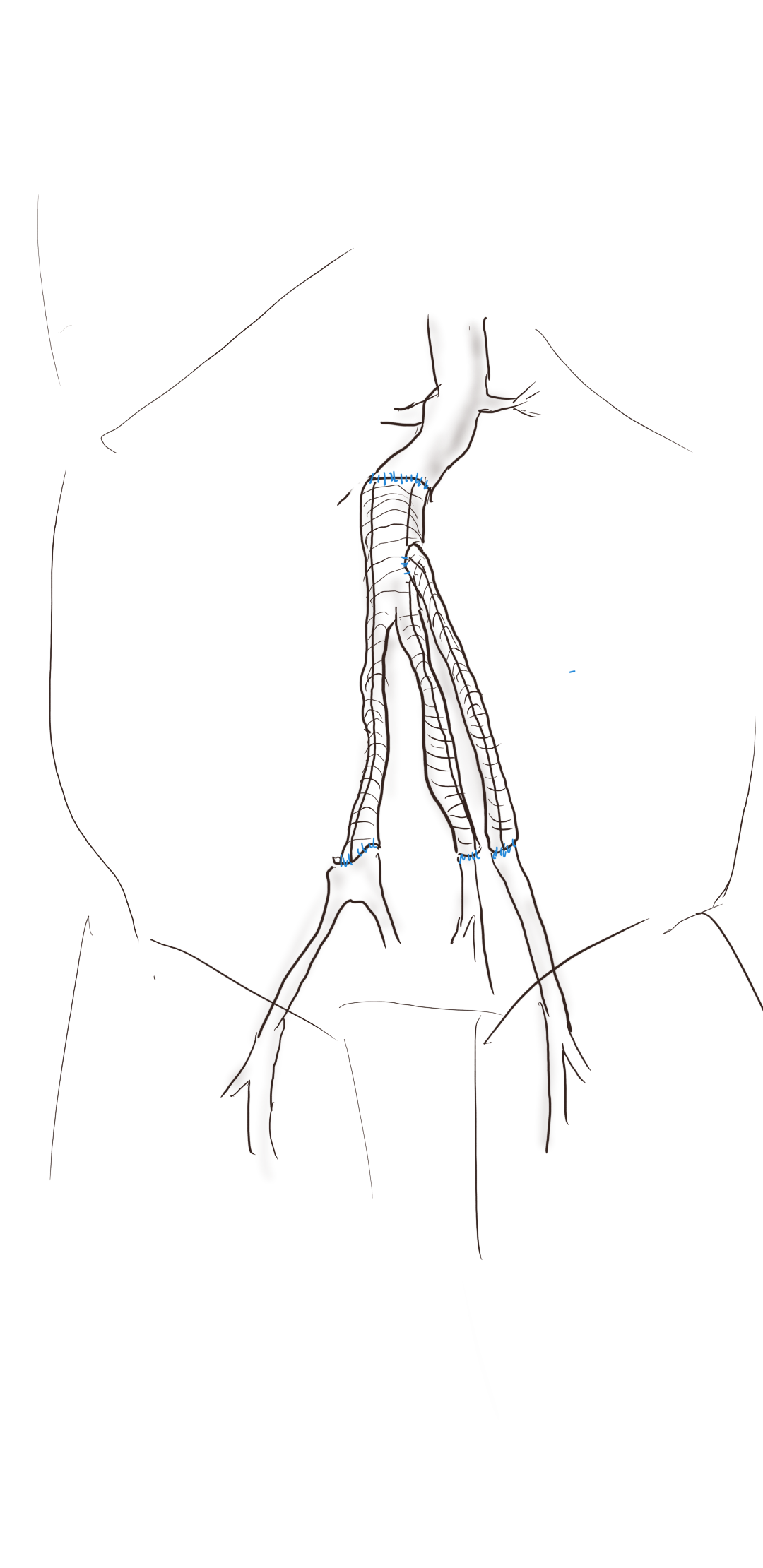
I remember in the mid-2000’s, driving very fast to Lutheran Hospital in Des Moines on a Saturday night to fix an aneurysm that had ruptured. He was a man over 70 years of age with a type III endoleak from a component separation. The endografts had been placed by a cardiac surgeon who had taken some courses. I rescued him by open replacement of the aneurysm with a tube graft after I pulled out the endografts. Later, as the patient recovered, I asked him why he never followed up as required on his stent graft. His answer was, in typical Iowa farmer fashion, “Welp. If it was fixed, why should I?”
Indeed, why should he? Looking at his chart from the time of his EVAR, he was determined to be a “high risk” patient, necessitating the new minimally invasive procedure EVAR in 2003. Seeing that he survived the stress test of a ruptured aneurysm, it was clear he was not all that “high risk.” I did reassure him that with the open repair, he was basically cured. Despite scheduling a followup appointment, he never showed up. And that was okay.
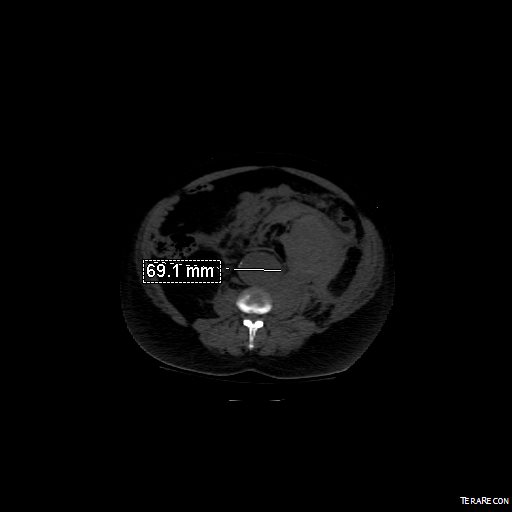
EVAR is a treatment for AAA, but currently not a cure. All of the devices instructions for use stipulate the need for lifelong followup with CT scans with contrast and visits with qualified specialists. As I have mentioned in the past, what other condition requires surveillance CT scans with contrast and followup with a specialist? Cancer in remission. For those with good cardiac risk and functional status, placing an endograft rather than open repair creates “Aortic Aneurysm in Remission.” If they are in the majority of patients with a stable aneurysm sac, their endografts are sitting in a bag of static, aging blood. If there are type II endoleaks, and it is my belief that the majority of stable aneurysm sacs have some type II endoleaks that blinker on and off depending on the hemodynamics, particularly through needle holes, they are circulating the products of breakdown of that bag of old blood and exposing a perfect culture medium to potential inoculation. These type II and IV endoleaks can inflate the aortic sac over time. Occasionally, the residual AAA sacs rupture, erasing any of the early advantage conferred by the minimally invasive index procedure in long term followup EVAR v OPEN repair.
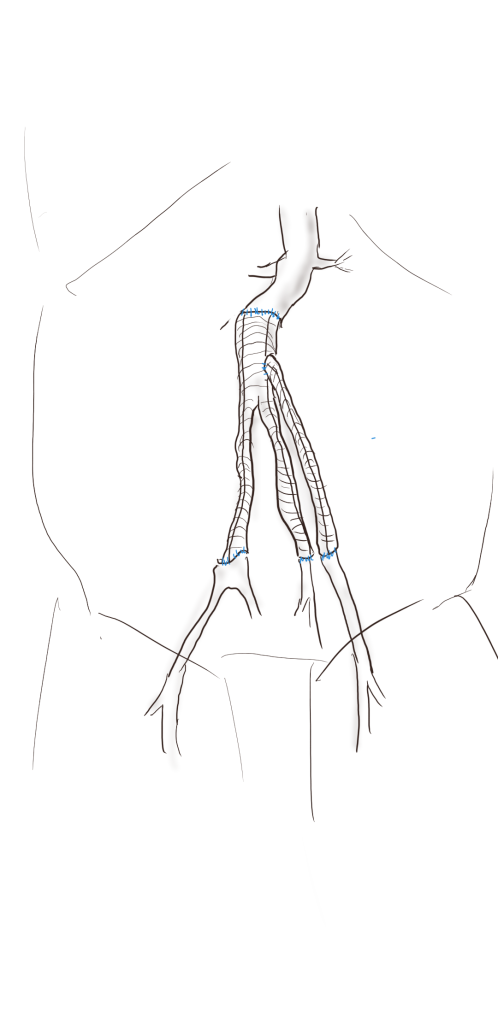
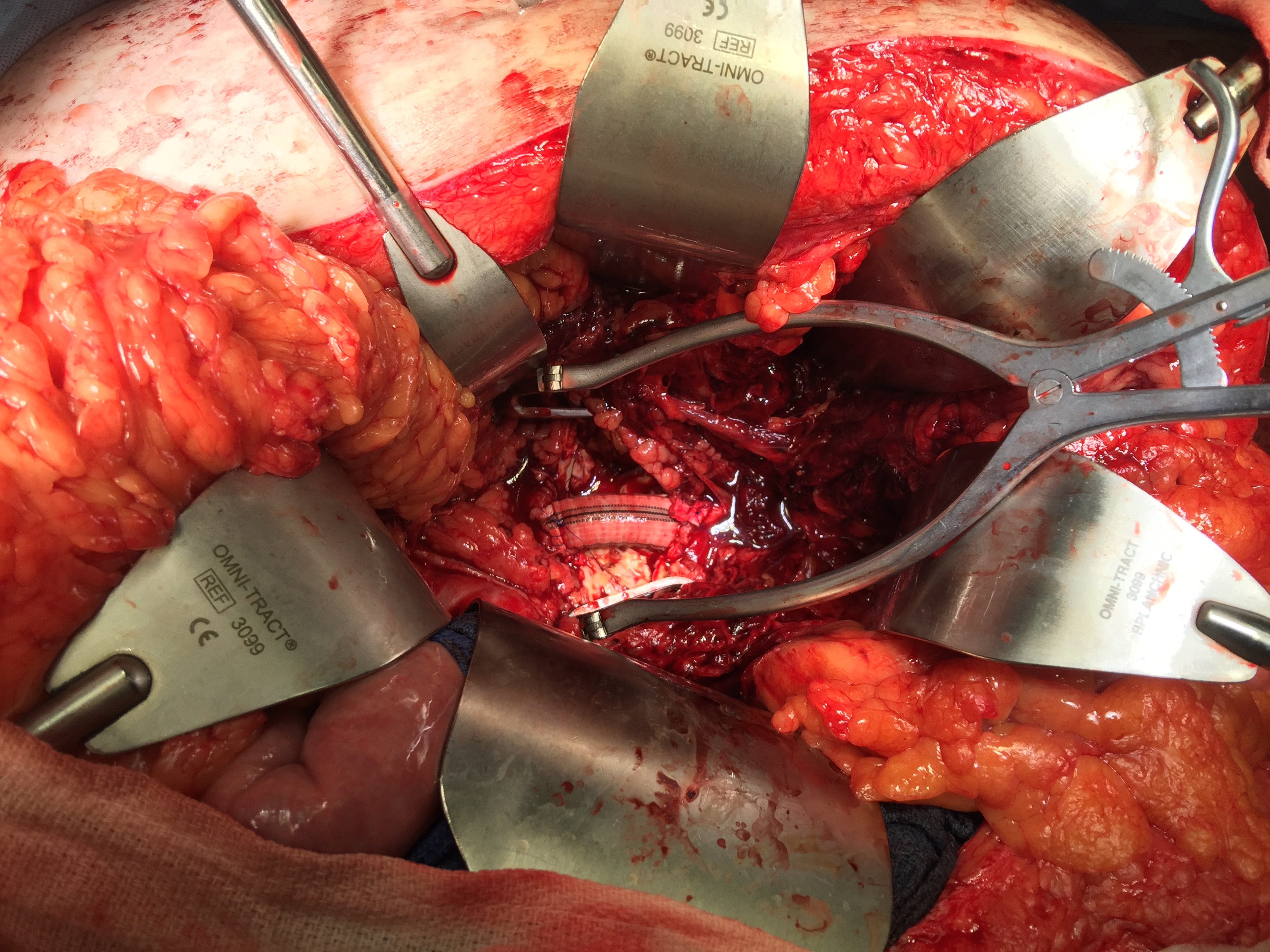
What is a cure? A cure is when you quell an infection with an antibiotic. A cure is when you’ve taken out an inflamed appendix. It’s when you’ve eradicated early stage cancer. It’s when you perform an open aortic graft and the patient can disappear after you remove the dressings and never followup, sure in the knowledge that the aneurysm in that spot will never bother them again. With EVAR, only a minority get to the state (figure at top) a sac shrunk intimately around the endograft. Most are not cured but enrolled in a regime of lifelong surveillance and maintenance.
EVAR does allow people to leave the hospital with less scarring and pain, but the consequences of its popularity are:
1. Letting more practitioners, not all of them vascular surgeons, treat aortic aneurysm disease with less training and with less or no ability to manage the inevitable failures surgically.
2. Creating the business model for “Advanced, Minimally Invasive, Super-Fantastic Aortic Centers of Excellence” which is predicated on the business of surveillance and maintenance of aortic endografts. It is a busy-ness that generates revenue, but burdens the country with more healthcare costs. It ultimately siphons business away from true centers of excellence involved in training the next generation of vascular surgeons.
3. Skewing the training curriculum of trainees to endovascular so much that I have met vascular surgeons who have done no aortic operations. That was the case when I sat in on an open aortic surgery class at the 2017 ESVS meeting in Lyons, France. All the attendees were very eager to try sewing anastomoses, but felt they needed proctoring which isn’t available.
4. Establishing the expectation that open aortic surgery is a failed, antiquarian, obsolete technique to be relegated to the history books. This last one is infuriating and not true but it is out there in the claims of the aorticians.
5. Resulting in palliation when the aortic aneurysm in remission ruptures and there are no readily available open-capable surgeons experienced in rescuing these patients. This happens. Don’t let it happen to you.
Various solutions have been broached including regionalization of aortic aneurysm care, superfellowships in exovascular surgery to complement the widespread endovascular training, and going back to open aortic surgery as the norm as had been proposed controversially in the UK. There is no turning back the clock. The moment that Dr. Parodi combined an aortic graft with Dr. Palmaz’s stent, a quantum leap occurred. The operation of aortic aneurysm surgery was changed from a challenging operation mastered by a few to a straightforward procedure performed by many.
Interesting to me is that illustration at the top of the post is of a common observation – the obliteration of the aortic aneurysm sac around a Guidant Ancure stent graft. When the sac disappears, it is as close to a cure that you can get. For some reason, I see this more frequently with Ancure than with other grafts over the past twenty years.
Odd fact -I may have been the last surgeon to implant an Ancure in the world. In 2003, I was treating a AAA with an Ancure graft when the delivery system froze in mid deployment. I called Dr. Dan Clair away from some meeting, and he called for pliers, screw drivers, and a saw, and after deconstructing the delivery system, deployed the graft and returned to his meeting with nary a word. The Guidant rep, who had been on the phone, looked up with saucer eyes, and said, “Wow. They’ve pulled Ancure off the market.”
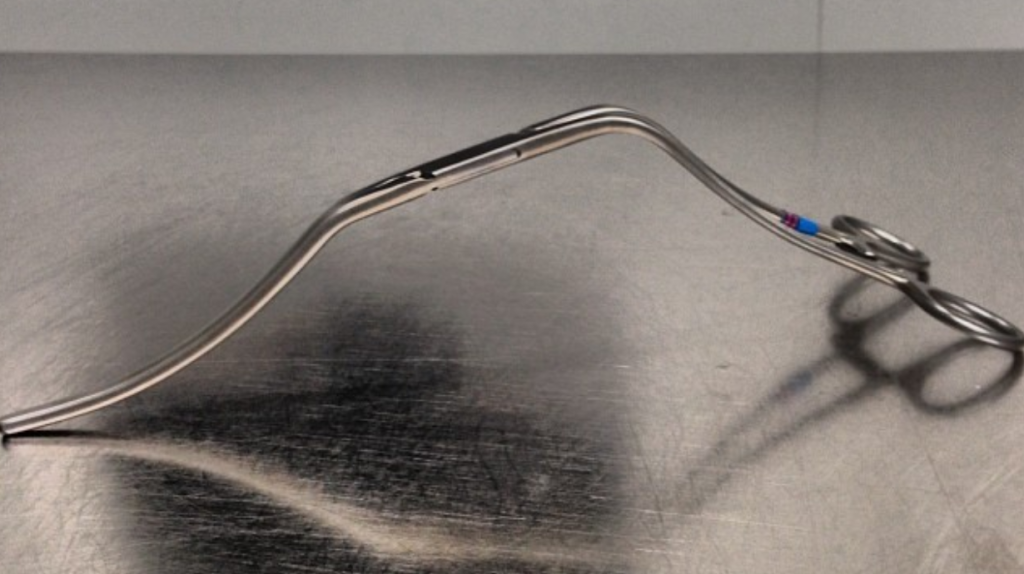
I think it is because of the design, which is now off the market. When stents are sewn to cloth, the needle holes leak, and leak particularly where the stent graft makes a turn, stretching the suture hole. Junctions and seams leak. The Ancure, aside from the stents at top and bottom in the seal zone, has no such holes as it is unsupported and manufactured as a single piece with no junctions or seams. It is the closest you get to sewing in a graft by open surgery. If it weren’t for its overly complicated delivery system which was its downfall, I think it would be in its third generation with visceral branches that are created off the textile machines rather than joined inside the patient. There are lessons to be learned from this abandoned tech.
I believe a treat once and walk-away cure is achievable in EVAR. The idea is not to be satisfied with anything less than a cure, anything that ends with aortic aneurysm in remission. We have to understand we have chosen a path of iteration and continuous but slow improvement in the EVAR space. The front end benefits of EVAR are clear but it is in the long term we have to focus. Until then, warranties would be great.