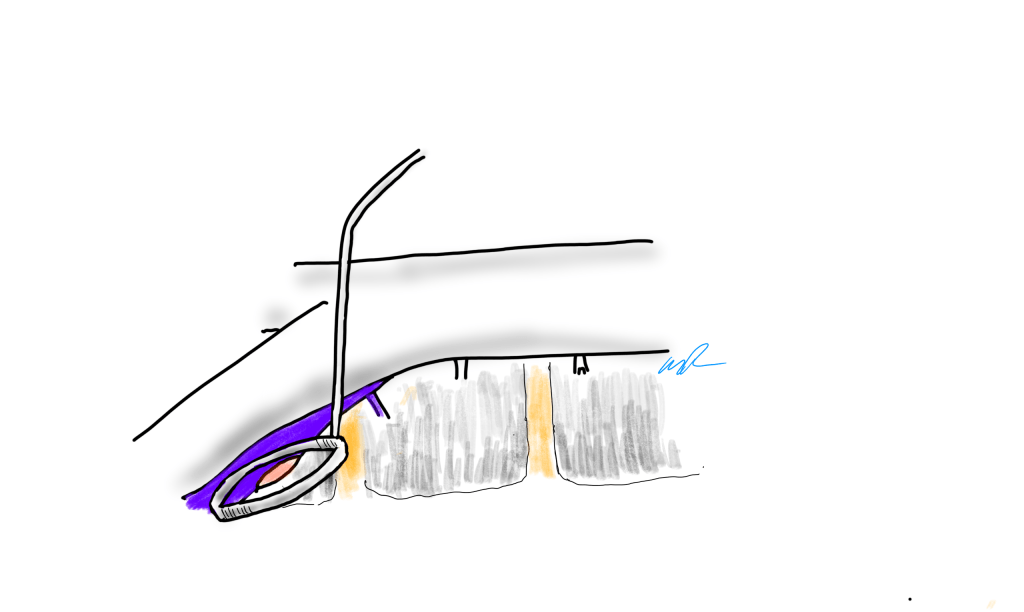
During a thoracoscopic lung resection, bleeding along staple lines, even of the main pulmonary artery, can be managed with a Park Clamp
The Park Clamp isn’t a true clamp, but rather a compressor. It was designed initialy for the troublesome venous bleeding. It is a ring with ridged edges to provide grip securely welded to a handle. It allows for circumferential compression of tissues, allowing for hemostasis while creating a open space for suturing. The picture above are my colleagues from CCAD -Drs. Andres Obeso and Redha Souilamas perfoming a partial pneumonectomy. The staple line on the artery was bleeding and this can be troublesome, and may require conversion to thoracotomy. The Park Clamp was inserted and provided excellent hemostasis (below).
Hemostasis achieved, a suture can be placed without ongoing hemorrhage without having to convert to a thoracotomy
During one of my cases as a fellow at the Mayo Clinic, I ran into venous bleeding behind the aortic bifurcation. Dr. Thomas Bower, recently retired, came in and lengthened the incision to create more space for more hands, and got all of us -me, the resident, the intern, the RNFA’s, to retract and compress with sponge-on-a-stick to repair the linear tear on the vena cava under the aortic bifurcation.
I’ve always hated this approach because outside of Mayo in 2002, it is very hard to get five people to become your voice activated retractor system, and the sponge on a stick only works well when you are on the hole and less effectively next to the hole. There had to be a better way.
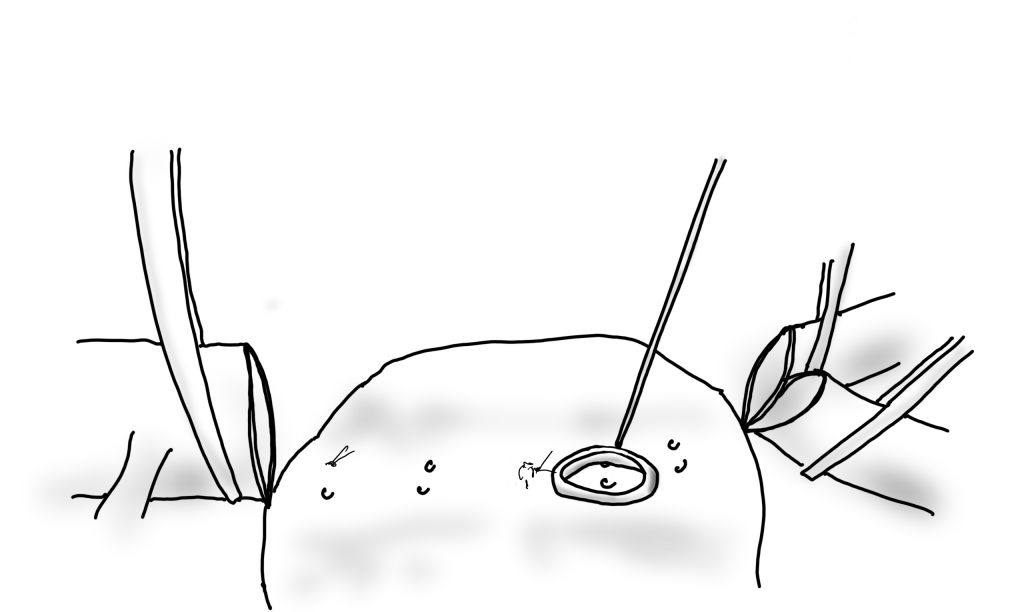
Spinal exposure at the L5-S1 level is treacherous because of the veins
When I returned to academic practice at the Cleveland Clinic, combined cases with other specialties got me operating on tight spaces, frequently heavily scarred, with many blood vessels to control, such as a retroperitoneal spinal exposure illustrated above.
The veins are fragile here and as they are in communication with the central veins, bleed copiously and rapidly.
Look above at the dreaded linear tear on the left iliac vein that can result from simple manipulation of this fragile structure -typically a tributary vein will anchor the iliac and simple retraction can cause a tear.
Sponge on a stick limits view of the injury
Using a sponge on a stick greatly hampers your ability to repair the injury. First, the people applying the sponge on a stick have to have some skill. Second, because they are long and straight, they are constrained by the incision you have created. When applied, the “airspace” above the injury is greatly reduced. Third, hemostasis is never complete unless the whole vein is compressed, which is challenging in the above scenario.
The handle can be bent to create more “airspace” for operating
When the ring is applied, two things happen. Hemostasis is in general complete and there is room to operate, in this case suture. Even in the instance where an artery is bleeding from a flat surface as in a bleeding duodenal ulcer or a lumbar artery in an open aorta, hemostasis is achievable.
Bleeding lumbar arterise can cause a significant blood loss in the time it takes to apply a suture. Fingers will occlude, but no one likes getting stuck with a needle.
The bleeding lumbar artery illustrated above responds well to ring compression. This is also the case where you have bleeding from scarred or irradiated tissue surfaces, or from varicose veins or AV fistulae from the skin. If you don’t have a Park Clamp, you can use the finger rings of the handle on a tonsil or Kelly clamp.
If you don’t have a Park Clamp, you can have one made or you can use the ring handle of a standard clamp.
There seems to be interest among surgeons who have seen this device used, and I will look into manufacturing these. I would not object to surgeons making their own for their personal use -taking apart a long tonsil clamp and bending the ring at a right angle should be simple enough. The clamps I use were manufactured at our prototypic facilities, but 3D printed ones should work fine.
And I will leave you with this final thought. I am in the profession of surgery, and at its core, it’s about helping the patient. If you adapt this idea and help someone, I will have fulfilled my duties.
The Long of It and the Short, or What You Are Trying to Do With That Level 82 Note on Your EMR?
I struggle to keep my sanity reading through electronic medical records. Medical billing pays by the amount of note written. Back in the 90’s, the insurance companies demanded that paper records be sent by mail or fax to confirm billing. Clerks in medical records departments would spend the whole day copying and faxing stacks of charts to payers and billers. EMRs were suppose to solve this, but the paradigm of the paper record lives on. Each note in the EMR is printable as a paper record for billing. It is a static text document. And like in the 90’s, billing is based on the amount of note written into the EMR. The simplest way to achieve this is to copy and paste what already exists elsewhere in the EMR -a past note, a systems review, a medical history, a spreadsheet of lab results, imaging reports. This gets you more note, more billing. The electronic medical record succeeds in its primary function as a cardboard box of copied records and as a cash register, but fails miserably in being an active part of patient care.
Any sane system would allow you to pick links to prior notes or tests -a referencing system to include even published articles, to show your logic and data, while allowing you to focus on the information that is important at the moment. The modern note needs to be turned into a searchable, linkable, living element in a dynamic database reflecting the patient’s status, a powerful tool in the patient’s care. There needs to be an App Store where third party vendors can craft solutions not imagined by the EMR. There needs to be a common file format to allow for interoperability and easy transfer of records between institutions -like JPGs and MPGs. There needs to be a complete re-engineering of the user interface. The various caregivers interacting with the EMR need to be allowed to input data in non-linear ways using mobile devices. The EMR needs to evolve to being a platform.
The Blue Ink
When I was a fellow in 2000, one of my staff, Ken Cherry, had this distinct light blue ink in his fountain pen that he wrote notes with in pithy, grammatically correct sentences conveying the diagnosis and plan. It was up to me, his fellow, to write the more detailed note, but there at the bottom, in a sky blue cursive fit for the Declaration of Independence, was the word. You just had to look for that ink in the chart to understand where the patient was and where he was going. He’d write something like, “This patient, who was seen in clinic with classic Leriche Syndrome, is now admitted with rest pain in his right foot. I intend to revascularize him after appropriate workup. My fellow will make these arrangements.” Stylistically, it was wonderful, but assumed a lot of contextual knowledge about Leriche Syndrome, and if you didn’t know, you could read Park’s two page note. He’s making the arrangements.
Compare that to an imaginary level 19 note (won’t burden you with it), rotten with copy pasted operative note and prior discharge summary, spreadsheet of laboratory values, and 12 system review of systems, 12 organ system examination, and multiparty listing of every organ in impression, bullet pointed plan, never mind that many of these have no relationship to the problem at hand. The first note is a financial disaster as it cannot be maximally billed, but it is full of meaning and action. The second note is unreadable and therefore likely unread. Like those strange tropical fruits that take power tools to get to a small bit of sweet at the center, the level 23 notes littering electronic medical records take time to pore over the chaff to get to the point which is often hidden -day to day only a few things may actually change on a note. There is just too much husk. Most of the action, the orders, have to be typed back into the note rather than automatically populating it. Supposedly, that function exists but the software has been written with the user interface of Windows from the early 1990’s and the functions are buried, only to be fished out by superusers and support staff that take time away from clinical duties to read about and learn.
Context Implied and Explicit
The fashioning of a good note recognizes that too much implied context results in confusion. Rather than say, “Leriche Syndrome,” one should say, “aortoiliac occlusive disease from advanced atherosclerosis resulting in a symptom complex of severe claudication known by the moniker, Leriche Syndrome.” The note needs to educate as much as it does document. The exposition of expertise needs to be explicit for the note to show value. Value and bill-ability do not live on the same axis. The reader should come away from the note with maximal meaning in the shortest amount of time. That means most consult notes and H&P’s need to be ideally case studies and earn their length and perform a teaching function.
Copy/Paste -Note as EMR Fractal
The position of the average physician is a poor one. The need to bill means writing long notes, but physically typing and formatting long notes is a drudgery that occupies a significant time away from seeing patients, performing procedures on patients, and thinking. The easy solution to this dilemma, the lack of time, is the Copy/Paste. There are notes where the entirety of past notes is copy pasted, creating a self-repeating element like a fractal where the entire EMR is reflected in the note. Like error mutations of the genes that persist and damage organisms, copying and pasting of documentation errors perpetuates itself and can cause disease. I remember years ago as a young staff being stuck by a needle during a procedure and dying a little inside when I checked the chart and found the patient was HIV positive. When I talked to the patient, I found out that was a persistent error, manually copied and pasted by residents and consultants, billed as a diagnosis, resulting in years of problems for the patient who had to threaten lawsuits to expunge that HIV status. Each note should be unique and uniquely authored by the caregiver, and if there is not much to report, necessarily brief. A daily summary should be generatable like those news apps that can scrape headlines and context out of the day’s production from the internet and present it to you in a easy to consume quadrilateral of data.
The Shield -Speaking to the Jury
A proper note will protect you. It is the only shield that protects you along with your education and reputation. Civil proceedings involve going over these notes in great detail and the notes should be either unimpeachably explicit or vague like a fortune cookie. Even the limited tech of current EMRs allows you to achieve granular levels of detail. I recommend referencing (but not copy/pasting) important societal guidelines and journal articles that reflect your thinking, but it the EMR does not make this easy. The hack is keeping these references as a macro to spew out relevant text. For example, if you chose not to operate on a 5.4cm AAA, after referencing the CT scan report, an image showing your measuring line, and the growth velocity from prior scans if available, a line reference to the SVS guidelines spat out by a macro gives you some shielding. But more important, in the ideal EMR, that reference would be that characteristic blue color of a hypertext link to the pubmed reference or PDF download. Hyperlinks within EMRs should be a thing. Your EMR note should be a hypertext document, not a text document, and allow referencing other notes and reports without copy/pasting them. Images, audio, and video should live within your EMR note as naturally as they do in every other document you create in 2020 that does not have to be excreted through a printer. The fact that these functions are extraneous to the primary function of the EMR -to be cheap to produce and maintain, and good for billing, means no innovation will occur for EMRs.
The Platform
EMRs vendors cling to their market share by making sharing of data impossible through proprietary data formats and security regimes. Health care systems have no incentive to make their patient information transferable beyond a minimum of paper or their PDF equivalent. Patient safety and information security is invoked for preventing needed innovation. For the patient, this can be a life or death issue -the ability to transfer health care data. Imagine if you are the patient with a ruptured aortic aneurysm who is transferred without the CT scan burned to a CD. In 2020, NO.ONE.USES.CD’s. I can download a 4K file of the last Avenger’s movie in 30 seconds on the right network, but a lifesaving CT scan -NO WAY!
A more everyday example is a patient seeking a second opinion or moving cities to a different health care system. The only way to move the data is an expensive printout of the chart. How can we keep this important information linked with the patient? Social media has cracked this. Your Facebook is a good model of what a potential EMR 2.0 could be. A patient-centric EMR would be controlled by the patient in terms of access control. Federal laws would prevent misbehavior by the EMR vendor. The patient’s data generated by practices or hospitals would be owned by these practices or hospitals but posted on the patient’s EMR, in specific specialty adapted formats. Temporal ordering would be natural, not based on shuffling reams of paper or virtually with PDFs with overlapping timelines. More importantly, imaging data and lab results would be immediately available to all healthcare providers through access to the patient’s EMR. Practices and hospitals would pay a nominal fee to the EMR provider much as advertisers are on Facebook. Patients would be in control of who gets access to the data, and importantly if they want to participate in research. App developers would proliferate and innovate in the space, providing functionality via apps in a marketplace, allowing different specialists look at the data in their own particular way, and patients to understand their data on their own terms. Gaming companies, for example, could take the virtual coordinates of a CT scan and match it up with ultrasound and MRI to do a lot of cool stuff. EMR 2.0 is not more ways to personalize your window with colorful graphics. EMR 2.0 is a complete upending of the way patient data is stored and moved, and it will take an act of Congress to make this happen. EMR 2.0 recognizes that it needs to become a platform and it needs to be a part of a collective national effort. EMR 2.0 needs to be a platform, not an app.
A Multimedia EMR
The EMR needs to incorporate multimedia. Current EMRs live in the tech levels of the early 1990’s. Imaging studies must live as actual windows in chart notes. Video or voice comments must be documentable in the chart. Hypertext to the resources of the internet must live in the chart. Data must flow just like blood.
This should suffice as an op note
Shape of the Future
As a vascular surgeon, the most important function is to provide an accurate documentation of the condition of the blood vessels to date, the current condition of the blood vessels, and the future fate of the blood vessels and the patient. Technology needs to help the vascular surgeon in this role, and most importantly, the patient. Tech is not a third party vendor in this battle space. Tech is a caregiver, and must be held to the same standards placed on physicians, nurses, and technicians. Until that day comes, we as vascular surgeons must write amazing, publishable case reports for the consult notes, and short pithy updates for the subsequent notes.
It is a rare day that passes without the announcement of a stroke alert at CCAD. A reflex arc of activity is initiated, as time becomes the critical metric of success. Patients with strokes have a limited window of time to reverse the effects of the arterial occlusion, and the whole hospital is organized around getting the patient into the angiographic suite to open up blood vessels. If you watch it happen, it is the pinnacle of modern medicine, to achieve what only a decade ago was deemed unachievable. It was built around a foundation laid by cardiologists for heart attacks -the STEMI alert. The teams practice like racing pit crews with a stopwatch to get a patient from the emergency room, to CT scan, to angio suite. A long time ago, as a young surgeon, I had to work hard to get institutional support of ruptured AAA and cold legs. Vascular surgery has traditionally struggled to get recognition for its patients, their diseases, and its work, which is nothing less than the most important safety net for any large general multi-specialty hospital, critical infrastructure like oxygen plumbing and backup generators. As I transition to that weird designation of mid-career surgeon (please don’t call me a senior surgeon), I have also appreciated that Steve Jobs aphorism about good artists copying, great artists stealing. It’s only stealing if you don’t give credit. Here is what I borrowed from the neurologists.
Acute mesenteric ischemia is an abdominal stroke. Use it in your conversations with other people as you speed your patients way into the angio suite. The reflex arc is in there. For the emergency department, the operating room, and all the physicians, acute mesenteric ischemia sounds like tummy trouble, but abdominal stroke brings sudden clarity to conversations like:
“Well, you’re in line behind a gallbladder and a cystoscopy. Is the patient NPO?”
Me: “It’s an abdominal stroke. We literally only have a few hours before the patient dies…”
“I’ll bring the backup team in!”
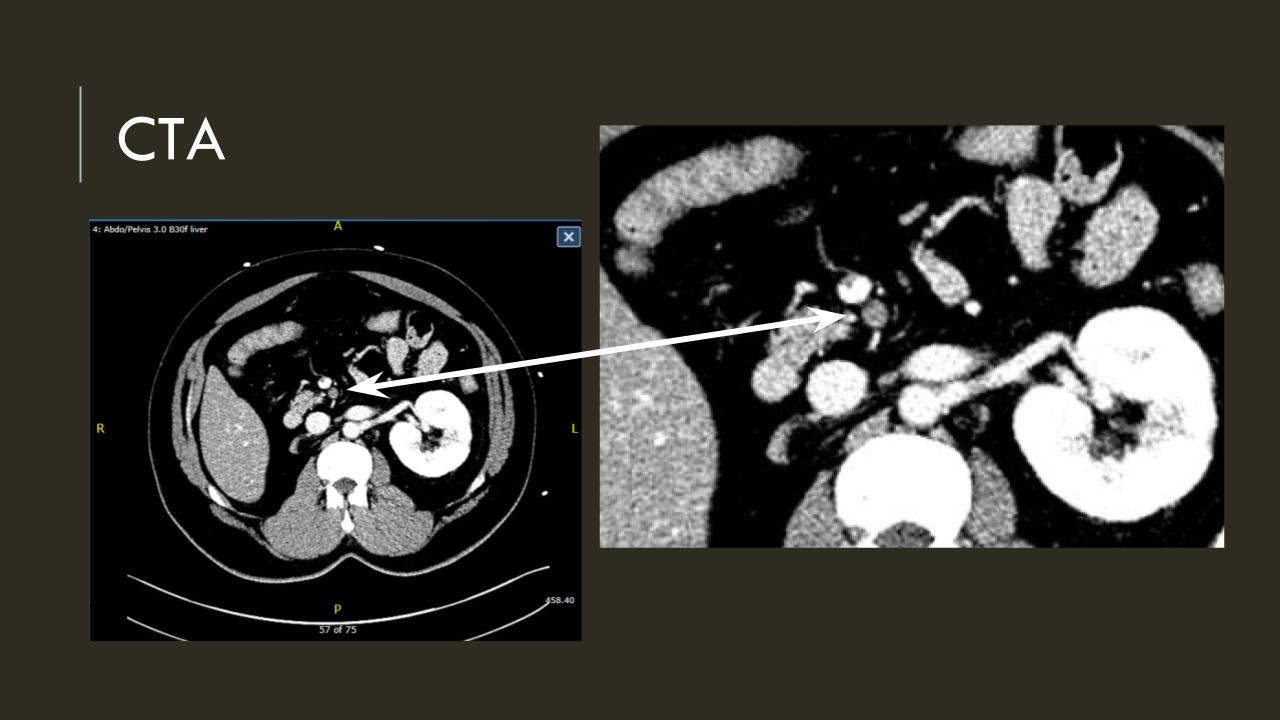
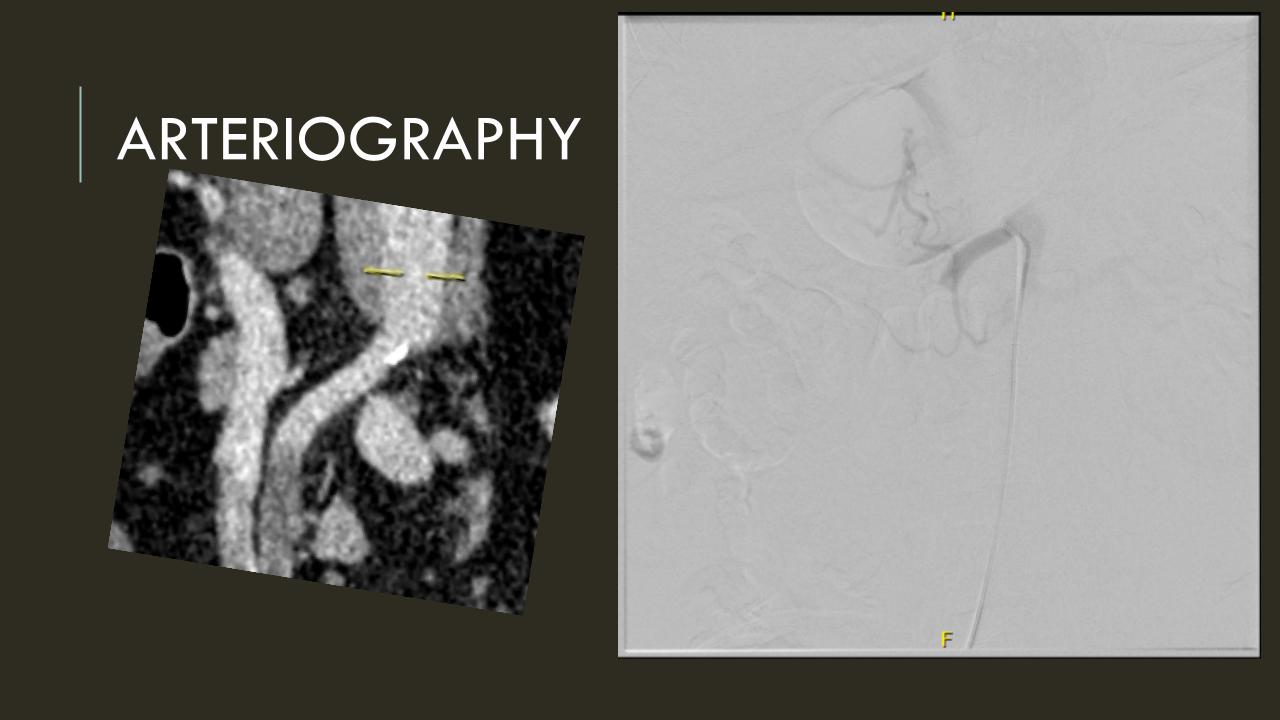
The patient is a middle aged man with risk factors of NIDDM and prior history of DVT who developed severe mid-abdominal pain at 5pm. He came to the ED at around 11pm and had a general surgery consultation who ordered a CT Angiogram showing SMA occlusion (pictured below).
Heparin was started, and at 11:30, vascular surgery was consulted. The patient had a soft, doughy texture to his abdomen, but great pain with palpation -classic pain out of proportion to the exam. Determining the patient to have acute mesenteric ischemia from a thromboembolism, I took the patient to our hybrid angiographic OR suite with the plan for arteriography, possible open thrombectomy, and exploratory laparotomy. Arteriography from femoral access showed an occlusion of the SMA beyond the middle colic artery, a typical pattern for an embolism that occurs when embolism lodges distally and propogates proximally (image below).
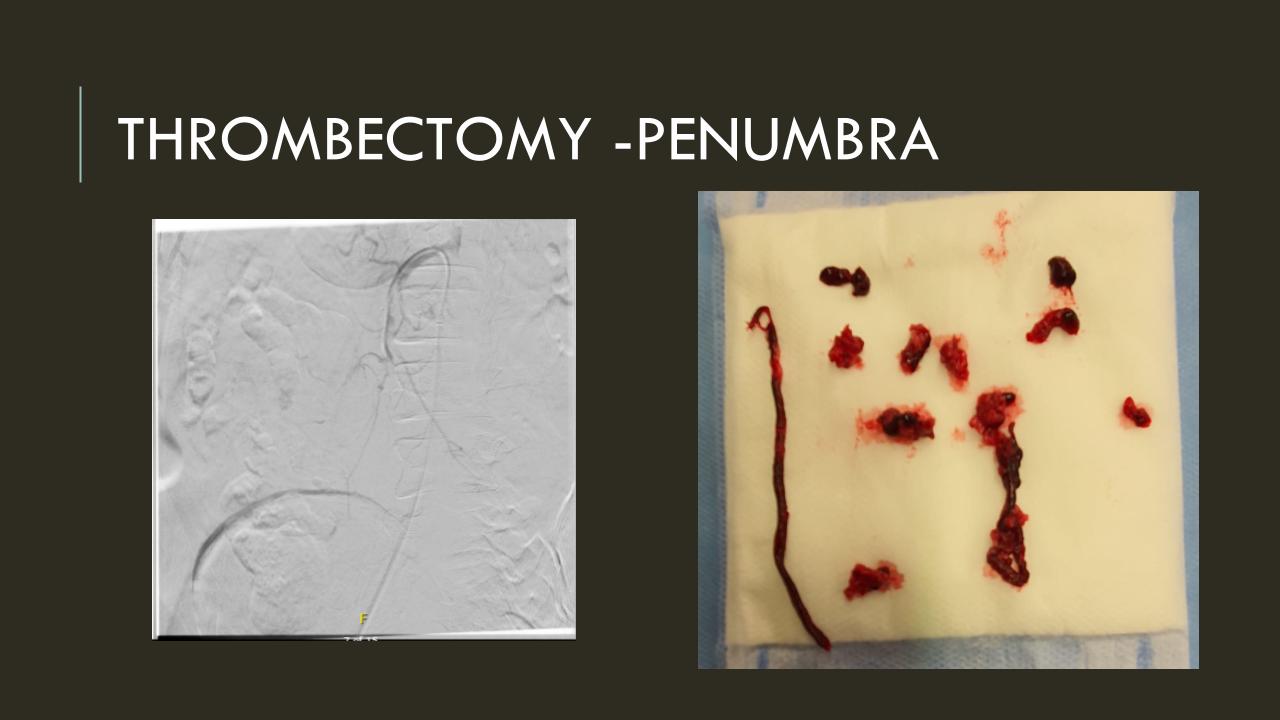
I got Glidewire access into the ileocolic terminus of the SMA, exchanged for a Rosen wire, over which I placed an 8F sheath into the proximal SMA. This was a rather large sheath meant to catch thrombus as I suctioned it out with a 6F Penumbra catheter. This is another technique I borrowed from the neurointerventionalists. Whenever a stroke alert is going on, curiosity drives me to peak in and see what marvelous gadget or gewgaw they are using, and I was impressed by how efficiently the neurointerventionalists were able to get to the smallest thrombus in the furthest branch vessels. I was prepped for open thrombectomy, consented for bypass if necessary, but having experience in suctioning clot through single catheters and sheaths, I thought the simple design of the Penumbra and its efficacy in the cerebral system could easily translate into the mesenteric.The problem with open thrombectomy is the inability to see if you have cleared thrombus from all the branches unless you do an arteriogram after you’ve completed your procedure. This may be a significant contributor to the 20-30% bowel resection rate that occurs on second look laparotomy in my old paper and in the literature since its publication.
The Penumbra was effective in removing much of the fresh thrombus, but I was also cognizant of the fact that pulling out the catheter will draw clot into the 8F sheath that did not make it into the catheter. I placed a wire, and removed the sheath to expel much of the bulky thrombus (picture below).
The completion angiogram (below) doesn’t show the intermediate angiograms showing thrombus that embolized to other arteries as I manipulated the catheters and thrombectomized -I was able to successfully retrieve these with selective catheterization, another neurointerventional series of maneuvers that I have successfully borrowed.
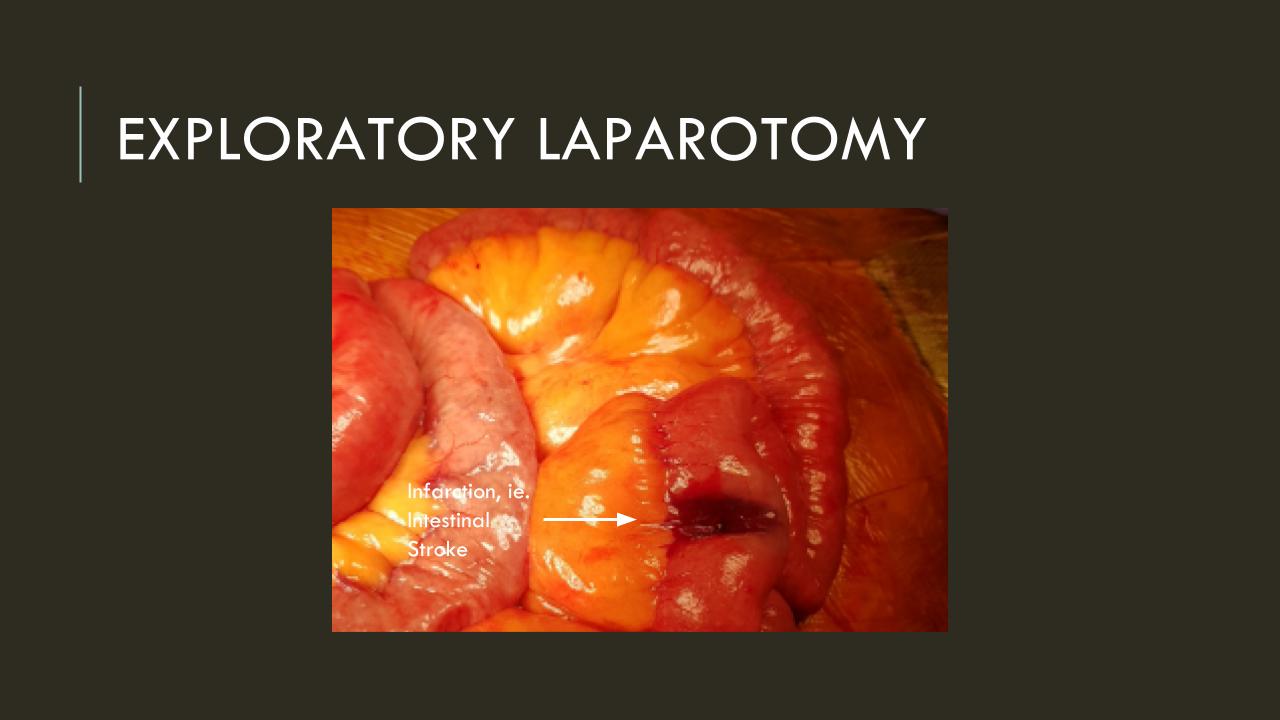
After being satisfied with the completion, I removed the sheaths and explored the abdomen finding this segment of infarcted small bowel (next image).
There was no question in my mind that there would be some dead bowel based on the time course described by the patient. Despite my excitement about calling for GIA staplers -I am general surgery boarded- I called in the general surgeons for their help in resecting and anastomosing this segment of bowel. They would be the ones taking the patient back for any second look laparotomy, although in this patient, I determined that there would likely be no need. After the anastomosis was completed, I did a Wood’s Lamp examination (pictured), which is accomplished with a black light after giving the patient an ampule or two of Fluorescein.
The bowel had a splotchy fluorescence pattern which is typical of ischemia-reperfusion. This is where you have to ask the anesthesiologist and any critical care specialist who follows -no pressors please! Edema won’t kill an anastomosis as badly as ischemia will, and the gut is as sensitive to norepinephrine as are the toes. Workup in the hospital including echocardiography and CTA of the entire aorta failed to reveal a proximal source or cardiac shunts or thrombus. The patient recovered and has recently followed up, eating well, and tolerating his anticoagulation which he will be on for life. I sent out the pictures to my neurointerventional friends with some glee, but also with the purpose of informing them that in the case that the vascular surgeons become incapacitated or quarantined due to the COVID-19 pandemic, their skills would be recruited in the care of an abdominal stroke -a blood vessel is a blood vessel. Acute mesenteric ischemia should be the first thing on everyone’s differential of sudden onset abdominal pain because of its time dependence, yet it does not have the same resonance to the unfamiliar as abdominal stroke. Survival is dismal when too much time and intestinal death has occurred. When associated with the stroke alert concept, it translates into processes already in place throughout the hospital and it becomes natural for everyone to appreciate the urgency of treating abdominal stroke. This is the system adopted by Roussel et al. in France, where they have regionalized care of intestinal stroke. They report mortality rate of 6.9%, which is in a selected population, but significantly lower than the traditionally reported 30-60% mortality.
I am still an advocate of an open approach, especially when angiographic resources are unavailable, and every trainee needs to be able to describe the exposure of the SMA, and management of acute mesenteric ischemia. Hopefully, everyone will appreciate the urgency of all the various ischemic conditions manifest in the peripheral circulation, but rebranding them as a stroke (leg stroke, hand stroke, intestinal stroke…) is helpful. Finally, there is no survival with dead bowel -it must be found through exploration and resected.
Reference:
Roussel A, Castel Y, et al. Revascularization of acute mesenteric ischemia after creation of a dedicated multidisciplinary center. J Vasc Surg. 2015 Nov;62(5):1251-6. doi: 10.1016/j.jvs.2015.06.204.
My Lenovo Yogabook C930 recently got a firmware update where the main screen image gets cloned to the e-ink display. By putting the device into tent mode, the LCD screen turns off and you now have a PC on an e-ink screen. Linked to a Bluetooth keyboard, it is a low power focused writing station, albeit with lag. Like other e-Ink screens, there is lag -kind of like a typewriter, but you can see it in full sunlight and theoretically there should be a benefit to battery life although I am holding my horses given the Intel chip burning in this device. I have been advocating for this feature for my e-ink Kindle readers. Imagine if you can write a book on a Kindle! It would be a simple OS update. Come on Amazon! Turn on a simple text editor and sync to the Amazon cloud and call it “Author.”
Kudos to Lenovo for the firmware update. I feel like I am part of a giant beta as the Yogabook C930 is gloriously half-baked. The fingerprint reader is still dreck. Freewrite should take note and hurry up with Traveler!
Distraction Free Writing: Portable, Disconnected, AA Battery Powered
Distraction free writing has been a buzzword. It used to be the norm with computers by their limitations and design to focus you on writing. Today, technology is increasingly put in front of you to entertain and distract. The problem for students and writers is that your computer and phone are gateways to music, video, and communication in ways that were only dreams twenty years ago. The key elements of distraction free writing are a decent keyboard, extended battery life, simple interfaces, lack of connectivity, and absence of party line operators. Each of these elements formed the core of our computers back in the 1980’s, when computers were rarely networked, they were all monochrome, and your words were all that you saw. This desire is driving the market for distraction free writing software and hardware, but you can find ways to create your own portable distraction free writing tools without dropping a fortune. And distraction-free writing is also intrusion-free -something to consider in today’s shifting privacy boundaries. At the end, the best distraction free options may be in reconsidering decades old devices that may be picked up cheaply used or at greatly reduced prices for new. Most current devices are made to last about a thousand recharges, and struggle with purposeful obsolescence. You may find that there are many fine older options that will suit your writing needs while greatly increasing your productivity while avoiding costs.
Consider the keyboards we had back in 1985. They were all mechanical spring keyboards which made a nice click sound. Writing was a tactile pleasure. This was in contrast to the membrane based keys seen on games and toys, and mistakes like the PCjr. You see them today as controls for microwave ovens. The moving keys send a message of accomplishment to your brain. Despite this, flat keyboards with no physical component are still being thrown up to see if they would stick. The smartphone keyboard on the first iPhone killed the physical ones on Blackberry and the Treo’s after all. Manufacturers are still experimenting with flat keyboards such as on the latest Yoga Book’s e-ink keyboard, and the upcoming Microsoft Surface Duo devices.
flat screen based keys like on the latest Yoga Book takes some getting used to
These software and touch display based keyboards rely on spelling correction and ultimately constant connectivity to minimize error. The push for ultra-portability means dispensing with the original mechanical keyboard which was descended from electric typewriters like the IBM Selectric. This resulted in the terribly mushy, mass produced keyboards introduced in the 1990’s, getting ever worse. The high point of this design viewpoint was introduced in the 2015 MacBook and recently retired in the 2019 Macbook Pro when Apple realized everyone hated typing on superflat keys meant to accommodate flatness over functionality. There is a welcome movement back to reasonable keyboards. I would even claim that the persistent life and value of the Thinkpad line is the focus on the keyboard that remains preserved after IBM sold it to Lenovo. The new-old keyboard on the 2019 MacBook Pro 16’s are a concession to the realization that typing is a core function of these machines.
There is a push back as writers, office workers, and gamers have created a market for mechanical keyboards. These are usually Bluetooth connected devices, and typically paired to tablets for writing. Unfortunately, separate keyboards connected to tablets are not as portable as a laptop.
QWERKYwriter is a retro mechanical keyboard for tablets but try taking that onto an airplane
I would argue that laptops are not as portable as they could be. The Freewrite (link) was designed with writers in mind as an update to electric typewriters with cloudbased file management and an e-ink display with days of battery life on a single charge. I almost bought one but the small display and the relatively bulky size kept me from springing. I have ordered a Freewrite Traveler (link) which is their mini-laptop version, but since I ordered one last spring, it has remained vaporware with its delivery date pushed back from summer 2019 to spring 2020.
Battery life is a sore point for me. Laptops are now expected to be wonderful if they exceed 8 hours of battery life, but I remember that the original portable computers like the Radio Shack 100 series could go days on AA batteries. Writing appliances were introduced in the 80’s including electric typewriters with single line LCD displays and single file memory which would allow you to compose and edit. I had such a device from Japan in high school that had a four line LCD display, built in thermoelectric (fax paper) printer, and battery life that went several days on 4 AA batteries.
By using computers and smartphones, which function as portable televisions and multi-function, shopping kiosks which use Watts of power, the trade off is battery life and constantly worrying about plugging in for a recharge. We forgot the days of battery life and are happy with 8 hours. The battery power bar is terribly distracting for me and I tend to stop working to find an outlet to recharge when it inevitably drops and when my productivity is nearly always highest. If I’m traveling, this means carrying the power brick, another injury to this one who remembers AA battery powered writing tools.
In 2017, the Samsung Galaxy Note 7 was famously recalled after spontaneously combusting and were banned from airplanes. All Lithium batteries must now be hand carried. Just recently, I was told while checking in that Apple Macbooks could not be turned on during flight because of heating issues. This is a consequence of the greatly increased energy densities of Lithium cells and their chemical volatility. AA batteries and their nickel metal hydride (NiMH) rechargeable variants suffer from no such problem.
Even with great battery life, you have to remember most of that power, and therefore bulk and weight of the Lithium batteries is devoted to painting vivid colors on the screen, communicating via radio signal to the world, and keeping dozens of apps updated on your activities, and not to writing.
The Lithium battery which can power a car because of its energy density is overkill if all you want is to write. The modern computer operating systems, Windows, MacOS, iOS, and Android, are all over-powered for the simple act of preserving words. Consider the lowly text file to a modern Word file. The text file for a novel might take kilobytes of memory, but the same Office Word file is measured in megabytes -thousands of times bigger. Try emailing a fully formatted Word file through your corporate firewalls if it exceeds your company’s limits on attachment file sizes. The size and complexity of information that is exchanged burns power. Compare that to the notes you might write onto paper. The few microcalories used to power your neurons and move pencil on paper, the motor and optics circuitry processing the information at a speed suitable for your ape brain.
My friend and early mentor, Professor David Tilson, refused to relinquish his DOS based word processor even well into the Windows era. And I understood. The monochrome and monotype letters forced you to look at the words and not the style of the words. While I admire Steve Jobs, and his introduction of fonts to our everyday lives, the ability to shape the look of your writing intrudes on its composition. Monochrome does not mean monotonous, and modern distraction-free software efforts like IA Writer embrace simplicity. The emergence of dark mode is another effort at rolling back the clock. When you enable it for your iPhone, it reaffirms the utility and critical need for focus and simplicity. Do you need millions of colors or just letters on a simple background? While you can change the color setting of your laptop screen or your writing software, the ultimate in monochrome experience is an e-ink display.
The e-ink display is what you see on Amazon Kindles. Originally meant for low power usage, high contrast functions like in store signs, e-Ink is currently used for e-Readers, although there is a niche market for e-ink based displays and tablets which do offer the low power hi contrast display perfect for a focused writing work station – you can find them on Amazon and eBay. Unfortunately, because these e-Ink tablets are run typically on Android, there is no escaping the internet on these, and because they do so, their battery lives are not that much different from standard tablets. What the we need is for Amazon to gift the writers of the world with Bluetooth or wired keyboard functionality to their Kindles and offer a text writer that can be synced to their cloud..
What the we need is for Amazon to gift the writers of the world with bluetooth or wired keyboard functionality to their Kindles and offer a text writer that can be synced to their cloud.
The constant need for connectivity drives software and hardware inefficiency. Writing requires intimacy and privacy. Just as you cannot write while engaged in a shouting match with someone, you cannot write with notifications of arriving messages, pictures, and videos. I cannot write while watching a movie or listening to certain music, but all of these distractions are baked into the function of modern computers and smartphones. This uses up battery life. The devices are in a race to maximize the battery and screen size at the cost of purpose and meaning aside from commerce.
Party line operators were a feature of the early telephone systems. Your locality was serviced by an operator that routed your calls and inevitably your conversations were open to intrusion both intentional and unintentional. When all your work is kept on a cloud server, it really is no different. And it isn’t that hackers that may take all your work. My generation grew up with the Cold War, and its dark tales of thought crimes and writers imprisoned for samizdat -ideas forbidden by a state entity. In a time when your social media is a subject for governmental and not just consumer interest, returning to off line options is something to consider seriously. The meaning of party line operators is in this context wholly changed.
The one feature of cloud based options is the convenience of accessing it across all of your devices. But are you really going to be writing on your iPhone, then on your desktop, then on your laptop, then from an airport kiosk? Your file can be lost during the sync process or changed to a competing version from another computer you were working on. And goodbye work if you get hacked or if your cloud service shuts you down or out. While you write, you have to keep a local version and back up to a nonvolatile storage option.
Not connecting to the internet saves you battery life. It also frees you from taking deep YouTube dives into funny cat videos or answering emails or Facebook posts. The stillness you need to just write is difficult to achieve with a modern laptop, tablet or smartphone. It can be attained with these older devices which people in the know still value decades after they left their boxes. I suggest these options if you are thinking of trying a focused writing appliance (a typewriter!).
Option 1: King Jim Pomera DM100 (link) is best described as a writing appliance designed in Japan adapted for the English speaking market. It is a sleek thin portable that allows one to type words unencumbered by internet. The files on it can be transferred to another computer by Bluetooth, and to smart phones by QR code which is cool. It runs for days on AA batteries, and has a backlit monochrome LCD screen. It is priced on th high end at 392.61, but receives the best rating on Amazon which to me is a 4.5. I never come across 5 star reviews that aren’t fake. One reviewers comment that the keyboard is cramped and takes getting used to. It can be used as a Bluetooth keyboard and stand for iOS devices.
Option 2: Neo 2 Alphasmart Word Processor with Full Size Keyboard,, Calculator
The Alphasmart Neo2 (link) was the last of a line of writing appliances put out by a pair of former Apple engineers who wanted to provide affordable word processing options on a full mechanical keyboard. The Neo2 is the most available and apparently the most usable, allowing one to type out hundreds of pages and transfer to a computer via USB connection. The screen is an LCD screen like on a calculator. The killer feature on this device is nearly forever battery life on AA cells. It has a rabid following of professional writers who appreciate the pared down experience for productive writing. It achieves that perfect 4.5 star rating. This is for a device discontinued in 2007 and sells for about 40-50USD in used condition. Reviewers rave about turning it on and instantly being able to type without bootup, and avoiding distraction by email, notifications, social media etc.
Option 3: Psion Series 5MX
The Psion Series 5MX represented the apex of portable computer design in the late 1990s. It was a computer made from the ground up from circuits, hardware, operating system, and apps by British engineers and it was a thing of beauty. Made in the late 1990’s, this device’s killer features, long battery life via AA cells, ultraportabiity, and lack of easy internet access puts it in a separate class. Not everyone like the keyboard, but I have long been able to type on it without difficulty with average to large sized hands. I had one during residency in the 1990’s and it followed me into fellowship. Before EHR, I composed full consultation notes and H&Ps on it and filed them on my password protected CF drive for later retrieval and update for frequent flyer patients. I picked up a pair of these for about 90USD from the Netherlands, but the going priced varies from about 70 to 200USD for a used one in good condition. New ones pop up but they go for nearly their original price -they are that good. I suspect I got a deal because they were Ericsson MC218, a Swedish licensed clone.
It has a compact flash drive, and with the save as text file function in the built-in word processor which works fast and reliably, it is possible to back up to a nonvolatile memory (the CF drive) and transfer to a regular computer. The one caveat is that the maximum size of CF drive it will see seems to be 128mB -that is megabytes which is hard to find. In certain older industrial machinery, instructions are uploaded via CF cards of these size, and so these cards are available on Amazon. Or look in a drawer for an old unused CF card.
I wrote this post on the Psion, and never once looked at emails, social media, or Youtube.
I wrote this post on the Psion, and never once looked at emails, social media, or Youtube.