Mid Century Modern is a design philosophy from the mid twentieth century that seemed terribly dated and out of style while I was growing up but now seems to have come back as people dig around their parents and grandparents’ stuff. Television shows like Mad Men and Marvelous Mrs. Maisel are rotten with mid-century design. Yet it is an apt term for vascular surgeons of a certain generation like me who at about fifty years of age remember a time when vascular surgery was about big incisions and bypass grafts. We were trained in open vascular surgery and rode along with (or were drowned by) the tsunami of endovascular techniques that have come to dominate. Most of us learned to do them as well. Mid-century vascular surgeons straddle the divide between our mentors who, like me, specialized in vascular after completing general surgery training and the current trainees who have trained solely in vascular surgery. At one time it was fashionable to believe that we were fossils. But, like the coelacanth discovered after an eon’s absence, guidelines and recommendations are being made for open surgery which is supposed to be making a comeback. But it turns out, open surgery-capable vascular surgeons are, like the coelacanth, rare, and endangered. Unless we completely change the way we train people today, open vascular surgery will become extinct. At first glance, it does not look good.
The Dinosaur
My first ever encounter with a vascular surgeon was in 1989, as a lab tech in Boston the year after I graduated from college. It was at the West Roxbury VA Hospital, and like the vets, this one chain smoked in his office. Friendly enough, but a bit aloof, he rasped out well elocuted English in the same way soldiers did in old war movies like The Longest Day. Laconic and Robert Mitchum-like. He would have been among the first generations of vascular surgeons, contemporary to Jack Wylie, Michael DeBakey, and other luminaries. He couldn’t have cared less, I believe, as he performed fem-pop and aortobi-iliac and femoral bypasses and carotid endarterectomies with a furious incandescence that didn’t jibe with his reserved demeanor outside the OR. He was equally fierce to the residents when he had to scrub in to get them out of jam. But he was kind to the medical students and pre-meds like me. His type of surgeon is most definitely extinct, remembered only in old war stories like this.
What is it about my generation of surgeons? We remember things and balance the new against the old ways. We remember a time before work hours restrictions but are young enough to understand why it is not too healthy to work 120 hours a week. Yet we are also conflicted about the benefits we retained from that kind of training, now viewed with about as much approval as Sparta’s agoge system of child abuse and military training. I trained at the outset of laparoscopic surgery, so I did about 50 open cholecystectomies before learning how to do laparoscopic cholecystectomies. Most of my appendectomies were done open. As were my colectomies, gastrectomies, thyroidectomies, mastectomies, and yes, aortic surgeries, carotid endarterectomies, arteriovenous fistulae, and leg bypasses. And I did them.
We All Agreed…
This was the deal. You worked at 110%, fell exhausted and gave a little more, and you were rewarded. That meant being up all night on call, but after morning rounds, you could turn your pager off and operate all day. If you were learning, you had to be prepared by knowing the patient, the disease, the anatomy, and the operation. If you were teaching, you had to have the approval of the attending who would be somewhere nearby, and never happy if you grabbed them. If you were chief resident, you were basically junior staff and expected to run your service like a practice. The leash was longer for those who could, and short for those who could not. In the grade before mine, it was pyramidal, meaning there was attrition of those who could not progress. Like ringing the bell at Navy SEAL school in Coronado, people quit. Or were, rarely, fired. Being categorical was seen as a kind of entitlement by the disbelieving chiefs welcoming the new categorical interns. Dishonesty was the worst sin, but weakness, like showing fatigue or expressing a desire to have a life outside of work, was equally bad. And training was long. Four years of medical school, followed by five years of general surgery residency with mine extended by a year of research between third and fourth year, and then followed by a two-year vascular fellowship. By the time I was a full-fledged vascular surgeon, I had college friends who had actual homes and summer homes, children, divorces, and travels around the world. They had lived real adult lives. I started out on life at 35 where everyone else had done it at 21. But I had 1600 cases in my residency, of which over 300 were major vascular including 50 open aortic cases, and nearly 500 cases during my fellowship, adding another 100 aortic cases, most of them open, as it was the first years that EVAR was introduced. Nothing better in the world than to start a case with Ken Cherry quipping over your shoulder -“make me proud.” I finished my endovascular training apprenticed to Dan Clair during my first staff job at Columbia P&S -cue Dan intoning “you’re killing me” over the Cath Lab’s PA from the control desk on the weekends we had time in there.
There is no going back…
That represented one way of training a vascular surgeon. Even after graduating, I never stopped learning and perfecting my craft. The two years at Columbia gave me insight on how to run a practice completely alone -I was the lone vascular surgeon up at the Allen Pavilion on the northern tip of Manhattan next to Baker’s Field. It taught me the critical importance of availability and extracting useful information over my tiny flip phone. During my private practice years in Iowa, I learned the amazing productivity that can be attained when you work in collaboration and partnership with cardiologists and cardiac surgeons -something I do today here in the Heart and Vascular Institute. I also learned how to use vascular technologists and the lab as a force multiplier. And it was during the Iowa years that I underwent a period of endo-enthusiasm followed by a realism and I performed over a hundred aorto-bifemoral bypasses on middle aged patients with an average length of stay of 3 days, no deaths. When I plunged back into academia, taking a position at Cleveland Clinic, I was apprenticed again to Dan, but this time in understanding how to use the whole clinic as a tool for taking impossibly challenging patients through to an acceptable resolution. All of that started with those frantic days on call as an intern at St. Luke’s Hospital, drawing blood cultures, placing IV’s, babysitting traumas in the CT scanner, and putting chest tubes into the perforated. But there is no going back. It is most definitely probably illegal today to subject people to the intensity and duration of experience that I went through. And I wouldn’t trade that experience for all the treasure in the world (although I do regret not buying Apple, Dell, and Microsoft in 1994).
What a completely trained vascular surgeon can do
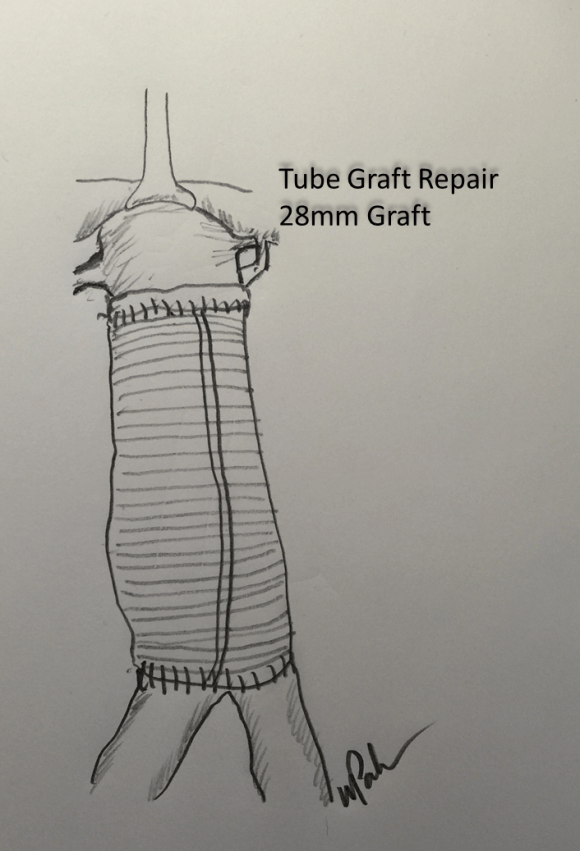
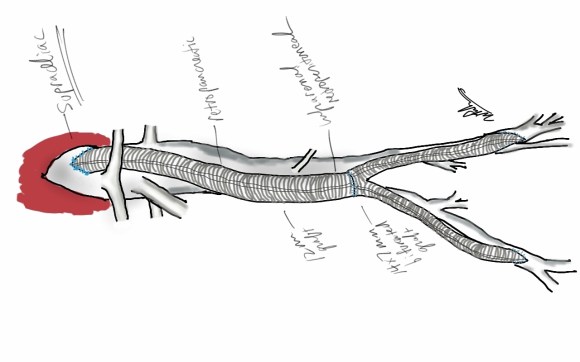
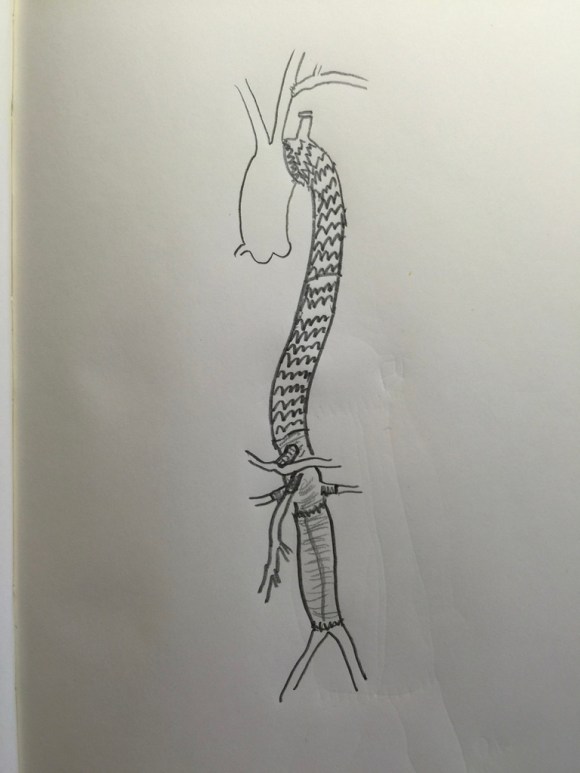
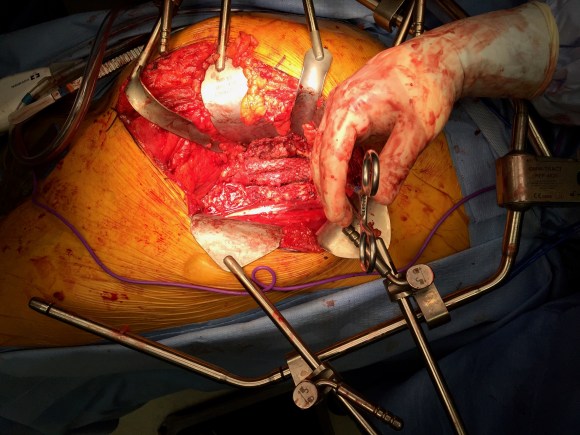
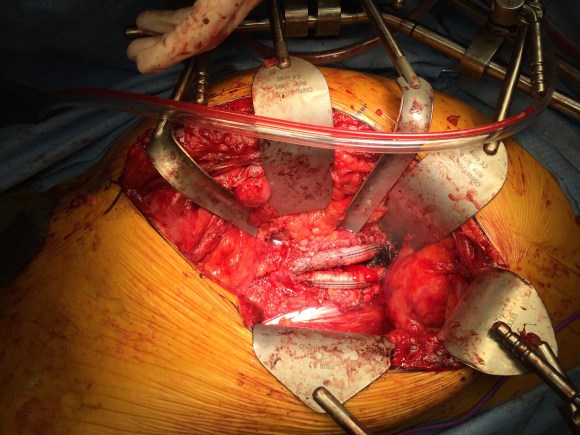
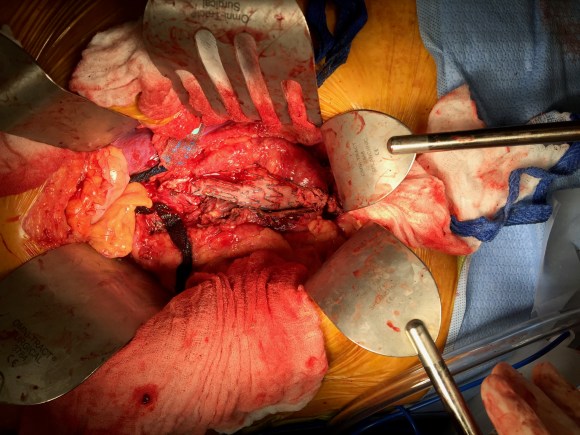
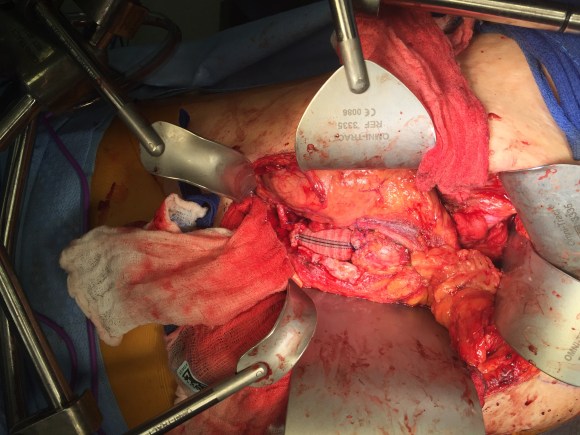
The hardest case that I have taken care of ever was at the Clinic a couple of years ago. The patient was a middle aged man who had ruptured an aortic aneurysm in another state some months prior and had undergone a repair complicated by a pancreatic injury along with some enterotomies resulting in a graft infection along with high output pancreatic and enteric fistulae from an open abdomen. He arrived cachectic, in septic shock and had a pseudoaneurysm from the distal anastomosis of a short tube graft. I immediately took him to the OR to place a stent graft across the pseudoaneurysm neck to prevent rupture and placed him on TPN to correct his cachexia. The abscesses and hematomata were drained percutaneously, and an effort was made to control the fistula with a heroic effort on the part of the ostomy team. He turned around and was able go to an LTAC on TPN and antibiotics. There he gained twenty pounds and returned flush and active. Stage two was three months later and done to replace the still infected grafts with cryopreserved homograft. I did this via a right retroperitoneal approach as the left side and abdomen were a mess from the inflammation. After I removed the grafts and sewed in the homograft, general surgery reorganized his bowel and discovered that he only had about 30cm of useable small bowel and would be on TPN for life. But he was alive and learning to walk again, and eventually came back 6 months later for follow-up and gave me a hug.
That case took all of my skill to solve, and I could not have done it without the whole hospital working in sync with me. When it comes my time, I wonder who would be able to do that for me?Who would manage my ruptured AAA properly and not have bowel and pancreatic injuries?
How to do a CABG according to Dr. Swistel
When I was an intern, I wanted to be a cardiac surgeon more than anything else, and got myself slotted for 6 months of cardiac during my second year. It was an unwanted rotation because of the 5am to 11pm hours, all nighters in the unit on call, and because the CT surgeons were notorious for not letting you do anything, except for Dan Swistel. Years before he had been one of us, a resident at St. Luke’s/Roosevelt and was Dr. George Green’s protege. He had a deal with us where he had you learn and master all the following steps in this order:
1. take vein
2. put in pacing wires and chest tubes
3. close chest
4. open chest
5. open the pericardium and set up the way he wanted
6. put the venous cannulas in
7. put the arterial cannulas and secondary lines in and go on bypass
8. decannulate and repair
9. dissect the aorta, set up and place the cross clamp
10. do the proximal anastomosis on the vein grafts
11. do the distal anastomosis on the vein grafts under the microscope which was the way he and Dr. Green did it.
12. dry up…really dry up and learn to come off pump
13. take mammary
14. book a ward service CABG and do it skin to skin
Through the history of St. Luke’s up to that point, most residents never got past taking vein. That was the great barrier, and most people really didn’t stick around after taking vein and closing the leg. They did not see the point of standing around and second or third assist. Those residents who were going to Cardiac did make it to taking the mammary, but only a handful by chief year. No one made it to 14. Dr. Swistel was always true to his word, even though some residents suspected this was all some bet that he had between himself and his brother who was not a cardiac surgeon -something about I can train a monkey to do this. To me, that last step, doing a CABG skin to skin, seemed like the final level of a very difficult computer game, like casting the One Ring into the volcano, like blowing up Agent Smith.
Every step on the ladder was something I immediately applied to my general surgery experience. On call and at home, I practiced. I practiced holding the instruments correctly and performing anastomoses on discarded grafts. I learned that every hard operation is made up of small technically feasible components, so I worked to make those moves natural and smooth. I progressed rapidly up the ladder and was by the end of my last cardiac rotation firmly at 13 on more than one occasion. Every other part of my skill set expanded during this time -central lines went smoothly, appendices and gall bladders were fished out efficiently, and fear shifted its focus to different things from what made me anxious as an intern. I learned the skill of keeping people alive through the night and making the call to take people back.
With some social engineering (ordering the cardiology fellows takeout Chinese) and vacation days traded, I got to that last step during my third year. If not a monkey, then at least Park. The act of learning and mastering each component skill lets you start and finish an operation. I don’t think Dr. Swistel was ever out to lunch while I was operating, but all those moments of letting me take the knife was crucial to my education and I am grateful to him and all my teachers, including my current partners and colleagues, as I approach PGY-25. As surgical educators, we must recognize that surgery at the sharp end of the knife is a precision craft that has to be taught much as tennis is taught starting with grip, stance, swing. That golf is learned on a driving range with a bucket of balls.
The Mid-Century Vascular Surgeon
Like Mid-Century Modern Design furniture, surgeons in my cohort are sought after by hospitals and practices for being able to let a hospital do more. What do I mean? A urologist resecting a kidney with a renal vein tumor thrombus extending into the inferior vena cava needs to have someone expose, extract, and repair the vena cava. A gynecologist debulking retroperitoneal metastases needs to be able to call for help when part of the aorta needs to go with the tumor. Cardiac surgeons need to be able to place ECMO cannulas in imaginative locations and not lose extremities in the process. A thoracic surgeon resecting a Pancoast tumor needs a vascular surgeon to repair the subclavian artery and vein. An orthopedic surgeon resecting a spindle cell tumor from the thigh needs help reconstructing the femoral artery and vein. And so on. We are safety net, the fire brigade, the SEAL team, and unfortunately many hospitals understand only when their last fully trained, full service vascular surgeon retires.
Vascular surgeons are a keystone species in a hospital’s ecosystem. When wolves were reintroduced to Yellowstone, it was noticed that decades later the forests returned to their ancient glory, that wetlands flourished breeding fish and insects and small mammal species, and the secondary predators that feed on them, and many missing bird species returned. Vascular surgeons capable of operating on the whole body as well as intervening on the whole body are increasingly a missing element in a hospital. And many of us chose to go missing -into our private endovascular suites and vein centers because it often does not pay to go do a 5-hour bypass when you can do three femoral angioplasties for claudication in the same time. Reading 10 carotid ultrasounds is easier on the back and more renumerative than a carotid endarterectomy. And I am not judging -it is a rational choice that is framed by the way healthcare is reimbursed.
The solution starts in the US with a shift in reimbursement to recognize the time and effort required to perform open vascular surgery well and to reward the programs and surgeons who are consistently good. Training in open vascular surgery will be sought after much as everyone wanted to be a cardiac surgeon back in the 1970’s. Government and society mandates set the menu, but the economics determine what is served.
And finally, every year thousands of surgeon-years of experience is retiring with the very skills that are now sought after. Rather than lose this human capital to golf courses and beaches, we should be grabbing them at the door. Like those mid-century chairs and tables, we have always been there somewhere, and its time to make some more.
















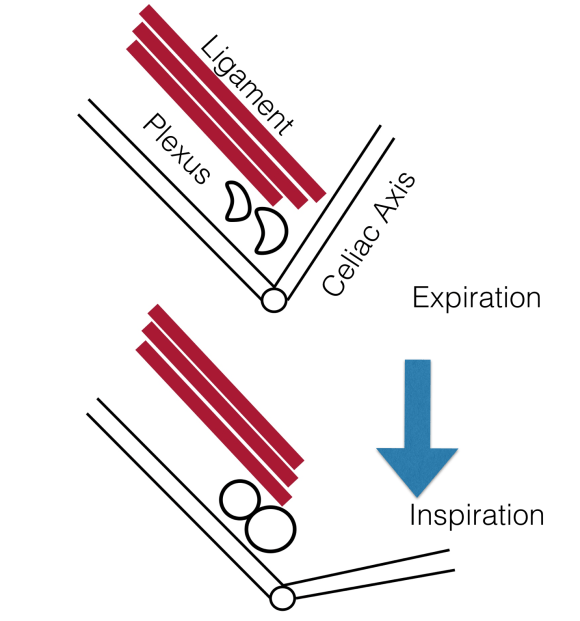 The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed.
The celiac plexus is caught under the median arcuate ligament and compressed. It causes a neuropathy that is felt in its visceral sensory distribution and the brain interprets these signals in the typical ways irritation of the stomach is interpreted -as pain, burning, nausea, sensations of bloating, and general malaise. These nerves can be turned off with a celiac plexus block and the effects tested by giving the patient a sandwich. When it works, the patient will say they will have had relief for the first time in years and operation to relieve the ligament compression and ablate the nerve can proceed. Same for many of the diseases listed. The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).
The swelling from varicoceles which I have also had feel nothing less than feeling the aftereffects of getting a kick in the balls -not the immediate sharp pain but imagine about 5 minutes after with the mild nausea, abdominal discomfort and desire not to move too much, and even a little flank pain. Imagine this occurring low in the pelvis with ovarian vein varices in pelvic congestion syndrome. This kind of swollen gonad pain afflicts many women whose pain is so frequently dismissed by male physicians because they have no context -well imagine getting kicked in the balls hard, wait about 5 minutes and that moment stretch it out to whenever you stand for a long period of time (below).