology fellows takeout Chinese) and vacation days traded, I got to that last step during my third year. If not a monkey, then at least Park. The act of learning and mastering each component skill lets you start and finish an operation. I don’t think Dr. Swistel was ever out to lunch while I was operating, but all those moments of letting me take the knife was crucial to my education and I am grateful to him and all my teachers, including my current partners and colleagues, as I approach PGY-25. As surgical educators, we must recognize that surgery at the sharp end of the knife is a precision craft that has to be taught much as tennis is taught starting with grip, stance, swing. That golf is learned on a driving range with a bucket of balls.
The Mid-Century Vascular Surgeon
Like Mid-Century Modern Design furniture, surgeons in my cohort are sought after by hospitals and practices for being able to let a hospital do more. What do I mean? A urologist resecting a kidney with a renal vein tumor thrombus extending into the inferior vena cava needs to have someone expose, extract, and repair the vena cava. A gynecologist debulking retroperitoneal metastases needs to be able to call for help when part of the aorta needs to go with the tumor. Cardiac surgeons need to be able to place ECMO cannulas in imaginative locations and not lose extremities in the process. A thoracic surgeon resecting a Pancoast tumor needs a vascular surgeon to repair the subclavian artery and vein. An orthopedic surgeon resecting a spindle cell tumor from the thigh needs help reconstructing the femoral artery and vein. And so on. We are safety net, the fire brigade, the SEAL team, and unfortunately many hospitals understand only when their last fully trained, full service vascular surgeon retires.
Vascular surgeons are a keystone species in a hospital’s ecosystem. When wolves were reintroduced to Yellowstone, it was noticed that decades later the forests returned to their ancient glory, that wetlands flourished breeding fish and insects and small mammal species, and the secondary predators that feed on them, and many missing bird species returned. Vascular surgeons capable of operating on the whole body as well as intervening on the whole body are increasingly a missing element in a hospital. And many of us chose to go missing -into our private endovascular suites and vein centers because it often does not pay to go do a 5-hour bypass when you can do three femoral angioplasties for claudication in the same time. Reading 10 carotid ultrasounds is easier on the back and more renumerative than a carotid endarterectomy. And I am not judging -it is a rational choice that is framed by the way healthcare is reimbursed.
The solution starts in the US with a shift in reimbursement to recognize the time and effort required to perform open vascular surgery well and to reward the programs and surgeons who are consistently good. Training in open vascular surgery will be sought after much as everyone wanted to be a cardiac surgeon back in the 1970’s. Government and society mandates set the menu, but the economics determine what is served.
And finally, every year thousands of surgeon-years of experience is retiring with the very skills that are now sought after. Rather than lose this human capital to golf courses and beaches, we should be grabbing them at the door. Like those mid-century chairs and tables, we have always been there somewhere, and its time to make some more.
It was only last month when I came across a post of an aortic aneurysm in a difficult spot (link) and I couldn’t help chiming in some comments. Reading it now, I sound insufferable, because I wrote,
“Depends on etiology and patient risk stratification. Also assuming aneurysm goes to level of SMA and right renal artery origins and involves side opposite celiac. Options depending on resources of your institute: 1.Open repair with cannulation for left heart bypass and/or circulatory arrest 2.Open debranching of common hepatic, SMA, R. Renal from infrarenal inflow and then TEVAR 3.FEVAR from custom graft from manufacturer on protocol 4.Parallel grafting to CA, SMA, R. RA with TEVAR 5.Surgeon modified FEVAR 6.Open Repair We would have a multidisciplinary huddle around this patient -Vascular, Cardiac Surgery, Cardiology, Anesthesia, and ID (if needed) to help choose. Be ready to refer to a center with more resources -including prepping patient for transfer and imaging -including uploading images to the cloud for transfer with patient’s permission. More info please”
More Info Please, Indeed
The post I commented on was of a saccular aneurysm in the transdiagphragmatic segment of aorta. Ironically, only a few weeks later, I got called from hospital transfer center about a patient with a leaking aortic aneurysm, a type V thoracoabdominal aortic aneurysm as it turned out, from an outside hospital, needing urgent attention, and we accepted in transfer based on the conversation I had with the tranferring physician. And that was the problem -usually in taking these inter-hospital transfers, you have to pray that the precious CT scans come along with the patient burned correctly onto a CD-ROM. You can buy and watch a movie in 4K resolution over the internet -about 4 gigabytes, but a patient’s CT scan which is about 200 megabytes -because of various self imposed limits, overly restrictive interpretations of laws, and lack of computer skills, these life saving images get transferred on CD in 2019. That last time I purchased a CD for anything was over 15 years ago.
An Interested Party
The technical solution –to use the internet to transfer critical life saving information between hospitals – came about when our IT folks took an interest in my quarterly complaint email about using the newfangled internet for sharing files. After mulling various solutions ranging from setting up a server to using commercial cloud solutoins, we came upon the compromise of using our internal cloud with an invitation sent to the outside hospital. I would send this invitation to upload the DICOM folder of the CD-ROM to an outisde email address. It was simple and as yet untried until this night. “Would the patient agree to have his CT scan information transmitted to us electronically?” I asked the other physician. He assured me that the patient was in agreement.
It Takes Two to Tango
Of course, being able to transfer these pictures requires a willing partner on the other side, and the referring physician made it clear he did not have the technical expertise to do so. It took a bit of social engineering to think about who would have that ability. Basically, aside from myself, who spend all their time in dark rooms in the hospital in front of giant computer monitors? The radiologists! I got through to the radiologist who had interpreted the report and explained the simple thing I needed. Gratefully, he agreed, and I sent him a link to our cloud server. I explained to him, “When you receive this, clicking the link opens a browser window and then you open the CD-ROM and find the DICOM folder and drag and drop it on the browser window.” The 200-500 megabytes of data then get sent in electronic form, as it was meant to in 2019.
The Internet Saves a Life
The brutal truth is that in locking down a computer system, many hospitals make it impossible to even load an outside CD-ROM, creating many self imposed barriers to care. Thankfully, at CCAD, we were able to work together to find a secure solution. With the CTA on our servers, I was able to review the study within 15 minutes of accepting the patient, and arrange for the right team to be assembled, and confirm that we had the right material (stent grafts) for treating the patient. When the patient arrived, OR was ready to go, saving hours of time that normally would have been required if the CT scan had to be reviewed from the CD-ROM that came with the patient. Sometimes, the CD-ROM does not come, and in a critical situation, the CTA has to be repeated with some risk to the patient for complications of the contrast and radiation.
What to Do
The patient had a 8cm sphere shaped aneurysm arising in the transdiagphragmatic aorta, leaking into the right pleural cavity.
The patient was otherwise a healthy middle aged man with risk factors of smoking and hypertension. The centerline reconstructions showed the thoracic aorta above the aneurysm to be around 20mm in diameter and same below, with the celiac axis and superior mesenteric artery in the potential seal zone of a stent graft. The only plaque seen was around the level of the renal arteries and was focal and calcified. Looking at the list I had made as a comment to the Linked-In post, I realized that I really only had one viable option.
Open repair, usually the most expeditious option, was made challenging by the right hemothorax, making a left thoracotomy hazardous if the lung had to be deflated. Cardiopulmonary bypass would have to be arranged for, and that adds a metabolic hit that greatly raises the stakes. Of the endovascular solutions, the only viable option was TEVAR to exclude the rupture and debranching of the celiac axis and superior mesenteric artery. To those who would advocate for parallel grafts, there was no room in the normal 20mm diameter aorta. And branch systems for rupture are some time in the future. Also, the patient was becoming hypotensive. So the planned operation was first TEVAR to stop the bleeding, and then open surgical debranching. A hybrid repair.
The smallest stent graft we have is a 21mm graft, but it would not be suitable for this aorta. In practice, the normal aorta is quite elastic and will dilate much more than what is captured on a CTA. The next size we have is 28mm graft and I chose this to exclude the rupture, which was done percutaneously.
As seen below, the graft excluded the celiac and SMA. Late in the phase of the final aortogram (second panel) there was an endoleak that persisteed despite multiple ballooning. The timing suggested the intercostals and phrenic vessels contributed to a type II endoleak, but it was concerning.
Find the Endoleak
The bypasses were sent from the infrarenal aorta to the common hepatic artery and the SMA close to its origin, and the origins of the celiac axis and SMA were clipped. The bypasses were then done with a 10x8mm bifurcate Dacron graft originally for axillofemoral bypassing. It had spiral rings which I removed at the anastomosis and this resulted in a kink at the closer bypass. Usually, I loop this for iliomesenteric bypass but there was not enough distance from the infrarenal aorta. I have to add a little trick I modified from my pediatric surgery experience as a resident -a Heinecke-Mikulwicz graftoplasty:
This worked to relieve the kink as evidenced on the aortogram above. After closing the laparotomy, I placed a chest tube in the right chest. The patient had a course prolonged by a classic systemic inflammatory response syndrome, with fevers, chills, and leukocytosis. He bled for a while but stopped with correction of his coagulopathy. All blood cultures were negative, but a CT scan was performed out of concern for the endoleak, and the possibility of continued bleeding.
No endoleak was detected as the sac was fully thrombosed. There was a consolidation of the blood in the right chest, but it resolved with fibrinolytic therapy.
Discussion
This case illustrates several points I have been making on this blog.
Hybrid repairs are not some kind of compromise but the full realization of a complete skill set. When students ask me how to judge a training program, one of the best metrics is how frequently are hybrid operations performed. It means either the endovascularist and open surgical operator are in complete synchrony or there are individual surgeons competent in both open and endovascular surgery. Hybrid operations, rather than being a compromise, are an optimization.
Time -Laying the stent graft across the celiac and SMA origins starts a warm ischemia clock. The liver and intestines, in my reckoning, should be able to tolerate the 2 hours of work to get the bypasses working. Cardiopulmonary bypass may give you less ichemia but at the metabolic cost of the pump time. These negative factors add up, but were surmounted by the fact that early control of hemorrhage was achieved. Stopping the bleeding and restoring flow are the core functions of vascular surgery.
Planning and preparation. The ability to see the CT images and prepare the teams and materiel before the patient transferred was lifesaving. This is where our IT gets credit for responding to a critical need and formulating a solution that meets internal policies, external regulations, and saves a life. It illustrates so many opportunities particularly with electronic medical records and their processes which focus more on documentation for billing. A discharge summary should be multimedia like this blog post and it should be normal and easy to generate. And finally, as clinicians, we should mind technology with as much attention as we give to the latest medical devices and techniques.
View out of my balcony, sometimes you need many pieces to assemble a beautiful whole
Innovating Our Way Out of Not Having Enough Vascular Surgeons
This year’s SVS meeting featured a sobering assessment about the vascular manpower deficit affecting North America at the E. Stanley Crawford Critical Issues Forum, moderated by Dr. Michel Makaroun, MD, president-elect of the SVS. 35-45% of practicing vascular surgeons plan on retiring in the next decade by conservative estimates. We are not attracting enough candidates for the training programs. The solutions, including decreasing the length of training, public relations campaigns, and incentivizing retention have had mixed results, but we have yet to see a sustainable rise in vascular surgeon numbers.
Burnout driven by lack of work-life balance, the advent of electronic medical records optimized for billing, the passing of the private practice era, and the constant need to adapt to new techniques, create a persistent downdraft on staffing. So as some hospital face the reality of having to contract services, little attention is given to delivering best care with the staffing that we have. Changing how we practice is the only viable solution.
There are an estimated 3000 active vascular surgeons in the US. Imagine if all the cheese needs of this country could only be met by 3000 artisanal cheesemakers who make cheeses one at a time and want to live in places with international airports, BMW dealerships, and major league sports teams, and must have 3-4 partners to share cheese call. If you are a rural hospital in dire need of vascular surgery services and your one vascular surgeon is retiring, you are probably SOL.
When I was training, vascular surgery was oft touted as a primary care specialty. And that is how many of us still practice, managing risk factors, monitoring mild disease, as well as planning and performing interventions and operations. As much as I enjoy that kind of interaction, the half hour to an hour visit for a head to toe cardiovascular survey and discussion, educating patients and families about pipes and pumps, is incredibly inefficient. A healthcare system, a hospital, facing a staffing shortfall, has to do everything possible keep that vascular surgeon in the OR during work hours.
What is the core function of a vascular surgeon? Making good decisions and executing plans well. Decisions require data. What is this data? We laud the history and physical examination, but this is a throwback to another era. If you look at the diagnosis of myocardial infarction, it is not standard practice for a cardiologist to come and get a history, examine the patient, and declare that the patient is having a heart attack based solely on history and physical examination. It is a triage nurse in the ED who draws labs and orders an EKG which is read by a machine. These data points will tell you if heart muscle is being damaged. A process is started which triggers a team to come and take care of this patient. The hospitals focused on this actually drill their cath lab teams like pit crews. A stopwatch starts with the goal of revascularization under an hour.
Not so with peripheral vascular disease. The ischemic foot might have only a few hours depending on its presentation before it is irretrievably lost, but no matter -they sit in the ED until a vascular surgeon comes to speak to the patient and family, examine them, and then order tests, admission, consults, and operating room -typically all by themselves. Getting these patients into the operating room is in many places hampered by the lack of dedicated OR staffing, radiology techs, anesthesiologists, space, equipment, and critical care capacity. During work hours, there are scheduled cases that have to be delayed or canceled for another time, which takes time to do. After hours, the patient may have too many comorbidities to handle safely with the available staff. The vascular surgeon may have to bargain and cajole, to align several factions whose attention is demanded by many equally important concerns. If you decide to hold a lavish dinner party of twenty important guests -reserving space, calling caterers, inviting guests, arranging transportation – on short notice, you might pull it off once, but if you do this regularly, you are a masochist of the first order.
In the heart attack model, the history and physical examination is relegated to a series of yes/no or how long questions, and positive responses trigger a series of coordinated actions of a system -a reflex. In the leg attack model, there is no such system. I have to blame the vascular surgeons for preserving the current model. Vascular surgeons are organized as a guild. Guilds are protective of their monopolies on skills and markets and fiercely resist change. Most vascular surgeons are terrified by loss of control, and cling to the notion of being misunderstood and unappreciated saviors. We can do better.
The area that needs streamlining is at the point of referral. The majority of time of a vascular surgeon is spent working up normal blood vessels, varicose and spider veins, leg edema and pain, and mild and moderate arterial atherosclerosis. This work initially does not require a vascular surgeon but rather a focused set of policies and initial diagnostic studies that can be administered or ordered by any caregiver. Reducing the need for vascular surgeons at this point in vascular care will go a long way in extending the vascular work force at hand.
Point of Care Blood Flow Evaluation
Finding and declaring blood vessels to be normal is challenging and too often time consuming. Streamlining this will go a long way in freeing vascular surgeons to take care of disease.
The average caregiver is an inconsistent pulse taker. The palpable pulses are not always easy to find. Asking over the phone or as policy for someone to examine pedal pulses -the posterior tibial artery and dorsalis pedis artery pulses, is challenging. A positive is just as likely to be true or false as a negative. No cardiologist would ask a similarly detailed and technical question about an MI. In fact, they can’t ask, “Is there a pulse in the LAD?” Cardiologists make do with tests easy to obtain and interpret with certainty -the plasma troponin level and the EKG. The EKG is read by an algorithm so established and so tested, that it should stand as an example of early machine intelligence taking over a human job -but I digress.
What is our EKG? It is not the ABI -the ankle brachial index, because it is terrible at identifying disease, and is difficult to obtain reliably without practice. The closest thing to an EKG we have in terms of simplicity and accuracy is the pulse volume recording, the PVR (figure below). A FloLab machine, the machine used to obtain PVRs, will basically run itself once the cuffs are correctly applied on the leg, and the tracings are very easy to interpret. Unlike an EKG, there are no electrodes whose locations you must memorize. If the closest vascular surgeon is an hour away by ambulance, the transfer of a patient with flat waveforms and ischemic foot does not require a consultation on site. The patient would go to the vascular surgeon with no time wasted and no kidneys injured by CTA’s that too often fail to travel with the patient. Unlike an EKG which can be performed by many caregivers, a PVR requires both the equipment and a vascular technologist. A vascular technologist is not available 24-7 in most hospitals, and FloLab machines purchased for vascular labs are not meant to be dragged around the hospital.
So let’s think out of the box about another box in every triage nurse’s cell, every ER and ICU bed, and on every hospital nursing floor. These are pulse oximeters with a digital tracing, and bonus points, some come with strip printers! Placing a pulse oximeter probe on the second toe and comparing to an erstwhile normal wave signal such as on an index finger can provide qualitative information about normality and disease. Normal waveforms and abnormal ones can be easily discerned. A flat line is another obvious finding when in comparison, a finger or an ear on the same patient has normal signals.
How much better would a vascular surgeon feel about a transfer call that has this information, “digital waveforms are flat in this patient with rest pain and a bruised toe.” How much better would a vascular surgeon feel about a call about a patient with “digital wave forms are normal in this patient with toe pain and a bruised toe. We got an x-ray and there was a fracture.” The communication can be quite detailed and refined. For example: “The patient had no pulses, we think. Digital wave forms were dampened but pulsatile in a patient with a bruised toe, we’ll send to vascular clinic in the morning.”
A study comparing pulse oximetry signals and ABI in type 2 Diabetes Mellitus found the following results (link).[i]
Method
Sensitivity
Specificity
PPV
NPV
Pulse oximetry
74.1%
95.7%
83.3%
92.7%
ABI
70.3%
87.1%
61.3%
91.0%
These data suggests pulse oximetry signal is equal to and somewhat better than ABI. Why is this important? Cost. This information is better than asking unsure people, “Is there a pulse?” A vascular technologist need not be on call 24/7. Extra FloLabs for ED, ICU, and floors need not be purchased. The pulse oximeter with waveform tracing is nearly ubiquitous wherever patient’s oxygenation needs to be assessed in most hospitals. While not perfect, it has great potential for serving as vascular surgery’s EKG machine for critical limb ischemia. Policies and algorithms can be built out in collaboration with Emergency Departments and nursing departments that can effectively determine if blood flow is normal or abnormal at point of care. Effective emergency responses to critical limb ischemia can be authored triggered by abnormal findings. Acute limb ischemia protocols based on time sensitive responses can be initiated. All of these can flow from referring entities being able to determine objectively normal or abnormal blood flow.
Clinic
The vascular clinic is a sorting process where patients are determined to be normal or have mild, moderate, or severe disease. The vast majority of the time spent in clinic can be spent in triage by trained nurses and testing by technologists. Clear pathways and guidelines can dictate the ordering of vascular laboratory tests obviating the need for vascular consultation at this stage. Patients with normal blood vessels and vascular function are sent back to their physicians with the normal report. Patients with mild disease and moderate disease are sent to a physician with specialization in cardiovascular medicine for management of risk factors and periodic surveillance. At any point in the process, a vascular surgeon can be called to provide guidance and direct patients to different tests and consultations. The patients needing operations, based on correct indications and imaging are sent to a focused clinic where the surgeon and interventional team can review films, determine the urgency of indications balanced against risk, and plan and schedule procedures. Currently, vascular surgeons do all of this by themselves, as well as make hospital rounds, perform procedures, and interpret vascular laboratory studies, seeing one patient at a time.
In introductory computer sciences courses, search algorithms are taught to be brute force if you look at one item at a time for the thing you want, and to be efficient if you have presorted those items because every time you look, you can exclude part of the data set, ever shrinking the pool in which you search, making the search shorter and faster
The shortfalls in vascular surgeon numbers have as much to do with this dependence on the star chef cooking up one meal at a time, rather than a team working off recipes, with the chef directing the flow and occasionally jumping by the fire to make the most difficult of dishes. The first restaurant can seat three parties. The latter, easily ten times the number. Everyone gets fed.
Only asking how many vascular surgeons you need misses the big picture because there are many equally important questions. How many vascular technologists do you need? An accredited laboratory provides the critical diagnostics upon which decisions are made, and the surgeon should oversee but not be directly involved in the initial screening. Nurses trained to triage and order vascular laboratory tests and even perform the simpler ones is the second need. Third, is the cardiovascular medicine physician who manages those patients discovered to have mild to moderate disease, and depending on symptoms, refers severely symptomatic moderate disease and severe disease to a scheduling clinic. The scheduling clinic is composed of both interventionalists and vascular surgeons who plan interventions and operations.
Surgeons must be in the operating room to be effective. A well thought out and organized system, with interlocking teams, and well disseminated basic knowledge and awareness of vascular diseases reduces the need for a vascular surgeon to be present all the time in many places and ultimately increases the effectiveness of the vascular surgeons that are available by keeping them in the operating room. The system needs to be set up by the surgeon to allow clinic to be a setting mostly for consenting the patient for an operation or a discussion of treatment options.
Finally, vascular surgeons must be aligned with all the resources of the hospital including the considerable numbers of interventional cardiologists and radiologists, neurologists, and nephrologists. There is no reason someone should wait a month to get on the OR list for an iliac angioplasty and stent if an equally skilled and privileged cardiologist or radiologist has an opening the next day. The surgeon’s special talent should be open surgery and hybrid surgery -that which mixes open surgery and intervention in optimal measures which is not possible from a purely percutaneous approach. The key is frequent and easy communication between specialities and trust built by being in one shared cardiovascular institute.
Execution
There is a critical need of good operators. The acuity of disease and their solutions demand the continued presence and availability of open surgery. The fact is, many solutions are optimal in a hybrid fashion and for peripheral vascular disease, these options can only be offered via a vascular surgeon trained in both open surgery and peripheral interventions, or in a combined effort of open surgeon and interventionalist. And many disease categories can only be managed by open surgery.
The reality is that silos, economics, and practice patterns prevent this kind of combined effort. Market forces have pushed the training of vascular surgeons forcefully into the interventional realm at the cost of open surgical training. Some of the geographic maldisdribution of vascular surgeons has to do with younger vascular surgeons flocking to established practices where there are senior surgeons more comfortable in opening a belly or chest (or both). The trap they and hospital systems fall into is then allowing these new recruits to become the interventional specialist of that group, relegating the aging open surgeon to a narrow role, and then finding that the hospital has a problem when that surgeon announces retirement at 60. Every year, millennia of surgical experience retires to beaches and golf courses. The hospital systems should recognize this brain drain as a crisis and create work arounds that keep these skills going. The other opportunity lost is close coordination with interventional cardiologists, radiologists, and nephrologists who in many cases compete with vascular surgeons for the same patients but treat the patients based on their training and skill sets to the exclusion of potentially better operations offered by surgeons. This disjointed care creates both suboptimal outcomes for patients and high costs for hospital systems.
Commerce should never dictate the fate of a patient. A particular point is where competencies and privileging overlap, and guidelines recommend intervention over surgery as in the case of a TASC A or B iliac artery lesion. A patient should not be kept waiting weeks for a spot on a busy surgeon’s OR schedule when an open interventional cardiologist or radiologist slot is available for a iliac stent the next day. It should be a matter of practice that these cases are discussed and distributed, optimally in a shared indication clinic or rounds. Patients bumped off of a surgeon’s elective schedules for emergencies who could be cared for by an interventional partner without an added delay should be given that option. This kind of change requires a commitment to continual reorganization and optimization into a vascular institute.
Conclusion
The perfect vascular surgeon is a unicorn -well skilled, and experienced in open vascular surgery, but also versatile, innovative, and skillful in wielding a wire. I can name just a handful of unicorns. An apt analogy from the book Moneyball is the signing of superstars in baseball on the free agent market. The upshot of that book is that you can arbitrage for the valued metrics through signing several utility players with an aptitude for one thing or another which in sum equals or exceeds that superstar and get the final result -wins, in the same proportions as overspending on a superstar. Rather than searching for that unicorn, it is more important to set up the right system. Screening, testing, and management of mild vascular disease by a nurses and cardiovascular medicine physicians, while directing operations and interventions to vascular surgeons, cardiologists, and interventional radiologists should be the next step in the evolution of vascular care systems. There will never be enough vascular surgeons in the current system. The critical and rare competency is open vascular surgical skill. A surgeon who performs only interventions is not an “advanced minimally invasive practitioner” but rather someone equally privileged as an interventional cardiologist or radiologist, and therefore easily replaceable by an interventional cardiologist or radiologist specializing in peripheral vascular disease. A surgeon skilled in open vascular surgery is becoming rarer every year, but they are still out there, looking at brochures of real estate in sunny places. A team consisting of a cardiovascular medicine physician, many vascular technologists, nurses specializing in vascular diseases, several interventionalists, and a vascular surgeon skilled in open vascular surgery working as a single unit, is far more easy to assemble than finding and recruiting a herd of unicorns.