Recently, an AI was fed the world literature on AAA repair and asked about guidelines and superiority of open versus endo repair. It concluded that the past twenty year, endografting has only benefitted the physicians and the device companies (this was present at VEITH). I recommend open to patients likely to benefit from it. I recommend EVAR same way. They are not equivalent especially when patients end up getting insurance denials. I hope it isn’t too late to turn this boat around and train surgeons on open techniques that seem to have been abandoned in many parts of the world.
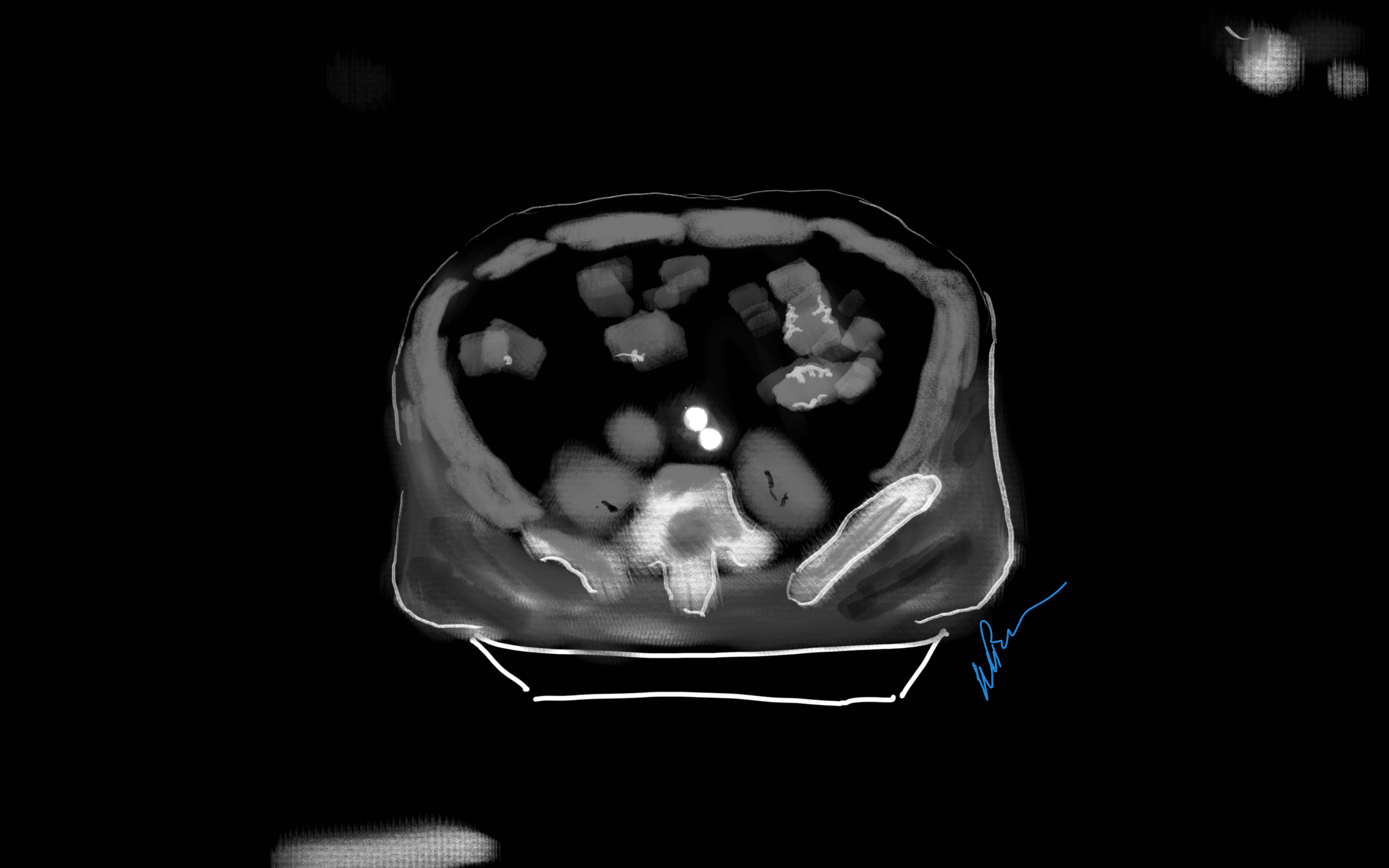
Look again, it is a doodle of a CT scan of a patient with an Ancure stent graft with sac shrinkage
I remember in the mid-2000’s, driving very fast to Lutheran Hospital in Des Moines on a Saturday night to fix an aneurysm that had ruptured. He was a man over 70 years of age with a type III endoleak from a component separation. The endografts had been placed by a cardiac surgeon who had taken some courses. I rescued him by open replacement of the aneurysm with a tube graft after I pulled out the endografts. Later, as the patient recovered, I asked him why he never followed up as required on his stent graft. His answer was, in typical Iowa farmer fashion, “Welp. If it was fixed, why should I?”
Indeed, why should he? Looking at his chart from the time of his EVAR, he was determined to be a “high risk” patient, necessitating the new minimally invasive procedure EVAR in 2003. Seeing that he survived the stress test of a ruptured aneurysm, it was clear he was not all that “high risk.” I did reassure him that with the open repair, he was basically cured. Despite scheduling a followup appointment, he never showed up. And that was okay.
EVAR is a treatment for AAA, but currently not a cure. All of the devices instructions for use stipulate the need for lifelong followup with CT scans with contrast and visits with qualified specialists. As I have mentioned in the past, what other condition requires surveillance CT scans with contrast and followup with a specialist? Cancer in remission. For those with good cardiac risk and functional status, placing an endograft rather than open repair creates “Aortic Aneurysm in Remission.” If they are in the majority of patients with a stable aneurysm sac, their endografts are sitting in a bag of static, aging blood. If there are type II endoleaks, and it is my belief that the majority of stable aneurysm sacs have some type II endoleaks that blinker on and off depending on the hemodynamics, particularly through needle holes, they are circulating the products of breakdown of that bag of old blood and exposing a perfect culture medium to potential inoculation. These type II and IV endoleaks can inflate the aortic sac over time. Occasionally, the residual AAA sacs rupture, erasing any of the early advantage conferred by the minimally invasive index procedure in long term followup EVAR v OPEN repair.
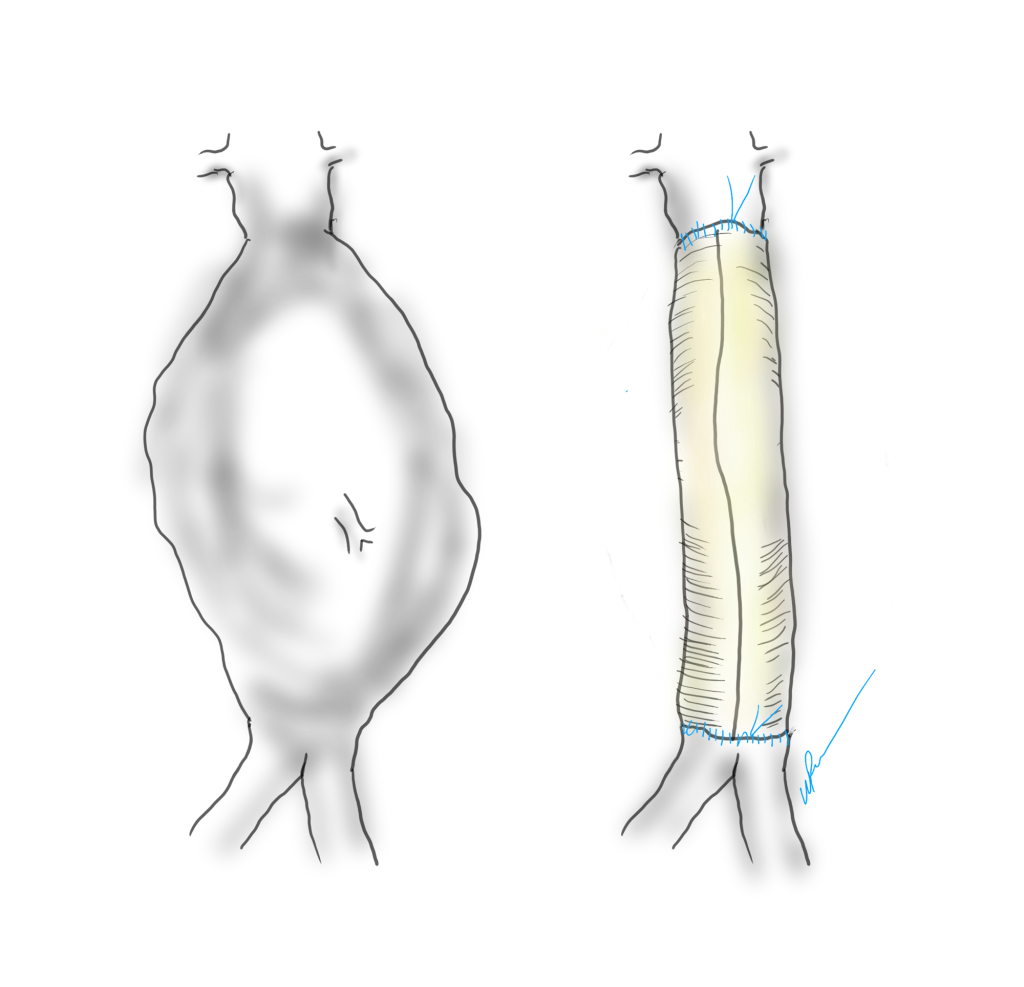
What is a cure? A cure is when you quell an infection with an antibiotic. A cure is when you’ve taken out an inflamed appendix. It’s when you’ve eradicated early stage cancer. It’s when you perform an open aortic graft and the patient can disappear after you remove the dressings and never followup, sure in the knowledge that the aneurysm in that spot will never bother them again. With EVAR, only a minority get to the state (figure at top) a sac shrunk intimately around the endograft. Most are not cured but enrolled in a regime of lifelong surveillance and maintenance.
EVAR does allow people to leave the hospital with less scarring and pain, but the consequences of its popularity are:
1. Letting more practitioners, not all of them vascular surgeons, treat aortic aneurysm disease with less training and with less or no ability to manage the inevitable failures surgically.
2. Creating the business model for “Advanced, Minimally Invasive, Super-Fantastic Aortic Centers of Excellence” which is predicated on the business of surveillance and maintenance of aortic endografts. It is a busy-ness that generates revenue, but burdens the country with more healthcare costs. It ultimately siphons business away from true centers of excellence involved in training the next generation of vascular surgeons.
3. Skewing the training curriculum of trainees to endovascular so much that I have met vascular surgeons who have done no aortic operations. That was the case when I sat in on an open aortic surgery class at the 2017 ESVS meeting in Lyons, France. All the attendees were very eager to try sewing anastomoses, but felt they needed proctoring which isn’t available.
4. Establishing the expectation that open aortic surgery is a failed, antiquarian, obsolete technique to be relegated to the history books. This last one is infuriating and not true but it is out there in the claims of the aorticians.
5. Resulting in palliation when the aortic aneurysm in remission ruptures and there are no readily available open-capable surgeons experienced in rescuing these patients. This happens. Don’t let it happen to you.
Various solutions have been broached including regionalization of aortic aneurysm care, superfellowships in exovascular surgery to complement the widespread endovascular training, and going back to open aortic surgery as the norm as had been proposed controversially in the UK. There is no turning back the clock. The moment that Dr. Parodi combined an aortic graft with Dr. Palmaz’s stent, a quantum leap occurred. The operation of aortic aneurysm surgery was changed from a challenging operation mastered by a few to a straightforward procedure performed by many.
Interesting to me is that illustration at the top of the post is of a common observation – the obliteration of the aortic aneurysm sac around a Guidant Ancure stent graft. When the sac disappears, it is as close to a cure that you can get. For some reason, I see this more frequently with Ancure than with other grafts over the past twenty years.
Odd fact -I may have been the last surgeon to implant an Ancure in the world. In 2003, I was treating a AAA with an Ancure graft when the delivery system froze in mid deployment. I called Dr. Dan Clair away from some meeting, and he called for pliers, screw drivers, and a saw, and after deconstructing the delivery system, deployed the graft and returned to his meeting with nary a word. The Guidant rep, who had been on the phone, looked up with saucer eyes, and said, “Wow. They’ve pulled Ancure off the market.”
I think it is because of the design, which is now off the market. When stents are sewn to cloth, the needle holes leak, and leak particularly where the stent graft makes a turn, stretching the suture hole. Junctions and seams leak. The Ancure, aside from the stents at top and bottom in the seal zone, has no such holes as it is unsupported and manufactured as a single piece with no junctions or seams. It is the closest you get to sewing in a graft by open surgery. If it weren’t for its overly complicated delivery system which was its downfall, I think it would be in its third generation with visceral branches that are created off the textile machines rather than joined inside the patient. There are lessons to be learned from this abandoned tech.
I believe a treat once and walk-away cure is achievable in EVAR. The idea is not to be satisfied with anything less than a cure, anything that ends with aortic aneurysm in remission. We have to understand we have chosen a path of iteration and continuous but slow improvement in the EVAR space. The front end benefits of EVAR are clear but it is in the long term we have to focus. Until then, warranties would be great.
The Long of It and the Short, or What You Are Trying to Do With That Level 82 Note on Your EMR?
I struggle to keep my sanity reading through electronic medical records. Medical billing pays by the amount of note written. Back in the 90’s, the insurance companies demanded that paper records be sent by mail or fax to confirm billing. Clerks in medical records departments would spend the whole day copying and faxing stacks of charts to payers and billers. EMRs were suppose to solve this, but the paradigm of the paper record lives on. Each note in the EMR is printable as a paper record for billing. It is a static text document. And like in the 90’s, billing is based on the amount of note written into the EMR. The simplest way to achieve this is to copy and paste what already exists elsewhere in the EMR -a past note, a systems review, a medical history, a spreadsheet of lab results, imaging reports. This gets you more note, more billing. The electronic medical record succeeds in its primary function as a cardboard box of copied records and as a cash register, but fails miserably in being an active part of patient care.
Any sane system would allow you to pick links to prior notes or tests -a referencing system to include even published articles, to show your logic and data, while allowing you to focus on the information that is important at the moment. The modern note needs to be turned into a searchable, linkable, living element in a dynamic database reflecting the patient’s status, a powerful tool in the patient’s care. There needs to be an App Store where third party vendors can craft solutions not imagined by the EMR. There needs to be a common file format to allow for interoperability and easy transfer of records between institutions -like JPGs and MPGs. There needs to be a complete re-engineering of the user interface. The various caregivers interacting with the EMR need to be allowed to input data in non-linear ways using mobile devices. The EMR needs to evolve to being a platform.
The Blue Ink
When I was a fellow in 2000, one of my staff, Ken Cherry, had this distinct light blue ink in his fountain pen that he wrote notes with in pithy, grammatically correct sentences conveying the diagnosis and plan. It was up to me, his fellow, to write the more detailed note, but there at the bottom, in a sky blue cursive fit for the Declaration of Independence, was the word. You just had to look for that ink in the chart to understand where the patient was and where he was going. He’d write something like, “This patient, who was seen in clinic with classic Leriche Syndrome, is now admitted with rest pain in his right foot. I intend to revascularize him after appropriate workup. My fellow will make these arrangements.” Stylistically, it was wonderful, but assumed a lot of contextual knowledge about Leriche Syndrome, and if you didn’t know, you could read Park’s two page note. He’s making the arrangements.
Compare that to an imaginary level 19 note (won’t burden you with it), rotten with copy pasted operative note and prior discharge summary, spreadsheet of laboratory values, and 12 system review of systems, 12 organ system examination, and multiparty listing of every organ in impression, bullet pointed plan, never mind that many of these have no relationship to the problem at hand. The first note is a financial disaster as it cannot be maximally billed, but it is full of meaning and action. The second note is unreadable and therefore likely unread. Like those strange tropical fruits that take power tools to get to a small bit of sweet at the center, the level 23 notes littering electronic medical records take time to pore over the chaff to get to the point which is often hidden -day to day only a few things may actually change on a note. There is just too much husk. Most of the action, the orders, have to be typed back into the note rather than automatically populating it. Supposedly, that function exists but the software has been written with the user interface of Windows from the early 1990’s and the functions are buried, only to be fished out by superusers and support staff that take time away from clinical duties to read about and learn.
Context Implied and Explicit
The fashioning of a good note recognizes that too much implied context results in confusion. Rather than say, “Leriche Syndrome,” one should say, “aortoiliac occlusive disease from advanced atherosclerosis resulting in a symptom complex of severe claudication known by the moniker, Leriche Syndrome.” The note needs to educate as much as it does document. The exposition of expertise needs to be explicit for the note to show value. Value and bill-ability do not live on the same axis. The reader should come away from the note with maximal meaning in the shortest amount of time. That means most consult notes and H&P’s need to be ideally case studies and earn their length and perform a teaching function.
Copy/Paste -Note as EMR Fractal
The position of the average physician is a poor one. The need to bill means writing long notes, but physically typing and formatting long notes is a drudgery that occupies a significant time away from seeing patients, performing procedures on patients, and thinking. The easy solution to this dilemma, the lack of time, is the Copy/Paste. There are notes where the entirety of past notes is copy pasted, creating a self-repeating element like a fractal where the entire EMR is reflected in the note. Like error mutations of the genes that persist and damage organisms, copying and pasting of documentation errors perpetuates itself and can cause disease. I remember years ago as a young staff being stuck by a needle during a procedure and dying a little inside when I checked the chart and found the patient was HIV positive. When I talked to the patient, I found out that was a persistent error, manually copied and pasted by residents and consultants, billed as a diagnosis, resulting in years of problems for the patient who had to threaten lawsuits to expunge that HIV status. Each note should be unique and uniquely authored by the caregiver, and if there is not much to report, necessarily brief. A daily summary should be generatable like those news apps that can scrape headlines and context out of the day’s production from the internet and present it to you in a easy to consume quadrilateral of data.
The Shield -Speaking to the Jury
A proper note will protect you. It is the only shield that protects you along with your education and reputation. Civil proceedings involve going over these notes in great detail and the notes should be either unimpeachably explicit or vague like a fortune cookie. Even the limited tech of current EMRs allows you to achieve granular levels of detail. I recommend referencing (but not copy/pasting) important societal guidelines and journal articles that reflect your thinking, but it the EMR does not make this easy. The hack is keeping these references as a macro to spew out relevant text. For example, if you chose not to operate on a 5.4cm AAA, after referencing the CT scan report, an image showing your measuring line, and the growth velocity from prior scans if available, a line reference to the SVS guidelines spat out by a macro gives you some shielding. But more important, in the ideal EMR, that reference would be that characteristic blue color of a hypertext link to the pubmed reference or PDF download. Hyperlinks within EMRs should be a thing. Your EMR note should be a hypertext document, not a text document, and allow referencing other notes and reports without copy/pasting them. Images, audio, and video should live within your EMR note as naturally as they do in every other document you create in 2020 that does not have to be excreted through a printer. The fact that these functions are extraneous to the primary function of the EMR -to be cheap to produce and maintain, and good for billing, means no innovation will occur for EMRs.
The Platform
EMRs vendors cling to their market share by making sharing of data impossible through proprietary data formats and security regimes. Health care systems have no incentive to make their patient information transferable beyond a minimum of paper or their PDF equivalent. Patient safety and information security is invoked for preventing needed innovation. For the patient, this can be a life or death issue -the ability to transfer health care data. Imagine if you are the patient with a ruptured aortic aneurysm who is transferred without the CT scan burned to a CD. In 2020, NO.ONE.USES.CD’s. I can download a 4K file of the last Avenger’s movie in 30 seconds on the right network, but a lifesaving CT scan -NO WAY!
A more everyday example is a patient seeking a second opinion or moving cities to a different health care system. The only way to move the data is an expensive printout of the chart. How can we keep this important information linked with the patient? Social media has cracked this. Your Facebook is a good model of what a potential EMR 2.0 could be. A patient-centric EMR would be controlled by the patient in terms of access control. Federal laws would prevent misbehavior by the EMR vendor. The patient’s data generated by practices or hospitals would be owned by these practices or hospitals but posted on the patient’s EMR, in specific specialty adapted formats. Temporal ordering would be natural, not based on shuffling reams of paper or virtually with PDFs with overlapping timelines. More importantly, imaging data and lab results would be immediately available to all healthcare providers through access to the patient’s EMR. Practices and hospitals would pay a nominal fee to the EMR provider much as advertisers are on Facebook. Patients would be in control of who gets access to the data, and importantly if they want to participate in research. App developers would proliferate and innovate in the space, providing functionality via apps in a marketplace, allowing different specialists look at the data in their own particular way, and patients to understand their data on their own terms. Gaming companies, for example, could take the virtual coordinates of a CT scan and match it up with ultrasound and MRI to do a lot of cool stuff. EMR 2.0 is not more ways to personalize your window with colorful graphics. EMR 2.0 is a complete upending of the way patient data is stored and moved, and it will take an act of Congress to make this happen. EMR 2.0 recognizes that it needs to become a platform and it needs to be a part of a collective national effort. EMR 2.0 needs to be a platform, not an app.
A Multimedia EMR
The EMR needs to incorporate multimedia. Current EMRs live in the tech levels of the early 1990’s. Imaging studies must live as actual windows in chart notes. Video or voice comments must be documentable in the chart. Hypertext to the resources of the internet must live in the chart. Data must flow just like blood.
This should suffice as an op note
Shape of the Future
As a vascular surgeon, the most important function is to provide an accurate documentation of the condition of the blood vessels to date, the current condition of the blood vessels, and the future fate of the blood vessels and the patient. Technology needs to help the vascular surgeon in this role, and most importantly, the patient. Tech is not a third party vendor in this battle space. Tech is a caregiver, and must be held to the same standards placed on physicians, nurses, and technicians. Until that day comes, we as vascular surgeons must write amazing, publishable case reports for the consult notes, and short pithy updates for the subsequent notes.