Distraction Free Writing: Portable, Disconnected, AA Battery Powered
Distraction free writing has been a buzzword. It used to be the norm with computers by their limitations and design to focus you on writing. Today, technology is increasingly put in front of you to entertain and distract. The problem for students and writers is that your computer and phone are gateways to music, video, and communication in ways that were only dreams twenty years ago. The key elements of distraction free writing are a decent keyboard, extended battery life, simple interfaces, lack of connectivity, and absence of party line operators. Each of these elements formed the core of our computers back in the 1980’s, when computers were rarely networked, they were all monochrome, and your words were all that you saw. This desire is driving the market for distraction free writing software and hardware, but you can find ways to create your own portable distraction free writing tools without dropping a fortune. And distraction-free writing is also intrusion-free -something to consider in today’s shifting privacy boundaries. At the end, the best distraction free options may be in reconsidering decades old devices that may be picked up cheaply used or at greatly reduced prices for new. Most current devices are made to last about a thousand recharges, and struggle with purposeful obsolescence. You may find that there are many fine older options that will suit your writing needs while greatly increasing your productivity while avoiding costs.
Consider the keyboards we had back in 1985. They were all mechanical spring keyboards which made a nice click sound. Writing was a tactile pleasure. This was in contrast to the membrane based keys seen on games and toys, and mistakes like the PCjr. You see them today as controls for microwave ovens. The moving keys send a message of accomplishment to your brain. Despite this, flat keyboards with no physical component are still being thrown up to see if they would stick. The smartphone keyboard on the first iPhone killed the physical ones on Blackberry and the Treo’s after all. Manufacturers are still experimenting with flat keyboards such as on the latest Yoga Book’s e-ink keyboard, and the upcoming Microsoft Surface Duo devices.

These software and touch display based keyboards rely on spelling correction and ultimately constant connectivity to minimize error. The push for ultra-portability means dispensing with the original mechanical keyboard which was descended from electric typewriters like the IBM Selectric. This resulted in the terribly mushy, mass produced keyboards introduced in the 1990’s, getting ever worse. The high point of this design viewpoint was introduced in the 2015 MacBook and recently retired in the 2019 Macbook Pro when Apple realized everyone hated typing on superflat keys meant to accommodate flatness over functionality. There is a welcome movement back to reasonable keyboards. I would even claim that the persistent life and value of the Thinkpad line is the focus on the keyboard that remains preserved after IBM sold it to Lenovo. The new-old keyboard on the 2019 MacBook Pro 16’s are a concession to the realization that typing is a core function of these machines.
There is a push back as writers, office workers, and gamers have created a market for mechanical keyboards. These are usually Bluetooth connected devices, and typically paired to tablets for writing. Unfortunately, separate keyboards connected to tablets are not as portable as a laptop. 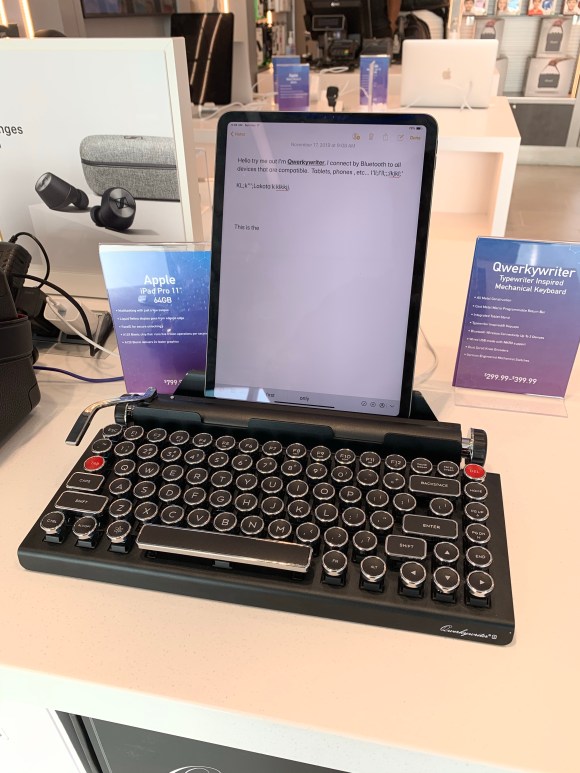
I would argue that laptops are not as portable as they could be. The Freewrite (link) was designed with writers in mind as an update to electric typewriters with cloudbased file management and an e-ink display with days of battery life on a single charge. I almost bought one but the small display and the relatively bulky size kept me from springing. I have ordered a Freewrite Traveler (link) which is their mini-laptop version, but since I ordered one last spring, it has remained vaporware with its delivery date pushed back from summer 2019 to spring 2020.
Battery life is a sore point for me. Laptops are now expected to be wonderful if they exceed 8 hours of battery life, but I remember that the original portable computers like the Radio Shack 100 series could go days on AA batteries. Writing appliances were introduced in the 80’s including electric typewriters with single line LCD displays and single file memory which would allow you to compose and edit. I had such a device from Japan in high school that had a four line LCD display, built in thermoelectric (fax paper) printer, and battery life that went several days on 4 AA batteries.
By using computers and smartphones, which function as portable televisions and multi-function, shopping kiosks which use Watts of power, the trade off is battery life and constantly worrying about plugging in for a recharge. We forgot the days of battery life and are happy with 8 hours. The battery power bar is terribly distracting for me and I tend to stop working to find an outlet to recharge when it inevitably drops and when my productivity is nearly always highest. If I’m traveling, this means carrying the power brick, another injury to this one who remembers AA battery powered writing tools.
In 2017, the Samsung Galaxy Note 7 was famously recalled after spontaneously combusting and were banned from airplanes. All Lithium batteries must now be hand carried. Just recently, I was told while checking in that Apple Macbooks could not be turned on during flight because of heating issues. This is a consequence of the greatly increased energy densities of Lithium cells and their chemical volatility. AA batteries and their nickel metal hydride (NiMH) rechargeable variants suffer from no such problem.
Even with great battery life, you have to remember most of that power, and therefore bulk and weight of the Lithium batteries is devoted to painting vivid colors on the screen, communicating via radio signal to the world, and keeping dozens of apps updated on your activities, and not to writing.
The Lithium battery which can power a car because of its energy density is overkill if all you want is to write. The modern computer operating systems, Windows, MacOS, iOS, and Android, are all over-powered for the simple act of preserving words. Consider the lowly text file to a modern Word file. The text file for a novel might take kilobytes of memory, but the same Office Word file is measured in megabytes -thousands of times bigger. Try emailing a fully formatted Word file through your corporate firewalls if it exceeds your company’s limits on attachment file sizes. The size and complexity of information that is exchanged burns power. Compare that to the notes you might write onto paper. The few microcalories used to power your neurons and move pencil on paper, the motor and optics circuitry processing the information at a speed suitable for your ape brain.
My friend and early mentor, Professor David Tilson, refused to relinquish his DOS based word processor even well into the Windows era. And I understood. The monochrome and monotype letters forced you to look at the words and not the style of the words. While I admire Steve Jobs, and his introduction of fonts to our everyday lives, the ability to shape the look of your writing intrudes on its composition. Monochrome does not mean monotonous, and modern distraction-free software efforts like IA Writer embrace simplicity. The emergence of dark mode is another effort at rolling back the clock. When you enable it for your iPhone, it reaffirms the utility and critical need for focus and simplicity. Do you need millions of colors or just letters on a simple background? While you can change the color setting of your laptop screen or your writing software, the ultimate in monochrome experience is an e-ink display.
The e-ink display is what you see on Amazon Kindles. Originally meant for low power usage, high contrast functions like in store signs, e-Ink is currently used for e-Readers, although there is a niche market for e-ink based displays and tablets which do offer the low power hi contrast display perfect for a focused writing work station – you can find them on Amazon and eBay. Unfortunately, because these e-Ink tablets are run typically on Android, there is no escaping the internet on these, and because they do so, their battery lives are not that much different from standard tablets. What the we need is for Amazon to gift the writers of the world with Bluetooth or wired keyboard functionality to their Kindles and offer a text writer that can be synced to their cloud..
What the we need is for Amazon to gift the writers of the world with bluetooth or wired keyboard functionality to their Kindles and offer a text writer that can be synced to their cloud.
The constant need for connectivity drives software and hardware inefficiency. Writing requires intimacy and privacy. Just as you cannot write while engaged in a shouting match with someone, you cannot write with notifications of arriving messages, pictures, and videos. I cannot write while watching a movie or listening to certain music, but all of these distractions are baked into the function of modern computers and smartphones. This uses up battery life. The devices are in a race to maximize the battery and screen size at the cost of purpose and meaning aside from commerce.
Party line operators were a feature of the early telephone systems. Your locality was serviced by an operator that routed your calls and inevitably your conversations were open to intrusion both intentional and unintentional. When all your work is kept on a cloud server, it really is no different. And it isn’t that hackers that may take all your work. My generation grew up with the Cold War, and its dark tales of thought crimes and writers imprisoned for samizdat -ideas forbidden by a state entity. In a time when your social media is a subject for governmental and not just consumer interest, returning to off line options is something to consider seriously. The meaning of party line operators is in this context wholly changed.
The one feature of cloud based options is the convenience of accessing it across all of your devices. But are you really going to be writing on your iPhone, then on your desktop, then on your laptop, then from an airport kiosk? Your file can be lost during the sync process or changed to a competing version from another computer you were working on. And goodbye work if you get hacked or if your cloud service shuts you down or out. While you write, you have to keep a local version and back up to a nonvolatile storage option.
Not connecting to the internet saves you battery life. It also frees you from taking deep YouTube dives into funny cat videos or answering emails or Facebook posts. The stillness you need to just write is difficult to achieve with a modern laptop, tablet or smartphone. It can be attained with these older devices which people in the know still value decades after they left their boxes. I suggest these options if you are thinking of trying a focused writing appliance (a typewriter!).
Option 1: King Jim Pomera DM100 (link) is best described as a writing appliance designed in Japan adapted for the English speaking market. It is a sleek thin portable that allows one to type words unencumbered by internet. The files on it can be transferred to another computer by Bluetooth, and to smart phones by QR code which is cool. It runs for days on AA batteries, and has a backlit monochrome LCD screen. It is priced on th high end at 392.61, but receives the best rating on Amazon which to me is a 4.5. I never come across 5 star reviews that aren’t fake. One reviewers comment that the keyboard is cramped and takes getting used to. It can be used as a Bluetooth keyboard and stand for iOS devices.
Option 2: Neo 2 Alphasmart Word Processor with Full Size Keyboard,, Calculator
The Alphasmart Neo2 (link) was the last of a line of writing appliances put out by a pair of former Apple engineers who wanted to provide affordable word processing options on a full mechanical keyboard. The Neo2 is the most available and apparently the most usable, allowing one to type out hundreds of pages and transfer to a computer via USB connection. The screen is an LCD screen like on a calculator. The killer feature on this device is nearly forever battery life on AA cells. It has a rabid following of professional writers who appreciate the pared down experience for productive writing. It achieves that perfect 4.5 star rating. This is for a device discontinued in 2007 and sells for about 40-50USD in used condition. Reviewers rave about turning it on and instantly being able to type without bootup, and avoiding distraction by email, notifications, social media etc.
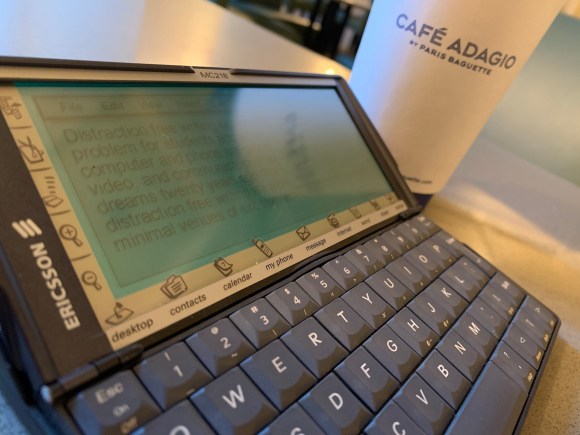
Option 3: Psion Series 5MX
The Psion Series 5MX represented the apex of portable computer design in the late 1990s. It was a computer made from the ground up from circuits, hardware, operating system, and apps by British engineers and it was a thing of beauty. Made in the late 1990’s, this device’s killer features, long battery life via AA cells, ultraportabiity, and lack of easy internet access puts it in a separate class. Not everyone like the keyboard, but I have long been able to type on it without difficulty with average to large sized hands. I had one during residency in the 1990’s and it followed me into fellowship. Before EHR, I composed full consultation notes and H&Ps on it and filed them on my password protected CF drive for later retrieval and update for frequent flyer patients. I picked up a pair of these for about 90USD from the Netherlands, but the going priced varies from about 70 to 200USD for a used one in good condition. New ones pop up but they go for nearly their original price -they are that good. I suspect I got a deal because they were Ericsson MC218, a Swedish licensed clone.
It has a compact flash drive, and with the save as text file function in the built-in word processor which works fast and reliably, it is possible to back up to a nonvolatile memory (the CF drive) and transfer to a regular computer. The one caveat is that the maximum size of CF drive it will see seems to be 128mB -that is megabytes which is hard to find. In certain older industrial machinery, instructions are uploaded via CF cards of these size, and so these cards are available on Amazon. Or look in a drawer for an old unused CF card.
I wrote this post on the Psion, and never once looked at emails, social media, or Youtube.











 They opened a branch in Manhattan, but my kids say it wasn’t as good as in Brooklyn. I can’t imagine what it must be like at the original store in Japan, but I am planning an entire trip just to eat ramen.
They opened a branch in Manhattan, but my kids say it wasn’t as good as in Brooklyn. I can’t imagine what it must be like at the original store in Japan, but I am planning an entire trip just to eat ramen.