
A nationwide analysis of median arcuate ligament release between 2010 and 2020: a NSQIP Study
— Read on link.springer.com/epdf/10.1007/s00464-022-09431-3
Tag: #vascsurg
I remember in the mid-2000’s, driving very fast to Lutheran Hospital in Des Moines on a Saturday night to fix an aneurysm that had ruptured. He was a man over 70 years of age with a type III endoleak from a component separation. The endografts had been placed by a cardiac surgeon who had taken some courses. I rescued him by open replacement of the aneurysm with a tube graft after I pulled out the endografts. Later, as the patient recovered, I asked him why he never followed up as required on his stent graft. His answer was, in typical Iowa farmer fashion, “Welp. If it was fixed, why should I?”
Indeed, why should he? Looking at his chart from the time of his EVAR, he was determined to be a “high risk” patient, necessitating the new minimally invasive procedure EVAR in 2003. Seeing that he survived the stress test of a ruptured aneurysm, it was clear he was not all that “high risk.” I did reassure him that with the open repair, he was basically cured. Despite scheduling a followup appointment, he never showed up. And that was okay.
EVAR is a treatment for AAA, but currently not a cure. All of the devices instructions for use stipulate the need for lifelong followup with CT scans with contrast and visits with qualified specialists. As I have mentioned in the past, what other condition requires surveillance CT scans with contrast and followup with a specialist? Cancer in remission. For those with good cardiac risk and functional status, placing an endograft rather than open repair creates “Aortic Aneurysm in Remission.” If they are in the majority of patients with a stable aneurysm sac, their endografts are sitting in a bag of static, aging blood. If there are type II endoleaks, and it is my belief that the majority of stable aneurysm sacs have some type II endoleaks that blinker on and off depending on the hemodynamics, particularly through needle holes, they are circulating the products of breakdown of that bag of old blood and exposing a perfect culture medium to potential inoculation. These type II and IV endoleaks can inflate the aortic sac over time. Occasionally, the residual AAA sacs rupture, erasing any of the early advantage conferred by the minimally invasive index procedure in long term followup EVAR v OPEN repair.
What is a cure? A cure is when you quell an infection with an antibiotic. A cure is when you’ve taken out an inflamed appendix. It’s when you’ve eradicated early stage cancer. It’s when you perform an open aortic graft and the patient can disappear after you remove the dressings and never followup, sure in the knowledge that the aneurysm in that spot will never bother them again. With EVAR, only a minority get to the state (figure at top) a sac shrunk intimately around the endograft. Most are not cured but enrolled in a regime of lifelong surveillance and maintenance.
EVAR does allow people to leave the hospital with less scarring and pain, but the consequences of its popularity are:
1. Letting more practitioners, not all of them vascular surgeons, treat aortic aneurysm disease with less training and with less or no ability to manage the inevitable failures surgically.
2. Creating the business model for “Advanced, Minimally Invasive, Super-Fantastic Aortic Centers of Excellence” which is predicated on the business of surveillance and maintenance of aortic endografts. It is a busy-ness that generates revenue, but burdens the country with more healthcare costs. It ultimately siphons business away from true centers of excellence involved in training the next generation of vascular surgeons.
3. Skewing the training curriculum of trainees to endovascular so much that I have met vascular surgeons who have done no aortic operations. That was the case when I sat in on an open aortic surgery class at the 2017 ESVS meeting in Lyons, France. All the attendees were very eager to try sewing anastomoses, but felt they needed proctoring which isn’t available.
4. Establishing the expectation that open aortic surgery is a failed, antiquarian, obsolete technique to be relegated to the history books. This last one is infuriating and not true but it is out there in the claims of the aorticians.
5. Resulting in palliation when the aortic aneurysm in remission ruptures and there are no readily available open-capable surgeons experienced in rescuing these patients. This happens. Don’t let it happen to you.
Various solutions have been broached including regionalization of aortic aneurysm care, superfellowships in exovascular surgery to complement the widespread endovascular training, and going back to open aortic surgery as the norm as had been proposed controversially in the UK. There is no turning back the clock. The moment that Dr. Parodi combined an aortic graft with Dr. Palmaz’s stent, a quantum leap occurred. The operation of aortic aneurysm surgery was changed from a challenging operation mastered by a few to a straightforward procedure performed by many.
Interesting to me is that illustration at the top of the post is of a common observation – the obliteration of the aortic aneurysm sac around a Guidant Ancure stent graft. When the sac disappears, it is as close to a cure that you can get. For some reason, I see this more frequently with Ancure than with other grafts over the past twenty years.
Odd fact -I may have been the last surgeon to implant an Ancure in the world. In 2003, I was treating a AAA with an Ancure graft when the delivery system froze in mid deployment. I called Dr. Dan Clair away from some meeting, and he called for pliers, screw drivers, and a saw, and after deconstructing the delivery system, deployed the graft and returned to his meeting with nary a word. The Guidant rep, who had been on the phone, looked up with saucer eyes, and said, “Wow. They’ve pulled Ancure off the market.”
I think it is because of the design, which is now off the market. When stents are sewn to cloth, the needle holes leak, and leak particularly where the stent graft makes a turn, stretching the suture hole. Junctions and seams leak. The Ancure, aside from the stents at top and bottom in the seal zone, has no such holes as it is unsupported and manufactured as a single piece with no junctions or seams. It is the closest you get to sewing in a graft by open surgery. If it weren’t for its overly complicated delivery system which was its downfall, I think it would be in its third generation with visceral branches that are created off the textile machines rather than joined inside the patient. There are lessons to be learned from this abandoned tech.
I believe a treat once and walk-away cure is achievable in EVAR. The idea is not to be satisfied with anything less than a cure, anything that ends with aortic aneurysm in remission. We have to understand we have chosen a path of iteration and continuous but slow improvement in the EVAR space. The front end benefits of EVAR are clear but it is in the long term we have to focus. Until then, warranties would be great.
The patient was a 50 something year old man who I took care of in 2016 before I left for Abu Dhabi. He had a background of hypertension, hypercholesterolemia, and IDDM with chronic immunosuppression for rheumatoid arthritis. For several weeks he had rest pain in his feet and impending gangrene of his left great toe. More worrisome was the development of punched out ulcers on his groin crease resulting in weeping wounds after a bout of cellulitis. He had no palpable femoral pulses. Pulse volume recordings showed flat lines from the thigh to the feet.

CTA of the abdomen and pelvis with runoff showed aortic occlusion due to heavily calcified plaque with reconstitution of the external iliac arteries via the internal iliac arteries. The common femoral arteries were only mildly diseased and there was patent runoff.


He was one of the rare instances of chronic limb threatening ischemia due to aortoiliac occlusive disease, AKA Leriche syndrome. The added background of autoimmunity made him vulnerable to the ulcers in the groin crease, and the infections there made access challenging.

The choices were endovascular versus open surgical repair. The groins were a problem with recent cellulitis, immunosuppression and open wounds, but with careful prep, and coverage with Ioban, access was possible, even for stent grafting. The problem was the aortic bifurcation was heavily calcified, and manipulating this likely thrombotic material with an end stump of aorta can cause renal embolism. There was a small risk of rupture at the bifurcation and of renal failure.
Standard aortobifemoral bypass graft was out of the question because of the lack of a safely clampable aorta -there was circumferential aortic plaque below and above the renal arteries and the infections in the groins would jeopardize any prosthetic graft. You have to respect unclampable aortas but like anything else, there are ways around it (link).
Regarding the groins, during fellowship, Dr. Thomas Bower used to take the distal anastomoses to the external iliac arteries which could be exposed via short lower abdominal incisions if not through the midline incision itself, avoiding groin incisions in hazardous groins.
I performed an aorto-bi-iliac bypass using the balloon in the infrarenal technique after obtaining supraceliac control described in my technical post (link).

I was able to endarterectomize a nice segment of aorta and anastomose end to side -always end to side as it preserves endovascular options. The distal anastomoses was to the external iliac arteries. He did well in the immediate postoperative period but I soon left for Abu Dhabi.
In the five years since the operation, he has needed an SMA stent and has devloped worsening CKD and autoimmune diseases. But one of the gratifying things is he healed his wounds on this groins and thighs and the left hallux, and pain has never recurred. He had a contrast CT at the 5 year point (figure) showing a widely patent graft, and he sought me out when he heard that I was back in Cleveland.

His PVRs remain normal (figure).

I’m not saying that iliac stents from the iliac bifurcation to the renal arteries was a bad option, but there is a particular sadness and weariness when I have to take care of occluded stents. As an engineer, what is worse than ballooning an occluded stent and placing another stent inside? Knowing what I know about cell biology, what is worse than lasering, drilling, cutting, that cicatricial scar tissue that is neointimal hyperplasia in terms of what you leave behind. This man still has decades left to live and he will have his bypass graft far longer than any stent. This durability, a byproduct of the technique, is a worthy virtue.
When I operated, he was in his mid fifties and despite his comorbidities, was able to undergo a big operation. Now he is in his sixties and his autoimmune issues have progressed to where he is suffering from stiff person syndrome with difficulty walking. His renal function is poor and overall he is a terrible open surgical candidate. If I had done interventions at that time, which I was tempted to, he could today be facing amputations in the setting of cytotoxic immunosuppression having run out of endovascular options.
We have lost too much to innovation. The fact is, aortic surgery for critical limb ischemia was once and it still is a thing, because it works.
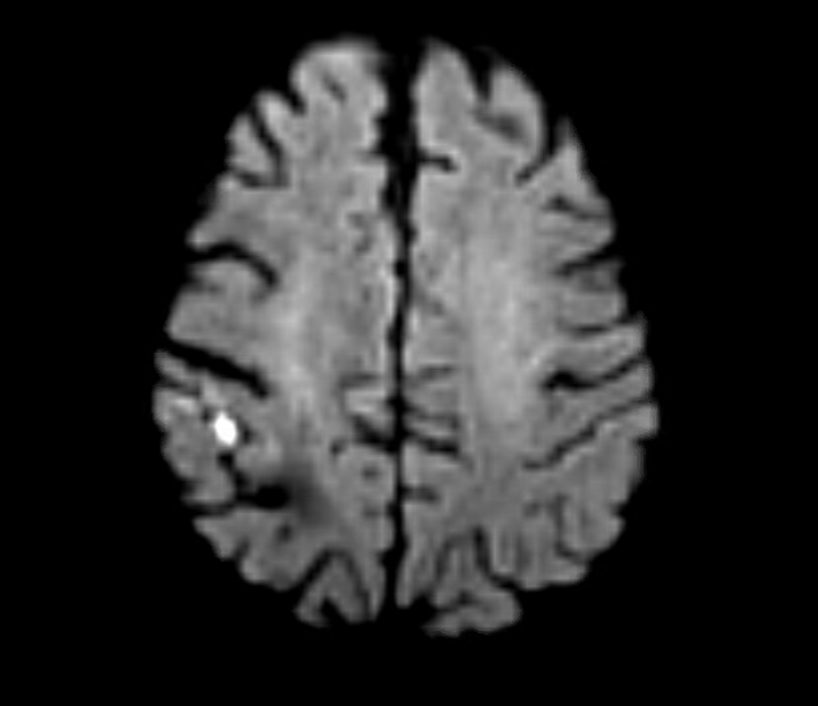
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
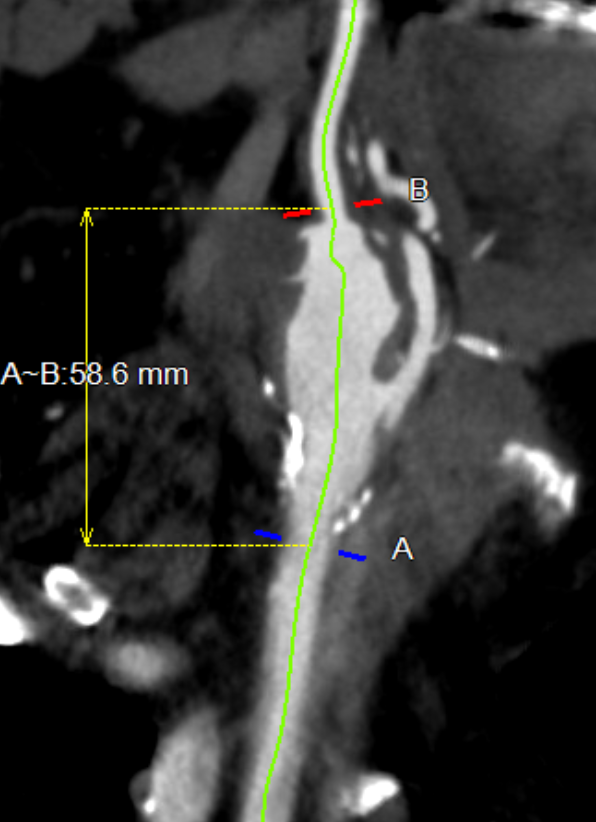
This was seen dramatically on carotid duplex below.

He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
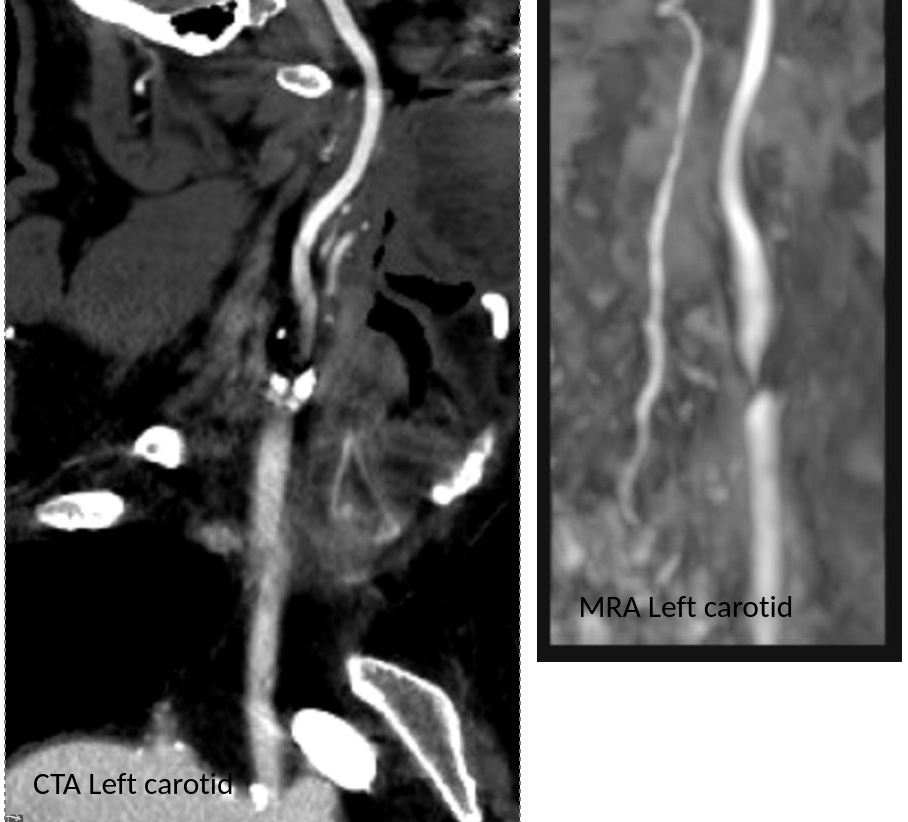
MRI confirmed a right hemispheric infarction and operation was planned.
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.

The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.

Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
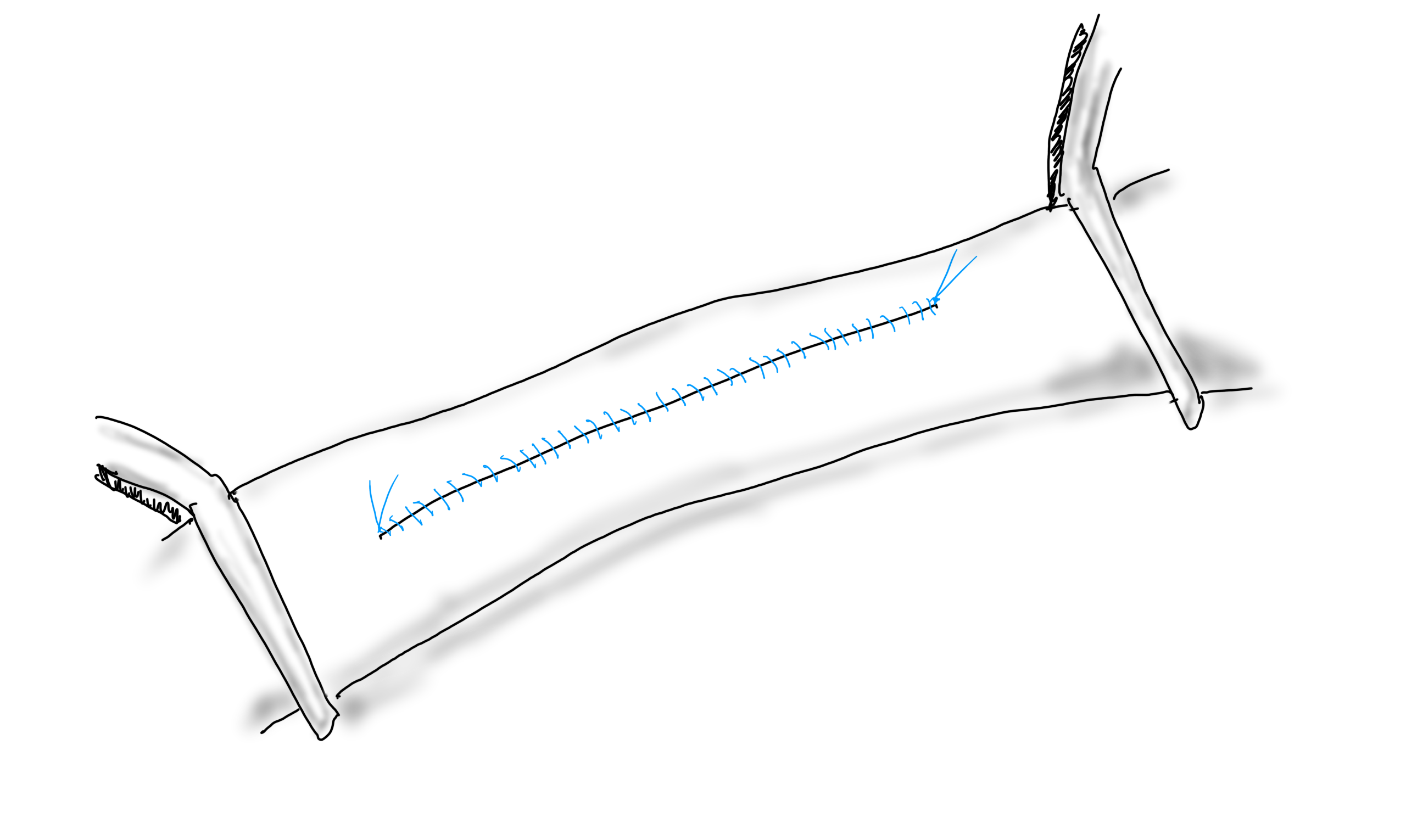
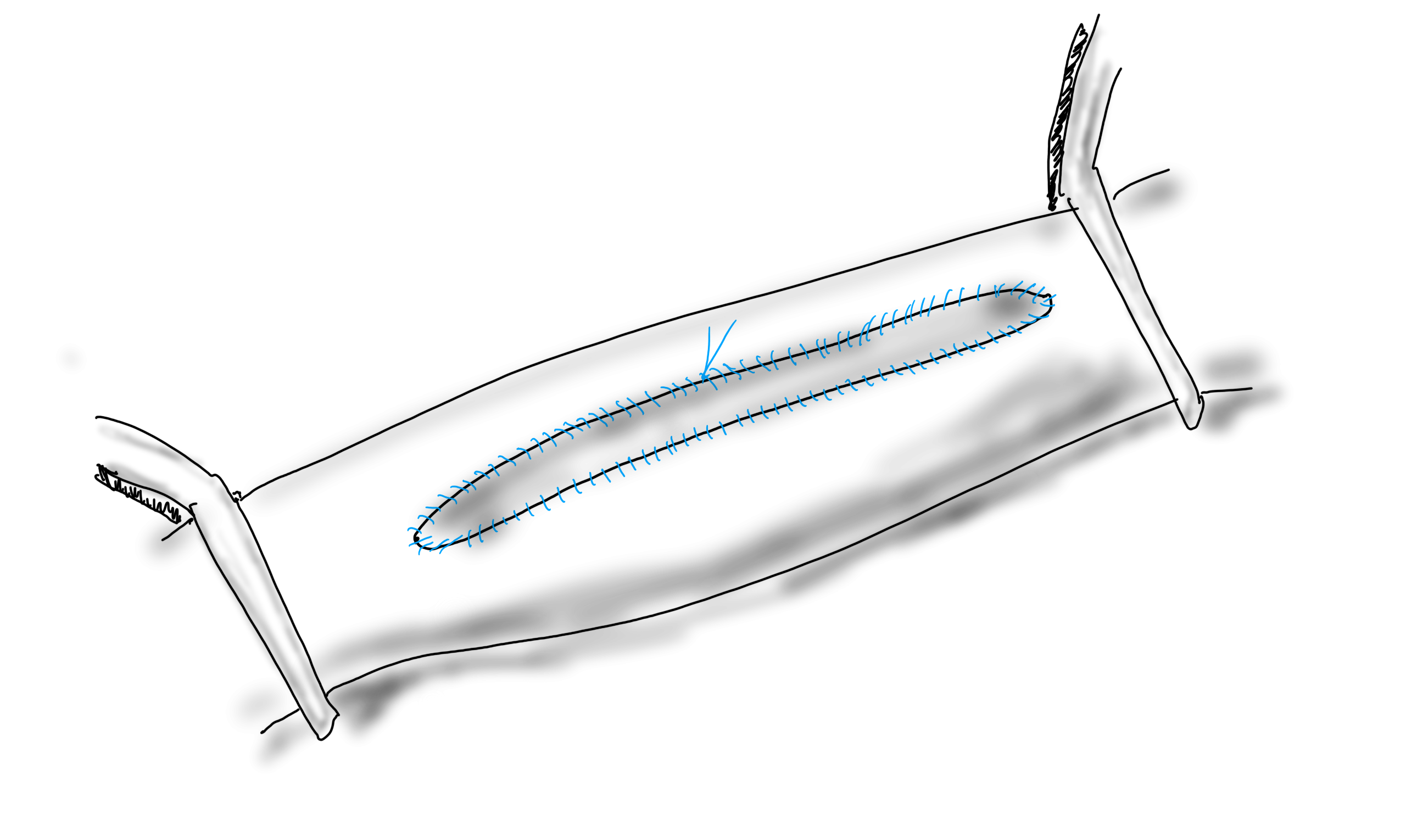
When you open an artery, you eventually have to close it (figure1).
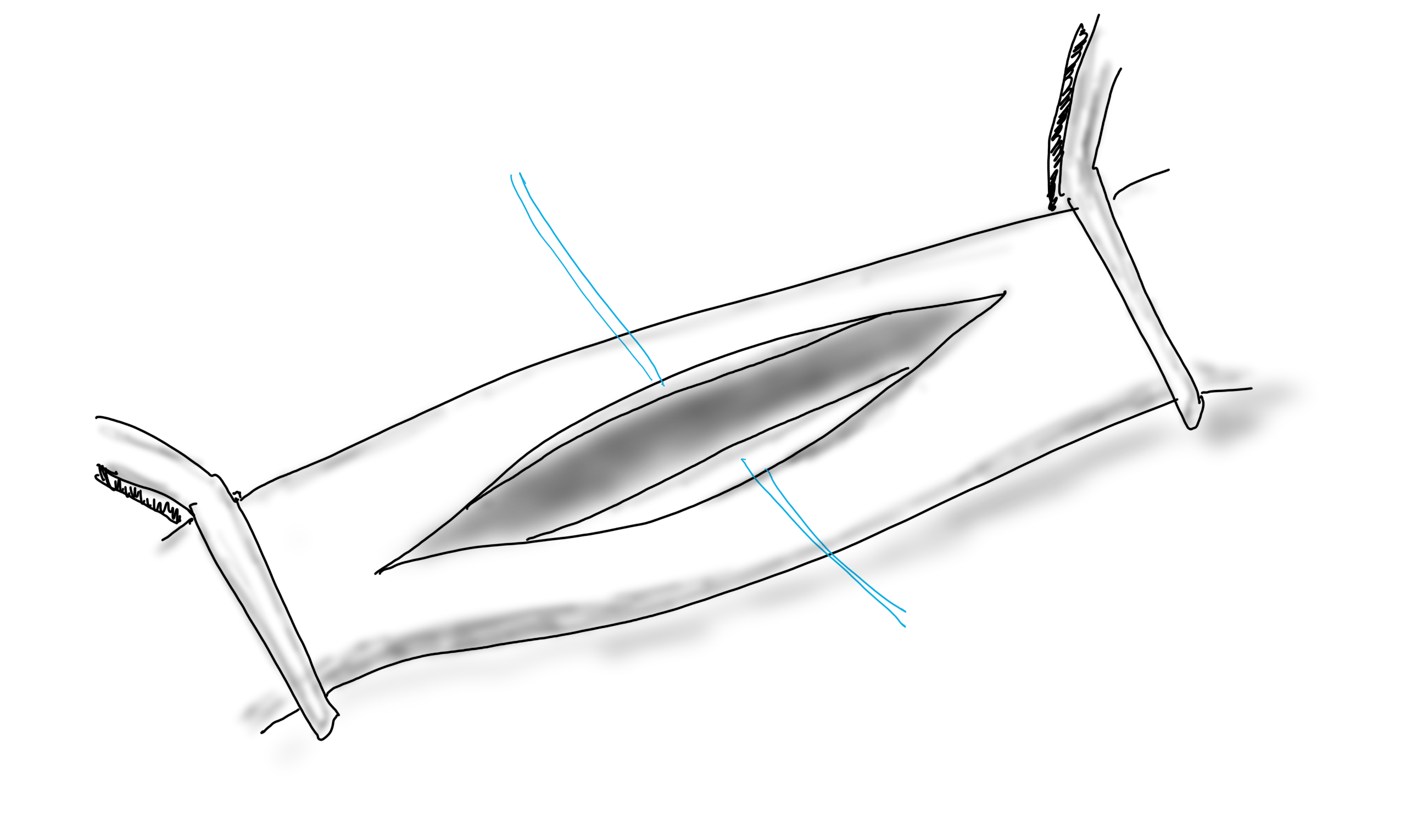
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.

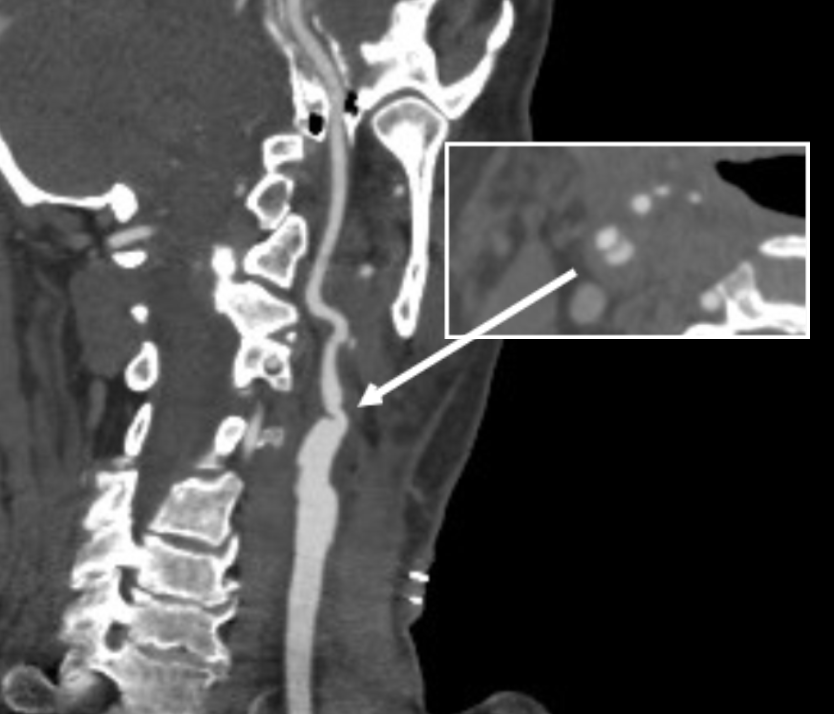
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).

The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.

Or you can do an eversion endarterectomy and avoid the problem entirely.

References
- Counsell C, Salinas R, Warlow C, Naylor R. Patch angioplasty versus primary closure for carotid endarterectomy. Cochrane Database Syst Rev. 2000;(2):CD000160. doi: 10.1002/14651858.CD000160. Update in: Cochrane Database Syst Rev. 2004;(2):CD000160. PMID: 10796309.
- Ho KJ, Nguyen LL, Menard MT. Intermediate-term outcome of carotid endarterectomy with bovine pericardial patch closure compared with Dacron patch and primary closure. J Vasc Surg. 2012 Mar;55(3):708-14. doi: 10.1016/j.jvs.2011.10.007. Epub 2012 Jan 4. PMID: 22226180.

The Park Clamp isn’t a true clamp, but rather a compressor. It was designed initialy for the troublesome venous bleeding. It is a ring with ridged edges to provide grip securely welded to a handle. It allows for circumferential compression of tissues, allowing for hemostasis while creating a open space for suturing. The picture above are my colleagues from CCAD -Drs. Andres Obeso and Redha Souilamas perfoming a partial pneumonectomy. The staple line on the artery was bleeding and this can be troublesome, and may require conversion to thoracotomy. The Park Clamp was inserted and provided excellent hemostasis (below).

During one of my cases as a fellow at the Mayo Clinic, I ran into venous bleeding behind the aortic bifurcation. Dr. Thomas Bower, recently retired, came in and lengthened the incision to create more space for more hands, and got all of us -me, the resident, the intern, the RNFA’s, to retract and compress with sponge-on-a-stick to repair the linear tear on the vena cava under the aortic bifurcation.
I’ve always hated this approach because outside of Mayo in 2002, it is very hard to get five people to become your voice activated retractor system, and the sponge on a stick only works well when you are on the hole and less effectively next to the hole. There had to be a better way.

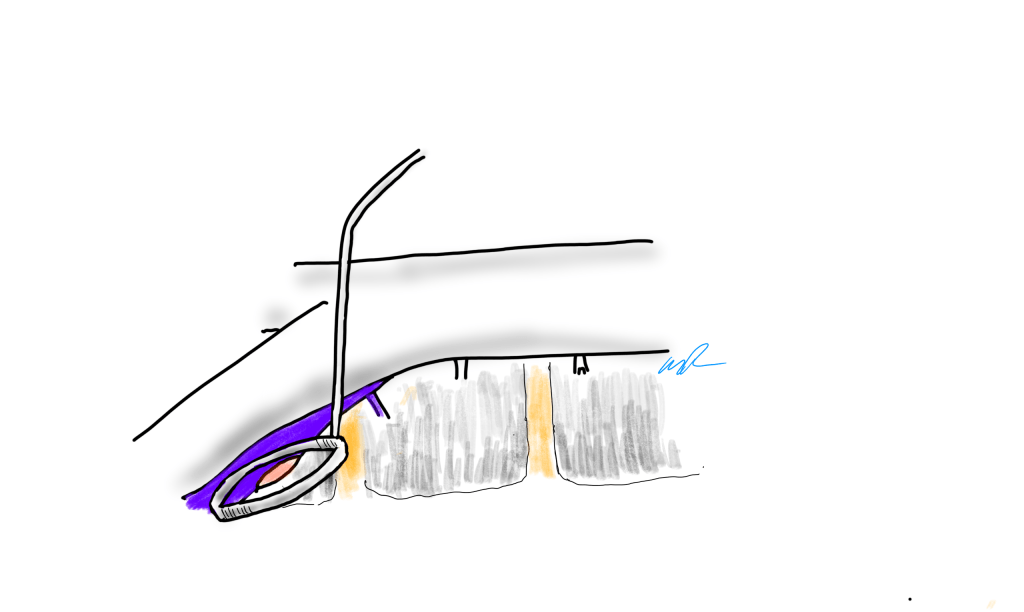
When I returned to academic practice at the Cleveland Clinic, combined cases with other specialties got me operating on tight spaces, frequently heavily scarred, with many blood vessels to control, such as a retroperitoneal spinal exposure illustrated above.

Look above at the dreaded linear tear on the left iliac vein that can result from simple manipulation of this fragile structure -typically a tributary vein will anchor the iliac and simple retraction can cause a tear.

Using a sponge on a stick greatly hampers your ability to repair the injury. First, the people applying the sponge on a stick have to have some skill. Second, because they are long and straight, they are constrained by the incision you have created. When applied, the “airspace” above the injury is greatly reduced. Third, hemostasis is never complete unless the whole vein is compressed, which is challenging in the above scenario.
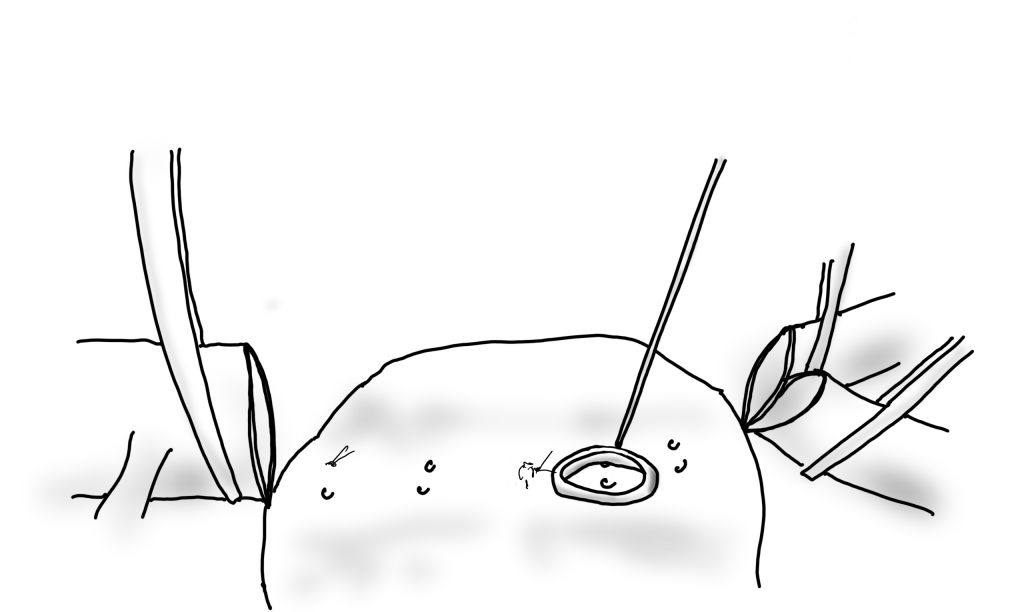
When the ring is applied, two things happen. Hemostasis is in general complete and there is room to operate, in this case suture. Even in the instance where an artery is bleeding from a flat surface as in a bleeding duodenal ulcer or a lumbar artery in an open aorta, hemostasis is achievable.

The bleeding lumbar artery illustrated above responds well to ring compression. This is also the case where you have bleeding from scarred or irradiated tissue surfaces, or from varicose veins or AV fistulae from the skin. If you don’t have a Park Clamp, you can use the finger rings of the handle on a tonsil or Kelly clamp.
There seems to be interest among surgeons who have seen this device used, and I will look into manufacturing these. I would not object to surgeons making their own for their personal use -taking apart a long tonsil clamp and bending the ring at a right angle should be simple enough. The clamps I use were manufactured at our prototypic facilities, but 3D printed ones should work fine.
And I will leave you with this final thought. I am in the profession of surgery, and at its core, it’s about helping the patient. If you adapt this idea and help someone, I will have fulfilled my duties.
The patient is a 70 year old man with risk factors of cigarette smoking, type II diabetes mellitus, hypertension, and hypercholesterolemia who presents with rest pain and gangrene of the tip of his left great toe. Several weeks prior to this, he went to his pharmacy and received a flu vaccination and picked up over the counter topical medication for an ingrown toenail. who developed pain from an ingrown toenail. Several weeks later, the tip of his toe blackened and the pain became unbearable and he came to the hospital.

Physical examination was notable for the dry gangrene affecting the distal phalanx of the left hallux. There was a left femoral pulse, but nothing was palpable below. His forefoot was cool and painful and this pain was relieved with dependency.

Pulse volume recording showed a drop in flow across the left knee and flate waveforms at the ankle, foot, and digits. The ABI was zero. WIfI 2 3 2, Stage 4, potential benefit of revascularization high (reference 1). CTA was performed and revealed patent aortoiliac segment, patent common femoral and profunda femoral arteries, with occlusion of the mid to distal SFA, reconstitution of the above knee popliteal artery with 2 vessel runoff via a patent posterior tibial and peroneal arteries.

The centerline reconstructions, adapted from aortic planning, lets me determine the character of the arteries for size, calcification, stiffness, collateralization, and length of occlusion. This was had low density and given the timecourse of the events -from claudication to gangrene, and the lack of collaterization implying an acute process possibly on a chronic lesion, I felt there was likely to be some thrombus burden over a chronic plaque across Hunter’s Canal with occlusion of the geniculate arteries. Usually, when the occlusion is chronic, femoropopliteal occlusions of this type come with an ABI of 0.5-0.7, not 0.

Global Limb Anatomical Staging System (GLASS) Classification of CLTI (reference 2) through the easy to use SVS calculator came out Stage II: Intermediate Complexity. I had the good fortune of being in the audience when GLASS was presented to a rapt audience in Lyons, France, by Dr. John White in 2017, at the ESVS meeting. I include it because Dr. Devin Zarkowsky on a tweet that generated this post wanted WIfI and GLASS. WIfI I find helpful. GLASS I am still figuring out, because it tends to tell me what I already know: this is a lesion of intermediate complexity that could go either way to open or endovascular.
Treatment options include:
- Endovascular -starting with POBA and escalating to various additional therapies such as stents, covered stents, DCB, drug coated stents, atherectomy, thrombectomy, thrombolysis (then any of the previously mentioned).
- Bypass with PTFE
- Bypass with vein

The data tells us so far that open or endovascular is broadly equivalent, but experience guides me. For rest pain, any incremental increase of flow will do, and it does not necessarily have to be in-line. For healing major tissue loss, there really can’t be enough flow. Bypasses with good runoff deliver a lot of flow. Bypasses with vein have great longevity and the shorter they are, the longer they last.
So is long patency important? Numerous studies have shown that patency does not impact limb salvage or amputation free survival, going to BASIL Trial (reference 3), but even stretching back to Dr. Frank Veith’s advocacy of PTFE bypass to infrageniculate targets (reference 4), patency does not add to limb salvage beyond the initial wound healing. The patency of a PTFE bypass to a tibial target is less than 20% at 5 years, but the limb salvage rate is a laudable 80% plus, and this is repeated in numerous evaluations of POBA, stents, and every new technology that has accrued in the nearly 4 decades since that paper.
What does patency buy you? Less reinterventions. There is nothing worse to me than having to reintervene within a year or two of an intervention. When a bypass works well, the patients just come for a hello-how-do-you-do for years. The BASIL trial concluded that bypass operations were more expensive, and I dispute this. In 2021, operations were far less expensive than the latest energy weapon, their box you have to purchase, and the catheters you use once and throw away. The argument given by interventionalists is that bypass operations are disfiguring and ridden with complications and that argument holds water as there are many points where vascular surgeons fail or have largely stopped work on investigating and optimizing open surgery. What if bypass surgery could be brought to the level of dialysis access surgery in terms of invasiveness? What if groin complications could be minimized? What if long filleting-type incisions of the thigh and leg could be eliminated entirely? What if edema could be prevented or minimized postoperatively to prevent serous drainage and infections? If you focus on the art of bypass surgery and choose patients well, you can get a quick, minimally invasive bypass with the overall physiologic impact of a Brescia-Cimino AV fistula. After considering endovascular, I chose bypass.
This patient had on mapping excellent saphenous vein between 3-5mm in diameter. He had excellent skin and was not obese. A vertical groin incision could be avoided by making a skin line incision over the saphenofemoral junction and transposing it to the adjacent SFA which was patent. Skin line oblique incisions in the groin heal much better than the standard vertical incisions, and it is possible to mobilize and expose the saphenous vein using an appendiceal retractor and clipping the generous proximal thigh tributary. In this patient, the most proximal incision was well away from the inguinal crease, the generator of wound infections in the groin. Essentially, if there is no groin incision there can be no groin complication.
The distal vein is mobilized first before dropping on the above knee popliteal artery which is exposed through a separate incision. This is because the AK POP space is best exposed over the sartorius, and the vein in this patient was well below (posterior) to the sartorius. The vein was tunneled under the sartorius to the AK POP. With the in-situ technique, the proximal anastomosis is completed, then the valves lysed with a retrograde LeMaitre valvulotome. Doing, after two or three passes, the pulse was strong, and the flow strong enough to fling the blood beyond the foot -a key step. If there is no such flow, if there is a weak pulse, or poor blood flight, I do one more pass of the valvulotome then duplex for any large diverting tributaries and tie them off one by one until good flow is achieved.
I do not mobilize the entire vein (and tie off every collateral) unless I cannot do an in-situ technique. It defeats the purpose of this beautiful minimally invasive procedure.

He recovered rapidly and was discharged home after a partial hallux amputation by podiatry. In followup, he was feeling better. All of his surgical wounds had healed. Duplex and ABI did find this:

I took him to the angiosuite for repair of this retained valve. Rarely, retained valves occur after in-situ bypasses, but require generally unsatisfactory solutions involving either open valvulectomy and patch venoplasty or stenting of a virgin vein. Valvulotomy is possible, but generally described as an open procedure as well, but I had other plans.
Downstream of this retained valve were tributaries which could be seen on duplex, and therefore accessible with a micropuncture needle. This would then allow for placement of a 4F sheath, through which the LeMaitre valvulotome would pass unhindered, allowing for valvulotomy. I would use this session in the angiosuite to deliver embolization coils to the diverting tributaries as well.


LeMaitre is a unique company in that it focuses on vascular surgical operations and arises from the original product and reason for the company the eponymous valvulotome. Because it comes sheathed in a low profile catheter, it is immediately familiar to modern surgeons even though it was made in another century.

Cutting the valves involved passing the valvulotome several under fluoroscopy through a 4F sheath placed through the tributary seen above. After the valvulotomy, the diverting tributaries, only one of which drained quickly into a deep vein, were coiled. At the end of the procedure, a manual cuff was found and an ABI checked. It was now 1.05.

In 2015, the Oxford English Dictionary added McGyver as a verb -“Make or repair (an object) in an improvised or inventive way, making use of whatever items are at hand.” A television show from the 80’s and early 90’s, the main character, McGyver, was able to make useful tools out of what was available, allowing him to come out victorious, but usually just survive. It is a useful concept that is a must have in managing complex and dynamic situations. Just because it hasn’t been done before to your knowledge doesn’t mean that it isn’t a simple solution. I have only one ask that LeMaitre flip their blades around and design an ante grade valvulotome. Those who know what I’m getting at know what I am getting at.
The LeMaitre valvulotome allows for in-situ saphenous vein bypass, a prototypical hybrid vascular procedure from the 80’s that portended the endovascular revolution that followed. It is meant to be used intraoperatively, but because of its low profile, it can be applied.
I will allow that this second procedure likely makes any argument to cost moot, but numerous incisions and extra time in the OR is avoided. The patient now has a vein bypass that could last many years which diminishes the need for follow up procedures to maintain assisted patency.
We will be arguing this point for years even after BEST-CLI is presented. BASIL-2 just closed enrollment. Hopefully we will get some clarity.
Reference
- Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014 Jan;59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12. PMID: 24126108.
- Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28. Erratum in: J Vasc Surg. 2019 Aug;70(2):662. PMID: 31159978; PMCID: PMC8365864.
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005 Dec 3;366(9501):1925-34. doi: 10.1016/S0140-6736(05)67704-5. PMID: 16325694.
- Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, Towne JB, Bernhard VM, Bonier P, Flinn WR, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg. 1986 Jan;3(1):104-14. doi: 10.1067/mva.1986.avs0030104. PMID: 3510323.
Okay, so I have made this intermittent list of top ten gadgets and gewgaws which I used to to call “Top Ten Things to Get Your Favorite Vascular Surgeon” but even in jest, over the years that I have been publishing this blog, the world has changed. As a watcher of technology, I have always had my eye out for the next great thing, and here is my list. I hope you all have a great Christmas and a wonderful New Year.
- Giant Laptops with Complications -old automatic watches with complications are still coveted, and the tech space is no different. Whereas, Apple has always veered to minimalism, there is an exuberance to adding “stuff” in among the Chinese manufacturers and ASUS is no different.

This laptop, the ASUS ZenBook Pro UX581 is a perfect example of innovation by jamming as much possible onto your ADHD-addled field of view. What would I use it for? Who knows, but I want!
2. Timex watches retroversions. Like automakers making updated versions of classic muscle cars, the old standby Timex, has launched watches that that make you want to party like it’s 1979.

The Navi XL Automatic 41mm by Timex is beautiful to look at and of all the knockoff Omega Seamasters out there, it is nice to see a classic American branded offering. Cheaper watches are a smart thing for surgeons in that it’s easy to lose them when you take them off to scrub for a case. While Apple watches are popular, the only square watches I like are Cartier Tanks, and for health data, I wear a Fitbit on my right wrist.
3. Entertainment tablets have made the large family TV obsolete. Add in good audio, and you have that weird future that they promised back in the 1980’s when they swindled your parents to buy a $3000 computer that really couldn’t do anything.

The Lenovo Yoga Tab is an incredible value for what you get which is a bright screen, fast enough processor, long battery life and great sound (JBL speakers with Dolby Atmos processing). It comes in 8, 10, and 13 inch sizes. Coupled with a keyboard and mouse, and an Office or Drive account, and you have a very portable workstation. The only thing missing is the ability to draw as it does not pair with a stylus.
4. E-ink based tablets. If you have ever had a Kindle, you know what an E-Ink based tablet is like. Viewable in direct light, these displays have the advantage of minimizing fatigue in the same way paper does compared to staring at a monitor. These 3rd generation tablets run full Android and can run the Kindle app, as well as advanced note taking and PDF markup software, and have that warm backlighting that comes with the modern Kindles.

The Boox Max Lumi does all of that. Paired with a keyboard, it recreates a basic typewriter well. It also functions as a second screen, allowing you to stare at and markup documents driven by a laptop computer. I want.
5. The modern update to the Psion Series 5mx. The Psion Series 5mx was a pocketable computer that ran a very efficient operating system, powered by two AA cells which lasted up to 40 hours, and had a tiny keyboard that with practice was fine for authoring chart notes that I would then print out to HP printers that that infrared ports (IrDA). This allowed me over a three year period of residency, to collect my personal EMR that I kept on a huge for that time 32mB flash drive. I sold my 5mx, along with a considerable box of hard to find accessories, to a journalist in Mexico who needed to author articles and fax them to his paper in 2007.
The Gemini PDA was made by a group of engineers and programmers who remember that time and updated the Psion Series 5mx form factor, down to the legendary keyboard. Available in Android and a Linux, it is a pocketable microlaptop.
6. Asian stationary, notebooks and pens, are next level. In certain malls in coastal cities in the US, you can find the odd Japanese store that has a section for stationary. The bindings are fantastic and the pens work forever. My favorites are mechanical pencils and fountain pens, which despite the incredible builds, are really affordable.

For example, the Planting Tree Paper Bind Ruled Notebook 5 Piece Set, available from Muji, is available for 2.99 on line and are great looking and durable.
7. Instant Coffee is anathema to serious coffee snobs. I have a friend who keeps a water heater, lab style glassware, digital food scale, and grinder to make a perfect cup of drip brewed coffee for himself -a fifteen minute process. The disposable pod coffees -blurgh. In Abu Dhabi, I got introduced to high end instant coffees at the grocery -the packaging and brands oozed luxury, and the coffee was much better than the instant coffee I grew up with.

Mount Hagen Fairtrade Organic Freeze Dried Coffee is what I found as an alternative to the old instant brands that represented bad instant coffee. This stuff mixes well with cold water as well, and delivers a bright kick of caffeine. It lets me make a to-go cup of coffee, well, instantly.
8. Headlights are always fun, but running in them is challenging because they sit off the center axis and tend to drop down. I have tried many times to incorporate them as cheap operating room headlamps, but failed largely as they are not bright enough. These light band headlamps which popped up in my Facebook were intriguing.

These lights (link) have both the light band which is amazingly bright and a regular flash light on the side, both of which can be turned on by waving your hand by a sensor next to your head. I thought this was the answer to my search for a cheap OR headlamp (the regular ones cost way over 1500USD), but the problem is that anyone looking at you is immediately blinded and their retinas seared. But for running, these forehead based high beams are amazing.
9. If you are surprised at the lack of Apple products, it’s because I typically aren’t in the market for them. They last forever. My 2007 Macbook Pro still runs, survived a major upgrade which included maxing out RAM and swapping the spinning platter hard drive for an SSD, resulting in lightning speed. Unfortunately, they are exhorbitantly expensive and so I find myself hesitating at purchasing a 2500USD laptop, especially one that I can no longer upgrade and maintain as I could the older Apple laptops. The problem is the battery and the SSD. They have finite lives. You can still buy batteries for the 2007 Macbook Pro, and get all day work from several batteries. Apple solves the problem of owners keeping their Apple gear for decades by imposing obsolescence, and recently even slowing down the performance of older machines to get owners to buy new iPhones.

So this makes the purchase of iPad, Macbook Pro, and even the iMac problematic in that they are all closed box systems with limited lifespans. Of the recent Apple products, the best bang for the buck comes from the Mac Mini. The older ones from 2012 can be found in droves, refurbished, and can still be upgraded, but the new ones with the blisteringly fast M1 chip that can run iOS apps is worthy of my consideration. It may be the last Mac that I ever purchase. My 2007 MacBook no longer runs the latest OS version, and I will be turning it into a Chromebook.
10. Typewriters are a fantastic way to write. They don’t let you check social media or email, and encourage that focused state where words just flow. That is the concept behind the Freewrite and its special edition Hemigwrite.

Whatever you type gets stored in you choice of cloud account, including Google, Dropbox, and Evernote. You can work on 3 different files, and as you type, the Wifi connection updates your file in the cloud. The keys are that clickety clack mechanism reminiscent of original keyboards from the 80’s, and the E-Ink screen, now backlit on this beautiful aluminum clad Hemingway edition of the Freewrite, makes it easy on the eyes. The great American novel awaits to come erupting out of your head.
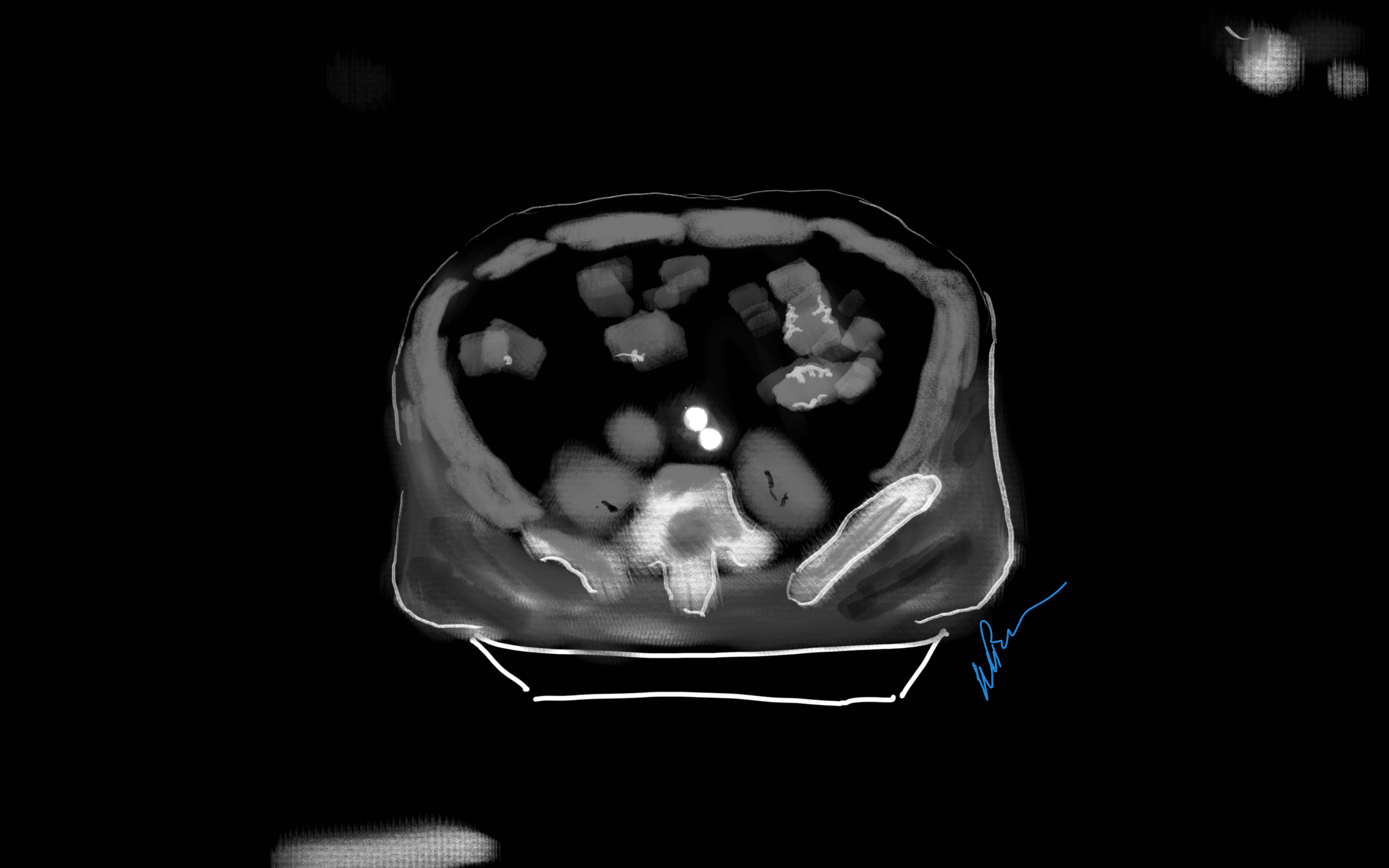
One of the greatest surgical texts, Cope’s Early Diagnosis of the Acute Abdomen, is something every surgical resident, vascular or general, should read. The mid-century edition which I owned during my residency, has since been updated, but the central message of the book is this: every complaint or pain the patient has comes from a nerve, either peripheral or visceral, and understanding the nature of the pain, you narrow the diagnosis to only a few possibilities. Irritation of the psoas muscle results in a characteristic pain that years of diagnosing appendicitis the old fashioned way -by exam, then operation, makes it easy to recognize, like Marilyn Manson showing up as your substitute teacher (I would have said Alice Cooper, but that completely dates me). When the psoas muscle is irritated, by a hematoma, injury, inflammation, or abscess, the muscle relays intense pain localized to the retroperitoneum. Stretching the muscle worsens the pain, and the patient is often seen with the ipsilateral hip flexed. The genitofemoral nerve which rides on top of the psoas, is triggered and there is pain referred to the groin and proximal anterior thigh. Seeing this, and fitting the story allows for a diagnosis, before imaging. Without this insight, there is no swift vector to treatment and resolution.

The patient, a middle aged man, had undergone a redo-iliac angioplasty and stent for left iliac in-stent restenosis. He relayed that on the table, he felt immediate left lower quadrant abdominal pain and the desire to flex his left hip. He was restrained, sedated, and the procedure finished -a covered stent had been placed. When he came to my office a month after his initial procedure done elsewhere, he was in wheel chair, unable to straighten his leg. He claimed before coming to see me, he had gone to another hospital, where he had a CT scan and was told nothing was wrong (will have to confirm). He was having subjective fevers at home.
On examination, he sat on the exam table with left hip flexed. His pedal pulses were easily palpable. He had furuncles in his groins which he relayed he had had all of his life. I sent him for CTA and subsequently admitted him for surgery.

The CT showed a large collection around the left iliac artery and stents and on the psoas muscle, an abscess. The blood cultures on admission were positive for Staphylococcus lugadensis sensitive to penicillin.
Putting the story together after the fact is much easier than when you are in the moment, but being aware of the location and type of pain should give you a clue. Very likely, he had a brief rupture on the angiosuite table resulting in his sudden pain, drowned out by the sedatives typically given in response to a patient moving when a stent is deployed. Inflating a balloon in an artery typically causes some discomfort -as the vessels are lined with visceral nerve fibers which are quite sensitive but less localizable than say a pin poking on the index finger. If you ever had bloating with gas, that general discomfort localizable to the mid abdomen, that nausea and discomfort is from stretched visceral pain fibers. If you have ever had dull aching pain of distended spider veins, that is visceral pain. It’s there, but you would not be able to pinpoint it exactly. That is not what this patient had when he flexed his hip on the angio suite table. While the covered stent was deploying, he likely briefly ruptured causing both somatic and visceral pain around his left common iliac artery and iliopsoas muscle. Additionally, if the sheath had been entered through an area of a skin abscess, likely the sheath, wires, and gloves were contaminated. Any handling of the balloon expandable stent graft, which I highly discourage, would have contaminated it, resulting in a device infection, which was made more likely due to his diabetes. As the hematoma got infected, it resulted in the worsening symptoms he was having of left lower quadrant abdominal pain, groin pain, thigh pain, and inability to straighten his hip without pain.
I took him to the operating room and drained his abscess, assisted by Dr. Andrew Tang, chief resident headed to CT Surgery fellowship here at the Clinic, and Dr. Jenny Chang, PGY 2 Surgery. I gave Dr. Chang a copy of Cope’s with the admonition to read it soon and pass it on, as most of the current generation claim no knowledge of this important text. While I am not against interventional drainage, it takes time to drain the collection through a tube whereas sticking your hand in, sampling the collection, observing the injury, and breaking up collections and washing out with brown-bubbly -a mix of betadine/peroxide diluted in saline, I believe speeds the recovery from the infection. His drainage was done through a retroperitoneal approach from the left side and notably, his psoas muscle while viable, did not retract to cautery energy, suggesting some degree of rhabdomyolysis. The iliac artery was an indurated, thickened, and hard from the calcium and plaque that was the original problem affecting his distal aorta and iliac arteries (see left arteriogram centerline). I placed a pair of JP drains, removed one that wasn’t draining much on POD #3, and the other about a week after discharge on POD#5. His WBC elevation which was never high promptly resolved. I kept him on oxacillin with consultation from ID, and waited. After 3 weeks, I repeated his CTA.

His right iliac centerline showed patent stent with diffuse plaque and calcium starting in mid infrarenal aorta.

His abscess had significantly resolved and his pain was gone. He was ambulating again.

The choices at this point were the following
- Continue treatment of patient with supressing antibiotics for life
- Resection of left iliac stent graft which is presumed to be infected
If resection chosen, the options for repair that I considered included:
- NAIS (ref 1). Neoaortoiliac System graft using femoral vein
- Aortoiliac homograft
- Rifampin soaked gelatin coated graft (ref 2)
- Extra-anatomic bypass with axillofemoral bypass or femorofemoral bypass.
- Aortoiliac endarterectomy and repair with bovine pericardial patch and graft
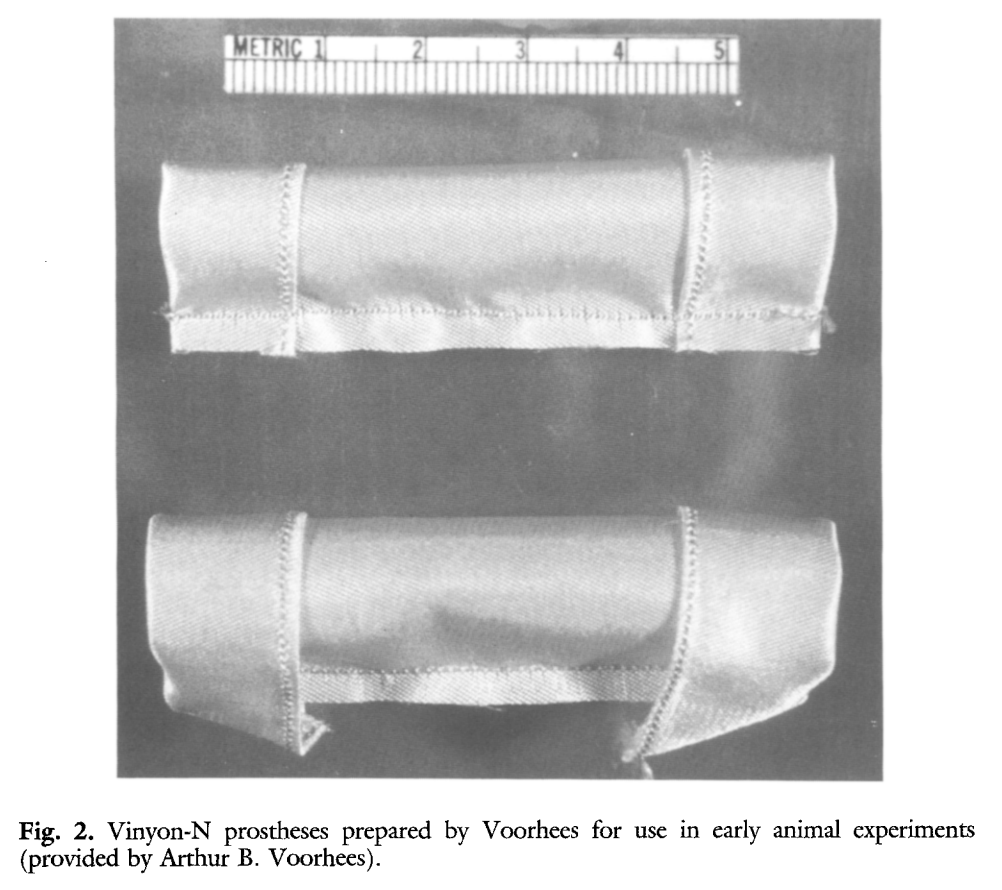
The choice of replacement is becoming clearer in that while rifampin soaked grafts offer immediacy and expedience, all grafts seem to be prone to reinfection at a higher rate than autologous material (ref 3). The NAIS bypass is a great option, but is hampered by the addition of several hours invested in harvest of the femoral veins. While it can be staged with mobilization done one day and harvest another, those added hours add complications. We often forget that the simple metric of procedure time is the most important determinant of complication rate. Any operation going over 2 hours risks wound infection for example simply from ambient colonization of the open wounds from the rain of dead skin from the surgeon’s face, aerosolized fecal flora from flatii (prohibited in my ORs). The microenvironment of the open wound is also room temperature and not 37, having an impact on organ function and hemostasis. The homograft is the original aortic graft -before Arthur Voorhees invented the cloth vascular graft as a resident at Columbia P&S (my medical school alma mater, ref 4), major hospitals had tissue banks of aortic homografts harvested from the recently deceased. Having homografts is now an outsourced function, but does require having proper refrigeration for the cyropreserved grafts and generally can’t be ordered with short notice.
Rifampin soaked grafts work well, especially wrapped in omental flap, in the short and medium term but suffer a reinfection rate that is higher than seen with autologous tissues, and prosthetic grafts without rifampin, such as PTFE for extraanatomic bypass, have the highest rates of reinfection (3), despite being the board answer decades ago.
Endarterectomy allows for use of native tissues for repair. The adventitia around plaque and stents, while thin, can support physiologic pressures, even when they have been occluded for years. And while practice of aortoiliac endarterectomy is a bit of a lost art, it has both a long history stretching back nearly a century and a modern track record with carotid and femoral endarterectomy. It is merely a matter of scale. Pinch and zoom in on a femoral endarterectomy at the bifurcation and you have the same case as with an aortic one.
The question is, is bovine pericardium more autologous than prosthetic? It is a decellularized sheet of collagen from a cow’s pericardium, used in heart valves and vascular patches, but only recently applied as a graft (ref 5-7). I have long used bovine pericardium as a patch with some caution, but the rule of thumb is are there well vascularized tissues around it? A layer of Scarpa’s fascia and fat in a groin wound are not sufficient to protect a bovine patch, but a sartorius flap is. For me, once the infected stent graft is out, knowing if the surrounding tissues bleeds well is an important one.
I chose to do aortoiliac endarterectomy. The patch and graft would be made with bovine pericardium, unless I found the left iliac segment to be devitalized and foul with anaerobic vapors, then, I would close and go NAIS or extra-anatomic. The key point is that choices have to be on the table and constantly rearranged during the conduct of the operation.
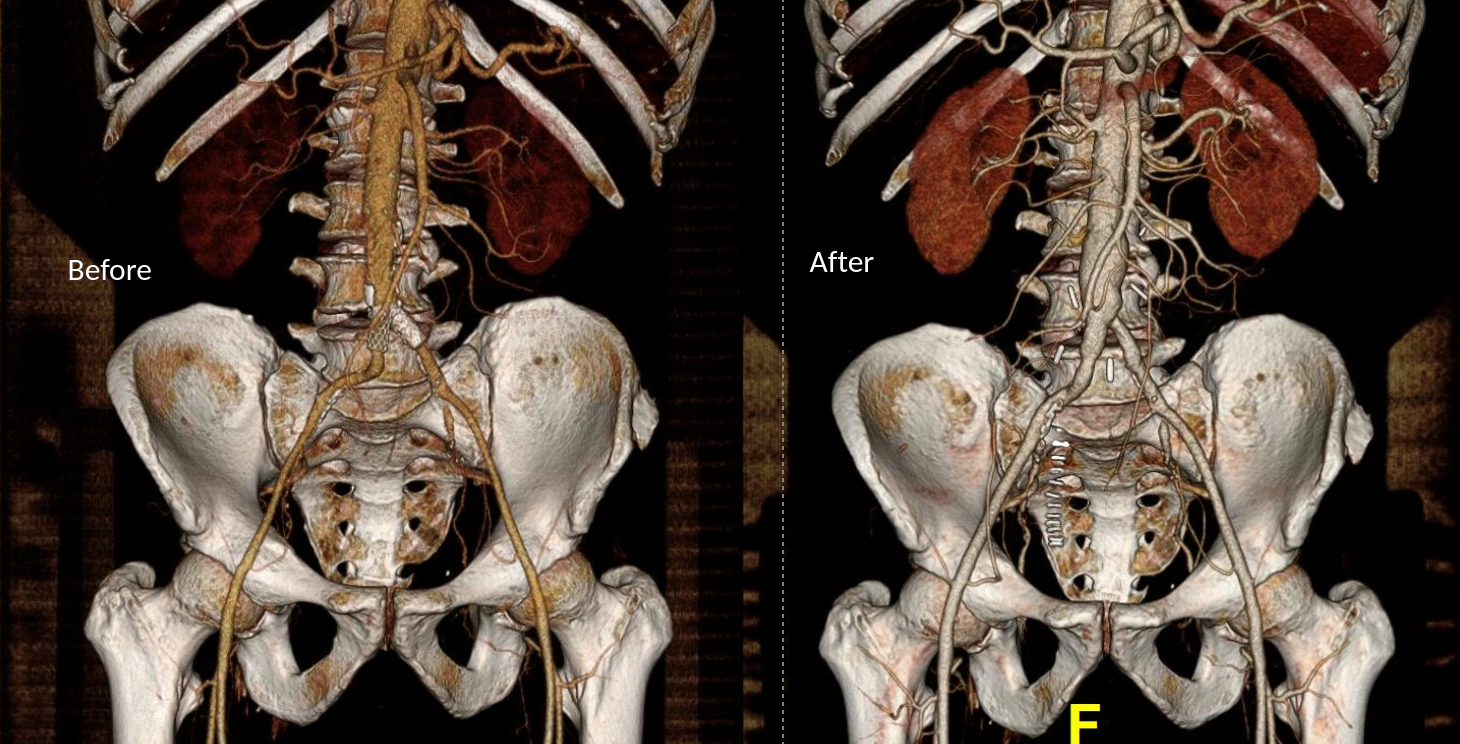
The patient was preoperatively vein mapped and had suitable deep femoral vein for bypass conduit, having robust duplicated systems that would impact the patient minimally. The patient was placed in a supine position and via a midline laparotomy, the infrarenal aorta and the common iliac arteries beyond the short iliac stents exposed. I chose this limited exposure as any further into the phlegmon on the left risk injury to ureter and vein. The aorta had a palpable demarcation between plaque and mildly diseased proximal segment, predicted by the CTA to be at the IMA. A longitudinal arteriotomy was created on the right side from mid aorta to mid right iliac, and the left side had a separate arteriotomy to release the stent. The plaque came out in a single specimen (image).

The left iliac artery was destroyed by the infection but the tissues around it bled avidly and were not foul or infected. I avoided excess debridement here as the iliac vein was intimate with the phlegmon. There was a 3cm gap. Again, I thought briefly about taking femoral vein, but proceeded to make a graft from the bovine pericardium. This was sewn around the rod portion of a renal vein retractor from the OMNI set. The finished product resembled Voorhees’ graft. It was sewn into the orifice of the iliac from inside the aorta and end to end to the freshened iliac stump. Unfortunately, the omentum was atropic across the transverse colon, but the tissues around the resected artery and stent graft bled well, indicating good penetration of antibiotic. The retroperitoneum was closed after hemostasis obtained. Dr. Shashank Sharma, our chief resident headed to a vascular surgery fellowship at the renown Houston Methodist next year got to see what is unfortunately a rare occurrence -an aortoiliac endarterectomy, which through me puts him three degrees of separation from Cid Dos Santos (ref 8). Dr. D’Andre Williams, PGY-2 Vascular Surgery Resident, got important lessons on sewing the aorta. She’s part of a fortunate cohort that get exposed to open aortic surgery at our main campus which is unfortunately rare throughout the world.

The final graphic shows the operative end result.

The patient recovered well and was discharged within the week with another month of IV antibiotics planned.
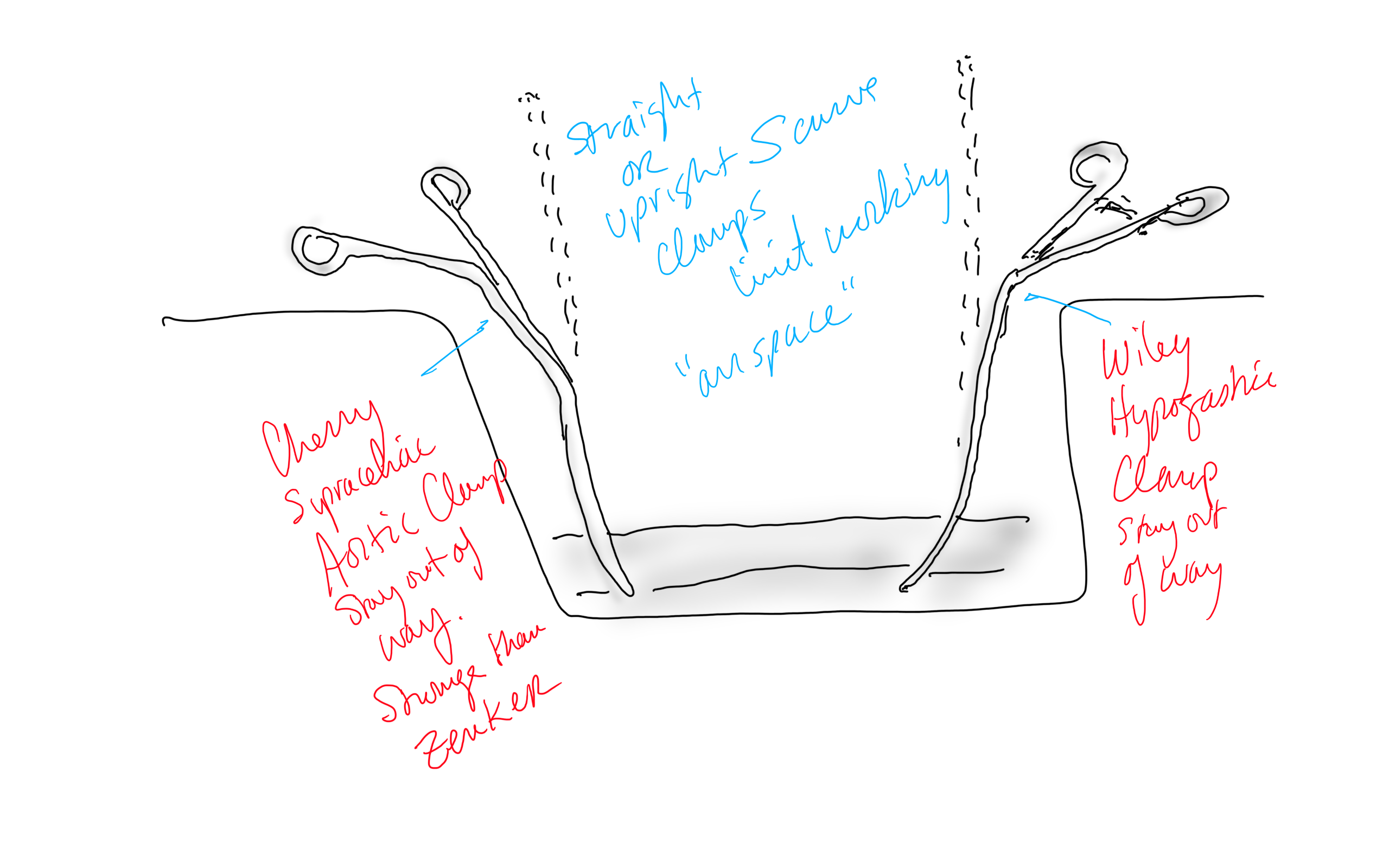
Conclusion: The operation was started at 8 in the morning and was done by lunch time. For aortic cases, this is a crucial metric, as when the clock winds past the surgeon’s comfort, the patient suffers even more. Adding the femoral vein for a NAIS may have been the textbook thing to do, but we don’t do extra-anatomic bypasses that much either. I don’t believe that adding two more hours for retrieving the femoral vein would have enhanced the procedure, and would have served to add potential areas for complication. Technically, the aorta closes much as with a carotid or femoral endarterectomy, but the adventia is thin and really should be sewn with 5-0 or 6-0 Prolene. The larger needles such as the SH size creates unnecessary bleeding unless sewn with a line of felt which could become infected. Despite the thinness, it will hold pressure if it is not infected. Clamps that bend out of the “airspace” above the laparotomy, such as the Cherry Supraceliac Clamp and Wiley Hypogastric Clamp, prevent limiting the operative space with long clamps such as aortic Fogarty or DeBakey clamps, while being stronger than the Zenker.
A final comment for Staphyloccocus lugudensis. This is the second major vascular graft infection with this organism I encountered this year. The other was an infected aortic stent graft. Lugudensis means from Lyons. I do not know why that is, but it is so far not the nasty player that is S. aureus. I am sure it will share some plasmids, and become resistant one day, but in the earlier case in Abu Dhabi and now this, it is sensitive to penicillin, and came from the skin at the femoral puncture site, and for this we are fortunate. Major vascular infections are one of the few areas that still demand open surgical skills, and we foresake them at great peril. It’s critical to remember all the collective memory of surgery from the past, or we will become mere technicians fixing whatever comes out of the radiologist’s report with whatever knowledge obtained from a Zoom meeting for the latest, greatest device.
Acknowledgement
Gratefully, the patient gave his permission, as with all patient, for use of his case for educational purposes.
References
- Chung J, Clagett GP. Neoaortoiliac System (NAIS) procedure for the treatment of the infected aortic graft. Semin Vasc Surg. 2011 Dec;24(4):220-6. doi: 10.1053/j.semvascsurg.2011.10.012. PMID: 22230677.
- Oderich GS, Bower TC, Hofer J, Kalra M, Duncan AA, Wilson JW, Cha S, Gloviczki P. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg. 2011 Jan;53(1):99-106, 107.e1-7; discussion 106-7. doi: 10.1016/j.jvs.2010.08.018. PMID: 21184932.
- Smeds MR, Duncan AA, Harlander-Locke MP, Lawrence PF, Lyden S, Fatima J, Eskandari MK; Vascular Low-Frequency Disease Consortium. Treatment and outcomes of aortic endograft infection. J Vasc Surg. 2016 Feb;63(2):332-40. doi: 10.1016/j.jvs.2015.08.113. PMID: 26804214.
- Smith RB 3rd. Arthur B. Voorhees, Jr.: pioneer vascular surgeon. J Vasc Surg. 1993 Sep;18(3):341-8. PMID: 8377227.
- Almási-Sperling V, Heger D, Meyer A, Lang W, Rother U. Treatment of aortic and peripheral prosthetic graft infections with bovine pericardium. J Vasc Surg. 2020 Feb;71(2):592-598. doi: 10.1016/j.jvs.2019.04.485. Epub 2019 Jul 18. PMID: 31327614.
- Lutz B, Reeps C, Biro G, Knappich C, Zimmermann A, Eckstein HH. Bovine Pericardium as New Technical Option for In Situ Reconstruction of Aortic Graft Infection. Ann Vasc Surg. 2017 May;41:118-126. doi: 10.1016/j.avsg.2016.07.098. Epub 2016 Nov 27. PMID: 27903471.
- Belkorissat RA, Sadoul C, Bouziane Z, Saba C, Salomon C, Malikov S, Settembre N. Tubular Reconstruction with Bovine Pericardium Xenografts to Treat Native Aortic Infections. Ann Vasc Surg. 2020 Apr;64:27-32. doi: 10.1016/j.avsg.2019.10.104. Epub 2020 Jan 10. PMID: 31931127.
- Barker WF. A history of endarterectomy. Perspectives in Vascular and Endovascular Therapy. 1991;4(1)1-12. doi:10.1177/153100359100400102
Categories
An Open Letter to LeMaitre Vascular
George W. LeMaitre, Chairman and Chief Executive Officer, LeMaitre Vascular, Inc.
Dear George,
If you go to the LeMaitre Vascular website, there is a link to the story about the company’s founding by your father, Dr. George Lemaitre, which I heard first hand over dinner hosted by him and your mother many years ago. The original LeMaitre Valvulotome has followed me through my career from surgery residency in the 90’s to a recently closed tenure as vascular chief at Cleveland Clinic Abu Dhabi. There is no in-situ bypass that I perform where I am not struck by your father’s story and by the ideals passed by him into the company he founded which had at its core the desire to help vascular surgeons take care of their patients. There are so many other companies, most of them in fact, in this vascular space who are investor-first when it comes to decisions about what diseases, procedures, and specialties to support, but LeMaitre Vascular has always felt different.
For decades, LeMaitre Vascular seemed focused on helping vascular surgeons care for their patients with unique, purpose-designed solutions. Engineering at its finest. It gave life to many ingenious products like Anastoclip, Unballoon, and LeverEdge, that seemed to spring from the minds of working surgeons and physicians directly into their hands, much like the valvulotome. The best ones appealed to the many surgeons who wanted to advantage their patients and their institutions with both lower cost, time efficiency, and equivalent or better outcomes to the usual way things are done. Unfortunately, we live in a universe where the incredibly potent gravitational pull of the investor interests is for high volume, high margin items. This pull greatly exceeds that of the bright yet smaller stars and moons that are common sense, durability, and sustainability. Items that drop out of peel packs, are used once, and thrown into a landfill, have become everything used in healthcare. The sudden absence of EndoRE (remote endarterectomy) on the LeMaitre product page speaks volumes to this. Something that is low volume, durable, subject to repeat use like a set of Vollmar Rings, which are purchase once and used for a long time, must have little appeal to those who author investor reports. It is in such an decision environment that EndoRE the product must have been cancelled from the LeMaitre Vascular web page (link). I wouldn’t think that LeMaitre would give up manufacturing the eponymous valvulotome for low sales figures, but it did give up on remote endarterectomy for that reason.
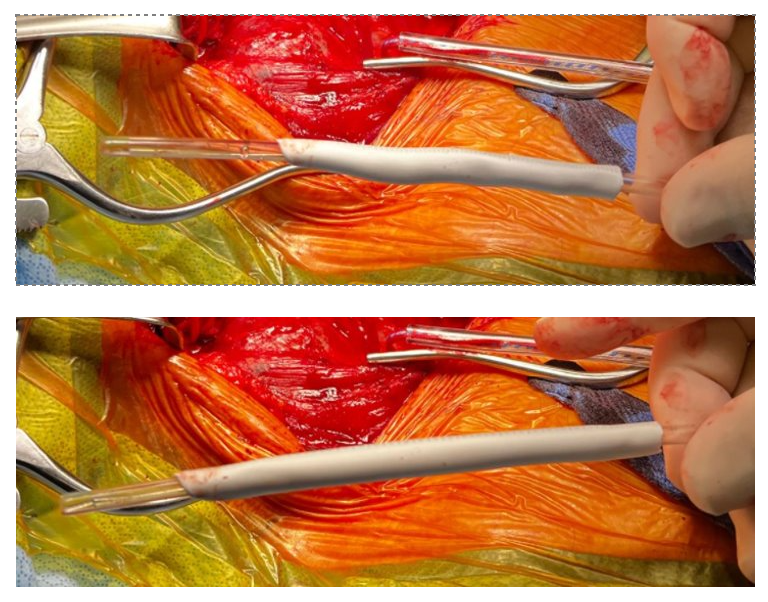
Let me show you one of the first cases I did after returning to Cleveland. I am now practicing at Fairview and Avon Hospitals, premier flagship hospitals in the Cleveland Clinic fleet, on Cleveland’s west side, and a patient arrived while I was on call with sudden onset of pain in his leg from a lack of blood flow. He had occlusive atherosclerotic plaque extending from his external iliac artery to the above knee popliteal artery causing ischemic rest pain.

I contacted LeMaitre Vascular and got in touch with your representative, L. Fisher, who promptly sent the Moll Ring Cutters I needed to perform a remote endarterectomy of the patient’s occlusive external iliac and superficial femoral artery plaque. The technical details of remote endarterectomy are have been covered in my blog (https://vascsurg.me/?s=endore), but in the end, through a 7cm incision in the groin (don’t believe the hype, this is minimally invasive), I restored his arteries to their original open condition. Shown below are the results. It was with great sadness that I heard that the LeMaitre Vascular equipment being sent were the last of the stock available in North America. The patient did very well, with the operation completed well before lunch, and is recovering rapidly from his small wound and big rescue. He gets to walk out of the hospital on two legs, but also with the surety that he avoided a major bypass operation, and avoided the short term gains of stenting from the aorta to the profunda -more peel packs and landfill items and a dubious long term durability. Hey, I even used a XenoSure patch on the common femoral.



Endarterectomy is foundational to vascular surgery going back to the work of Professors J. Cid Dos Santos and E. Jack Wiley. Through Dr. Kenneth J. Cherry, who trained under Dr. Wiley, and who trained me, I can claim two degrees of separation from the originator of endarterectomy, and this drives my passion for preserving this critical tool in our vascular kit. The basic tools, the endarterectomy rings, are as old as vascular surgery itself. To lose a critical supplier, particularly in a time when the pendulum to open surgery is swinging back, when the best results come from combining traditional surgery and cutting edge endovascular techniques in hybrid procedures such as EndoRE, when the coming healthcare cost-apocalypse will cause everyone to question the value of thousand dollars-plus items dropped from peel packs, is devastating.
I get it that the aSpire stent never panned out, and that disposable dissector/cutters never moved that well, and that you run a business, not a charity. But I do believe that best companies reflect the best values of their people, such as the prompt action and followup of your rep L. Fisher who by getting us the rare supplies, helped in achieving this patient’s excellent results. While I believe there is a business case to be made in preserving and relaunching EndoRE, as endarterectomy has proved to be future proof for nearly a century, I believe more strongly that it is the right thing to do.
Sincerely
W. Michael Park
