

Being a homeowner, you are sometimes stuck negotiating a repair with various workmen whose knowledge of building esoterica is only exceeded by their subliminal contempt of a man who can’t rip out flooring and drywall to renovate a kitchen or bathroom. I can only hope that I don’t come off that way when discussing human plumbing. It was a year into my ownership of my current home that I noticed that many of the drains in the window wells were clogged. A very unpleasant afternoon was spent digging out soil and leaves while trying to snake a coat hanger (access wire), and when I gave up, I tried to call a plumber. Only it was the wrong specialist. “You want a sewer guy.”
The sewer gentleman was a meticulously groomed Italian immigrant who walked about the house after inspecting the drain in question. After some harumphing, he declared he needed to do some tests which included running dye through the various downspouts around the house and drains in the house. Contrast drainography! To top it off, he wanted to run a camera on a flexible tube through to check out the drains. Endoscopy! Plumbing, he sniffed, was easy, but drains were an art.
For the record, our basement was dry, but I could see the money meter whirring away. It was only a few weeks removed from a spring storm where several homes a few blocks away had catastrophic flooding when rains overwhelmed the capacity of their drainage –Drainage Insufficiency!
The testing was fine, but he ended up recommending resealing the entire East side of the house and rebuilding the window wells, because while the house was dry, it was compensating by rerouting a lot of drainage down gutters and the downsloping lawn to the street –Collaterals! and he couldn’t promise the house wouldn’t flood with a torrential month of rain which Shaker Heights is prone to being downwind of the Lake.
And it is with this wisdom that I see the increasing numbers of chronic venous occlusions. For example, the patient whose venogram is pictured above initially complained to her obstetrician of persistent heaviness in the pelvis and swelling of the legs after delivering a healthy baby. MRV showed abundant pelvic collateral veins and she was referred to me.
Our first test in our clinic is a venous duplex of both legs and the abdominal veins. There was an occlusion of the inferior vena cava below the renal veins extending the the iliac veins bilaterally. I am about to give a talk on this and I composited the ultrasound.

She had iliocaval occlusion, chronic. Her symptoms were over two years, and were ever worsening. She hadn’t developed permanent skin changes of chronic venous insufficiency, but probably would in a decade or sooner. I recommended venography and an attempt at recanalization.
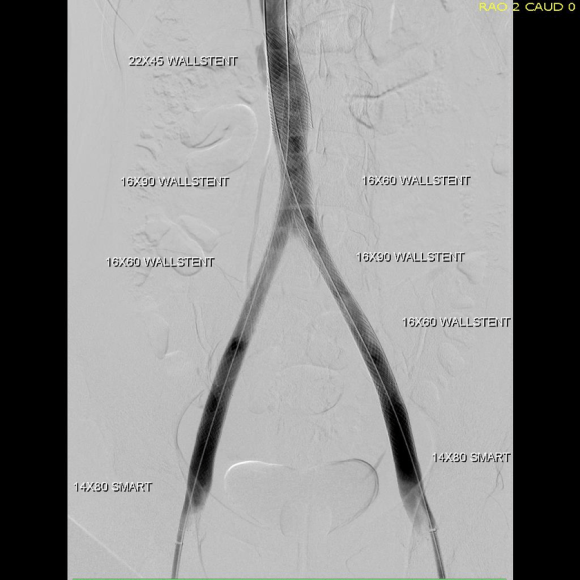
The procedure went well, and her symptoms abated. For my trainees, the absence of collaterals in the after image is the sign that hemodynamically, the revascularization is the preferred route of egress. Surprisingly, this has stayed open over two years, but again, my exceedingly well paid sewer gentleman consultant, had something to say about it.
Drainage, he declared, was different from plumbing, because things move slower and there is usually solid matter -poop, leaves, dead birds, etc., to contend with. Larger, high volume drains do best with a direct in-line connection with the city sewer, while downspouts and window wells with their twists and turns and only occasional flushings clog up too well. Wise words.
It gave me a reason why iliocaval venous interventions did so much better than femoropopliteal ones.

Venous interventions connect confluences to the main drain, in most cases the suprarenal inferior vena cava. The iliocaval segment drains the common femoral confluence, which even in the worst of chronic lower extremity DVT’s, seems to reopen with several months of anticoagulation. Not the same for the popliteal confluence which, getting much less blood flow to drain, and having a smaller diameter, stents in the femoropopliteal veins just don’t do as well. Plus, it has to drain against a greater hydrostatic pressure. The drain guy’s wisdom seems to apply. It also has implications for the kind of stents we place, and the kinds that are being developed specifically for the venous side.
