The patient, now in his 90’s, found out about his aortic and iliac artery aneurysms in his early 80’s, had been offered repair, but had refused. Several years ago, one of my partners emergently repaired his ruptured AAA (abdominal aortic aneurysm) via a retroperitoneal approach using a tube graft. At the time of the repair of the AAA, the common iliac artery aneurysms (CIAA’s) were not ruptured and would have added risky time to the repair. He survived and had a postop CT done about two years ago which showed his CIAA’s.
Two years agoThe patient chose not to pursue repair of these aneurysms, I assume figuring that at his age, he’d again take the chance that he would pass on without the hassle of another procedure.
He was recently admitted for treatment of another condition, when his physicians noted a large visible pulsatile mass on his lower abdomen.
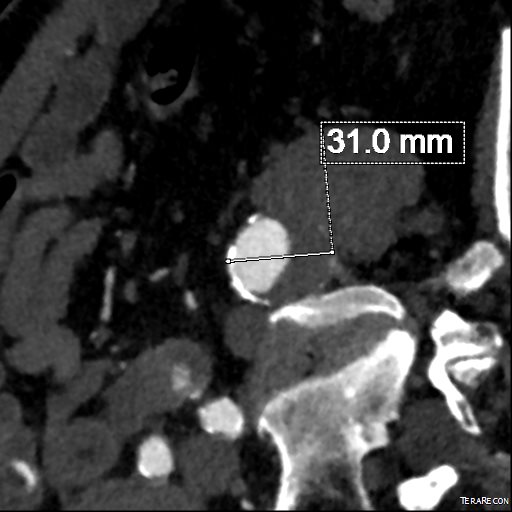
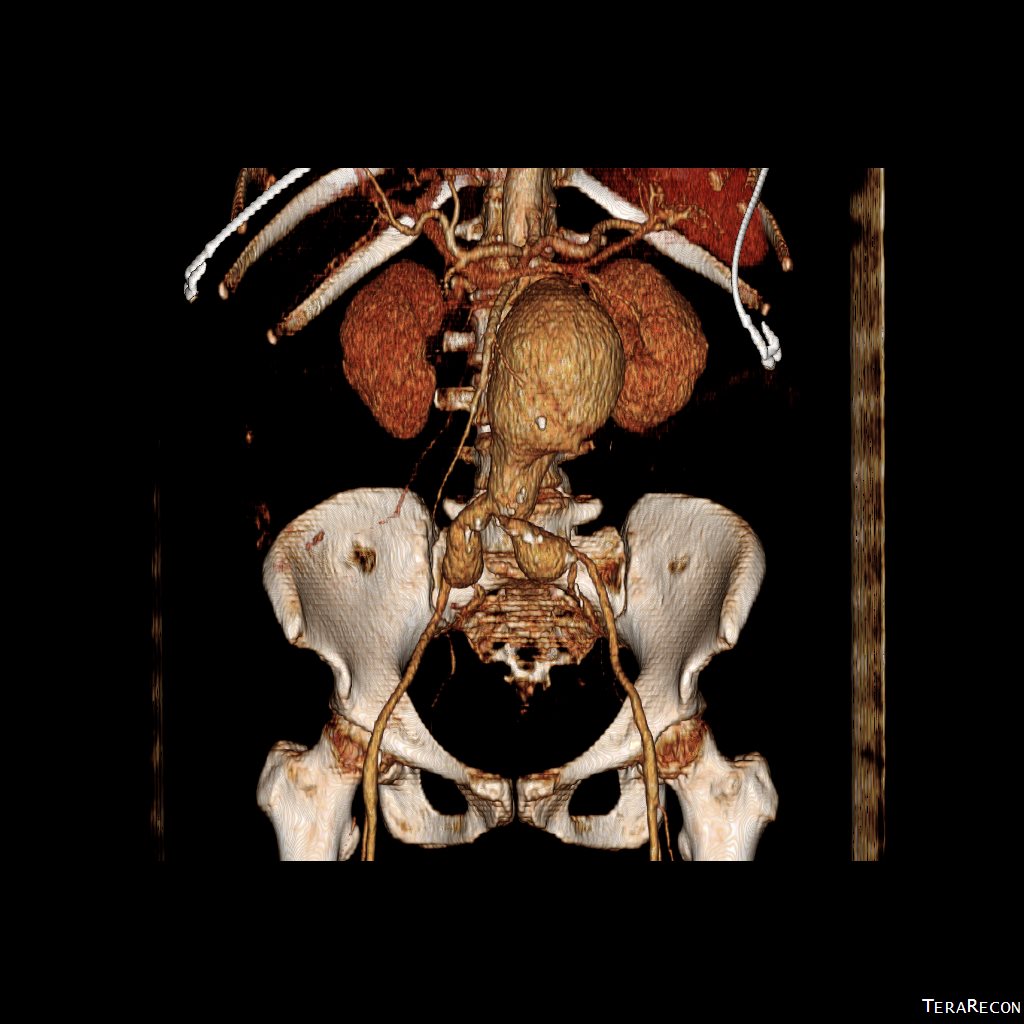
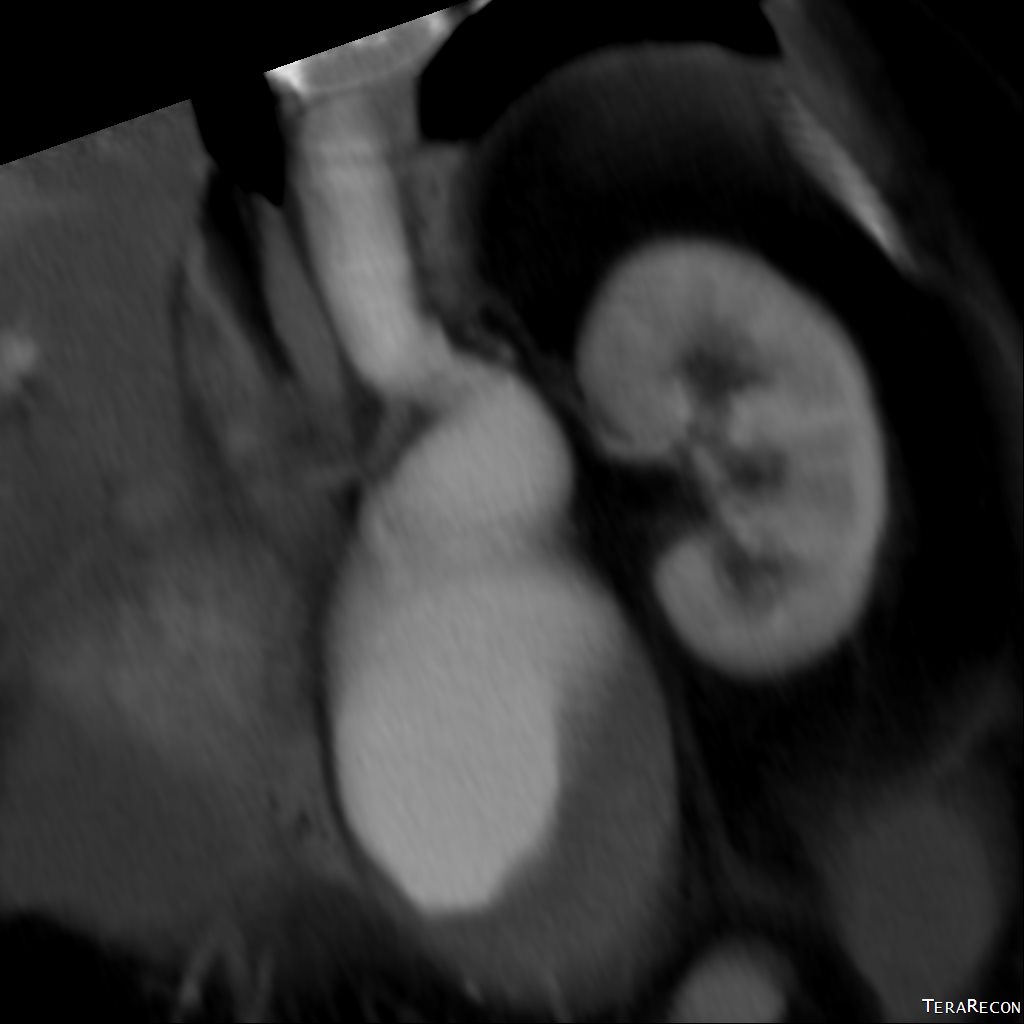
A CT scan was performed. It showed a 13 cm left common iliac artery aneurysm which was responsible for the visible puslatile mass and a large right common iliac artery aneurysm. The left internal iliac artery was thrombosed. His right common iliac artery aneurysm was over 5cm in size.
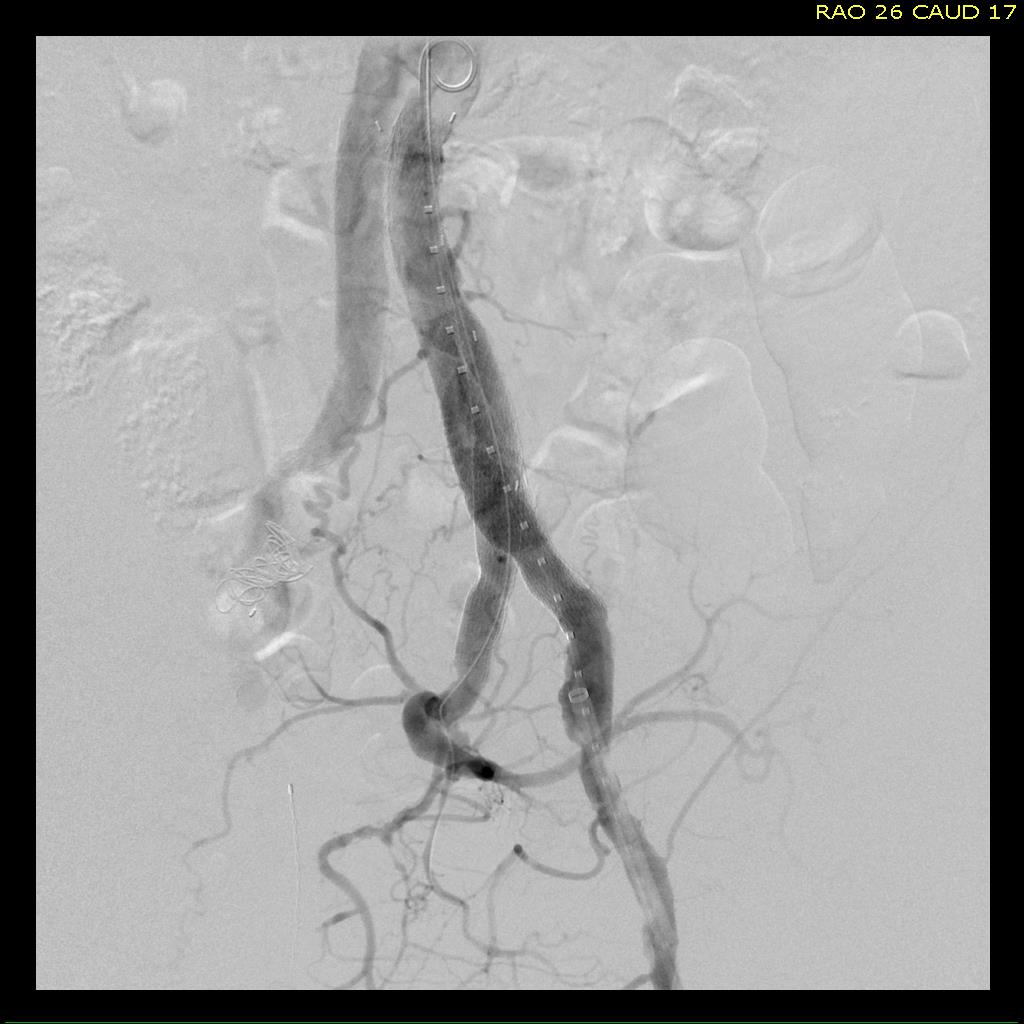
My partner, Dr. Ezequiel Parodi, was consulted for this case. He performed a percutaneous EVAR. The procedure was made difficult by tortuosity in iliac artery and the tube graft in the aorta requiring a secondary access from the arm to straighten out and advance the stent graft (aka body floss). Dr. Ezequiel Parodi
In followup, the aneurysms decreased in size and showed no endoleak around a patent stent graft.
Common iliac artery aneurysms expand at a rate proportional to their starting size and have increased rates of expansion in those with prior aortic aneurysm expansion (ref 1). Rupture probably signals a tendency to expand rapidly. There is evidence that iliac ectasia and aneurysms left over after tube graft repair (aorto-aortic) of AAA is benign and can be safely observed (ref 2), but these were all small at the start.
I had been trained at the dusk of the open surgical era and the dictum was aortobi-iliac bypasses to avoid future problems with the iliac arteries. With EVAR, and soon bifurcated iliac branched stent-grafts (currently on trial), staged repair of metachronous iliac aneurysms after tube graft repair of AAA has not only an appeal, but some logic as open bypass to iliac bifurcations, particularly in large men, is challenging and potentially morbid. This is a case of a patient who had a large iliac aneurysm that was not repaired initially due to the exigencies of ruptured AAA and had refused planned staged repair. His aneurysm grew from over 5cm to 13cm in 2 years time without rupturing. Such good fortune is very rare.
Vascular surgeons like to collect large aneurysm stories like fishermen talk about big fish. This is the largest unruptured common iliac artery aneurysm I have seen. While it is baffling to many who are in healthcare, it is important to understand noncompliance is common. Denial is a powerful urge, and a uniquely human one.
The patient presented with complaints of leg and foot pain with sitting and short distance calf claudication, being unable to walk more than 100 feet. This is unusual because sitting usually relieves ischemic rest pain. He is in late middle age and developed claudication a year prior to presentation that was treated with stent grafting of his superficial femoral artery from its origin to Hunter’s canal at his local hospital. This relieved his claudication only briefly, but when the pain recurred a few months after treatment, it was far worse than what he had originally. Now, when he sat at his desk, his foot would go numb very quickly and he would have to lie down to relieve his pain.
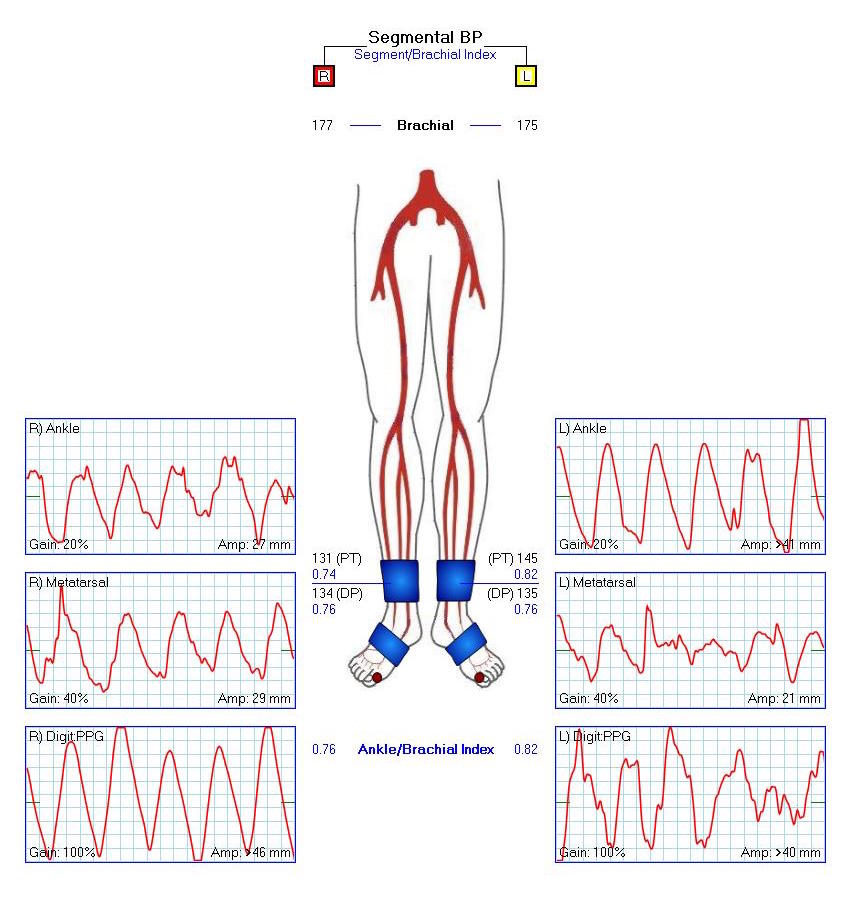
On examination, the patient was moderately obese with overhanging belly. He had a palpable right femoral pulse, but nothing below was palpable. He had multiphasic signals in the dorsalis pedis and posterior tibial arteries. The left leg had a normal arterial exam. Pulse volume recording and segmental pressures were measured:
These are taken with the patient lying down which was the position that relieved his pain, and the PVR’s show some diminishment of inflow. It would be easy at this point to declare the patient’s pain to be due to neuropathy or spinal stenosis, but because of his inability to walk more than a hundred feet and because of his severe pain with sitting, I went ahead and obtained a CTA.
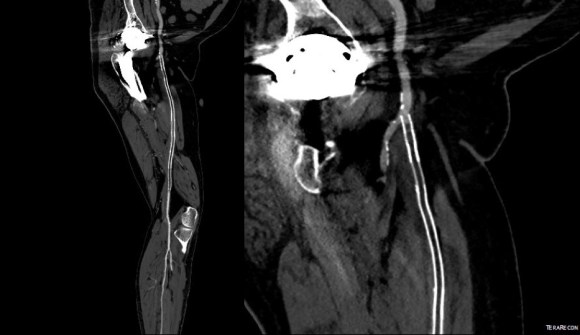
The CTA showed he had an occluded superficial femoral artery (SFA) with patent profunda femoral artery (PFA) with reconstitution of an above knee popliteal artery with multivessel runoff. The 3DVR image showed his inguinal crease to be right over the femoral bifurcation which is not an unsual finding, but his stent graft was partially occluding his profunda femoral artery.
I decided to take him to the operating room to relieve his PFA of this obstruction. My plan was to remove the stent graft at the origin of the SFA and at the same time, remove the plaque and occluded stent graft from his SFA to restore it to patency.
In the OR, on exposing his SFA, I discovered that because of his overhanging belly, his inguinal ligament had sagged and was compressing his femoral bifurcation.
This explained his presentation. The stent graft really had no chance as when he sat, the belly and ligament compressed it at the origin, and because it partially occluded the origin of the PFA, sitting probably pinched off flow completely. The 3dVR image shows the mid segment of PFA to have little contrast density -this is not because of thrombus, but because of the obstruction, the PFA was getting collateral flow from the hypogastric artery.
The stent graft was removed at its origin via a longitudinal arteriotomy after remote endarterectomy of the distal graft.
In this case, the Multitool (LeMaitre) was useful in dissecting the plaque and stent graft because of its relatively stiff shaft compared to the standard Vollmer rings. The technique of EndoRE has been described in prior posts (link).
The stent graft came out in a single segment -they come out easier than bare stents.
The patient regained palpable pulses in his right foot and recovered well, being discharged home after a 4 day stay.
While one could argue that just taking out the short piece of occlusive stent graft over the PFA was all that was necessary, I feel that there is no added harm in sending down a dissector around the stent, and in this patient there was restoration of his SFA patency which was the intent of the original procedure.
Unlike PTFE bypasses that sometimes fail with thromboembolism, SFA EndoRE fails with development of focal stenoses. From a conversation I had with Dr. Frans Moll at the VEITH meeting, I found that he has had good experience with using drug coated balloons in the treatment of these recurrent stenoses.
At the time of discharge, the patient was relieved of his rest pain, and was no longer claudicating. The common femoral artery, its bifurcation, and the profunda femoral artery remain resistent to attempts at endovascular treatment, and remain in the domain of open surgery. And in retrospect, the history and physical examination had all the clues to the eventual answer to the oddities of the patient’s complaints. The combination of inguinal crease, abdominal pannus, and low hanging inguinal ligament meant these structures acted to crush the stent graft and femoral bifurcation.
The patient was referred to me after having undergone an intervention for chronic mesenteric ischemia. She is over 70 years of age and had lost over thirty pounds in 3 months due to severe abdominal pain with eating. A month prior to seeing me, she had undergone arteriography at an outside hospital and was found to have occlusion of her celiac axis (CA) and superior mesenteric artery (SMA) with a small but patent inferior mesenteric artery. Attempt at recanalization, done from left brachial access, of the SMA was abandoned after the patient started having pain, and the inferior mesenteric artery was accessed and stented with a balloon expandable stent. Despite the stent, the pain persisted. On examination, she was cachectic, weighing about a hundred pounds, and had moderate to severe pain with abdominal palpation. CT angiography (shown above) showed a chronically occluded CA and SMA and a patent stent to the IMA.
After discussion with the patient about the possibility of a bypass, we decided to proceed with diagnostic arteriography and an attempt at recanalization. When planning these, I always try to come from the groin first as most of the time I am able to revascularize from below. I try to avoid 6F sheaths in the arms of thin cachectic patients -women especially where the brachial artery is likely the same diameter as a 6F sheath. The only downside about coming from below is that it is technically challenging and the stent comes off at a higher angle than the SMA typically has in situ.
The image below shows the procedure:
The series of images shows the initial aortogram and access. The superior mesenteric artery has a stenosis at the origin, with an area of post stenotic dilatation or small aneurysm, which occludes beyond the first three branches of the SMA. The IMA fails to feed the bowel -the later phases not shown shows filling from the SMA segment to the CA and ileal branches.
The key step to this procedure is in getting “deep” access with a wire -in this case a floppy Glidewire, which I used to cross the occluded SMA. There is feedback from the tip which occurs if you spin it without a torque device. The wire has the quality, a feature really, of being tacky when dry, allowing for a great deal of coaxial spin with your first two fingers and your thumb. The tip transmits information about what it is crossing as you spin it -this is something that is hard to teach at first, but is gained largely through experience, but I learned it from Dan Clair over a decade ago when he barked at me to get rid of the torque device (“a tool for babies!”). The tip will go where it should if you spin, not push.
Once the wire is buried, a suitable catheter that tracks well is brought across the occlusion. Again, while there are many catheters that can do this, the Glide Catheter is suitable again from spinning across an occlusion over the wire that would push out the lowest profile and equally hyrdophillic catheters. Once the catheter is buried, a suitably stiff wire (in this case a Rosen wire) should be brought across -this widens the arc created by the wire as it goes up and over the SMA origin and allows for delivery balloons and stents. Using the balloon-piton technique (a requisite for FEVAR), the sheath is brought into the SMA, securing access into it.
The occlusion in the mid-SMA ballooned nicely and did not require a stent -a nonocclusive dissection is seen but I chose not to treat this as placing a stent is likely to cause as many problems as solve and the dissection is in line with flow. The origin was stented with a balloon expandable stent -having the patient awake is useful in determining if the stent is “big enough.” Final arteriography in two planes is shows below.
Gratifyingly, the entire mesenteric system in the CA (foregut) and SMA (midgut) lit up. I admitted her for observation as I have seen patients develop bowel infarction with reperfusion which may be due to embolization but I think just as likely due to edema. Food needs to be reintroduced slowly as there maybe metabolic consequences to rapid refeeding. Her baseline lactate was 2.6mMol/L but came down to 0.8mMol/L the next day. Her other labs were normal. Her pain remitted and she was able to tolerate a regular diet by postoperative day 2.
Discussion:
Mesenteric ischemia is a particularly morbid condition. When it presents acutely, there is a high mortality rate (ref 1). Revascularization in good risk individuals is still bypass surgery (ref 2,3). The inferior mesenteric artery offers a dismal revascularization target for this reason -while the artery will remodel and dilated in the setting of mesenteric ischemia, its orifice from the aorta does not and is usually no more than 1-2mm from birth to adulthood. Also, while the large bowel will get perfusion from the IMA, and the foregut may get collateral flow from collaterals fed from the middle colic via the Arc of Riolan, the midgut does not get sufficient flow from from the IMA because it requires the longest path to fill the ileal and jejunal branches. The development of atherosclerosis in the aorta further complicates attempts at stenting. Despite this, it is still attempted (ref 4) and in 4 patients was successful at relieving pain for short periods of time, with one patient requiring eventual bypass despite characterization as “high risk.” It is a reflection of how poorly this vessel does with intervention that this 4 case series is the largest in the literature.
The analogy to IMA stenting in the legs is stenting of a heavily diseased profunda femoral artery in the setting of critical limb ischemia with femoropopliteal occlusive disease. It is occasionally successful in the short term, but will only delay the inevitable operation. There are no low risk patients with severe weight loss due to mesenteric ischemia. Aggressive intervention offers a path of survival for these patients, and but long term results are only possible with bypass.
Park WM, Cherry KJ, Jr, Chua HK, Clark RC, Jenkins G, Harmsen WS, et al. Current results of open revascularization for chronic mesenteric ischemia: a standard for comparison. J Vasc Surg. 2002;35(5):853–859.
Kasirajan K, O’Hara PJ, Gray BH, Hertzer NR, Clair DG, Greenberg RK, et al. Chronic mesenteric ischemia: open surgery versus percutaneous angioplasty and stenting. J Vasc Surg. 2001;33:63–71.
Wohlauer M, Kobeiter H, Desgranges P, Becquemin JP, Cochennec F. Inferior Mesenteric Artery Stenting as a Novel Treatment for Chronic Mesenteric Ischemia in Patients with an Occluded Superior Mesenteric Artery and Celiac Trunk. Eur J Vasc Endovasc Surg. 2014;27(3):e21-e23.
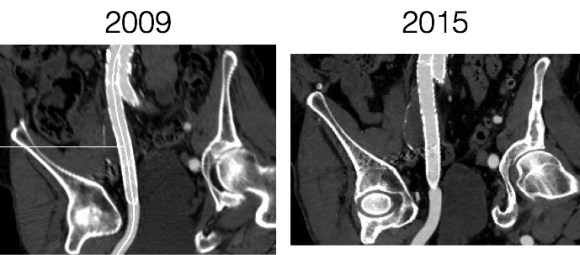
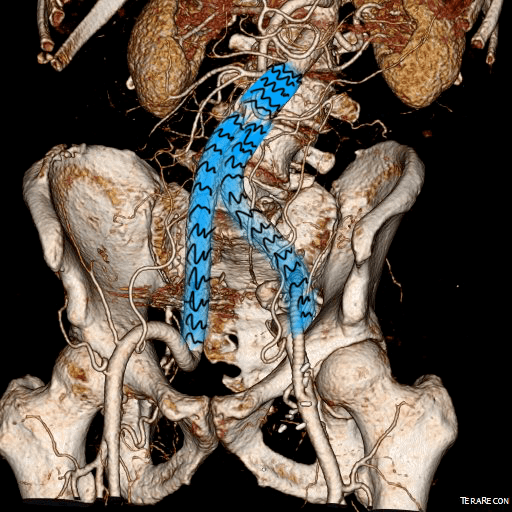
The patient had undergone EVAR for bilateral common iliac artery aneurysm with the original Gore Excluder stent graft a dozen years before with coil embolization and extension to the external iliac on the larger side and femoral to internal iliac artery bypass on the other side. A coagulopathy, one of the clotting factor deficiencies, had made him high risk for bleeding with major open surgery. His aneurysms never shrank but remained stable and without visible endoleak by CT for a long time resulting in ever longer intervals between followup.
2013
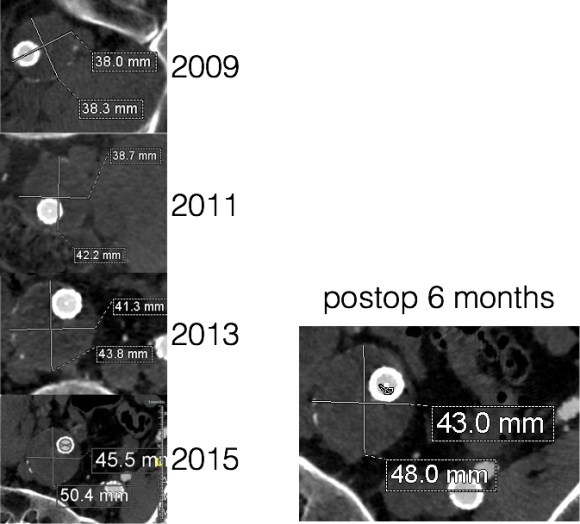
Between 2009 and 2013, there was subtle enlargement on the embolized side without a type I or type III leak, and the patient was brought back a year and a half later, with further growth of the sac.
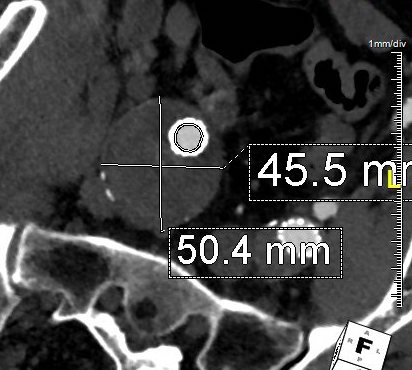
2015
This was a relatively rare type IV endoleak that was causing sac enlargement due to excessive graft porosity of the original Excluder’s graft material. Its treatment is either explantation or relining. We chose to reline the graft with an Excluder aortic cuff at the top and two Excluder iliac limbs.
This was done percutaneously and in short followup, there has been stabilization and even some reduction in the aneurysm circumference.
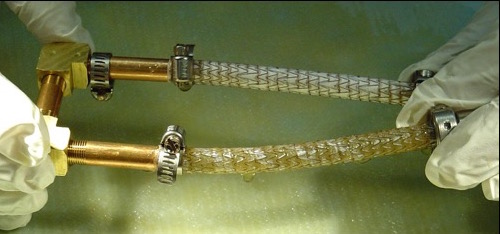
It was long known that a certain percentage of PTFE grafts “back in the day” would sweat ultrafiltrated plasma. The relative porosity of the grafts allowed for transudation of a protein rich fluid.
Tanski W, Fillinger M. J Vasc Surg 2007;45(2):243-249.
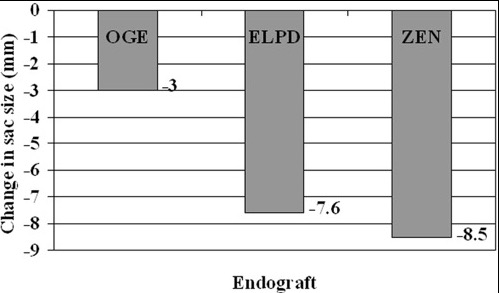
This results in a hygroma formation. I remember seeing this in AV graft fistulae back in the 90’s -after flow was introduced, the grafts would start sweating! The newer grafts are lower porosity and this is seen very infrequently. Drs. Morasch and Makaroun published a paper in 2006 comparing parallel series of patients who received the original Gore Excluder (OGE), the currently available Excluder Low-Permeability Device (ELPD), and the Zenith device (ZEN). Sac enlargement occurred in equal measure between OGE and ZEN but zero was reported for the ELPD.
Haider S et al. J Vasc Surg 2006;44(4):694-700.
The ELPD had higher rates of sac shrinkage than the OGE, and equal rates of sac shrinkage compared to ZEN.
Haider S et al. J Vasc Surg 2006;44(4):694-700.
The diagnosis in my patient’s case came about through serial followup through a decade. While I doubt that the aneurysm would have ruptured in the same way as in a Type I, II, or III endoleak, I am sure it would have progressed to developing symptoms from aneurysmal distension or local pelvic compression.
Is it possible to visualize this kind of endoleak at the time it is suspected? I came across a case series from the Netherlands using Gadofosveset trisodium which takes longer to clear than the usual Gd-based MR contrasts and they successfully visualized transudative leaks in 3 serial patients with the original Excluder graft.
Cornelissen SA et al. J Vasc Surg 2008;47(4):861-864.
The problem is that Gd-based contrasts have toxicity, especially for patients with poor renal function. The protocol is time consuming. And I suspect that ten years out, a lot of grafts will have positive findings, especially cloth based grafts that are sutured to their supporting stents, without clinical basis for treatment as their sacs size are likely stable on a year to year basis.
That said, as we are well into the second decade of commercially available stent grafts, it is even more important than ever to continue lifelong followup even for what is assumed stable, patent grafts and anatomy.
The patient, a younger middle aged woman, was referred for treatment of a large, growing infrarenal AAA over 8cm in size complicating a severe pancreatitis. The pancreatitis occurred about a month prior to presentation and resulted in a substantial pancreatic leak. At the time of that presentation, her AAA was found incidentally and was about 7cm. In the interval, her pain resolved and she was asymptomatic. On examination, her abdomen was soft, and a large aortic aneurysm was easily palpable.
Pancreatitis with surrounding retroperitoneal fluid leak
CT scan was performed showing an enlarging AAA over 8am and abundant retroperitoneal pancreatic fluid without abscess or infection. The AAA was infrarenal but complicated by a severely tortuous, short infrarenal neck with 90 degrees of angulation and about 8mm in length. As the pancreatic leak was yet early in the process, no pseudo aneurysms had formed. MRCP showed no active leak.
Short neckGreater than 90 degree neck angulation
Other than the pancreatitis, the patient, who was in her 50’s, was an otherwise good risk patient.
The treatment options were:
1. Wait until pancreatic fluid resolution or pseudo aneurysm formation, then standard open repair of the large aortoiliac arterial aneurysm. Not desirable because of the relatively rapid aneurysm growth and current size.
2. EVAR -This is outside the IFU for any of the available devices because of the highly tortuous neck anatomy. While note shown, the external iliac arteries were 5mm in diameter, but in the absence of plaque, was possibly due to spasm. The Nellix device is yet on trial, but there are limits on how much you can straighten this neck. The devices with suprarenal stents end up straightening out the graft with deployment of the graft in an ellipse. This also means loss of seal zone length which decreases with oblique deployment. FEVAR is not possible because of this neck tortuosity as well but was considered briefly.
3. Homograft repair or Rifampin soaked graft repair -The former is costly and still susceptible to infection from a virulent organism as is the latter, but both are likely safe with likely foregut flora.
4. Neo-Aorta reconstruction (NAS) with deep femoral vein. This could work, but is time consuming and relatively morbid. The tactic of mobilizing the vein and then repairing the aneurysm in a separate, staged fashion the following day or two is reported to shorten the overall operative time. This patient would require both femoral veins to be harvested.
5. Aneurysm exclusion and extra-anatomic bypass with axillofemoral bypass. Offered to complete this list, this is the least desirable option given the poor long term behavior of axillofemoral bypasses in younger patients.
When faced with this kind of challenge, it makes sense and should be standard practice to get the opinion of the group. I happen to have excellent partners to run this kind of cases. The consensus was this: EVAR with accepting a short term result to temporize until definitive repair could be done. I found this acceptable. I chose to use the Excluder device because it allows for redos of the proximal deployment (C3 Delivery system) and the 23mm and 26mm devices used 16F access. A detailed discussion with the patient and the intention to eventually definitively repair open was discussed and patient was agreeable to proceeding. Plan B’s of Rifampin soaked graft replacement and NAS was also discussed.
I tried two things that was different. I felt that a stiff wire would result in horizontal orientation of the top of the graft, and so I placed a bend in the wire. Prior experience with unintended bends in wires have taught me that passing these wires is largely tolerated as long as it is done through catheters and sheaths. The other thing I did was bend the top of the delivery system -this was done with some care as I did not want to detach the contraining mechanism.
The wire and delivery system modification did tilt the top of the graft away from the left side of the aorta. It had the unintended effect of keeping the wall grabbing anchors away from the near wall while constrained.
It didn’t tilt the graft as much as I would have liked, but the graft deployed in a left to right fashion that allowed for controlled delivery across all of the available neck. Gratifyingly there was seal (below). I flared the right, while excluding the left iliac bifurcation because of the larger iliac aneurysm.
As this was done percutaneously, the patient recovered rapidly and was discharged a day later. The question philosophically for me is if the seal remains intact, would there ever be a need for explantation? The patient only received perioperative antibiotics, and I felt long term antibiotics was not indicated. Standard followup was arranged.
There is no question there is a need for devices designed for this kind of neck anatomy. These devices need to bend over to angles at least 90 degrees and unbend based on delivery system design. They need to be low profile as this facilitated repair in this patient with small access vessels.
update:
After she recovered, her interesting case was published as a case report in BMJ:
Karam PA, Moslim MA, Park WM, Morris-Stiff G. Abdominal aortic aneurysm in the setting of Clostridium perfringens pancreatitis. BMJ Case Rep. 2017 Aug 7;2017:bcr2016218549. doi: 10.1136/bcr-2016-218549. PMID: 28790092; PMCID: PMC5612546.
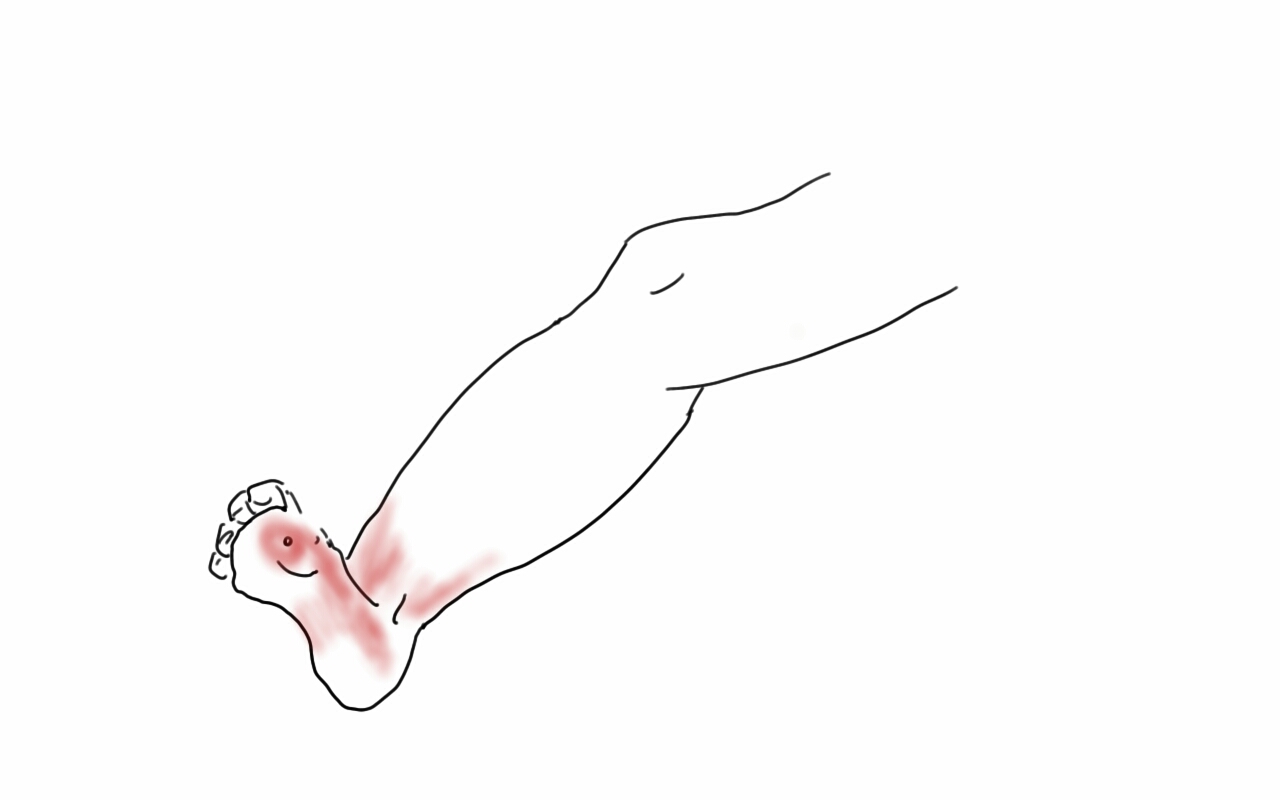
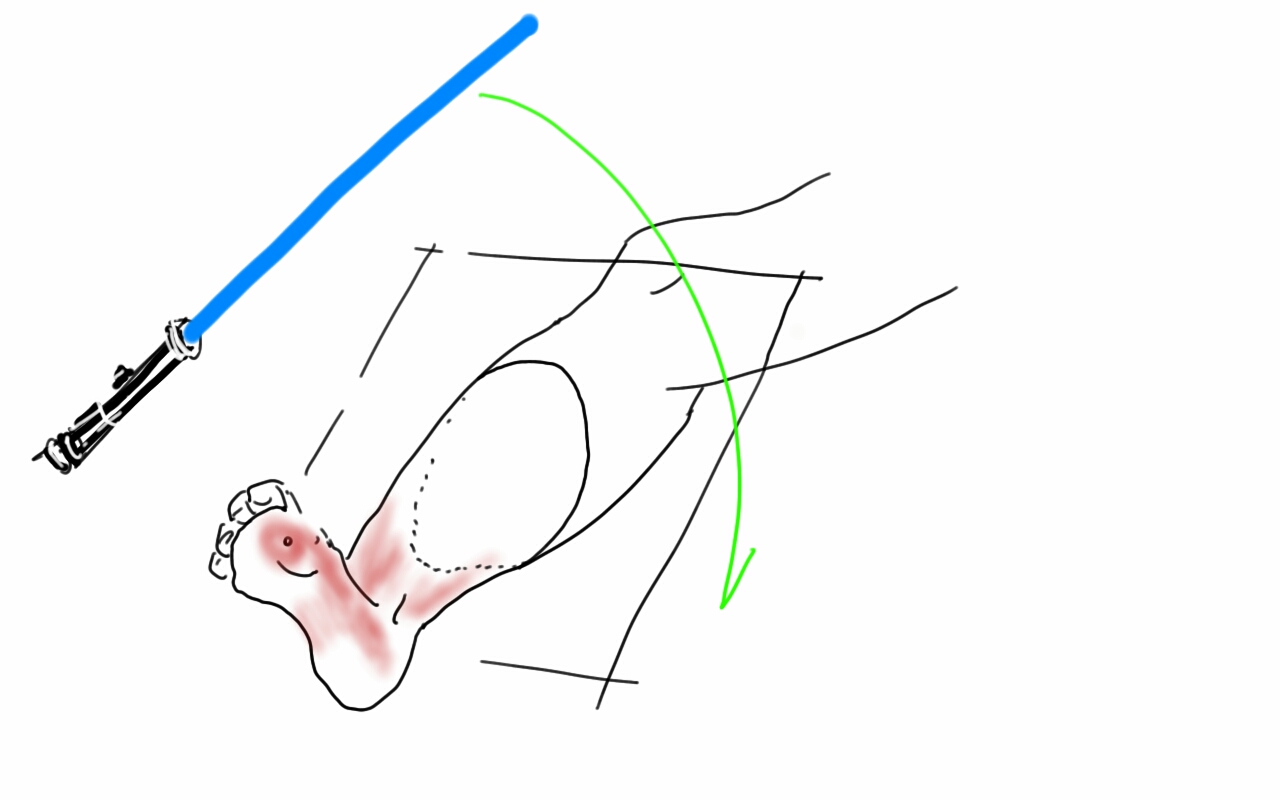
At one time, I was performing below knee amputations in the same way that most textbooks prescribe. This patient presented with severe foot and leg infection with exposed tendons and cellulitis secondary to advanced diabetic neuropathy and arteriopathy.
My sketch above showed the situation which we treated with two stage guillotine and final BKA. At the final stage, standard technique involves creating the classic flap shown below.
This is a tricky flap to make well because there are many variables -the amount of muscle left, the thickness of the subcutaneous fat, the vascular supply, etc. The biggest criticism I have of this flap is that it is prone to edema particularly in the meaty posterior flap, putting great stress on the skin sutures or staples. This then creates fat or skin necrosis in the posterior flap, or muscle necrosis resulting in wound infections and hospital readmissions, which are particularly at risk for need for further leg amputation in these patients with diabetes. I have to confess, while I could figure out how to cut the flap in the end, it was really hard to teach, and if it is hard to teach, you have to figure out a better way.
Here is the better way. The idea goes to the concept that the weight is borne in a distributive ring around the stump. The muscle on the tibia does not create a heel to bear weight on and so serves only the purpose of delivering blood to the overlying skin. So you only need the gastrocnemii and Achilles tendon for fascial closure, and maybe a little soleus. The elimination of posterior compartment muscle bulk greatly reduces the tension on the fascia and skin.
The incision can be simplified by cutting the flap along an oblique 2D plane -a light saber cut!
The posterior flap is reduced to just Achilles and a layer of soleus muscle, but otherwise, the internal bone and muscle organization is cut as below:
The skin at this point is never touched with a surgical instrument, only the subcutaneous later or fascia. Using interrupted absorbable heavy gauge monofilament (single strand of the double looped PDS used for abdominal closure is plenty of suture), interrupted buried sutures are placed in the fascia from middle outwards.
This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
The skin is dress with a single layer of Xeroform and fluff gauze and gently a compressive dressing is applied from stump to above the knee, while keeping the knee cap exposed -the knee cap is prone to skin necrosis with ACE wraps that are left unattended.
The wound’s ability to heal is now largely a function of keeping the suture line tension and edema free. Edema is the great killer of these flaps and the problem with sutures or staples here is that edema creates zones of skin necrosis under these staples that then results in a postop wound breakdown and infection. With these simple steps largely copied from our plastic surgical confreres, I have been able to create very functional stumps with low morbidity.
This patient is 3 months from her 2 stage amputation and is walking on her prosthetic leg and is very happy. Notice, the dog ears have contracted!
The images above show a patient with on isolated occlusion of his left common iliac artery. He was young, in his forties, but was a heavy smoker and suddenly developed claudication of his left leg which interfered with his work. He quit smoking and did not progress with exercise. Discussion involving possible stenting was made and initially offered but he turned it down because erroneously he assumed that his father’s coronary stents were the same as an iliac stent in terms of longevity. I do think that common iliac and aortoiliac occlusive disease is well treated with stents, but I felt it was possible to do a common iliac endarterectomy. We went over these images together and he settled on proceeding with endarterectomy.
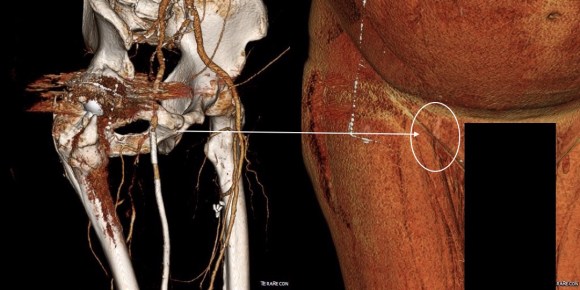
The images show how well the 3D Volume Rendering, which I mentally call Virtual Reality, of CTA makes it possible to plan out operations and exposures virtually. The bottom left image shows the surgeon’s eye view of the exposed vessel.
Below, the virtual and the actual are juxtaposed.
The outline on the virtual image (volume rendered) shows the areas of retraction -for the trainees, the retractor systems work to make quadrilaterals out of linear incisions, and as a rule, the incision should be twice the length of the square that you want to expose. The end points of the endarterectomy were at the aortic and iliac bifurcations.
The arteriotomy was repaired with a patch at the iliac bifurcation -the common iliac was large and was repaired primarily.
The specimen below was fibrocalcific. The thing about this disease is that the plaque truly has no endpoint -intimal thickening and mild plaque was present that could be taken all the way to the aortic root and to the feet on the other end!
This patient did very well and had palpable pulses. He did not develop neointimal hyperplasia and successfully quit smoking.
One of the exciting developments is the ongoing development of wearable virtual reality and display solutions -particularly from the gaming industry. The gaming industry ironically drives all computer imaging because that is where the money is at. The advances in imaging trickle down to medicine -the VR images seen here are the result of the same algorithms that drive first person shooting games. It would be great to see this displayed intraop on a HoloLens, on a virtually positioned screen behind the assistant!
The figure above shows the summarizes the problem that brought the patient to his local hospital and triggered his transfer to our acute aortic syndrome unit. The concept is that all chest pain of cardiovascular origin gets intake through a vast intensive care unit staffed by cardiovascular intensivists. Stabilization, workup, transfer to operating room or interventional suite all happens in an ICU that encompasses almost a city block.
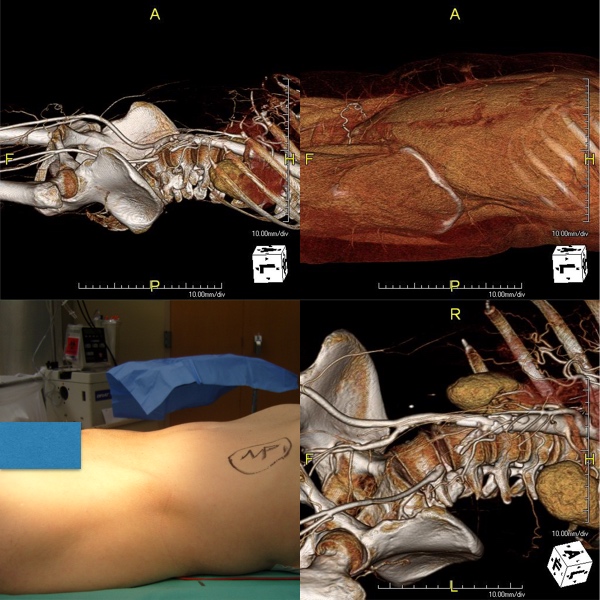
The patient is an older middle aged man with sudden onset of back and abdominal pain. He was on coumadin for a prior SMV thrombosis and treatment for a ruptured appendicitis -antibiotics with plan for staged appendectomy. CT at his local hospital revealed a type B aortic dissection (TBAD) that extended into his superior mesenteric artery.
Bovine arch and TBAD in 3DVR view on TeraRecon Aquarius reconstruction.The aortic dissection terminated in the infrarenal aorta. The celiac and SMA had true and false lumen perfusion, the right kidney was perfused through the false lumen, the left through the true. Both legs received true lumen flow.
The dissection started at the left subclavian artery origin. The false lumen compressed the true lumen up at the proximal descending thoracic aorta. This is an important finding because in this configuration with much of the filling of the dissection from the distal reentry sites, the false lumen acts like a pressurized, compressive lesion. With time, the adventitia around the false lumen may become aneurysmal if the false lumen fails to thrombose or obliterate. When the dissection is acute, the flap may cause a direct obstruction to flow or a dynamic one that depends on the pressure difference between true and false lumen.
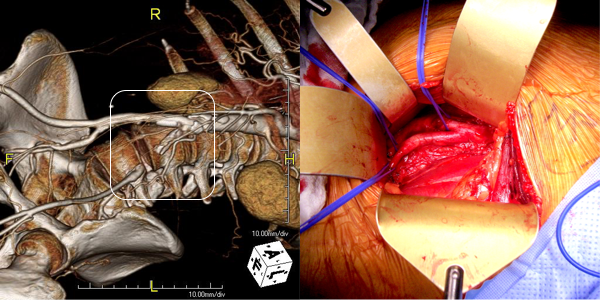
In this patient, thrombosis occured in the SMA beyond the origin due to dissection and decreased flow. This was consistent with the patient’s complaint of generalized abdominal pain and examination findings of pain out of proportion to the exam, indicating acute mesenteric ischemia.
His laboratory findings were within normal ranges, indicating this was early in the process. It is important to remember that no lab value correlates with acute mesenteric ischemia except very late in the process, and acute mesenteric ischemia remains a clinical diagnosis (reference 1) that is associated with a high mortality rate.
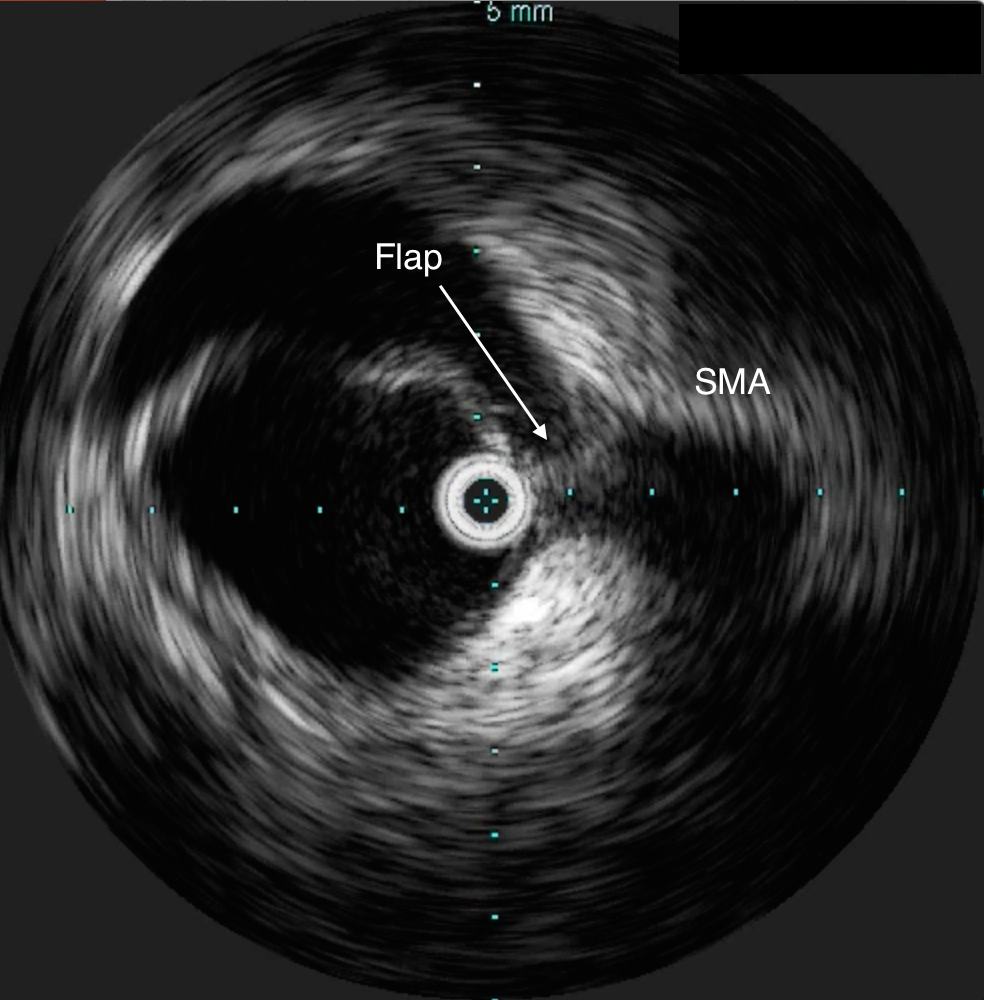
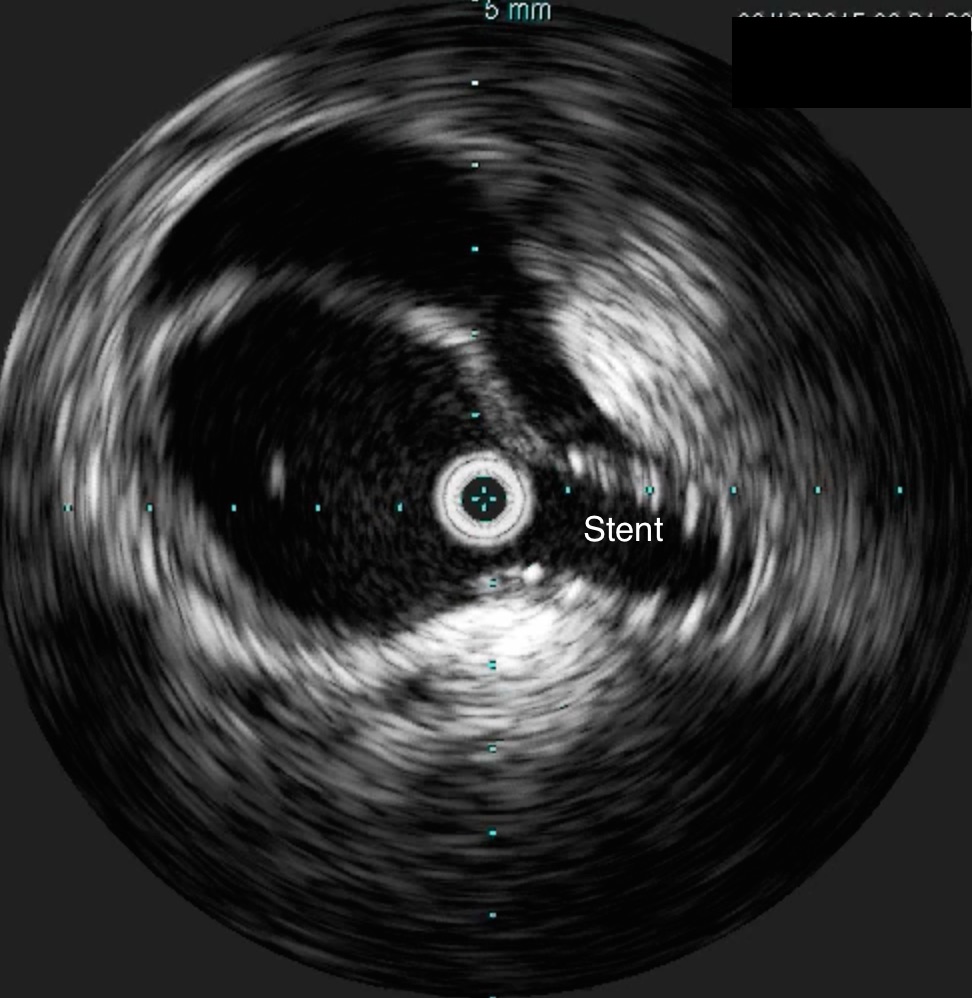
He was taken to the hybrid operating room. Right groin access was achieved and wire access to the arch was achieved. IVUS (Intravascular ultrasound, Volcano) was used to confirm the location of the wire -I believe this is an important adjunct as simply passing the wire doesn’t guarantee travel up the true lumen.
IVUS confirming true lumen access, and dissection flap compressing SMA originA conformable TAG endograft (CTAG, Gore) was delivered through a 24F sheath into position. Two devices were used to cover the thoracic aorta from the left subclavian artery to a position immediately above the celiac axis. The left subclavian was partially covered -the bare stents covering the rest.
Partial coverage of the left subclavian artery confirmed by persistence of strong left brachial artery pulse Post Deployment of two 40mmx20cm CTAG (Gore) endograftsThis excluded the proximal entry tear of the TBAD. IVUS (image below) showed improved lumenal diameter of the true lumen into the SMA.
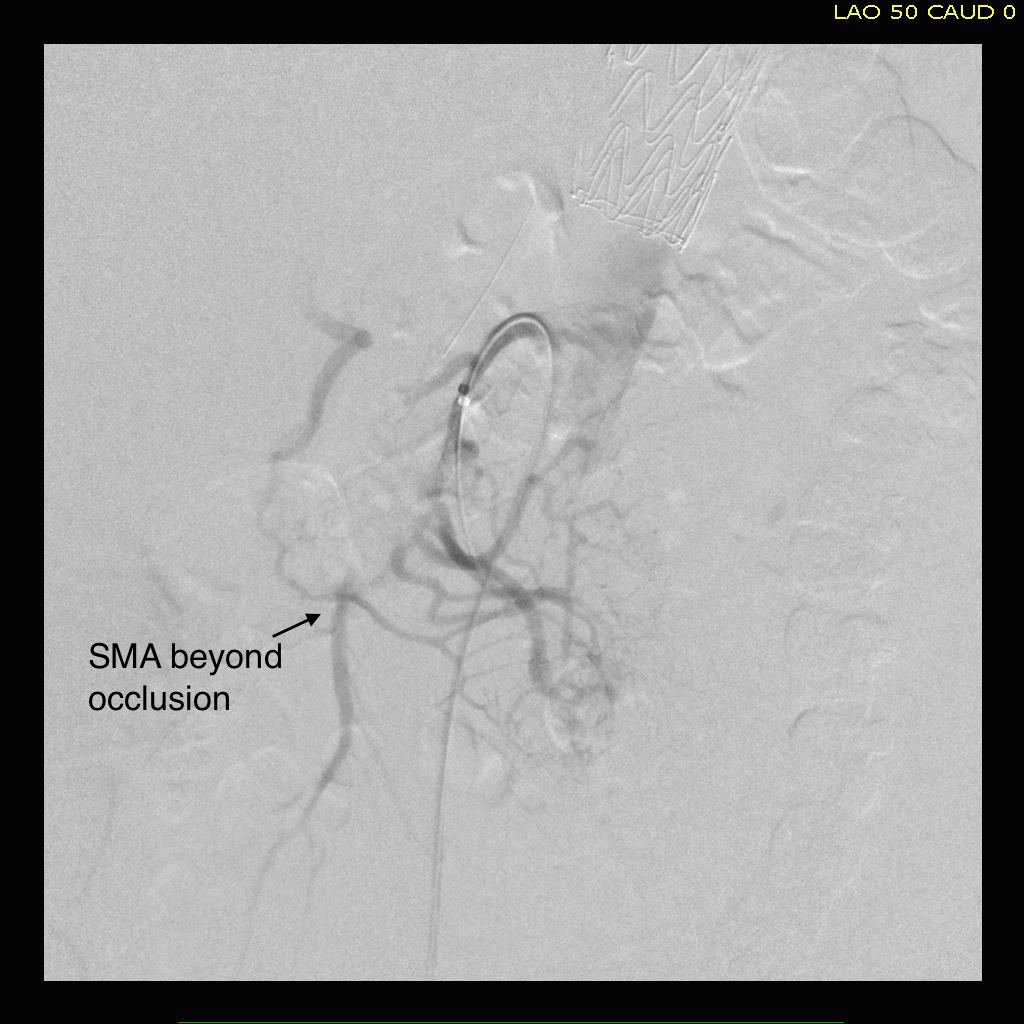
After stent graft placement in the thoracic aorta, the true lumen into the SMA expandsOnce this was done, wire access into the SMA was achieved. This was technically challenging from the groin, and the backup plan was access from the left brachial artery which had been prepped. With patience, 6French access into the SMA was achieved. The origin was stented with a balloon expandable 8mm x3cm stent -sizing was based on IVUS and CT. This creates an alarming arteriogram as the stent appears oversized on subsequent runs -it is important to remember that the false lumen still takes up space beyond. Arteriography located the thrombosed segment and the reconstituted SMA beyond.
Wire access was achieved across the thrombus. At this point, I had a range of options for thrombectomy including simply aspirating which retracting a catheter. This was not optimal as I could lose subsequent wire access or reenter the false lumen. The other option was an open thrombectomy and patch angioplasty -the thighs were prepped in case we had to harvest vein. Again, in the setting of dissection and going into the mesentery, an open revascularization while feasible, is challenging.
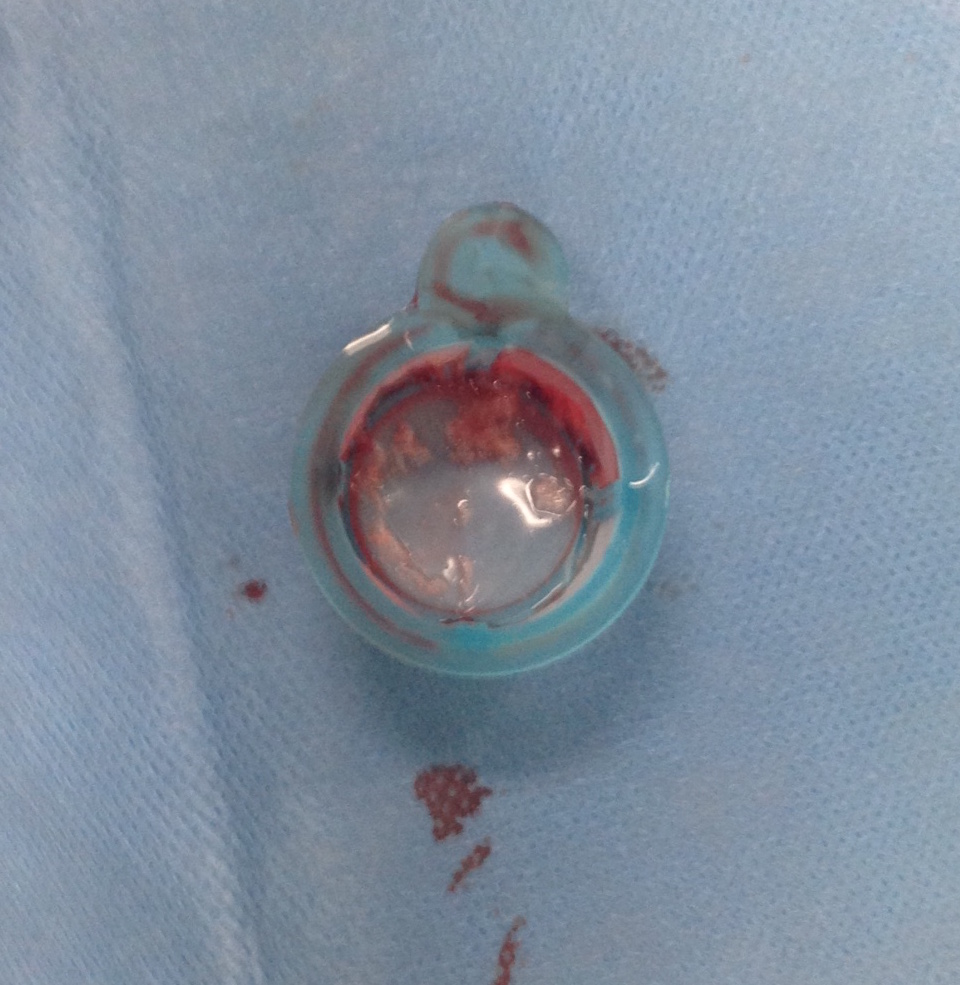
Thrombectomy catheters like Angiojet were available, but I chose to try the Export aspiration catheter (Medtronic). It is simple to set up and goes over a 0.14 wire. It is designed for the coronaries which have a similar lumenal diameter as the SMA. It worked well in this setting in retrieving thrombus which had a pale element that may have indicated some chronicity.
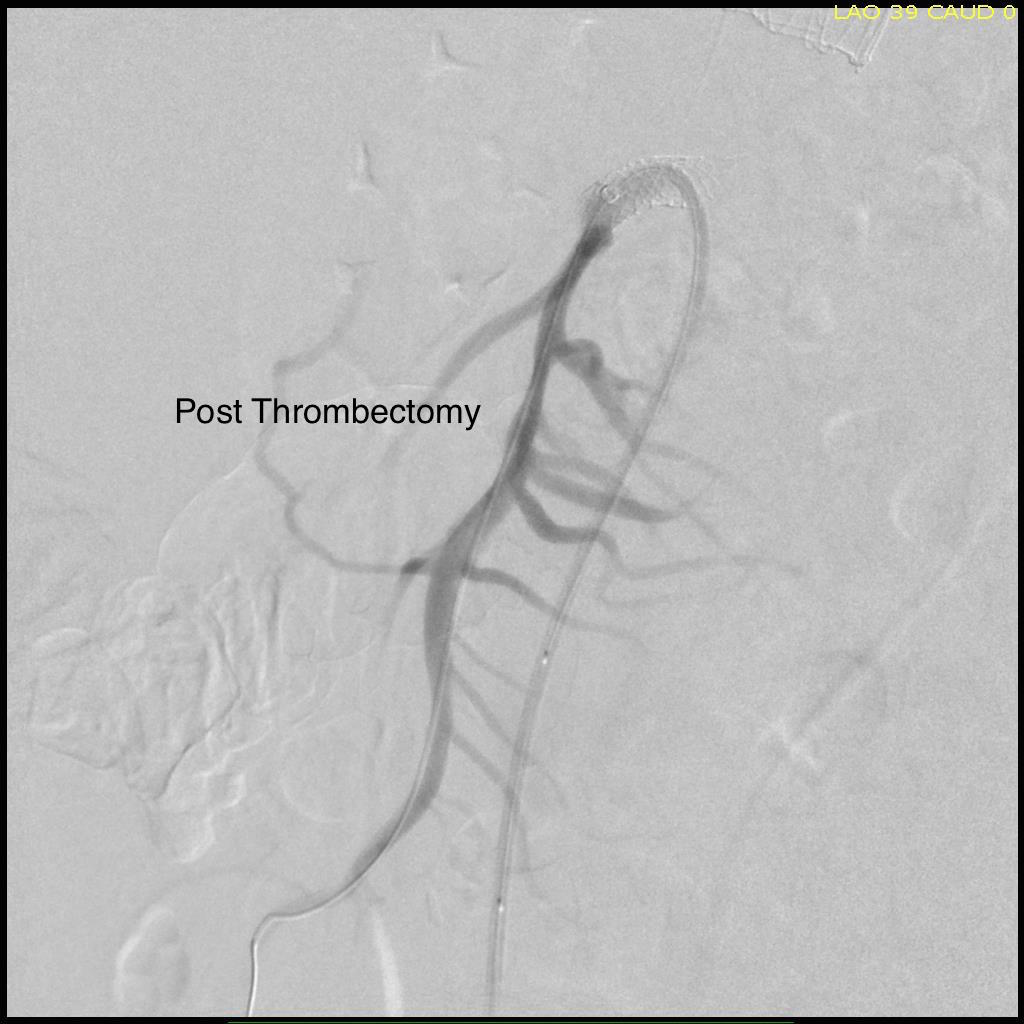
The completion arteriogram was satisfying.
The SMA completely filled as did the celiac axis and both renal arteries. I opted not to treat the right renal artery as we had given 250mL of contrast, and it was filling well without intervention. The patient was making excellent urine and his blood pressure had been maintained with mean arterial pressures above 70mmHg. At this point, IVUS confirmed good deployment of the stent.
The sheath was removed and the access site repaired. The general surgeons explored the patient and found all the bowel to be well perfused with pulsatile flows seen in the mesenteric arcade. The appendix was removed.
On waking, the patient was noted to not move his legs. A spinal drain was expertly placed by our cardiac anesthesia staff and his blood pressure was raised to MAP’s above 80. He recovered motor function in his legs soon after. I usually don’t place preop CSF drains in thisscenario in the presence of good pelvic circulation, no history of infrarenal aortic interventions, and patency of the left subclavian artery. That said, with TEVAR of TBAD, there is a small incidence of paraplegia (1-5%) which I emphasize in my preoperative discussion.
He was started on heparin anticoagulation postop because of his history of SMV and now SMA thrombosis, interrupting it briefly to remove the CSF drain. A CTA was obtained to confirm absence of bleeding showing obliteration of the dissection in the aorta and good patency through the true lumen of the SMA.
Most importantly, he had complete relief of his abdominal pain.
The treatment of acute mesenteric ischemia has greatly evolved since I presented my paper in 2002. While open revascularization remains a gold standard, it is becoming increasingly apparent that good to better results may be obtained with an endovascular approach. Dan Clair, our chair, has made the comment that early revascularization with endovascular technique is analogous to emergent PTCA in occlusions of the coronary system and that re-establishing flow is a critical first step.
Open exploration still is the mainstay of managing acute mesenteric ischemia, but laparoscopic exploration remains feasible. This patient underwent open conversion after an initial laparoscopic exploration to remove a ruptured retrocecal appendix that had been treated for over a month on antibiotics. Without bowel necrosis, a second look is usually unnecessary, but is critical when threatened bowel is left behind.
Reference
Park WM et al. J Vasc Surg. 2002 Mar;35(3):445-52.
This patient had developed metachronous common iliac artery aneurysms after aorto-bi-iliac graft placement of a AAA a decade ago. This is not infrequent occurence in a significant number of patients with aneurysmal degeneration seen in the thoracic or visceral segment abdominal aorta, iliac arteries, and popliteal arteries, years after a primary AAA repair. The patients are often older than they were at the original repair, with concomitant risk factors, and so a minimally invasive option is preferred.
Right CIAA -vulnerable tissue
The teaching during my fellowship was that aorto-iliac bypasses for aneurysmal disease were to be taken to the iliac bifurcation to go around vulnerable tissues. These tissues vulnerable to aneurysmal degeneration were infrarenal aorta up to the renal artery origins, common iliac and internal iliac arteries, and popliteal arteries. An anastomosis to the iliac bifurcation however normal appearing may degenerate given enough time. This patient developed a saccular aneurysm on the right iliac bifurcation and a small internal iliac artery aneurysm (1.5cm).
This was treated with coil embolization and stent graft from the right iliac limb to the external iliac artery.
This is the standard endovascular therapy for common iliac artery aneurysms, and acceptable in the setting of unilateral disease, and in a staged fashion has been considered acceptable for bilateral disease, acknowledging there is a 10-40% incidence of buttock claudication and when the contralateral hypogastric is occluded or when the patient is diabetic, the risk of buttock or colorectal necrosis is not insignificant. The patient had transiently some buttock claudication and hip and thigh neuralgia with walking but this improved in the weeks leading up to treating his left common iliac artery aneurysm.
Left CIAA
The left common iliac artery bifurcation is sometimes challenging to access from a midline incision and exposure requiring a separate sigmoid mobilization. In men, the narrow pelvis can increase the challenge, so it is without fault that sometimes common iliac artery is left behind. This is what became aneurysmal, developing into a 3.0cm fusiform aneurysm beyond the left limb of the graft.
The internal iliac artery had a moderate 50-75% stenosis at its origin but was not aneurysmal, and I chose to revascularize this. The patient was sexually active and walked for exercise. My options included proceeding with left hypogastric embolization and stent grafting, mirroring the right but with a significant risk for buttock claudication, sexual dysfunction, and a small risk for colorectal ischemia. Other option is an external iliac or common femoral to internal iliac artery bypass which is an excellent option in good risk patients.
Endovascular options
Iliac branched stent grafts are undergoing trial. My center is participating in both available industrial FDA approval trials (disclosure, I am site PI for the Gore trial), but this patient’s presentation and anatomy exclude him from the trials. The final option is placing a parallel stent grafts -one to the internal iliac artery and the other to the external iliac artery from a large common iliac stent graft. While not ideal, until branched grafts become available, this remains a viable option. The principle is to size the grafts to minimize potential gutters between the grafts, and have long seal zones to minimize the impact of the gutters. Access from two points is required to get two grafts into position. With the acute angle of the aortobi-iliac graft, up and over access is generally not possible. The 10mm Viabahn graft that I chose to place in the hypogastric requires a 12Fr sheath, which cannot be placed from the brachial artery, so I prepped for an axillary cutdown. The left common femoral access was percutaneous.
The left CFA access allowed placement of a 16mmx10cm Excluder iliac graft limb to cover the aneurysm down to the iliac bifurcation. The left axillary arterial cutdown access allowed placement of a 12Fr sheath (Flexor) to allow access of the left internal iliac artery and safe delivery of a 10mm Viabahn stent graft. The left external iliac artery was sealed with a 13mm Viabahn stent graft that was deployed simultaneously. Ballooning was performed to both.
Completion
No leak was seen. The axillary access was repaired directly and the CFA access was repaired with two Perclose S devices.
Discussion
Despite initial acceptance of bilateral hypogastric occlusion, even staged, it can be the cause of significant disability aside from buttock claudication, which sometimes does not remit with exercise. Ischemia of the pelvis can drive a plexopathy that can result in motor and sensory neuropathy and disability. Death can occur. Preserving one of the hypogastrics can go a long way to preventing these complications, and everyone eagerly awaits adding iliac branched grafts to the armamentarium.
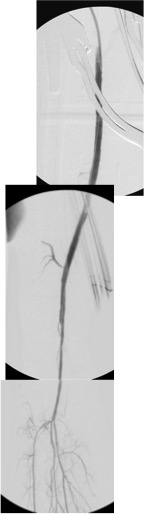
CTA on left shows occlusive plaque in SFA but contiguous plaque from external iliac origin into the popliteal artery. This was removed with EndoRE resulting in restoration of original artery patency -arteriogram on right. A single short stent was placed in the EIA origin and the above knee popliteal artery received a short stent as well.
This patient is a 90 plus year old man who developed ever worsening claudication to the point he was disabled and more worryingly, had developed pain over his left heel. His ABI’s were severely diminished.
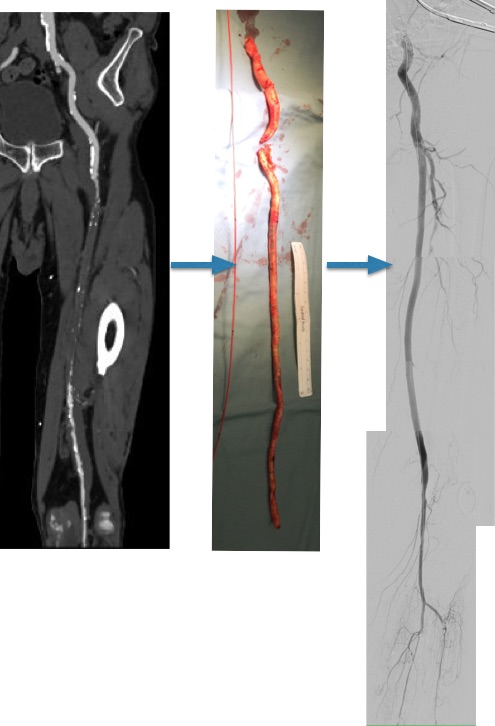
CTA showed that he had an occluded SFA with above knee reconstitute, but also had only single vessel runoff to the foot via a heavily diseased posterior tibial artery that had serial mild to moderate stenoses.
An attempt at endovascular recanalization was performed at an outside institution, but the SFA lesion could not be crossed. Bypass was not a good option -the ipsilateral saphenous vein had been harvested for CABG, and a long operation was going to have a significant impact on this patient who also had mild dementia and drank 2-3 glasses of wine a day. It is not uncommon to have a successful operation, but have the patient lose 2-3 months in recovering from the physical effects of a long operation as well as from perioperative delirium.
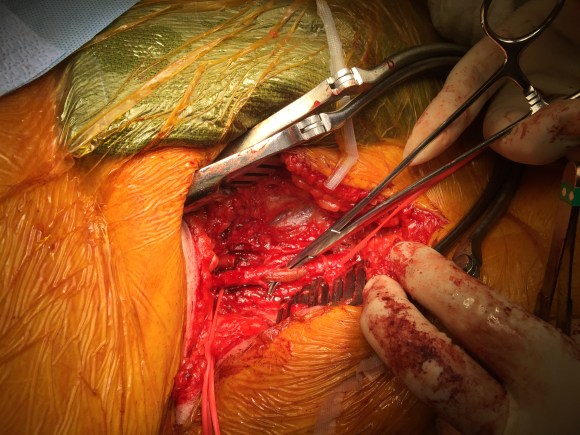
I felt that removing the occlusive plaque from his arteries offered a minimally invasive solution. The plaque was easily accessible via an oblique, skin line incision in the groin, and clearance could be performed from the external iliac artery origin to the planned endpoint slightly beyond Hunter’s canal. While the outflow was not perfect, in my experience, aside from a single native vein bypass, long segment restoration of vessel elasticity results in very acceptable patency rates.
Remote endarterectomy is a bit of a lost art from the early days of vascular surgery. A ring dissector (Vollmer Ring Dissector, LeMaitre Vascular) is used to liberate the plaque from the remnant adventia. A cutting device (Moll Ring Cutter, LeMaitre Vascular) shown third from left below is used to divide the plaque.
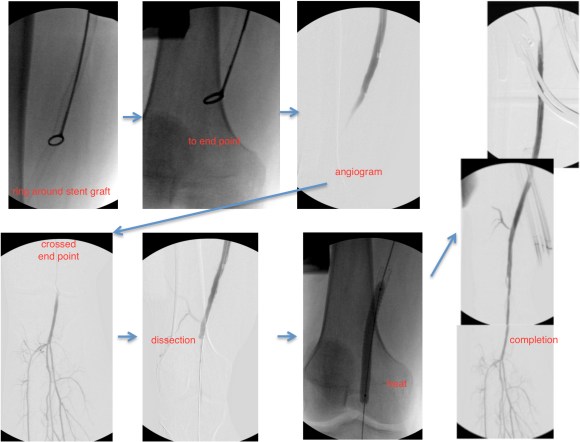
The common femoral artery plaque is usually contiguous with plaque in the external iliac artery and surgeons who perform a lot of CFA endarterectomy have various maneuvers to remove as much plaque as possible, up to stenting the end point of the plaque down to the endarterectomy patch. I have never been satisfied with this because the EIA behaves differenty than the CIA (am looking into this!) in my experience and placing stents even minimally across the inguinal ligament is not desirable. Sending the dissector up to the EIA origin frees the plaque to be removed completely with the CFA plaque. The clip below shows the Vollmer Ring dissecting plaque up to the EIA origin. I do this over a wire in the pelvis because in the rare instance of leak or rupture, rapid control is possible without having to open the abdomen.
Once freed, the cutter is used to transect the plaque and the end point is tacked down with a stent at the distal common iliac/EIA origin which is a better place for a stent than the inguinal ligament.
The PFA in this patient did not require endarterectomy and reconstruction, but if it did, I would have made the arteriotomy go onto the profunda from the CFA. The SFA plaque is then mobilized with the Vollmer ring. I don’t do this over a wire, but have a definite end point in mind based on what I see on CTA.
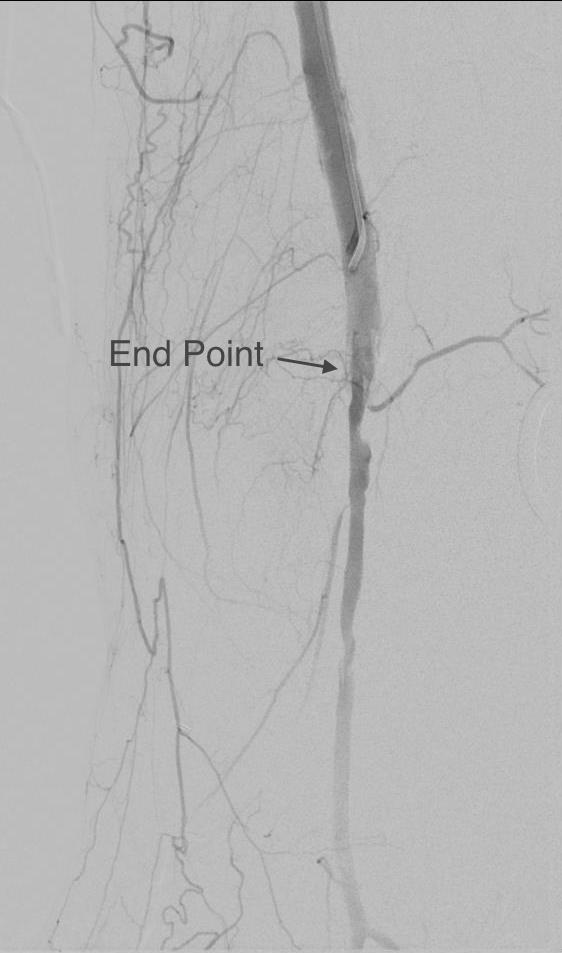
The CTA (images earlier) shows that the above knee popliteal artery has no significant calcified plaque. This doesn’t mean there isn’t fibrotic plaque. Cutting the plaque as in the clip below results in a coned in antegrade dissection which has to be crossed in the true lumen.
This is technically the most difficult part of the EndoRE procedure and it requires good imaging and wire skills. The trick here is that an ultrasound guided puncture of the popliteal or tibial vessel can give you distal true lumen access if needed. It was not necessary in this patient. The better maneuver is if the end point is surgically accessible is to cut down and tack down the plaque and patch the arteriotomy.
The patient regained multiphasic PT and DP signals at the end of the case, after the common femoral artery was patched and flow restored. The small groin incision was closed with a running absorbable monofilament after multilayer deep closure. The patient had a blood loss of 50mL. An ilioinguinal field block and local anesthesia provided excellent pain control. Postoperative ABI was improved to 0.82 from 0.34 and all pain was relieved. The patient felt good enough to go home on postoperative day 1.
This illustrates what I feel to be a best application of both open and endovascular techniques. The above knee popliteal stent is short and in a position that is not going to result in fracture. The external iliac stent is in a protected position in the pelvis and quite large -10mm, which I expect will stay open for the life of the patient. The profunda femoral artery, the rescue artery, is widely patent, and numerous collaterals off the SFA have been restored to patency which I feel aid in maintaining the patency of this repair, along with the restored elasticity of the artery which mimics the biomechanics of autologous vein.
In most patients with compromised outflow, I start warfarin along with ASA at 81mg. Because of his age, I opted for Plavix+ASA. These fail with the development of random TASC A restenoses along the SFA which are amenable to balloon angioplasty. The role of drug eluting balloons in this situation is unknown but theoretically promising. Occlusion through thrombosis does not result in embolization and limb loss as in failure of prosthetic bypass grafts (another option in this patient), but rather leaves a situation where endovascular thrombectomy or lysis is technically feasible.
The great thing is that this is by far superior to stenting of a TASC D femoral arterial lesion.











 The patient regained palpable pulses in his right foot and recovered well, being discharged home after a 4 day stay.
The patient regained palpable pulses in his right foot and recovered well, being discharged home after a 4 day stay.















 This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.