
The rise of cardiopulmonary bypass life support has also given a rise to the need to keep large, obstructive cannulas in femoral arteries. ECMO cannulas are often kept in for days, and it is not uncommon to discover limb ischemia and infarction relatively late. This can be avoided by placing a distal perfusion cannula to shunt blood to the leg early in the ECMO process. The ECMO cannulas have a convenient side port to send a little flow to a 6F sheath placed in the femoral or popliteal artery. This is an established technique (reference 1, sketch below), and it works despite the modest flows achieved because it does not take much to keep the leg alive. These patients are not walking, nor are they need to heal leg wounds, so just enough blood flow means something just a little more than what they get when the common femoral artery is completely occluded by the life support cannulas. What is fascinating to me is that these shunts can pptentially help to save limbs when used as temporary extracorporeal bypasses when definitive vascular surgical care is not immediately available.

When I was a medical student, I took on a research project after my first year where I had a Langendorff preparation of a rat heart (below).
My project was to take a rat heart and keep it alive, beating, and even working, through a perfusion apparatus and place this inside a superconductive magnet to obtain Phosphorus nuclear magnetic resonance spectra -intracellular metabolism data including concentration of ATP, intracellular pH, and ATP/ADP ratio. While the project was successful -I am quite proud to have been the only person at Columbia to have successfully acquired NMR-S data with living beating heart, I moved on to other interests and took away this concept: with oxygenated, glucose enriched, isoosmolar fluid perfused at arterial pressure, any organ can be kept alive, possibly indefinitely, including a brain which only recently others have found possible (reference 2) in reputable scientific circles, but the the Nature publishing Yalies were scooped by the Simpsons decades ago (below), and maybe Mary Shelley centuries before,

This is the simple idea. Revascularization is keeping the target vascular bed alive by delivering oxygenated blood. With a shunt, it could be little, it could be a lot, but it certainly is better than zero, and even a little can buy you time.
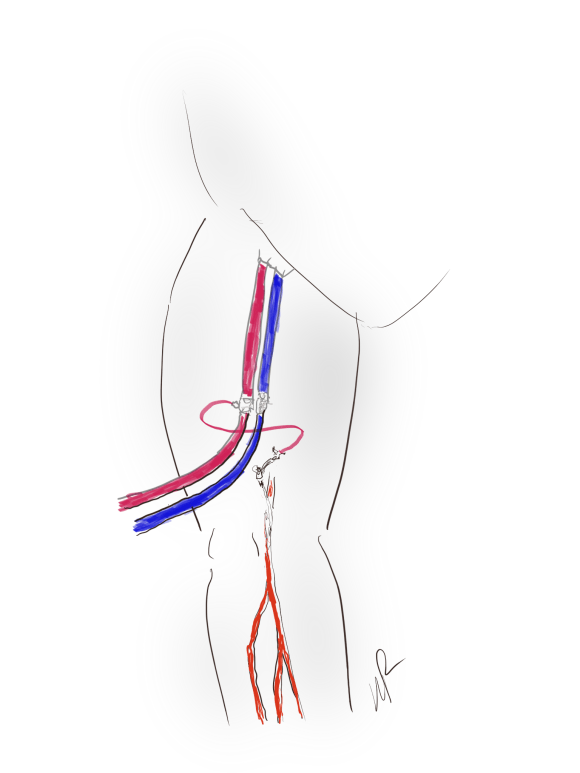
The breakthrough that I had was several years ago, a patient arrived from another hospital with an Impella pump which did not have a side port like an ECMO cannula. It is a large catheter that augments cardiac output and in the patient that I was asked to see this patient as their leg was cold and pulseless. Their cardiac output was very poor, and they were sustaining an augmented systolic pressure in the 90’s. There was no way to get this patient to the operating room for a revascularization of any sort. It did strike me that the patient had the misfortune of having catastrophic heart failure in the absence of significant athersclerosis and had normal brachial arteries. After discussing the ramifications with the ICU and family, I placed a brachial artery 5F cannula, and connected it to a 5F sheath I placed in the superficial femoral artery below the occlusive common femoral sheath (figure below). A doppler on the tubing connecting the two cannulas confirmed flow and the patient’s left hand maintained a pulsatile oximetry waveform. The leg pinked up and eventually there was a signal in the foot. This managed to perfuse the leg which did better than the patient who succumbed to multiorgan failure from heart failure. The leg did great.
Which leads me to these thoughts. Most hospitals are good at diagnosing large vessel occlusion via CTA. Most hospitals have doctors who can place arterial lines with ultrasound guidance. In the instance of aortoiliac occlusion or femoral occlusion from thromboemboliem, time is a critical limiting factor to limb salvage. Many hospitals do not have vascular surgeons. Many hospitals transfer these patients with a heparin drip but in the ischemic condition. Transfer arrangements may take hours. Why not ameliorate this situation by having an appropriate physician -an anesthesiologist, an intensivist, an EM physician, place an ultrasound guided radial or brachial arterial line, connect to arterial line tubing to a dorsalis pedis arterial line. Tape it all down on the patient after confirming flow (crude sketch below). This would be better than the three extra hours of ischemia the patient gets hit with on transfer. No one would transport a donor kidney without adequate perfusion and protection, but dying legs get transferred all the time with established warm ischemia. If done well, it might turn an emergency procedure into an urgent, semi-elective one. Have the vascular surgeon video conference in to confirm the absence of blood flow and appropriateness of temporary shunting.

If we are to live in a world with less vascular surgeons, then the radius of survival has to be extended with use of technology and simple ideas such as this. Comments are welcome.
Reference
1. Foltan M, Philipp A, Göbölös L, Holzamer A,
Schneckenpointner R, Lehle K, Kornilov I, Schmid C, Lunz D. Quantitative assessment of peripheral limb perfusion using a modified distal arterial cannula in venoarterial ECMO settings. Perfusion. 2019 Mar 13:267659118816934. doi: 10.1177/0267659118816934.
2. Vrselja, Z., Daniele, S. G., Silbereis, J., Talpo, F., Morozov, Y. M., Sousa, A. M. Mario, S., Mihovil, P., Navjot, K., Zhuan, Z. W., Liu, Z., Alkawadri, R., Sinusas, A. J., Latham, S.R., Waxman, S. G., & Sestan, N. (2019). Restoration of brain circulation and cellular functions hours post-mortem. Nature, 568(7752), 336–343.
