
Steve Jobs is credited with popularizing the saying credited to Pablo Picasso, “good artists copy, great artists steal.” While its provenance may be apocryphal, it makes an excellent point about how we learn. Even in the lack of understanding, it is still possible to learn by copying. Toddlers do this. We, as land mammals, are hard wired to copy.
Take for example this patient below with Leriche syndrome with a triad of smoking, claudication, and impotence.

Because of his relative youth, being his 50’s, I felt the most appropriate procedure was an aortobifemoral bypass.

The only real complexity to manage was the severe stenosis he had in his left renal artery.

The options included
- renal endarterectomy as part of aortic thromboendarterectomy
- renal artery bypass from the aortic graft
- reimplantation of renal artery
- something else
Something Else: The complexity of renal revascularization creates risk. An antegrade endarterectomy of the renal artery would be done below a suprarenal clamp, adding to clamp time. A bypass would require the kidney to bide its time during the proximal aortic anastomosis, and the anastomosis for a jump graft, then the anastomosis to the left renal artery. This renal ischemia time can be extended by cooling the kidneys with cold (5 degree) LR, but why risk it? A renal endarterectomy can devolve into a visceral segment endarterectomy. After an hour, a nephrectomy.
That’s where this whole copying concept comes into play. Back in 2012, I worked with Dr. Jeanwan Kang, who had just come out of training with Dr. Richard Cambria. We were doing a type IV thoracoabdominal aortic aneurysm, and the right renal artery had a ostial stenosis. While I was figuring out the best way to manage this, Dr. Kang asked for a 6x18mm renal stent and an insufflator. She stuck the stent into the renal orifice and deployed the stent, opening the orifice. I had to find my jaw which had dropped to the floor.
Now, ten years on, that’s how I managed this patient’s ostial renal artery stenosis.
The patient’s thrombotic plaque went up to the renal origins and needed to be endarterectomized, but embarking on a renal endarterectomy adds potentially harmful renal ischemia time. Therefore, through the vertical aortotomy, I was able to get a clean end point to the aortic thromboendarterectomy and position a stent in the renal orifice and deploy it.
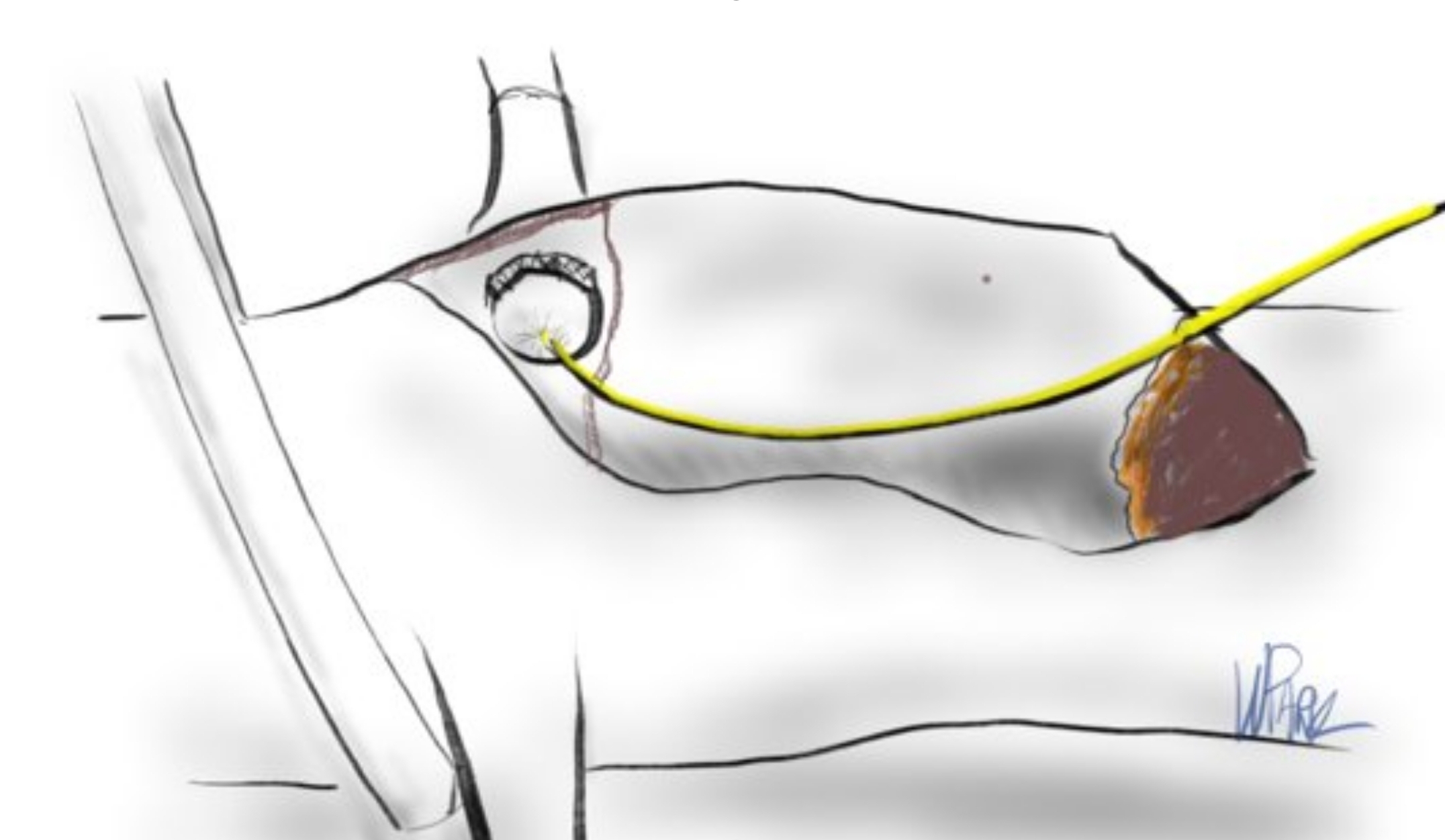
Once the stent was deployed, the aorta was partially closed primarily to allow the clamp to be moved below the renal arteries. This all took less than ten minutes of ischemia time. The aortic graft was then sewn end to side to the remaining aortotomy.
The patient recovered and was discharged on POD#6 with normal renal function. In followup, his CTA showed excellent graft and stent patency.

The centerline view of the renal stent shows it to be widely patent.

The patient is walking well without limitations and has improved blood pressure control, achieving normotensions at times.
If you are curious about the results from MGH, I refer you to their paper on 67 patients treated with open hybrid revascularization of the renal artery during complex aortic reconstructions (reference). At a mean followup of a year, they reported a 98% stent patency.
There is a comfort in sticking to what you know. The extreme example of this is the practitioner who graduates with a skill set from training and never expands on it. Yet there is an opportunity cost to blind devotion to sticking what you know and that is never growing. I recall this in the panel discussions during the VEITH Symposia I used to sneak into as a resident in the 90’s where great authorities pooh-poohed or condemned anything endovascular.
It’s a sign of a nimble mind that Dr. Cambria, after learning endovascular techniques mid-career, adapted these skills to his open surgical toolkit. His trainee, Dr. Kang, soon after, taught me.
Or was I just looking over her shoulders taking notes?
Reference:
Patel R, Conrad MF, Paruchuri V, Kwolek CJ, Cambria RP. Balloon expandable stents facilitate right renal artery reconstruction during complex open aortic aneurysm repair. J Vasc Surg. 2010 Feb;51(2):310-5. doi: 10.1016/j.jvs.2009.04.079. Epub 2009 Oct 22. PMID: 19853403.
