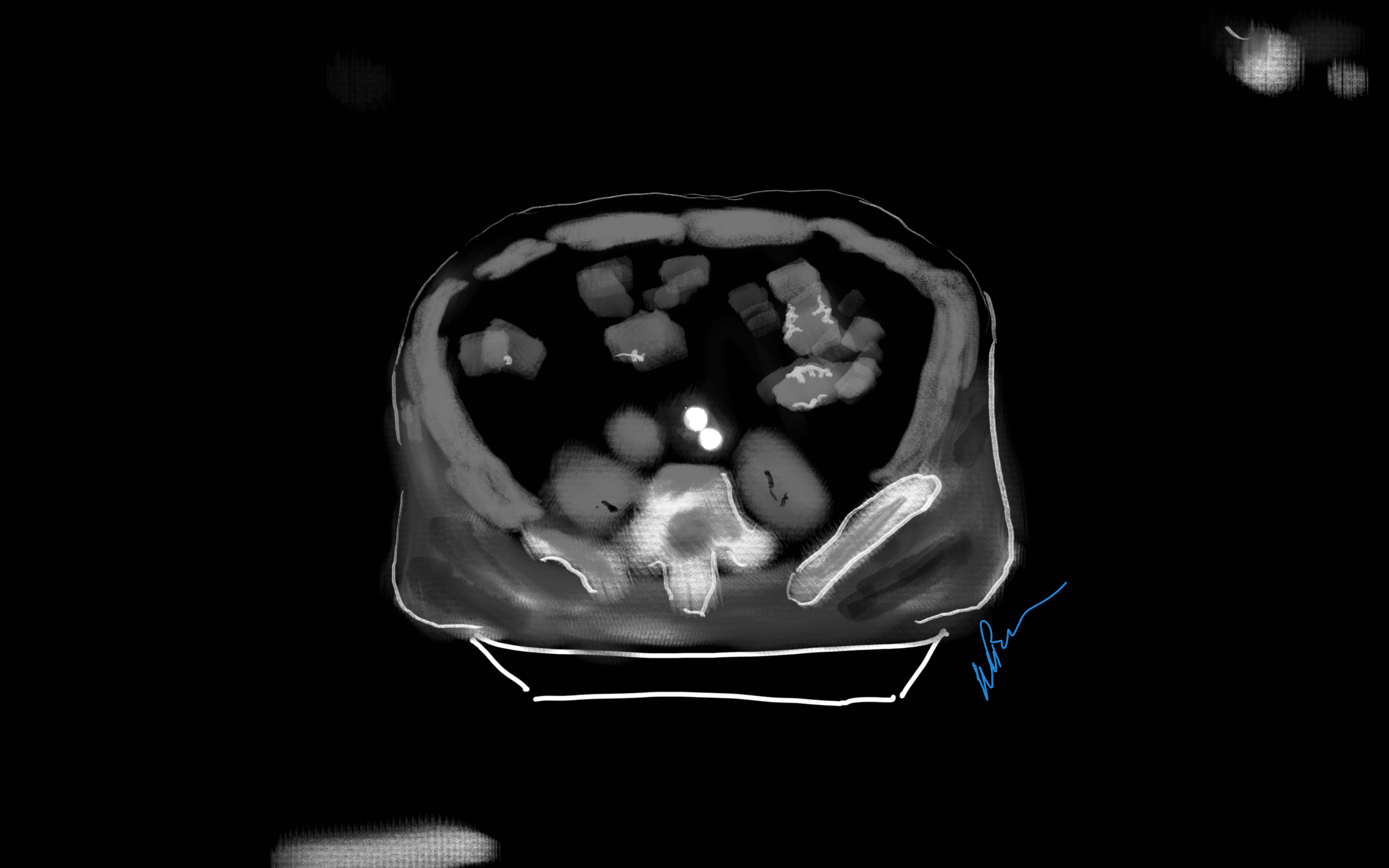
Look again, it is a doodle of a CT scan of a patient with an Ancure stent graft with sac shrinkage
I remember in the mid-2000’s, driving very fast to Lutheran Hospital in Des Moines on a Saturday night to fix an aneurysm that had ruptured. He was a man over 70 years of age with a type III endoleak from a component separation. The endografts had been placed by a cardiac surgeon who had taken some courses. I rescued him by open replacement of the aneurysm with a tube graft after I pulled out the endografts. Later, as the patient recovered, I asked him why he never followed up as required on his stent graft. His answer was, in typical Iowa farmer fashion, “Welp. If it was fixed, why should I?”
Indeed, why should he? Looking at his chart from the time of his EVAR, he was determined to be a “high risk” patient, necessitating the new minimally invasive procedure EVAR in 2003. Seeing that he survived the stress test of a ruptured aneurysm, it was clear he was not all that “high risk.” I did reassure him that with the open repair, he was basically cured. Despite scheduling a followup appointment, he never showed up. And that was okay.
EVAR is a treatment for AAA, but currently not a cure. All of the devices instructions for use stipulate the need for lifelong followup with CT scans with contrast and visits with qualified specialists. As I have mentioned in the past, what other condition requires surveillance CT scans with contrast and followup with a specialist? Cancer in remission. For those with good cardiac risk and functional status, placing an endograft rather than open repair creates “Aortic Aneurysm in Remission.” If they are in the majority of patients with a stable aneurysm sac, their endografts are sitting in a bag of static, aging blood. If there are type II endoleaks, and it is my belief that the majority of stable aneurysm sacs have some type II endoleaks that blinker on and off depending on the hemodynamics, particularly through needle holes, they are circulating the products of breakdown of that bag of old blood and exposing a perfect culture medium to potential inoculation. These type II and IV endoleaks can inflate the aortic sac over time. Occasionally, the residual AAA sacs rupture, erasing any of the early advantage conferred by the minimally invasive index procedure in long term followup EVAR v OPEN repair.
What is a cure? A cure is when you quell an infection with an antibiotic. A cure is when you’ve taken out an inflamed appendix. It’s when you’ve eradicated early stage cancer. It’s when you perform an open aortic graft and the patient can disappear after you remove the dressings and never followup, sure in the knowledge that the aneurysm in that spot will never bother them again. With EVAR, only a minority get to the state (figure at top) a sac shrunk intimately around the endograft. Most are not cured but enrolled in a regime of lifelong surveillance and maintenance.
EVAR does allow people to leave the hospital with less scarring and pain, but the consequences of its popularity are:
1. Letting more practitioners, not all of them vascular surgeons, treat aortic aneurysm disease with less training and with less or no ability to manage the inevitable failures surgically.
2. Creating the business model for “Advanced, Minimally Invasive, Super-Fantastic Aortic Centers of Excellence” which is predicated on the business of surveillance and maintenance of aortic endografts. It is a busy-ness that generates revenue, but burdens the country with more healthcare costs. It ultimately siphons business away from true centers of excellence involved in training the next generation of vascular surgeons.
3. Skewing the training curriculum of trainees to endovascular so much that I have met vascular surgeons who have done no aortic operations. That was the case when I sat in on an open aortic surgery class at the 2017 ESVS meeting in Lyons, France. All the attendees were very eager to try sewing anastomoses, but felt they needed proctoring which isn’t available.
4. Establishing the expectation that open aortic surgery is a failed, antiquarian, obsolete technique to be relegated to the history books. This last one is infuriating and not true but it is out there in the claims of the aorticians.
5. Resulting in palliation when the aortic aneurysm in remission ruptures and there are no readily available open-capable surgeons experienced in rescuing these patients. This happens. Don’t let it happen to you.
Various solutions have been broached including regionalization of aortic aneurysm care, superfellowships in exovascular surgery to complement the widespread endovascular training, and going back to open aortic surgery as the norm as had been proposed controversially in the UK. There is no turning back the clock. The moment that Dr. Parodi combined an aortic graft with Dr. Palmaz’s stent, a quantum leap occurred. The operation of aortic aneurysm surgery was changed from a challenging operation mastered by a few to a straightforward procedure performed by many.
Interesting to me is that illustration at the top of the post is of a common observation – the obliteration of the aortic aneurysm sac around a Guidant Ancure stent graft. When the sac disappears, it is as close to a cure that you can get. For some reason, I see this more frequently with Ancure than with other grafts over the past twenty years.
Odd fact -I may have been the last surgeon to implant an Ancure in the world. In 2003, I was treating a AAA with an Ancure graft when the delivery system froze in mid deployment. I called Dr. Dan Clair away from some meeting, and he called for pliers, screw drivers, and a saw, and after deconstructing the delivery system, deployed the graft and returned to his meeting with nary a word. The Guidant rep, who had been on the phone, looked up with saucer eyes, and said, “Wow. They’ve pulled Ancure off the market.”
I think it is because of the design, which is now off the market. When stents are sewn to cloth, the needle holes leak, and leak particularly where the stent graft makes a turn, stretching the suture hole. Junctions and seams leak. The Ancure, aside from the stents at top and bottom in the seal zone, has no such holes as it is unsupported and manufactured as a single piece with no junctions or seams. It is the closest you get to sewing in a graft by open surgery. If it weren’t for its overly complicated delivery system which was its downfall, I think it would be in its third generation with visceral branches that are created off the textile machines rather than joined inside the patient. There are lessons to be learned from this abandoned tech.
I believe a treat once and walk-away cure is achievable in EVAR. The idea is not to be satisfied with anything less than a cure, anything that ends with aortic aneurysm in remission. We have to understand we have chosen a path of iteration and continuous but slow improvement in the EVAR space. The front end benefits of EVAR are clear but it is in the long term we have to focus. Until then, warranties would be great.
Patient with infected femoral pseudoaneurysm, skin necrosis, about to blow
A surgeon from Nepal posted a case of a ruptured common femoral pseudoaneurysm infected from IV drug abuse on LinkedIn. The comments centered around typical textbook responses which were:
Ligate, debride, obturator bypass
In situ bypass with femoral vein +/- sartorius flap
Rifampin soaked graft or crypreserved allograft
Ligate only
My preferred treatment is #2, in-situ bypass with harvest of adjacent deep femoral vein. I never liked that procedure because in general in these patients, everything bleeds. Then I had a thought -how about if you mobilize the external iliac artery in the pelvis over its entire length and pull it out from under the inguinal ligament to sew to the femoral bifurcation or SFA? That is, when you enter the pelvic retroperitoneum to gain proximal control:
The external iliac artery is usually redundant and elastic in young people
You mobilize the external iliac artery from the iliac bifurcation to the inguinal ligament, detaching the inferior epigastrics as a last step. And then you pull it out from under the inguinal ligament, and anastomose it to the femoral bifurcation or the SFA.
The mobilized external iliac artery is pulled down to reach normal femoral artery. The distance x is the length of CFA that needs replacing
This makes sense because in young people and those with AAA and minimal atherosclerosis, the external iliac artery is both redundant and elastic, making it suitable for a pull down transposition. But then, how do you know as you mobilize the artery in the pelvis that you have enough to pull down?
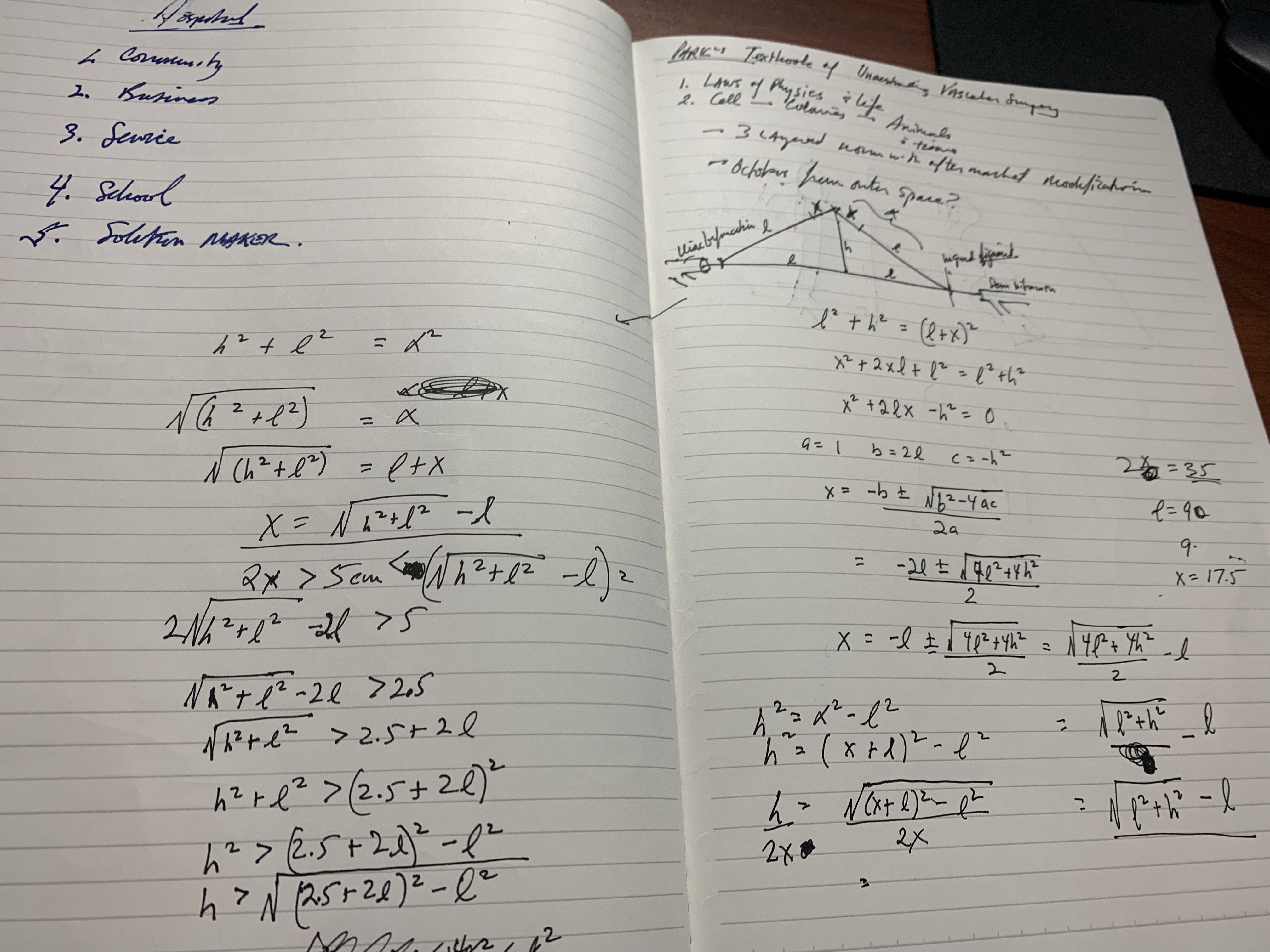
Pythagoras figured that out two an a half millenia ago. If you measure the straight line distance from iliac bifurcation to the takeoff of the inferior epigastric arteries, you get the straight line external iliac artery distance. The length of the common femoral artery which is the excess EIA length needed, is assigned the value x. Then the height of the stretched artery off the line between the iliac bifurcation and the inguinal ligament will determine how much extra artery you have.
Taking these values, I did some maths.
The solution for h, the height, is highlighted in yellow below. (note, the variable x in my notes is half the length of CFA, l is half the length of EIA, ie. 2x is CFA length).
Creating a spreadsheet for CFA lengths from 2 to 6cm and EIA straight distances of 5-10cm, the ratio of height H to CFA length varies from a minimum of 0.7 to maximum of 1.7 with an average of 1.1. That means the majority of the time, if you get 1.5x the length of CFA height off the pelvis, you should reach.
If you are short, you can detach the profunda and mobilize the SFA, pulling upwards, then reattach the PFA. Though this is entirely a thought experiment, there is no reason why it should not work. As with most things, I predict that it already has been done!
The advantages are using autologous tissues and leveraging the natural anatomy. There is a cost benefit in that OR time is shorter with less time for venous harvest and avoiding grafts, patches, and devices. The patient would avoid ischemia as would happen in the staged repair. The disadvantage is when you are short, but if you mobilize the appropriate amount (height off pelvis at least 1.5x the CFA length) you should be okay. The more curvature and tortuosity seen on 3DVR recontstruction and absence of significant atherosclerosis would predict feasibility.
Every once in a while, I will make an exception to the SVS guidelines on AAA repair with regard to size at time of repair (link). I have a bunch of excuses. When I trained in 2000-2002 with several giants of vascular surgery, there was some controversy when the first guidelines came out in 2003 (link). The board answer became 5.5cm that year, but where I trained, it was a minority opinion held by Dr. Jeb Hallett. The majority was in the belief that as long as operative mortality was low, even high risk AAA repair could be undertaken (link). The published risk for Mayo was low, and that came from both technical excellence and high volume (more on that later). The criteria during my fellowship was 4.5cm in good risk patients for open repair based on data generated in the 1980’s and 90’s during Dr. Hollier’s tenure.
Then as now, the debate centered around the balance of risk. At specialty centers that achieved less than 1% mortality rate for elective open AAA repair, 4.5cm in good risk patients would seem perfectly reasonable. But given the 5-10% mortality seen in the Medicare database at that time for community practice, the 5.5 cm criteria was not only good science, it was prudent. The first set of guidelines held off the contentious volume recommendations that was the nidus of conflict within other surgical societies.
The advent of endovascular was a game changer -the mortality rate in the Medicare databases was 1-2% for EVAR in the community setting, meaning more surgeons in most hospitals could achieve tertiary center levels of mortality with this new technology. The issue was never really settled in my mind through the 2000’s, even with the PIVOTAL Study. I enrolled patients into the PIVOTAL Study (link) at that 4.5cm threshold during my time in Iowa. Eventually I lost equipoise and I stopped enrolling after a handful of patients. It had to do with graft durability.
Around that time, I took two patients in a row to the operating room for sac expansion without identifiable endoleak. They were Dacron and stent-based endografts placed about 5-7 years before by another surgeon and aortography failed to show type I or III endoleak. Sac growth was over a centimeter in 6 months and the aneurysm size was over 6cm in both. I chose to marsupialize the sac and oversew any leaks, with the plan to replace the graft if there was a significant leak. On opening the sac, no significant lumbar or IMA leaks were encountered but in these patients a stream of blood could be seen coming from the sutures securing the stents. It was the same graft that was in the trial, the AneuRx, and that was when I realized that these grafts have the potential to fail in the same way that patio umbrellas leak after years of use -cloth sewn to rigid metal with movement wears open the cloth wherever there is stitching. This did not happen with open repair. I lost enthusiasm for the trial as I lost faith in this graft which was retired from the market. I placed pledgetted sutures to close the leaks on both patients, and closed the aneurysm sac tightly around the graft in one patient who was higher risk, and replaced the stent graft in the other.
There are some exceptions to justify repair of 4.5-5.5cm AAA. During my time in practice, there were patients who lived far away from major medical centers who would not survive a ruptured AAA even if the rupture rate was low and who confessed they only came into town every five years or so. There were patients who suffered from clinical anxiety whose AAA was documented by a psychiatrist to amplify their anxiety. There were patients with vague abdominal pain for whom thorough workup have ruled out gastrointestinal causes and every visit to the ER triggered a CT scan to rule out AAA rupture. And there seemed to be some patients who seemed to have such perfect anatomy for EVAR, whose risks were low, and whose growth rates were so consistent that their repairs could be timed on the calendar. Some combination of these factors and lobbying on the part of the patient got them their repair in the 5cm range. And they still do.
The patient is a man in his sixties with hypertension who presented with a 4.7cm AAA which in various reports he came with described 5.2×4.7cm. After review of his images, it was clear it was 4.7cm. If measured on a typical axial cut CT scan or a horizontally oriented ultrasound probe, a cylindrical aortic aneurysm will be seen as an ellipse in cross section. A radiology report will typically report an aneurysms length and the anteroposterior and lateral dimensions. If you cut a sausage at an angle, the ovals you cut can be quite wide but the smaller length of the oval reflects the diameter of the sausage.
Looking back at his records, for three years he had multiple CT scans for abdominal pain showing the AAA and a well documented record of growth of about 2-3mm annually -the normal growth rate. He asked me to prognosticate and so I relayed that 4.7cm in 2017 with a 3mm growth rate, we would be operating in 2020. The anatomy was favorable with a long infrarenal neck and good iliac arteries for distal seal and access. He was quite anxious as whenever he had abdominal pain, his local doctors would discuss the AAA and its risks or order a CT. After a long discussion and considerable lobbying by the patient and family, I agreed to repair his 4.7cm AAA.
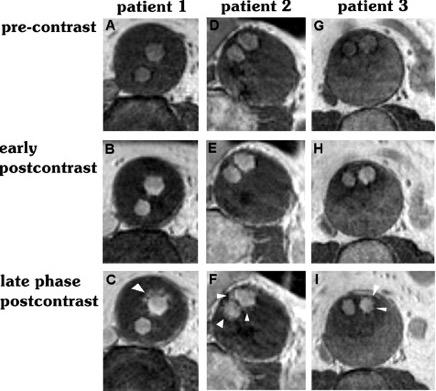
The EVAR was performed percutaneously. No endoleak was detected by completion arteriography (figure). He was soon discharged and was grateful. In followup, CT scan showed excellent coverage of the proximal and distal zones and absence of type III endoleaks. There was increased density to suggest a type II leak, but his inferior mesenteric artery was not the source of it. over a three year period, his aneurysm sac continued its 2-3mm of annual growth despite the presence of the the stent graft.
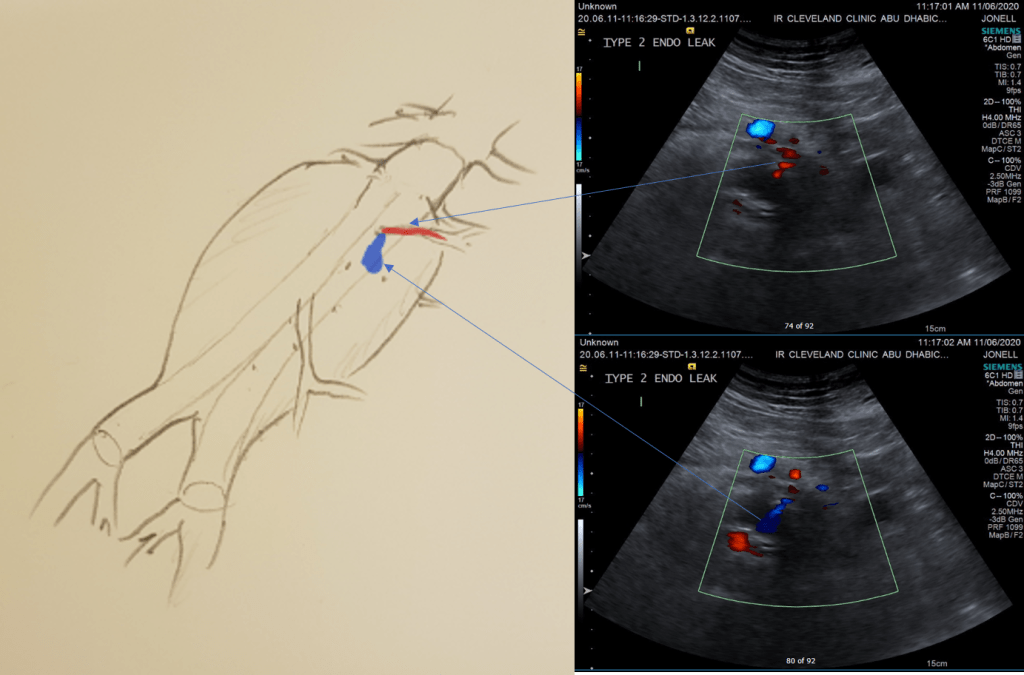
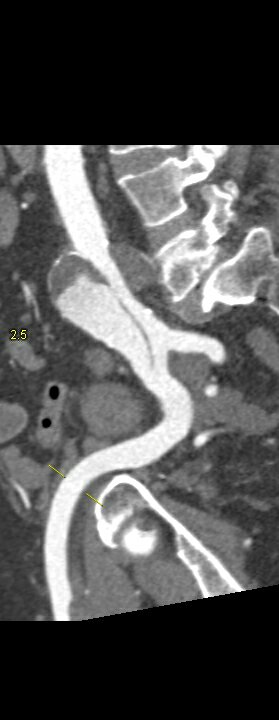
While CT failed to locate this endoleak, abdominal duplex ultrasound did showing flow from a small surface vessel (duplex below, figure at beginning of post). It was not the inferior mesenteric artery which can be treated endovascularly (link) or laparoscopically (link). CT scan suggested that it was one of those anterior branch vessels that one would encounter in exposing the aorta. Usually these were higher up as accessory phrenic arteries, but these fragile vessels, larger than vasovasorum, but smaller than named aortic branches, are seen feeding the tissues of the retroperitoneum.
Ultrasound revealed the type II endoleak from an anterior retroperitoneal branch artery.
Type II endoleaks are not benign. The flow of blood into the aneurysm sac after stent graft repair is almost never benign. It is a contained hemorrhage. There are three components to the pressure signal seen by the aortic aneurysmal wall that could trigger breakdown, remodeling, and aneurysm growth. They include pressure, heart rate, and the rate of change of pressure. The presence of fresh thrombus may play an inflammatory role. Some endoleaks clearly have a circuit and others are sacs at the terminus of their feeding vessels, never shutting down because the AAA sac can both accept and eject the blood flow. Changes in AAA sac morphology due to sac growth can cause problems with marginal seals, component separation, and component wear. Sac growth can cause pain. Ruptures, while rare, can cause death. Mostly, type II endoleaks generate more procedures because it is hard to ignore continued growth.
Review of aortogram from device implantation showed a small anterior artery arising from the proximal aortic sac (arrow)
Three years of followup showed growth of the AAA sac to 5.5cm, which ironically threshold for repair. Again, no type I or III endoleak could be seen. He reached his calculated repair date, and I discussed our options in detail.
1. Do nothing, keep following
2. Endovascular attempt
3. Open surgery, marsupialization
4. Laparoscopic ligation of target vessel
Doing nothing hasn’t worked for 3 years. What would more time buy? Endovascular -to where. The IMA is the usual target for an endovascular attempt, although iliolumbar access is possible (link), we really needed to fix this with one attempt. Open surgery is a great option -a short supraumbilical incision is all that would be needed to open the AAA sac and oversew the collaterals. The patient did not want a laparotomy. There are reports of laparoscopic guided endovascular access with endovascular coiling of the remnant sac with fluoroscopy. This adheres to the letter of the claim of minimal access, but really?
I compromised with the patient and offered laparoscopy. I have ligated the IMA a handful of times laparoscopically -these are relatively fast and straightforward cases. As I had the location of the endoleak, I felt it should be straighforward to dissect out the anterior sac much as in open repair and clip this vessel.
Use of ultrasound allowed localization of the leak and identification of the artery for clipping.
Of course, what should have been a 30 minute procedure through a minilaparotomy became a two hour enterprise getting through scar tissue (not the first time encountering this after EVAR) while pushing away retroperitoneum. I recruited the help of general surgery to get extra hands, but the patient was well aware that there was a good chance of conversion. Patience won out as the artery was ultimately clipped and endoleak no longer seen on ultrasound.
I waited a year before putting this together as I wanted CT followup. The sac stopped growing and has shrunk a bit back to 5cm or so. There will be those who argue that nothing needed to have been done about this leak as it would have stopped growing eventually, but I would counter that an aneurysm sac that kept growing like the stent graft never went in is one demanding attention. The key role of duplex ultrasound cannot be minimized. We have an excellent team of vascular scientists (their title in Europe), and postop duplex confirmed closure of the leak.
Not seeing the leak anymore is a positive, but the stent graft remains.
The patient is quite satisfied having avoided laparotomy. His hospital stay was but a few days. During my conversations with our general surgeons who are amazing laparoscopists, that this would have been a nice case with the robot. That’s a post for another day.
The definition of success in this case and many EVAR’s plagued by type II leaks leaves me wondering. Excellent marketing of the word “minimally invasive” has subtly defined laparotomy as failure, and not just in vascular surgery. When costs and efficacy are reviewed as we come out of this pandemic, I suspect that open surgery will selectively have its day in the sun. A ten blade, a retractor, a 3-0 silk is so much more cost effective than five ports and disposable instruments. And a stent graft system?
Despite all the advances in endovascular repair of thoracoabdominal aortic aneurysms, no data shows their superiority in the mid to long term compared to open repair. That is why branched stent graft programs occur hand-in-hand with robust open surgical programs, to offer durable open solutions to younger healthier patients while mitigating risk in older sicker patients by going with a branched or fenestrated device. Despite these advances, clamp time and visceral ischemia persists as a challenge to safe performance of open thoracoabdominal aortic surgery. Even a straightforward group IV requires the surgeon to be swift. Time on an thoracic aortic clamp results in visceral ischemia with a predictable response of coagulopathy, acidosis, systemic inflammation, and renal insufficiency. Adding cardiopulmonary bypass mitigates some things (distal ischemia, normothermia, hypertension) but brings on other complexities (cannulation, circuitry, coagulopathy). Sewing to a Carrel patch allows one to perform one large anastomosis rather than four individual ones, gaining speed and time, but compromises by leaving aneurysmal tissue which could progress to a troublesome patch aneurysm. TAAA is a condition that demands referral to high volume centers. It is in high volume centers that these apex predator surgical conditions can be subdued. It is in these centers that branched/fenestrated stent graft programs can offer treatment for patients high risk for open repair. It is in these centers that patients can avoid compromises such as snorkels and chimneys. Unfortunately, these centers are long air flights away and the means of the patients may not match the desires. Out here in Abu Dhabi, half a world away from Cleveland, Rochester, Houston, Boston, Chapel Hill, New York, and Seattle, and over six hours from major centers in Europe, we usually have to find our own way. Thankfully, we have the resources in experienced staff and abundant materiel.
During my time at the main campus of Cleveland Clinic, I came to appreciate the hospital as a highly evolved tool for healing, but for open repair of TAAA, it still falls on the operating surgeon and the choices made that shaped the outcome. In this most invasive of operations, simplicity and efficiency translating to speed offers the only consistent path to success. My partner, Dr. Houssam Younes, who trained in Houston, mentioned that Dr. Joseph Coselli, has clamp times approaching 30 minutes for group II TAAA -an almost inhuman speed achieved by doing these cases every day. For this reason, stent grafts are popular because repair of aortic aneurysms can be achieved by more practitioners in widely distributed settings. Because of the marketing of all things minimally being better, patients come asking for endovascular.
Case
The patient is a fifty-something smoker who had a prior type B aortic dissection nearly a decade past who presented with substernal chest pain radiating to the back. He was found on CTA (figure below) to have a 6.5cm extant V TAAA starting above the diaphragm and ending at the level of the renal arteries.
Closer inspection revealed it to be aneurysmal degeneration of the aorta at a large false lumen fenestration. The aneurysm had grown eccentrically into the patient’s right chest and retroperitoneum. The remaining dissection above to the left subclavian artery and to the aortic bifurcation was chronic and thrombosed. His pain waxed and waned with hypertension which initially had to be controlled with parenteral agents. His cardiac workup revealed normal ejection fraction and valve function, and no critical coronary artery disease on coronary CTA. Pulmonary consultation deemed him a low pulmonary risk for major surgery. I offered him open repair, and initially the patient balked, asking for an endovascular repair, but I carefully walked him through the concepts, principles, and data guiding my recommendation. Yes, in a rupture, I have stented and followed with visceral debranching (link) and we have placed multiple snorkels in a very high risk octogenarian with a rupture, but who would offer endovascular repair to an otherwise good risk 50 year old?
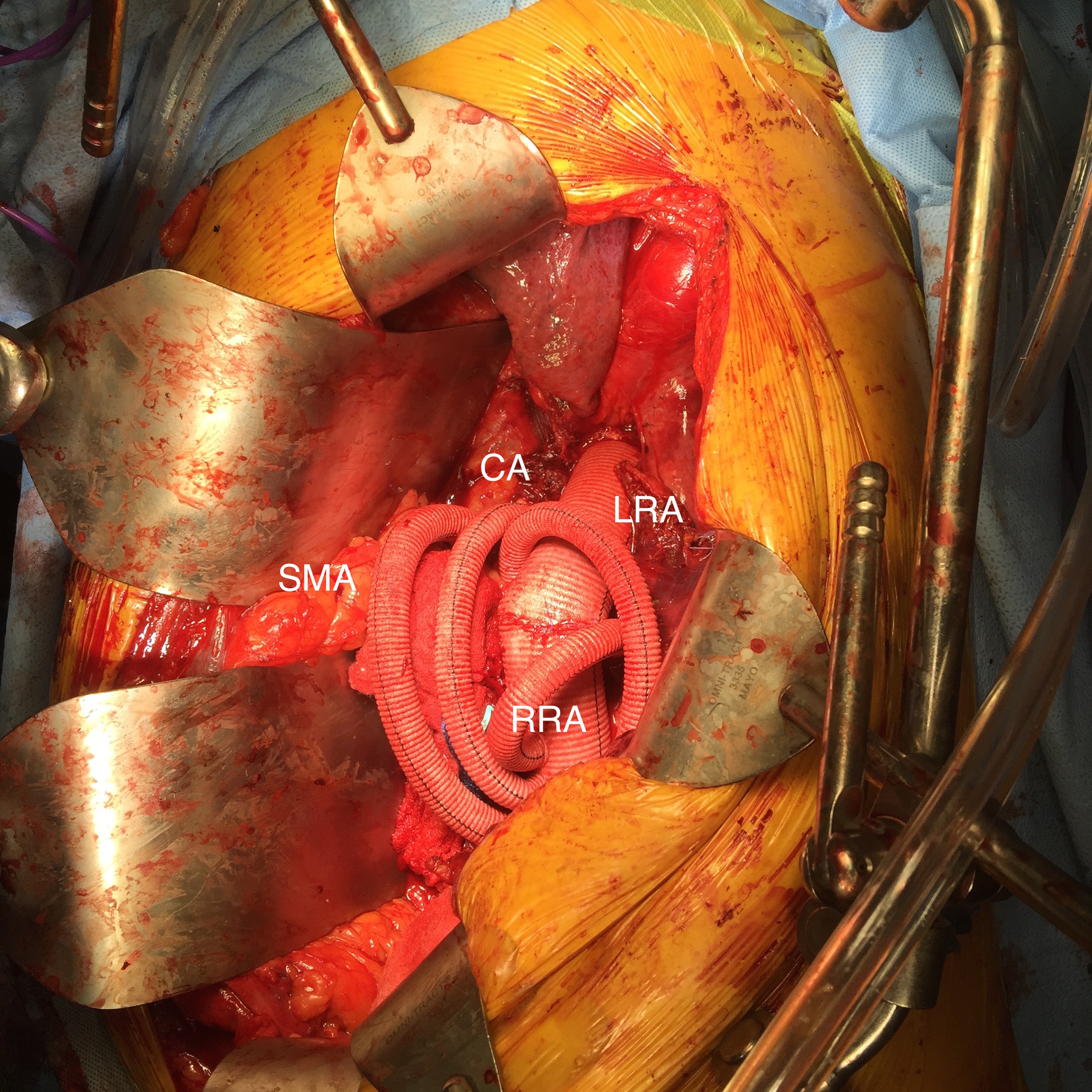
The operation was initially planned in the standard way with cell salvage, plan for clamping in the transition point where the descending thoracic aorta took a rightward turn. The sequence of operation was for proximal anastomosis, right renal anastomosis, cooling the left kidney, celiac axis (CA), superior mesenteric artery (SMA), left kidney, and finally distal anastomosis with reimplantation of any prominent intercostal vessels. Preop imaging suggested the one at the T12 level was large. CT surgery was asked to be available for cardiopulmonary bypass via left atrium and femoral vein. Cardiac anesthesia and I had a discussion about intraoperative monitoring and management. Plans were made for CSF drainage -despite recent papers suggesting as much harm as benefit from these drains, I still feel critical time is lost if the patient is ventilated for a prolonged period postop and motor evoked potential monitoring is not available. The culture of CCAD mirrors that of Cleveland Clinic’s main campus in Ohio, and collaboration is ingrained. It was also serendipitous that one of the clinical associates, Dr. Niranjan Hiremath, had a particular interest and training in aortic surgery and suggested something amazing.
The Game is Changed
Dr. Hiremath trained in both vascular surgery and cardiothoracic surgery in Melbourne under Dr. Matalanis. Drs. Matalanis and Ch’ng published a series of 5 patients done with a separate branched bypass to the visceral vessels fed from the cardiopulmonary bypass circuit (reference). A separate aortic bypass was then performed and this truncal visceral graft was anastomosed to the main aortic graft. It was a visceral branch application of what is commonly done for the aortic arch great vessels. It was clear to me that this concept eliminated the need for desperate speed, and minimized clamp time to the 5-15 minutes required for each visceral branch anastomosis. A game changer.
My process for incorporating new concepts to an operation requires comfort and familiarity. The familiarity with this modification had everything to do with my extensive use of shunts during peripheral bypass surgery. Placing the shunt into one of the renal branches of a 4 branch Coselli graft turns this graft into a live blood vessel. By fixing the proximal and distal ends of the graft in the correct orientation and position relative to the branches, each of the visceral branches could be anastomosed to the graft one at a time while the patient’s aorta remained unclamped. This is best described with the sketches I put together for the preop huddle (gif and figure below).
Even though I have done many of these operations, because of the smaller population at risk, thoracoabdominal aortic aneurysms are a relatively low frequency disease and no assumptions can be made. The fact was, it took very little convincing for me to understand this concept as a game changer, but I took the liberty of modifying it for the particular situation of the patient. Every operation is ultimately another quantum of experience for the people involved to take away priceless information for the next one which will always be unique. We must take these as opportunities for improvement. For once in a long time, I felt this would be a big improvement.
Day of Surgery
Our operations always start with a huddle, but this one was different because of the numbers of people involved. There were the cardiac anesthesiologists, some of the best I have ever worked with in my career led by Dr. Dominique Prudhomme. The cardiac surgeons, Dr. Tareq Aleneiti and Hiremath, who planted this idea, along with the perfusion team, cardiovascular nursing team, and my partner Dr. Younes walked through the steps of the operation with me, with bailout points and plans B and C (CPB with hypothermia and circulatory arrest as a last resort for any unforeseen uncontrollable bleeding). I felt like I was the ringleader in a heist movie, only in this case, rather than jewels, we were grabbing something actually priceless (figure 3).
The patient was placed in the right lateral decubitus position across the table break in the golf backswing position with pelvis relatively flat to the shoulders which were upright. The incision extended from the top of the sixth rib into the abdomen. This dissection is really two -the thoracotomy and separation of the peritoneum from the retroperitoneum linked by the takedown of the diaphragm and cutting of the costal margin. It is a tactile portion of the operation -only the hands really understand when to pull down and separate the two layers. The celiac and SMA are entangled in myenteric plexus which had to be cut to exposure sewable lengths of both. The left renal artery was also tricky in that the prior inflammation of the dissection resulted in stickiness of the tissues. It goes quickly and we have this exposure (figure 4).
Heparinized
The patient is heparinized with a goal ACT around 250. Not enough for CPB, but good enough for rock and roll. The cardiac surgeons placed a cannula within a double ring of advential sutures, cinched with Rummel tourniquets and secured with an 0 silk tie -a maneuver I did many times myself during my cardiac rotations in residency. This was placed on a Y connector, one branch going to the CPB pump in case of a need to go to plan C, and the other to a tubing connector inserted into the right renal artery branch of the Coselli graft -a slight modification of the original plan (figure 5).
The other branches were simply clamped and the aortic ends of the graft were rolled up with a straight Kelly and secondarily clamped with aortic clamps -this gave weight to the ends letting them be positioned in a way that kept the branches oriented properly. There is need for precision and prediction as everything rotates back 45-90 degrees and the viscera sit on the grafts and the anastomoses. That is why keeping some length is crucial -this length accommodates this rotation. The Coselli graft is opened to systemic pressure by releasing the shunt. The proximal and distal ends of the main graft are twisted and double clamped to position the graft branches in the correct radial and z-axis orientation.
The aortic and branch exposure with takedown of the diaphragm is a standard exposure. One technical difference for this procedure is the need to expose about 2cm of the CA and SMA. Typically, only enough to clamp the vessel is necessary in standard surgery as these vessels are prepared with aortic buttons or anastomosed as an island patch. These vessels are surrounded by myenteric nerve plexus which feels like fascia or scar tissue but can be divide. Use of a hook cautery typically used in laparoscopic surgery along with a Ligasure speeds dissection.
These arteries, starting with the left renal artery, are ligated at the origin and divided for end to end anastomoses to the Coselli graft branches. As these arteries are only briefly clamped for the anastomosis while the remainder are getting flow from the aorta or the shunted Coselli graft, visceral ischemia is minimized. I still chilled the kidneys with manual injections of cold Ringer’s Lactate via large syringes and Stoney injector tips. The final product is shown on figure 6.
The operation no longer felt like a sprint. The atmosphere was lively and relaxed -something that does not happen in these cases even at closing as exhausted residents or fellows focus on stitching together all the separated layers of the patient’s chest and abdomen. I played a soundtrack of classic Bollywood tracks, alternating between mellow and lively.
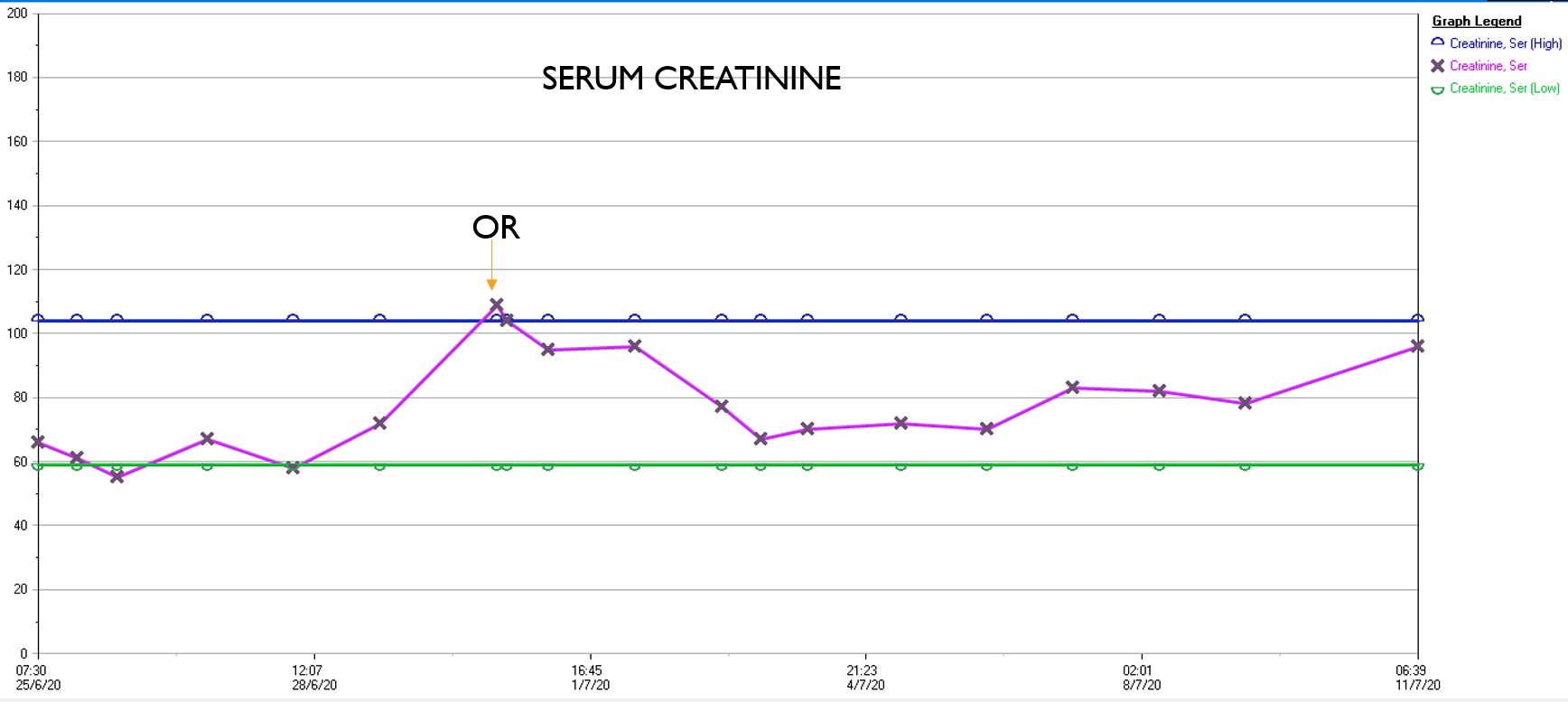
What was striking was the absence of the need for blood transfusion -about a liter and half ended up in the cell saver, and the patient received 2 units of plasma, out of tradition. The patient had a minimal brief plasma lactate elevation which did not persist. He was closed with a chest tube and brought to the cardiac intensive care unit, stable, not on pressors. He was extubated that night, and moved all of his limbs to command. The chest tube was removed on POD#2, and he left the unit to recuperate on the floor. Amazingly, his serum creatinine did not rise significantly. Prior to clamping he received the usual cocktail of mannitol but it was likely unnecessary. Most of these patients, even with revascularizing first after the proximal aortic anastomosis in the fastest of hands, there is at least 30 minutes of ischemia manifest postoperatively as a rise in the creatinine with recovery in most. This rise was brief and transient (graph).
In the visceral circulation, the ischemia in the normal open repair is manifest postoperatively as systemic inflammation requiring pressors, persistent lactic acidosis, and coagulopathy, which at best is transient but at worst, fatal. This patient had no significant shift in any of these parameters. He had his CSF drain removed POD#2 after clamping for 24 hours, and was discharged home POD#11, having to recover from right chest atelectasis and a blood patch placed for persistent headache. CTA prior to discharge showed a good result. The left renal graft had been on stretch but was rendered redundant on repositioning of the viscera. No stenoses were noted.
Aftermath
Of course we are writing this case up, but case reports by their form cannot be overly enthusiastic whereas on my personal blog I can be excited. The normal course of postoperative recovery, the ebb and flow taught in surgical critical care books, is a result of ischemia, blood loss and replacement, fluid resuscitation, and cardiopulmonary support. Add to that cardiopulmonary bypass and you get an additional hurdle for the patient to recover from. This technique of shunting reminds me most of the temporary axillofemoral bypass. When I was a fellow at Mayo, I assisted Audra Noel in taking an elderly patient with a 25% ejection fraction through open aortic surgery with nearly miraculous recovery largely by avoiding the factors that trigger the ebb and flow. This technique is easier but mandates a strong normal segment of thoracic aorta to serve as inflow, otherwise an axillary artery will need to be cannulated.
Spinal cord protection is made easier with this technique by avoiding the massive fluid shifts, the pressors, and the acidosis in a typical thoracoabdominal aortic aneurysm repair. The blood pressure and cardiac output were never seriously perturbed. Several large intercostals and lumbar arteries were encountered and they backbled so avidly, after the short operation that I really felt there was no need to revascularize them. The spinal drain was kept open only for a day, and kept another day clamped to ensure that it would not be needed before removing it.
If you accept that spinal cord ischemia is multifactorial, we had avoided those factors. The absence of massive blood loss, negligible pressor use, no fluid shifts, minimal ischemia, no significant acidosis, no prolonged OR and clamp times, no blood transfusions, and the presence of avid back bleeding suggesting strong collateralization, compelled me to end the operation without revascularizing these intercostal vessels.
The patient recuperated for an ten days after his operation but was walking from postoperative day #1. He had atelectasis due to mucus plugging in his right lung base and was treated for aspiration, but clinically did not have a pneumonia and his atelectasis cleared with chest physiotherapy and nebulizers and was discharged home. Gratefully, he has given us permission to discuss and study his case.
There is no success in these cases without a team, and we are blessed with talented caregivers. This technique greatly reduces the physiologic impact of this surgery on the patient, reducing the injury to the equivalent of a broad sword cut from chest to abdomen that missed all the vital organs and vessels. In the right hands, this concept will broaden the appeal of open repair of these challenging aneurysms.
Reference
Matalanis G, Ch’ng SL. Semin Thoracic Surg 31:8:708-12.
The patient is an active man in his 60’s with a history of hypertension who had known about a right common iliac artery aneurysm for several years and had come for an opinion. He was asymptomatic of pain. He had a prior splenic artery aneurysm embolization about a decade prior to presentation.. CT scan showed a large eccentric aneurysm arising from a retrograde chronic dissection dilating the right common iliac artery to over 4cm. This is typically iatrogenic, but impossible to know for sure. The left common iliac artery was ectatic to 2cm as was the aorta to 3 cm and all were “wavy.” This sort of tortuosity is the result of remodeling in the axis of flow resulting in lengthening of the artery and is found in those with the substrate for aneurysmal degeneration (footnote). He did not smoke and he could climb stairs without dyspnea or chest pain.
On examination, he was a fit middle aged man with a slight paunch. His abdomen was soft and his peripheral pulses were present and normal. Laboratory results were normal, including creatinine. EKG and echocardiogram were also normal.Treatment options were discussed in detail. The patient was paying for the operation himself and wanted to understand in detail the possible options. These included
1. Open aortobi-iliac bypass with a jump bypass to the right internal iliac artery
2. Open aortobi-iliac bypass with ligation of right internal iliac artery
3. EVAR with right external iliac extension after embolization of right internal iliac artery
4. EVAR with parallel grafts to right external and internal iliac artery (off label)
5. EVAR with iliac branched graft to right internal and external iliac artery (off label)
People are known to react with emotions and to decide typically for near term gain over far term benefits. The offer of an operation involving laparotomy and a possible weeklong hospitalization with all the attendant risks of death, heart attack, stroke, ileus, wound infection, pneumonia, organ failure and so on provides a stark contrast to the appeal of endovascular repair which can be done percutaneously, with local anesthesia, and with a short hospital stay. The lifelong CT scans are in the murky future compared to the present which is sharply in focus. This is why few people save for retirement, why profligate grasshoppers far outnumber industrious ants. In the same vein, the offer of an “advanced minimally invasive” solution plays to several cognitive biases that exists in the mind of not only the patient but the health-care provider. These include this preference for short term gain over long term gain, but also viewing all innovation as being necessarily better than what was available.
After going over the operation in great detail, the patient cut me off when I mentioned the need for lifelong followup CT scanning. Because he lives in several countries, typically, he has to pay for his healthcare out of pocket and he balked at the notion of paying for an annual CT scan. He was also disdainful of the possibility of reintervention (quoted at 10%) and having to pay for it. Also, the stent grafts, which he would have to pay for, end up being as costly as a new luxury sedan based on local pricing.
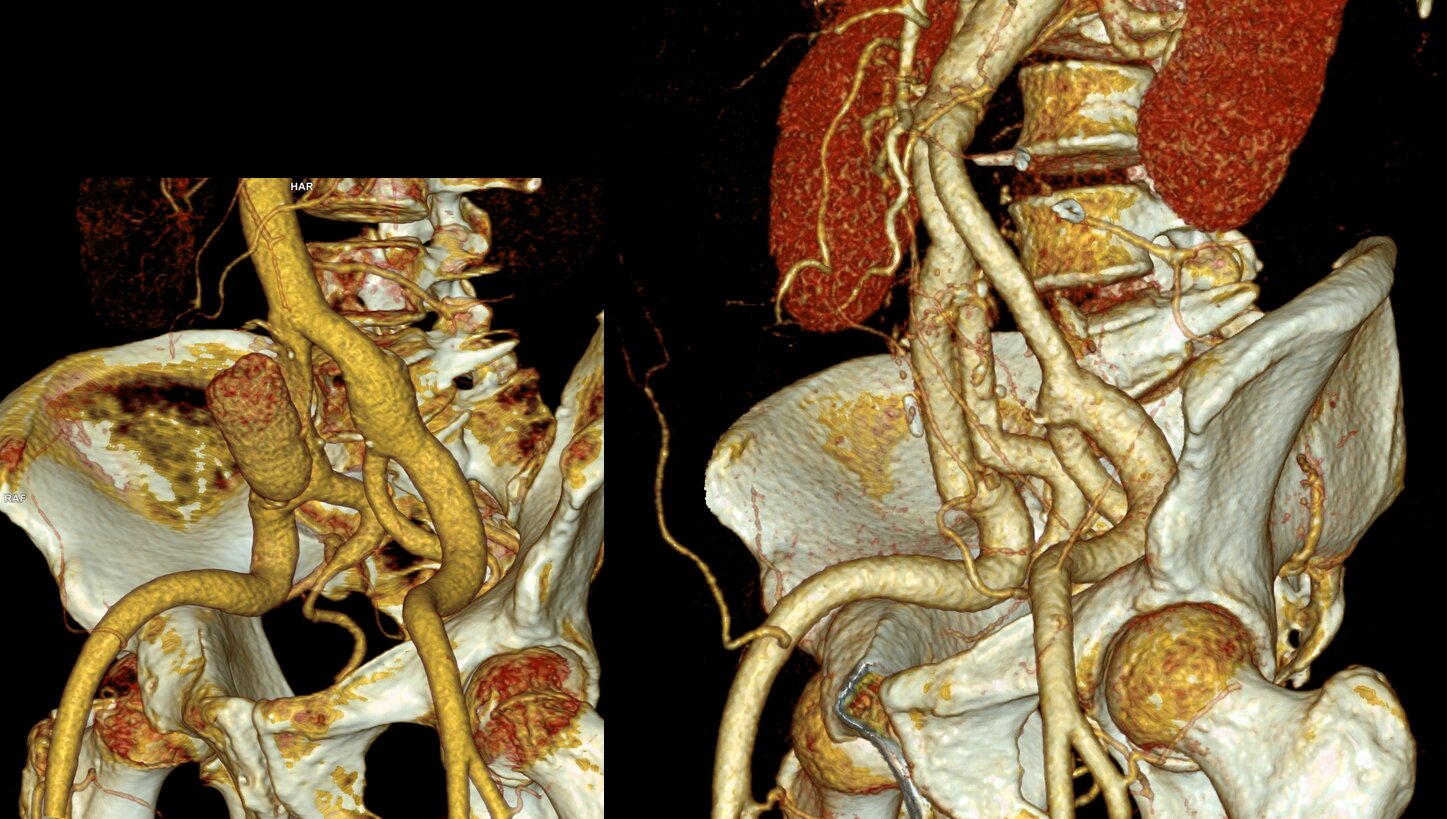
We chose open surgical repair via a midline laparotomy. An aortobi-iliac bypass was performed from proximal aorta to right internal iliac artery and left common iliac artery bifurcation with a jump bypass from the right graft branch to the right external iliac artery. Technically, this sequence was chosen for ease of access to the internal iliac artery with the external clear of graft. Operative time was 3 hours. He was in the ICU for one night. He went home after 10 days after contracting a UTI. In followup three weeks after discharge, because he had fevers, a CT scan was performed (figure). He was treated for an upper respiratory infection which cleared, and he has been doing well since. We are both happy that he will never need a followup CT scan.
Before and After
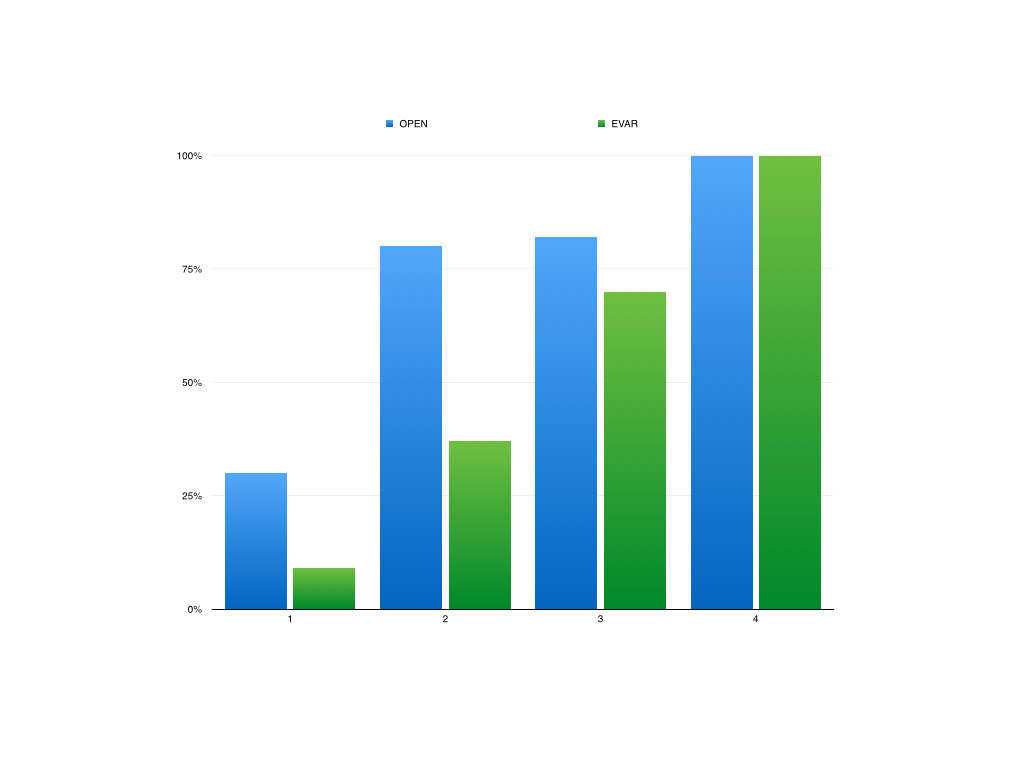
The literature supports this stance. The long term followup of the EVAR-1 Trial (Reference 1) is an example. This was the late followup of the prospective randomized study looking at open surgery versus EVAR in 1252 patients. The initial EVAR 1 findings are well known and put into question the long term benefits of EVAR as the initial mortality benefit of EVAR is lost within a few years of treatment. At a mean of 12.7 years of followup, there were more deaths from aortic aneurysm rupture and aneurysm related death in the EVAR group compared OPEN surgery (adjusted HR 5.82, p=.0064), with 13 AAA ruptures. I have mentioned before that the failure of a handful of pacemakers drove the Guidant company to recall over 20,000 of their devices. Plus, the cost of annual CT scans in the treatment group and cost of devices and cost of reintervention have driven the UK’s NICE Guidelines recommending against EVAR in elective AAA repair. The meta-analysis of EVAR-1, DREAM, OVER, and ACE trials comprising 2783 patients is confirmatory, that aneurysm related mortality was significantly higher after the initial mortality benefit of EVAR fades away, and that patients of marginal fitness gain no advantage from EVAR, particularly those with heart or renal disease, and those with PAD had lower mortality in the period of 6 months to 4 years (reference 2).
I post this case, because despite a complications, in this case UTI and URI, the patient did fine. So why is open aortic surgery considered a dying art? Why is there such pushback against the UK NICE Guidelines?During my residency in the 1990’s, in the heyday of open surgery, I observed a lot of mediocre vascular surgeons and a very few great ones. The average vascular surgeon would take 6-8 hours to perform open aortic surgery, and the patient would come out with a typical picture of oliguria, third spacing, SIRS, that would generate a 1-2 week stay that would even be described as the normal and expected course for AAA repair in surgical and critical care textbooks. The best surgeons back in the day did these operations under 3 hours with 100mL blood loss and the patients would spend a day in the ICU (often not needing it), and 3-7 days in the hospital, but they were the exception.A higher percentage of surgeons today can do EVAR well than surgeons 25 years ago could perform competent open aortic surgery. Most surgeons graduating from training rarely see or do open aortic surgery compared to the multitude of interventions. Capable open surgery basically is not available outside of a few centers, and most surgeons admit to not having equipoise to start a new trial with modern devices. Open aortic surgery is a lost art, like growing your own vegetables, dressing your own game, reading cursive script, and dialing a rotary telephone.
It is not for a lack of desire. I have several younger colleagues I have met or interacted with via social media who have an intense interest in gaining open vascular skills. They have organized open skills courses at major European vascular meetings, but I believe that is not enough.The need for exovascular fellowship, the running topic of conversation of older surgeons through the 2000’s, is never as critical as it is now as we see milennia of surgeon-years of experience retiring to golf courses and cottages. The recommendation for preferring open surgery in the younger and fitter patients is sadly out of reach for most patients and surgeons. The same passion in disseminating endovascular knowledge needs to be applied to repair the damage to vascular education by over-relying on and over-prescribing endovascular approaches.
Finally, and sadly, this patient is the exception. When given clear options and outcomes and costs, this patient made a rational decision, choosing value over convenience.
Pearls for finding AAA:
1. Tortuosity of the internal carotid arteries including loops and hairpin turns found in patients particularly smokers implies the present of a AAA until proved otherwise
2. Palpating bounding popliteal or pedal pulses in an older smoker implies the presence of a AAA until proved otherwise. Especially if the medical student can feel these pulses.
3. African-American Females with Diabetes almost never get AAA.
4. Palpate their abdomen
View out of my balcony, sometimes you need many pieces to assemble a beautiful whole
Innovating Our Way Out of Not Having Enough Vascular Surgeons
This year’s SVS meeting featured a sobering assessment about the vascular manpower deficit affecting North America at the E. Stanley Crawford Critical Issues Forum, moderated by Dr. Michel Makaroun, MD, president-elect of the SVS. 35-45% of practicing vascular surgeons plan on retiring in the next decade by conservative estimates. We are not attracting enough candidates for the training programs. The solutions, including decreasing the length of training, public relations campaigns, and incentivizing retention have had mixed results, but we have yet to see a sustainable rise in vascular surgeon numbers.
Burnout driven by lack of work-life balance, the advent of electronic medical records optimized for billing, the passing of the private practice era, and the constant need to adapt to new techniques, create a persistent downdraft on staffing. So as some hospital face the reality of having to contract services, little attention is given to delivering best care with the staffing that we have. Changing how we practice is the only viable solution.
There are an estimated 3000 active vascular surgeons in the US. Imagine if all the cheese needs of this country could only be met by 3000 artisanal cheesemakers who make cheeses one at a time and want to live in places with international airports, BMW dealerships, and major league sports teams, and must have 3-4 partners to share cheese call. If you are a rural hospital in dire need of vascular surgery services and your one vascular surgeon is retiring, you are probably SOL.
When I was training, vascular surgery was oft touted as a primary care specialty. And that is how many of us still practice, managing risk factors, monitoring mild disease, as well as planning and performing interventions and operations. As much as I enjoy that kind of interaction, the half hour to an hour visit for a head to toe cardiovascular survey and discussion, educating patients and families about pipes and pumps, is incredibly inefficient. A healthcare system, a hospital, facing a staffing shortfall, has to do everything possible keep that vascular surgeon in the OR during work hours.
What is the core function of a vascular surgeon? Making good decisions and executing plans well. Decisions require data. What is this data? We laud the history and physical examination, but this is a throwback to another era. If you look at the diagnosis of myocardial infarction, it is not standard practice for a cardiologist to come and get a history, examine the patient, and declare that the patient is having a heart attack based solely on history and physical examination. It is a triage nurse in the ED who draws labs and orders an EKG which is read by a machine. These data points will tell you if heart muscle is being damaged. A process is started which triggers a team to come and take care of this patient. The hospitals focused on this actually drill their cath lab teams like pit crews. A stopwatch starts with the goal of revascularization under an hour.
Not so with peripheral vascular disease. The ischemic foot might have only a few hours depending on its presentation before it is irretrievably lost, but no matter -they sit in the ED until a vascular surgeon comes to speak to the patient and family, examine them, and then order tests, admission, consults, and operating room -typically all by themselves. Getting these patients into the operating room is in many places hampered by the lack of dedicated OR staffing, radiology techs, anesthesiologists, space, equipment, and critical care capacity. During work hours, there are scheduled cases that have to be delayed or canceled for another time, which takes time to do. After hours, the patient may have too many comorbidities to handle safely with the available staff. The vascular surgeon may have to bargain and cajole, to align several factions whose attention is demanded by many equally important concerns. If you decide to hold a lavish dinner party of twenty important guests -reserving space, calling caterers, inviting guests, arranging transportation – on short notice, you might pull it off once, but if you do this regularly, you are a masochist of the first order.
In the heart attack model, the history and physical examination is relegated to a series of yes/no or how long questions, and positive responses trigger a series of coordinated actions of a system -a reflex. In the leg attack model, there is no such system. I have to blame the vascular surgeons for preserving the current model. Vascular surgeons are organized as a guild. Guilds are protective of their monopolies on skills and markets and fiercely resist change. Most vascular surgeons are terrified by loss of control, and cling to the notion of being misunderstood and unappreciated saviors. We can do better.
The area that needs streamlining is at the point of referral. The majority of time of a vascular surgeon is spent working up normal blood vessels, varicose and spider veins, leg edema and pain, and mild and moderate arterial atherosclerosis. This work initially does not require a vascular surgeon but rather a focused set of policies and initial diagnostic studies that can be administered or ordered by any caregiver. Reducing the need for vascular surgeons at this point in vascular care will go a long way in extending the vascular work force at hand.
Point of Care Blood Flow Evaluation
Finding and declaring blood vessels to be normal is challenging and too often time consuming. Streamlining this will go a long way in freeing vascular surgeons to take care of disease.
The average caregiver is an inconsistent pulse taker. The palpable pulses are not always easy to find. Asking over the phone or as policy for someone to examine pedal pulses -the posterior tibial artery and dorsalis pedis artery pulses, is challenging. A positive is just as likely to be true or false as a negative. No cardiologist would ask a similarly detailed and technical question about an MI. In fact, they can’t ask, “Is there a pulse in the LAD?” Cardiologists make do with tests easy to obtain and interpret with certainty -the plasma troponin level and the EKG. The EKG is read by an algorithm so established and so tested, that it should stand as an example of early machine intelligence taking over a human job -but I digress.
What is our EKG? It is not the ABI -the ankle brachial index, because it is terrible at identifying disease, and is difficult to obtain reliably without practice. The closest thing to an EKG we have in terms of simplicity and accuracy is the pulse volume recording, the PVR (figure below). A FloLab machine, the machine used to obtain PVRs, will basically run itself once the cuffs are correctly applied on the leg, and the tracings are very easy to interpret. Unlike an EKG, there are no electrodes whose locations you must memorize. If the closest vascular surgeon is an hour away by ambulance, the transfer of a patient with flat waveforms and ischemic foot does not require a consultation on site. The patient would go to the vascular surgeon with no time wasted and no kidneys injured by CTA’s that too often fail to travel with the patient. Unlike an EKG which can be performed by many caregivers, a PVR requires both the equipment and a vascular technologist. A vascular technologist is not available 24-7 in most hospitals, and FloLab machines purchased for vascular labs are not meant to be dragged around the hospital.
So let’s think out of the box about another box in every triage nurse’s cell, every ER and ICU bed, and on every hospital nursing floor. These are pulse oximeters with a digital tracing, and bonus points, some come with strip printers! Placing a pulse oximeter probe on the second toe and comparing to an erstwhile normal wave signal such as on an index finger can provide qualitative information about normality and disease. Normal waveforms and abnormal ones can be easily discerned. A flat line is another obvious finding when in comparison, a finger or an ear on the same patient has normal signals.
How much better would a vascular surgeon feel about a transfer call that has this information, “digital waveforms are flat in this patient with rest pain and a bruised toe.” How much better would a vascular surgeon feel about a call about a patient with “digital wave forms are normal in this patient with toe pain and a bruised toe. We got an x-ray and there was a fracture.” The communication can be quite detailed and refined. For example: “The patient had no pulses, we think. Digital wave forms were dampened but pulsatile in a patient with a bruised toe, we’ll send to vascular clinic in the morning.”
A study comparing pulse oximetry signals and ABI in type 2 Diabetes Mellitus found the following results (link).[i]
Method
Sensitivity
Specificity
PPV
NPV
Pulse oximetry
74.1%
95.7%
83.3%
92.7%
ABI
70.3%
87.1%
61.3%
91.0%
These data suggests pulse oximetry signal is equal to and somewhat better than ABI. Why is this important? Cost. This information is better than asking unsure people, “Is there a pulse?” A vascular technologist need not be on call 24/7. Extra FloLabs for ED, ICU, and floors need not be purchased. The pulse oximeter with waveform tracing is nearly ubiquitous wherever patient’s oxygenation needs to be assessed in most hospitals. While not perfect, it has great potential for serving as vascular surgery’s EKG machine for critical limb ischemia. Policies and algorithms can be built out in collaboration with Emergency Departments and nursing departments that can effectively determine if blood flow is normal or abnormal at point of care. Effective emergency responses to critical limb ischemia can be authored triggered by abnormal findings. Acute limb ischemia protocols based on time sensitive responses can be initiated. All of these can flow from referring entities being able to determine objectively normal or abnormal blood flow.
Clinic
The vascular clinic is a sorting process where patients are determined to be normal or have mild, moderate, or severe disease. The vast majority of the time spent in clinic can be spent in triage by trained nurses and testing by technologists. Clear pathways and guidelines can dictate the ordering of vascular laboratory tests obviating the need for vascular consultation at this stage. Patients with normal blood vessels and vascular function are sent back to their physicians with the normal report. Patients with mild disease and moderate disease are sent to a physician with specialization in cardiovascular medicine for management of risk factors and periodic surveillance. At any point in the process, a vascular surgeon can be called to provide guidance and direct patients to different tests and consultations. The patients needing operations, based on correct indications and imaging are sent to a focused clinic where the surgeon and interventional team can review films, determine the urgency of indications balanced against risk, and plan and schedule procedures. Currently, vascular surgeons do all of this by themselves, as well as make hospital rounds, perform procedures, and interpret vascular laboratory studies, seeing one patient at a time.
In introductory computer sciences courses, search algorithms are taught to be brute force if you look at one item at a time for the thing you want, and to be efficient if you have presorted those items because every time you look, you can exclude part of the data set, ever shrinking the pool in which you search, making the search shorter and faster
The shortfalls in vascular surgeon numbers have as much to do with this dependence on the star chef cooking up one meal at a time, rather than a team working off recipes, with the chef directing the flow and occasionally jumping by the fire to make the most difficult of dishes. The first restaurant can seat three parties. The latter, easily ten times the number. Everyone gets fed.
Only asking how many vascular surgeons you need misses the big picture because there are many equally important questions. How many vascular technologists do you need? An accredited laboratory provides the critical diagnostics upon which decisions are made, and the surgeon should oversee but not be directly involved in the initial screening. Nurses trained to triage and order vascular laboratory tests and even perform the simpler ones is the second need. Third, is the cardiovascular medicine physician who manages those patients discovered to have mild to moderate disease, and depending on symptoms, refers severely symptomatic moderate disease and severe disease to a scheduling clinic. The scheduling clinic is composed of both interventionalists and vascular surgeons who plan interventions and operations.
Surgeons must be in the operating room to be effective. A well thought out and organized system, with interlocking teams, and well disseminated basic knowledge and awareness of vascular diseases reduces the need for a vascular surgeon to be present all the time in many places and ultimately increases the effectiveness of the vascular surgeons that are available by keeping them in the operating room. The system needs to be set up by the surgeon to allow clinic to be a setting mostly for consenting the patient for an operation or a discussion of treatment options.
Finally, vascular surgeons must be aligned with all the resources of the hospital including the considerable numbers of interventional cardiologists and radiologists, neurologists, and nephrologists. There is no reason someone should wait a month to get on the OR list for an iliac angioplasty and stent if an equally skilled and privileged cardiologist or radiologist has an opening the next day. The surgeon’s special talent should be open surgery and hybrid surgery -that which mixes open surgery and intervention in optimal measures which is not possible from a purely percutaneous approach. The key is frequent and easy communication between specialities and trust built by being in one shared cardiovascular institute.
Execution
There is a critical need of good operators. The acuity of disease and their solutions demand the continued presence and availability of open surgery. The fact is, many solutions are optimal in a hybrid fashion and for peripheral vascular disease, these options can only be offered via a vascular surgeon trained in both open surgery and peripheral interventions, or in a combined effort of open surgeon and interventionalist. And many disease categories can only be managed by open surgery.
The reality is that silos, economics, and practice patterns prevent this kind of combined effort. Market forces have pushed the training of vascular surgeons forcefully into the interventional realm at the cost of open surgical training. Some of the geographic maldisdribution of vascular surgeons has to do with younger vascular surgeons flocking to established practices where there are senior surgeons more comfortable in opening a belly or chest (or both). The trap they and hospital systems fall into is then allowing these new recruits to become the interventional specialist of that group, relegating the aging open surgeon to a narrow role, and then finding that the hospital has a problem when that surgeon announces retirement at 60. Every year, millennia of surgical experience retires to beaches and golf courses. The hospital systems should recognize this brain drain as a crisis and create work arounds that keep these skills going. The other opportunity lost is close coordination with interventional cardiologists, radiologists, and nephrologists who in many cases compete with vascular surgeons for the same patients but treat the patients based on their training and skill sets to the exclusion of potentially better operations offered by surgeons. This disjointed care creates both suboptimal outcomes for patients and high costs for hospital systems.
Commerce should never dictate the fate of a patient. A particular point is where competencies and privileging overlap, and guidelines recommend intervention over surgery as in the case of a TASC A or B iliac artery lesion. A patient should not be kept waiting weeks for a spot on a busy surgeon’s OR schedule when an open interventional cardiologist or radiologist slot is available for a iliac stent the next day. It should be a matter of practice that these cases are discussed and distributed, optimally in a shared indication clinic or rounds. Patients bumped off of a surgeon’s elective schedules for emergencies who could be cared for by an interventional partner without an added delay should be given that option. This kind of change requires a commitment to continual reorganization and optimization into a vascular institute.
Conclusion
The perfect vascular surgeon is a unicorn -well skilled, and experienced in open vascular surgery, but also versatile, innovative, and skillful in wielding a wire. I can name just a handful of unicorns. An apt analogy from the book Moneyball is the signing of superstars in baseball on the free agent market. The upshot of that book is that you can arbitrage for the valued metrics through signing several utility players with an aptitude for one thing or another which in sum equals or exceeds that superstar and get the final result -wins, in the same proportions as overspending on a superstar. Rather than searching for that unicorn, it is more important to set up the right system. Screening, testing, and management of mild vascular disease by a nurses and cardiovascular medicine physicians, while directing operations and interventions to vascular surgeons, cardiologists, and interventional radiologists should be the next step in the evolution of vascular care systems. There will never be enough vascular surgeons in the current system. The critical and rare competency is open vascular surgical skill. A surgeon who performs only interventions is not an “advanced minimally invasive practitioner” but rather someone equally privileged as an interventional cardiologist or radiologist, and therefore easily replaceable by an interventional cardiologist or radiologist specializing in peripheral vascular disease. A surgeon skilled in open vascular surgery is becoming rarer every year, but they are still out there, looking at brochures of real estate in sunny places. A team consisting of a cardiovascular medicine physician, many vascular technologists, nurses specializing in vascular diseases, several interventionalists, and a vascular surgeon skilled in open vascular surgery working as a single unit, is far more easy to assemble than finding and recruiting a herd of unicorns.
Drs. Roy Miler and Xiao Yi Teng performing anastomosis on open coversion of an aortic stent graft, now graduated and in practice. A significant part of their open aortic experience is in addressing failing stent grafts.
I recently had to remove a stent graft for infection and got to thinking about how the number of people who could comfortably and confidently manage that has thinned out in the world through the unintended consequence of the medical device market place. In every surgical specialty over the past twenty years, many open procedures were replaced with a minimally invasive option which generally involved adoption of new technology and large costs to the hospital. These newer procedures were touted as easier on the patient while being easier to perform for the average physician than the open procedure that they were replacing. That was the other selling point -that one could do several of these operations in the time it took one open procedure. In most cases, they were at best almost as good as the open procedure but at higher cost.
In the marketplace, minimally invasive always wins. In many specialties it became untenable to practice without marketing these “advanced minimally invasive” skills. Hence, the wide adoption of robotics in urology outside major academic centers -during those years of rapid adoption the surgeons would get flown to a course, work on an animal model, then for their first case a proctor would be flown out and voila -a minimally invasive specialist is born. The problem comes when learning these skills displaces the learning of traditional open surgical skills. In general surgery, it is not uncommon to hear of residents graduating without having ever having done an open cholecystectomy. It is also the case that many vascular trainees graduate with but a few if any open aortic cases. What happens when minimally invasive options run out? Who will do my carotid endarterectomy or open AAA repair?
The first case is an elderly man with an enlarging AAA sac despite having had EVAR about seven years prior. No endoleak was demonstrated but the proximal seal was short on CT. Also, it was a first generation graft which is prone to “peek a boo” endoleaks from graft junctions and stent anchoring sutures. On that last point, I use the analogy of a patio umbrella -after seven seasons, they can leak where cloth is sewn to the metal struts. It is very hard to demonstrate leak of this kind on CTA or duplex ultrasound because they are small. The patient had his EVAR because he was considered high risk for open repair at the time of his operation -moderate COPD, mild cardiac dysfunction. His sac had enlarged to over 6cm in a short time, and therefore open conversion was undertaken. No clinical signs of infection were present. A retroperitoneal approach was undertaken. After clamps were positioned, the sac was opened.
The picture does not show it, but a leak from the posterior proximal seal zone was seen with clamp off. The clamp was reapplied and the graft transected flush to the aortic neck. A bifurcated graft was sewn to this neck incorporating the main body stent graft and aortic neck in a generous running suture. The left iliac limb came out well and the new graft limb sewn to the iliac orifice, the right iliac limb was harder to clamp and therefore I clamped the stent graft and sewed the open graft to the stent graft.
The patient recovered well and went home within the week. He was relieved at no longer needing annual CT scans.
Who needs annual CT scans? Patients with metastatic cancer in remission.
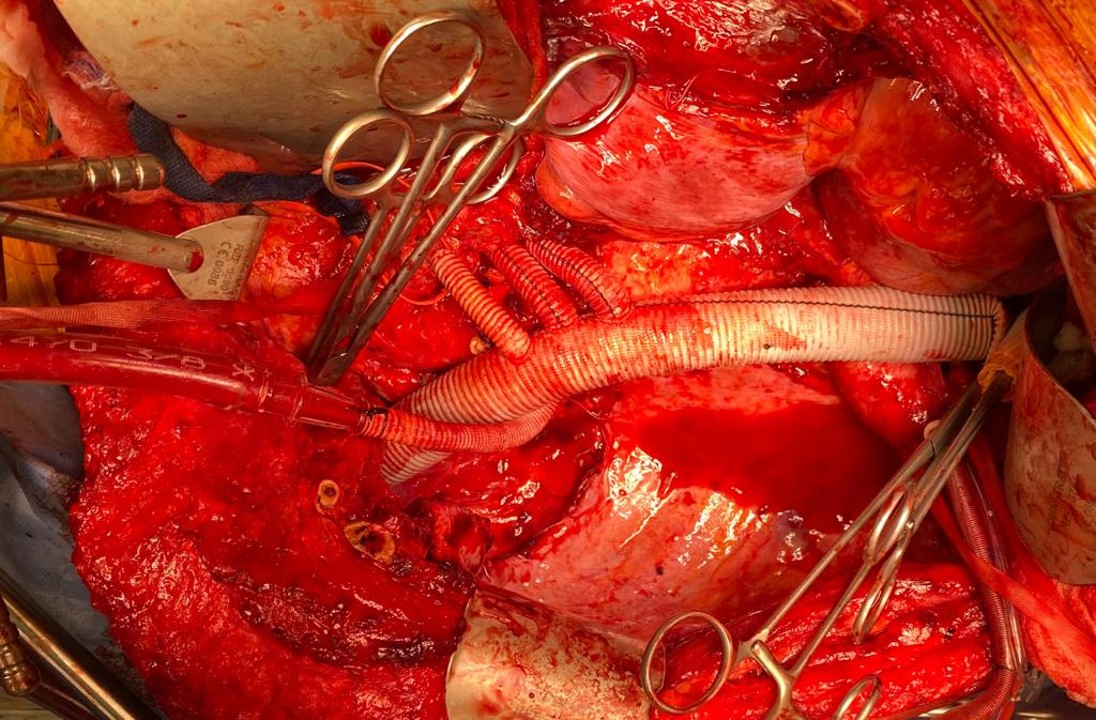
The second patient was an older man referred for enlarging AAA sac without visible endoleak. The aneurysm had grown over 7cm and was causing discomfort with bending forward. He too had been deemed high risk for open repair prior to his EVAR. If he had had an early generation Excluder graft, the possibility of ultrafiltration would be more likely and relining the graft would be reasonable (link). This was again a cloth and metal stent graft which can develop intermittent bleeding from graft to stent sutures, and I don’t think relining will help.
The patient was taken for open repair (above), and on opening the AAA sac, bleeding could be seen coming from the flow divider. It stopped with pressure, but I replaced the graft in a limited fashion from the neck to the iliac limbs as in the first case. This patient did very well and was discharged home under a week.
The third patient was another fellow referred from outside who had an EVAR for a very short and angulated neck, and a secondary procedure with an aortic extension in an attempt to seal the leak had been done. This failed to seal the type Ia leak. This patient too was deemed too high risk for open surgery of what was basically a juxtarenal AAA with very tortuous anatomy.
The patient was taken for open repair, and the stent grafts slid out easily (below).
A tube graft was sewn to the short aortic neck and distally anastomosed to the main body of the stent graft -with pledgets because of the thin PTFE graft material in this particular graft. This patient did well and went home within a week.
All three cases are patients who were deemed originally too high risk for open repair, who underwent EVAR, then underwent explantation of their failing stent graft. Only one involved a patient whose graft was placed off the IFU (short angled neck), but the rationale was that he was too high risk.
What is high risk? In non-ruptured, non-infected explantation of failing stent graft, the mortality is 3% (ref 2) from an earlier series from Cleveland Clinic. With stent graft infection, the 30-day mortality of surgical management from a multi-institutional series was 11% (ref 3) when there was no rupture. From a Mayo Clinic series, stent graft resection for infection came with a 4% 30-day mortality (ref 4). These were nominally all high risk patients at the time of the original EVAR.
Real world risk is a range at the intersection of patient risk and the expertise of the operating room, critical care, and hospital floor teams. The constant factor is the surgeon.
Endografts for AAA disease (EVAR, endovascular aortic aneurysm repair), makes simple work of a traditionally complex operation, the open aortic aneurysm repair. The issue has been the cost and risks of long term followup as well as endograft failure and aneurysm rupture. The Instructions For Use on these devices recommend a preop, a followup 1 month, 6 month, and 12 month CTA (with contrast) and annual followup with CTA for life. These devices were meant to treat high risk patients but high risk patients with limited life spans do not benefit from EVAR (ref 1, EVAR-2 Trial). These have lead the NHS in the UK to propose that EVAR has no role in the elective repair of abdominal aortic aneurysms in their draft proposal for the NICE guidelines for management of AAA (link). While this is a critical discussion, it is a discussion that is coming at least ten years too late. A generation of surgeons have been brought up with endovascular repair, and to suddenly announce that they must become DeBakey’s, Wiley’s, Imperato’s, and Rutherford’s is wishful thinking at best or wilful rationing of services at worst.
In 2006, Guidant pacemakers were recalled because of a 1000 cases of possible capacitor failure out of 28,000 implants for a failure rate of 3.7% -there were 2 deaths for a fatality rate of 0.00007%. EVAR-1 Trial’s 8 year result (ref 5) reported 16 aneurysm related deaths out of 339 patients (1.3%) in the EVAR group compared to 3 aneurysm related deaths out of 333 patients (0.2%) in the OPEN group.
Academic medical centers, behemoths though they are, serve a critical function in that they are critical repositories of human capital. The elders of vascular surgery, that first and second generation of surgeons who trained and received board certification, are still there and serving a vital role in preserving open aortic surgery. My generation -the ones who trained in both open and endovascular, are still here, but market forces have pushed many of my colleagues into becoming pure endovascularists. The younger generation recognizes this and last year, I sat in on an open surgical technique course at the ESVS meeting in Lyons organized by Dr. Fernando Gallardo and colleagues. It was fully attended and wonderfully proctored by master surgeons. This is of critical importance and not a trivial matter. As in the 2000’s when endovascular training was offered as a postgraduate fellowship in centers of excellence, there is no doubt in my mind that today, exovascular fellowships need to be considered and planned and that current training must reinvigorate and reincorporate their open surgical components.
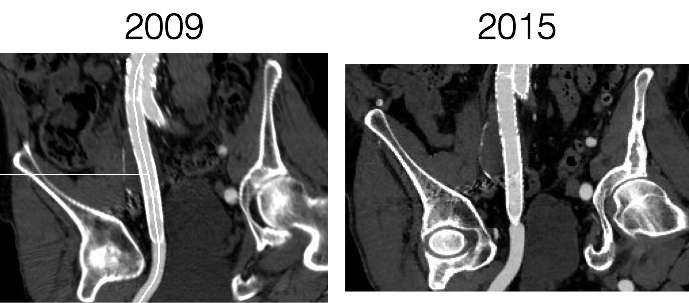
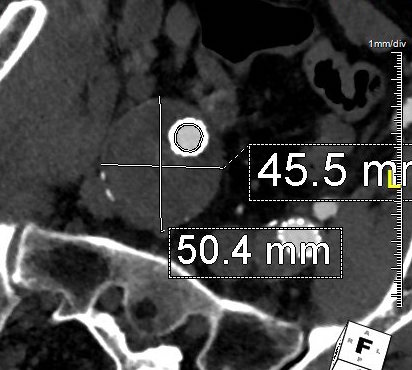
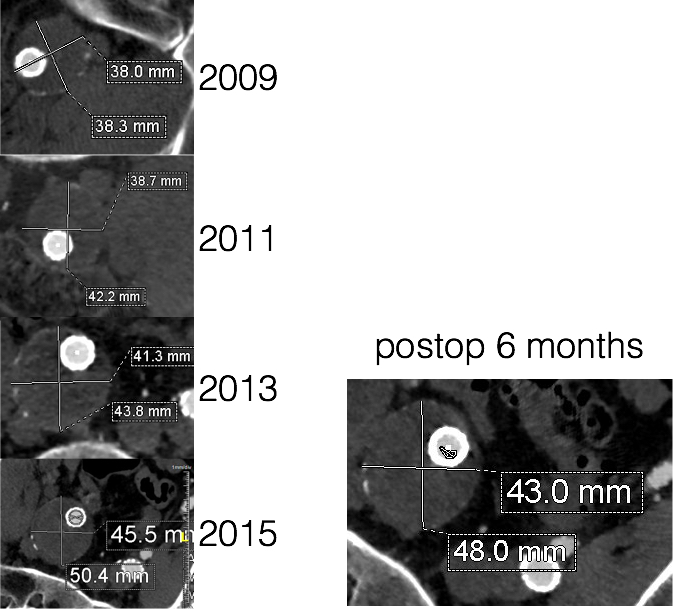
The patient had undergone EVAR for bilateral common iliac artery aneurysm with the original Gore Excluder stent graft a dozen years before with coil embolization and extension to the external iliac on the larger side and femoral to internal iliac artery bypass on the other side. A coagulopathy, one of the clotting factor deficiencies, had made him high risk for bleeding with major open surgery. His aneurysms never shrank but remained stable and without visible endoleak by CT for a long time resulting in ever longer intervals between followup.
2013
Between 2009 and 2013, there was subtle enlargement on the embolized side without a type I or type III leak, and the patient was brought back a year and a half later, with further growth of the sac.
2015
This was a relatively rare type IV endoleak that was causing sac enlargement due to excessive graft porosity of the original Excluder’s graft material. Its treatment is either explantation or relining. We chose to reline the graft with an Excluder aortic cuff at the top and two Excluder iliac limbs.
This was done percutaneously and in short followup, there has been stabilization and even some reduction in the aneurysm circumference.
It was long known that a certain percentage of PTFE grafts “back in the day” would sweat ultrafiltrated plasma. The relative porosity of the grafts allowed for transudation of a protein rich fluid.
Tanski W, Fillinger M. J Vasc Surg 2007;45(2):243-249.
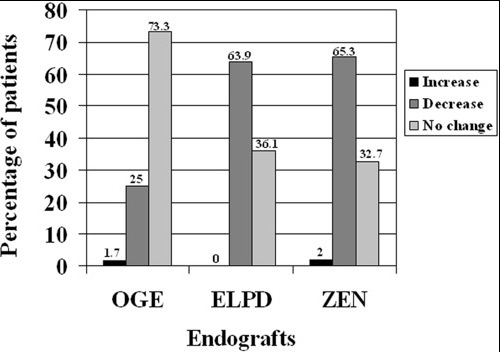
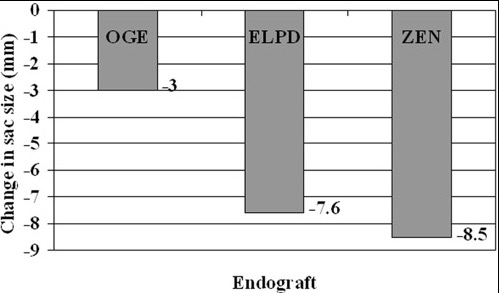
This results in a hygroma formation. I remember seeing this in AV graft fistulae back in the 90’s -after flow was introduced, the grafts would start sweating! The newer grafts are lower porosity and this is seen very infrequently. Drs. Morasch and Makaroun published a paper in 2006 comparing parallel series of patients who received the original Gore Excluder (OGE), the currently available Excluder Low-Permeability Device (ELPD), and the Zenith device (ZEN). Sac enlargement occurred in equal measure between OGE and ZEN but zero was reported for the ELPD.
Haider S et al. J Vasc Surg 2006;44(4):694-700.
The ELPD had higher rates of sac shrinkage than the OGE, and equal rates of sac shrinkage compared to ZEN.
Haider S et al. J Vasc Surg 2006;44(4):694-700.
The diagnosis in my patient’s case came about through serial followup through a decade. While I doubt that the aneurysm would have ruptured in the same way as in a Type I, II, or III endoleak, I am sure it would have progressed to developing symptoms from aneurysmal distension or local pelvic compression.
Is it possible to visualize this kind of endoleak at the time it is suspected? I came across a case series from the Netherlands using Gadofosveset trisodium which takes longer to clear than the usual Gd-based MR contrasts and they successfully visualized transudative leaks in 3 serial patients with the original Excluder graft.
Cornelissen SA et al. J Vasc Surg 2008;47(4):861-864.
The problem is that Gd-based contrasts have toxicity, especially for patients with poor renal function. The protocol is time consuming. And I suspect that ten years out, a lot of grafts will have positive findings, especially cloth based grafts that are sutured to their supporting stents, without clinical basis for treatment as their sacs size are likely stable on a year to year basis.
That said, as we are well into the second decade of commercially available stent grafts, it is even more important than ever to continue lifelong followup even for what is assumed stable, patent grafts and anatomy.
The patient, an active 88 year old man, was transferred from an outside institution after a CT scan revealed a 9cm thoracoabdominal aortic aneurysm on workup of sudden onset back pain. On transfer, his blood pressure was stable but low in the 90’s. On arrival, his blood pressure dropped into the 60’s but responded to resuscitation, and after a detailed conversation with him about the risks of emergent repair, we brought him to the operating room.
The CT scan showed an 8.3cm extant III thoracabdominal aortic aneurysm which originated slightly above the diaphgragmatic hiatus and extended to the aortic bifurcation in two lobes. The larger lobe involved the visceral vessels and the infrarenal component was about 5cm.
While there was no frank rupture on the CT, the outside report mentioned haziness of the posterior wall consistent with ongoing rupture. Examination was significant for hypotension, abdominal and back pain, and a large pulsatile mass in the abdomen.
Despite the lack of contrast on this study, I was able to get a centerline reconstruction. The 3D virtual reality view then allows me to plan the operation virtually. The red and blue lines above bracket the beginning and end of the aortic aneurysm with the patient in a right lateral decubitus projection. A thoracoabdominal incision starting on the 8th rib was planned.
The patient remained stable through the intubation with a dual lumen endotracheal tube. The chest was entered and the left lung collapsed and the thoracic aorta in the chest was controlled for clamping. The retroperitoneum was dissected and the abdominal contents allowed to fall away exposing the remainder of the aneurysm. The diaphragm was taken down circumferentially. The aneurysm was leaking -not frankly but there was blood visible on the surface like a bruised, overripe plum of unusually large size.
The aorta was clamped in the chest after giving the patient 5000 units of heparin -I often don’t if there is a lot of blood loss and I anticipate factor depletion. The transdiaphragmatic aorta was controlled and the celiac axis (CA), superior mesenteric artery (SMA), and left renal artery were controlled with vessel loops. The aortic bifurcation was controlled as well after I considered anastomosing to the narrow segment of aorta around the renal arteries. While saving the infrarenal aneurysm for later has an appeal, I feel that if you cut the graft and start sewing to the aorta and find that it is not of good quality, you have wasted time. The aortic clamp was moved down from the chest to the transdiagphragmatic aorta which was now mobilized. This avoided for me some spinal cord ischemia but can be a risky move because the aorta was not healthy even in the nonaneurysmal segments. A 32mm Dacron graft what had 4 branches was brought into the field and anastomosed proximally with 4-0 polypropylene suture.
I picked up using narrow gauge suture for aortic anastomoses from my cardiothoracic surgery confreres at the Clinic (Eric Roselli, MD). They will use 5-0 polypropylene with the idea that the smaller needles result in smaller needle holes. I used to use 2-0 suture with an MH needle and have seen my partners be successful at it, often buttressing the anastomosis with a gusset (Dan Clair), but this patient had the tensile strength to take suture well so I went with the smaller SH needle and smaller gauge suture. Other maneuvers include sewing to a strip of Teflon, or in the case of terrible aortic tissues, using interrupted sutures which give some added stability but at the cost of time (credit to Tom Bower).
Time is the killer. While cell salvage gives you some margin for blood loss, this is lost with coagulopathy and hypothermia. The grafts to the viscera were sent from distal to proximal -I feel this greatly eases wire access if needed from a femoral access. There can be a problem with twisting, and I avoid this two ways -by allowing for generous length with looping around the main graft to create forgiveness -closing the retroperitoneum inevitably twists the graft -this I credit to my former partner Pat O’Hara who retired last year. The right renal artery received the first graft while cold saline was given to the left renal artery which was revascularized last. Neither had ostial lesions which I have learned to stent with a bare metal stent directly with the artery open -this I credit to Jeanwan Kang, MD, one of my current partners. The CA graft resulted in great back bleeding from the SMA. The SMA graft and left renal artery grafts completed the visceral segment of the case.
The distal anastomosis was challenging because the bifurcation was heavily calcified. I have to say, the distal often will give me fits when the proximal does not because of the calcium. I generally do perform an endarectomy, but this often results in very poor remnant adventitia. The advice here is be prepared to go distally, but consider that it may add time to the case.
The hemostasis was obtained -the most important factor in hemostasis is early and successful repercussion. The wound was restored with repair of the diaphragm, closure of the chest over two chest tubes and closure of the abdomen.
The success of these patients only begins with the operation which I cannot do without the active participation of our cardiac anesthesia, nursing, and trainees -our fellow Eric Shang did his work competently. I am fortunate to have strong help in our vascular intensive care unit. There, my patient was actively resuscitated with blood product, stabilized, and weaned off the ventilator within 2 days. Fortunately, he was not paralyzed by this operation which can happen in up to 10% of patient. Also, his renal function stabilized and he never required dialysis. He was eventually discharged to rehab in under 2 weeks. He returned to my office about a month after the rupture, walked in, accompanied by his family. He was making progress with his rehab, and his wounds had healed well.
Various indices are formulated to predict outcome, which traditionally are viewed as poor for open repair on octogenarians. I am still old fashioned and rely on the “eyeball” test. Several risk stratifying schemes have been published. Most recently, the group from Harborview (link, another link) published a simple stratification scheme for infrarenal AAA rupture. Garland et al (in press) found that having combinations of the following factors predicted mortality well for ruptured AAA including:
Age >76
preop Cr>2.0mg/dL
BP<70mmHg at any point
arterial pH<7.2
Mortality risk
If this was a ruptured infrarenal AAA, the patient had two of the risk factors -age>76 and BP<70mmHg, which conferred a risk of 80% mortality for open repair, which translates to a higher number for thoracoabdominal aortic aneurysm repair.
One of our recent aortic fellows, Muhammad Aftab, published the Baylor experience on open repair of TAAA when he was there and found that for open repair, rupture conferred an independent risk for death with a OR of 5.7.
Despite the dismal statistics, several intangibles did favor survival in the patient. He was at 88 still a working professional. He exercised everyday and was fit. He did not drink to excess and never smoked. And he had complete understanding during our preoperative conversation and had a strong grip. And he survived waiting several hours at his hospital for workup and eventual transfer which is a stress test. This last factor accounts for the higher mortality rates for rupture that occurs in hospitals and in places like Seattle where the EMS transport is highly efficient, and better mortality rates at rural referral centers like Mayo where the filtering effect of time leaves a greater proportion of patients likely to survive an operation for rupture.
Reference
Aftab et al. J Thorac Cardiovasc Surg 2015;149:S34-S41