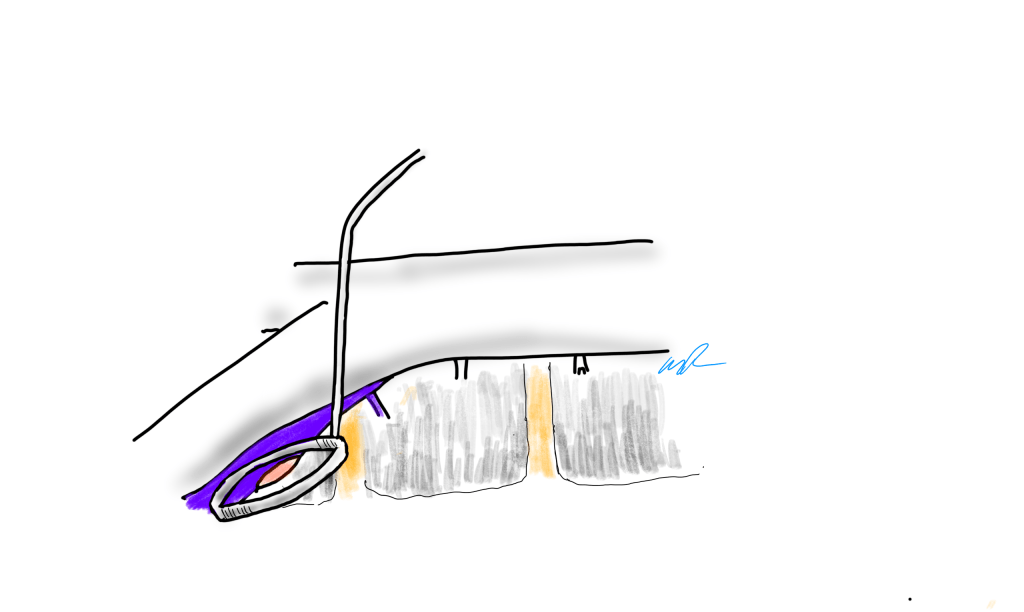
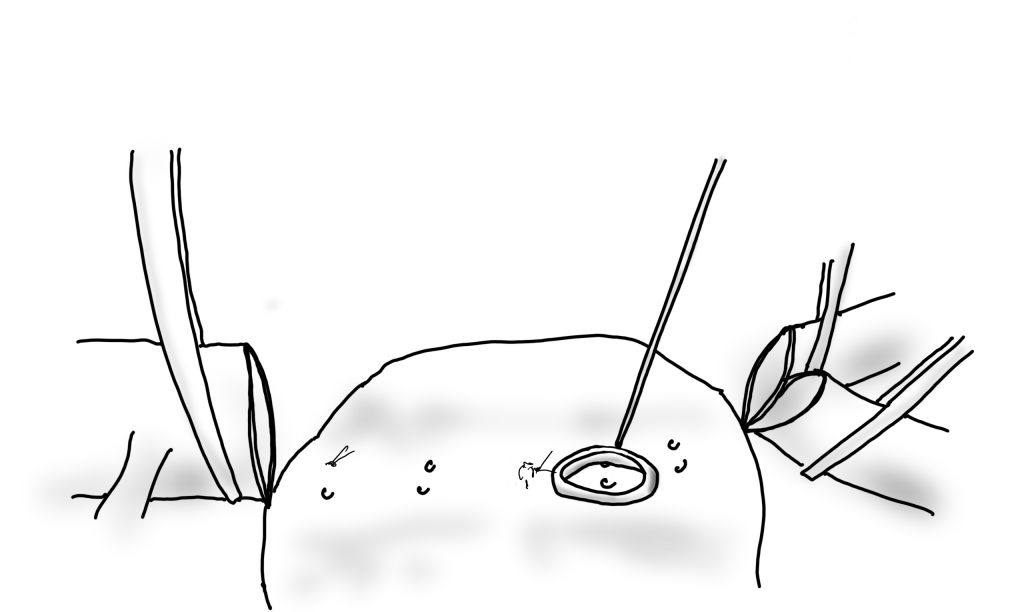
PTFE bypass to a smaller tibial artery with Taylor vein patch
One of the conclusions of the BEST-CLI trial (ref 1) was that of equivalency between alternate bypass conduits and interventions when a single saphenous vein is not available. I recently contacted Dr. Matt Menard to see if there had been subgroup analysis of these bypasses which represents a heterogeneous group of conduits including PTFE, PTFE with vein patch, spliced vein, composite vein, and even possibly allograft. The results from the abstract were intriguing -“83 of 194 patients (42.8%) in the surgical group and in 95 of 199 patients (47.7%) in the endovascular group (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; P = 0.12) after a median follow-up of 1.6 years” with the primary MALE endpoint. If this was a football game, there would be a video review of the call. And they are looking at this, I was assured by Matt, but we would all have to wait for this year’s SVS VAM. Dr. Matt Menard is coming to speak at our 12th Annual Vascular Disease Update (link) which I highly encourage you to register and attend (addendum).
The Cohort 1 from BEST-CLI is an illustration of the vascular surgeons’ LIMA to LAD. It’s something we already knew from years of experience, but laid out in level 1 data (below).
The BEST-CLI paper is short on detail about cohort 2. This is where a lot of clinical decisions get made, and I suspect the vast majority of patients are getting interventions because fewer surgeons are facile with leg bypasses and vein patches.
Why the vein patch? While not a panacea for the lack of vein, from its inception, it has proved a worthy adjunct in limb salvage. Decades before endovascular therapies showed good limb salvage with modest to poor patency rates, Dr. Frank Veith showed that infrageniculate PTFE bypasses showed good limb salvage with poor patency (reference 2). Vein patches, such as the Taylor patch illustrated at the top, showed good patencies (reference 3) in an era where DOACS, DAPT, and statins were not available.
Results of the Taylor Patch from Mr. RS Taylor.
Why a patch works is debated. Some feel it is the modification of the end to side anastomosis that creates an optimal shape for containing turbulence which leads to intimal hyperplasia. This was the concept behind the Distaflo graft which I tried but have abandoned for not improving patency in my personal experience.
The Distaflow Mini-Cuff which applies the concept of flow optimization by the shape of the anastomosis achieved by vein cuffs.
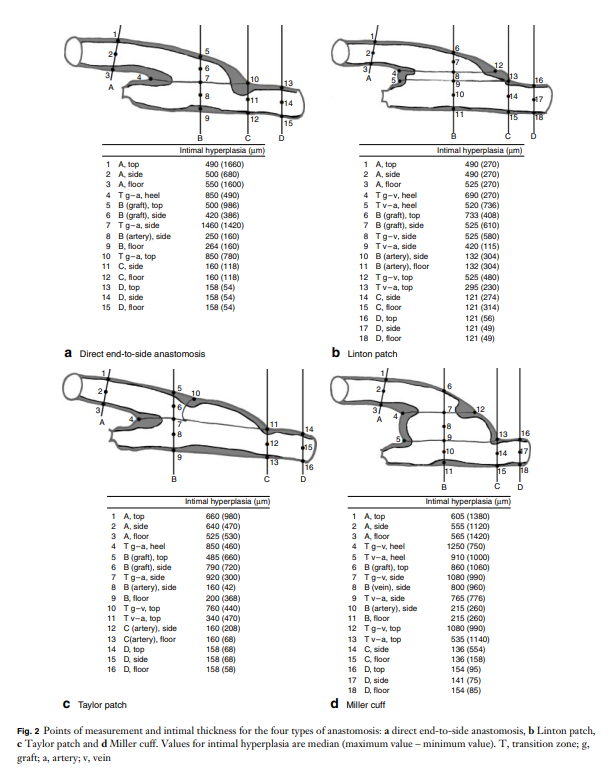
The best explanation of why vein cuffs work is from an animal study from Vienna. Intimal hyperplasia is best explained as a foreign body reaction and the reaction is worse with a true foreign body than with autologous materials. A simple anastomosis with PTFE to tibial artery creates a ring of hyperplasia. Vein patching moves this severe foreign body reaction off of the artery, leaving a gentler vein to artery reaction to occur on the outflow (reference 4).
My final point is that these surgical papers used to be the mainstay of podium presentation in the 90’s and ’00’s, but are now infrequent as the bulk of the time at these meetings is devoted to gadgets which almost always involves purchasing a box and contracting for disposables (the printer and ink business model). I am going to review our institutional results of these PTFE bypasses, and hope to see more from other groups. I look forward to the BEST-CLI papers to come, and other trials.
References
Farber A, Menard MT, et al. BEST-CLI Investigators. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N Engl J Med. 2022 Dec 22;387(25):2305-2316. doi: 10.1056/NEJMoa2207899. Epub 2022 Nov 7. PMID: 36342173.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
Taylor RS, Loh A, McFarland RJ, Cox M, Chester JF. Improved technique for polytetrafluoroethylene bypass grafting: long-term results using anastomotic vein patches. Br J Surg. 1992 Apr;79(4):348-54. doi: 10.1002/bjs.1800790424. PMID: 1576506.
Trubel W, Schima H, Czerny M, Perktold K, Schimek MG, Polterauer P. Experimental comparison of four methods of end-to-side anastomosis with expanded polytetrafluoroethylene. Br J Surg. 2004 Feb;91(2):159-67. doi: 10.1002/bjs.4388. PMID: 14760662.
Addendum
The Annual Vascular Update at University Hospital has something for everyone, including a presentation on IRAD by Dr. Santi Trimarchi, and BEST-CLI by Dr. Matthew Menard. Local faculty from Cleveland are also featured in a broad review of vascular medicine and surgery chaired by Drs. Mehdi Shishehbor, Heather Gornik, and our chair in vascular surgery, Dr. Jae Sung Cho. Link. I will be presenting on neurovascular compression syndromes and renal failure/heart failure.
During a thoracoscopic lung resection, bleeding along staple lines, even of the main pulmonary artery, can be managed with a Park Clamp
The Park Clamp isn’t a true clamp, but rather a compressor. It was designed initialy for the troublesome venous bleeding. It is a ring with ridged edges to provide grip securely welded to a handle. It allows for circumferential compression of tissues, allowing for hemostasis while creating a open space for suturing. The picture above are my colleagues from CCAD -Drs. Andres Obeso and Redha Souilamas perfoming a partial pneumonectomy. The staple line on the artery was bleeding and this can be troublesome, and may require conversion to thoracotomy. The Park Clamp was inserted and provided excellent hemostasis (below).
Hemostasis achieved, a suture can be placed without ongoing hemorrhage without having to convert to a thoracotomy
During one of my cases as a fellow at the Mayo Clinic, I ran into venous bleeding behind the aortic bifurcation. Dr. Thomas Bower, recently retired, came in and lengthened the incision to create more space for more hands, and got all of us -me, the resident, the intern, the RNFA’s, to retract and compress with sponge-on-a-stick to repair the linear tear on the vena cava under the aortic bifurcation.
I’ve always hated this approach because outside of Mayo in 2002, it is very hard to get five people to become your voice activated retractor system, and the sponge on a stick only works well when you are on the hole and less effectively next to the hole. There had to be a better way.
Spinal exposure at the L5-S1 level is treacherous because of the veins
When I returned to academic practice at the Cleveland Clinic, combined cases with other specialties got me operating on tight spaces, frequently heavily scarred, with many blood vessels to control, such as a retroperitoneal spinal exposure illustrated above.
The veins are fragile here and as they are in communication with the central veins, bleed copiously and rapidly.
Look above at the dreaded linear tear on the left iliac vein that can result from simple manipulation of this fragile structure -typically a tributary vein will anchor the iliac and simple retraction can cause a tear.
Sponge on a stick limits view of the injury
Using a sponge on a stick greatly hampers your ability to repair the injury. First, the people applying the sponge on a stick have to have some skill. Second, because they are long and straight, they are constrained by the incision you have created. When applied, the “airspace” above the injury is greatly reduced. Third, hemostasis is never complete unless the whole vein is compressed, which is challenging in the above scenario.
The handle can be bent to create more “airspace” for operating
When the ring is applied, two things happen. Hemostasis is in general complete and there is room to operate, in this case suture. Even in the instance where an artery is bleeding from a flat surface as in a bleeding duodenal ulcer or a lumbar artery in an open aorta, hemostasis is achievable.
Bleeding lumbar arterise can cause a significant blood loss in the time it takes to apply a suture. Fingers will occlude, but no one likes getting stuck with a needle.
The bleeding lumbar artery illustrated above responds well to ring compression. This is also the case where you have bleeding from scarred or irradiated tissue surfaces, or from varicose veins or AV fistulae from the skin. If you don’t have a Park Clamp, you can use the finger rings of the handle on a tonsil or Kelly clamp.
If you don’t have a Park Clamp, you can have one made or you can use the ring handle of a standard clamp.
There seems to be interest among surgeons who have seen this device used, and I will look into manufacturing these. I would not object to surgeons making their own for their personal use -taking apart a long tonsil clamp and bending the ring at a right angle should be simple enough. The clamps I use were manufactured at our prototypic facilities, but 3D printed ones should work fine.
And I will leave you with this final thought. I am in the profession of surgery, and at its core, it’s about helping the patient. If you adapt this idea and help someone, I will have fulfilled my duties.
The patient is a 70 year old man with risk factors of cigarette smoking, type II diabetes mellitus, hypertension, and hypercholesterolemia who presents with rest pain and gangrene of the tip of his left great toe. Several weeks prior to this, he went to his pharmacy and received a flu vaccination and picked up over the counter topical medication for an ingrown toenail. who developed pain from an ingrown toenail. Several weeks later, the tip of his toe blackened and the pain became unbearable and he came to the hospital.
No pulses, dry gangrene of tip of toe
Physical examination was notable for the dry gangrene affecting the distal phalanx of the left hallux. There was a left femoral pulse, but nothing was palpable below. His forefoot was cool and painful and this pain was relieved with dependency.
Pulse volume recording showed a drop in flow across the left knee and flate waveforms at the ankle, foot, and digits. The ABI was zero. WIfI 2 3 2, Stage 4, potential benefit of revascularization high (reference 1). CTA was performed and revealed patent aortoiliac segment, patent common femoral and profunda femoral arteries, with occlusion of the mid to distal SFA, reconstitution of the above knee popliteal artery with 2 vessel runoff via a patent posterior tibial and peroneal arteries.
CTA VR Reconstruction Shows Reconstitution of AK POP and 2V Runoff via PT and Peroneal Arteries
The centerline reconstructions, adapted from aortic planning, lets me determine the character of the arteries for size, calcification, stiffness, collateralization, and length of occlusion. This was had low density and given the timecourse of the events -from claudication to gangrene, and the lack of collaterization implying an acute process possibly on a chronic lesion, I felt there was likely to be some thrombus burden over a chronic plaque across Hunter’s Canal with occlusion of the geniculate arteries. Usually, when the occlusion is chronic, femoropopliteal occlusions of this type come with an ABI of 0.5-0.7, not 0.
Global Limb Anatomical Staging System (GLASS) Classification of CLTI (reference 2) through the easy to use SVS calculator came out Stage II: Intermediate Complexity. I had the good fortune of being in the audience when GLASS was presented to a rapt audience in Lyons, France, by Dr. John White in 2017, at the ESVS meeting. I include it because Dr. Devin Zarkowsky on a tweet that generated this post wanted WIfI and GLASS. WIfI I find helpful. GLASS I am still figuring out, because it tends to tell me what I already know: this is a lesion of intermediate complexity that could go either way to open or endovascular.
Treatment options include:
Endovascular -starting with POBA and escalating to various additional therapies such as stents, covered stents, DCB, drug coated stents, atherectomy, thrombectomy, thrombolysis (then any of the previously mentioned).
Bypass with PTFE
Bypass with vein
White Arrows Show the Excellent GSV
The data tells us so far that open or endovascular is broadly equivalent, but experience guides me. For rest pain, any incremental increase of flow will do, and it does not necessarily have to be in-line. For healing major tissue loss, there really can’t be enough flow. Bypasses with good runoff deliver a lot of flow. Bypasses with vein have great longevity and the shorter they are, the longer they last.
So is long patency important? Numerous studies have shown that patency does not impact limb salvage or amputation free survival, going to BASIL Trial (reference 3), but even stretching back to Dr. Frank Veith’s advocacy of PTFE bypass to infrageniculate targets (reference 4), patency does not add to limb salvage beyond the initial wound healing. The patency of a PTFE bypass to a tibial target is less than 20% at 5 years, but the limb salvage rate is a laudable 80% plus, and this is repeated in numerous evaluations of POBA, stents, and every new technology that has accrued in the nearly 4 decades since that paper.
What does patency buy you? Less reinterventions. There is nothing worse to me than having to reintervene within a year or two of an intervention. When a bypass works well, the patients just come for a hello-how-do-you-do for years. The BASIL trial concluded that bypass operations were more expensive, and I dispute this. In 2021, operations were far less expensive than the latest energy weapon, their box you have to purchase, and the catheters you use once and throw away. The argument given by interventionalists is that bypass operations are disfiguring and ridden with complications and that argument holds water as there are many points where vascular surgeons fail or have largely stopped work on investigating and optimizing open surgery. What if bypass surgery could be brought to the level of dialysis access surgery in terms of invasiveness? What if groin complications could be minimized? What if long filleting-type incisions of the thigh and leg could be eliminated entirely? What if edema could be prevented or minimized postoperatively to prevent serous drainage and infections? If you focus on the art of bypass surgery and choose patients well, you can get a quick, minimally invasive bypass with the overall physiologic impact of a Brescia-Cimino AV fistula. After considering endovascular, I chose bypass.
This patient had on mapping excellent saphenous vein between 3-5mm in diameter. He had excellent skin and was not obese. A vertical groin incision could be avoided by making a skin line incision over the saphenofemoral junction and transposing it to the adjacent SFA which was patent. Skin line oblique incisions in the groin heal much better than the standard vertical incisions, and it is possible to mobilize and expose the saphenous vein using an appendiceal retractor and clipping the generous proximal thigh tributary. In this patient, the most proximal incision was well away from the inguinal crease, the generator of wound infections in the groin. Essentially, if there is no groin incision there can be no groin complication.
The distal vein is mobilized first before dropping on the above knee popliteal artery which is exposed through a separate incision. This is because the AK POP space is best exposed over the sartorius, and the vein in this patient was well below (posterior) to the sartorius. The vein was tunneled under the sartorius to the AK POP. With the in-situ technique, the proximal anastomosis is completed, then the valves lysed with a retrograde LeMaitre valvulotome. Doing, after two or three passes, the pulse was strong, and the flow strong enough to fling the blood beyond the foot -a key step. If there is no such flow, if there is a weak pulse, or poor blood flight, I do one more pass of the valvulotome then duplex for any large diverting tributaries and tie them off one by one until good flow is achieved.
I do not mobilize the entire vein (and tie off every collateral) unless I cannot do an in-situ technique. It defeats the purpose of this beautiful minimally invasive procedure.
Femoral artery to above knee popliteal bypass with in-situ vein
He recovered rapidly and was discharged home after a partial hallux amputation by podiatry. In followup, he was feeling better. All of his surgical wounds had healed. Duplex and ABI did find this:
Retained valve, very hard to see but present on B-mode, causing a hemodynamically significant stenosis, with ABI of 0.57
I took him to the angiosuite for repair of this retained valve. Rarely, retained valves occur after in-situ bypasses, but require generally unsatisfactory solutions involving either open valvulectomy and patch venoplasty or stenting of a virgin vein. Valvulotomy is possible, but generally described as an open procedure as well, but I had other plans.
Downstream of this retained valve were tributaries which could be seen on duplex, and therefore accessible with a micropuncture needle. This would then allow for placement of a 4F sheath, through which the LeMaitre valvulotome would pass unhindered, allowing for valvulotomy. I would use this session in the angiosuite to deliver embolization coils to the diverting tributaries as well.
Arteriography reveals a retained valve and diverting AVF’sRetained valve catches the catheter sent up and over from the other side
LeMaitre is a unique company in that it focuses on vascular surgical operations and arises from the original product and reason for the company the eponymous valvulotome. Because it comes sheathed in a low profile catheter, it is immediately familiar to modern surgeons even though it was made in another century.
Cutting of retained valve with LeMaitre valvulotome using ultrasound guidance
Cutting the valves involved passing the valvulotome several under fluoroscopy through a 4F sheath placed through the tributary seen above. After the valvulotomy, the diverting tributaries, only one of which drained quickly into a deep vein, were coiled. At the end of the procedure, a manual cuff was found and an ABI checked. It was now 1.05.
Diverting tributaries coiled
In 2015, the Oxford English Dictionary added McGyver as a verb -“Make or repair (an object) in an improvised or inventive way, making use of whatever items are at hand.” A television show from the 80’s and early 90’s, the main character, McGyver, was able to make useful tools out of what was available, allowing him to come out victorious, but usually just survive. It is a useful concept that is a must have in managing complex and dynamic situations. Just because it hasn’t been done before to your knowledge doesn’t mean that it isn’t a simple solution. I have only one ask that LeMaitre flip their blades around and design an ante grade valvulotome. Those who know what I’m getting at know what I am getting at.
The LeMaitre valvulotome allows for in-situ saphenous vein bypass, a prototypical hybrid vascular procedure from the 80’s that portended the endovascular revolution that followed. It is meant to be used intraoperatively, but because of its low profile, it can be applied.
I will allow that this second procedure likely makes any argument to cost moot, but numerous incisions and extra time in the OR is avoided. The patient now has a vein bypass that could last many years which diminishes the need for follow up procedures to maintain assisted patency.
We will be arguing this point for years even after BEST-CLI is presented. BASIL-2 just closed enrollment. Hopefully we will get some clarity.
Reference
Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014 Jan;59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12. PMID: 24126108.
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28. Erratum in: J Vasc Surg. 2019 Aug;70(2):662. PMID: 31159978; PMCID: PMC8365864.
Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005 Dec 3;366(9501):1925-34. doi: 10.1016/S0140-6736(05)67704-5. PMID: 16325694.
Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
One of the greatest surgical texts, Cope’s Early Diagnosis of the Acute Abdomen, is something every surgical resident, vascular or general, should read. The mid-century edition which I owned during my residency, has since been updated, but the central message of the book is this: every complaint or pain the patient has comes from a nerve, either peripheral or visceral, and understanding the nature of the pain, you narrow the diagnosis to only a few possibilities. Irritation of the psoas muscle results in a characteristic pain that years of diagnosing appendicitis the old fashioned way -by exam, then operation, makes it easy to recognize, like Marilyn Manson showing up as your substitute teacher (I would have said Alice Cooper, but that completely dates me). When the psoas muscle is irritated, by a hematoma, injury, inflammation, or abscess, the muscle relays intense pain localized to the retroperitoneum. Stretching the muscle worsens the pain, and the patient is often seen with the ipsilateral hip flexed. The genitofemoral nerve which rides on top of the psoas, is triggered and there is pain referred to the groin and proximal anterior thigh. Seeing this, and fitting the story allows for a diagnosis, before imaging. Without this insight, there is no swift vector to treatment and resolution.
Patient with inability to straighten left hip after iliac stent placement
The patient, a middle aged man, had undergone a redo-iliac angioplasty and stent for left iliac in-stent restenosis. He relayed that on the table, he felt immediate left lower quadrant abdominal pain and the desire to flex his left hip. He was restrained, sedated, and the procedure finished -a covered stent had been placed. When he came to my office a month after his initial procedure done elsewhere, he was in wheel chair, unable to straighten his leg. He claimed before coming to see me, he had gone to another hospital, where he had a CT scan and was told nothing was wrong (will have to confirm). He was having subjective fevers at home.
On examination, he sat on the exam table with left hip flexed. His pedal pulses were easily palpable. He had furuncles in his groins which he relayed he had had all of his life. I sent him for CTA and subsequently admitted him for surgery.
left iliopsoas abscess
The CT showed a large collection around the left iliac artery and stents and on the psoas muscle, an abscess. The blood cultures on admission were positive for Staphylococcus lugadensis sensitive to penicillin.
Putting the story together after the fact is much easier than when you are in the moment, but being aware of the location and type of pain should give you a clue. Very likely, he had a brief rupture on the angiosuite table resulting in his sudden pain, drowned out by the sedatives typically given in response to a patient moving when a stent is deployed. Inflating a balloon in an artery typically causes some discomfort -as the vessels are lined with visceral nerve fibers which are quite sensitive but less localizable than say a pin poking on the index finger. If you ever had bloating with gas, that general discomfort localizable to the mid abdomen, that nausea and discomfort is from stretched visceral pain fibers. If you have ever had dull aching pain of distended spider veins, that is visceral pain. It’s there, but you would not be able to pinpoint it exactly. That is not what this patient had when he flexed his hip on the angio suite table. While the covered stent was deploying, he likely briefly ruptured causing both somatic and visceral pain around his left common iliac artery and iliopsoas muscle. Additionally, if the sheath had been entered through an area of a skin abscess, likely the sheath, wires, and gloves were contaminated. Any handling of the balloon expandable stent graft, which I highly discourage, would have contaminated it, resulting in a device infection, which was made more likely due to his diabetes. As the hematoma got infected, it resulted in the worsening symptoms he was having of left lower quadrant abdominal pain, groin pain, thigh pain, and inability to straighten his hip without pain.
I took him to the operating room and drained his abscess, assisted by Dr. Andrew Tang, chief resident headed to CT Surgery fellowship here at the Clinic, and Dr. Jenny Chang, PGY 2 Surgery. I gave Dr. Chang a copy of Cope’s with the admonition to read it soon and pass it on, as most of the current generation claim no knowledge of this important text. While I am not against interventional drainage, it takes time to drain the collection through a tube whereas sticking your hand in, sampling the collection, observing the injury, and breaking up collections and washing out with brown-bubbly -a mix of betadine/peroxide diluted in saline, I believe speeds the recovery from the infection. His drainage was done through a retroperitoneal approach from the left side and notably, his psoas muscle while viable, did not retract to cautery energy, suggesting some degree of rhabdomyolysis. The iliac artery was an indurated, thickened, and hard from the calcium and plaque that was the original problem affecting his distal aorta and iliac arteries (see left arteriogram centerline). I placed a pair of JP drains, removed one that wasn’t draining much on POD #3, and the other about a week after discharge on POD#5. His WBC elevation which was never high promptly resolved. I kept him on oxacillin with consultation from ID, and waited. After 3 weeks, I repeated his CTA.
His right iliac centerline showed patent stent with diffuse plaque and calcium starting in mid infrarenal aorta.
His abscess had significantly resolved and his pain was gone. He was ambulating again.
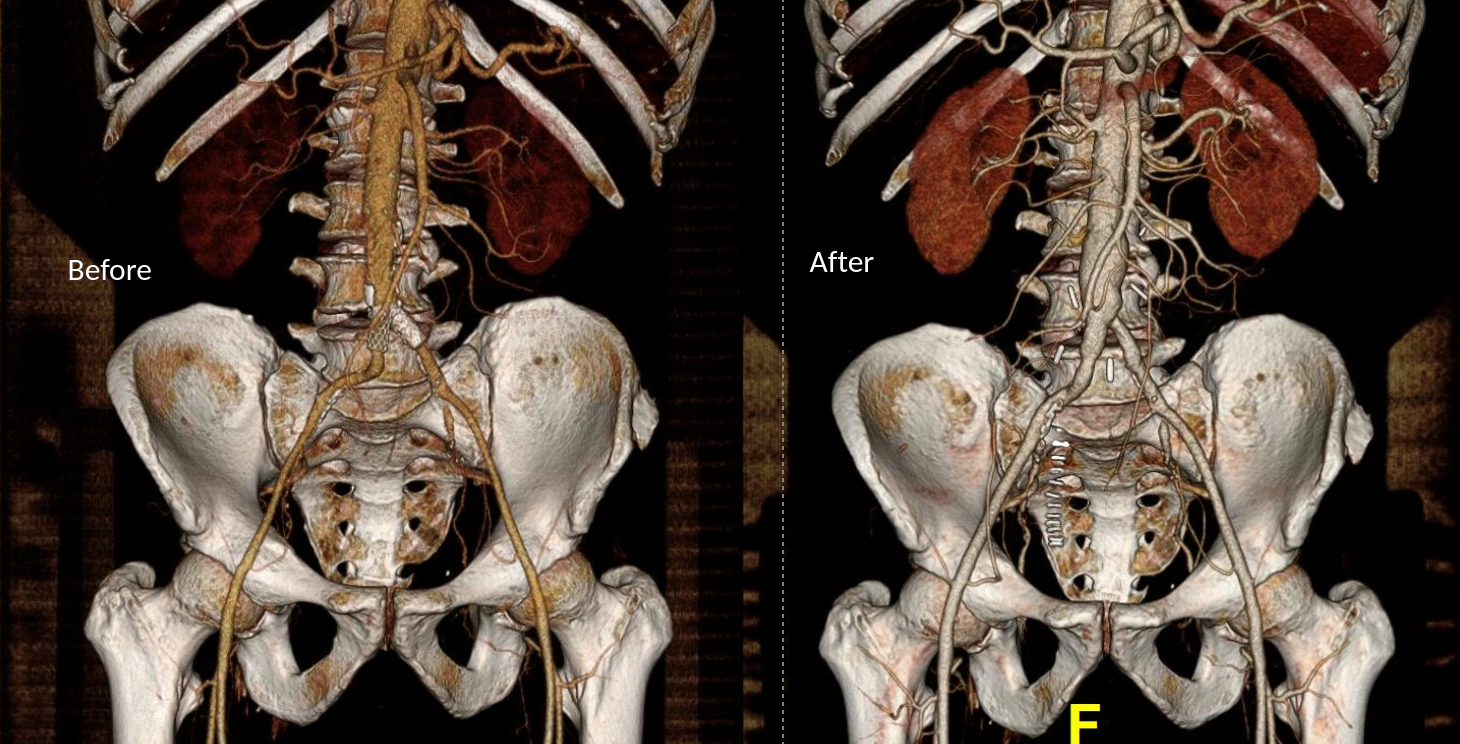
Before and after abscess drainage
The choices at this point were the following
Continue treatment of patient with supressing antibiotics for life
Resection of left iliac stent graft which is presumed to be infected
If resection chosen, the options for repair that I considered included:
NAIS (ref 1). Neoaortoiliac System graft using femoral vein
Aortoiliac homograft
Rifampin soaked gelatin coated graft (ref 2)
Extra-anatomic bypass with axillofemoral bypass or femorofemoral bypass.
Aortoiliac endarterectomy and repair with bovine pericardial patch and graft
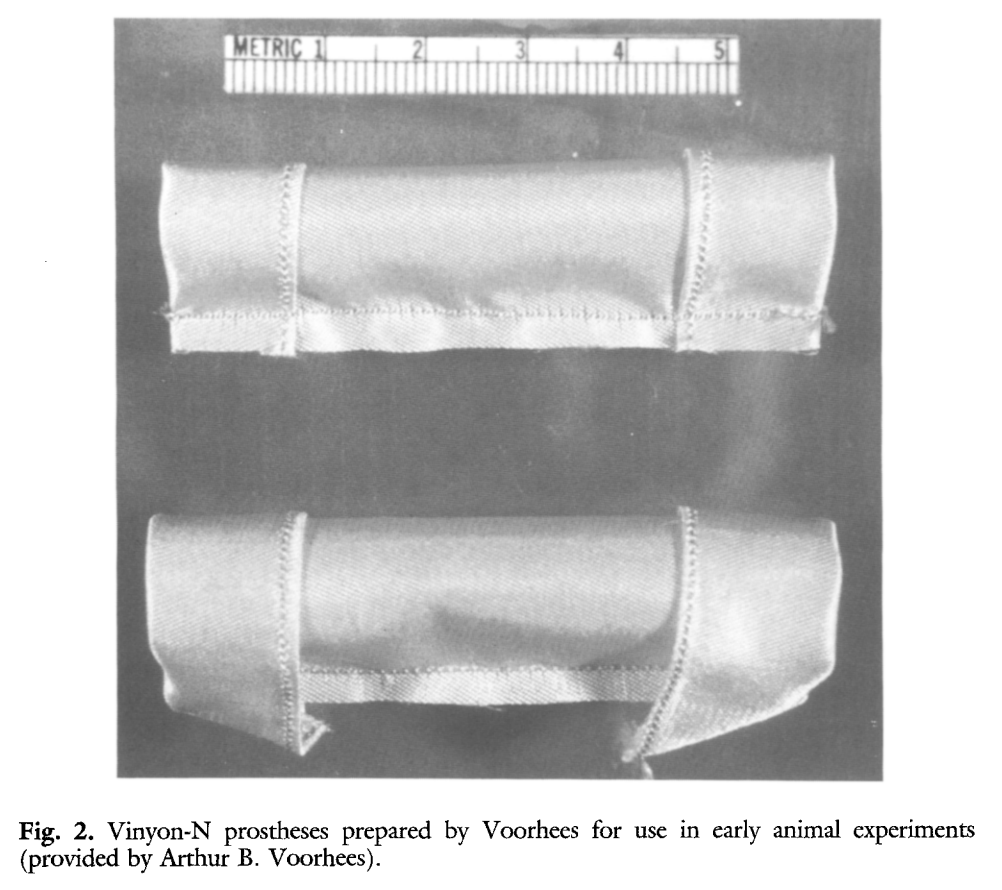
The choice of replacement is becoming clearer in that while rifampin soaked grafts offer immediacy and expedience, all grafts seem to be prone to reinfection at a higher rate than autologous material (ref 3). The NAIS bypass is a great option, but is hampered by the addition of several hours invested in harvest of the femoral veins. While it can be staged with mobilization done one day and harvest another, those added hours add complications. We often forget that the simple metric of procedure time is the most important determinant of complication rate. Any operation going over 2 hours risks wound infection for example simply from ambient colonization of the open wounds from the rain of dead skin from the surgeon’s face, aerosolized fecal flora from flatii (prohibited in my ORs). The microenvironment of the open wound is also room temperature and not 37, having an impact on organ function and hemostasis. The homograft is the original aortic graft -before Arthur Voorhees invented the cloth vascular graft as a resident at Columbia P&S (my medical school alma mater, ref 4), major hospitals had tissue banks of aortic homografts harvested from the recently deceased. Having homografts is now an outsourced function, but does require having proper refrigeration for the cyropreserved grafts and generally can’t be ordered with short notice.
Rifampin soaked grafts work well, especially wrapped in omental flap, in the short and medium term but suffer a reinfection rate that is higher than seen with autologous tissues, and prosthetic grafts without rifampin, such as PTFE for extraanatomic bypass, have the highest rates of reinfection (3), despite being the board answer decades ago.
Endarterectomy allows for use of native tissues for repair. The adventitia around plaque and stents, while thin, can support physiologic pressures, even when they have been occluded for years. And while practice of aortoiliac endarterectomy is a bit of a lost art, it has both a long history stretching back nearly a century and a modern track record with carotid and femoral endarterectomy. It is merely a matter of scale. Pinch and zoom in on a femoral endarterectomy at the bifurcation and you have the same case as with an aortic one.
The question is, is bovine pericardium more autologous than prosthetic? It is a decellularized sheet of collagen from a cow’s pericardium, used in heart valves and vascular patches, but only recently applied as a graft (ref 5-7). I have long used bovine pericardium as a patch with some caution, but the rule of thumb is are there well vascularized tissues around it? A layer of Scarpa’s fascia and fat in a groin wound are not sufficient to protect a bovine patch, but a sartorius flap is. For me, once the infected stent graft is out, knowing if the surrounding tissues bleeds well is an important one.
I chose to do aortoiliac endarterectomy. The patch and graft would be made with bovine pericardium, unless I found the left iliac segment to be devitalized and foul with anaerobic vapors, then, I would close and go NAIS or extra-anatomic. The key point is that choices have to be on the table and constantly rearranged during the conduct of the operation.
The patient was preoperatively vein mapped and had suitable deep femoral vein for bypass conduit, having robust duplicated systems that would impact the patient minimally. The patient was placed in a supine position and via a midline laparotomy, the infrarenal aorta and the common iliac arteries beyond the short iliac stents exposed. I chose this limited exposure as any further into the phlegmon on the left risk injury to ureter and vein. The aorta had a palpable demarcation between plaque and mildly diseased proximal segment, predicted by the CTA to be at the IMA. A longitudinal arteriotomy was created on the right side from mid aorta to mid right iliac, and the left side had a separate arteriotomy to release the stent. The plaque came out in a single specimen (image).
The exposed stent is the left iliac stent holding within a stent graft.
The left iliac artery was destroyed by the infection but the tissues around it bled avidly and were not foul or infected. I avoided excess debridement here as the iliac vein was intimate with the phlegmon. There was a 3cm gap. Again, I thought briefly about taking femoral vein, but proceeded to make a graft from the bovine pericardium. This was sewn around the rod portion of a renal vein retractor from the OMNI set. The finished product resembled Voorhees’ graft. It was sewn into the orifice of the iliac from inside the aorta and end to end to the freshened iliac stump. Unfortunately, the omentum was atropic across the transverse colon, but the tissues around the resected artery and stent graft bled well, indicating good penetration of antibiotic. The retroperitoneum was closed after hemostasis obtained. Dr. Shashank Sharma, our chief resident headed to a vascular surgery fellowship at the renown Houston Methodist next year got to see what is unfortunately a rare occurrence -an aortoiliac endarterectomy, which through me puts him three degrees of separation from Cid Dos Santos (ref 8). Dr. D’Andre Williams, PGY-2 Vascular Surgery Resident, got important lessons on sewing the aorta. She’s part of a fortunate cohort that get exposed to open aortic surgery at our main campus which is unfortunately rare throughout the world.
The pericardium was soaked in rifampin, but probably did not bond to the collagen.
The final graphic shows the operative end result.
The patient recovered well and was discharged within the week with another month of IV antibiotics planned.
Before and After
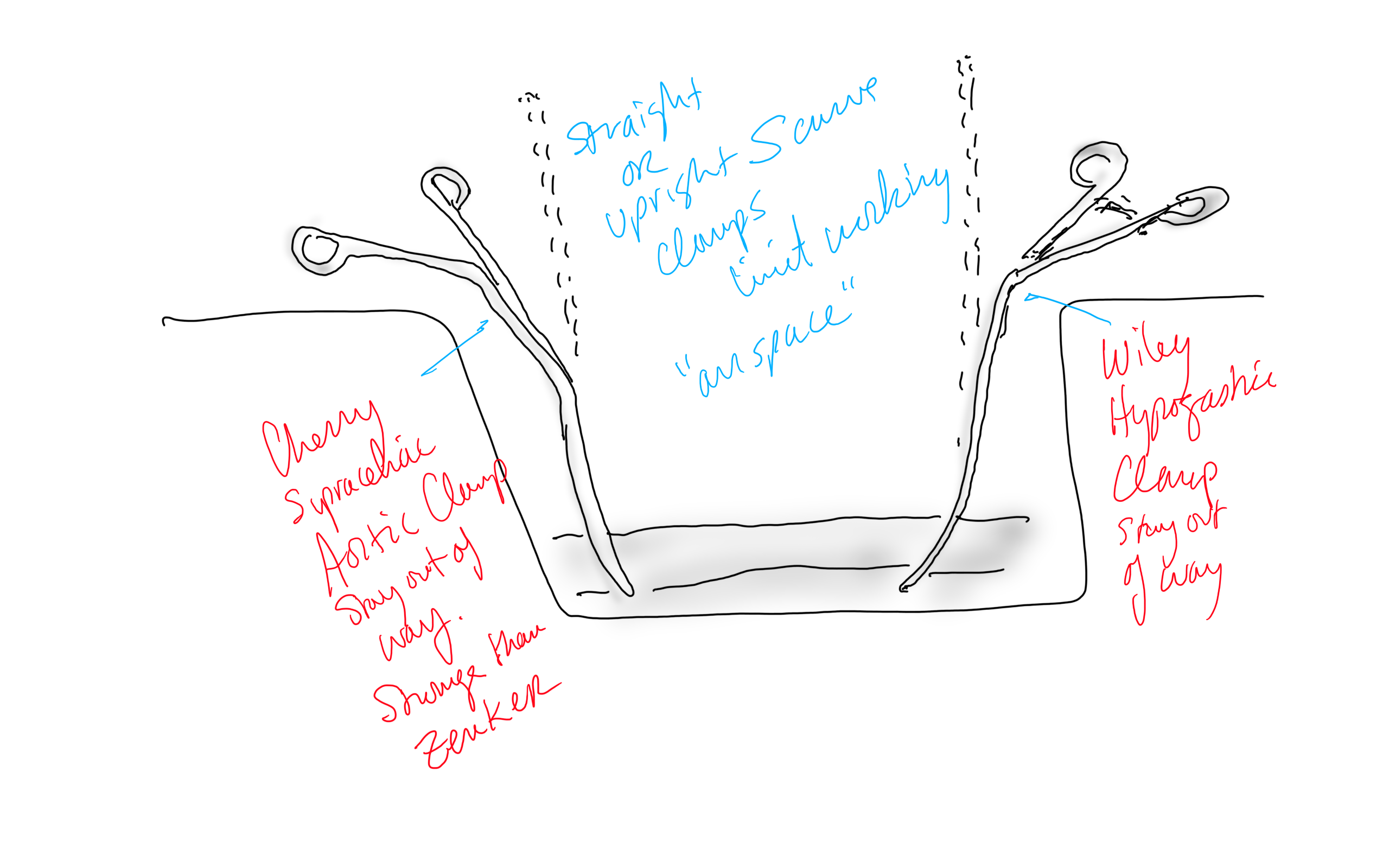
Conclusion: The operation was started at 8 in the morning and was done by lunch time. For aortic cases, this is a crucial metric, as when the clock winds past the surgeon’s comfort, the patient suffers even more. Adding the femoral vein for a NAIS may have been the textbook thing to do, but we don’t do extra-anatomic bypasses that much either. I don’t believe that adding two more hours for retrieving the femoral vein would have enhanced the procedure, and would have served to add potential areas for complication. Technically, the aorta closes much as with a carotid or femoral endarterectomy, but the adventia is thin and really should be sewn with 5-0 or 6-0 Prolene. The larger needles such as the SH size creates unnecessary bleeding unless sewn with a line of felt which could become infected. Despite the thinness, it will hold pressure if it is not infected. Clamps that bend out of the “airspace” above the laparotomy, such as the Cherry Supraceliac Clamp and Wiley Hypogastric Clamp, prevent limiting the operative space with long clamps such as aortic Fogarty or DeBakey clamps, while being stronger than the Zenker.
A final comment for Staphyloccocus lugudensis. This is the second major vascular graft infection with this organism I encountered this year. The other was an infected aortic stent graft. Lugudensis means from Lyons. I do not know why that is, but it is so far not the nasty player that is S. aureus. I am sure it will share some plasmids, and become resistant one day, but in the earlier case in Abu Dhabi and now this, it is sensitive to penicillin, and came from the skin at the femoral puncture site, and for this we are fortunate. Major vascular infections are one of the few areas that still demand open surgical skills, and we foresake them at great peril. It’s critical to remember all the collective memory of surgery from the past, or we will become mere technicians fixing whatever comes out of the radiologist’s report with whatever knowledge obtained from a Zoom meeting for the latest, greatest device.
Acknowledgement
Gratefully, the patient gave his permission, as with all patient, for use of his case for educational purposes.
References
Chung J, Clagett GP. Neoaortoiliac System (NAIS) procedure for the treatment of the infected aortic graft. Semin Vasc Surg. 2011 Dec;24(4):220-6. doi: 10.1053/j.semvascsurg.2011.10.012. PMID: 22230677.
Oderich GS, Bower TC, Hofer J, Kalra M, Duncan AA, Wilson JW, Cha S, Gloviczki P. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011 Jan;53(1):99-106, 107.e1-7; discussion 106-7. doi: 10.1016/j.jvs.2010.08.018. PMID: 21184932.
Smith RB 3rd. Arthur B. Voorhees, Jr.: pioneer vascular surgeon. J Vasc Surg. 1993 Sep;18(3):341-8. PMID: 8377227.
Almási-Sperling V, Heger D, Meyer A, Lang W, Rother U. Treatment of aortic and peripheral prosthetic graft infections with bovine pericardium. J Vasc Surg. 2020 Feb;71(2):592-598. doi: 10.1016/j.jvs.2019.04.485. Epub 2019 Jul 18. PMID: 31327614.
Lutz B, Reeps C, Biro G, Knappich C, Zimmermann A, Eckstein HH. Bovine Pericardium as New Technical Option for In Situ Reconstruction of Aortic Graft Infection. Ann Vasc Surg. 2017 May;41:118-126. doi: 10.1016/j.avsg.2016.07.098. Epub 2016 Nov 27. PMID: 27903471.
Belkorissat RA, Sadoul C, Bouziane Z, Saba C, Salomon C, Malikov S, Settembre N. Tubular Reconstruction with Bovine Pericardium Xenografts to Treat Native Aortic Infections. Ann Vasc Surg. 2020 Apr;64:27-32. doi: 10.1016/j.avsg.2019.10.104. Epub 2020 Jan 10. PMID: 31931127.
Barker WF. A history of endarterectomy. Perspectives in Vascular and Endovascular Therapy. 1991;4(1)1-12. doi:10.1177/153100359100400102
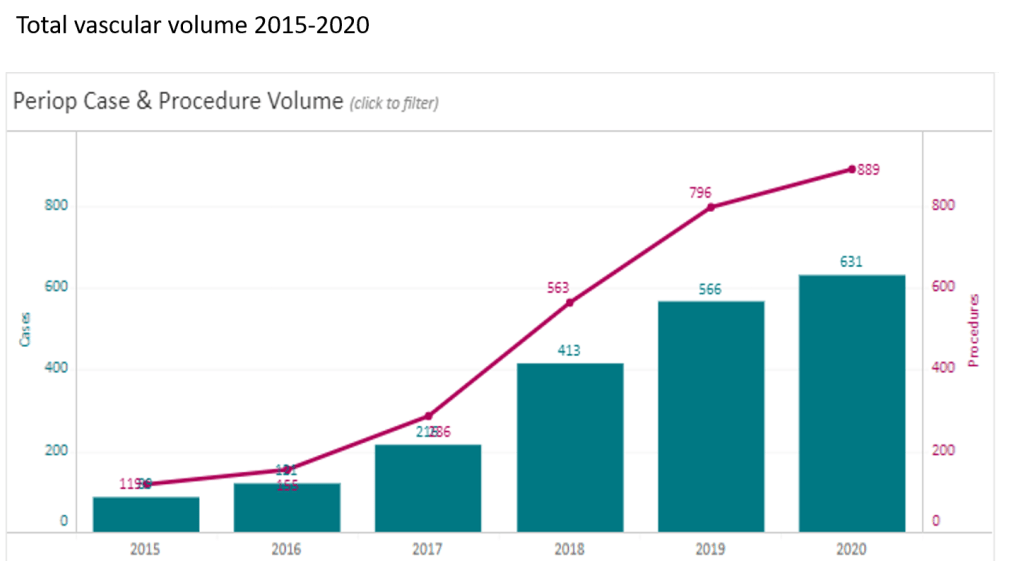
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
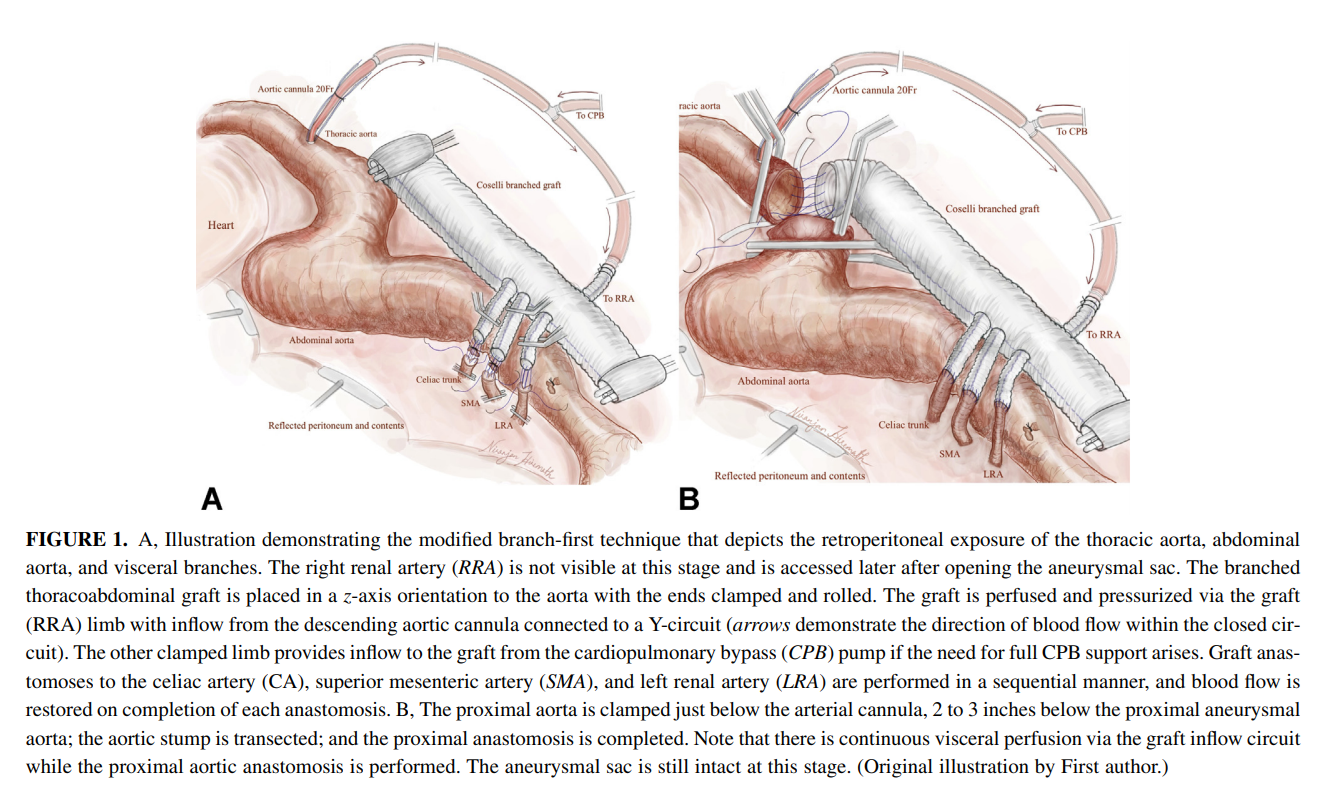
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
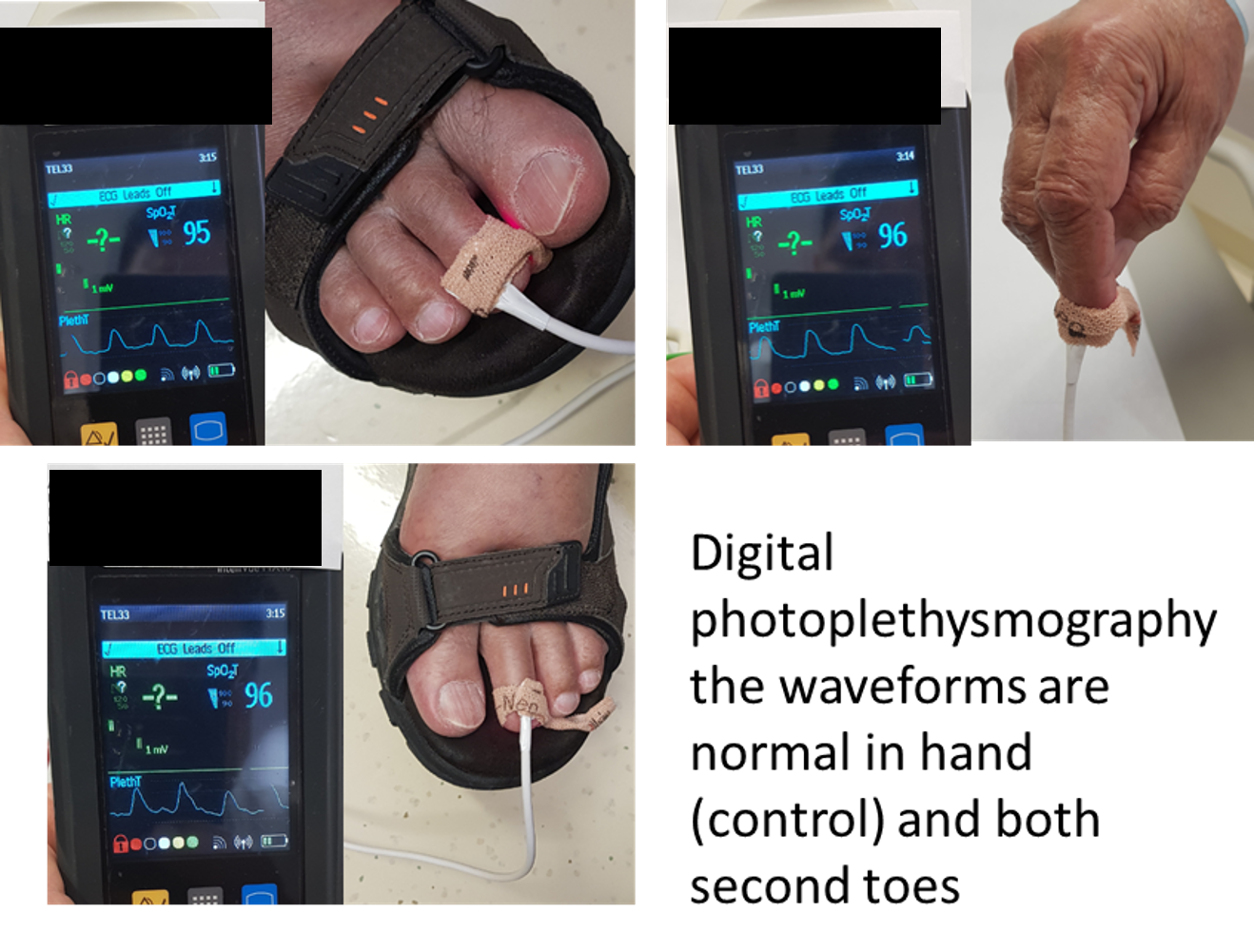
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.
This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).
an abnormal DPPG captured with a hospital ICU pulse oximeter
We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).
At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).
The distal perfusion cannula is in the dorsalis pedis artery
This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery
The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).
Pulmonary artery staple line bleeding controlled, ready for suturing.
In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.