

Innovating Our Way Out of Not Having Enough Vascular Surgeons
This year’s SVS meeting featured a sobering assessment about the vascular manpower deficit affecting North America at the E. Stanley Crawford Critical Issues Forum, moderated by Dr. Michel Makaroun, MD, president-elect of the SVS. 35-45% of practicing vascular surgeons plan on retiring in the next decade by conservative estimates. We are not attracting enough candidates for the training programs. The solutions, including decreasing the length of training, public relations campaigns, and incentivizing retention have had mixed results, but we have yet to see a sustainable rise in vascular surgeon numbers.
Burnout driven by lack of work-life balance, the advent of electronic medical records optimized for billing, the passing of the private practice era, and the constant need to adapt to new techniques, create a persistent downdraft on staffing. So as some hospital face the reality of having to contract services, little attention is given to delivering best care with the staffing that we have. Changing how we practice is the only viable solution.
There are an estimated 3000 active vascular surgeons in the US. Imagine if all the cheese needs of this country could only be met by 3000 artisanal cheesemakers who make cheeses one at a time and want to live in places with international airports, BMW dealerships, and major league sports teams, and must have 3-4 partners to share cheese call. If you are a rural hospital in dire need of vascular surgery services and your one vascular surgeon is retiring, you are probably SOL.
When I was training, vascular surgery was oft touted as a primary care specialty. And that is how many of us still practice, managing risk factors, monitoring mild disease, as well as planning and performing interventions and operations. As much as I enjoy that kind of interaction, the half hour to an hour visit for a head to toe cardiovascular survey and discussion, educating patients and families about pipes and pumps, is incredibly inefficient. A healthcare system, a hospital, facing a staffing shortfall, has to do everything possible keep that vascular surgeon in the OR during work hours.
What is the core function of a vascular surgeon? Making good decisions and executing plans well. Decisions require data. What is this data? We laud the history and physical examination, but this is a throwback to another era. If you look at the diagnosis of myocardial infarction, it is not standard practice for a cardiologist to come and get a history, examine the patient, and declare that the patient is having a heart attack based solely on history and physical examination. It is a triage nurse in the ED who draws labs and orders an EKG which is read by a machine. These data points will tell you if heart muscle is being damaged. A process is started which triggers a team to come and take care of this patient. The hospitals focused on this actually drill their cath lab teams like pit crews. A stopwatch starts with the goal of revascularization under an hour.
Not so with peripheral vascular disease. The ischemic foot might have only a few hours depending on its presentation before it is irretrievably lost, but no matter -they sit in the ED until a vascular surgeon comes to speak to the patient and family, examine them, and then order tests, admission, consults, and operating room -typically all by themselves. Getting these patients into the operating room is in many places hampered by the lack of dedicated OR staffing, radiology techs, anesthesiologists, space, equipment, and critical care capacity. During work hours, there are scheduled cases that have to be delayed or canceled for another time, which takes time to do. After hours, the patient may have too many comorbidities to handle safely with the available staff. The vascular surgeon may have to bargain and cajole, to align several factions whose attention is demanded by many equally important concerns. If you decide to hold a lavish dinner party of twenty important guests -reserving space, calling caterers, inviting guests, arranging transportation – on short notice, you might pull it off once, but if you do this regularly, you are a masochist of the first order.
In the heart attack model, the history and physical examination is relegated to a series of yes/no or how long questions, and positive responses trigger a series of coordinated actions of a system -a reflex. In the leg attack model, there is no such system. I have to blame the vascular surgeons for preserving the current model. Vascular surgeons are organized as a guild. Guilds are protective of their monopolies on skills and markets and fiercely resist change. Most vascular surgeons are terrified by loss of control, and cling to the notion of being misunderstood and unappreciated saviors. We can do better.
The area that needs streamlining is at the point of referral. The majority of time of a vascular surgeon is spent working up normal blood vessels, varicose and spider veins, leg edema and pain, and mild and moderate arterial atherosclerosis. This work initially does not require a vascular surgeon but rather a focused set of policies and initial diagnostic studies that can be administered or ordered by any caregiver. Reducing the need for vascular surgeons at this point in vascular care will go a long way in extending the vascular work force at hand.
Point of Care Blood Flow Evaluation
Finding and declaring blood vessels to be normal is challenging and too often time consuming. Streamlining this will go a long way in freeing vascular surgeons to take care of disease.
The average caregiver is an inconsistent pulse taker. The palpable pulses are not always easy to find. Asking over the phone or as policy for someone to examine pedal pulses -the posterior tibial artery and dorsalis pedis artery pulses, is challenging. A positive is just as likely to be true or false as a negative. No cardiologist would ask a similarly detailed and technical question about an MI. In fact, they can’t ask, “Is there a pulse in the LAD?” Cardiologists make do with tests easy to obtain and interpret with certainty -the plasma troponin level and the EKG. The EKG is read by an algorithm so established and so tested, that it should stand as an example of early machine intelligence taking over a human job -but I digress.
What is our EKG? It is not the ABI -the ankle brachial index, because it is terrible at identifying disease, and is difficult to obtain reliably without practice. The closest thing to an EKG we have in terms of simplicity and accuracy is the pulse volume recording, the PVR (figure below). A FloLab machine, the machine used to obtain PVRs, will basically run itself once the cuffs are correctly applied on the leg, and the tracings are very easy to interpret. Unlike an EKG, there are no electrodes whose locations you must memorize. If the closest vascular surgeon is an hour away by ambulance, the transfer of a patient with flat waveforms and ischemic foot does not require a consultation on site. The patient would go to the vascular surgeon with no time wasted and no kidneys injured by CTA’s that too often fail to travel with the patient. Unlike an EKG which can be performed by many caregivers, a PVR requires both the equipment and a vascular technologist. A vascular technologist is not available 24-7 in most hospitals, and FloLab machines purchased for vascular labs are not meant to be dragged around the hospital.

So let’s think out of the box about another box in every triage nurse’s cell, every ER and ICU bed, and on every hospital nursing floor. These are pulse oximeters with a digital tracing, and bonus points, some come with strip printers! Placing a pulse oximeter probe on the second toe and comparing to an erstwhile normal wave signal such as on an index finger can provide qualitative information about normality and disease. Normal waveforms and abnormal ones can be easily discerned. A flat line is another obvious finding when in comparison, a finger or an ear on the same patient has normal signals.
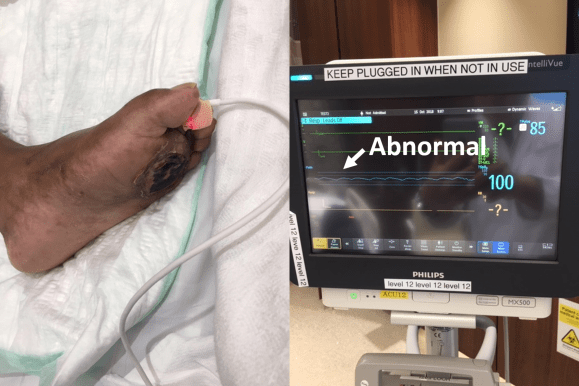

How much better would a vascular surgeon feel about a transfer call that has this information, “digital waveforms are flat in this patient with rest pain and a bruised toe.” How much better would a vascular surgeon feel about a call about a patient with “digital wave forms are normal in this patient with toe pain and a bruised toe. We got an x-ray and there was a fracture.” The communication can be quite detailed and refined. For example: “The patient had no pulses, we think. Digital wave forms were dampened but pulsatile in a patient with a bruised toe, we’ll send to vascular clinic in the morning.”
A study comparing pulse oximetry signals and ABI in type 2 Diabetes Mellitus found the following results (link).[i]
| Method | Sensitivity | Specificity | PPV | NPV |
| Pulse oximetry | 74.1% | 95.7% | 83.3% | 92.7% |
| ABI | 70.3% | 87.1% | 61.3% | 91.0% |
These data suggests pulse oximetry signal is equal to and somewhat better than ABI. Why is this important? Cost. This information is better than asking unsure people, “Is there a pulse?” A vascular technologist need not be on call 24/7. Extra FloLabs for ED, ICU, and floors need not be purchased. The pulse oximeter with waveform tracing is nearly ubiquitous wherever patient’s oxygenation needs to be assessed in most hospitals. While not perfect, it has great potential for serving as vascular surgery’s EKG machine for critical limb ischemia. Policies and algorithms can be built out in collaboration with Emergency Departments and nursing departments that can effectively determine if blood flow is normal or abnormal at point of care. Effective emergency responses to critical limb ischemia can be authored triggered by abnormal findings. Acute limb ischemia protocols based on time sensitive responses can be initiated. All of these can flow from referring entities being able to determine objectively normal or abnormal blood flow.
Clinic
The vascular clinic is a sorting process where patients are determined to be normal or have mild, moderate, or severe disease. The vast majority of the time spent in clinic can be spent in triage by trained nurses and testing by technologists. Clear pathways and guidelines can dictate the ordering of vascular laboratory tests obviating the need for vascular consultation at this stage. Patients with normal blood vessels and vascular function are sent back to their physicians with the normal report. Patients with mild disease and moderate disease are sent to a physician with specialization in cardiovascular medicine for management of risk factors and periodic surveillance. At any point in the process, a vascular surgeon can be called to provide guidance and direct patients to different tests and consultations. The patients needing operations, based on correct indications and imaging are sent to a focused clinic where the surgeon and interventional team can review films, determine the urgency of indications balanced against risk, and plan and schedule procedures. Currently, vascular surgeons do all of this by themselves, as well as make hospital rounds, perform procedures, and interpret vascular laboratory studies, seeing one patient at a time.
In introductory computer sciences courses, search algorithms are taught to be brute force if you look at one item at a time for the thing you want, and to be efficient if you have presorted those items because every time you look, you can exclude part of the data set, ever shrinking the pool in which you search, making the search shorter and faster
The shortfalls in vascular surgeon numbers have as much to do with this dependence on the star chef cooking up one meal at a time, rather than a team working off recipes, with the chef directing the flow and occasionally jumping by the fire to make the most difficult of dishes. The first restaurant can seat three parties. The latter, easily ten times the number. Everyone gets fed.
Only asking how many vascular surgeons you need misses the big picture because there are many equally important questions. How many vascular technologists do you need? An accredited laboratory provides the critical diagnostics upon which decisions are made, and the surgeon should oversee but not be directly involved in the initial screening. Nurses trained to triage and order vascular laboratory tests and even perform the simpler ones is the second need. Third, is the cardiovascular medicine physician who manages those patients discovered to have mild to moderate disease, and depending on symptoms, refers severely symptomatic moderate disease and severe disease to a scheduling clinic. The scheduling clinic is composed of both interventionalists and vascular surgeons who plan interventions and operations.
Surgeons must be in the operating room to be effective. A well thought out and organized system, with interlocking teams, and well disseminated basic knowledge and awareness of vascular diseases reduces the need for a vascular surgeon to be present all the time in many places and ultimately increases the effectiveness of the vascular surgeons that are available by keeping them in the operating room. The system needs to be set up by the surgeon to allow clinic to be a setting mostly for consenting the patient for an operation or a discussion of treatment options.
Finally, vascular surgeons must be aligned with all the resources of the hospital including the considerable numbers of interventional cardiologists and radiologists, neurologists, and nephrologists. There is no reason someone should wait a month to get on the OR list for an iliac angioplasty and stent if an equally skilled and privileged cardiologist or radiologist has an opening the next day. The surgeon’s special talent should be open surgery and hybrid surgery -that which mixes open surgery and intervention in optimal measures which is not possible from a purely percutaneous approach. The key is frequent and easy communication between specialities and trust built by being in one shared cardiovascular institute.
Execution
There is a critical need of good operators. The acuity of disease and their solutions demand the continued presence and availability of open surgery. The fact is, many solutions are optimal in a hybrid fashion and for peripheral vascular disease, these options can only be offered via a vascular surgeon trained in both open surgery and peripheral interventions, or in a combined effort of open surgeon and interventionalist. And many disease categories can only be managed by open surgery.
The reality is that silos, economics, and practice patterns prevent this kind of combined effort. Market forces have pushed the training of vascular surgeons forcefully into the interventional realm at the cost of open surgical training. Some of the geographic maldisdribution of vascular surgeons has to do with younger vascular surgeons flocking to established practices where there are senior surgeons more comfortable in opening a belly or chest (or both). The trap they and hospital systems fall into is then allowing these new recruits to become the interventional specialist of that group, relegating the aging open surgeon to a narrow role, and then finding that the hospital has a problem when that surgeon announces retirement at 60. Every year, millennia of surgical experience retires to beaches and golf courses. The hospital systems should recognize this brain drain as a crisis and create work arounds that keep these skills going. The other opportunity lost is close coordination with interventional cardiologists, radiologists, and nephrologists who in many cases compete with vascular surgeons for the same patients but treat the patients based on their training and skill sets to the exclusion of potentially better operations offered by surgeons. This disjointed care creates both suboptimal outcomes for patients and high costs for hospital systems.
Commerce should never dictate the fate of a patient. A particular point is where competencies and privileging overlap, and guidelines recommend intervention over surgery as in the case of a TASC A or B iliac artery lesion. A patient should not be kept waiting weeks for a spot on a busy surgeon’s OR schedule when an open interventional cardiologist or radiologist slot is available for a iliac stent the next day. It should be a matter of practice that these cases are discussed and distributed, optimally in a shared indication clinic or rounds. Patients bumped off of a surgeon’s elective schedules for emergencies who could be cared for by an interventional partner without an added delay should be given that option. This kind of change requires a commitment to continual reorganization and optimization into a vascular institute.
Conclusion
The perfect vascular surgeon is a unicorn -well skilled, and experienced in open vascular surgery, but also versatile, innovative, and skillful in wielding a wire. I can name just a handful of unicorns. An apt analogy from the book Moneyball is the signing of superstars in baseball on the free agent market. The upshot of that book is that you can arbitrage for the valued metrics through signing several utility players with an aptitude for one thing or another which in sum equals or exceeds that superstar and get the final result -wins, in the same proportions as overspending on a superstar. Rather than searching for that unicorn, it is more important to set up the right system. Screening, testing, and management of mild vascular disease by a nurses and cardiovascular medicine physicians, while directing operations and interventions to vascular surgeons, cardiologists, and interventional radiologists should be the next step in the evolution of vascular care systems. There will never be enough vascular surgeons in the current system. The critical and rare competency is open vascular surgical skill. A surgeon who performs only interventions is not an “advanced minimally invasive practitioner” but rather someone equally privileged as an interventional cardiologist or radiologist, and therefore easily replaceable by an interventional cardiologist or radiologist specializing in peripheral vascular disease. A surgeon skilled in open vascular surgery is becoming rarer every year, but they are still out there, looking at brochures of real estate in sunny places. A team consisting of a cardiovascular medicine physician, many vascular technologists, nurses specializing in vascular diseases, several interventionalists, and a vascular surgeon skilled in open vascular surgery working as a single unit, is far more easy to assemble than finding and recruiting a herd of unicorns.
[i] Kumar MS et al. J Assoc Physicians India. 2016;64(8): 38-43. https://www.ncbi.nlm.nih.gov/pubmed/27762107
