Patient with infected femoral pseudoaneurysm, skin necrosis, about to blow
A surgeon from Nepal posted a case of a ruptured common femoral pseudoaneurysm infected from IV drug abuse on LinkedIn. The comments centered around typical textbook responses which were:
Ligate, debride, obturator bypass
In situ bypass with femoral vein +/- sartorius flap
Rifampin soaked graft or crypreserved allograft
Ligate only
My preferred treatment is #2, in-situ bypass with harvest of adjacent deep femoral vein. I never liked that procedure because in general in these patients, everything bleeds. Then I had a thought -how about if you mobilize the external iliac artery in the pelvis over its entire length and pull it out from under the inguinal ligament to sew to the femoral bifurcation or SFA? That is, when you enter the pelvic retroperitoneum to gain proximal control:
The external iliac artery is usually redundant and elastic in young people
You mobilize the external iliac artery from the iliac bifurcation to the inguinal ligament, detaching the inferior epigastrics as a last step. And then you pull it out from under the inguinal ligament, and anastomose it to the femoral bifurcation or the SFA.
The mobilized external iliac artery is pulled down to reach normal femoral artery. The distance x is the length of CFA that needs replacing
This makes sense because in young people and those with AAA and minimal atherosclerosis, the external iliac artery is both redundant and elastic, making it suitable for a pull down transposition. But then, how do you know as you mobilize the artery in the pelvis that you have enough to pull down?
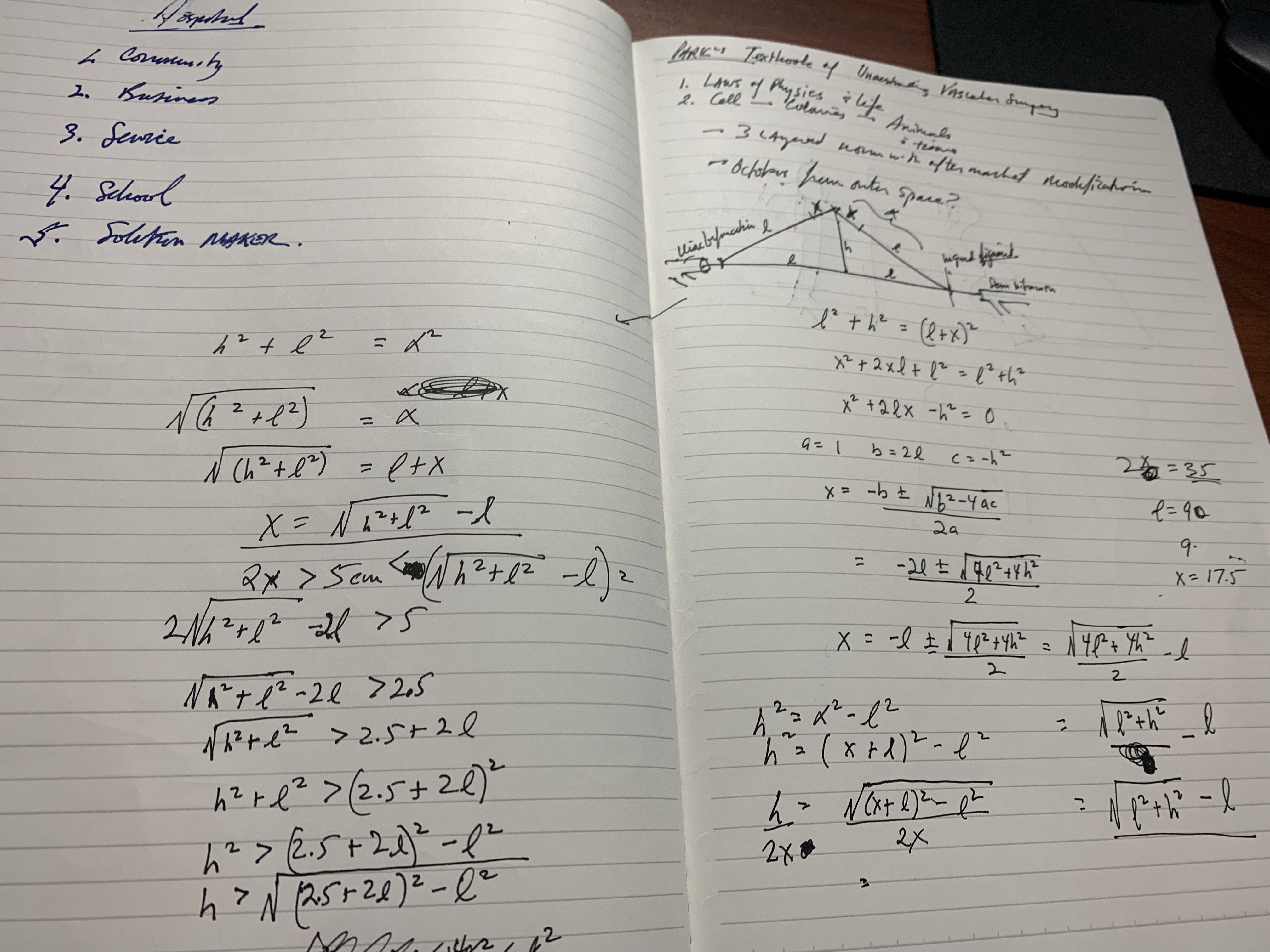
Pythagoras figured that out two an a half millenia ago. If you measure the straight line distance from iliac bifurcation to the takeoff of the inferior epigastric arteries, you get the straight line external iliac artery distance. The length of the common femoral artery which is the excess EIA length needed, is assigned the value x. Then the height of the stretched artery off the line between the iliac bifurcation and the inguinal ligament will determine how much extra artery you have.
Taking these values, I did some maths.
The solution for h, the height, is highlighted in yellow below. (note, the variable x in my notes is half the length of CFA, l is half the length of EIA, ie. 2x is CFA length).
Creating a spreadsheet for CFA lengths from 2 to 6cm and EIA straight distances of 5-10cm, the ratio of height H to CFA length varies from a minimum of 0.7 to maximum of 1.7 with an average of 1.1. That means the majority of the time, if you get 1.5x the length of CFA height off the pelvis, you should reach.
If you are short, you can detach the profunda and mobilize the SFA, pulling upwards, then reattach the PFA. Though this is entirely a thought experiment, there is no reason why it should not work. As with most things, I predict that it already has been done!
The advantages are using autologous tissues and leveraging the natural anatomy. There is a cost benefit in that OR time is shorter with less time for venous harvest and avoiding grafts, patches, and devices. The patient would avoid ischemia as would happen in the staged repair. The disadvantage is when you are short, but if you mobilize the appropriate amount (height off pelvis at least 1.5x the CFA length) you should be okay. The more curvature and tortuosity seen on 3DVR recontstruction and absence of significant atherosclerosis would predict feasibility.
One of the greatest surgical texts, Cope’s Early Diagnosis of the Acute Abdomen, is something every surgical resident, vascular or general, should read. The mid-century edition which I owned during my residency, has since been updated, but the central message of the book is this: every complaint or pain the patient has comes from a nerve, either peripheral or visceral, and understanding the nature of the pain, you narrow the diagnosis to only a few possibilities. Irritation of the psoas muscle results in a characteristic pain that years of diagnosing appendicitis the old fashioned way -by exam, then operation, makes it easy to recognize, like Marilyn Manson showing up as your substitute teacher (I would have said Alice Cooper, but that completely dates me). When the psoas muscle is irritated, by a hematoma, injury, inflammation, or abscess, the muscle relays intense pain localized to the retroperitoneum. Stretching the muscle worsens the pain, and the patient is often seen with the ipsilateral hip flexed. The genitofemoral nerve which rides on top of the psoas, is triggered and there is pain referred to the groin and proximal anterior thigh. Seeing this, and fitting the story allows for a diagnosis, before imaging. Without this insight, there is no swift vector to treatment and resolution.
Patient with inability to straighten left hip after iliac stent placement
The patient, a middle aged man, had undergone a redo-iliac angioplasty and stent for left iliac in-stent restenosis. He relayed that on the table, he felt immediate left lower quadrant abdominal pain and the desire to flex his left hip. He was restrained, sedated, and the procedure finished -a covered stent had been placed. When he came to my office a month after his initial procedure done elsewhere, he was in wheel chair, unable to straighten his leg. He claimed before coming to see me, he had gone to another hospital, where he had a CT scan and was told nothing was wrong (will have to confirm). He was having subjective fevers at home.
On examination, he sat on the exam table with left hip flexed. His pedal pulses were easily palpable. He had furuncles in his groins which he relayed he had had all of his life. I sent him for CTA and subsequently admitted him for surgery.
left iliopsoas abscess
The CT showed a large collection around the left iliac artery and stents and on the psoas muscle, an abscess. The blood cultures on admission were positive for Staphylococcus lugadensis sensitive to penicillin.
Putting the story together after the fact is much easier than when you are in the moment, but being aware of the location and type of pain should give you a clue. Very likely, he had a brief rupture on the angiosuite table resulting in his sudden pain, drowned out by the sedatives typically given in response to a patient moving when a stent is deployed. Inflating a balloon in an artery typically causes some discomfort -as the vessels are lined with visceral nerve fibers which are quite sensitive but less localizable than say a pin poking on the index finger. If you ever had bloating with gas, that general discomfort localizable to the mid abdomen, that nausea and discomfort is from stretched visceral pain fibers. If you have ever had dull aching pain of distended spider veins, that is visceral pain. It’s there, but you would not be able to pinpoint it exactly. That is not what this patient had when he flexed his hip on the angio suite table. While the covered stent was deploying, he likely briefly ruptured causing both somatic and visceral pain around his left common iliac artery and iliopsoas muscle. Additionally, if the sheath had been entered through an area of a skin abscess, likely the sheath, wires, and gloves were contaminated. Any handling of the balloon expandable stent graft, which I highly discourage, would have contaminated it, resulting in a device infection, which was made more likely due to his diabetes. As the hematoma got infected, it resulted in the worsening symptoms he was having of left lower quadrant abdominal pain, groin pain, thigh pain, and inability to straighten his hip without pain.
I took him to the operating room and drained his abscess, assisted by Dr. Andrew Tang, chief resident headed to CT Surgery fellowship here at the Clinic, and Dr. Jenny Chang, PGY 2 Surgery. I gave Dr. Chang a copy of Cope’s with the admonition to read it soon and pass it on, as most of the current generation claim no knowledge of this important text. While I am not against interventional drainage, it takes time to drain the collection through a tube whereas sticking your hand in, sampling the collection, observing the injury, and breaking up collections and washing out with brown-bubbly -a mix of betadine/peroxide diluted in saline, I believe speeds the recovery from the infection. His drainage was done through a retroperitoneal approach from the left side and notably, his psoas muscle while viable, did not retract to cautery energy, suggesting some degree of rhabdomyolysis. The iliac artery was an indurated, thickened, and hard from the calcium and plaque that was the original problem affecting his distal aorta and iliac arteries (see left arteriogram centerline). I placed a pair of JP drains, removed one that wasn’t draining much on POD #3, and the other about a week after discharge on POD#5. His WBC elevation which was never high promptly resolved. I kept him on oxacillin with consultation from ID, and waited. After 3 weeks, I repeated his CTA.
His right iliac centerline showed patent stent with diffuse plaque and calcium starting in mid infrarenal aorta.
His abscess had significantly resolved and his pain was gone. He was ambulating again.
Before and after abscess drainage
The choices at this point were the following
Continue treatment of patient with supressing antibiotics for life
Resection of left iliac stent graft which is presumed to be infected
If resection chosen, the options for repair that I considered included:
NAIS (ref 1). Neoaortoiliac System graft using femoral vein
Aortoiliac homograft
Rifampin soaked gelatin coated graft (ref 2)
Extra-anatomic bypass with axillofemoral bypass or femorofemoral bypass.
Aortoiliac endarterectomy and repair with bovine pericardial patch and graft
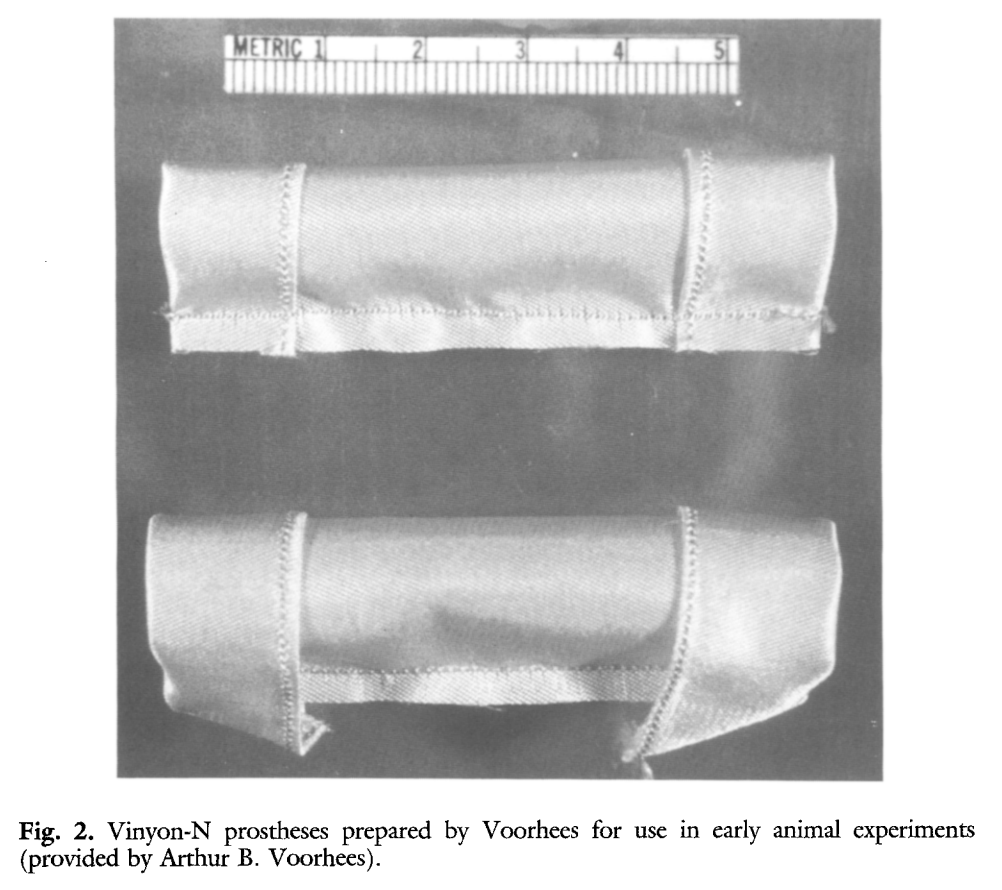
The choice of replacement is becoming clearer in that while rifampin soaked grafts offer immediacy and expedience, all grafts seem to be prone to reinfection at a higher rate than autologous material (ref 3). The NAIS bypass is a great option, but is hampered by the addition of several hours invested in harvest of the femoral veins. While it can be staged with mobilization done one day and harvest another, those added hours add complications. We often forget that the simple metric of procedure time is the most important determinant of complication rate. Any operation going over 2 hours risks wound infection for example simply from ambient colonization of the open wounds from the rain of dead skin from the surgeon’s face, aerosolized fecal flora from flatii (prohibited in my ORs). The microenvironment of the open wound is also room temperature and not 37, having an impact on organ function and hemostasis. The homograft is the original aortic graft -before Arthur Voorhees invented the cloth vascular graft as a resident at Columbia P&S (my medical school alma mater, ref 4), major hospitals had tissue banks of aortic homografts harvested from the recently deceased. Having homografts is now an outsourced function, but does require having proper refrigeration for the cyropreserved grafts and generally can’t be ordered with short notice.
Rifampin soaked grafts work well, especially wrapped in omental flap, in the short and medium term but suffer a reinfection rate that is higher than seen with autologous tissues, and prosthetic grafts without rifampin, such as PTFE for extraanatomic bypass, have the highest rates of reinfection (3), despite being the board answer decades ago.
Endarterectomy allows for use of native tissues for repair. The adventitia around plaque and stents, while thin, can support physiologic pressures, even when they have been occluded for years. And while practice of aortoiliac endarterectomy is a bit of a lost art, it has both a long history stretching back nearly a century and a modern track record with carotid and femoral endarterectomy. It is merely a matter of scale. Pinch and zoom in on a femoral endarterectomy at the bifurcation and you have the same case as with an aortic one.
The question is, is bovine pericardium more autologous than prosthetic? It is a decellularized sheet of collagen from a cow’s pericardium, used in heart valves and vascular patches, but only recently applied as a graft (ref 5-7). I have long used bovine pericardium as a patch with some caution, but the rule of thumb is are there well vascularized tissues around it? A layer of Scarpa’s fascia and fat in a groin wound are not sufficient to protect a bovine patch, but a sartorius flap is. For me, once the infected stent graft is out, knowing if the surrounding tissues bleeds well is an important one.
I chose to do aortoiliac endarterectomy. The patch and graft would be made with bovine pericardium, unless I found the left iliac segment to be devitalized and foul with anaerobic vapors, then, I would close and go NAIS or extra-anatomic. The key point is that choices have to be on the table and constantly rearranged during the conduct of the operation.
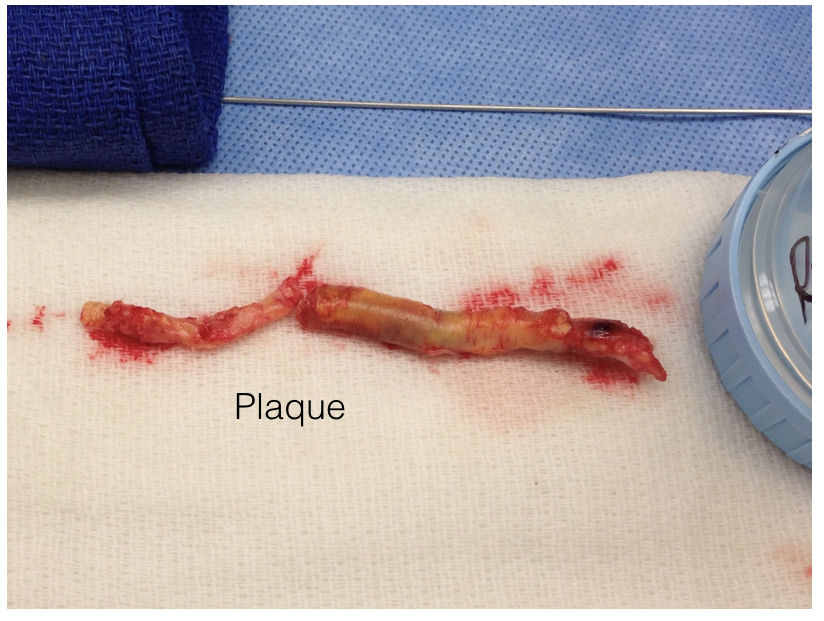
The patient was preoperatively vein mapped and had suitable deep femoral vein for bypass conduit, having robust duplicated systems that would impact the patient minimally. The patient was placed in a supine position and via a midline laparotomy, the infrarenal aorta and the common iliac arteries beyond the short iliac stents exposed. I chose this limited exposure as any further into the phlegmon on the left risk injury to ureter and vein. The aorta had a palpable demarcation between plaque and mildly diseased proximal segment, predicted by the CTA to be at the IMA. A longitudinal arteriotomy was created on the right side from mid aorta to mid right iliac, and the left side had a separate arteriotomy to release the stent. The plaque came out in a single specimen (image).
The exposed stent is the left iliac stent holding within a stent graft.
The left iliac artery was destroyed by the infection but the tissues around it bled avidly and were not foul or infected. I avoided excess debridement here as the iliac vein was intimate with the phlegmon. There was a 3cm gap. Again, I thought briefly about taking femoral vein, but proceeded to make a graft from the bovine pericardium. This was sewn around the rod portion of a renal vein retractor from the OMNI set. The finished product resembled Voorhees’ graft. It was sewn into the orifice of the iliac from inside the aorta and end to end to the freshened iliac stump. Unfortunately, the omentum was atropic across the transverse colon, but the tissues around the resected artery and stent graft bled well, indicating good penetration of antibiotic. The retroperitoneum was closed after hemostasis obtained. Dr. Shashank Sharma, our chief resident headed to a vascular surgery fellowship at the renown Houston Methodist next year got to see what is unfortunately a rare occurrence -an aortoiliac endarterectomy, which through me puts him three degrees of separation from Cid Dos Santos (ref 8). Dr. D’Andre Williams, PGY-2 Vascular Surgery Resident, got important lessons on sewing the aorta. She’s part of a fortunate cohort that get exposed to open aortic surgery at our main campus which is unfortunately rare throughout the world.
The pericardium was soaked in rifampin, but probably did not bond to the collagen.
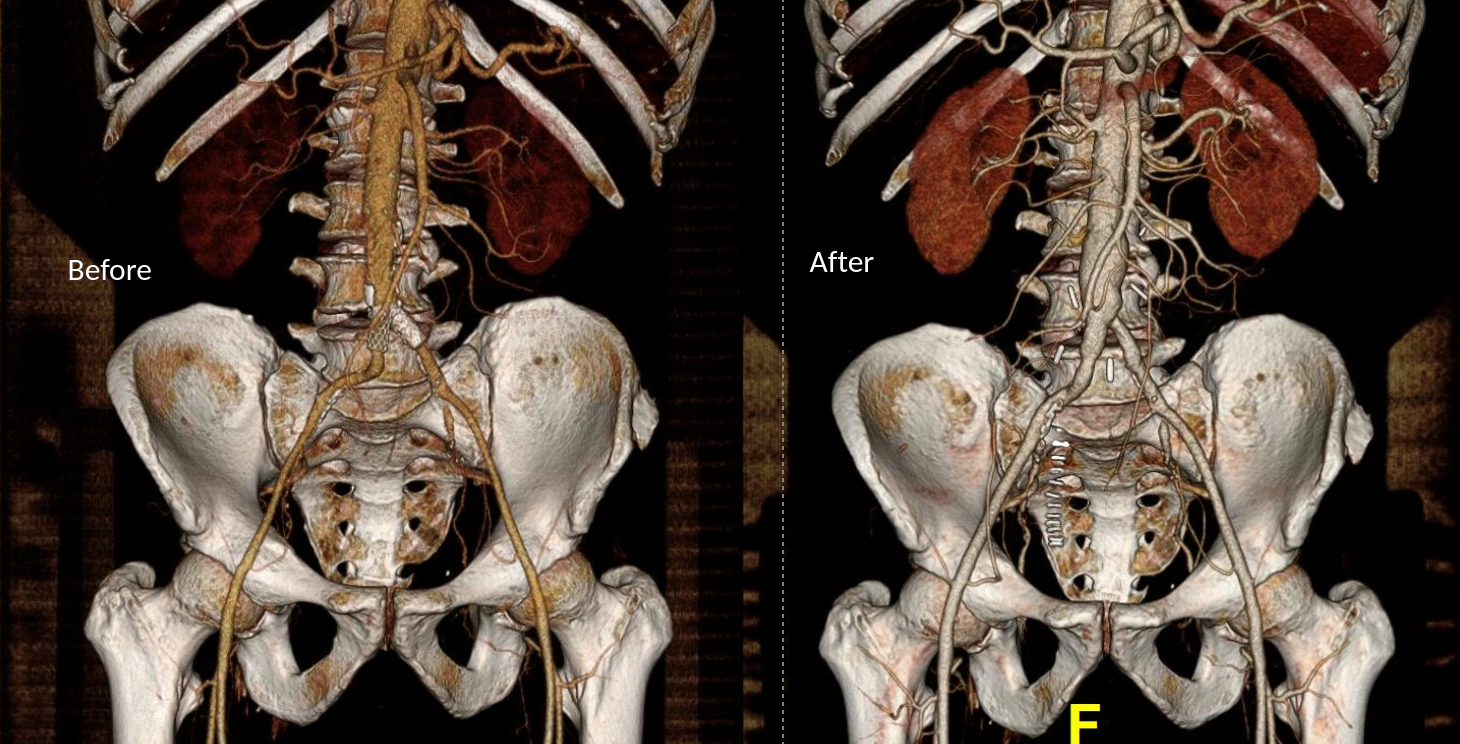
The final graphic shows the operative end result.
The patient recovered well and was discharged within the week with another month of IV antibiotics planned.
Before and After
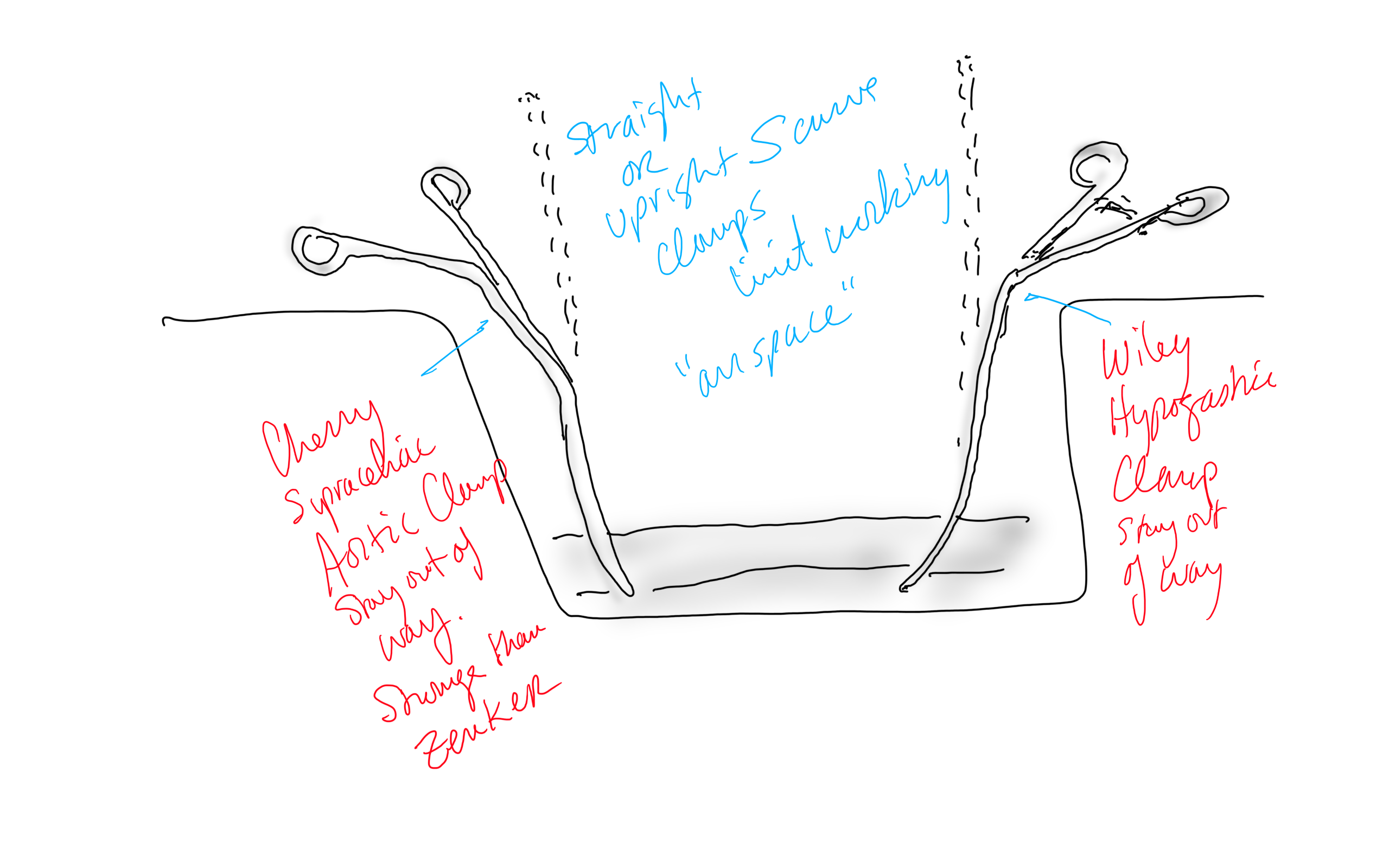
Conclusion: The operation was started at 8 in the morning and was done by lunch time. For aortic cases, this is a crucial metric, as when the clock winds past the surgeon’s comfort, the patient suffers even more. Adding the femoral vein for a NAIS may have been the textbook thing to do, but we don’t do extra-anatomic bypasses that much either. I don’t believe that adding two more hours for retrieving the femoral vein would have enhanced the procedure, and would have served to add potential areas for complication. Technically, the aorta closes much as with a carotid or femoral endarterectomy, but the adventia is thin and really should be sewn with 5-0 or 6-0 Prolene. The larger needles such as the SH size creates unnecessary bleeding unless sewn with a line of felt which could become infected. Despite the thinness, it will hold pressure if it is not infected. Clamps that bend out of the “airspace” above the laparotomy, such as the Cherry Supraceliac Clamp and Wiley Hypogastric Clamp, prevent limiting the operative space with long clamps such as aortic Fogarty or DeBakey clamps, while being stronger than the Zenker.
A final comment for Staphyloccocus lugudensis. This is the second major vascular graft infection with this organism I encountered this year. The other was an infected aortic stent graft. Lugudensis means from Lyons. I do not know why that is, but it is so far not the nasty player that is S. aureus. I am sure it will share some plasmids, and become resistant one day, but in the earlier case in Abu Dhabi and now this, it is sensitive to penicillin, and came from the skin at the femoral puncture site, and for this we are fortunate. Major vascular infections are one of the few areas that still demand open surgical skills, and we foresake them at great peril. It’s critical to remember all the collective memory of surgery from the past, or we will become mere technicians fixing whatever comes out of the radiologist’s report with whatever knowledge obtained from a Zoom meeting for the latest, greatest device.
Acknowledgement
Gratefully, the patient gave his permission, as with all patient, for use of his case for educational purposes.
References
Chung J, Clagett GP. Neoaortoiliac System (NAIS) procedure for the treatment of the infected aortic graft. Semin Vasc Surg. 2011 Dec;24(4):220-6. doi: 10.1053/j.semvascsurg.2011.10.012. PMID: 22230677.
Oderich GS, Bower TC, Hofer J, Kalra M, Duncan AA, Wilson JW, Cha S, Gloviczki P. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011 Jan;53(1):99-106, 107.e1-7; discussion 106-7. doi: 10.1016/j.jvs.2010.08.018. PMID: 21184932.
Smith RB 3rd. Arthur B. Voorhees, Jr.: pioneer vascular surgeon. J Vasc Surg. 1993 Sep;18(3):341-8. PMID: 8377227.
Almási-Sperling V, Heger D, Meyer A, Lang W, Rother U. Treatment of aortic and peripheral prosthetic graft infections with bovine pericardium. J Vasc Surg. 2020 Feb;71(2):592-598. doi: 10.1016/j.jvs.2019.04.485. Epub 2019 Jul 18. PMID: 31327614.
Lutz B, Reeps C, Biro G, Knappich C, Zimmermann A, Eckstein HH. Bovine Pericardium as New Technical Option for In Situ Reconstruction of Aortic Graft Infection. Ann Vasc Surg. 2017 May;41:118-126. doi: 10.1016/j.avsg.2016.07.098. Epub 2016 Nov 27. PMID: 27903471.
Belkorissat RA, Sadoul C, Bouziane Z, Saba C, Salomon C, Malikov S, Settembre N. Tubular Reconstruction with Bovine Pericardium Xenografts to Treat Native Aortic Infections. Ann Vasc Surg. 2020 Apr;64:27-32. doi: 10.1016/j.avsg.2019.10.104. Epub 2020 Jan 10. PMID: 31931127.
Barker WF. A history of endarterectomy. Perspectives in Vascular and Endovascular Therapy. 1991;4(1)1-12. doi:10.1177/153100359100400102
If you work long enough, you will not only see everything, but you may end up doing something that you say you would never do. You will be confronted with a scenario that would test not just your skills but also your boundaries. The adage, never say never is a warning that all of us may face a choice -to remain rigidly consistent with some earlier proclamation or to excuse a little hypocrisy for the sake of the patient.
At one point in recent years, I saw a patient who had an axillary artery to anterior tibial artery bypass with PTFE (figure above). That was a kind of marvel to me, but my initial response was a bit of a sneer.
“Who does this?” I thought.
Giving it some thought, the rationale could have been to spare the patient from a hip disarticulation as the patient had had failed revascularizations and was occluded from the infrarenal aorta to the anterior tibial artery on that side. If you see such a thing, it sparks wonder as it feels both wrong and splendid at the same time because some surgeon had the audacity to pull it off. By the time I saw it, the patient had avulsed the proximal anastomosis, infarcted their leg to their thigh, and was headed for a hip disarticulation, four years after the creation of the bypass. Four years of patency!
It was no wonder I remembered this case when this middle aged man presented to our clinic with a gangrenous right third toe. He had diabetes, hypertension, CAD with prior PTCA, prior acute mesenteric ischemia with bowel resection with an SMA stent, CHF with moderately reduced EF, CKD, and aortoiliac occlusive disease treated in past with aorto-bi-iliac bypass, left to right fem-fem bypass complicated by graft infection requiring resection of the fem-fem bypass, with subsequent development of rest pain on left leg and gangrene on right leg. He had been told at his home institution that he required eventual bilateral hip disarticulations. At the time of consultation, he was minimally ambulatory, limited by severe pain. He had been this way for over a year.
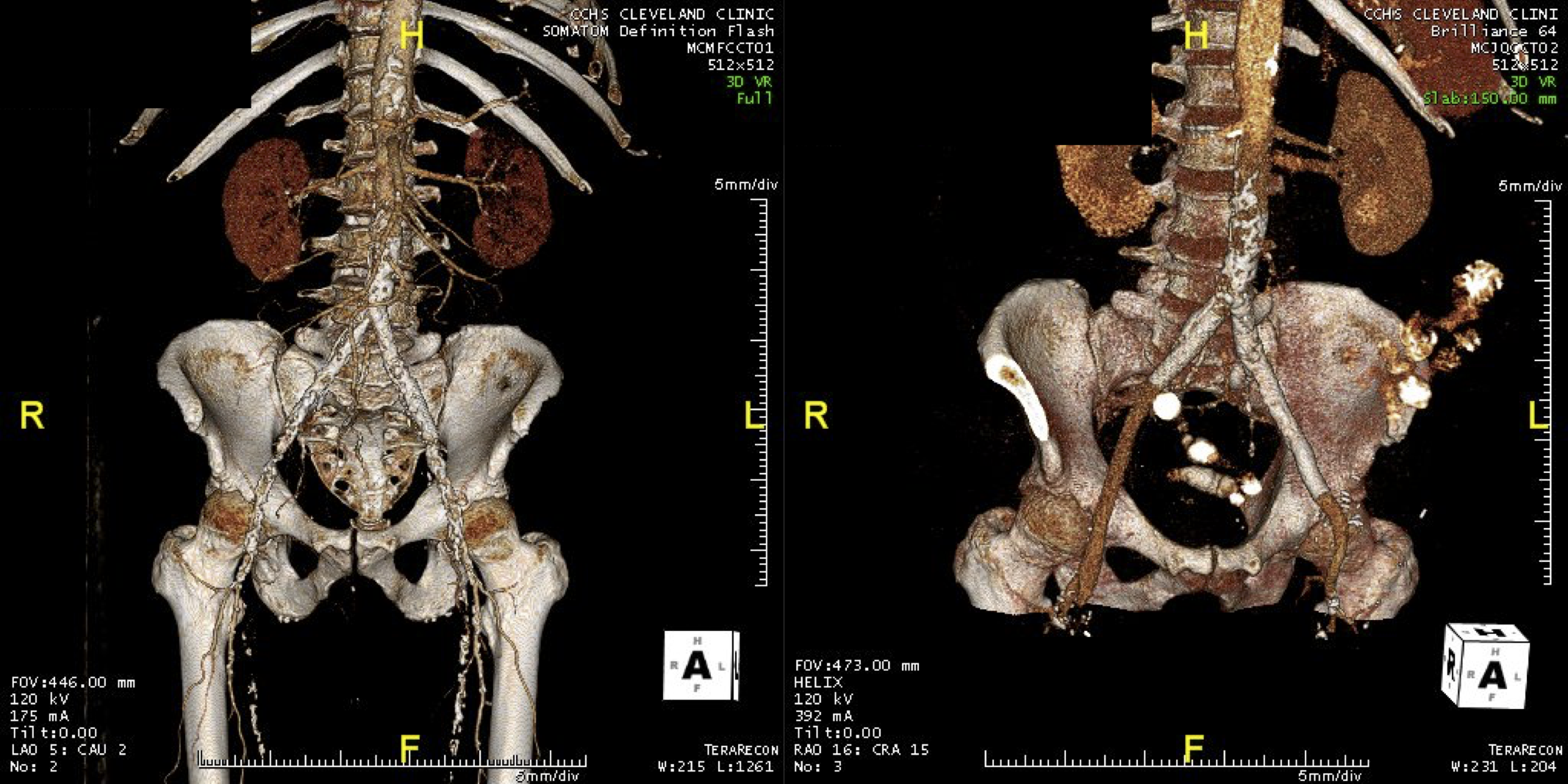
On examination, he had heavy scarring in both groins from prior open incisions healed by secondary intention, a midline laparotomy incision. He had weak bilateral axillary and brachial artery pulses. He had no pulses in either leg. The right foot had gangrene of the distal phalanx of the third toe. The both feet were anemic and painful -the left foot had more dependent rubor. Pulse volume recordings were flat in both legs. TCPO2 was in the 20-40mmHg range at the thighs bilaterally suggesting reduced potential for healing an above knee amputation. Vein mapping showed no suitable saphenous vein in either leg. CTA (figure below) showed both external iliac arteries to be occluded or absent and the common femoral arteries to be occluded or missing bilaterally.
The left femoral bifurcation was preserved and the left SFA was patent into small underfilled tibial vessels. On the right, there was an isolated segment of profunda femoral artery that reconstituted from pelvic collaterals. The right below knee popliteal artery reconstituted and had underfilled but patent three vessel runoff (figure below).
posterior view of right popliteal reconstitution
The patient was admitted for workup and treatment. Heparin drip was started. In the setting of rest pain, I find that heparin drip improves circulation and symptoms even though it shouldn’t. I don’t have a great explanation for this, but it does, and I would welcome comments. To better assess how much operation the patient could tolerate, a cardiac risk assessment was performed. He was deemed a moderate to severely elevated risk due to his EF of 35% but had a normal nuclear stress test.
The options I presented to the patient were
1. Hip disarticulations
2. Bilateral above knee amputations with a wait and see approach to hip disrticulation
3. Sympathectomy
4. Axillo-profunda or popliteal bypass on right and Axillo femoral bypass on left
5. Ilio-right popliteal and left femoral bypass.
6. Thoracic or supraceliac aorta to right profunda and left femoral bypass
Hip disarticulation is the bogeyman of leg amputations done for peripheral vascular disease. When done for trauma or cancer in young people, the ability to rehab and walk again is excellent. When done for tissue loss in elderly, non-ambulatory patients, the reported mortality of the operation rises to above 50%. It is usually posed as a lead in to comfort measures. The above knee amputations were not likely to heal despite the neither here nor there findings of the TCPO2 which is only good when the results or normal or dismally low. Sympathectomy is an option for those without options, but this patient still had options, I felt.
Any revascularization relies on the choice of inflow, outlow, and conduit. In endovascular revascularizations, the conduit is the previously occluded vessels, but in this instance, because of the infected grafts, there was neither continuity, nor a good option even if there was as the common femoral artery is a terrible recipient of endovascular therapy. The options then devolve to choosing an inflow. The axillary arteries are technically easiest to access and manage and form the basis of treatment of high risk patients requiring limb salvage who have no endovascular options. The axillofemoral bypass is given a bad reputation of having a poor patency, but the key is the quality of the vessels and the number of potential tension, compression, and kink points. I think the reason why the axillary to anterior tibial bypass lasted for four years in the first patient had to do with his immobility, and the pristine nature of the anterior tibial artery -the only patent vessel below his umbilicus. Here to, the inflow disease appears to have spared his right popliteal artery and his left superficial femoral artery.
The only compromise with an axillary artery inflow is the amount of potential flow. In a patient with a 6-7mm axillary artery, the amount of flow going to both an arm and a leg, and a lower torso, would greatly exceed the flow capacity of that vessel. The infrarenal aorta on this man is graft and is relatively inaccessible due to the prior laparotomy for acute mesenteric ischemia, signalling the high likelihood of adhesions. The supraceliac aorta is an excellent inflow source and I have had good results dissecting it out laparoscopically as it is often deep and narrow an exposure to try to dissect open -While the retroperitoneal tunneling can be tricky, it is not insurmountable and good bypasses can result (link).
My eye focused on the left iliac graft which perfused the internal iliac artery on that side. The graft was generous, and likely a dilated 8mm graft, and could be exposed via a left lower quadrant retroperitoneal exposure (the transplant exposure). This would allow me to to then tunnel to avoid the terribly scarred groins. On the right side, the obdurator canal could be traversed into the postioer compartment of the thigh -a graft could be sent to the below knee popliteal artery with a side graft to the tiny profunda femoral artery. On the left, the graft could be tunneled laterally near the insertion of the sartorius muscle and onto the superficial femoral artery. All of the incisions would be made in virgin skin, the only redo dissection being digging out the left iliac graft while avoiding injury to the ureter.
So I proposed a ilio-popliteal bypass. Not quite an axillo-tibial bypass, but almost there. There was some karmic balance being restored by my taking decision. It would be with PTFE all around. I quoted a 5-15% risk of major morbidity and mortality, lifelong anticoagulation, and right third toe amputation. The patient agreed.
sketch of iliopopliteal and iliofemoral bypassrs
The operation was done in a hybrid suite, as should all limb salvage cases. The retroperitoneal dissection was challenging because of the heavy scar tissue around the well incorporated iliac bypass, but with patience, a clampable 3cm segment was achieved. I am a big fan of Wylie hypogastric clamps because they stay out of the way when placed in a tight narrow spot, and for that same reason, I prefer the Cherry supraceliac aortic clamp. They were designed by my mentor, Ken Cherry, and his mentor, Jack Wylie for this kind of operation. A few venous bleeders were easily handled with my ring compressors (below), and I hope to continue this chain of innovation, but I digress.
a Park clamp
The bladder was dissected off the pubis to allow the graft to be tunneled to the right pelvis. A counter incision in the right lower quadrant abdomen and a mid thigh incision mobilizins the anterior compartment muscles to the posterior compartment allowed me to tunnel across the obturator foramen. The obdurator vessels need to be avoided or there will be bleeding. this mid thigh incision allowed exposure of the profunda femoral artery more proximally and allowe the graft to be tunneled anatomically to the below knee popliteal artery for anastomosis. A jump graft was taken off this graft on the thigh to the profunda femoral artery which was small and diseased -no more than 2mm in size. An axillary bypass to this profunda would be doomed to the compromised patency rate published for ax-fem bypasses giving them a bad name. The left superficial femoral artery was exposed and provided outflow to the left iliofemoral bypass which was tunneled far laterally under the inguinal ligament to avoid the scar tissue where the common femoral artery was.
There was immediately multiphasic signal in both feet on release of clamps. After closure of all the incisions and dressings, the right middle toe was amputated.
The patient recently came back for an 8 month followup. His grafts remained patent and he was walking without limitations. Given the high quality of the inflow (large iliac graft), and the amount of decent outflow -the right popliteal and profunda, the left superficial femoral and retrograde to the profunda, gives the patients some surety of longevity for his grafts. These grafts will need lifelong surveillance.
I have since opened my mind a bit about that axillary artery to anterior tibial artery bypass. When given the choice between comfort measures for an otherwise nonambulatory but alert patient and hip disarticulation with its attendant high risk, a bypass from a large axillary artery to a large, relatively disease free anterior tibial artery is not the worst thing that could happen. For that patient, it gave them 4 more years with their family, which in any measure, is priceless. To that patient’s family, that surgeon was a savior.
Drs. Roy Miler and Xiao Yi Teng performing anastomosis on open coversion of an aortic stent graft, now graduated and in practice. A significant part of their open aortic experience is in addressing failing stent grafts.
I recently had to remove a stent graft for infection and got to thinking about how the number of people who could comfortably and confidently manage that has thinned out in the world through the unintended consequence of the medical device market place. In every surgical specialty over the past twenty years, many open procedures were replaced with a minimally invasive option which generally involved adoption of new technology and large costs to the hospital. These newer procedures were touted as easier on the patient while being easier to perform for the average physician than the open procedure that they were replacing. That was the other selling point -that one could do several of these operations in the time it took one open procedure. In most cases, they were at best almost as good as the open procedure but at higher cost.
In the marketplace, minimally invasive always wins. In many specialties it became untenable to practice without marketing these “advanced minimally invasive” skills. Hence, the wide adoption of robotics in urology outside major academic centers -during those years of rapid adoption the surgeons would get flown to a course, work on an animal model, then for their first case a proctor would be flown out and voila -a minimally invasive specialist is born. The problem comes when learning these skills displaces the learning of traditional open surgical skills. In general surgery, it is not uncommon to hear of residents graduating without having ever having done an open cholecystectomy. It is also the case that many vascular trainees graduate with but a few if any open aortic cases. What happens when minimally invasive options run out? Who will do my carotid endarterectomy or open AAA repair?
The first case is an elderly man with an enlarging AAA sac despite having had EVAR about seven years prior. No endoleak was demonstrated but the proximal seal was short on CT. Also, it was a first generation graft which is prone to “peek a boo” endoleaks from graft junctions and stent anchoring sutures. On that last point, I use the analogy of a patio umbrella -after seven seasons, they can leak where cloth is sewn to the metal struts. It is very hard to demonstrate leak of this kind on CTA or duplex ultrasound because they are small. The patient had his EVAR because he was considered high risk for open repair at the time of his operation -moderate COPD, mild cardiac dysfunction. His sac had enlarged to over 6cm in a short time, and therefore open conversion was undertaken. No clinical signs of infection were present. A retroperitoneal approach was undertaken. After clamps were positioned, the sac was opened.
The picture does not show it, but a leak from the posterior proximal seal zone was seen with clamp off. The clamp was reapplied and the graft transected flush to the aortic neck. A bifurcated graft was sewn to this neck incorporating the main body stent graft and aortic neck in a generous running suture. The left iliac limb came out well and the new graft limb sewn to the iliac orifice, the right iliac limb was harder to clamp and therefore I clamped the stent graft and sewed the open graft to the stent graft.
The patient recovered well and went home within the week. He was relieved at no longer needing annual CT scans.
Who needs annual CT scans? Patients with metastatic cancer in remission.
The second patient was an older man referred for enlarging AAA sac without visible endoleak. The aneurysm had grown over 7cm and was causing discomfort with bending forward. He too had been deemed high risk for open repair prior to his EVAR. If he had had an early generation Excluder graft, the possibility of ultrafiltration would be more likely and relining the graft would be reasonable (link). This was again a cloth and metal stent graft which can develop intermittent bleeding from graft to stent sutures, and I don’t think relining will help.
The patient was taken for open repair (above), and on opening the AAA sac, bleeding could be seen coming from the flow divider. It stopped with pressure, but I replaced the graft in a limited fashion from the neck to the iliac limbs as in the first case. This patient did very well and was discharged home under a week.
The third patient was another fellow referred from outside who had an EVAR for a very short and angulated neck, and a secondary procedure with an aortic extension in an attempt to seal the leak had been done. This failed to seal the type Ia leak. This patient too was deemed too high risk for open surgery of what was basically a juxtarenal AAA with very tortuous anatomy.
The patient was taken for open repair, and the stent grafts slid out easily (below).
A tube graft was sewn to the short aortic neck and distally anastomosed to the main body of the stent graft -with pledgets because of the thin PTFE graft material in this particular graft. This patient did well and went home within a week.
All three cases are patients who were deemed originally too high risk for open repair, who underwent EVAR, then underwent explantation of their failing stent graft. Only one involved a patient whose graft was placed off the IFU (short angled neck), but the rationale was that he was too high risk.
What is high risk? In non-ruptured, non-infected explantation of failing stent graft, the mortality is 3% (ref 2) from an earlier series from Cleveland Clinic. With stent graft infection, the 30-day mortality of surgical management from a multi-institutional series was 11% (ref 3) when there was no rupture. From a Mayo Clinic series, stent graft resection for infection came with a 4% 30-day mortality (ref 4). These were nominally all high risk patients at the time of the original EVAR.
Real world risk is a range at the intersection of patient risk and the expertise of the operating room, critical care, and hospital floor teams. The constant factor is the surgeon.
Endografts for AAA disease (EVAR, endovascular aortic aneurysm repair), makes simple work of a traditionally complex operation, the open aortic aneurysm repair. The issue has been the cost and risks of long term followup as well as endograft failure and aneurysm rupture. The Instructions For Use on these devices recommend a preop, a followup 1 month, 6 month, and 12 month CTA (with contrast) and annual followup with CTA for life. These devices were meant to treat high risk patients but high risk patients with limited life spans do not benefit from EVAR (ref 1, EVAR-2 Trial). These have lead the NHS in the UK to propose that EVAR has no role in the elective repair of abdominal aortic aneurysms in their draft proposal for the NICE guidelines for management of AAA (link). While this is a critical discussion, it is a discussion that is coming at least ten years too late. A generation of surgeons have been brought up with endovascular repair, and to suddenly announce that they must become DeBakey’s, Wiley’s, Imperato’s, and Rutherford’s is wishful thinking at best or wilful rationing of services at worst.
In 2006, Guidant pacemakers were recalled because of a 1000 cases of possible capacitor failure out of 28,000 implants for a failure rate of 3.7% -there were 2 deaths for a fatality rate of 0.00007%. EVAR-1 Trial’s 8 year result (ref 5) reported 16 aneurysm related deaths out of 339 patients (1.3%) in the EVAR group compared to 3 aneurysm related deaths out of 333 patients (0.2%) in the OPEN group.
Academic medical centers, behemoths though they are, serve a critical function in that they are critical repositories of human capital. The elders of vascular surgery, that first and second generation of surgeons who trained and received board certification, are still there and serving a vital role in preserving open aortic surgery. My generation -the ones who trained in both open and endovascular, are still here, but market forces have pushed many of my colleagues into becoming pure endovascularists. The younger generation recognizes this and last year, I sat in on an open surgical technique course at the ESVS meeting in Lyons organized by Dr. Fernando Gallardo and colleagues. It was fully attended and wonderfully proctored by master surgeons. This is of critical importance and not a trivial matter. As in the 2000’s when endovascular training was offered as a postgraduate fellowship in centers of excellence, there is no doubt in my mind that today, exovascular fellowships need to be considered and planned and that current training must reinvigorate and reincorporate their open surgical components.
Leriche Syndrome -one of those disease names that adds to our work in a way that an ICD codes and even the “aortoiliac occlusive disease” fails to describe. When I hear someone described as having Leriche Syndrome, I think about a sad, chain smoking man, unmanned, complaining of legs that cramp up at fifty feet, pulseless.
The CT scan will occasionally show an aorta ringed by calcium in the usual places that are targetrs for clamping below and above the level of the renal arteries. Even without the circumferential calcium, a bulky posterior plaque presages the inability to safely clamp the aorta. Woe to the surgeon who blithely clamps a calcified lesion and finds that the rocky fragments have broken the aorta underneath the clamp! The first way to deal with this is to look for ways not to clamp the aorta, by planning an endovascular procedure, but circumstances may necessitate the need to control the aorta despite the unclampability.
The traditional methods of avoiding clamping the calcifed peri-renal aorta are extra-anatomic bypasses including femorofemoral bypass and axillo-femoral bypass. I propose these following options for the consideration when the patient needs a more durable solution while avoiding a heavily diseased aorta.
Not Clamping I:
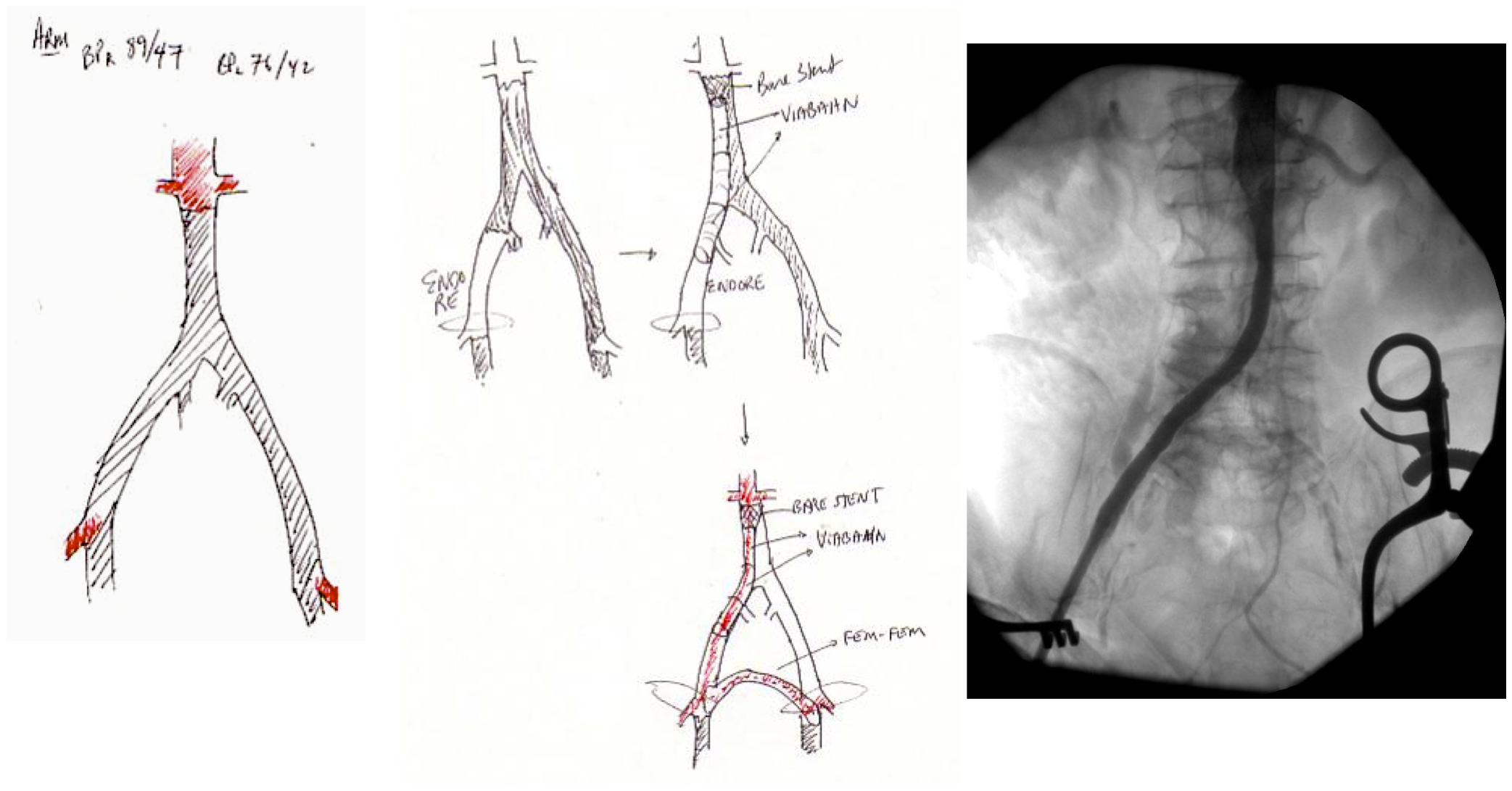
An EndoABF (actually EndoRE-ABF)
EndoABF does work to avoid clamping -these are common femoral endarterectomies supplemented by stenting of the aortoiliac segment, including in those with appropriate anatomy, a bifurcated aortic stent graft. This is often not possible to treat both sides, but one side is usually more accessible. Often, people will compromise and perform an AUI-FEM-FEM, but I have found the fem-fem bypass to be the weak link, as you are drawing flow for the lower half of the body through a diseased external iliac artery. The orientation of the proximal anastomosis is unfavorable and in the instance of highly laminar or organized flow, the bypass is vulnerable to competitive flow on the target leg, leading to thrombosis.
AUI prior to fem-fem bypass for acute aortoiliac occlusion causing critical limb ischemia
The femorofemoral bypass is the option of patients whose options have largely run out. It is made worse when fed by an axillofemoral bypass. Sometimes, you have no choice, but in the more elective circumstance, you do.
Not Clamping II:
The second method is performing a aorto-uni-iliac stent graft into a conduit sewn end to end to the common iliac aftery, oversewing the distal iliac bifurcation.
The conduit is 12mm in diameter, the key is to deliver the stent graft across the anastomosis, sealing it. The conduit is then sewn to the side of a fem-fem bypass in the pelvis, maintaining antegrade flow to both legs. The other option is to sew the conduit to a 14×7 bifurcated graft. Illustrated above is this 12mm conduit sewn end to end to the diseased common iliac artery with wire access into the aorta and a aorto-uni-iliac device. Typically, a small AUI converter (Cook, Medtronic) can be used, but the aorta is often too small even for a 24mm device, and an iliac limb with a generous sized docking segment (Gore) ending in a 12mm diameter fits nicely. Below is a CTA from such a case, where the stent graft is deployed across the anastomosis, sealing it off from anastomotic leaks (exoleaks).
Not Clamping III:
Often, the infrarenal aorta is soft anteriorly and affected only by posterior plaque at the level of the renal arteries. While a clamp is still not entirely safe (I prefer clamping transversely in the same orientation as the plaque with a DeBakey sidewinder clamp), a balloon is possible. I do this by nicking the aorta -simple application of a finger is sufficient to stop the bleeding if you have ever poked the ascending aorta to place cardioplegia line.
A Foley catheter is inserted and inflated. The Foley’s are more durable and resist puncture better than a large Fogarty. This is usually sufficient for control, although supraceliac control prior to doing this step is advised. The aorta can be endarterectomized and sewn to the graft quite easily with this non-clamp.
This has worked well, Although pictured above with an end-to end anastomosis planned, it works just as well end-to-side. I actually prefer end to side whenever possible because it preserves the occluded native vessels for future intervention in line.
The Non-Thoraco-Bi-Femoral Bypass
The typical board answer for the non-clampable aorta is taking the inflow from the thoracic aorta or from the axillary artery -neither of which are good options. The first because the patient is positioned in right lateral decubitus and tunneling is not trivial. The second because of long term durability. The supraceliac aorta, technically it is the thoracic aorta, is often spared from severe plaque and clampable. Retropancreatic tunelling is straightforward, and a 12 or 14mm straight graft can be tunelled in this fashion from the lesser sac to the infrarenal retroperitoneum. It then sewn to the supraceliac aorta and then anastomosed to a 12x6mm or 14x7mm bifurcated aorto-bifemoral bypass, of which limbs are tunneled to the groins.
This worked very well recently, allowing a middle aged patient with severe medical problems, occluded aorta and iliac arteries, with critical limb ischemia, survive with minimal blood loss and home under 5 days. It delivers excellent flow to both legs in an antegrade fashion. Dr. Lew Schwartz gave me a list of references showing that this is not novel, but represents a rediscovery as the papers were published in the 80’s [reference], and buttresses the principle that innovations in open vascular surgery are exceedingly rare, largely because we have been preceeded by smart people.
Conclusion: All of these come about through application of some common sense and surgical principles. The most important this is that the aorta is the best inflow source and reconstructing it with the normal forward flow of down each leg and not reversing directions as in a fem-fem bypass gives each of these options a hemodynamic advantage.
References for Supraceliac Aorta to Lower Extremity Bypass
Surgery [Surgery] 1987 Mar; Vol. 101 (3), pp. 323-8.
The principles of salvage are in rescuing valuable undamaged goods in the setting of catastrophe. This guided me when a patient was flown in from an outside institution to our ICU with a saline soaked OR towel in his right groin -he had had an aorto-bifemoral bypass for aorto-iliac occlusive disease a year prior, but had never properly healed his right groin wound which continued to drain despite VAC therapy and wound care. On revealing his groin, this is what I saw:
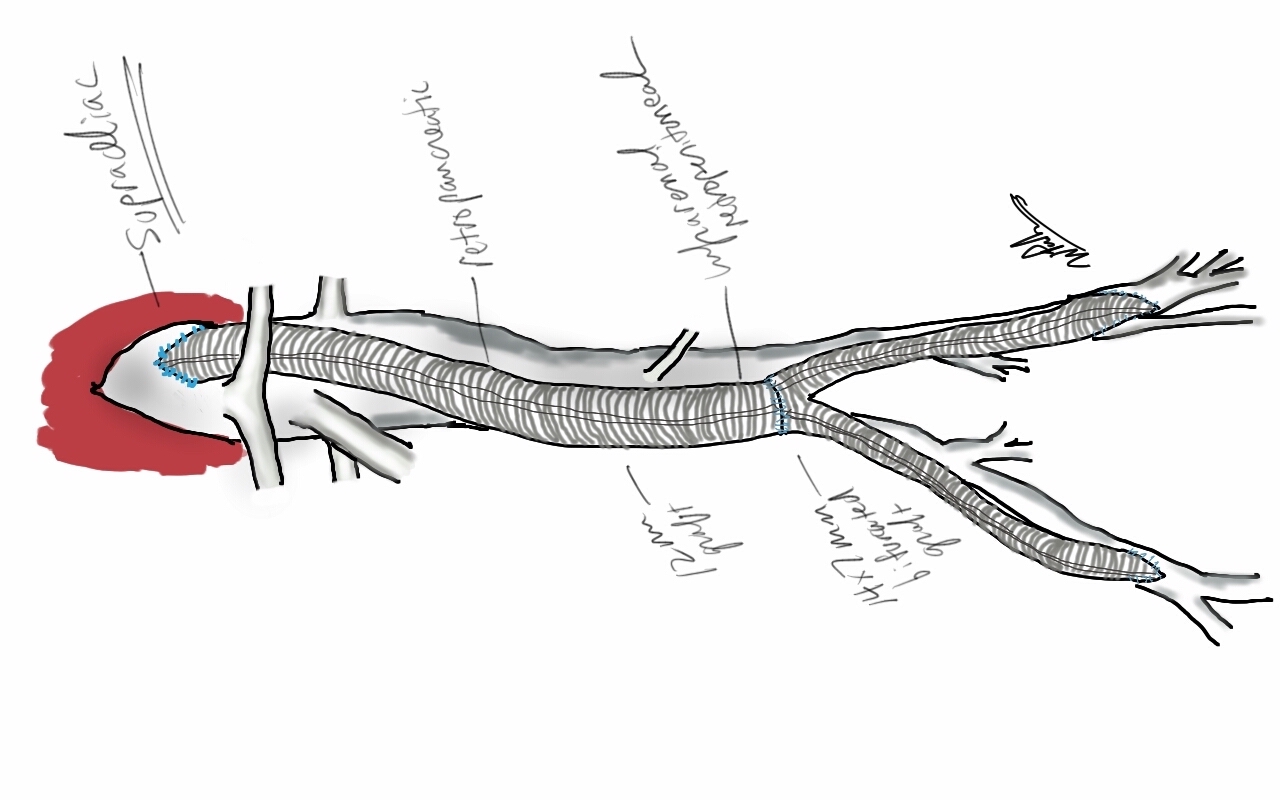
A CT scan was sent with the patient but has been lost to time, and it showed a patent aorto-bifemoral bypass send flow around an occluded distal aorta and iliac arteries. The graft did not have a telltale haze around it nor a dark halo of fluid which signaled to me that it was likely well incorporated and only sick in the exposed part. The patient was not septic, but had grown MRSA from the wound which was granulating from the extensive wound care that had been delivered.
I felt that it would be possible to move his anastomosis point more proximally on the external iliac in a sterile field (figure above), and then close, then endarterectomize the occluded external iliac artery after removing the distal graft, then after vein patching, cover the repair with a sartorius muscle flap. It would salvage the remaining graft and avoid a much larger, more intense operation which was plan B. To prepare for that, I had his deep femoral veins mapped.
The patient was prepped and draped, the groin was excluded by placing a lap pad soaked in peroxide/betadine/saline solution (recipe for “brown bubbly” liter saline, a bottle of peroxide, a bottle of betadine), and covering with an adesive drape. The rest of the abdomen was then draped with a second large adhesive drape. A retroperitoneal (transplant-type) right lower quadrant incision was made (below) and the external iliac artery and graft were exposed. As predicted on CT, the graft was well incorporated.
The external iliac artery was opened and focally endarterectomized of occlusive plaque (image below). The adventitia had good quality despite the longstanding occlusion.
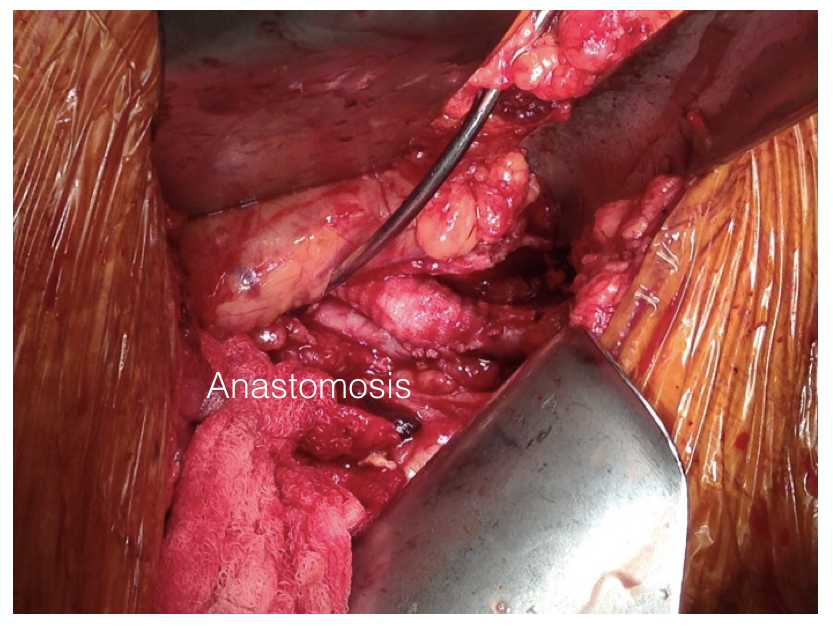
The graft was mobilized and transected and anastomosed end to side to this segment of artery (below). Dissecting was made difficult by how well incorporated it was.
The wound was irrigated (with brown bubbly) and closed, dressed, and sealed over with the adhesive drape. The groin wound was then revealed and the graft pulled out (below).
Remote endarterectomy using a Vollmer ring was used -in this case I didn’t use fluoroscopy given the short distance to the terminus of the plaque which i had mobilized in the pelvis.
The plaque came out easily and was not infected appearing. It is shown below ex vivo.
A segment of saphenous vein was harvested from the patient medially and the arteriotomy was patched. The sartorius muscle was mobilized and applied as a flap over this. The wound was irrigated with brown bubbly and packed open with the intention of VAC application.
The patient healed very rapidly and remains infection free. I had used this approach on several occasions in the past and twice more recently. It truly is salvage as it preserves the uninfected graft while never exposing it to the infection in the process of operating. It avoids having to remove the whole graft which then damages the left side -I have seen other surgeons take this approach elsewhere taking a all-or-nothing approach to graft infection to considerable morbidity to the patient. It avoids having to harvest deep femoral vein -another large operation to which the body responds truculently. The patient recently came by for his 4 year followup, still smoking, but legs preserved.
Followup At 4 Years
The patient came back in followup -it has been 4 years since his infection was repaired. He was complaining of short distance claudication. His wound healed well and remains closed. CTA shows along with his short segment SFA occlusion which we will treat, a widely patent R. EIA (below).
The remote endarterectomy of the external iliac artery remains patent. Compare this to the preop CTA which I found and wasn’t available when I posted this case originally:
The chronically occluded EIA can be readily seen. The artery shown in the current CTA is that recanalized artery.















 If you work long enough, you will not only see everything, but you may end up doing something that you say you would never do. You will be confronted with a scenario that would test not just your skills but also your boundaries. The adage, never say never is a warning that all of us may face a choice -to remain rigidly consistent with some earlier proclamation or to excuse a little hypocrisy for the sake of the patient.
If you work long enough, you will not only see everything, but you may end up doing something that you say you would never do. You will be confronted with a scenario that would test not just your skills but also your boundaries. The adage, never say never is a warning that all of us may face a choice -to remain rigidly consistent with some earlier proclamation or to excuse a little hypocrisy for the sake of the patient.