
The patient is a young woman who presented with classic symptoms and findings of median arcuate ligament syndrome (MALS). She avoided food because eating triggered severe pain in her upper abdomen. Over a year, this resulted in 15 pounds of weight loss. As a result, she no longer had the energy to work or exercise. She had an extensive gastrointestinal workup including blood work (LFT’s, amylase, cholesterol panel), abdominal CT scan, and upper endoscopy which were normal except for the finding of narrowing of the celiac axis due to compression by the median arcuate ligament. Examination was notable for upper abdominal pain exacerbated by pressure and seated, hunched-over posture. Unfortunately, due to her health insurance, surgery was not covered and she did not want any. So I recommended she try the following.
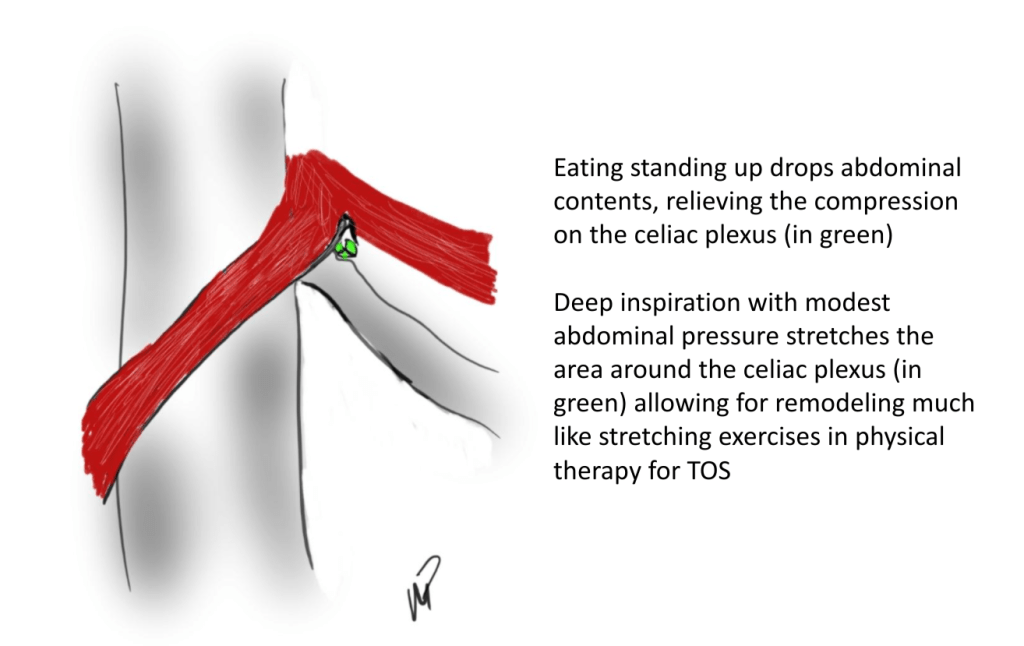
- Eat standing up with good posture, shoulder back, back arched, taking deep breaths and holding once food passes
- Practice upward facing dog yoga pose (figure) 5 reps daily with deep inhalation breath holds. If this is difficult, do this standing up.
- Improve the posture during seated work, never hunch over and pressed forward with “shrimp back,” periodically take a deep breath and hold with excellent posture.

Over the past several years, I’ve noted that most patients respond to this, even in acute MALS pain situations (yes, there is acute MALS like slipped discs, for another post). That patient came back a few weeks later reporting that she was able to eat more food, more frequently. She also acknowledged compliance with the exercise and postural adjustments at work. A month later she reported regaining her lost weight and only mild pain with sitting in a car for a long time. She was still eating standing up, and she was grateful for having been treated without surgery.
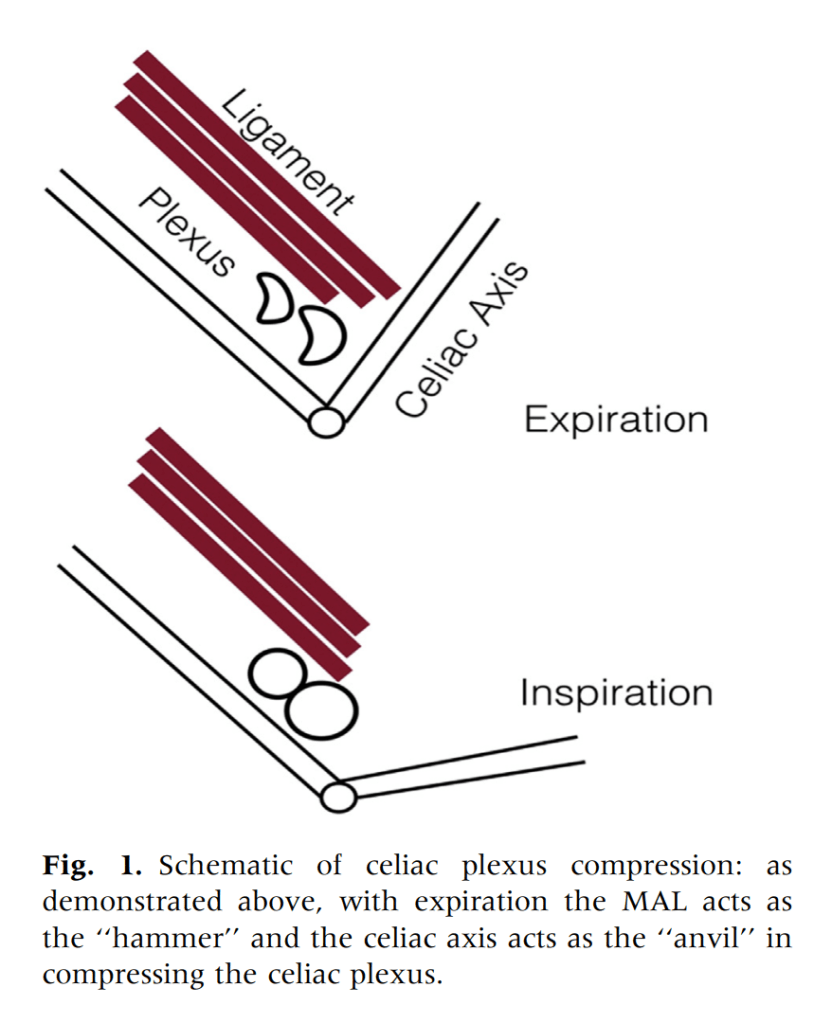
We have postulated that MALS is a nerve compression syndrome of the celiac plexus by the median arcuate ligament (reference). There are two consequences to MALS, neither of which is mesenteric ischemia. The first is this compression of the celiac plexus with injury resulting in inflammation and fibrosis, resulting in further compression and a neuropathy of the celiac plexus. This neuropathy triggers aberrant pain sensations in response to eating. The other consequence is remodeling and injury due to arterial compression. The celiac axis can develop post-stenotic dilatation, growing large enough to be considered aneurysmal. The compression can damage the intima resulting in dissection. The artery can be injured and a pseudoaneurysm can develop. Finally, the aneurysmal segments may develop thrombosis and be the source of thromboembolism, usually to the spleen. Even when the celiac axis clots off, unless there has been resectional surgery such as a Whipple or splenectomy, the stomach gets enough collateral flow that ischemia is rare when celiac axis occlusion occurs. So similarly to thoracic outlet syndrome (TOS), there is a neurogenic MALS and an arterial MALS.
The first line of therapy in neurogenic TOS is physical therapy. With symptomatic MALS, I wondered if there could be physical therapy as well. This young woman and others I have managed nonoperatively suggests good response in some, and partial response in most to exercises and maneuvers designed to address the compression.
Currently, in lieu of celiac plexus block, I have patients treat their MALS nonoperatively using the above protocol for 2-4 weeks, typically while they undergo further workup to rule out more common gastrointestinal etiologies of their abdominal pain, and many have been able to improve their circumstances with these measures alone. This patient chose not to have operation as she was able to live symptom free and regain lost weight with these recommendations alone.

Addendum
I received a comment from Ms. Suzanne Peek, president of the National MALS Foundation, who correctly pointed out not everyone presents in this way. I agree each patient undergoes a unique journey that is often marked by diagnostic delays because this is a rare condition. As I stated, not every patient responds to this regimen and after work up typically will undergo surgery to which in our published results 85% have a positive response to when diagnosed with MALS. Is certainly an area of further study to see if more people can respond to this non-operative approach. Our previous protocol which we instituted after the publication of our report was to use celiac plexus blockade as a diagnostic study and occasionally permanent blockade as therapy for those with prohibitive operative risk. A positive response to this regimen may signal a positive response to surgical celiac plexus ablation.
Reference
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.

15 replies on “Nonoperative management of median arcuate ligament syndrome (MALS)”
I have MALS – pain left and right side
They said also o have IBS and to remove the gallbladder too ( no stones ) the contraction fraction ! I’m not so surgery friendly ! Would love to schedule an appointment
LikeLike
My office number is +1-216-844-3013
LikeLike
Where is this doctor located?
LikeLike
I am practicing at University Hospitals of Case Western Reserve University in Cleveland, Ohio.
LikeLike
Do patients with MALS usually need more than one surgery?
LikeLike
About 5-10 percent patient have recurrent MALS and respond to a second release if compression demonstrated in CT or duplex. If there is no compression but a stenosisnin the celiac, I have had response with stenting the celiac. Finally there may be some degree of causalgia type neuropathy that may need long term care with a pain specialist versed in abdominal pain syndromes.
LikeLike
How often do patients with MALS need a second surgery or more for any related/extended treatment?
LikeLike
I woke up one morning 2 years ago with intense left sided low back pain. After seeing several drs with no answers and mris I went to a spinal surgeon who suggested I may have a compression that’s causing my pain and referred me to a vascular dr. I went to a different vascular dr who said I have no compressions based on pelvic ct scan. I went to er for chest pain weeks later and they found the compression via ct scan. I was told by my dr this type of compression could not interfere with my back and because I don’t have pain after eating not to worry. I’m starting to get circulation problems in my legs now. Could this be all connected to this type of compression?
LikeLike
Have you seen any cases in which the opposite was the case and that standing (or sitting) up straight and/or deep breathing brings on or worsens symptoms, and hunching relieves it?
LikeLike
Yes. But there has to be a mechanism for the pain. A reasonable explanation, a theory of the disease.
LikeLike
This is almost too good. Do most patients find relief by stretching and eating standing up. Any food to avoid?
LikeLike
My son has severe POTS. He also has MALS. But little to no Gastro symptoms. Could the MALS be causing his POTS? Trying to determine if surgery may be a good idea. Everything I see involves patients w both POTS and Gastro symptoms. I cannot find any case reports where MALS patients w only POTS had surgery.
LikeLike
This is amazing but I just have one question. Why does hunching over not help. I thought that would loosen everything giving relief as opposed to standing up that stretches everything, that would apply pressure.
LikeLike
This sounds amazing but I have one question. Why does hunching over make it worse. I thought that would loosen everything providing relief, as opposed to standing that would stretch everything applying pressure.
LikeLike
Like anything in medicine, it depends. There are some people who find relief with balling up. For others, sitting hunched over at a desk or in a car drives the organs and the celiac axis upwards and pinches the nerves, resulting in more pain.
LikeLike