In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.








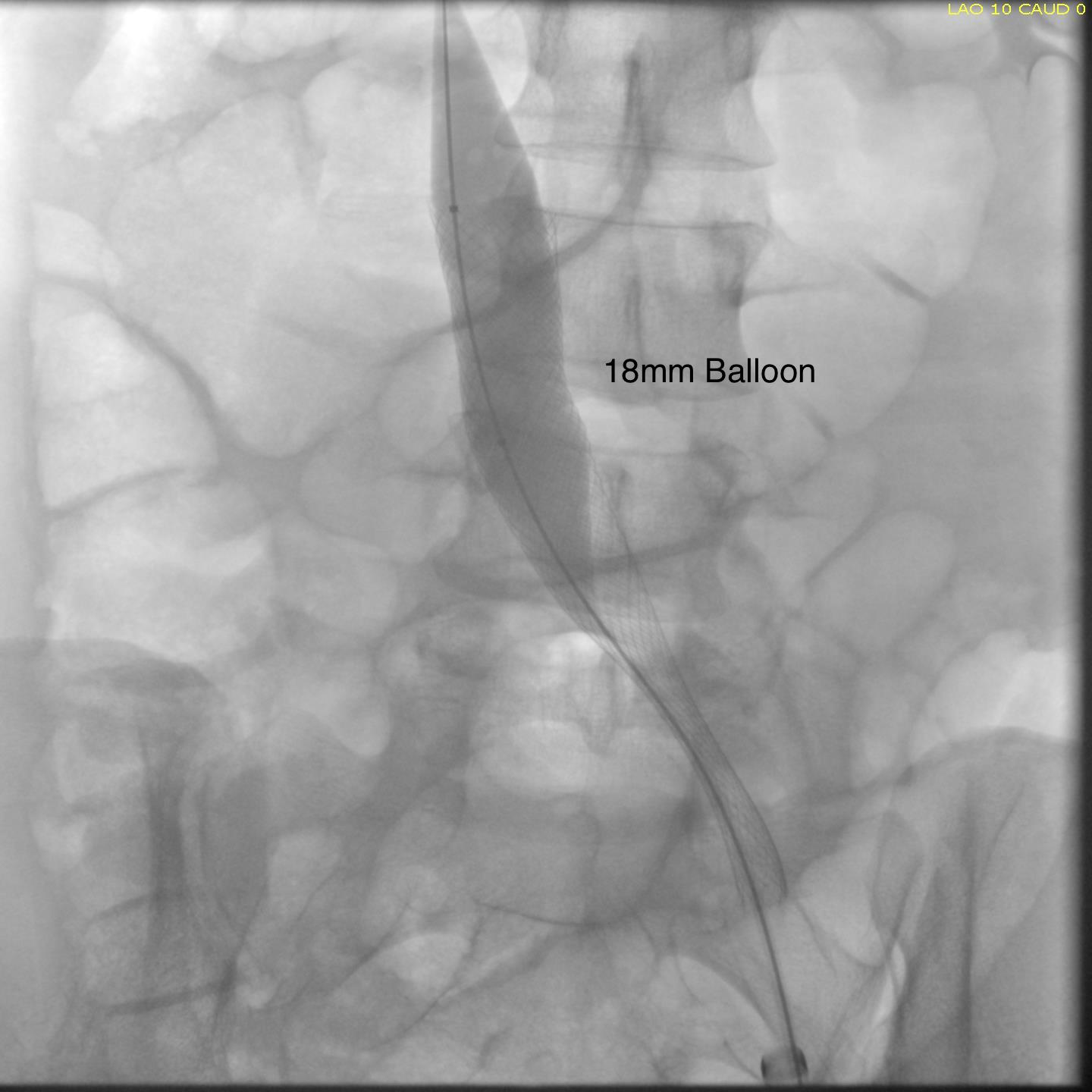
 The patient is a young woman who three weeks prior to presentation developed sudden low back pain and left leg pain while exercising on an elliptical. This pain worsened through the subsequent weeks and she developed fevers, chills, and night sweats, and she came to the emergency department. There, she was found to have left thigh and leg swelling. Duplex revealed a left iliofemoral DVT starting from the iliocaval tributary and extending to her left femoral vein (figure above). A CT scan revealed a pulmonary embolism to the left lung (below). No precipitating factors were present. Vascular surgery was consulted.
The patient is a young woman who three weeks prior to presentation developed sudden low back pain and left leg pain while exercising on an elliptical. This pain worsened through the subsequent weeks and she developed fevers, chills, and night sweats, and she came to the emergency department. There, she was found to have left thigh and leg swelling. Duplex revealed a left iliofemoral DVT starting from the iliocaval tributary and extending to her left femoral vein (figure above). A CT scan revealed a pulmonary embolism to the left lung (below). No precipitating factors were present. Vascular surgery was consulted.