

At one time, I was performing below knee amputations in the same way that most textbooks prescribe. This patient presented with severe foot and leg infection with exposed tendons and cellulitis secondary to advanced diabetic neuropathy and arteriopathy. 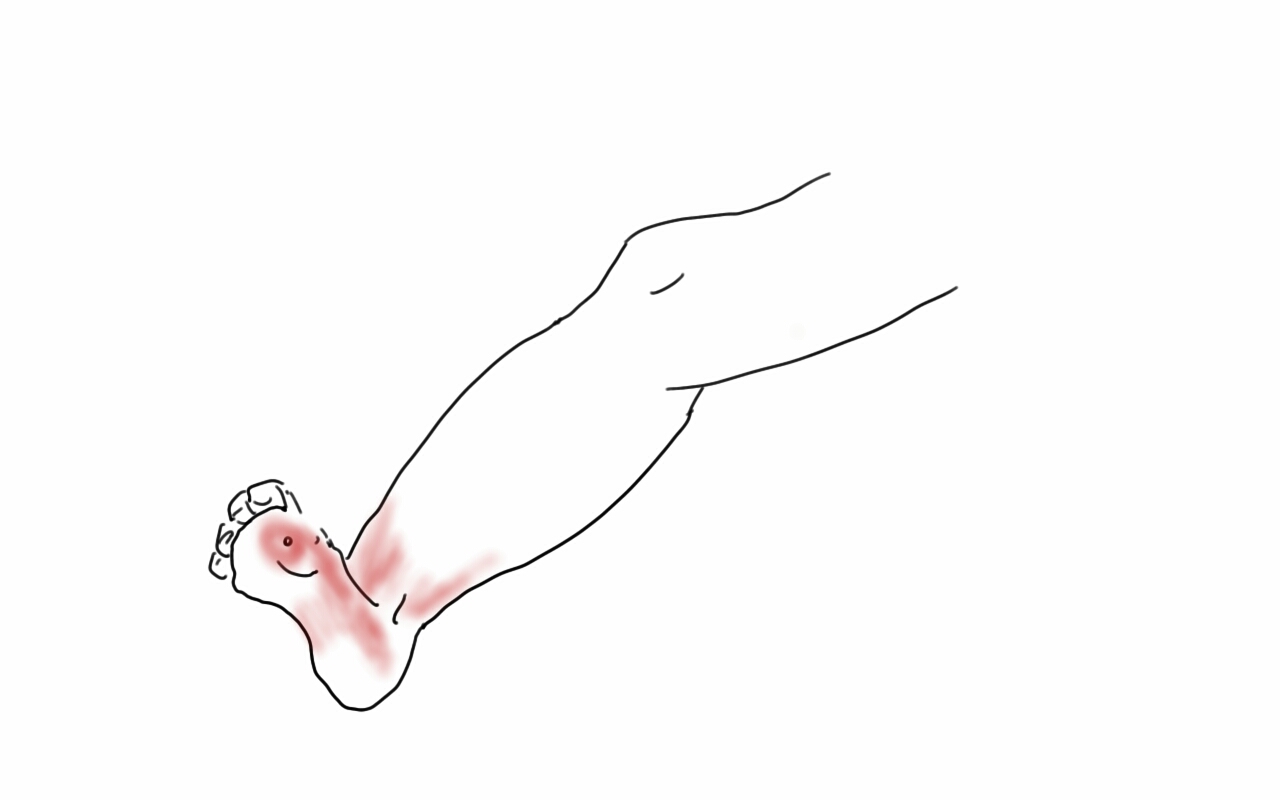
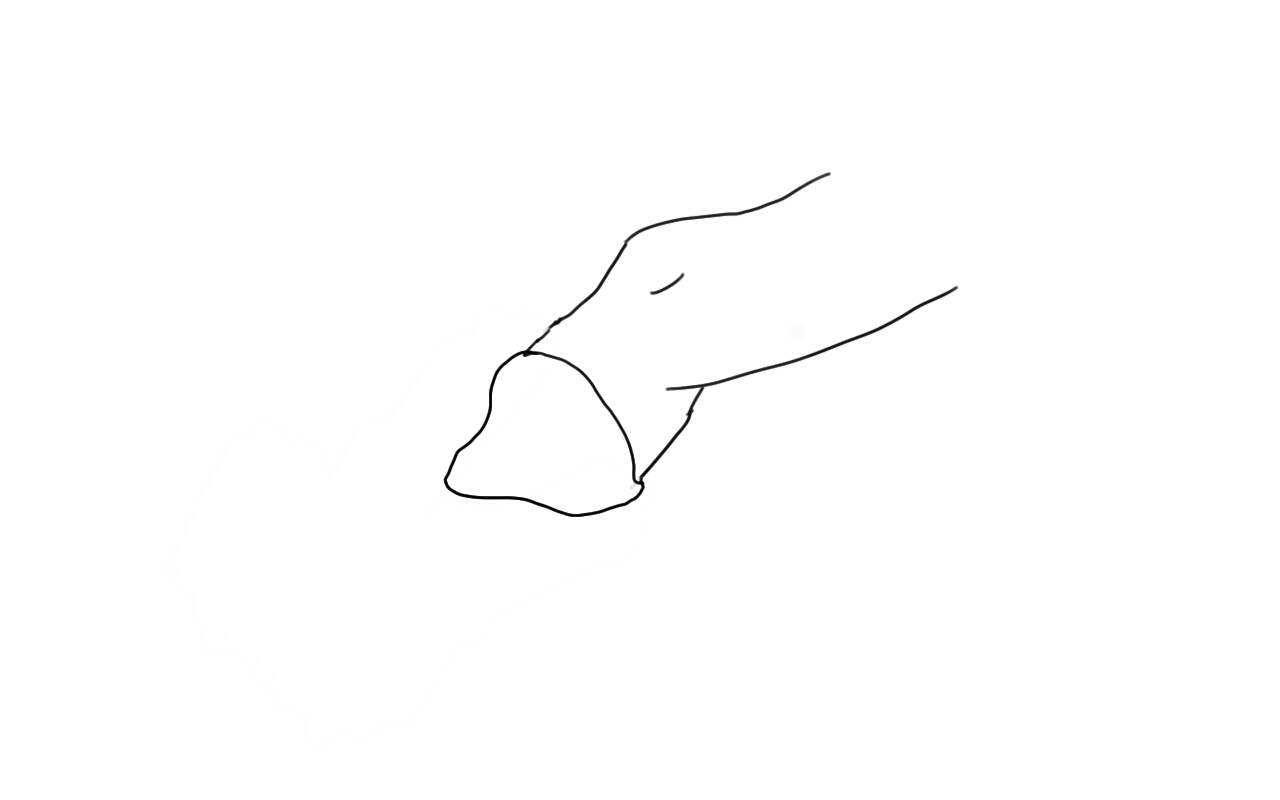
My sketch above showed the situation which we treated with two stage guillotine and final BKA. At the final stage, standard technique involves creating the classic flap shown below.

This is a tricky flap to make well because there are many variables -the amount of muscle left, the thickness of the subcutaneous fat, the vascular supply, etc. The biggest criticism I have of this flap is that it is prone to edema particularly in the meaty posterior flap, putting great stress on the skin sutures or staples. This then creates fat or skin necrosis in the posterior flap, or muscle necrosis resulting in wound infections and hospital readmissions, which are particularly at risk for need for further leg amputation in these patients with diabetes. I have to confess, while I could figure out how to cut the flap in the end, it was really hard to teach, and if it is hard to teach, you have to figure out a better way.
Here is the better way. The idea goes to the concept that the weight is borne in a distributive ring around the stump. The muscle on the tibia does not create a heel to bear weight on and so serves only the purpose of delivering blood to the overlying skin. So you only need the gastrocnemii and Achilles tendon for fascial closure, and maybe a little soleus. The elimination of posterior compartment muscle bulk greatly reduces the tension on the fascia and skin.
The incision can be simplified by cutting the flap along an oblique 2D plane -a light saber cut!
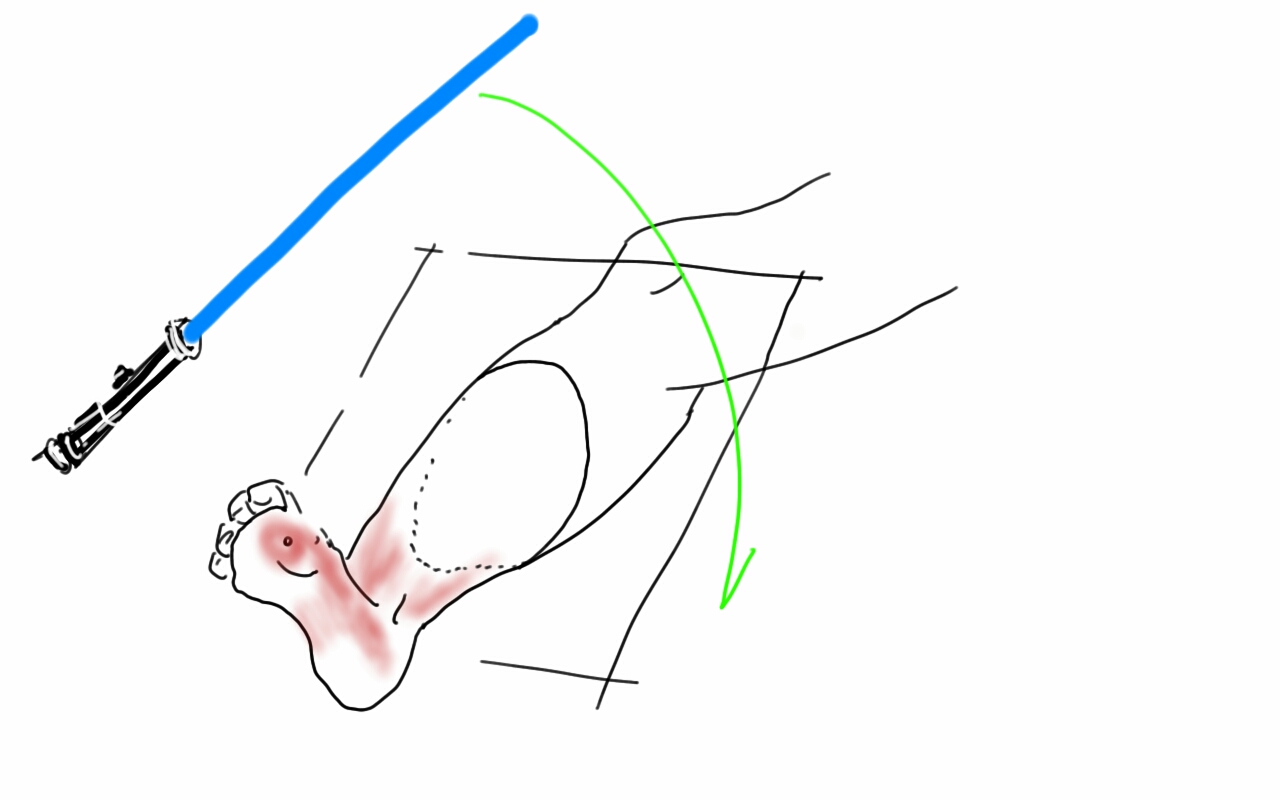
The posterior flap is reduced to just Achilles and a layer of soleus muscle, but otherwise, the internal bone and muscle organization is cut as below:

The skin at this point is never touched with a surgical instrument, only the subcutaneous later or fascia. Using interrupted absorbable heavy gauge monofilament (single strand of the double looped PDS used for abdominal closure is plenty of suture), interrupted buried sutures are placed in the fascia from middle outwards.
 This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
The skin is dress with a single layer of Xeroform and fluff gauze and gently a compressive dressing is applied from stump to above the knee, while keeping the knee cap exposed -the knee cap is prone to skin necrosis with ACE wraps that are left unattended.
The wound’s ability to heal is now largely a function of keeping the suture line tension and edema free. Edema is the great killer of these flaps and the problem with sutures or staples here is that edema creates zones of skin necrosis under these staples that then results in a postop wound breakdown and infection. With these simple steps largely copied from our plastic surgical confreres, I have been able to create very functional stumps with low morbidity.

This patient is 3 months from her 2 stage amputation and is walking on her prosthetic leg and is very happy. Notice, the dog ears have contracted!
