The patient is an elderly woman who had severe rest pain due to popliteal artery and tibial occlusion. She had no leg veins and sparse arm veins which would have to be spliced to achieve a femoro-peroneal bypass. Her preop CTA showed a patent SFA and proximal popliteal artery occluding above the joint and reconstituting only the peroneal artery. I planned for a retrograde popliteal remote endarterectomy tibioperoneal trunk endarterectomy via a below knee exposure with patch angioplasty of the arteriotomy, the bailout would be a short arm vein bypass from the above knee popliteal artery to peroneal artery.
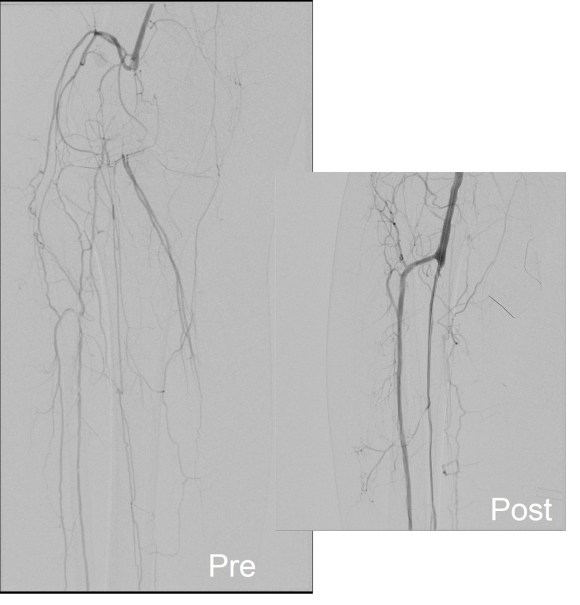
Arteriography was performed via a left common femoral access and is shown below.


The popliteal artery was occluded and there was a very small peroneal artery that continued down the leg with seeming occlusion of the anterior and posterior tibial arteries. The popliteal and anterior tibial artery were exposed through a below knee incision taking care to avoid venous injury which can be troublesome source of bleeding. The tibioperoneal trunk down to the bifurcation and origin of the peroneal artery was exposed through the same incision. And anterior tibial artery origin was controlled with a vessel loop largely out of habit although it seemed clear it was occluded, as were the proximal popliteal and tibioperoneal trunk branches. The arteriotomy was created from the tibioperoneal trunk to the popliteal artery and endarterectomy was performed from distal to proximal to create a starting point for the ring dissectors used in remote endarterectomy. The anterior tibial plaque branched off much like an external carotid artery plaque and I decided to see what would happen if I did an eversion endarterectomy. I was able to mobilize a short length of the artery and was able to pull as I endarterectomized around the plaque and it thinned very nicely and came out with a gossamer end point. More gratifyingly, the backbleeding was excellent –this was controlled with the vessel loop very nicely. The retrograde popliteal endarterectomy was performed as described in another post in another case –link. The artery was then patched and completion arteriography was performed.


What was fascinating was it seemed I had reopened not just the pop-peroneal axis but the anterior tibial artery was also open, very dramatically so. The patient also had a bounding dorsalis pedis artery pulse. She recovered and went home two days later and in three years of followup while I was still in Iowa, she remained widely patent, maintained on Coumadin anticoagulation.
Popliteal endarterectomy for localized popliteal artery disease has been described (reference) with decent short term patency and successful limb salvage. Nasr et al. performed their endarterectomy via a posterior exposure. I think I recall coming across this in a book chapter from the old Wylie textbook which is long out of print. I think that the anterior tibial artery never lit up well because it was part of a highly developed collateral network, but it was patent all along. Duplex which was not done, would have given a better indication of its patency. I think that the patency of the popliteal endarterectomy is related to its relative shortness and in this case, the added outflow cannot hurt.
Reference
Nasr H et al. Popliteal endarterectomy for localized popliteal artery disease. Ann Vasc Surg 2014 (in press).