I recently had lunch with Dr. PJ O’Hara, emeritus professor, and former partner of mine from the Cleveland Clinic. We hadn’t met since 2018 at the VAM in Boston, while I was still in Abu Dhabi. It was a recent case I did that caused me to reach out. I won’t be posting that recent case in detail today -it was a patient who had had multiple aortoiliac interventions for aortic bifurcation disease, but who closed up their stents within a few months of intervention. Rather than subject that patient to another round of interventions, I chose aortoiliac endarterectomy because the prior interventions failed to address the basic problem of the undersized aorta and iliac arteries.
The last case that Dr. O’Hara did before retiring was an aortoiliac endarterectomy which I assisted with, nearly a decade ago. During that case, Dr. O’Hara mentioned a video he had put together for an SVS meeting. He was kind enough to give me a copy share.
Aortoiliac endarterectomy -forget thee not!
The modern application of this technique is in the removal of occluded aortoiliac stents. The aorta and iliac arteries are restored, and yes, stents can go back in if needed.
A quick survey of some of my contacts at major centers reveals that this technique is rapidly becoming forgotten as its practitioner retire or revert to teaching the technically easier aortobifemoral bypass (ABF) graft. I hope to revive this because I know there are many patients who have challenging anatomy for ABF but potentially could undergo plaque and stent removal and restoration of their aorta and iliac arteries.
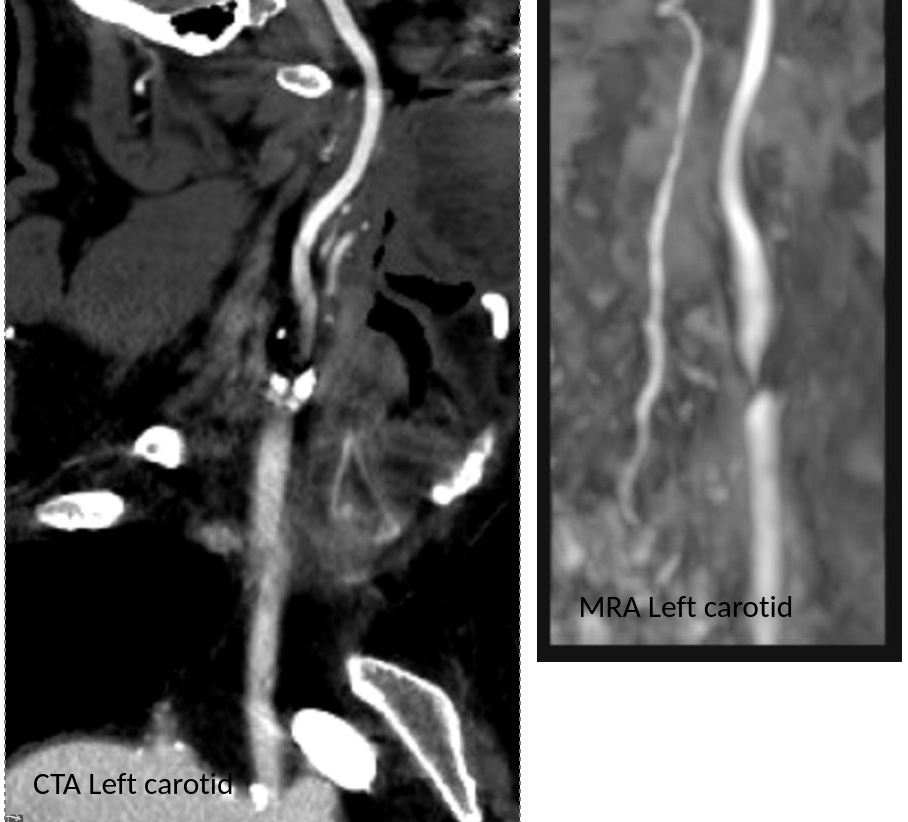
CTA tends to overread stenoses which was in the 60-79% range on duplex
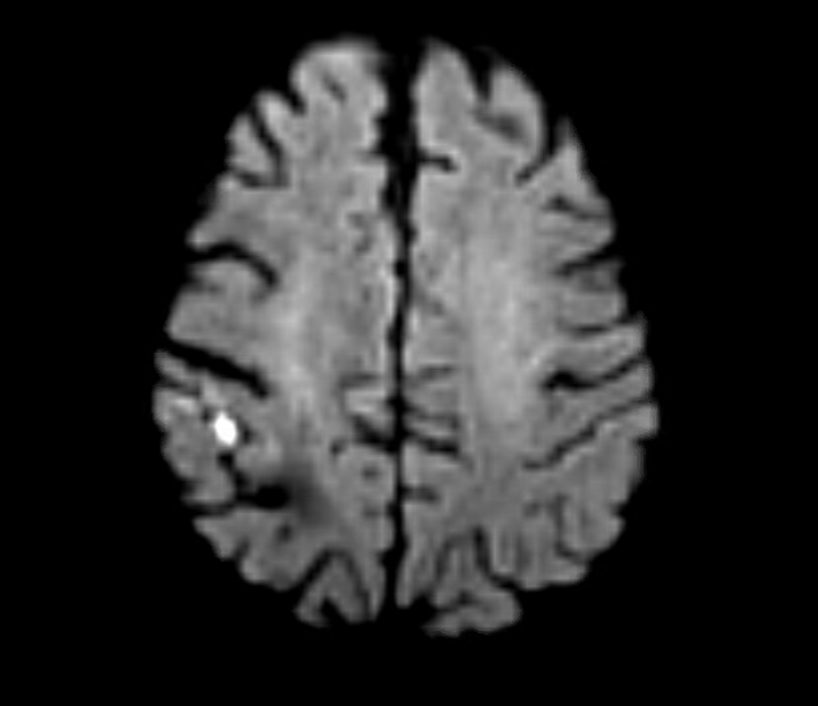
The patient is a middle aged executive who complains of bouts of aphasia triggered by intense conversations and business meetings. It first occurred while driving to Dubai on a conference call. Since then, they occurred several times a week, typically triggered during meetings where he needs to think and speak. Casual conversation and cognition does not seem to trigger this. Workup revealed a heterogeneous plaque affecting the left ICA with velocities in the 60-79% range. CTA confirmed this plaque. MRI failed to show any stroke or other lesions. Neurology evaluation showed normal exam. The patient underwent endarterectomy, and had a normal recovery. In followup, he denied any further episodes of aphasia.
Standard endarterectomy with patch
Aphasia, the loss of function in the language centers, typically of the left brain, although in a minority, it may live in the right hemisphere, is terrifying manifestation of stroke. This case, if examined superficially, is nothing special in that TIA’s associated with a reasonable culprit lesion went away after elimination of that culprit lesion. To me, it was fascinating because it represents a possible case of brain claudication.
The human brain is believed to have evolved to its large size in conjunction with bipedalism, social hunting and gathering, and climate change in the Great Rift Valley favoring a savannah over forests, that created heat stresses on the brain, favoring the development of sweating and redundancies in brain tissue. The advent of fire and cooking enhanced available calories to feed this enlarged brain’s metabolic needs. When the metabolism isn’t supported through adequate blood supply, the brain tissue dies. Rarely, it blinkers on and off, and even more rarely, this occurs in the motor strip triggering today a neurologic evaluation including a carotid duplex that brings these patients to our attention. The fascinating question for me is, does increased metabolic demand in the form of complex thinking result in a supply-demand mismatch much as seen in exercise induced angina or claudication? If it can, can we test for it?
The tests we have available are hemodynamically based. At its simplest, after carotid angiography, an occluding balloon can be inflated to test for symptoms. This is an archaic test and I do not do it. There are nuclear medicine, PET CT, and MRI tests that use pharmacologic agents to induce hypotension, but again, for this patient, it wouldn’t apply. This patient needed the equivalent of a treadmill in the MRI machine. Maybe having him read a dry, technical treatise on neurobiology taped to the MRI tube?
I went to the OR with the indication of TIAs associated with a >50% lesion, but I did tell the patient that it was possible his thinking-induced aphasia would not remit. Thankfully it did.
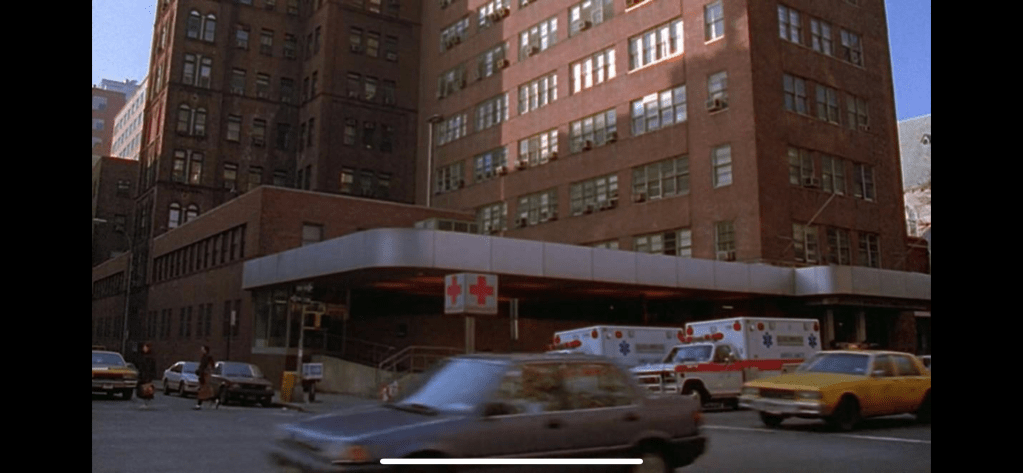
Every time someone on Seinfeld went to the hospital, a stock scene (above) would play. It’s the old ER of Roosevelt Hospital on 9th Ave before the renovations moved it to current 59th street entrance. I was a surgery resident there in the 90’s and watched each Seinfeld episode for the upper West Side stuff that would pop up. The soup Na2i was a few blocks over. Not seen on this pic is the Sym’s operating theater designed by Dr. Charles McBurney which is a designated landmark and currently a private school for “gifted but difficult” children (link). I used to round on patients in the red building -they would be ten in a room separated, if lucky, by rolling privacy screens. My sister was born here. John Lennon died here. All that gone, because hospital buildings are like dressings on a city’s wounds and need to be changed every generation. In fact, it’s not even called Roosevelt Hospital any more.
Roosevelt Hospital’s name was changed to Mount Sinai West, and its sister hospital, St. Luke’s, was changed to Mount Sinai Morningside. I would like to imagine that it was vengeance a century in the making, for pearl clutching slights originating from the gilded age, of blue bloods v. upstart Jews. Because no matter how far you are from the shtetl, there is always another golden door closed to you in New York City. So it seemed for me, an immigrant who had worked hard to get to Harvard College, and Columbia P&S, to look with squinted eyes at my letter on match day and see St. Luke’s/Roosevelt Hospital Center, my last choice that I listed out of a general interest to avoid not matching.
When I landed on St. Luke’s-Roosevelt for my general surgery training, the house officers were quartered in the older parts of the hospital, some rooms dating back to the 19th century, unchanged like unearthed chambers from Pompeii. Both hospitals still had the open wards for the “ward” patients with segregation of the private patients up in the towers. For a time, they still had seamstresses to mend your white coat and cafeterias that still cooked their foods fresh. The resident’s lounge at St. Luke’s was like a frat house common room from the thirties, with a scratched-up pool table, a broken piano, pedastaled hotel ashtrays, and card tables. An old handprinted sign (which I regret not taking) listed the house officer’s rules and entitlements which included two beers or a shot of whiskey per night on call.
After my intern year, both hospitals started sorely needed renovations. The surgery office had to be cleaned out, and behind an antique cabinet, wooden boxes of chromic cat-gut suture were found, still in their glass tubes and preserving fluids, little brown skeins of suture floating like preserved fetuses, a strange message from a faraway time. I ran into Walter Wichern, chairman emeritus, who showed up randomly to the hospital in blue blazer and bow tie. I had just stained my dress shirt pocket with my soon-to-be-lost Mont Blanc fountain pen, and he launched into a story about how he repaired a ruptured aortic aneurysm back in 60’s by cutting his new polyester dress shirt into a tube and sewing a graft out of it down in the laundry, after hearing a talk from Arthur Vorhees at P&S. And he was smiling an enigmatic little smile, recalling how that patient on being discharged gifted him annually with ten new dress shirts every year. I later found out that Dr. Wichern was famously taciturn, and I had somehow unlocked an achievement -getting a story out of an old surgeon. It was around then that I had started to feel that it wasn’t all a big mistake.
When I recently changed hospitals from the Cleveland Clinic to University Hospitals, I had to submit documents for privileging, and I get a testy email. “Where did you do your residency?” The administrator couldn’t find St. Luke’s/Roosevelt anywhere on the ACGME website, or even on Google. When I offered the new names, the reply came back, “They only have records going back to when they took over in 2008.” I briefly contemplated retiring, then asked if sending pictures of my framed degrees would be sufficient. Only partly, was the reply. She wanted witnesses.
My first night on call was terrifying. I was on call with Bobby Borromeo -my fellow intern, Anil Hingorani -our PGY4, and Jesse Jean-Claude -our Chief Resident. All of us are now practicing vascular surgeons -Bobby (fellowship Yale), Anil (fellowship Montefiore), Jesse (fellowship UCSF), and myself (fellowship Mayo), embarked on a night of call that involved no sleep and little food. The single moment I recall was taking Bobby through a blood draw and filling the forms for processing the labs and performing EKGs with an antique strip recorder, cutting and pasting the strips onto a formatted sheet for the chart. Bobby didn’t know how because there were many people to do these things in his home hospital in the Phillipines. For myself, I knew the two hospitals from my rotations during medical school. I could draw blood and cut, sew and tie above my level from my time as a senior student at P&S. I got a bit too comfortable with my privilege, and I was still thinking I should have been somewhere else. Over breakfast, I absentmindedly voiced this out loud and was corrected in a way that is no longer possible in 2022. It was the tone that I remember, of being chewed out.
One of chiefs snapped at me,”You have no idea how big and important these hospitals are. They are older than all the other hospitals here in NY. McBurney did the first appy here. Halsted was chief at Roosevelt and invented cancer surgery and the surgical residency. Green invented the LIMA bypass at St. Luke’s. Our chiefs go to better fellowships year over year than any other hospital in Manhattan. You should be grateful to be allowed to round with us.”
Tie given out at graduation, designed by Howard Nay, MD (link), RIP. One of the few keepsakes of my time there. Dr. Skip Nay, was old school, and gave everyone nicknames. Learning surgery from him was like taking blues guitar lessons from Mr. Robert Leroy Johnson.
It was by my third year I got used to the 120 hours a week. It is only now a quarter century later, that I value it. I was expending my. youth living and breathing surgery in the latter days of St. Luke’s and Roosevelt Hospitals. I was missing my friend’s weddings, missing time with my wife, seeing New York during the glory of the 90’s through the dank recesses of a trauma bay. I was six figures in debt, but I could take out your appendix in twenty minutes. I had just signed on for a year of research with the peerless Dr. David Tilson and was not looking forward to telling my wife who found the original five year deal of residency interminable. Add to that, two years of fellowship. Walking out on the deck of the call room overlooking the Cathedral of St. John the Divine and Columbia’s campus, listening for the sirens, I really felt the spirit of the hospital.
It’s not the name of the place, neither its splendor nor its comforts, but the commitment of the people in the teams that you build, which allows you to do great things. And yet…
Summer 2022, in front of Mt. Sinai West, formerly and forever Roosevelt Hospital.
A New Day -created by @nightcafestudios AI upon my suggestion.
Ten years ago, I joined the Cleveland Clinic. I worked five years at the main campus as teaching faculty. I learned as much as I taught, as I got to apply the accumulated volume of experience and knowledge from the previous decades in New York, Rochester (MN), and Des Moines. Five years ago, I took myself and my family to Abu Dhabi, and started a vascular surgery program at CCAD (Cleveland Clinic Abu Dhabi). Last year, still in the middle of the second year of the pandemic, we returned, and I had the privilege of working at Cleveland Clinic Fairview and Cleveland Clinic Avon on Cleveland’s west side. This spring, I made the decision to join University Hospitals, where I will be starting this August. I crave these new days and am so grateful to have them. Thank you, Cleveland Clinic, for ten amazing years. Hello University Hospitals! I can be reached at docpark(at)golfism.org during this transition.
Steve Jobs is credited with popularizing the saying credited to Pablo Picasso, “good artists copy, great artists steal.” While its provenance may be apocryphal, it makes an excellent point about how we learn. Even in the lack of understanding, it is still possible to learn by copying. Toddlers do this. We, as land mammals, are hard wired to copy.
Take for example this patient below with Leriche syndrome with a triad of smoking, claudication, and impotence.
Aortoiliac occlusive disease with history of smoking, claudication, and impotence in a middle aged man = Leriche Syndrome
Because of his relative youth, being his 50’s, I felt the most appropriate procedure was an aortobifemoral bypass.
I frequently use these diagrams to illustrate for the patient.
The only real complexity to manage was the severe stenosis he had in his left renal artery.
A severe stenosis of left renal artery
The options included
renal endarterectomy as part of aortic thromboendarterectomy
renal artery bypass from the aortic graft
reimplantation of renal artery
something else
Something Else: The complexity of renal revascularization creates risk. An antegrade endarterectomy of the renal artery would be done below a suprarenal clamp, adding to clamp time. A bypass would require the kidney to bide its time during the proximal aortic anastomosis, and the anastomosis for a jump graft, then the anastomosis to the left renal artery. This renal ischemia time can be extended by cooling the kidneys with cold (5 degree) LR, but why risk it? A renal endarterectomy can devolve into a visceral segment endarterectomy. After an hour, a nephrectomy.
That’s where this whole copying concept comes into play. Back in 2012, I worked with Dr. Jeanwan Kang, who had just come out of training with Dr. Richard Cambria. We were doing a type IV thoracoabdominal aortic aneurysm, and the right renal artery had a ostial stenosis. While I was figuring out the best way to manage this, Dr. Kang asked for a 6x18mm renal stent and an insufflator. She stuck the stent into the renal orifice and deployed the stent, opening the orifice. I had to find my jaw which had dropped to the floor.
Now, ten years on, that’s how I managed this patient’s ostial renal artery stenosis.
The patient’s thrombotic plaque went up to the renal origins and needed to be endarterectomized, but embarking on a renal endarterectomy adds potentially harmful renal ischemia time. Therefore, through the vertical aortotomy, I was able to get a clean end point to the aortic thromboendarterectomy and position a stent in the renal orifice and deploy it.
After thromboendarterectomy of the aortic plaque, the left renal ostium is treated with a balloon expandable stent. The aorta then is partially closed primarily to move the clamp below the renal arteries
Once the stent was deployed, the aorta was partially closed primarily to allow the clamp to be moved below the renal arteries. This all took less than ten minutes of ischemia time. The aortic graft was then sewn end to side to the remaining aortotomy.
The patient recovered and was discharged on POD#6 with normal renal function. In followup, his CTA showed excellent graft and stent patency.
A followup CTA shows a patent 14x7mm aortobifemoral bypass. I choose the bypass based on avoiding excess size mismatching distally as I find that patients who get 20x10mm grafts run into problem with mural thrombus because of limited flows into smaller femoral vessels. The renal stent is patent.
The centerline view of the renal stent shows it to be widely patent.
Patent stent with avoidance of the pitfalls of a renal endarterectomy
The patient is walking well without limitations and has improved blood pressure control, achieving normotensions at times.
If you are curious about the results from MGH, I refer you to their paper on 67 patients treated with open hybrid revascularization of the renal artery during complex aortic reconstructions (reference). At a mean followup of a year, they reported a 98% stent patency.
There is a comfort in sticking to what you know. The extreme example of this is the practitioner who graduates with a skill set from training and never expands on it. Yet there is an opportunity cost to blind devotion to sticking what you know and that is never growing. I recall this in the panel discussions during the VEITH Symposia I used to sneak into as a resident in the 90’s where great authorities pooh-poohed or condemned anything endovascular.
It’s a sign of a nimble mind that Dr. Cambria, after learning endovascular techniques mid-career, adapted these skills to his open surgical toolkit. His trainee, Dr. Kang, soon after, taught me.
Or was I just looking over her shoulders taking notes?
Reference:
Patel R, Conrad MF, Paruchuri V, Kwolek CJ, Cambria RP. Balloon expandable stents facilitate right renal artery reconstruction during complex open aortic aneurysm repair. J Vasc Surg. 2010 Feb;51(2):310-5. doi: 10.1016/j.jvs.2009.04.079. Epub 2009 Oct 22. PMID: 19853403.
Look again, it is a doodle of a CT scan of a patient with an Ancure stent graft with sac shrinkage
I remember in the mid-2000’s, driving very fast to Lutheran Hospital in Des Moines on a Saturday night to fix an aneurysm that had ruptured. He was a man over 70 years of age with a type III endoleak from a component separation. The endografts had been placed by a cardiac surgeon who had taken some courses. I rescued him by open replacement of the aneurysm with a tube graft after I pulled out the endografts. Later, as the patient recovered, I asked him why he never followed up as required on his stent graft. His answer was, in typical Iowa farmer fashion, “Welp. If it was fixed, why should I?”
Indeed, why should he? Looking at his chart from the time of his EVAR, he was determined to be a “high risk” patient, necessitating the new minimally invasive procedure EVAR in 2003. Seeing that he survived the stress test of a ruptured aneurysm, it was clear he was not all that “high risk.” I did reassure him that with the open repair, he was basically cured. Despite scheduling a followup appointment, he never showed up. And that was okay.
EVAR is a treatment for AAA, but currently not a cure. All of the devices instructions for use stipulate the need for lifelong followup with CT scans with contrast and visits with qualified specialists. As I have mentioned in the past, what other condition requires surveillance CT scans with contrast and followup with a specialist? Cancer in remission. For those with good cardiac risk and functional status, placing an endograft rather than open repair creates “Aortic Aneurysm in Remission.” If they are in the majority of patients with a stable aneurysm sac, their endografts are sitting in a bag of static, aging blood. If there are type II endoleaks, and it is my belief that the majority of stable aneurysm sacs have some type II endoleaks that blinker on and off depending on the hemodynamics, particularly through needle holes, they are circulating the products of breakdown of that bag of old blood and exposing a perfect culture medium to potential inoculation. These type II and IV endoleaks can inflate the aortic sac over time. Occasionally, the residual AAA sacs rupture, erasing any of the early advantage conferred by the minimally invasive index procedure in long term followup EVAR v OPEN repair.
What is a cure? A cure is when you quell an infection with an antibiotic. A cure is when you’ve taken out an inflamed appendix. It’s when you’ve eradicated early stage cancer. It’s when you perform an open aortic graft and the patient can disappear after you remove the dressings and never followup, sure in the knowledge that the aneurysm in that spot will never bother them again. With EVAR, only a minority get to the state (figure at top) a sac shrunk intimately around the endograft. Most are not cured but enrolled in a regime of lifelong surveillance and maintenance.
EVAR does allow people to leave the hospital with less scarring and pain, but the consequences of its popularity are:
1. Letting more practitioners, not all of them vascular surgeons, treat aortic aneurysm disease with less training and with less or no ability to manage the inevitable failures surgically.
2. Creating the business model for “Advanced, Minimally Invasive, Super-Fantastic Aortic Centers of Excellence” which is predicated on the business of surveillance and maintenance of aortic endografts. It is a busy-ness that generates revenue, but burdens the country with more healthcare costs. It ultimately siphons business away from true centers of excellence involved in training the next generation of vascular surgeons.
3. Skewing the training curriculum of trainees to endovascular so much that I have met vascular surgeons who have done no aortic operations. That was the case when I sat in on an open aortic surgery class at the 2017 ESVS meeting in Lyons, France. All the attendees were very eager to try sewing anastomoses, but felt they needed proctoring which isn’t available.
4. Establishing the expectation that open aortic surgery is a failed, antiquarian, obsolete technique to be relegated to the history books. This last one is infuriating and not true but it is out there in the claims of the aorticians.
5. Resulting in palliation when the aortic aneurysm in remission ruptures and there are no readily available open-capable surgeons experienced in rescuing these patients. This happens. Don’t let it happen to you.
Various solutions have been broached including regionalization of aortic aneurysm care, superfellowships in exovascular surgery to complement the widespread endovascular training, and going back to open aortic surgery as the norm as had been proposed controversially in the UK. There is no turning back the clock. The moment that Dr. Parodi combined an aortic graft with Dr. Palmaz’s stent, a quantum leap occurred. The operation of aortic aneurysm surgery was changed from a challenging operation mastered by a few to a straightforward procedure performed by many.
Interesting to me is that illustration at the top of the post is of a common observation – the obliteration of the aortic aneurysm sac around a Guidant Ancure stent graft. When the sac disappears, it is as close to a cure that you can get. For some reason, I see this more frequently with Ancure than with other grafts over the past twenty years.
Odd fact -I may have been the last surgeon to implant an Ancure in the world. In 2003, I was treating a AAA with an Ancure graft when the delivery system froze in mid deployment. I called Dr. Dan Clair away from some meeting, and he called for pliers, screw drivers, and a saw, and after deconstructing the delivery system, deployed the graft and returned to his meeting with nary a word. The Guidant rep, who had been on the phone, looked up with saucer eyes, and said, “Wow. They’ve pulled Ancure off the market.”
I think it is because of the design, which is now off the market. When stents are sewn to cloth, the needle holes leak, and leak particularly where the stent graft makes a turn, stretching the suture hole. Junctions and seams leak. The Ancure, aside from the stents at top and bottom in the seal zone, has no such holes as it is unsupported and manufactured as a single piece with no junctions or seams. It is the closest you get to sewing in a graft by open surgery. If it weren’t for its overly complicated delivery system which was its downfall, I think it would be in its third generation with visceral branches that are created off the textile machines rather than joined inside the patient. There are lessons to be learned from this abandoned tech.
I believe a treat once and walk-away cure is achievable in EVAR. The idea is not to be satisfied with anything less than a cure, anything that ends with aortic aneurysm in remission. We have to understand we have chosen a path of iteration and continuous but slow improvement in the EVAR space. The front end benefits of EVAR are clear but it is in the long term we have to focus. Until then, warranties would be great.
The patient was a 50 something year old man who I took care of in 2016 before I left for Abu Dhabi. He had a background of hypertension, hypercholesterolemia, and IDDM with chronic immunosuppression for rheumatoid arthritis. For several weeks he had rest pain in his feet and impending gangrene of his left great toe. More worrisome was the development of punched out ulcers on his groin crease resulting in weeping wounds after a bout of cellulitis. He had no palpable femoral pulses. Pulse volume recordings showed flat lines from the thigh to the feet.
CTA of the abdomen and pelvis with runoff showed aortic occlusion due to heavily calcified plaque with reconstitution of the external iliac arteries via the internal iliac arteries. The common femoral arteries were only mildly diseased and there was patent runoff.
Centerline up right femoral into aorta shows occluded aorto-iliac segment and diseased external iliac artery. Centerline up left femoral into aorta shows mirror image of disease on left side
He was one of the rare instances of chronic limb threatening ischemia due to aortoiliac occlusive disease, AKA Leriche syndrome. The added background of autoimmunity made him vulnerable to the ulcers in the groin crease, and the infections there made access challenging.
Leriche Syndrome
The choices were endovascular versus open surgical repair. The groins were a problem with recent cellulitis, immunosuppression and open wounds, but with careful prep, and coverage with Ioban, access was possible, even for stent grafting. The problem was the aortic bifurcation was heavily calcified, and manipulating this likely thrombotic material with an end stump of aorta can cause renal embolism. There was a small risk of rupture at the bifurcation and of renal failure.
Standard aortobifemoral bypass graft was out of the question because of the lack of a safely clampable aorta -there was circumferential aortic plaque below and above the renal arteries and the infections in the groins would jeopardize any prosthetic graft. You have to respect unclampable aortas but like anything else, there are ways around it (link).
Regarding the groins, during fellowship, Dr. Thomas Bower used to take the distal anastomoses to the external iliac arteries which could be exposed via short lower abdominal incisions if not through the midline incision itself, avoiding groin incisions in hazardous groins.
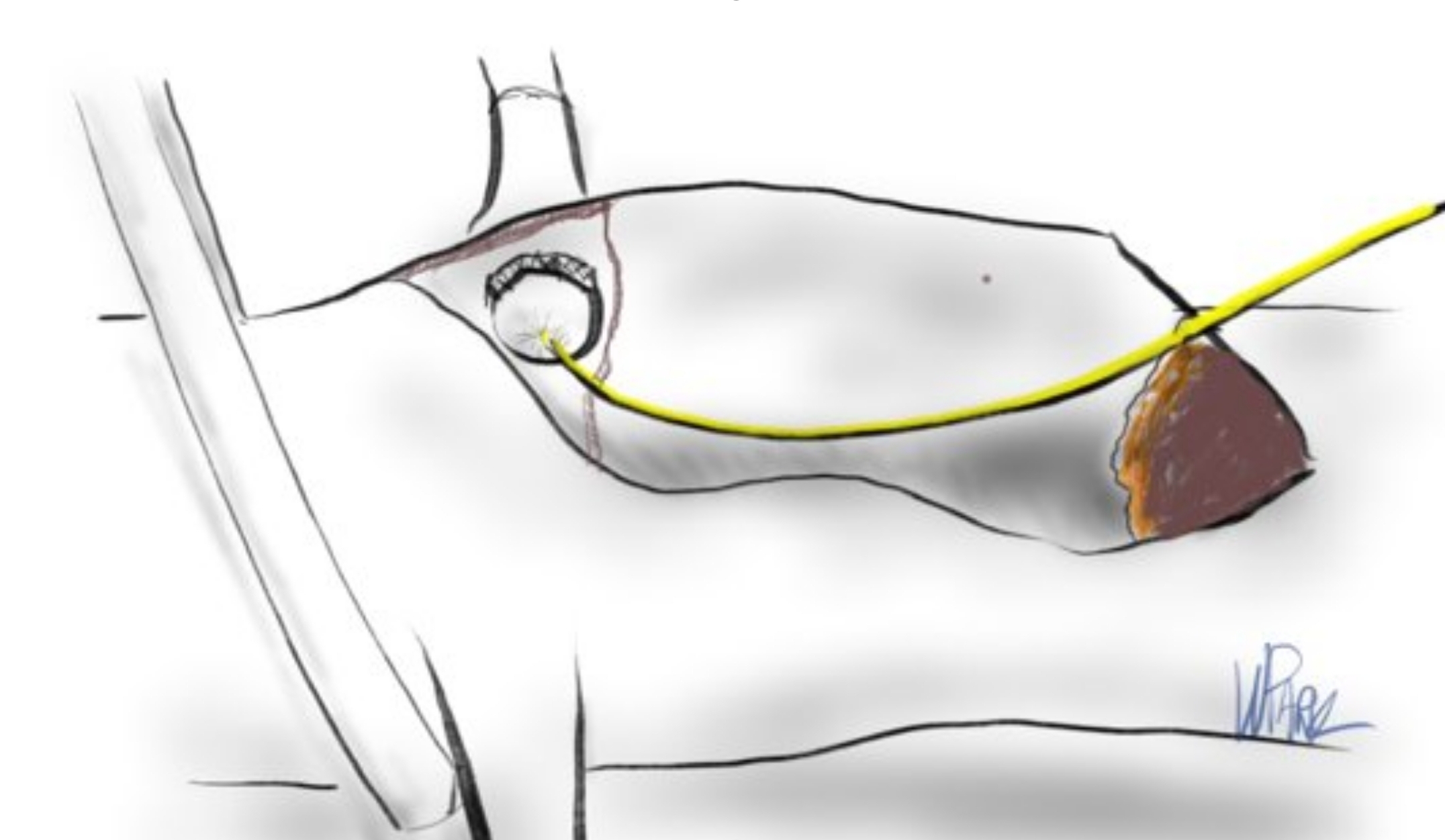
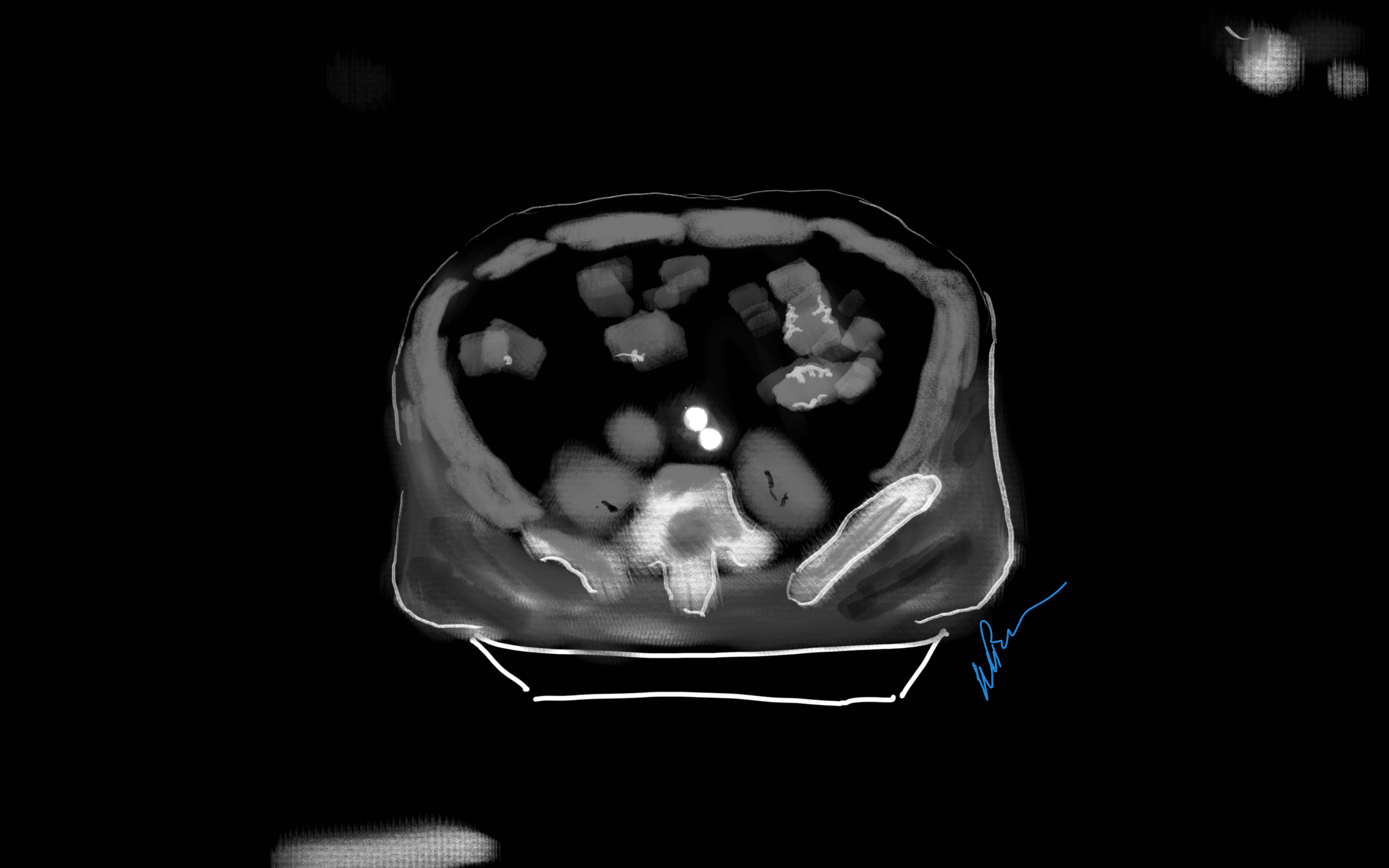
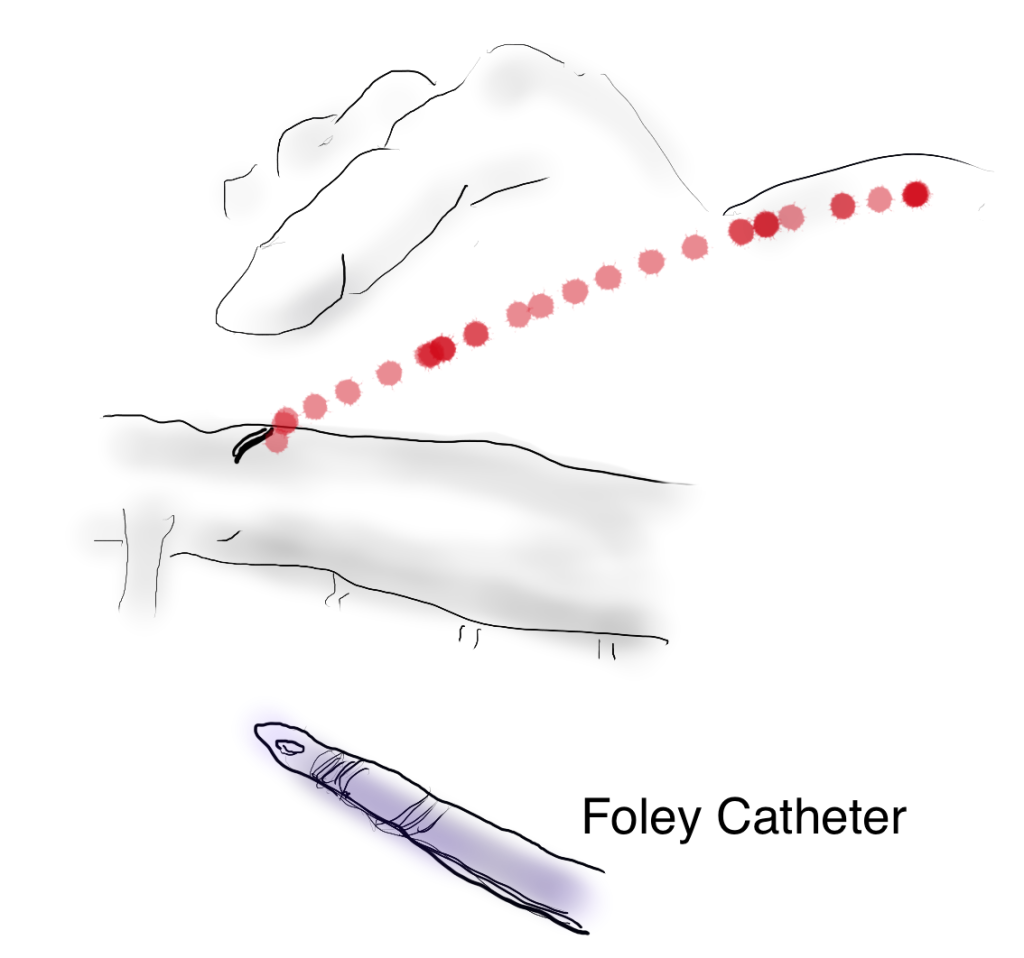
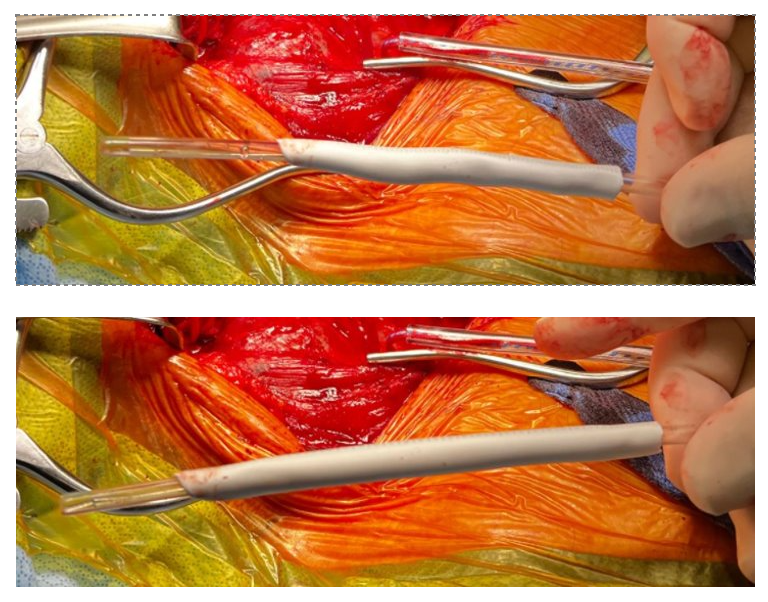
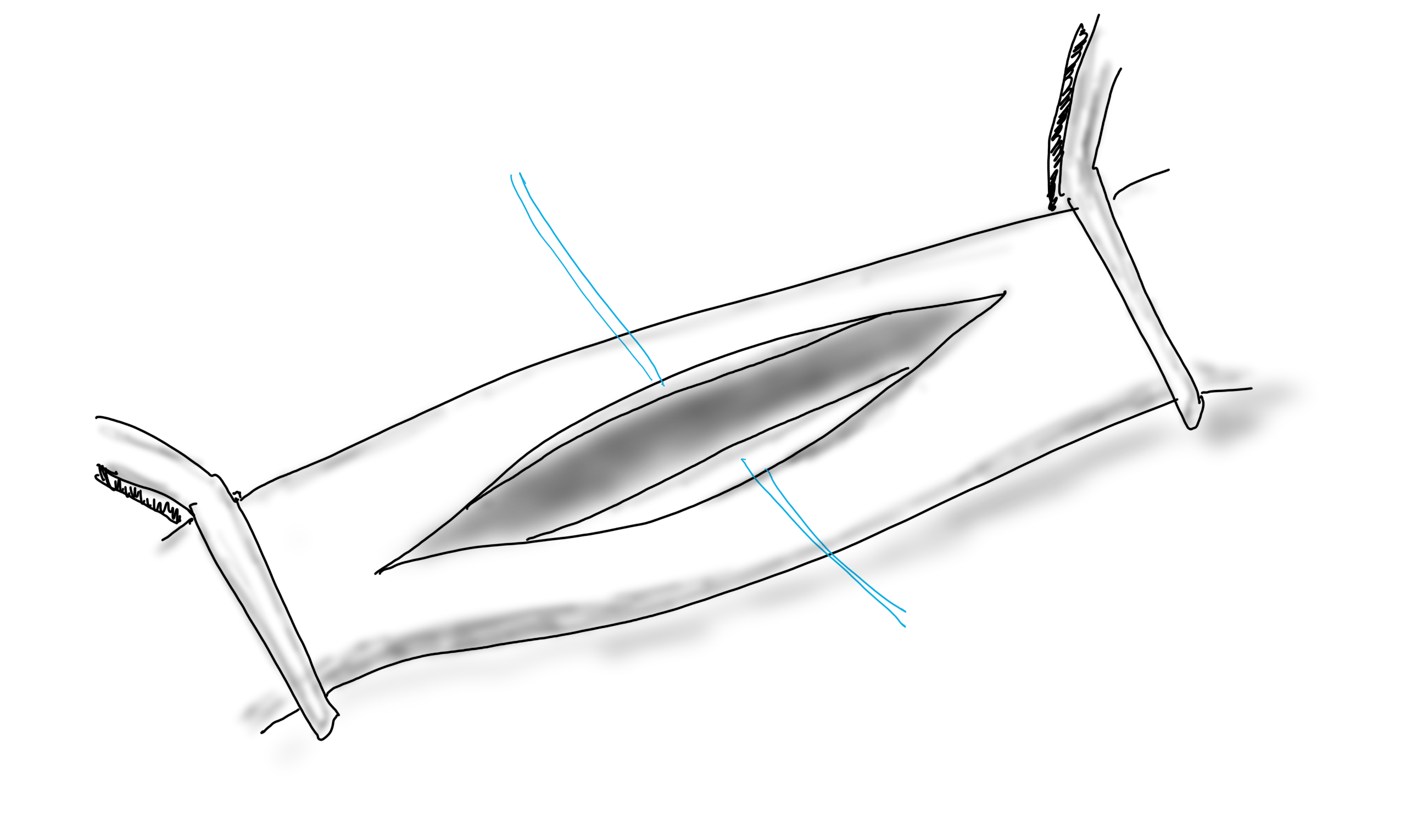
I performed an aorto-bi-iliac bypass using the balloon in the infrarenal technique after obtaining supraceliac control described in my technical post (link).
A small aortotomy can be controlled with a finger and a foley easily slipped in -just remember to clamp itThis typically provides adequate hemostasis and space to perform a proximal anastomosis
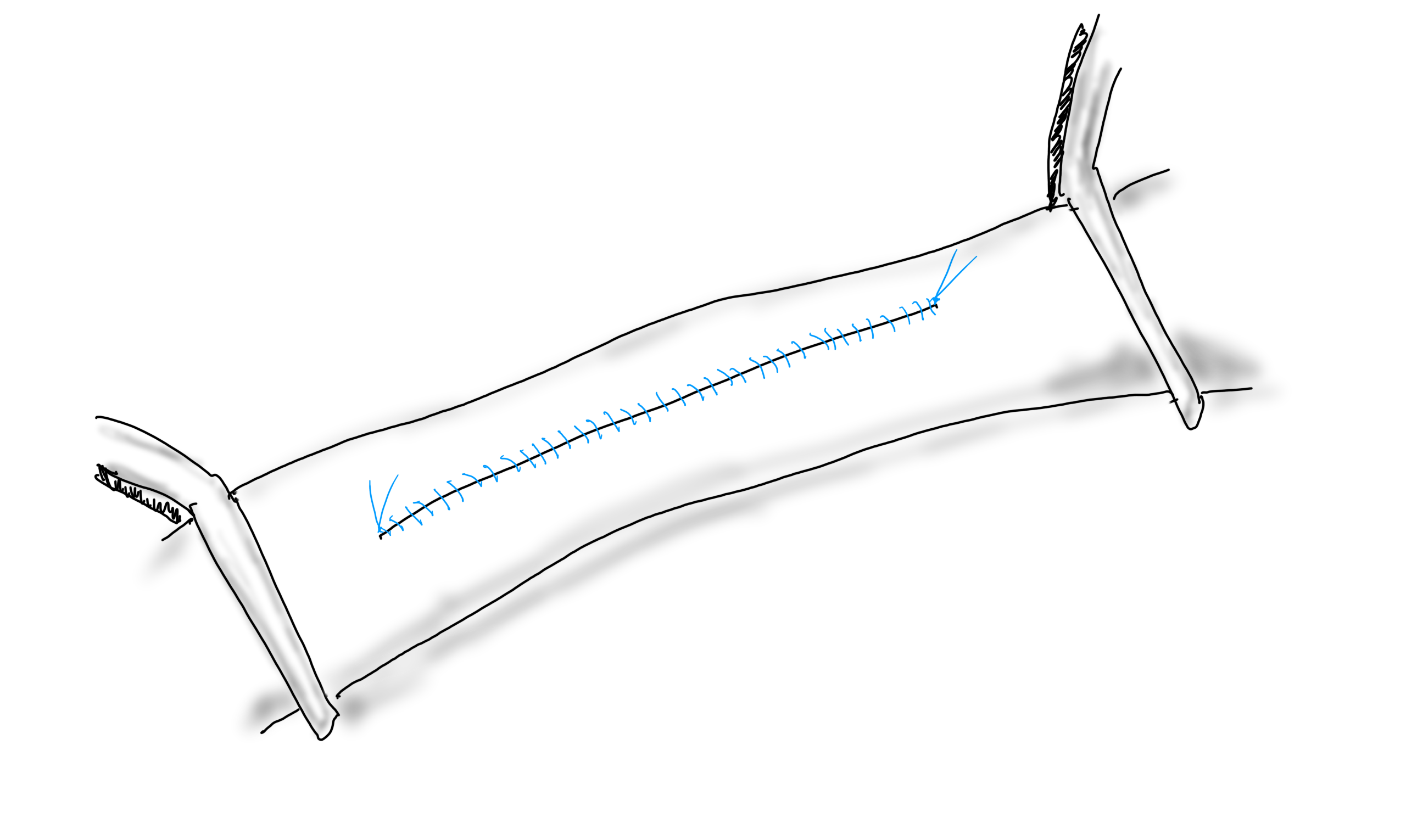
I was able to endarterectomize a nice segment of aorta and anastomose end to side -always end to side as it preserves endovascular options. The distal anastomoses was to the external iliac arteries. He did well in the immediate postoperative period but I soon left for Abu Dhabi.
In the five years since the operation, he has needed an SMA stent and has devloped worsening CKD and autoimmune diseases. But one of the gratifying things is he healed his wounds on this groins and thighs and the left hallux, and pain has never recurred. He had a contrast CT at the 5 year point (figure) showing a widely patent graft, and he sought me out when he heard that I was back in Cleveland.
His PVRs remain normal (figure).
The PVRs and ABI’s remain robustly normal even after 5 years
I’m not saying that iliac stents from the iliac bifurcation to the renal arteries was a bad option, but there is a particular sadness and weariness when I have to take care of occluded stents. As an engineer, what is worse than ballooning an occluded stent and placing another stent inside? Knowing what I know about cell biology, what is worse than lasering, drilling, cutting, that cicatricial scar tissue that is neointimal hyperplasia in terms of what you leave behind. This man still has decades left to live and he will have his bypass graft far longer than any stent. This durability, a byproduct of the technique, is a worthy virtue.
When I operated, he was in his mid fifties and despite his comorbidities, was able to undergo a big operation. Now he is in his sixties and his autoimmune issues have progressed to where he is suffering from stiff person syndrome with difficulty walking. His renal function is poor and overall he is a terrible open surgical candidate. If I had done interventions at that time, which I was tempted to, he could today be facing amputations in the setting of cytotoxic immunosuppression having run out of endovascular options.
We have lost too much to innovation. The fact is, aortic surgery for critical limb ischemia was once and it still is a thing, because it works.
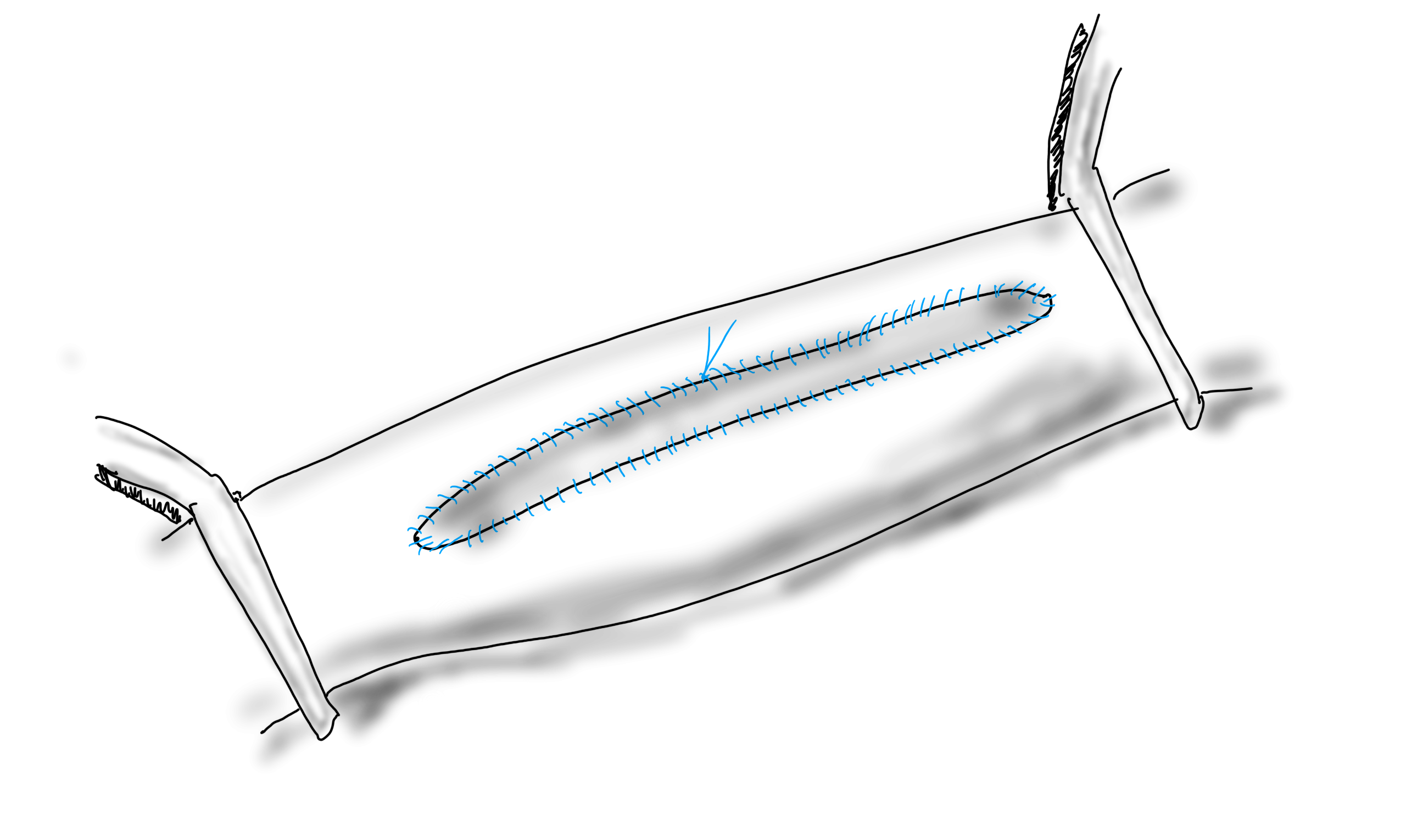
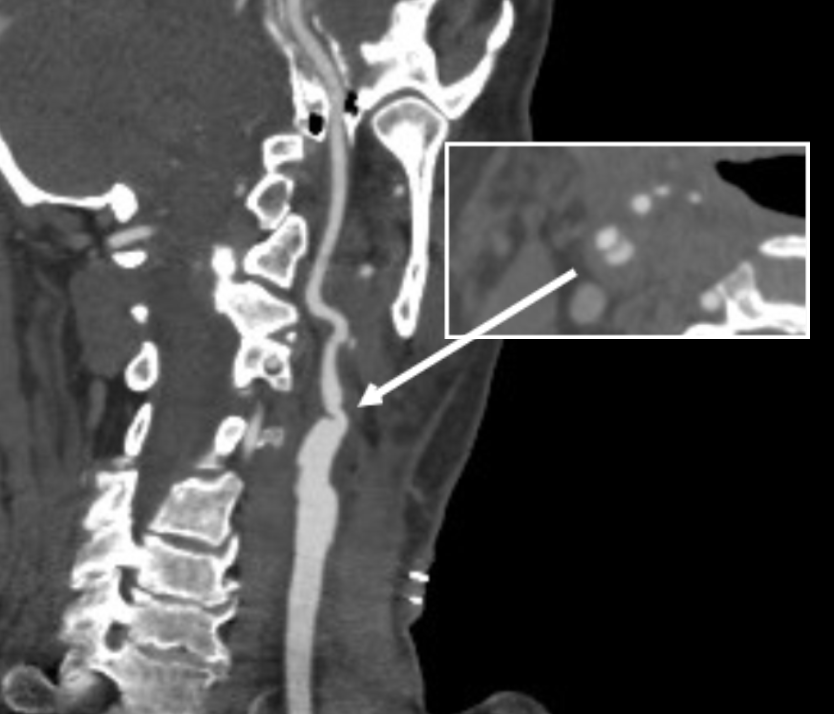
The patient is a man in his 80’s who presented with left sided weakness and dysarthria. Over 25 years before, he had undergone a carotid endarterectomy after a stroke, and had remained stroke free since. Per protocol, he received systemic thrombolysis and underwent CT angiography which revealed a right sided patch pseudoaneurysm.
Patch pseudoaneurysm with irregularities in lumenal wall of mural thrombus in right carotid bulb
This was seen dramatically on carotid duplex below.
Mural thrombus at carotid bifurcation compresses the right IJ vein
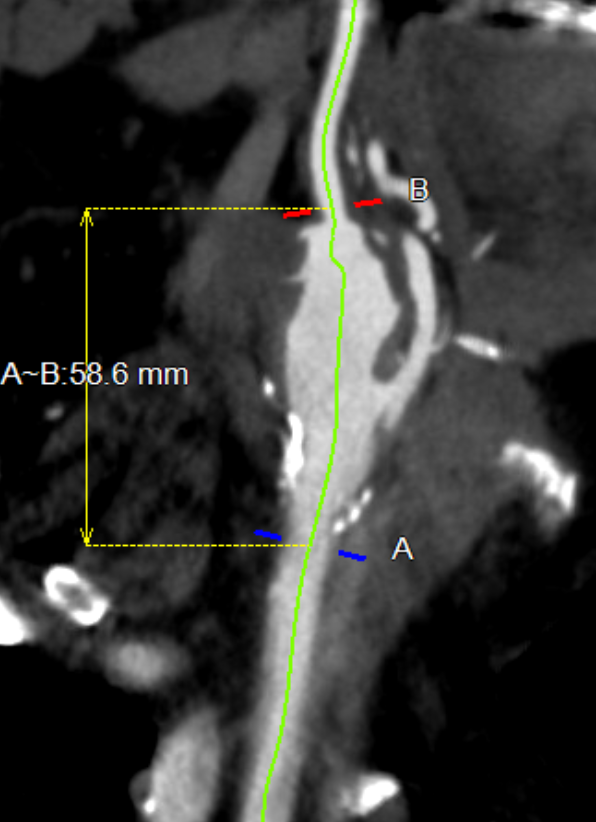
He stabilized and regained much of his function on the left arm and leg, while having a residual paresthesia of the left leg. His dysarthria resolved. His left carotid system was affected by a severe stenosis confirmed on MRA.
Duplex confirmed a tight stenosis of the left ICA with biphasic flows in the ECA.
MRI confirmed a right hemispheric infarction and operation was planned.
Right sided embolic stroke in MCA distribution
One of the great thing about working in a group ours is that we can bounce ideas off of each other and the consensus was for repair of the right carotid aneurysm. No mention was made of stent grafting which would have meant sacrificing the external carotid artery. I feel that the ECA provides some degree of long term insurance much like a good profunda femoral artery does for the common femoral. Shunting was considered a good idea because of the contralateral severe disease.
For me, the technical issue was the size mismatch between the common carotid artery which was around 8mm and the internal carotid which was about 4mm. Sizing for the CCA would leave a step down in lumen size that would result in increased velocities in the smaller ICA, potentially resulting in shear/turbulence/injury. Re-implanting the ECA on a 7mm PTFE graft would draw off some of that flow, but then you might end up with accumulation of mural thrombus on the graft beyond the ECA takeoff -the original problem to begin with. Looking on the shelf, I saw a 4-7mm tapered PTFE graft which was appropriately sized on both ends and would avoid the mentioned issues.
The aneurysm remained thankfully intact during its dissection
The aneurysm remained thankfully intact during its dissection, but to make sure I had control, the CCA at the base of the neck was controlled much as in a TCAR. The next step was in finding the ICA over the hump of the aneurysm and getting a vessel loop doubly around it. The ECA was easily found and controlled. I left the aneurysm alone to avoid perturbing the clot until I had the ICA clamped.
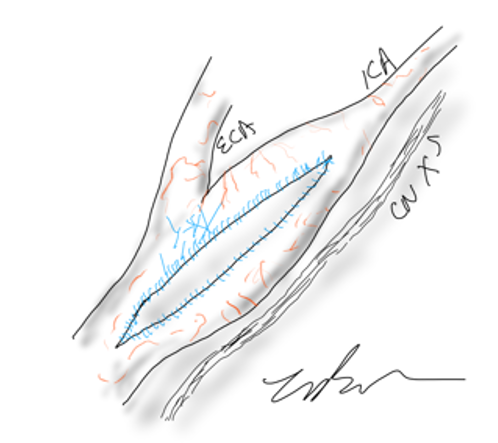
To perform the graft implantation while on shunt, I did the old trick of placing the shunt through the graft. The carotids were clamped and the aneurysm opened. The shunt was inserted into the ICA and CCA and shunt flow started. The ICA anastomosis was done first and the fit was perfect.
Stretch and unstretch, the 4mm end was tapered for the anastomosis on the ICA
The second anastomosis was end to side ECA to graft. The last anastomosis was the proximal to the CCA and it was completed loosely to allow the shunt to be removed then closed after flushing.
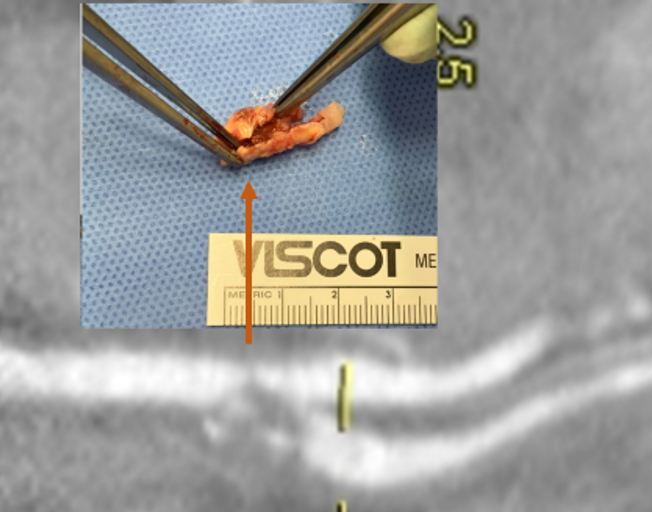
After completing the repair, the aneurysm was explored by my chief resident Dr. Shashank Sharma, who will continue his training in vascular surgery at Houston Methodist next year, and the patch was retrieved. It was sterile.
The patch, retrieved floating in the lateral part of the pseudoaneurysm, appears to have been cut from its original configuration
Back in the 90’s, when I was a resident at Roosevelt Hospital in New York, I scrubbed in on a carotid operation. Dr. Eric Moore, among the first generation of general surgeons to train in a vascular surgery fellowship, was operating. The patient was billed as having a rare carotid aneurysm but in fact had a patch pseudoaneurysm. What was lost on me at the time as we dissected out the dilated bloated artery and replaced it with a graft was the complication was a consequence of the choices made at the carotid endarterectomy done years past. The aneurysm would not have been possible if a saphenous vein patch hadn’t been placed. After resecting the aneurysmal carotid artery, we cut it open. It was lined with the yellow and green mush outside a layer of hard brown laminate thrombus, a kind of AAA in miniature. Dr. Moore muttered, “we should write this up,” and I thought about it briefly, but couldn’t get excited. Now a quarter century later, I am interested because it is poorly studied.
When you open an artery, you eventually have to close it (figure1).
A longitudinal arteriotomy
If the arteriotomy is in a transverse orientation, you can simply close it because all the sutures can be placed in the axis of flow. This is an important concept when sewing anastomoses -the sutures at the heel and toe need to be placed aligned with the longitudinal axis of the artery. This may shorten the artery but never narrows it. Any suture placed with a bite length of x with an angle θ away from the direction of flow narrows the artery by 2x(sine(θ)). The problem with primary closure, particularly of a small artery is that it narrows the vessel, decreasing the circumference by x, the length of the bite.
Primary closure narrows the artery…unless the adventitia stretches after endarterectomy.
You can sometimes get away with it because after endarterectomy, the adventitia may stretch and accomodate the bites without loss of circumference. To avoid this, since time immemorial, we have been taught that a patch should be applied.
Appropriately sized patch prevents narrowing, but also prevents excess widening
If the suture’s bite is 1mm on both patch and arterial wall, to have no effect on the artery in terms of narrowing or excessively widening the vesssel, the patch theoretically needs to be no wider than 2mm. For the purposes of handling, a wider patch is desired, so let’s say the ideal patch should about 5mm wide. Unfortunately, the precut carotid patches, both bovine pericardium and Dacron, are in the box pre-cut up to 8mm in width. A slim 5mm patch is available in Dacron but who sews in Dacron patches?
Is 8mm too wide? In some patients I believe it is.
Sometimes, the precut patch that is 8mm wide is too big, adding up to 50% to the circumference on a small artery, therefore 50% to the diameter, making the artery aneurysmal. If you see this, you should correct it.
When an 8mm wide patch is sewn on to an ICA at the carotid bifurcation which is 6mm wide, about 6mm is added to the circumference, which results in adding 2mm to the diameter, or 33%. 133% is close to the 150% which is the definition of an aneurysm. There are animal models of aortic aneurysm which involve sewing on a large bovine pericardial patch. While reading carotid ultrasounds, it is not uncommon to come across patient’s after carotid endarterectomy whose patched segments are lined with thrombus, the identifying marker of an aneurysm (picture below).
Patient post carotid endarterectomy over a decade ago now has clot lining a carotid patch aneurysm
The image above is a late presentation in a patient who is asymptomatic of stroke -am observing for now as I have just performed an eversion endarterectomy on the other side. Reading many ultrasounds, on occasion, I will see thrombus-like material accumulating on a patched artery early. And every once in a while, you come across an awkward, oversized patch such as this:
This patch is oversized but also ends where the left ICA makes a sharp turn, something you see more often on the left than on the right. This CT was taken after the patient had a postop TIA and may have formed emboli in the cul-de-sac created by the patch. DAPT was started.
I am not advocating primary closure. It is well established that primary closure of carotid arteries is associated with increased rates of stroke and restenosis in multiple studies and meta-analyses (ref 1), but there are surgeons who still close primarily.
Dr. Matthew Menard (ref 2) et alia found, along with the primary finding greenlighting bovine pericardial patch for the rest of us, that patch pseudoaneurysms are exceedingly rare. I do wonder if each of the ultrasounds were checked for the development of mural thrombus in the followup period. And what do you do about it?
Technically speaking, I advocate developing a sense of beauty when looking at the final product of an endarterectomy. I am not advocating trimming the patch all the time, but I frequently do, but rather to purposely tailor the repair well to recreate the sizes and dimensions that the body originally intended to have.
Patch angioplasty, using bovine pericardium, full width accommodated from about the time the Menard paper came out, taken on an iPhone 3.
Or you can do an eversion endarterectomy and avoid the problem entirely.
Postop 1 month post eversion endarterectomy duplex above shows a normal ICA with very little evidence I was ever there
When I was a young attending at the Allen Pavilion of Columbia Presbyterian Hospital, I was called into an operating room for a stat consult on a patient about to undergo a cholecystectomy. During the case, the IV had infiltrated and a bag of saline had filled the patient’s hand and forearm with saline, causing the hand to look like an inflated glove. The fingers were cool and white and the edema was firm but yielded to touch.
I elevated the hand and firmly squeezed the edema out of each digit, then gently massaged the edema from the hand onto the forearm. From there, I pushed the edema onto the arm. I then wrapped the hand up in an Ace wrap, and suspended it from an IV pole and returned to my case. Later, I returned and the hand was restored, warm, and perfused.
The lymphatics serve to move extracellular fluid (link). They can be overwhelmed much as drainage from a house can be overwhelmed resulting in puddles and ponds (link). This extracellular space has been “discovered” to be a new organ, but vascular surgeons have known about it for some time. Ultrastructurally, it is very close to a sea sponge with lattices of structural protein connecting cells to form tissues. And like a sea sponge, the salty water can be squeezed out or drained using gravity.
In olden times in central Europe, if you had chronic leg ulcers, you went to abbeys that specialized in their care. There, nuns would milk the edema out of your leg swollen typically from parasites and dress the leg and ulcer in linen cloth soaked in special oils. This is how Dr. Paul Gerson Unna came up with his eponymous Unna’s Boot, substituting Zinc Oxide paste which created a bacteriostatic environment.
Professor Paul Gerson Unna
Every year or so, I will be consulted for what I term a lymphatic emergency. A subset of this is phlegmasia. Whatever color you find -alba (white) or cerulea (blue) is really no matter -who really knows which comes first? It is an emergency in that the time clock for arterial ischemia -minutes to an hour for nerves, an hour to 6 for skeletal muscles, 6-12 for skin and bone, are all in play. The instinct is to go right to fasciotomy, but what you are usually doing is releasing the extracellular space, and the muscles are typically fine, even though their compartment pressures were very high.
Take this patient who developed severe upper extremity edema in the recovery phase after a cardiac arrest.
The ICU staff noted the had discoloration about four hours after the arrest. There were no arterial pulses and the forearm and hand were rock hard, the finger tips ice cold. Compartment pressures measured using the arterial line and needle method didn’t drop after the initial flush of saline below 70mmHg. While I could have been justified in performing upper extremity fasciotomy and even trying thrombectomy in a critically ill, coagulopathic patient on multiple pressors, I could just as easily have been on solid ground for saying the life was more valuable than the dominant hand. Both would have been the wrong move.
I performed the nun’s milking maneuver mentioned at the beginning and lacking an Unna’s boot, I compressed and elevated the best I could with double gloving using a small sized glove and ACE wrap.
Notice the edema has segregated into the arm.
In the morning, taking down the dressing, and re-compressing, there was now a radial artery signal and the fingers were a much improved color. The pulse-oximeter waveform was near normal. As an aside -the pulse oximeter uses the same technology as the digital photoplethysmography for generating toe waveforms in the vascular lab -ie. a vascular lab at every bedside! We have collected and are analyzing the data on this for publication.
The pulse oximetry waveform is the same tech as digital photoplethysmography. Cotton cast padding (Webril) and Coban wrap is a good method of compression that avoids the problems with ACE wrapping.
It’s a hard thing to not run off to the operating room in most cases because that is how we are trained, but understanding how a patient got to that point is crucial in deciding if compression alone will work. If they call you from the ER about a patient with a swollen cold foot with diminished signals, you have to figure out the mechanism. Was it arterial occlusion, rest pain, and chronic dependency of the foot that resulted in this? Typically the swelling appears late. Was it heart failure and inability to walk, resulting in the patient sitting all day in a chair that is the cause? Was it pregnancy with a DVT? Was it the deadly sin of sloth? Only in arterial occlusion in a chronic presentation would compression be contraindicate. In this ICU case, the lack of arterial signal is secondary to the swelling, not the cause of it.
Elevation alone does not manage edema well. Only hanging upside down or being in water up to your neck…
Compression is a necessary component of treating lymphedema emergencies because elevation alone may be insufficient, particularly in the leg.
Wrapping a leg is a critically, undertaught skill. Also, never cover the knee cap.
Elastic compression is ubiquitously available as the ACE wrap, but they can shift and move and roll, causing zones of excess and not enough compression. TED hose and compression stockings are definitely helpful in long term management, but with legs, compression needs to go up to the knee joint, or up to the groin, never halfway or the edema will create a line of ischemia at the end of the stocking that blisters when the stocking is removed, and can progress to full thickness necrosis. Cotton cast padding and Coban, or an Unna’s Boot may be the safest in terms of avoiding skin injury.
ACE wrapping is never taught adequately, and for it to work well and avoid injury to the skin, the wrapping has to be reapplied several times a day. It should be a prerequisite for nursing and medical student certification, as edema is the most common vascular disease.
Moving into our new home after four years out of country, I welcome an old friend from storage, but also unfortunately a health hazard, only mitigated by being fully reclinable.