
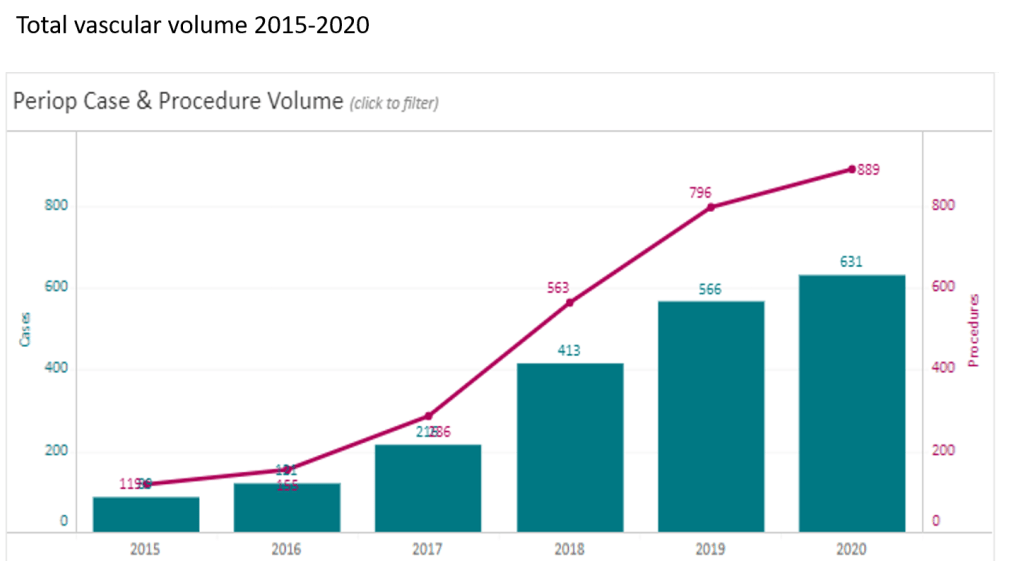
At CCAD, during my 4 years here as chief of vascular surgery, I had the privilege of working with excellent colleagues in a world class facility in an amazing and generous host nation. Over that time, our operative case volumes grew rapidly (figure below) as we proved our worth.
Our unique situation as both a main campus of Cleveland Clinic and a startup in 2015 with a fraction of the systems already in place at Cleveland made innovation a necessity. When making do became making great, we achieved the world class results as we were tasked to do. I count 5 off the top off my head in vascular, but there are many more that we do every day, contributed by all the team members. It is in the Cleveland Clinic’s DNA, from its origins century ago in the vasty fields of wartime France, this systemic mission to make things better. I think a lot of how our founders worked from necessity near the trenches in operating theaters within tents, sleeping on rough cots, thousands of miles from Cleveland. It is working in a startup hospital here, a stunning facility endowed by the Emirate of Abu Dhabi, that I realized that practical innovations were the lifeblood of hospitals in times past, and that it continues to have meaning when lives are saved. In a world where costs, not ideas, will, or skills, limit the availability of healthcare, cost innovation will play a large role in its salvation.
Innovation #1: Debranching Thoracoabdominal Aortic Aneurysm
The thoracoabdominal aortic aneurysm (TAAA) is the most challenging operation to do either with open or endovascular approaches because of the complications associated with the procedure including bleeding, kidney failure, spinal cord ischemia, and death. You really can only get good by doing a lot of these regularly, as it brings with it precious experience for the OR, ICU, rehab, and floor staff. The patients with TAAA presenting to CCAD do not always have the opportunity to travel to one of the acknowledged aortic centers (with which each of the faculty here have close ties), and we must offer results that match those other centers. To me, the biggest hassle and source of complication with an open TAAA repair is the drying up of bleeding at the end of the case, the result of long visceral clamp times. Long procedure time prolongs the case and exposes the patient to a more turbulent and prolonged recovery and higher risk.
Endovascular repair with branched or fenestrated stent grafts offers one solution in avoiding the thoracoabdominal exposure and long procedure times. Unfortunately, a significant minority of patients do not have the anatomy for endovascular approaches. We have the skills, staffing, and facilities to offer both approaches, but are handicapped by low volume. Review of our volumes show that aortic aneurysm disease is dwarfed by diabetic circulatory problems. So to offer these patients the same results with open aortic surgery as the patients I had at main campus in Cleveland, I had to cheat a bit by rearranging the deck. How so? By turning the highwire act of thoracoabdominal aortic aneurysm surgery and turning into a deliberate walk on a low balance beam. By debranching the visceral branches from the graft one by one, the visceral ischemia time is minimized (video) or largely eliminated.
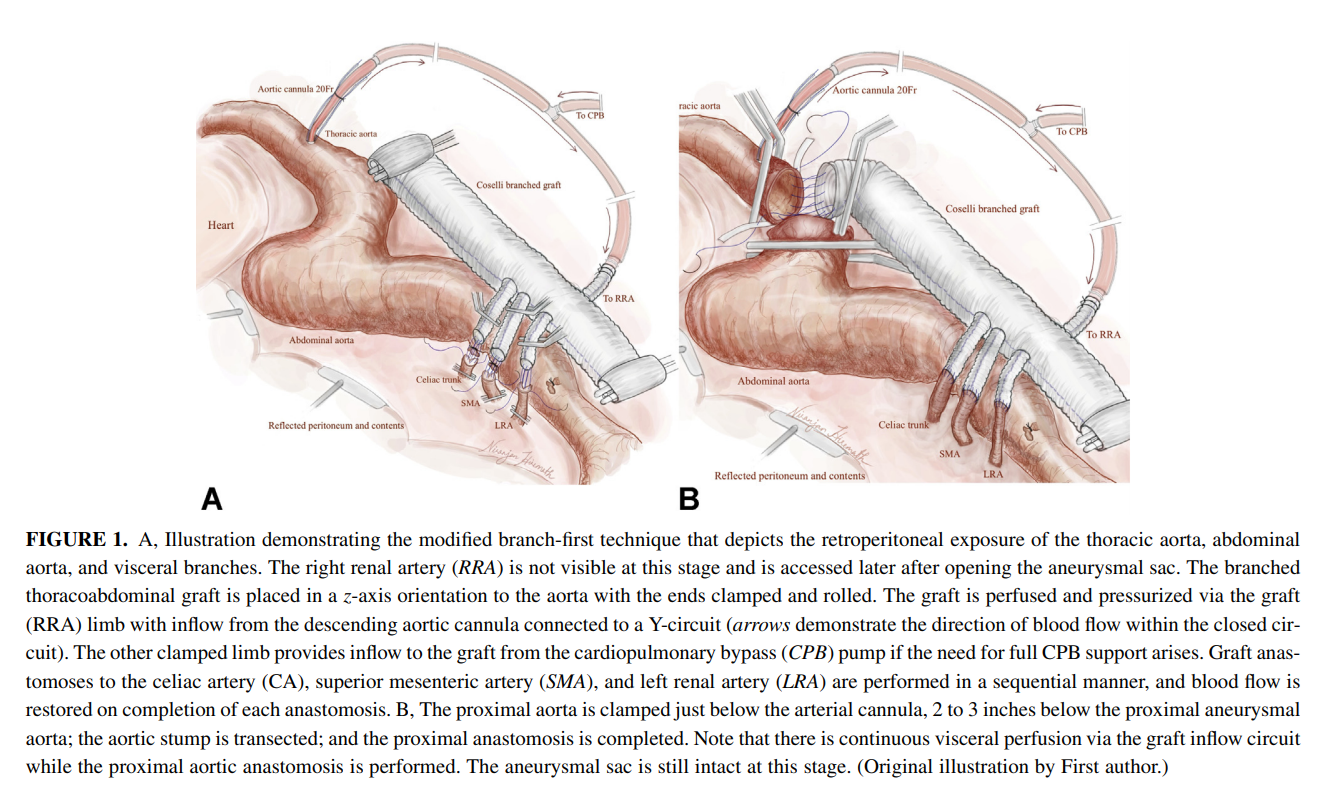
I discussed this with Dr. Niranjen Hiremath, our aortic trained clinical associate and like all things in medicine, a similar concept was applied by his mentor, Dr. Matalanis in Australia, to the aortic arch. We have performed two of these and both patients survived and are doing well, including the most recent one with a hybrid extant 2 repair. We published the technique after the first case in Journal of Thoracic and Cardiovascular Surgery (figure below, reference 1). I also presented the first case on this blog (link). More gratifying are the reports of adoption of this technique around the world. The patients come out of the operation without the torrent of coagulopathic bleeding seen with the traditional technique.
Innovation #2, The Vascular Lab in Every Patient’s Room
One of the things that happened early in my tenure was realizing how limited the tools available for vascular assessment were for non vascular caregivers. Both the physical examination with pulse palpation and pulse Doppler examination are challenging to master and usually fail to answer the simple question: is there enough perfusion? The absence of a pulse or Doppler signal in the hands of a non-vascular caregiver is an inconstant thing, and various projects have been undertaken that do not specifically address the triage gap that vascular surgery has compared to cardiology for chest pain. Not all chest pains are referred to cardiology. Only those those patients who pass the screening test of EKG and serum troponin levels are referred. My first inclination was to budget for pulse volume recording machines to be located in the ED and ICU’s of the hospital, but it was not a simple solution and would require stretching the limited vascular lab staff. Then it dawned on me that the toe waveforms offered a solution. On the PVR machines, the toe waveforms are captured by transmitting red laser light through the nail of the toe. A receptor captures a waveform (figure below) that is reflects the passage of blood that absorbs that red light.

This is in fact the identical technology in a pulse oximeter which has extra circuitry to calculate an oxygen saturation. I was not interested in the saturation, but rather the waveform. It turns out, for all practical purposes, the waveform given by pulse oximeter units is qualitatively the same as that given by the pulse volume recorder’s digital plethysmograph (figure below).
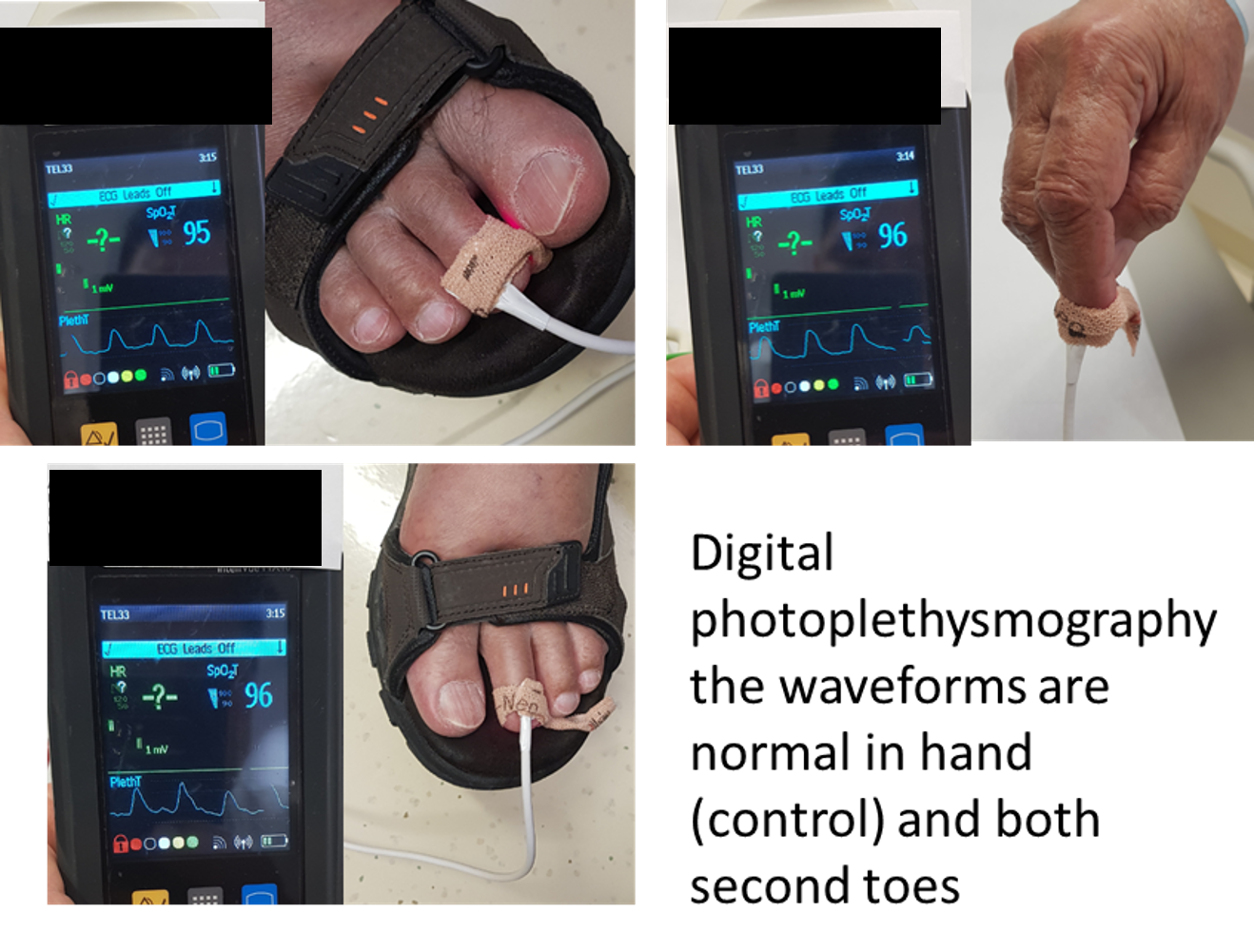
So now, when I get a phone call from the ED that a patient has no DP or PT pulse, I ask the caller to place a pulse oximeter with a waveform trace on the patient’s second toe (or nearest extant toe). I then ask, is there a waveform? The presence of a waveform, no matter how dampened, means the patient does not face acute ischemia, and can safely wait until the morning, avoiding a drive in the middle of the night (figure below, severely dampened waveforms).

We are validating this with a study that has completed data collection and hope to present this simple test to a broad audience. This is something akin to having a point of care vascular lab study that can answer a simple question: is there blood flow at the level of the toes? The finer points of “how much blood flow” can be answered by formal testing but that keen absence of broad vascular assessment skills among healthcare providers and absence of a simple test like an EKG for MI will feel less sharp, particularly because of the near universal availability of a pulse oximeter with waveform display throughout most hospitals.
Innovation #3: Assessing for Visceral Malperfusion before Surgery for Aortic Dissection
The typical scenario for a sad ending is this: a patient undergoes emergency surgery for an ascending aortic dissection. The operation ends in the middle of the night. The morning labs show a lactate of 10 which had been rising since the end of the operation from a high borderline level of 2. The urine output also dropped to zero. The patient remains intubated and has palpable femoral pulses, but now has a distended abdomen full of bowel gas, and is unable to report pain. The decision is made to get a CTA on top of the ones the patient received preoperatively which nearly guarantees permanent renal failure and need for hemodialysis. The descending aortic portion of the dissection is noted to be causing a malperfusion of the SMA and left renal artery, and there is pneumatosis of the small bowel through transverse colon which are resected after revascularization. The patient recovers with a jejunostopy and lifelong TPN and hemodialysis. This sad scenario is what I thought about when I was asked to assess a patient intraoperatively without a femoral pulses after an aortic dissection for possible visceral malperfusion. The question was if CT with contrast was indicated. Having an RVT credential (I’m old), I frequently do my own scans, and have found under general anesthesia, the abdomen is easy to scan well. The patient is typically prepped from neck to toes for the operation, so sliding in with an abdominal probe was simple. It is possible to get excellent windows on the visceral segment abdominal aorta with long axis and short axis views of the celiac axis, SMA, renal arteries, and iiac and lower extremity arteries (figure below).

At CCAD, the patients also get a TEE, and the arch and descending thoracic aorta is well visualized. That first patient underwent a femorofemoral bypass for the lower extremity malperfusion, and I found that the left renal artery had obstruction, but the right did not. The patient was reassessed at the end of the case and good visceral perfusion was seen at that point. I realized I was onto something, and whenever possible now for ascending aortic dissections, myself or the vascular tech is called to evaluate the visceral and lower extremity arteries at the beginning of the case, avoiding contrast studies. We are submitting the experience as an abstract for the STS conference.
Innovation #4: Retrograde tibial artery distal perfusion cannulas for ECMO
This past year, ECMO has been lifesaving for many patients facing cardiovascular collapse from COVID and other conditions. Once the cannulas go in, a hypoxic patient in heart failure has a chance at recovery. The drama of the moment causes the caregivers to overlook the fact that up to 10 percent of patients without a distal perfusion cannula will develop leg ischemia, and that after 6 hours, irreversible will occur leading in neuromuscular death and limb loss. This has happened for two patients transferred for care this year. The problem is that the skill of placing a antegrade femoral artery distal perfusion cannula in the proximal thigh is not always present, and the ability to judge perfusion is degraded with ECMO flow. While older patients on ECMO may have significant arterial disease, young patients generally do not, and I saw that as an opportunity for simplifying the distal perfusion cannula by placing a 5F micropuncture sheath into the dorsalis pedis artery (figure below).

This provided sufficient flow to avoid limb loss in a series of patients on which we published a technical article (reference 2) and presented. The retrograde access of these supericial vessels is within the technical envelope of most intensivists and cardiologists, those who most frequently place emergency ECMO cannulae. It was gratifying to catch up with one of my first patients who walked in with both legs, having undergone a heart transplant while bridged with ECMO.
Innovation #5: Park Clamp Used in Thoracoscopic and Laparoscopic Surgery

The Park Clamp (link) is a circular compressor that is intended to compress bleeding tissues allowing for suturing within the circle. I invented this while at main campus, and missing it sorely, had two custom made at the prototyping facility at Cleveland Clinic and shipped into CCAD. It is particularly useful in venous bleeding during spinal exposures, redo groins around the profunda, and retroperitoneal tumor resection. Dr. Redha Souilamas, chief of thoracic surgery (image above) found it particularly useful in thoracoscopic pneumonectomies, when staple line bleeding is encountered on the pulmonary artery (image below).

In laparoscopic surgery, it is possible to introduce the compressor via a small incision and this will allow for laparoscopic suturing of a vascular injury in a bloodless field. I was able to resect an IVC tumor thrombus with Dr. Waleed Hassen using this device to achieve hemostasis. The critical feature of the Park Clamp, lacking a manufacturer, is that we made it ourselves in our own hospital.
Conclusion: a modest proposal or how cost innovation will save health care
Inventions and innovations exist in a vacuum unless they are implemented, and this requires the will to accept the possibility of a better way. You should never be satisfied with the status quo if there is harm to be reduced. There has to be buy in from everyone involved or you get the situation I had when I was a PGY-2 in 1995 in the ICU. Being the surgical ICU resident, I was called nearly hourly to change the dressing on a patient with HIV and necrotizing pancreatitis with an open abdomen. There was over a liter an hour of exudate soaking the dressings and pads, making it a nightmare for the nurses. After a third round of this and feeling it would interrupt lunch, I came upon a plan for covering the wound with lap pads, overlaying a chest tube, and sealing everything with an Ioban. With the chest tube to negative pressure via a Pleuravac, the calls to change the patient’s dressing ceased, and the nurses no longer hand to change the bedding hourly -bedding that was soaked with HIV positive exudate. I was very pleased about this until I was stat called to the director’s office. I was given the dressing down of my life -how dare I experiment on his patient and didn’t I think that placing a suction on the transverse colon would result in a fistula? I hung my head in shame and took down the dressing. Of course, readers will know that this preceded the VAC dressing by about a decade, and negative pressure wound therapy is now a multi-billion dollar industry. What it teaches me to this day is that progress only happens when success is actually seen by everyone, but also there has to be buy-in from the stakeholders -the people who bear responsibility for any bad outcomes -fistula and death in the case of this proto-VAC dressing. Without convincing everyone, there is no success, and the invention goes off to die.
The fact is, one time early in my tenure here at CCAD, we ran out of negative pressure pumps, and I placed this chest tube/Pleurevac dressing on a patient with a large groin wound that was leaking high volumes of exudate and lymph. After two days, when a VAC pump became available, the patient’s groin turned out to be clean and granulating and it came to me that the next great leap in innovation is low cost innovation.
Cost Innovation, to name it, is using what is available, sometimes repurposing, or at others, dialing back the clock, to replace costly things that threaten to break a hospital’s finances while maintaining quality. It was only a few generations ago when hospitals were self contained communities. Rather than use peel packs of disposable gowns and drapes, there were tailors, seamstresses, and launderers making and maintaining the same. The Mayo Clinic was making its own insulin after discovering it and gave away the recipe out of concern for ethics -out of believing it is wrong to profit from a life threatening condition. We have the technology and capacity to make low cost endoscopes and reprocess them -possibly undercutting current costs by a factor of a thousand. We slaughter millions of hogs and cows annually, but harvest no heparin from them in the US. Laser CNC cutters, 3D printers, and enthusiastic makers have proliferated and could make every item that we currently open from a peel pack, use once, and discard into landfills -one only has to look at the cottage industry of face shields and hand sanitizers that bloomed last year during the pandemic. Pharmacists are fully capable and trained to manufacture custom pills and compound salves and solutions by the gallons if only if they are allowed to, saving hospitals millions in cost of medications sold in blister packs and tiny tubes and bottles. Stents can be printed in-house, and stent grafts can be custom made (link). Every town or city has tradespeople who can work stainless steel, plastic, and glass, or make and program custom computers -it is a short jump to making medical equipment at scale in your hospital.
Cost innovation is the only way out for the inflationary cost cycle that has throttled healthcare throughout the world. We have become a world where healthcare is delivered out of peel packs and million dollar investments to perform single procedures is considered normal and desirable, almost to the point of thinking people as coming in disposable peel packs. When I watch shows about hospitals a century ago, such as The Knick, I don’t guffaw at the old-timey medical stuff. I see a fervent environment of innovation in purposeful communities of specialized workers within hospital walls. We need to return to such practicality if we are to break out of the plastic peel pack.
References
- Hiremath N, Younes H, Aleinati T, Park WM. Open repair of extent-III thoracoabdominal aortic aneurysm using a modified branch-first technique. JTCVS Tech. 2021 Mar 13;7:29-31. doi: 10.1016/j.xjtc.2021.03.014. PMID: 34318197; PMCID: PMC8312144.
- Göbölös L, Hogan M, Kakar V, Raposo N, Sänger S, Bhatnagar G, Park WM. Alternative option for limb reperfusion cannula placement for percutaneous femoral veno-arterial ECMO. Perfusion. 2021 Mar 26:2676591211003282. doi: 10.1177/02676591211003282. Epub ahead of print. PMID: 33765883.
