CTA tends to overread stenoses which was in the 60-79% range on duplex
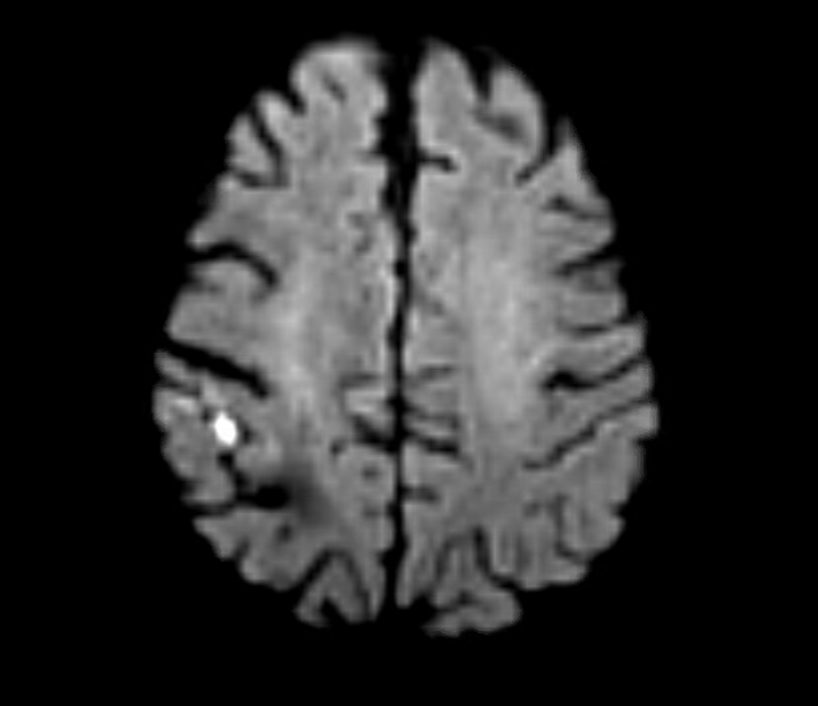
The patient is a middle aged executive who complains of bouts of aphasia triggered by intense conversations and business meetings. It first occurred while driving to Dubai on a conference call. Since then, they occurred several times a week, typically triggered during meetings where he needs to think and speak. Casual conversation and cognition does not seem to trigger this. Workup revealed a heterogeneous plaque affecting the left ICA with velocities in the 60-79% range. CTA confirmed this plaque. MRI failed to show any stroke or other lesions. Neurology evaluation showed normal exam. The patient underwent endarterectomy, and had a normal recovery. In followup, he denied any further episodes of aphasia.
Standard endarterectomy with patch
Aphasia, the loss of function in the language centers, typically of the left brain, although in a minority, it may live in the right hemisphere, is terrifying manifestation of stroke. This case, if examined superficially, is nothing special in that TIA’s associated with a reasonable culprit lesion went away after elimination of that culprit lesion. To me, it was fascinating because it represents a possible case of brain claudication.
The human brain is believed to have evolved to its large size in conjunction with bipedalism, social hunting and gathering, and climate change in the Great Rift Valley favoring a savannah over forests, that created heat stresses on the brain, favoring the development of sweating and redundancies in brain tissue. The advent of fire and cooking enhanced available calories to feed this enlarged brain’s metabolic needs. When the metabolism isn’t supported through adequate blood supply, the brain tissue dies. Rarely, it blinkers on and off, and even more rarely, this occurs in the motor strip triggering today a neurologic evaluation including a carotid duplex that brings these patients to our attention. The fascinating question for me is, does increased metabolic demand in the form of complex thinking result in a supply-demand mismatch much as seen in exercise induced angina or claudication? If it can, can we test for it?
The tests we have available are hemodynamically based. At its simplest, after carotid angiography, an occluding balloon can be inflated to test for symptoms. This is an archaic test and I do not do it. There are nuclear medicine, PET CT, and MRI tests that use pharmacologic agents to induce hypotension, but again, for this patient, it wouldn’t apply. This patient needed the equivalent of a treadmill in the MRI machine. Maybe having him read a dry, technical treatise on neurobiology taped to the MRI tube?
I went to the OR with the indication of TIAs associated with a >50% lesion, but I did tell the patient that it was possible his thinking-induced aphasia would not remit. Thankfully it did.
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
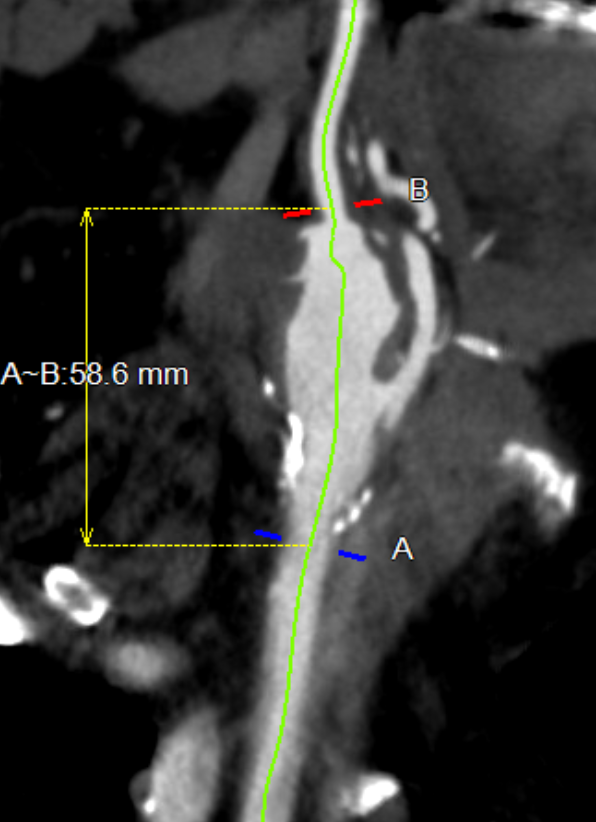
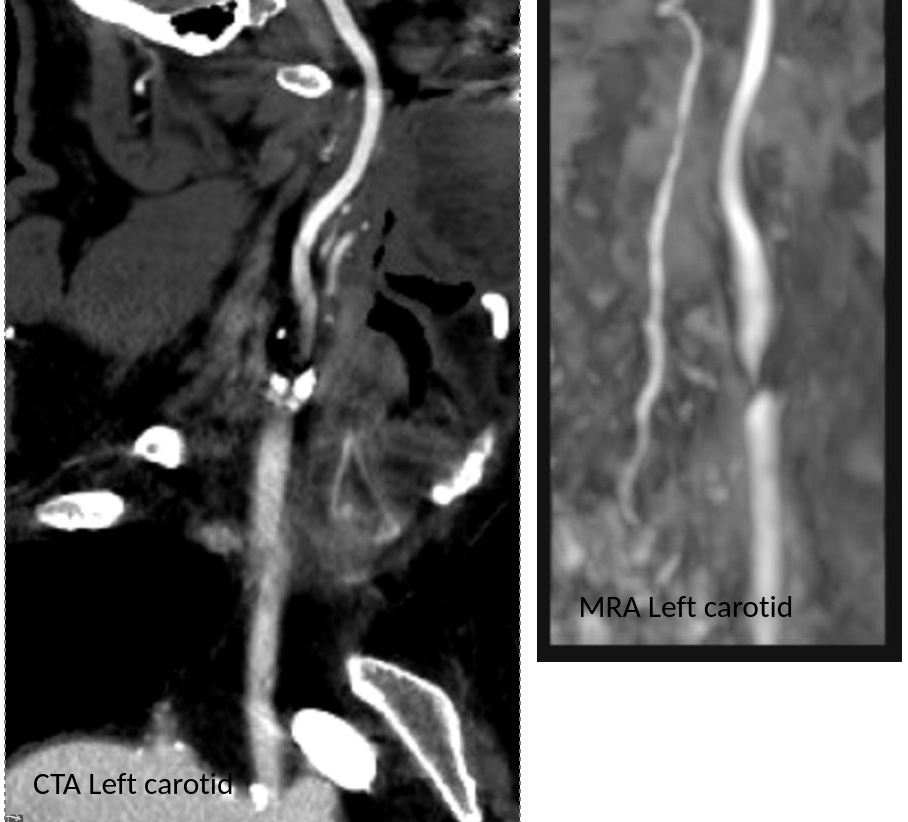
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
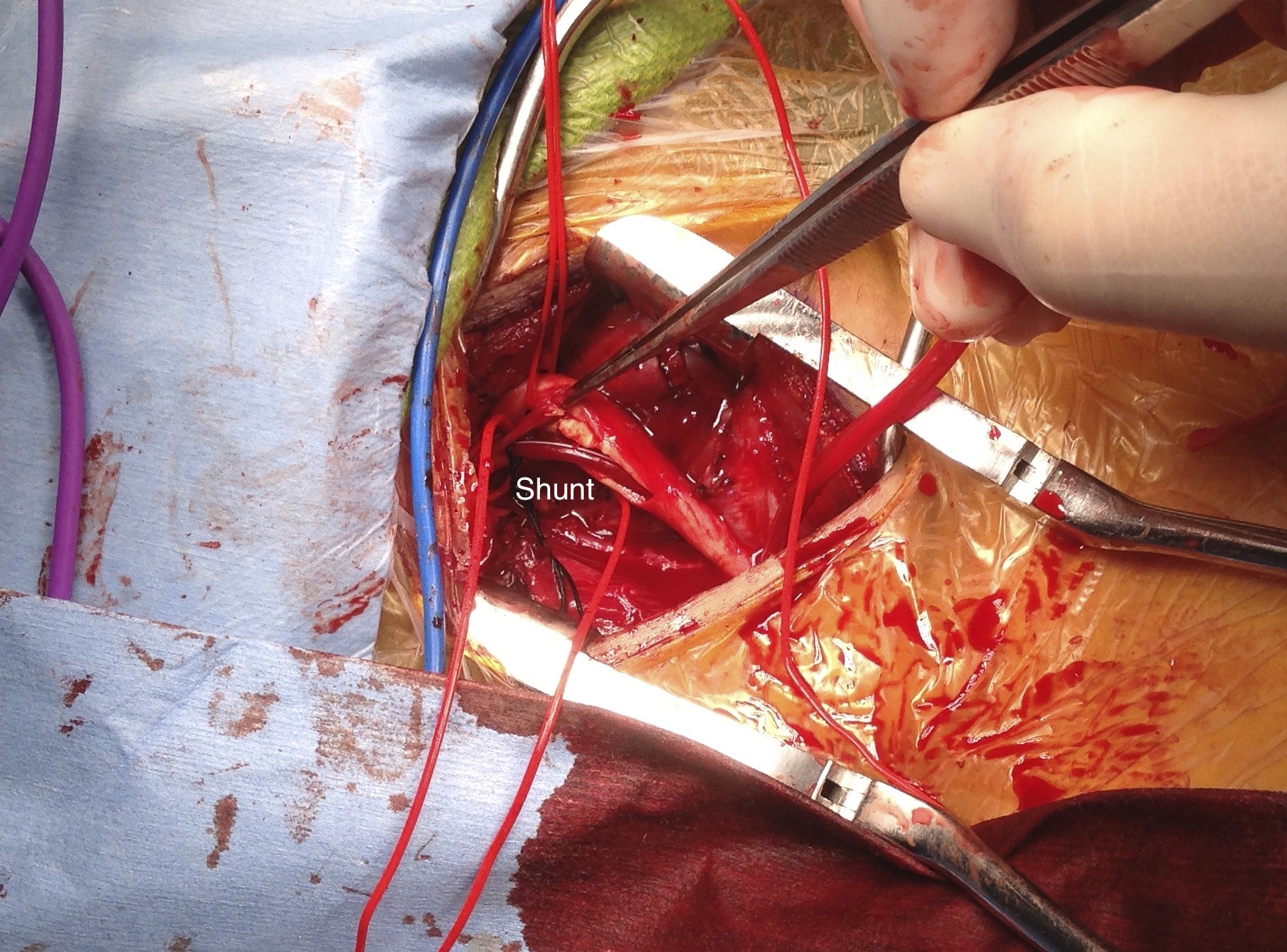
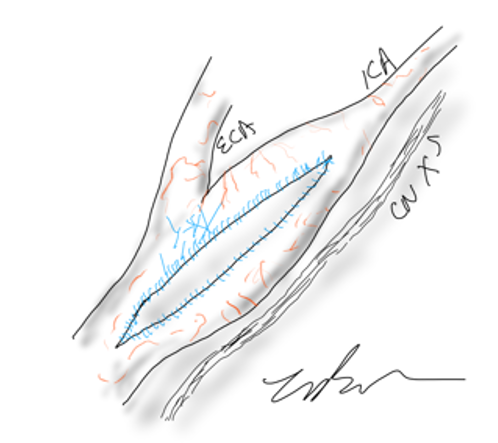
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
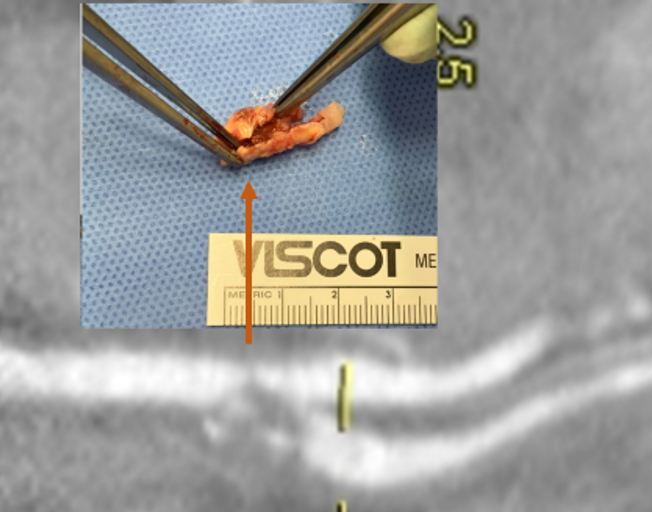
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
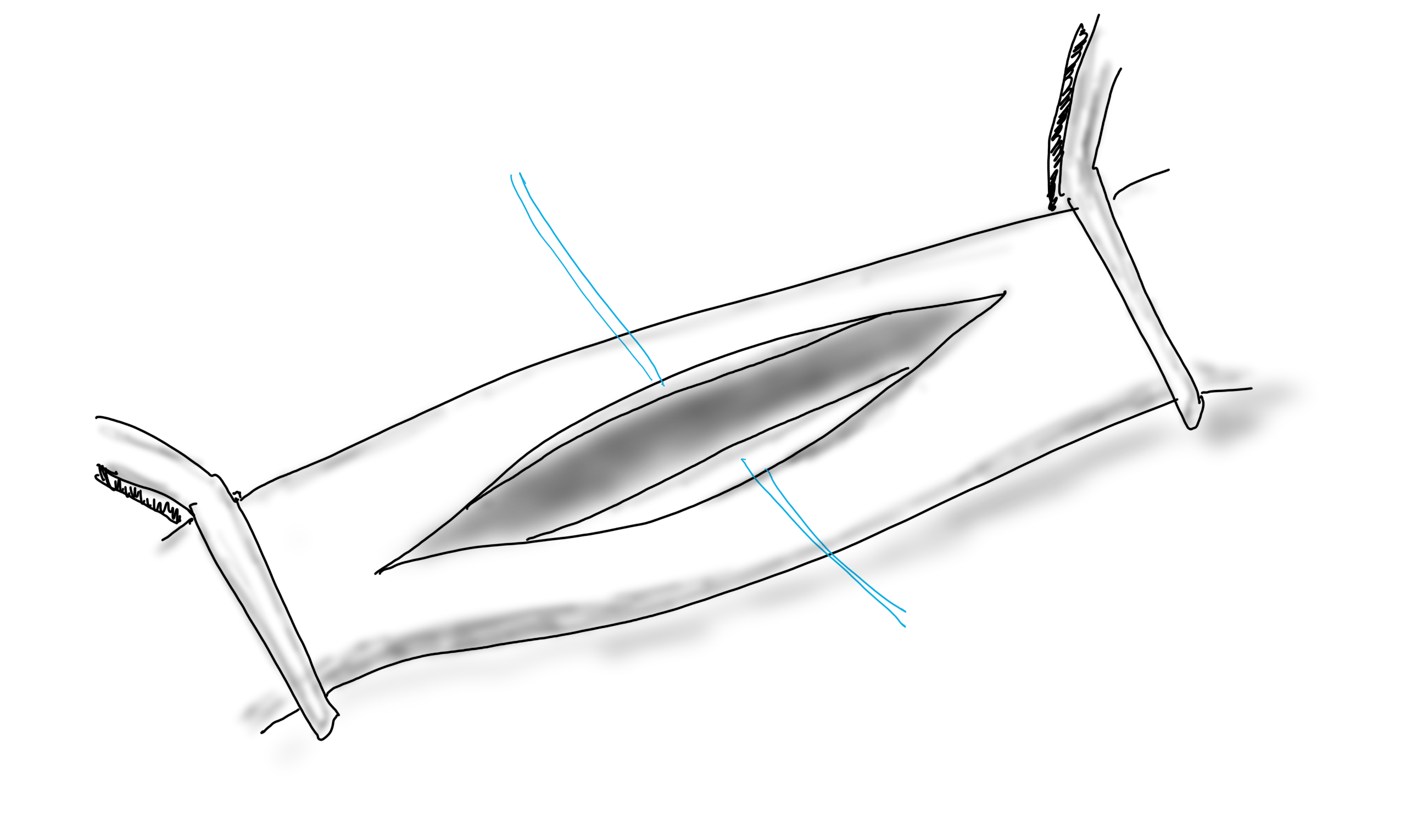
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
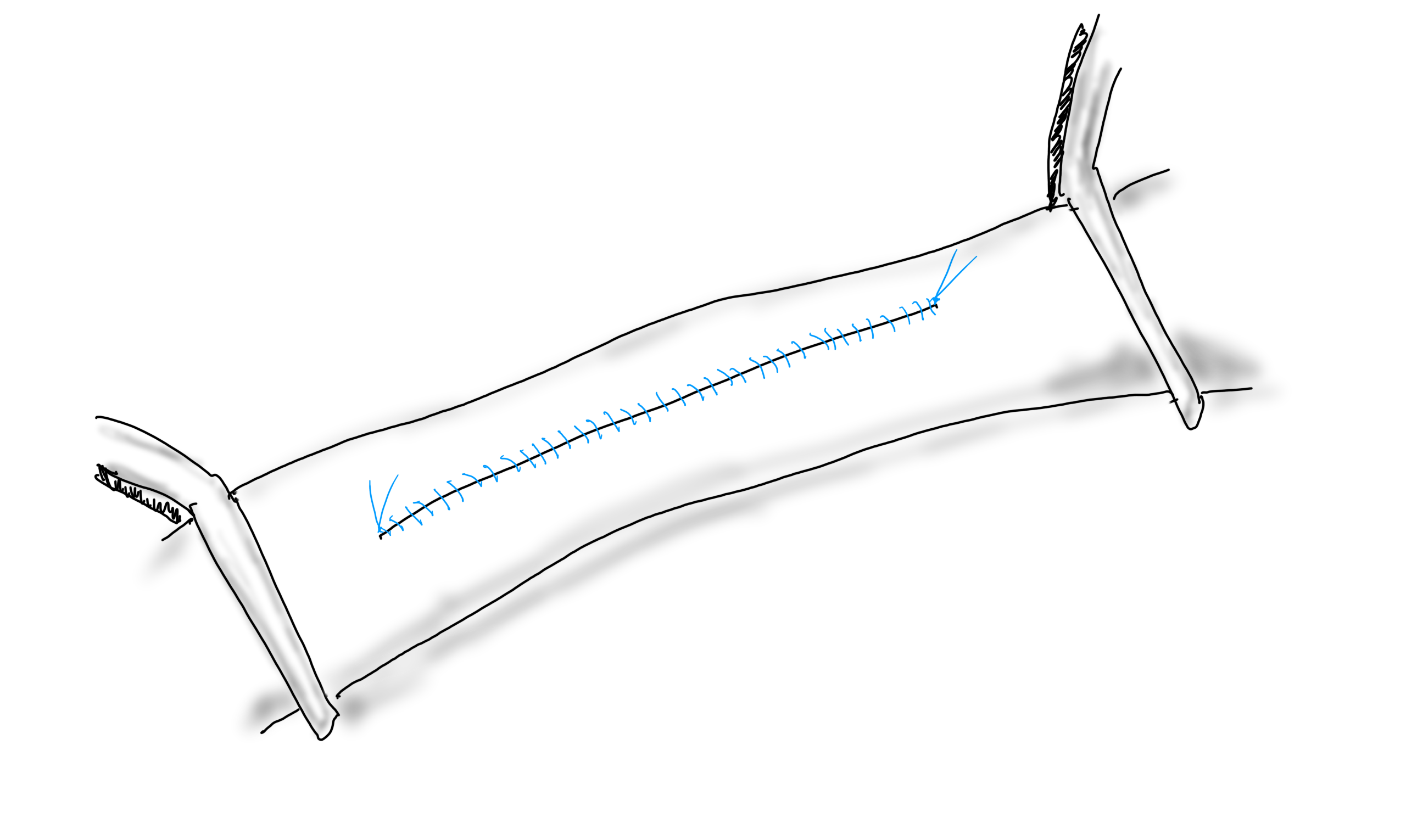
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
Tracheal deviation due to iatrogenic carotid pseudoaneurysm
History
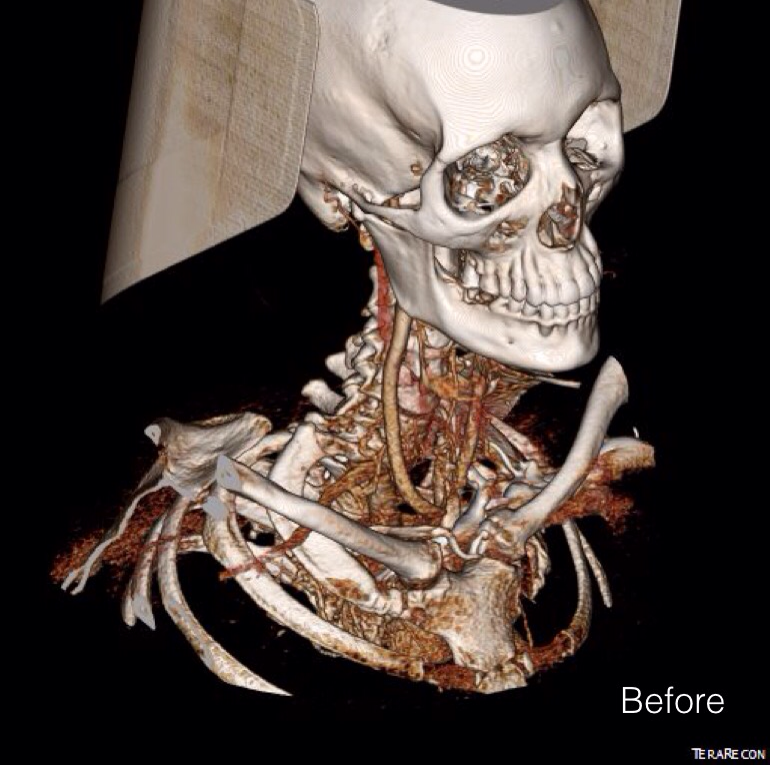
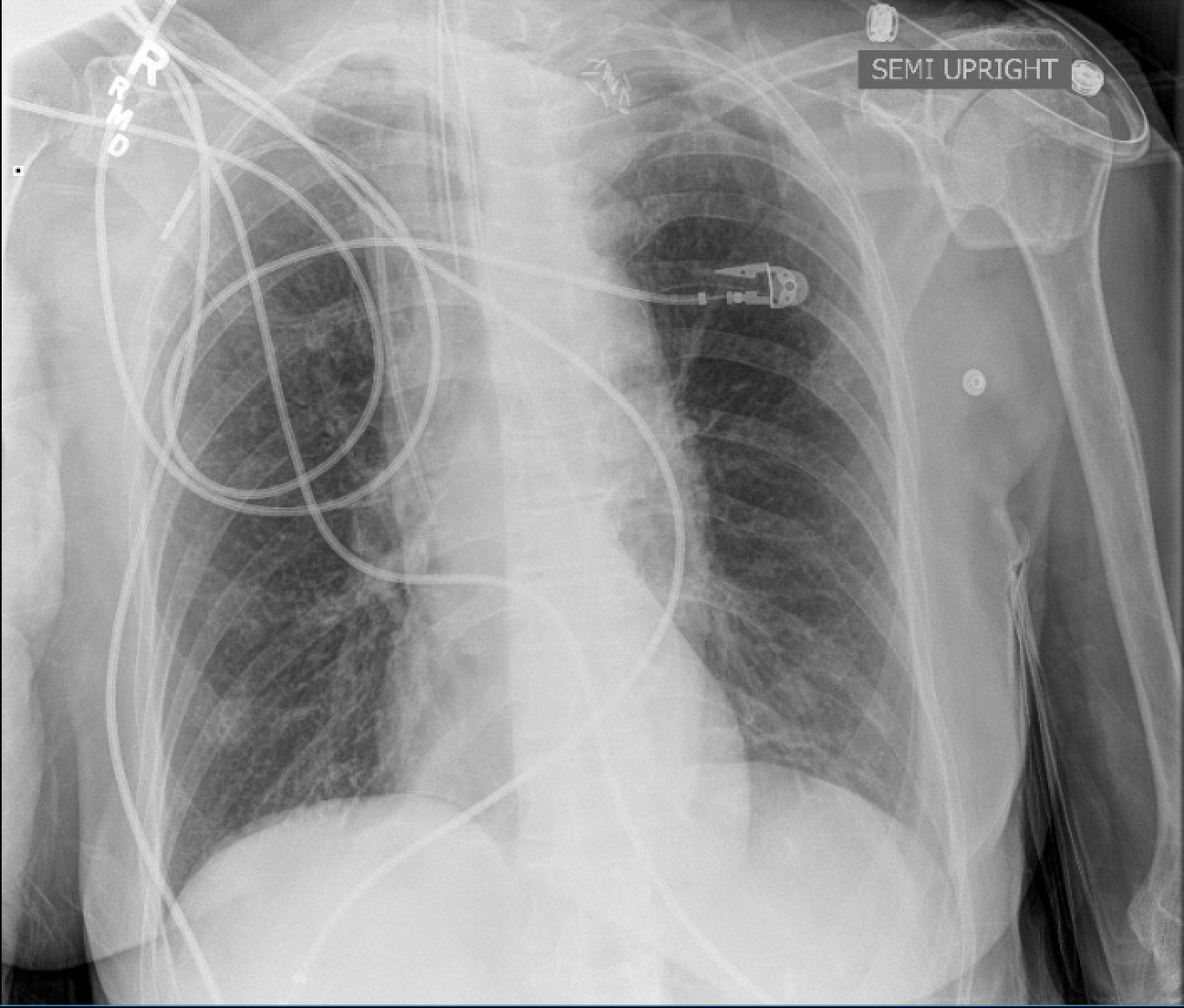
The patient is an 80 year old woman with lung cancer who was getting a port placed at her home institution. It was to be a left subclavian venous port, but when access was not gained, a left internal jugular venous port was attempted, but after the intitial stick and sheath placement, pulsatile bleeding was recognized and the sheath removed. Hemostasis was achieved with clips and the wound closed and a right internal jugular venous port was placed. The postprocedural CXR shown above showed tracheal deviation and numerous clips from the initial port placement attempt, and a CT scan with contrast (unavailable) showed a carotid pseudoaneurysm of 3cm projecting posteriorly behind the pharynx/esophagus. She was kept intubated and sedated, and transferred for management.
On examination, her vital signs were stable. She had 2cm of tracheal deviation and swelling was apparent at the base of the neck. While my trainees may be better versed at this than I at the particulars of this, my old general surgery trauma training kicked in, as she had a Zone I neck carotid injury, which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
Open repair
Endovascular repair from femoral access
Hybrid repair
Open Repair
Open repair is the approach of choice for zone 2 injuries because aerodigestive tract injuries can also be addressed and the exposure is straightforward. For Zone 1 injury, the exposure is potentially possible from a neck exposure, but in my experience, jumping into these without prepping for a sternotomy puts you into a situation without a plan B. The exposure of the carotid artery at this level becomes challenging with hemorrage from the artery once the compression from the hematoma or pseudoaneurysm is released. A sternotomy in this elderly woman, while not optimal, may be necessary if open control is required, but the best plan is to avoid this.
Endovascular Options
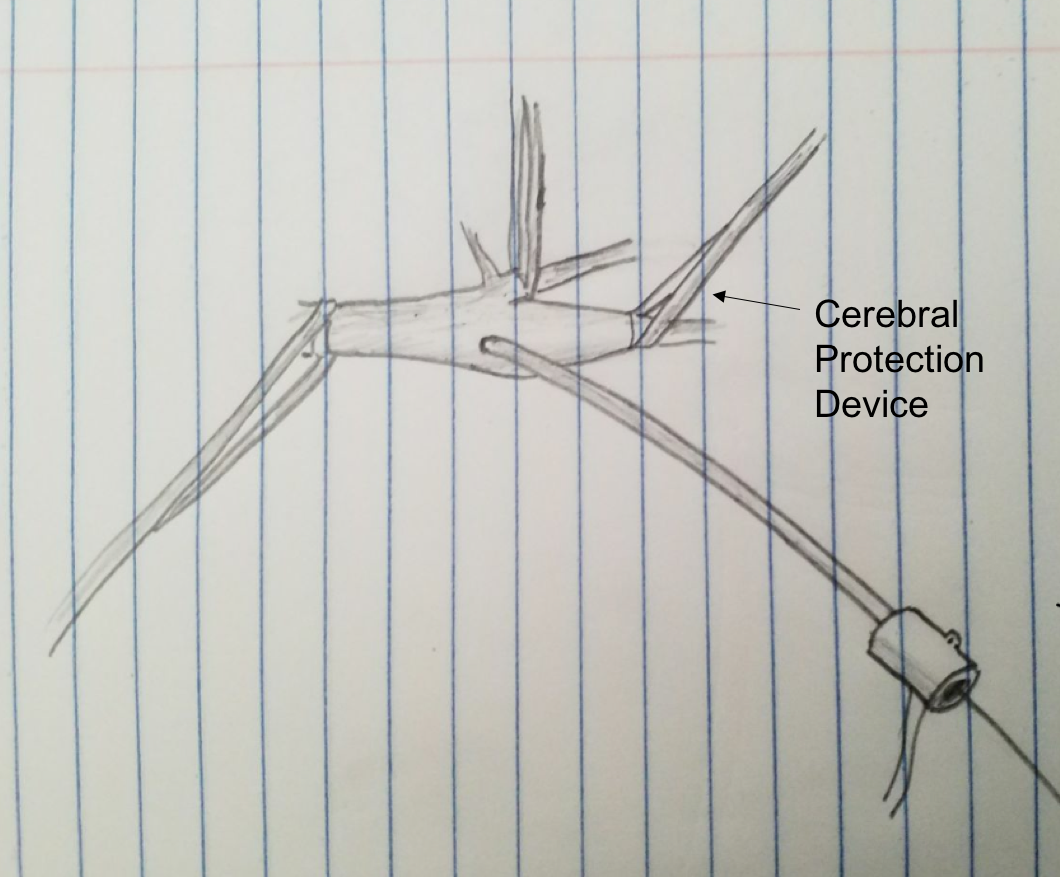
This should be a straightforward repair from an endovascular approach, even with the larger sheath required for the covered stents. A purely endovascular approach is problematic for two reasons. One, cerebral protection devices are built for bare carotid stents and not peripheral stent grafts, but this is not prohibitive -it should be fine. Without a planned drainage, the hematoma would be left behind which could cause prolonged intubation and problems with swallowing -both an issue for an elderly patient battling lung cancer. Endovascular access could provide proximal control for an open attempt from above, but instrumenting from the arch in an 80 year old has a known 0.5-1% stroke rate.
Hybrid Repair
A hybrid open approach with exposure at the carotid bifurcation offers several advantages. With control of the internal carotid artery, cerebral protection is assured while the carotid artery is manipulated. At the end of the procedure, the internal carotid can be backbled through the access site with the common carotid artery clamped. The hematoma could be avoided until the stent graft is deployed. An unprotected maniplation in the arch can be avoided. Once the stent graft is deployed, drainage of the hematoma can be performed.
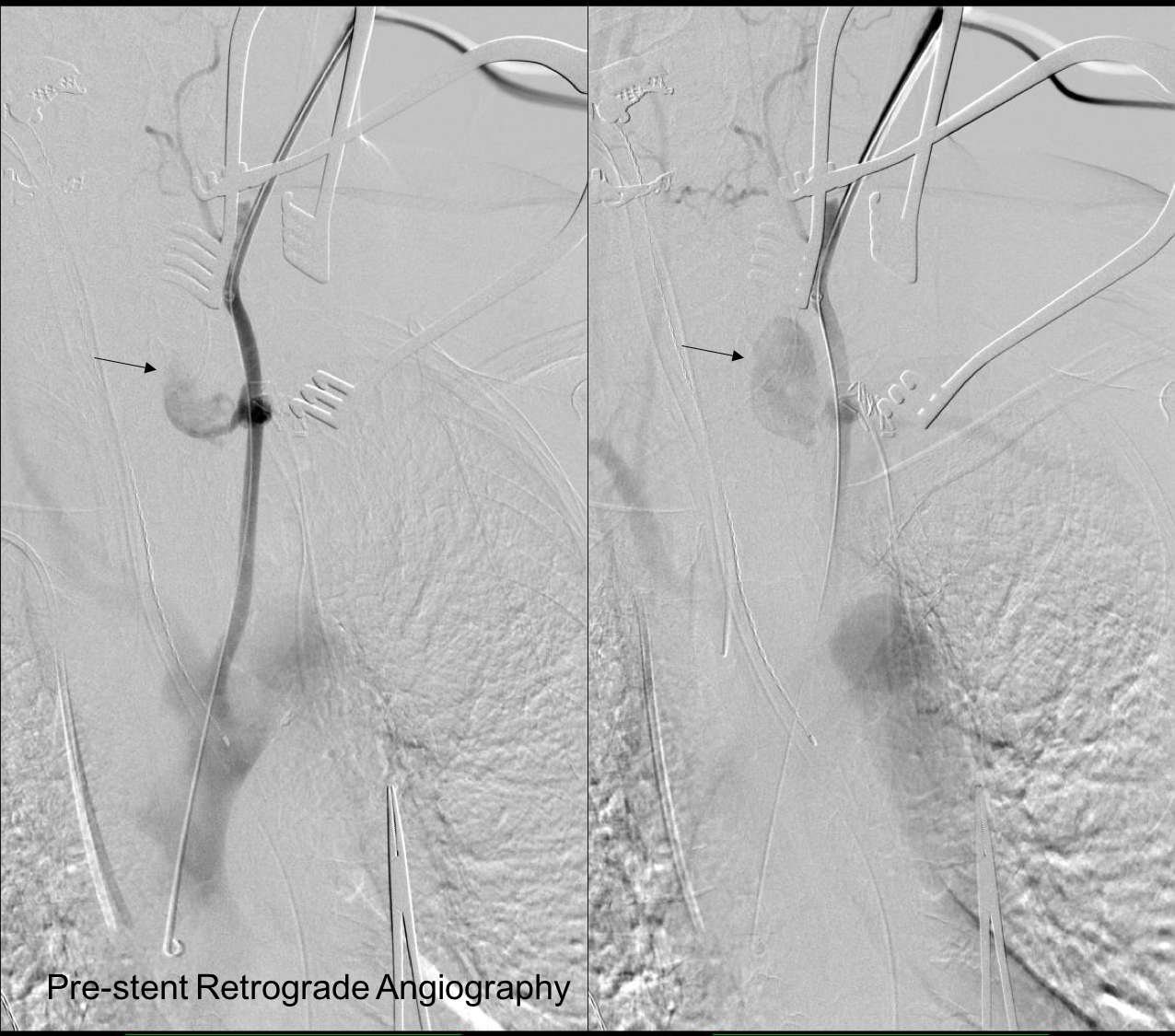
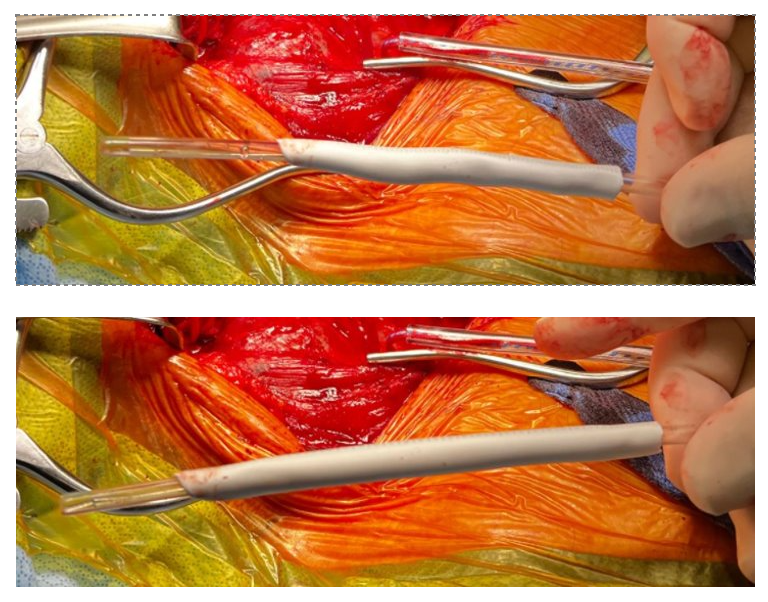
This required setting up a table off the patient’s left that allowed the wire to lie flat to be manipulated by my right hand. The carotid bifurcation was accessed through a small oblique skin line incision and the common, internal, and external carotid arteries, which were relatively atherosclerosis free, were controlled with vessel loops. The patient was heparinized. The internal carotid was occluded with the loop, and the common carotid below the bifurcation was accessed and an 8F sheath with a marker tip inserted over wire. Arteriography showed the injury and pseudoaneurysm.
The location of the injury based on CT and on this angio would have baited a younger me into directly exposing it, but experience has taught me that which occasionally you can get away with it, the downsides -massive hemorrhage, stroke, need for sternotomy, just aren’t worth it. The sheath was brought across the injury and a Viabahn stent graft was deployed across the injury.
The hemorrhage was controlled and the hematoma was then exposed and drained -the cavity was relatively small and accepted the tip of a Yankauer suction easily. A Jackson-Pratt drain was placed. The access site was repaired after flushing and retrograde venting as described.
She recovered rapidly after extubation postop. She was able to breath and swallow without difficulty and had suffered neither stroke nor cranial nerve injury. The drain was removed on postop day 2.
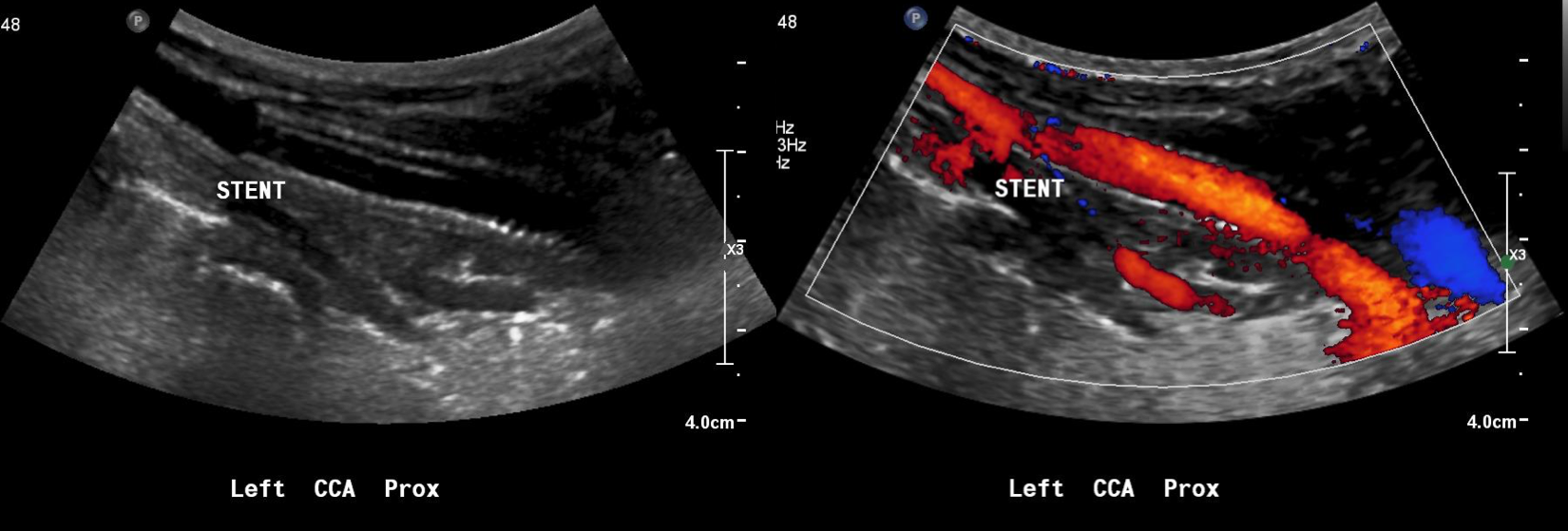
The patient recently returned for a 6 month followup. Duplex showed wide patency of her stent.
More gratifyingly, her port was removed as her cancer was controlled with an oral regimen.
Discussion
Let me start with my bias that all penetrating trauma should be approached in a hybrid endovascular OR. It is a natural setting for trauma and this case illustrates that. In a hybrid operating room, central aortic and venous injuries can be controlled endovascularly while open repair, including salvage packing, can be done. Excess morbidity of central vascular exposures can be avoided. Temporary IVC filters can be placed if indicated (becoming rarer and rarer). Cardiopulmonary bypass can be started.
In this patient, hybrid therapy brought the best of both techniques and avoided many of the pitfalls of the purely open or endovascular approach. For stable zone I penetrating injuries of the neck, it is clear that this is a reasonable approach.
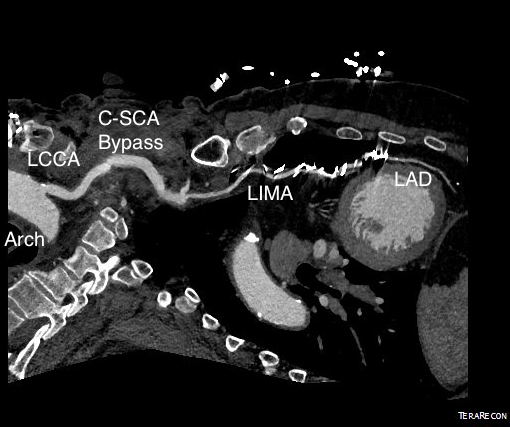
Patient is a 77 year old man with history of HTN, hyperlipidemia, former smoking, and CAD with CABGx5 and bilateral lower extremity bypasses who developed unstable angina consisting of neck and throat pain. He underwent catheterization at an outside hospital and found to have 100% LAD occlusion, a diseased, small patent left main and left circumflex (the profunda femoral artery of the heart!), 100% RCA occlusion, a patent but diseased SVG to distal RCA, and a patent LIMA graft to distal LAD but with severe plaque and near occlusion of his proximal left subclavian artery.
He had an NSTEMI. His vitals signs stabilized in the coronary care unit and he was sent to a telemetry floor. Whenever he walked, he would get the jaw pain, and this would also occur sporadically while recumbent.
On examination, he had no left brachial pulse, only a monophonic signal there, and bounding femoral pulses where there were the origins of bilateral femoral-tibial bypasses. His radial artery pulse was diminished on the right and absent on the left. Both saphenous veins had been harvested as were arm veins for the left leg bypass.
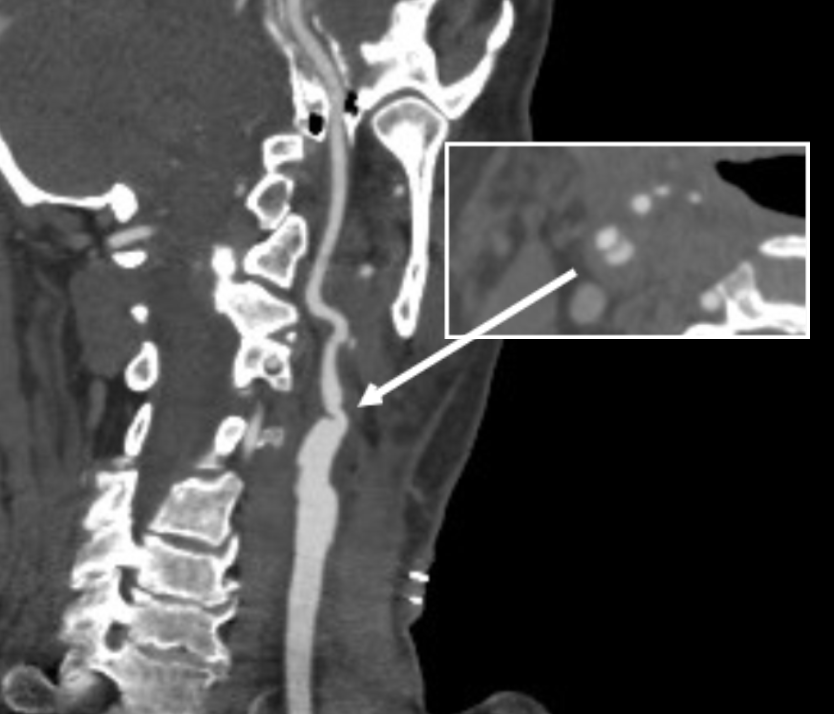
CTA shows the left subclavian artery to be occluded at its origin.
Heavily calcified occlusive plaque in left subclavian artery
Arrow points to LSCA origin with plaque
Cardiac surgery, interventional cardiology, and vascular surgery were called in for consultation. Cardiology consultation (Drs. Kapadia and Shisheboor) felt, and I agreed, that the left subclavian lesion was a poor candidate for recanalization and stenting. CT Surgery (Dr. Faisal Bakaeen) and I had a long discussion regarding alternate conduits, as he had unknown radial but likely radial artery disease, and had all usable veins previously harvested. I brought up a free RIMA graft -I had worked with Dr. Daniel Swistel, in NYC as a resident, who was Dr. George Green’s protege, and as a medical student at P&S I scrubbed Dr. Green’s final cardiac case. He routinely performed bilateral ITA bypasses decades before all-arterial revascularizations were routine. I get enthusiastic talking about cardiac disease! Walking through all the options -does anyone use deep femoral vein as coronary bypass conduit -we agreed ultimately that the best option would be a carotid-subclavian bypass with plenty of backup.
At its heart, it would be this vascular surgeon’s attempt at an off-pump single vessel CABG (above). Preparations were made with cardiac anesthesia and cardiac surgery to place an IABP (intra-aortic balloon pump) if he became unstable. For my part, the operation was straightforward, but I was going to have to go about it efficiently. I also figured that with a clamp beyond the LIMA takeoff, no significant change would occur to the coronary flow from the LIMA graft. So I hoped as I worked very deliberately. We kept him on the hypertensive side during the case.
The operation went well. The patient’s angina resolved and a followup CT showed the patent bypass feeding the LIMA and LAD.
LIMA bypass not well visualized on coronary CTA because of the clips used in dissecting them. Perhaps we will switch to clips that are invisible to x-ray one day.
Composite CTA showing the bypass
His resting angina resolved. He followed up a month later and was very pleased. Moreover, he had a brachial and radial artery pulse and a general weakness of the left arm that he never complained about before lifted.
Discussion
The carotid subclavian bypass is something that really needs to be in the armamentarium of a modern vascular surgeon. Though out of print, Wylie’s Atlas (the unabridged, multivolume version) is available used through online sellers, and is useful for elucidating the anatomy which boils down to avoiding cutting the important structures -the phrenic nerve, the vagus nerve, the brachial plexus, branches of the subclavian including the vertebral artery, while cutting away muscles -lateral head of sternocleidomastoid, any part of the omohyoid, the anterior scalene muscle. And dividing the lymphatic duct if encountered. And tunneling under the jugular vein. And minding the buttery fragility of the SCA. The best technical paper out there is by Dr. Mark Morasch and it mostly deals with carotid-subclavian transposition (reference 1) but has excellent figures on bypass as well. I do both transposition and bypass, but for brevity, I prefer bypass.
This is not a unique problem, having been reported in the literature. An unusual variant of this is coronary sbuclavian steal syndrome (reference 2), which refers to reversal of flow in the LIMA bypass in the setting of subclavian artery occlusion and left arm exertion -which was not the case here, but interesting enough to mention. Here, it was a straightforward case of managing the hemodynamics. The key point of operating on such a patient was having the surety of quick response in the case of ischemic heart failure -we operated in the cardiovascular operating rooms with rows of perfusion pumps and balloon pumps and VADs and ECMOs at the ready. Indeed, this result could not have been so straightforward and routine seeming without the combined effort and experience of the whole Heart and Vascular Institute from nursing to consultant staff.
Reference
Morasch MD. Technique for subclavian to carotid transposition, tips, and tricks. J Vasc Surg 2009;49:251-4.
Cua B et al. Review of coronary subclavian steal syndrome. J Cardiol. 2017 Apr 14. pii: S0914-5087(17)30090-4. doi: 10.1016/j.jjcc.2017.02.012. [Epub ahead of print]
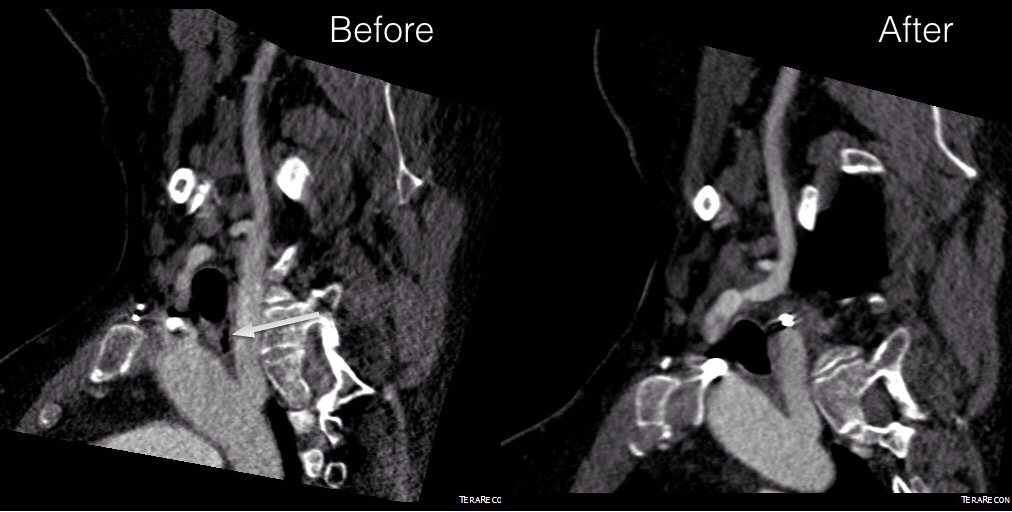
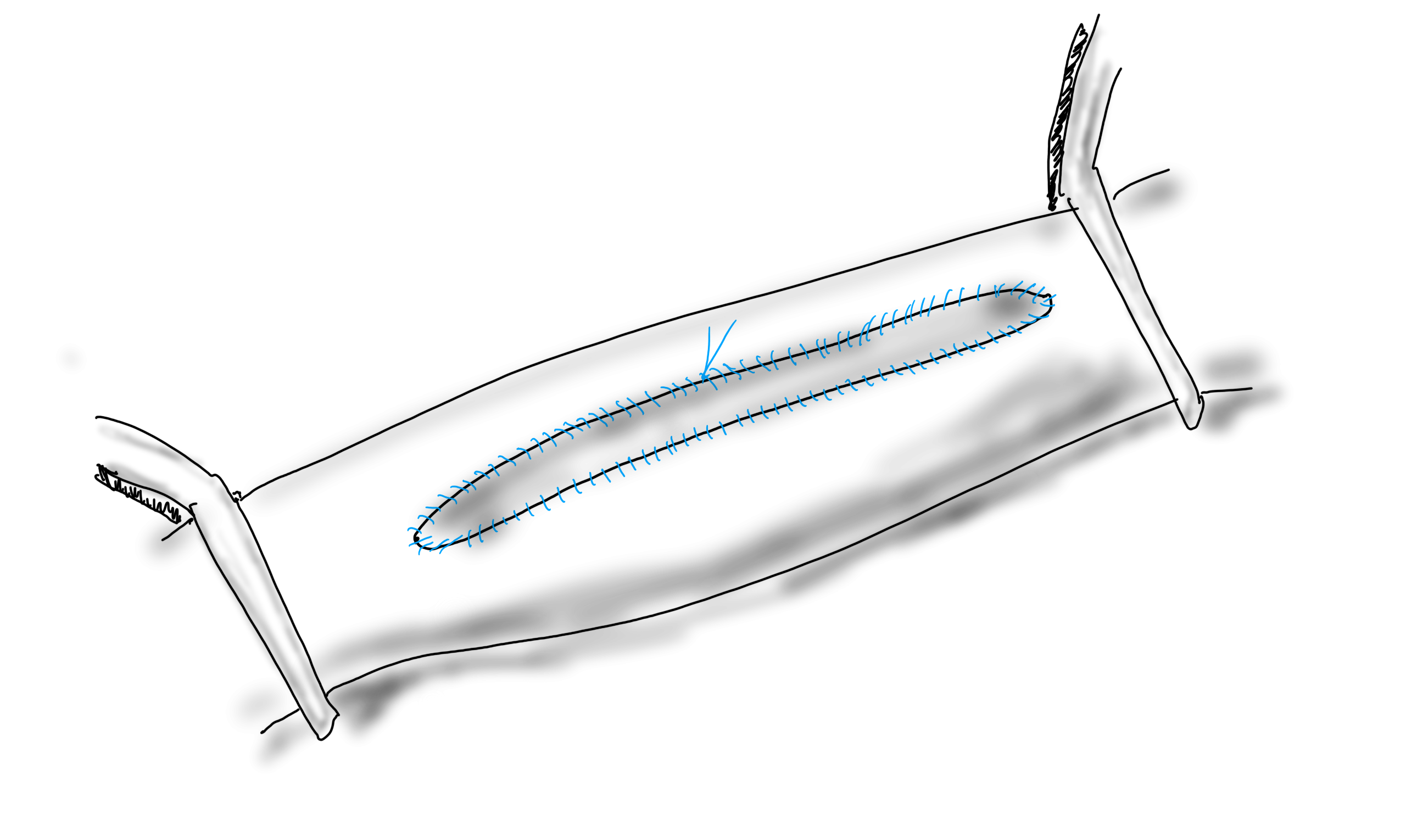
Arrow points to the esophagus. Tension is maintained by the tether on either side of the esophagus. By releasing one side, the tension is relieved.
The patient had been suffering with dysphagia for over a decade and had had extensive head and neck work up which found a goiter. Medical treatment of this goiter failed to relieve the lingering sensation of food getting stuck and the constant feelingof choking. It was only after a search for mediastinal sources of dysphagia that an aberrant right subclavian artery was found.
One of the advantages of working at the Clinics (I was a fellow at the Mayo, and currently on staff the the Cleveland) is that the infrequent is common while the common is rare. Recently in clinic, I had not one but two patients with dysphagia lusoria. It was the observation of Dan Clair’s, chairman emeritus, that by simply transposing the aberrant and yet nonaneurysmal right subclavian artery, the tension on the esophagus and trachea are relieved. Or as the dictum might go: it takes two hands to garrote someone.
The question is then what to do with the stump? The natural history of the untreated stump is unknown but may be more benign than one might assume. It certainly doesn’t degenerate into an aneurysm all the time -chest CT’s are fairly common and when these are discovered, they are not usually aneurysmal like persistent sciatic arteries which present typically as aneurysms with thromboembolism. Perhaps because we don’t sit on the subclavian artery as we would on a persistent sciatic artery that these aberrant right subclavian arteries don’t degenerate.
The old fashioned way I learned to treat these aneurysms (Kommerell Diverticula) was through a high thoracotomy and short graft repair of the aorta, replacing the origin of the diverticulum. This is a dangerous operation for an older, sicker, and often cachectic patient. The more recent reports involve a left carotid subclavian bypass or transposition and TEVAR after a right carotid subclavian revascularization. This second step may be unecessary if the non-aneurysmal stump proves to be benign. I don’t recommend coil embolization of the stump as mass effect of packed coils adjacent to the esophagus can cause dysphagia to recur, and this may necessitate an open resection and repair (observation, DC).
The patient underwent a successful right carotid subclavian transposition and had immediate relief of her dysphagia for the first time in over a decade, especially because she had been told she may have been imagining the discomfort. Kudos to her physicians who ordered the CT of the chest that discovered her arch anomaly. Follow up at 6 weeks showed a stable subclavian stump and patent transposition (images above). My plan is for regular interval CT’s with increasing intervals as time passes.
Our journal club today is discussing one of the many trials that have tried to validate endovascular renal denervation to control severe hypertension. One of the devices I was on trial for back in the 00’s was the CVRx Rheos trial which stimulated the carotid sinus using a surgically placed electrode and generator. While the approval trial failed in the US, it was approved in Europe and my observation of over 30 patients who had this at my center at that time was that it was effective. So effective that I believe many patients stopped taking their pills in exchange for electrical energy -some patients required at least once a year generator changes, often more, but they had normal blood pressures and less to none of the side effects of their medications which frequently exceeded 5 agents.
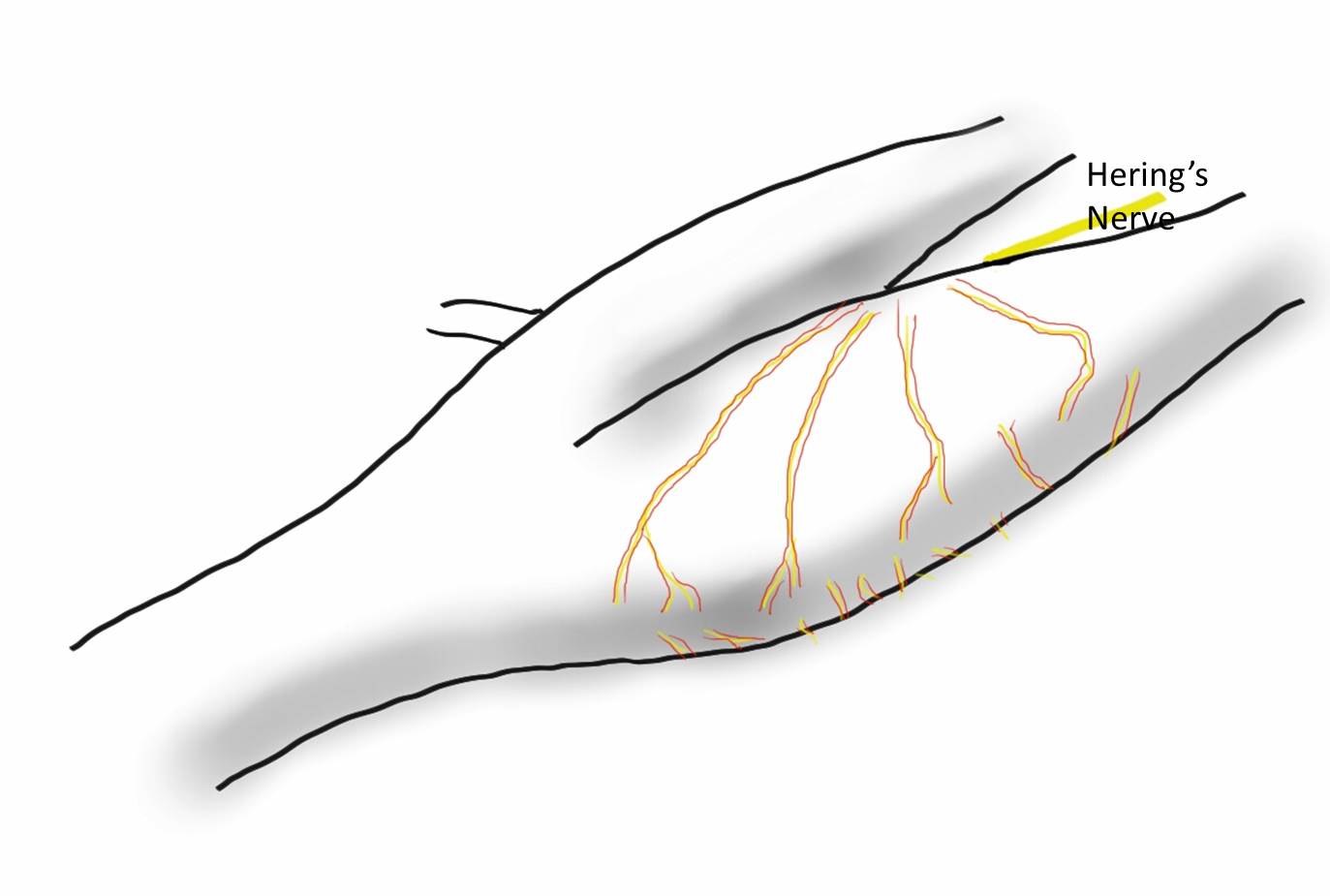
I have observed that on the carotid baroreceptor, which is shaped like an aneurysm by the way, there are paired vasovasorum in the pattern seen above. The only other time I have seen paired arteries is with a nerve. The baroreceptor nerves are very hard to see, but they are there and you can find them between these paired vessels.
The observation that the baroreceptor looks like an aortic aneurysm isn’t a silly one. The area of maximal wall tension is in regions of greatest curvature change and these, teleologically, would be the shape of a baroreceptor. The stiffening of these regions with atherosclerotic plaque would decrease the signal sent to modulate blood pressure and heart rate, and create a pathologic cycle of increasing pressures in response to increased vessel stiffness and vice versa. Just saying.
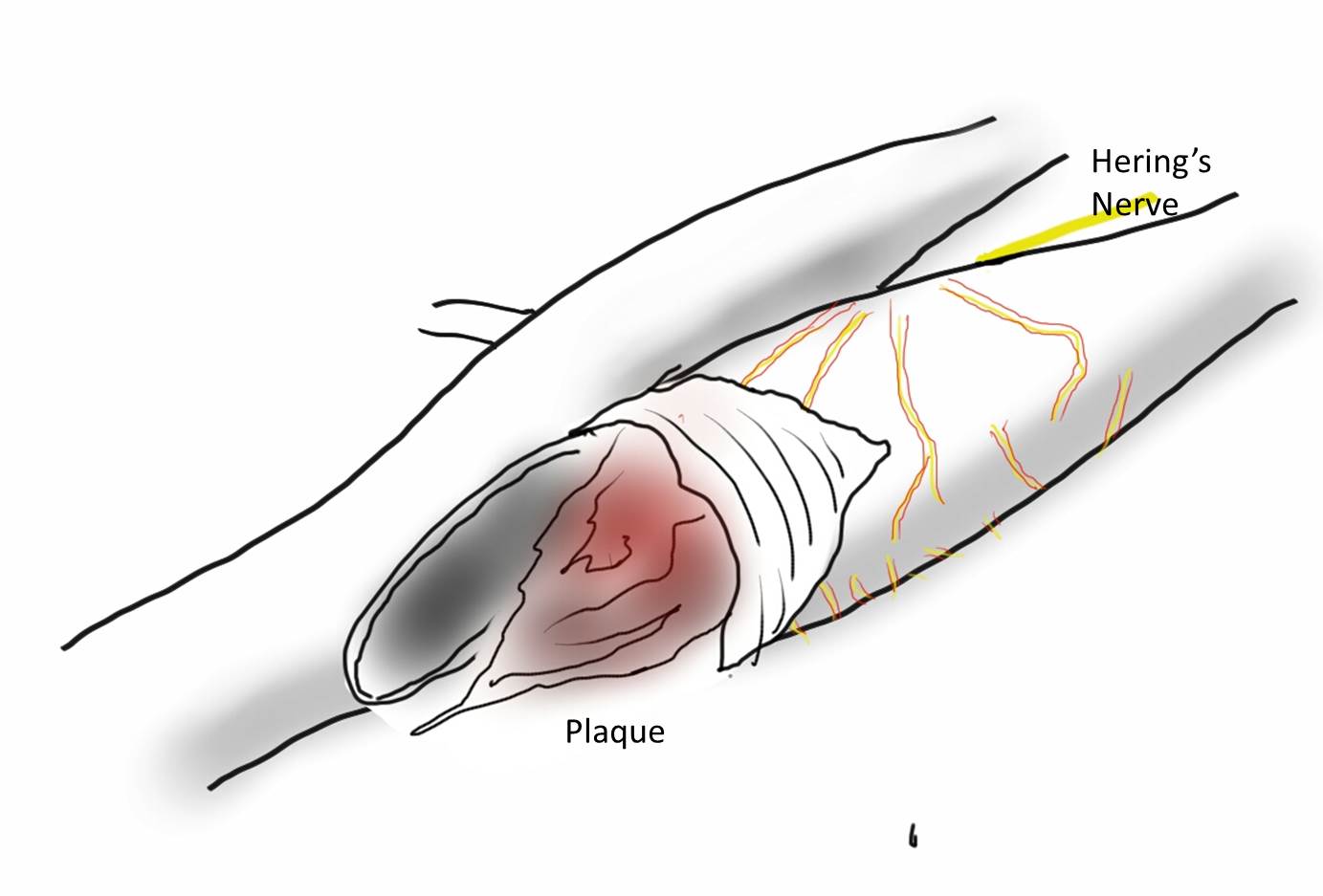
I began to wonder if restoring the elasticicty of these vessels and the shape of the baroreceptor would have a lasting impact on blood pressure. The operation is eversion carotid endarterectomy with sparing of Hering’s nerve.
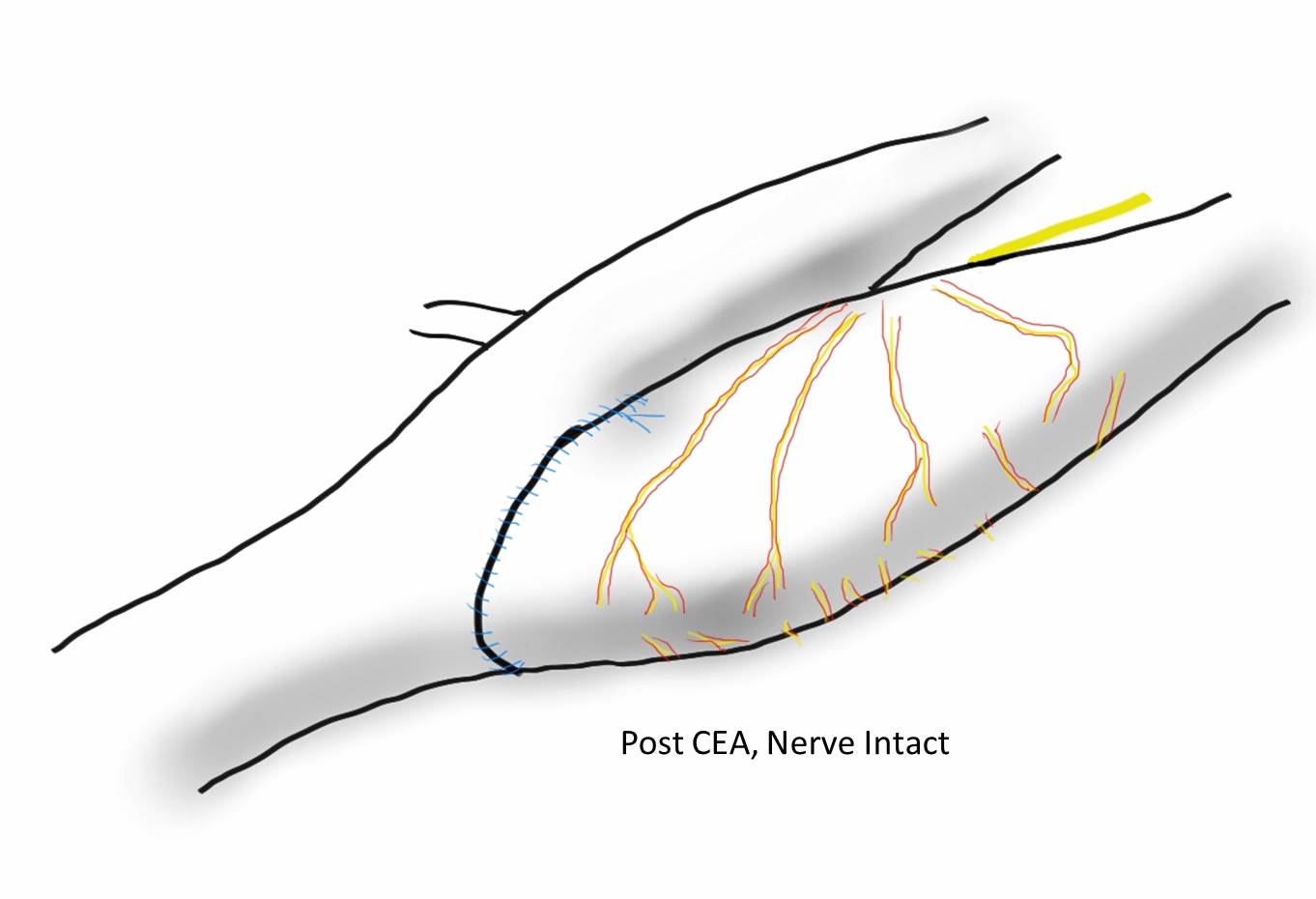
The plaque can be removed without stripping the carotid sinus nerves, resulting in restoration of the sinus/baroreceptor complex.
This would result in bradycardia/hypotension, which I have observed in a percentage of my eversion endarterectomy patients. Cutting the nerves results in hypertension, and was the subject of a paper from Montefiore (reference).
However, the proximal ICA at the carotid bifurcation was mobilized circumferentially to facilitate its transection from the CCA at the carotid bulb. During this approach, carotid sinus nerve fibers derived from the glossopharyngeal nerve and innervating the carotid body within the adventitia of the proximal ICA were routinely divided (Mehta et al.)
In that paper, hypertension was seen in 24% of patients undergoing eversion CEA with denervation compared to 6% undergoing standard endarterectomy, and as an aggregate occured for a prolonged period of time:
The hypotension and bradycardia that I observe in nerve sparing eversion endarterectomy appears to be transient, but it is my unstudied observation that some of these patients subsequently have a lower need for blood pressure medication. This will deserve further study, but may explain the variable results of denervation procedures aiming to control hypertension. To some extent, all blood vessels are innervated and provide an aggregate signal to the CNS. Without understanding the central pathways of hypertension, the baroreceptors offer the best way of controlling blood pressure without medication like lighting a flame under a thermostat to get the building colder.
I was asked to assist one of my otolaryngology colleagues in extirpating a neck tumor that encroached on the carotid artery at the base of the skull early in my career. While the operation was complex and interesting, the most impressive part of it was the complete exposure of the neck from base of skull to the base of neck that was possible with an oblique skin line incision. This challenged bias I had about “exposure,” because up to that time, I had done the mastoid process to manubrium incision along the anterior border of the sternocleidomastoid muscle. What was doubly remarkable was that the incision was invisible in followup despite curling from ear to epiglottis because it was hidden in the fold under the submandibular fat.
This patient above had his carotid endarterectomy performed with a skin line incision. He didn’t even need his beard shaved for the operation.
The key is developing subplatysmal flaps like the kind you make with thyroidectomy. This allows cephalad and caudad exposure. More exposure means just extending the incision medially and laterally. These flaps heal well. This with retraction allows for excellent exposure of the neck.
The other advantage is that the fat is never cut across but completely avoided if you go under it and lift it up. The incision is far less disfiguring and heals well because the forces co-apt the skin without relying on tension from the closing sutures. Preop planning with CTA and 3D virtual reconstruction confirm where the incision should be placed. But most of all, the patients appreciate not having a scar on the neck that they have to constantly explain.
Planning starts with visualizing the proximal and distal extend of plaque needed to be removed.
The 3D reconstruction view can be “Window Level”-ed to bring in soft tissues and skin to anticipate the operative exposure.
Experience has shown me that it is possible to avoid cutting through the fat on the neck, and what is visually the lower part of the face as much as it is the neck, but performing this oblique incision in the skin fold.
The patient, a 47 year old woman, was referred for syncope, but it was much worse than that. Excessive stress, standing, and thinking hard were described as causes of her syncope. Frequent headaches and lethargy lead to inability to keep a job. Several MVA’s resulted in revocation of her driver’s license. Added to that was a two to three pack a day cigarette habit. Her cardiac workup was negative, but it was noted that her carotid duplex was notable for a left ICA occlusion and left vertebral occlusion. Blood pressure in both arms was in the 70’s systolic while in her better thigh it was 90’s. She had an open right carotid system but the flows in the common carotid were attenuated. CTA of the arch revealed severe arch disease affecting the origins of her great vessels. The innominate artery was severely diseased to its bifurcation with a small <2mm channel of flow. She had a dominant right vertebral artery that was patent, and the right ICA had moderate disease at its origin. This was in 2009, and I entertained intervention, but wasn’t all that confident that kissing stents into the innominate was all that great of an option even though there are reports of innominate interventions in the literature. I had the opportunity to perform a handful of great vessel reconstruction with Ken Cherry during my fellowship and felt that this was an ideal case for an innominate endarterectomy.
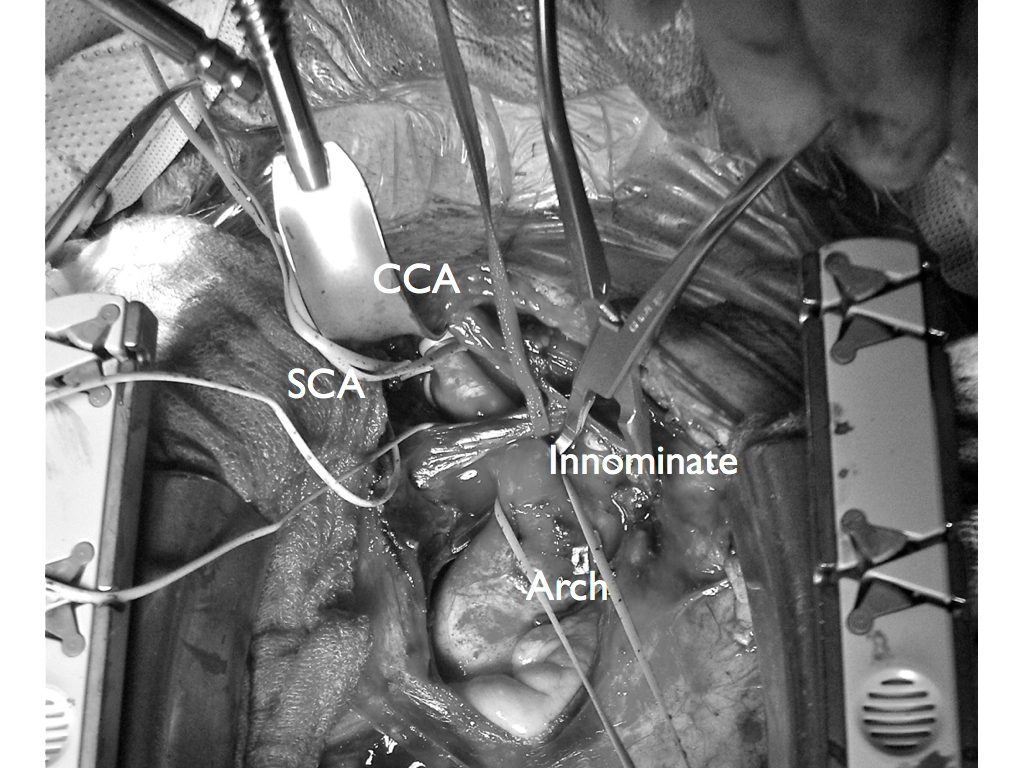
This is one of those rare and infrequent cases from vascular surgery history. The exposures is one of the grand vistas of vascular surgery. The arch, thankfully, was only calcified at the origins of the vessel and clamped well. The endarterectomy was not that much different from an aortoiliac endarterectomy with a fibrocalcific plaque and was extended onto the common carotid while the origin plaque of the subclavian was plucked cleanly. The phrenic and vagus nerves were protected. The patient was centrally hypertensive as found by a long femoral arterial line and was kept that way for the duration of the clamp. A bovine pericardial patch was applied and the sternum was closed over a mediastinal chest tube.
The recovery was impressive for the patient’s immediately improved state of consciousness, lack of lethargy, and improved cognition. She was herself impressed enough to quit smoking during that admission for good. Her right brachial cuff pressure now correlated well. She went home POD 5. When I last saw her 2 years later, she was employed and symptom free with continued patency of her repair, consistent with the earlier reports of this operation (Cherry et al. J Vasc Surg; 989;9:718-14).
Maybe it’s the way the the bilateral dorsal aortas resolve into an asymmetric arch, but there is asymmetry in the carotid arteries which lets me look at a lateral carotid arteriogram and reliably predict which carotid artery it is. Image I is the usual conformation of the right ICA takeoff which may be tucked ,medially and posteriorly toward the pharynx. Image II is the typical forked appearance of the left ICA, and because it is longer and the plaque usually ends at the bend, this makes an eversion easier on that side. I began noticing this when I was on the CVRx trial applying stimulator leads on the carotids.








 which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were:
which in my experience is highly morbid despite how stable the patient was. Point again to trainees, this is no different from someone having stabbed this patient with a knife at the base of the neck. My options were: