
One of the greatest surgical texts, Cope’s Early Diagnosis of the Acute Abdomen, is something every surgical resident, vascular or general, should read. The mid-century edition which I owned during my residency, has since been updated, but the central message of the book is this: every complaint or pain the patient has comes from a nerve, either peripheral or visceral, and understanding the nature of the pain, you narrow the diagnosis to only a few possibilities. Irritation of the psoas muscle results in a characteristic pain that years of diagnosing appendicitis the old fashioned way -by exam, then operation, makes it easy to recognize, like Marilyn Manson showing up as your substitute teacher (I would have said Alice Cooper, but that completely dates me). When the psoas muscle is irritated, by a hematoma, injury, inflammation, or abscess, the muscle relays intense pain localized to the retroperitoneum. Stretching the muscle worsens the pain, and the patient is often seen with the ipsilateral hip flexed. The genitofemoral nerve which rides on top of the psoas, is triggered and there is pain referred to the groin and proximal anterior thigh. Seeing this, and fitting the story allows for a diagnosis, before imaging. Without this insight, there is no swift vector to treatment and resolution.

The patient, a middle aged man, had undergone a redo-iliac angioplasty and stent for left iliac in-stent restenosis. He relayed that on the table, he felt immediate left lower quadrant abdominal pain and the desire to flex his left hip. He was restrained, sedated, and the procedure finished -a covered stent had been placed. When he came to my office a month after his initial procedure done elsewhere, he was in wheel chair, unable to straighten his leg. He claimed before coming to see me, he had gone to another hospital, where he had a CT scan and was told nothing was wrong (will have to confirm). He was having subjective fevers at home.
On examination, he sat on the exam table with left hip flexed. His pedal pulses were easily palpable. He had furuncles in his groins which he relayed he had had all of his life. I sent him for CTA and subsequently admitted him for surgery.

The CT showed a large collection around the left iliac artery and stents and on the psoas muscle, an abscess. The blood cultures on admission were positive for Staphylococcus lugadensis sensitive to penicillin.
Putting the story together after the fact is much easier than when you are in the moment, but being aware of the location and type of pain should give you a clue. Very likely, he had a brief rupture on the angiosuite table resulting in his sudden pain, drowned out by the sedatives typically given in response to a patient moving when a stent is deployed. Inflating a balloon in an artery typically causes some discomfort -as the vessels are lined with visceral nerve fibers which are quite sensitive but less localizable than say a pin poking on the index finger. If you ever had bloating with gas, that general discomfort localizable to the mid abdomen, that nausea and discomfort is from stretched visceral pain fibers. If you have ever had dull aching pain of distended spider veins, that is visceral pain. It’s there, but you would not be able to pinpoint it exactly. That is not what this patient had when he flexed his hip on the angio suite table. While the covered stent was deploying, he likely briefly ruptured causing both somatic and visceral pain around his left common iliac artery and iliopsoas muscle. Additionally, if the sheath had been entered through an area of a skin abscess, likely the sheath, wires, and gloves were contaminated. Any handling of the balloon expandable stent graft, which I highly discourage, would have contaminated it, resulting in a device infection, which was made more likely due to his diabetes. As the hematoma got infected, it resulted in the worsening symptoms he was having of left lower quadrant abdominal pain, groin pain, thigh pain, and inability to straighten his hip without pain.
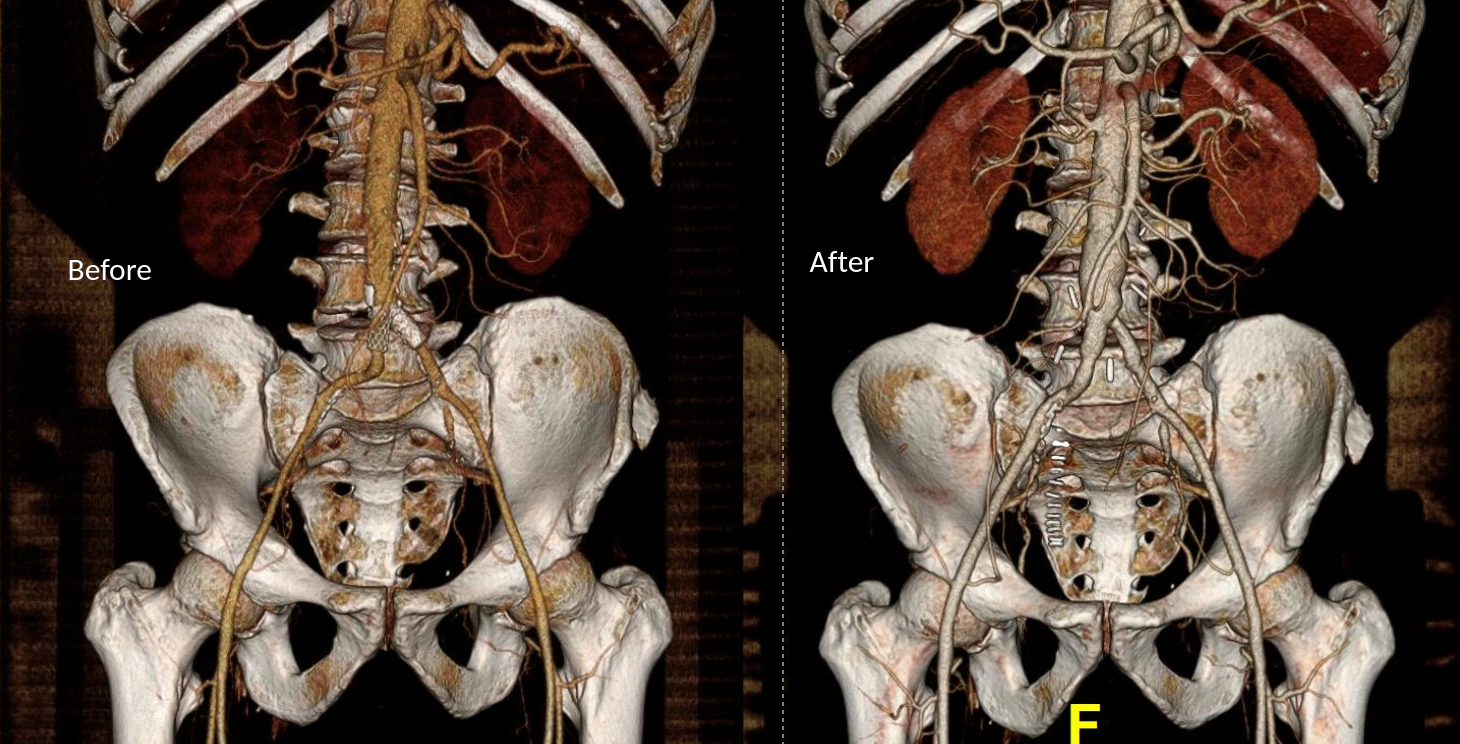
I took him to the operating room and drained his abscess, assisted by Dr. Andrew Tang, chief resident headed to CT Surgery fellowship here at the Clinic, and Dr. Jenny Chang, PGY 2 Surgery. I gave Dr. Chang a copy of Cope’s with the admonition to read it soon and pass it on, as most of the current generation claim no knowledge of this important text. While I am not against interventional drainage, it takes time to drain the collection through a tube whereas sticking your hand in, sampling the collection, observing the injury, and breaking up collections and washing out with brown-bubbly -a mix of betadine/peroxide diluted in saline, I believe speeds the recovery from the infection. His drainage was done through a retroperitoneal approach from the left side and notably, his psoas muscle while viable, did not retract to cautery energy, suggesting some degree of rhabdomyolysis. The iliac artery was an indurated, thickened, and hard from the calcium and plaque that was the original problem affecting his distal aorta and iliac arteries (see left arteriogram centerline). I placed a pair of JP drains, removed one that wasn’t draining much on POD #3, and the other about a week after discharge on POD#5. His WBC elevation which was never high promptly resolved. I kept him on oxacillin with consultation from ID, and waited. After 3 weeks, I repeated his CTA.

His right iliac centerline showed patent stent with diffuse plaque and calcium starting in mid infrarenal aorta.

His abscess had significantly resolved and his pain was gone. He was ambulating again.

The choices at this point were the following
- Continue treatment of patient with supressing antibiotics for life
- Resection of left iliac stent graft which is presumed to be infected
If resection chosen, the options for repair that I considered included:
- NAIS (ref 1). Neoaortoiliac System graft using femoral vein
- Aortoiliac homograft
- Rifampin soaked gelatin coated graft (ref 2)
- Extra-anatomic bypass with axillofemoral bypass or femorofemoral bypass.
- Aortoiliac endarterectomy and repair with bovine pericardial patch and graft
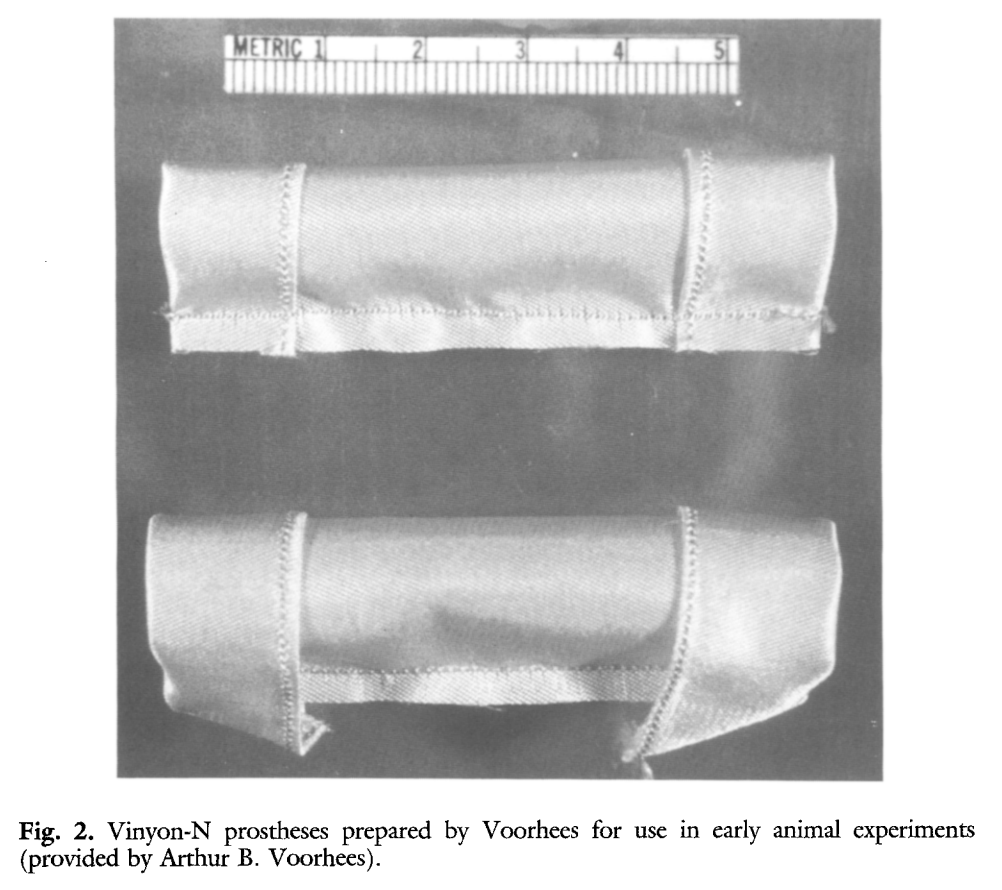
The choice of replacement is becoming clearer in that while rifampin soaked grafts offer immediacy and expedience, all grafts seem to be prone to reinfection at a higher rate than autologous material (ref 3). The NAIS bypass is a great option, but is hampered by the addition of several hours invested in harvest of the femoral veins. While it can be staged with mobilization done one day and harvest another, those added hours add complications. We often forget that the simple metric of procedure time is the most important determinant of complication rate. Any operation going over 2 hours risks wound infection for example simply from ambient colonization of the open wounds from the rain of dead skin from the surgeon’s face, aerosolized fecal flora from flatii (prohibited in my ORs). The microenvironment of the open wound is also room temperature and not 37, having an impact on organ function and hemostasis. The homograft is the original aortic graft -before Arthur Voorhees invented the cloth vascular graft as a resident at Columbia P&S (my medical school alma mater, ref 4), major hospitals had tissue banks of aortic homografts harvested from the recently deceased. Having homografts is now an outsourced function, but does require having proper refrigeration for the cyropreserved grafts and generally can’t be ordered with short notice.
Rifampin soaked grafts work well, especially wrapped in omental flap, in the short and medium term but suffer a reinfection rate that is higher than seen with autologous tissues, and prosthetic grafts without rifampin, such as PTFE for extraanatomic bypass, have the highest rates of reinfection (3), despite being the board answer decades ago.
Endarterectomy allows for use of native tissues for repair. The adventitia around plaque and stents, while thin, can support physiologic pressures, even when they have been occluded for years. And while practice of aortoiliac endarterectomy is a bit of a lost art, it has both a long history stretching back nearly a century and a modern track record with carotid and femoral endarterectomy. It is merely a matter of scale. Pinch and zoom in on a femoral endarterectomy at the bifurcation and you have the same case as with an aortic one.
The question is, is bovine pericardium more autologous than prosthetic? It is a decellularized sheet of collagen from a cow’s pericardium, used in heart valves and vascular patches, but only recently applied as a graft (ref 5-7). I have long used bovine pericardium as a patch with some caution, but the rule of thumb is are there well vascularized tissues around it? A layer of Scarpa’s fascia and fat in a groin wound are not sufficient to protect a bovine patch, but a sartorius flap is. For me, once the infected stent graft is out, knowing if the surrounding tissues bleeds well is an important one.
I chose to do aortoiliac endarterectomy. The patch and graft would be made with bovine pericardium, unless I found the left iliac segment to be devitalized and foul with anaerobic vapors, then, I would close and go NAIS or extra-anatomic. The key point is that choices have to be on the table and constantly rearranged during the conduct of the operation.
The patient was preoperatively vein mapped and had suitable deep femoral vein for bypass conduit, having robust duplicated systems that would impact the patient minimally. The patient was placed in a supine position and via a midline laparotomy, the infrarenal aorta and the common iliac arteries beyond the short iliac stents exposed. I chose this limited exposure as any further into the phlegmon on the left risk injury to ureter and vein. The aorta had a palpable demarcation between plaque and mildly diseased proximal segment, predicted by the CTA to be at the IMA. A longitudinal arteriotomy was created on the right side from mid aorta to mid right iliac, and the left side had a separate arteriotomy to release the stent. The plaque came out in a single specimen (image).

The left iliac artery was destroyed by the infection but the tissues around it bled avidly and were not foul or infected. I avoided excess debridement here as the iliac vein was intimate with the phlegmon. There was a 3cm gap. Again, I thought briefly about taking femoral vein, but proceeded to make a graft from the bovine pericardium. This was sewn around the rod portion of a renal vein retractor from the OMNI set. The finished product resembled Voorhees’ graft. It was sewn into the orifice of the iliac from inside the aorta and end to end to the freshened iliac stump. Unfortunately, the omentum was atropic across the transverse colon, but the tissues around the resected artery and stent graft bled well, indicating good penetration of antibiotic. The retroperitoneum was closed after hemostasis obtained. Dr. Shashank Sharma, our chief resident headed to a vascular surgery fellowship at the renown Houston Methodist next year got to see what is unfortunately a rare occurrence -an aortoiliac endarterectomy, which through me puts him three degrees of separation from Cid Dos Santos (ref 8). Dr. D’Andre Williams, PGY-2 Vascular Surgery Resident, got important lessons on sewing the aorta. She’s part of a fortunate cohort that get exposed to open aortic surgery at our main campus which is unfortunately rare throughout the world.

The final graphic shows the operative end result.

The patient recovered well and was discharged within the week with another month of IV antibiotics planned.
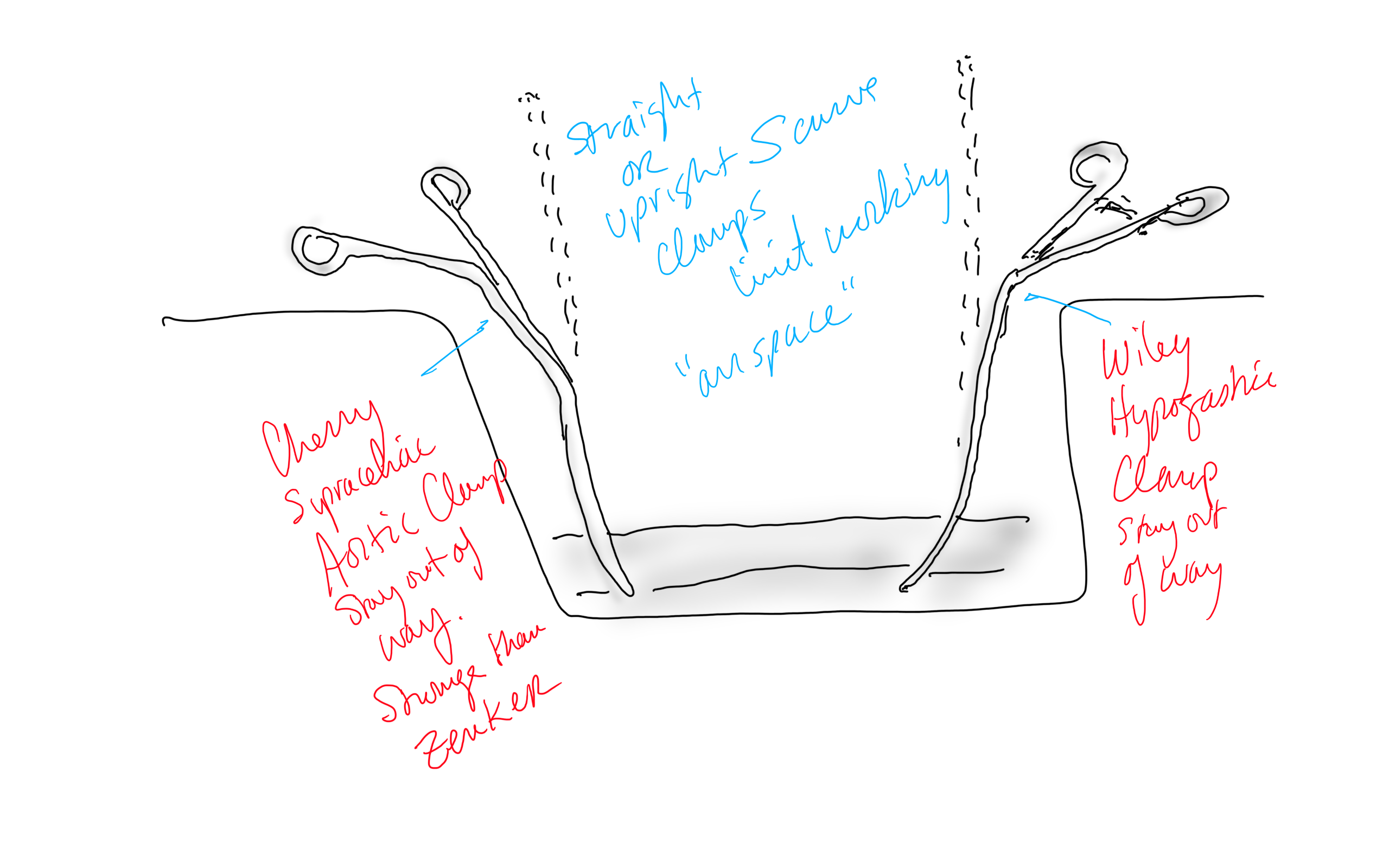
Conclusion: The operation was started at 8 in the morning and was done by lunch time. For aortic cases, this is a crucial metric, as when the clock winds past the surgeon’s comfort, the patient suffers even more. Adding the femoral vein for a NAIS may have been the textbook thing to do, but we don’t do extra-anatomic bypasses that much either. I don’t believe that adding two more hours for retrieving the femoral vein would have enhanced the procedure, and would have served to add potential areas for complication. Technically, the aorta closes much as with a carotid or femoral endarterectomy, but the adventia is thin and really should be sewn with 5-0 or 6-0 Prolene. The larger needles such as the SH size creates unnecessary bleeding unless sewn with a line of felt which could become infected. Despite the thinness, it will hold pressure if it is not infected. Clamps that bend out of the “airspace” above the laparotomy, such as the Cherry Supraceliac Clamp and Wiley Hypogastric Clamp, prevent limiting the operative space with long clamps such as aortic Fogarty or DeBakey clamps, while being stronger than the Zenker.
A final comment for Staphyloccocus lugudensis. This is the second major vascular graft infection with this organism I encountered this year. The other was an infected aortic stent graft. Lugudensis means from Lyons. I do not know why that is, but it is so far not the nasty player that is S. aureus. I am sure it will share some plasmids, and become resistant one day, but in the earlier case in Abu Dhabi and now this, it is sensitive to penicillin, and came from the skin at the femoral puncture site, and for this we are fortunate. Major vascular infections are one of the few areas that still demand open surgical skills, and we foresake them at great peril. It’s critical to remember all the collective memory of surgery from the past, or we will become mere technicians fixing whatever comes out of the radiologist’s report with whatever knowledge obtained from a Zoom meeting for the latest, greatest device.
Acknowledgement
Gratefully, the patient gave his permission, as with all patient, for use of his case for educational purposes.
References
- Chung J, Clagett GP. Neoaortoiliac System (NAIS) procedure for the treatment of the infected aortic graft. Semin Vasc Surg. 2011 Dec;24(4):220-6. doi: 10.1053/j.semvascsurg.2011.10.012. PMID: 22230677.
- Oderich GS, Bower TC, Hofer J, Kalra M, Duncan AA, Wilson JW, Cha S, Gloviczki P. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011 Jan;53(1):99-106, 107.e1-7; discussion 106-7. doi: 10.1016/j.jvs.2010.08.018. PMID: 21184932.
- Smeds MR, Duncan AA, Harlander-Locke MP, Lawrence PF, Lyden S, Fatima J, Eskandari MK; Vascular Low-Frequency Disease Consortium. Treatment and outcomes of aortic endograft infection. J Vasc Surg. 2016 Feb;63(2):332-40. doi: 10.1016/j.jvs.2015.08.113. PMID: 26804214.
- Smith RB 3rd. Arthur B. Voorhees, Jr.: pioneer vascular surgeon. J Vasc Surg. 1993 Sep;18(3):341-8. PMID: 8377227.
- Almási-Sperling V, Heger D, Meyer A, Lang W, Rother U. Treatment of aortic and peripheral prosthetic graft infections with bovine pericardium. J Vasc Surg. 2020 Feb;71(2):592-598. doi: 10.1016/j.jvs.2019.04.485. Epub 2019 Jul 18. PMID: 31327614.
- Lutz B, Reeps C, Biro G, Knappich C, Zimmermann A, Eckstein HH. Bovine Pericardium as New Technical Option for In Situ Reconstruction of Aortic Graft Infection. Ann Vasc Surg. 2017 May;41:118-126. doi: 10.1016/j.avsg.2016.07.098. Epub 2016 Nov 27. PMID: 27903471.
- Belkorissat RA, Sadoul C, Bouziane Z, Saba C, Salomon C, Malikov S, Settembre N. Tubular Reconstruction with Bovine Pericardium Xenografts to Treat Native Aortic Infections. Ann Vasc Surg. 2020 Apr;64:27-32. doi: 10.1016/j.avsg.2019.10.104. Epub 2020 Jan 10. PMID: 31931127.
- Barker WF. A history of endarterectomy. Perspectives in Vascular and Endovascular Therapy. 1991;4(1)1-12. doi:10.1177/153100359100400102
